 Samantha R. Philip
Samantha R. Philip Erin C. Standen
Erin C. Standen Jordan Schueler3
Jordan Schueler3 Sherecce A. Fields
Sherecce A. Fields Sean M. Phelan
Sean M. Phelan- 1Department of Psychological and Brain Sciences, Texas A&M University, College Station, TX, United States
- 2Robert D. and Patricia E. Kern Center for the Science of Health Care Delivery, Mayo Clinic, Rochester, MN, United States
- 3Department of Pediatrics, Baylor College of Medicine, Houston, TX, United States
- 4Division of Health Care Delivery Research, Mayo Clinic, Rochester, MN, United States
Introduction: Weight bias is a pervasive form of prejudice, most deeply and directly harming individuals in larger bodies. Although the mental health field strives to promote the delivery of equitable, culturally sensitive care, the prevalence and nature of weight bias in therapeutic contexts are not well understood. This scoping review examines how weight bias manifests within mental health settings and its impacts on client care and outcomes, exploring the issue from both client and provider lenses.
Methods: A total of 43 studies meeting search criteria were identified from a systematic search process.
Results: Findings indicate that mental health professionals (MHPs) hold negative stereotypes toward larger-bodied individuals. Although MHPs were less likely to report having negative attitudes, they reported a high prevalence of weight bias in their colleagues. Studies using experimental designs demonstrated that providers’ clinical judgment and decision-making were impacted by client body size, generally showing that higher-weight clients were perceived to have lower global functioning, greater pathology, and more negative attributes than lower-weight clients. When the client was described with restrictive eating disorder symptomatology, however, MHPs rated higher-weight clients as less severe and recommended less intensive treatment compared to lower-weight clients. Qualitative studies from client samples revealed experiences of weight stigma during treatment, including MHPs’ expressions of implicit and explicit weight bias, assumptions and misattributions based on the clients’ weight, unsolicited (direct or subtle) weight loss advice, and differential treatment based on size. Experiences of weight bias were harmful to the client’s therapeutic progress and undermined their trust in their provider and the mental health system at large.
Discussion: The body of evidence suggests that weight bias is a serious and significant barrier to the provision of equitable mental health treatment and mental health equity.
1 Introduction
Weight bias, defined as negative, prejudicial, or stereotypical beliefs and attitudes directed toward individuals in larger bodies is a well-documented phenomenon impacting the health and well-being of people in larger bodies (1). Prior studies demonstrate that weight bias manifests at structural, institutional, interpersonal, and intrapersonal levels, presenting across life domains (e.g., employment, education, and healthcare) and relationships (e.g., social, familial, and romantic) (2, 3). Experiences of weight stigma are associated with poor mental and physical health outcomes, including increased risk for psychological disorders (e.g., anxiety, depression, substance use disorder, suicidality) (4–6), healthcare avoidance (7), cardiovascular disease markers (4, 5), and a 60% increased risk of death (8). Weight stigma is conjectured to drive health inequities through direct and indirect pathways. The experience of weight stigma has been found to trigger the body’s physiological stress response (9); over time, this chronic stress reaction can increase the allostatic load (10), which is associated with worse health outcomes (11). In medical settings, weight bias is theorized to drive adverse health outcomes through healthcare providers’ biased decision-making and the corrosive effects of provider bias on the patient-provider relationship, leading patients to seek new providers, delay care, or avoid healthcare altogether (12).
When individuals who have experienced stigmatization present to therapy, mental health professionals (MHPs) must understand that clients’ mental health challenges may have been caused or exacerbated by experiences of discrimination (see Meyer and Frost; 13). This recognition represents a facet of cultural competence, which is a core aspect of mental health training programs that is acknowledged in the ethics codes across disciplines (e.g., APA, ACA, NASW, AAMFT). Cultural competence emphasizes self-awareness, knowledge, and skills as a foundation for the provision of high-quality mental health services to individuals of diverse backgrounds (14). Indicators of cultural competence are associated with positive therapeutic outcomes (15). In contrast, perceived microaggressions—defined as “commonplace daily verbal, behavioral, or environmental indignities, whether intentional or unintentional that communicate hostile, derogatory, or negative insults to a target person or group” (16), are negatively associated with therapeutic processes (e.g., therapeutic alliance, perceived cultural humility) and therapeutic outcomes (e.g., improvement in mental health outcomes, satisfaction, and psychological well-being) (17).
Concerningly, the literature indicates that mental health training programs rarely address issues related to weight, including education on weight bias, the complex interaction of factors that influence weight, and how to work with higher-weight clients who struggle with body image or desire to lose weight (18–21). For example, marriage and family therapy trainees, faculty, and clinicians reported that they had not received training on how to effectively work with higher-weight clients, despite treating them in practice (21, 22). Furthermore, a textbook analysis of graduate-level multicultural textbooks revealed that topics of weight stigma and body size as a diversity issue were only addressed in a minority of textbooks, and when addressed, were done so minimally (23). A qualitative study among mental health trainees found that they desire weight bias training to be folded into diversity courses, or to be integrated more broadly throughout training, similar to how identities like race, gender, and sexual orientation are consistently considered (21).
The apparent lack of training on weight bias and weight-related considerations in mental health training programs increases the likelihood that MHPs’ existing biases—shaped by prevailing cultural messages equating weight with health and morality—are left unexamined and unchecked. Indeed, studies indicate that mental health professionals hold weight bias (24–26) and that this bias is perceived by higher-weight individuals (27–29). Drawing from the sizable body of literature in the medical field documenting the detrimental effect of healthcare provider bias on the patient-provider relationship and patient outcomes (7, 30, 31)— and extrapolating from the documented impact of race-based microaggressions on the therapeutic relationship and outcomes (17)— we conjecture that MHPs’ biases may interfere with the therapeutic alliance and treatment progress, potentially reducing individuals’ engagement with mental health services altogether.
The purpose of this scoping review was to examine how weight bias manifests within mental health settings and its impacts on client care, experiences, and outcomes. Specifically, our research questions are: (1) To what extent do MHPs hold bias against higher-weight people? (2) How does provider weight bias influence clinical judgments and decisions? (3) What are the common manifestations of provider weight bias from the client perspective? And (4) What is the impact of perceived provider bias on client experiences? As an emerging body of literature, this scoping review provides a broad overview of the state of the evidence from both client and MHP perspectives. Unless otherwise specified, the terms “mental health professional” and “provider” are used interchangeably to describe psychologists, psychiatrists, therapists, mental health social workers, counselors, and trainees within these fields, and the term “client” is used to describe individuals who received mental health services.
2 Methods
To conduct our scoping review, we utilized the methodological framework put forth by Arksey and O’Malley (32). The four stages after identification of our research questions include: identifying potentially relevant studies, study selection, charting the data, and collating, summarizing, and reporting the results.
2.1 Literature Search
Key terms were identified to locate studies relevant to the research questions. The following search terms were used: [“weight stigma” OR “weight bias” OR “weight-based microaggression” OR “body size” OR “anti-fat” OR “fat-phobia” OR “fat phobia”] for weight bias, [“therapeutic setting” OR “therapy” OR “mental health treatment” OR “mental health provider” OR “psychologist” OR “psycholog*” OR “social worker” OR “counselor” OR “marriage and family therapist” OR “treatment” OR “milieu” OR “residential” OR “higher levels of care” OR “intensive outpatient” OR “day program” OR “psychological intervention” OR “rapport” OR “clinic”] for mental health settings. The search terms were entered into the databases, combined with the term “and.” To be included, the article needed to be empirical, in English language, and published before December 2024. Review articles and other secondary sources were excluded to ensure the analysis of primary data.
2.2 Databases
Five databases were utilized to identify relevant articles: PubMed, APA PsycInfo, ERIC, MEDLINE, and ProQuest eBook Central. PubMed and MEDLINE—both premier resources for biomedical literature—offered access to peer-reviewed research with strong medical relevance (e.g., from medical, psychiatric, and public health journals), providing studies focused on weight stigma in psychological or psychiatric treatment. We utilized APA PsycInfo as a comprehensive resource for peer-reviewed scholarly literature in psychology, providing access to literature focused on behavioral science and mental health, which were of high relevance to our search. ERIC, a database for educational literature, provided empirical literature related to weight bias in educational and training contexts, ensuring that our review included trainee samples. Finally, ProQuest eBook Central provided access to scholarly books, dissertations, and theses, allowing access to essential grey literature rounding out the body of empirical research.
A total of 11,035 articles were found using the above search terms and databases and were imported into Covidence, a tool for conducting reviews and meta-analyses of the literature.
2.3 Study selection
Five independent reviewers screened titles and abstracts. Each title and abstract were reviewed independently by two reviewers, and conflicts were discussed and resolved by consensus between reviewers with reference to pre-defined criteria. If conflicts persisted, the first author was prearranged to make the final determination, but consensus was reached on all cases. The remaining articles were then subject to a full-text review, by which two independent coders read the full text and determined eligibility. Again, conflicts were resolved through discussion and consensus. Articles were included if they were original studies that examined the presence or impact of weight bias in MHPs, or the experience or impact of weight bias experienced by individuals in mental health settings. Articles were excluded if they did not explicitly measure weight bias in mental health settings or MHPs, or if they were not original research papers (e.g., reviews, perspective papers). Quantitative and qualitative studies were included. This process identified 37 suitable articles. Six additional articles were found as part of the researchers’ library or located in the reference lists of relevant articles. A PRISMA flow diagram (see Figure 1) depicts the process and reasons for which studies were included and excluded.
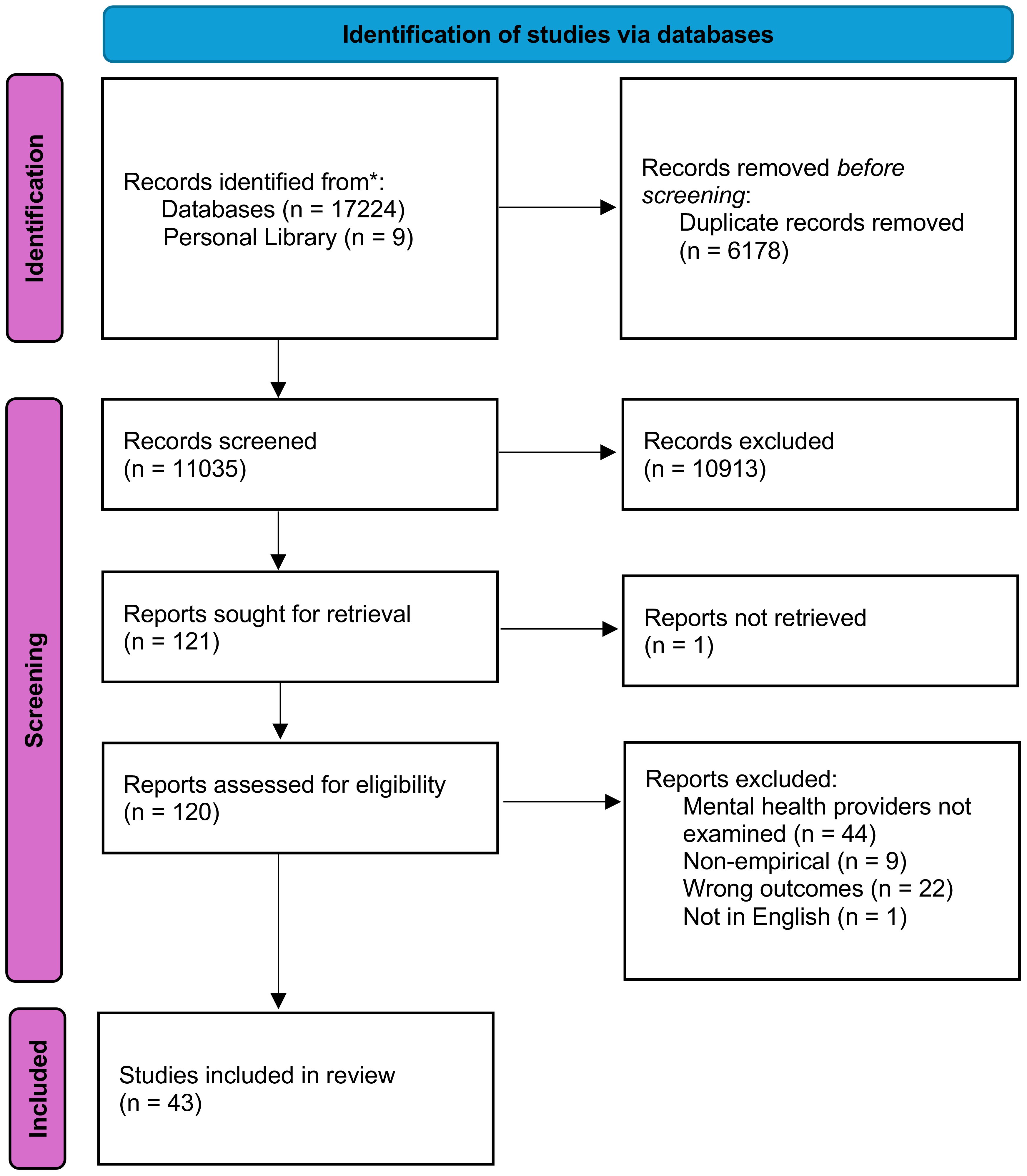
Figure 1. PRISMA flow diagram of identification of articles. Three studies were published as both dissertations and journal articles; each was only counted once.
2.4 Data charting, collation, and summarization
Data was extracted from each of the identified studies using a Covidence data extraction form modified by the study authors. As our scoping review did not examine intervention studies, we removed all intervention-related details from the template extraction form (e.g., interventions, comparators, exposures, etc.). To capture experimental studies that used a manipulation (e.g., manipulating vignettes by client body size), we inserted a textbox question about manipulation details. Additionally, as our scoping review included studies of qualitative, quantitative, and mixed methodologies—and therefore varied outcomes (e.g., qualitative themes, self-reported measures)—the “Results data” section of the original template was modified to create 15 textbox responses by which study authors could input up to 15 key results from the manuscript.
The charted data included authors, year of publication, study location, study aims, manipulation details (if applicable), study design, study population, sample size, demographic information, outcome measures, and key results. Each step was extracted by two independent study authors to ensure reliability. The data were then thematically organized using deductive followed by inductive qualitative coding scheme. First, a top-down, or deductive, approach was used to create higher-order codes (i.e., by perspective, study design, and context). Next, a bottom-up, or inductive, approach was used, in which all themes and findings were extracted from each study. From there, categories were created by grouping studies with like-themes/findings together.
3 Results
3.1 Characteristics of Included Studies
The majority of included studies were based in the United States [n= 37 (86.0%)], with the remaining studies based in other nations (i.e., Canada, Netherlands, France, Mexico; [n= 4 (9.3%)] or international samples [n= 2 (4.6%)]. Most studies used observational methodologies [n= 18 (31.9%)], followed by experimental [n= 11 (25.6%)], qualitative [n= 10 (23.3%)], mixed methods [n= 3 (7.0%)], and quasi-experimental designs [n= 1 (2.3%)]. Of the three mixed methods papers, we only extracted data from the qualitative portion for two (33, 34) as the quantitative data in these studies were not relevant to our research question.
Most studies included mixed-gender samples [n= 34 (79.1%)], and the remaining studies included female-identifying participants only [n= 2 (4.7%)]. One study (2.3%) used two samples, one with only female participants, and one mixed sample, and six studies (14%) did not report participants’ gender. Approximately two-thirds of studies examined weight bias in samples of mental health professionals [n= 29 (67.4%)] and one-third sampled from mental health clients [n= 14 (32.5%)]. For study characteristics and key results for MHP and client samples, see Tables 1 and 2, respectively.

Table 1. Characteristics and key findings of 29 studies examining provider weight bias in MHP samples.
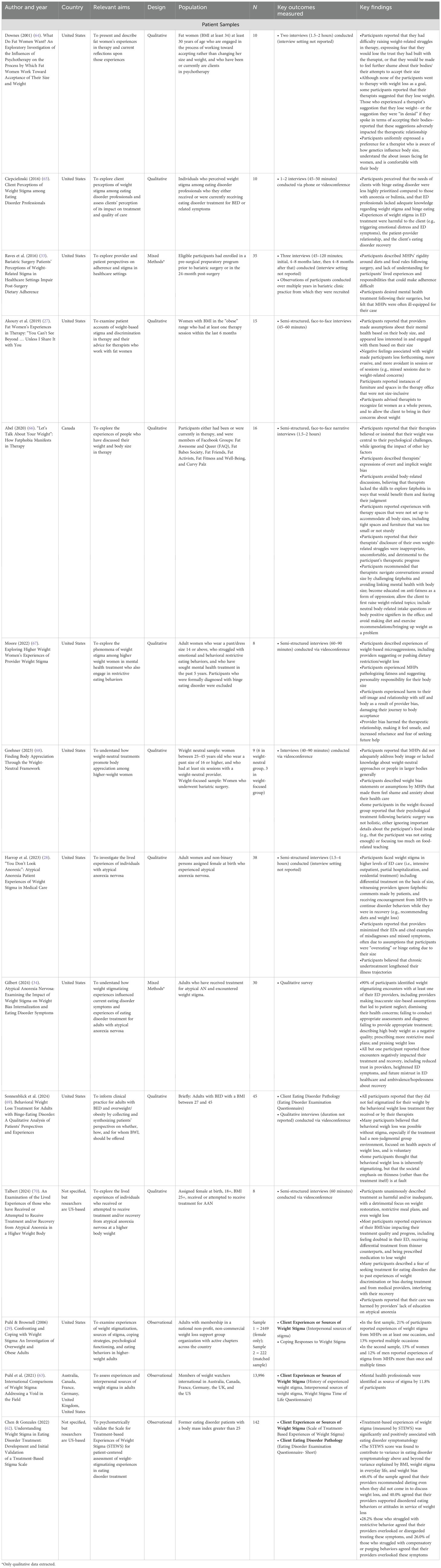
Table 2. Characteristics of 14 studies examining provider weight bias in client samples.
3.2 Findings from MHP Samples
3.2.1 Experimental studies
A total of eleven experimental (35–46) and one quasi-experimental (40) studies evaluated the impact of client body size on clinical decision-making in MHPs. Of the 12 total studies, nine described a client with general mental health challenges, and three described a client presenting with eating pathology. These categories are summarized separately due to the unique manifestations of weight bias in an eating disorder context.
3.2.1.1 Impact of body size on perceptions of general psychopathology
Seven of nine studies (35, 36, 38–41, 45) measured the MHP’s perception of the client’s psychological severity and examined differences by weight condition. Four studies found that higher-weight clients were assigned greater psychological severity than lower-weight clients (35, 36, 38, 39). One study found the opposite trend, with the lower-weight condition being assigned greater dysfunction than the higher-weight condition (40). Two studies found no difference in perceived symptom severity across weight condition (41, 45).
Six of nine studies (36–38, 40–42) assessed MHP’s provisional diagnosis and/or treatment goals for the client. Four studies found differences by clients’ described body size, including higher-weight clients being more likely to be diagnosed with an adjustment disorder when lower-weight clients were more likely to be diagnosed with relational problems (38); an eating disorder when average-weight clients were more likely to be diagnosed with an adjustment disorder (37); and moderate or severe MDD (42). Further, respondents were more likely to indicate “increasing sexual satisfaction” and weight loss as treatment goals for clients described as “fat” or “obese” (37, 41). Two studies did not find differences by client body size (36, 40).
Five of nine studies (35, 36, 38, 40, 41) measured symptom attributions that MHPs made about the described client. Four of the studies demonstrated that higher-weight clients were rated more negatively than lower-weight clients (38), such as being rated higher on symptoms including agitation, emotional behavior, impaired judgment, and inadequate hygiene (35), being rated less attractive and more embarrassed (36), or being described as suffering from a personality disorder or possible emotional, physical, and/or sexual abuse (40).
Four of nine studies (35, 40, 41, 45) measured the MHP’s interest in working with the client. Across studies, no significant differences were found based on client body size. One observational study also found no differences in provider preference or interest in working with clients based on body size (47). One study found significant differences on a subscale measuring the MHP’s belief in the client’s ability to achieve their therapy goals, with lower-weight clients being ranked more favorably than higher-weight clients (45). Finally, seven of nine (35–37, 39–41, 45) studies measured the predicted prognosis for the client. Six studies found no difference by body size (35, 36, 39–41, 45). One study found that the higher-weight client was expected to have a longer course of treatment (37).
3.2.1.1.1 Interactions with provider attributes
Four studies examined interaction effects by MHP attributes (35, 37, 38, 41). Female providers demonstrated a higher degree of weight bias than male providers (35, 37, 38) in three of four studies. Age also emerged as a significant moderator, with younger MHPs tending to demonstrate more biased responses (35, 37) in two studies, with the opposite pattern found in one study (41).
3.2.1.2 Impact of body size on perceptions of eating pathology
All three studies (43, 44, 46) described a client with symptoms consistent with a restrictive eating disorder. Each of the studies examined how MHPs assigned diagnoses and symptoms to the client based on the client’s body size. The studies consistently reflected that MHPs were less likely to consider restrictive eating disorder pathology for higher-weight clients. For example, one study found that clients described as “overweight” were less likely to receive a diagnosis of anorexia nervosa or atypical anorexia nervosa than those described as “underweight,” (43), and another found that MHPs were more likely to label the lower-weight client with an eating disorder or possible eating disorder (46). Silbiger’s (2024) study also demonstrated that 53.2% of MHPs completely missed the presence of eating disorder symptoms in the client. Across studies, providers assigned higher symptoms of anorexia to the lower-weight client compared to the higher-weight client conditions (43, 44, 46).
All three studies assessed providers’ judgments surrounding treatment planning and/or referrals. Across studies, higher-weight clients were perceived as needing less care, with providers recommending fewer treatment sessions (43), being less likely to schedule a medical follow-up (44, 46), and being less likely to be recommended specialized eating disorder treatment. Relatedly, McAshan’s (2018) study found that the lower-weight client’s eating disorder was perceived as significantly more severe than the higher-weight client’s (44).
3.2.2 Observational studies
Sixteen studies used observational methodologies to examine the presence of provider weight bias (25, 26, 42, 47–59), 13 of which measured explicit weight bias in MHPs (25, 26, 42, 48–54, 56–59). Two of the aforementioned studies also examined MHPs’ feelings of competence for working with larger-bodied clients (49, 54). One observational study (47) examined MHPs’ ranked preference for working with clients based on body size; these findings were described above given the stronger conceptual fit.
3.2.2.1 Prevalence of explicit weight bias
Evidence of weight-stigmatizing beliefs and attitudes in MHPs emerged across the 13 studies (25, 26, 42, 48–54, 56–59) measuring anti-fat attitudes. Multiple studies found evidence of MHPs endorsing negative stereotypes about higher-weight people (42, 49, 50, 52, 56, 59), and some found evidence of MHPs’ endorsement of negative attitudes toward higher-weight people or clients (56, 57, 59), though providers endorsed negative attitudes at low rates relative to their endorsement of negative stereotypes (51, 54, 58). In studies that compared MHPs to other medical professionals (e.g., pediatricians, GPs, nursing students), MHPs consistently reported lower levels of weight bias (25, 53, 58). Interestingly, one study found that—despite lower self-reported weight bias—MHPs reported similar levels of perceived weight bias among colleagues as in other disciplines (58). Two other studies reflected similar patterns; although MHPs endorsed relatively low levels of weight bias in themselves, they indicated a high degree of weight bias exhibited among colleagues in their field (49, 54).
3.2.2.1.1 Demographic diLerences in weight bias
Nine of the 13 above studies (26, 48–50, 52, 55–57, 59) examined differences in provider bias by gender, age, weight and related experiences, race/ethnicity, and training or experience level. Of the five studies (52, 55–57, 59) that examined how gender influenced weight bias, four studies found no differences in anti-fat attitudes or beliefs between men and women (52, 56, 57, 59), but one study found that MHPs who identified as nonbinary had lower controllability beliefs than those who identified as men or women (57). One study found that being male was associated with higher levels of weight bias (55). Two studies examined the impact of age, with one study finding that younger providers reported more tolerance for higher-weight clients (48), while another study found no differences by age (52). Three studies examined the role of racial and ethnic differences (26, 56, 57), with two studies finding that white MHPs held higher levels of weight bias than non-white MHPs (26, 57) and one study finding no differences by race (56).
Five studies examined the role of training and years of experience on provider biases, with consistent evidence that more years of experience was associated with less weight bias (26, 49, 50, 57, 59). Furthermore, one study reflected that receiving training on weight bias was negatively associated with weight bias (55). Five studies (48, 50, 52, 56, 57) examined the role of the MHPs’ weight and weight-related experiences; three studies found that weight bias was not influenced by MHPs’ BMI/perceived weight (52, 56, 57) or body concerns (57). In contrast, two studies found that weight bias was inversely related to higher BMI (48, 50), as well as a family history of “obesity”, having more higher-weight friends, and having a higher percentage of clients in larger bodies (48). One study found that MHPs with higher eating disorder symptoms observed more weight bias among their peers and providers in healthcare settings (50). One study found that MHPs who were actively attempting to lose weight endorsed more negative attitudes about treating higher-weight clients (50).
3.2.2.2 MHP preparedness to work with higher-weight clients
Two studies (49, 54) examined MHPs’ comfort working with higher-weight clients. In Lee et al.’s (2020) study that sampled clinical and counseling psychology doctoral students of APA-accredited programs, 58.2% of trainees indicated that they would feel comfortable broaching body image in a session, but 49.1% indicated that they would feel incompetent working with body image in a session. In contrast, a study sampling from eating disorder providers found that they largely felt confident (88%) and professionally prepared (84%) to provide quality care to higher-weight clients (49).
3.2.3 Qualitative and mixed-methods studies
Two studies that shed light on providers’ weight bias utilized qualitative methods (60, 61). Hedden’s (2024) study used a Q methodology to understand early counselors’ attitudes and beliefs about weight and size, while Aza’s (2009) study involved interviews with MHPs to understand their internal reactions to higher-weight clients. Both studies suggested that most providers feel compelled to help their higher-weight clients lose weight, citing concerns about health at higher body weights. Hedden’s (2024) study also revealed that a subgroup of MHPs overtly rejected the notion of fat liberation and fat-affirming care, while another subgroup disagreed with the idea of providers not assisting with weight loss and simply holding space for clients (61).
Aza’s (2009) study—focused on MHPs reactions to female clients in larger bodies—found that most providers endorsed weight bias toward higher-weight women, and experienced intense affective responses in their presence, including devaluation, fear, shame, and confusion. Some providers in the study described microaggressions they committed toward higher-weight clients, including providing higher-weight female clients with unsolicited weight loss advice (microinsult) and subtly dismissing a client’s feelings when she described a recent experience of weight discrimination (microinvalidation) (60).
Both studies also found evidence of a small subgroup of providers with weight-inclusive mindsets and practices. In Hedden’s (2024) study, the authors found that a small subgroup of providers (4 of 24) took a firm position in opposition to diets and diet culture and believed in fat-affirming care. In Aza’s (2009) study, 3 of 12 providers used size-inclusive language and described the value of normalizing and celebrating diverse body shapes and sizes.
3.3 Findings from client samples
3.3.1 Observational studies
Three observational studies examined clients’ reports of weight stigma from MHPs (29, 62, 63). Puhl and Brownell’s (2006) study included two samples. In the larger female-only sample (N=2,440), 21% of participants reported that they had experienced weight stigma from MHPs on at least one occasion, and 13% reported that they had multiple experiences of weight stigma from MHPs. In the second, mixed-gender sample where men and women were matched for age and BMI (N=222), 13% of women and 12% of men reported weight stigma from mental health providers on multiple occasions (29). In a subsequent study using an international sample (i.e., Australia, Canada, France, Germany, United Kingdom, United States) of adults enrolled in Weight Watchers International, 11.8% of participants reported experiencing weight stigma from a MHP at least once. No national differences were found (63).
The third study sampled participants with a history of an eating disorder and with a body mass index greater than 25 (62). Nearly half of the sample (46.4%) endorsed that their MHPs recommended dieting even when they did not come in to discuss weight loss, and 40% of participants agreed that their providers were in support of disordered eating behaviors and attitudes in service of weight loss. Of those who struggled with restrictive behaviors and compensatory/purging behaviors, 28.2% and 26.0%, respectively, reported that their providers overlooked or disregarded those symptoms (68).
3.3.2 Qualitative Studies
A total of 11 qualitative studies (27, 28, 33, 34, 64–70) examined experiences of weight stigma in mental health settings from the client perspective. Of the 11, six were from participants in general mental health settings (27, 33, 64, 66–68), and five (28, 34, 65, 69, 70) were from participants in eating disorder settings. Due to the unique manifestations of weight bias in eating disorder settings, these subgroups are reported separately.
3.3.2.1 Common manifestations and impacts of weight stigma in general outpatient treatment settings
Provider weight bias was described by participants as most commonly manifesting through MHPs’ subtle and overt communication around exercise, body size, and weight loss (66, 67), suggestions of personal responsibility for body size (67), nonverbal cues (e.g., appearing less interested and engaged with them; 27), and MHPs’ overemphasis on clients’ weight, leading them to mis-conceptualize clients’ challenges (27, 66–68). Four studies found that participants reported that providers made unsolicited weight loss recommendations (27, 64, 66, 67) and further doubled down on their weight loss agenda despite participants’ desire to work on accepting their bodies (66, 67). Three studies found that MHPs engaged in self-disclosure around their weight and weight-related behaviors (27, 66, 67), with one study demonstrating that almost half of the participants reported their providers self-disclosing along these lines (27). Participants from two studies reported that these self-disclosures were inappropriate and detrimental (66), making the space feel less safe for clients healing from disordered eating (67). In the two identified studies involving individuals that underwent bariatric surgery, participants reported MHPs’ over-focus on food-related teaching and rules that were not aligned with clients’ holistic needs for therapy (33, 68).
Three qualitative studies (64, 65, 68) documented the impact of perceived provider weight bias on the client and/or the therapeutic relationship. Each study demonstrated serious consequences of experiences of mental health professionals’ weight bias. Participants described how provider weight bias undermined the therapeutic relationship, making the therapeutic relationship feel unsafe, reducing trust, and increasing participants’ reluctance to seek help from future MHPs (64, 67). Additionally, provider weight bias stunted clients’ therapeutic progress, with participants describing how provider bias damaged their self-image and relationships with themselves, heightened shame and anxiety, and compelled them to question their journey of self- and body-acceptance (67, 68). In turn, participants reported feeling more disconnected from their bodies and poorer relationships with food and exercise (67).
Four studies (27, 64, 69, 70) uncovered themes related to clients’ willingness to discuss their weight with their MHPs. All four studies found that participants were reluctant to bring up their weight in therapy and/or that their weight (and associated shame or self-consciousness) made them more evasive and avoidant in therapy sessions (27, 64, 66, 68). Two studies found that participants reported explicitly avoiding or fearing having discussions about their bodies with their provider for fear of judgment or a poor reaction from the provider that could undermine trust and safety (64, 66). One study found that participants believed that MHPs lacked the necessary skills to help them in this realm (66).
Four studies demonstrated participants’ sentiments that MHPs lack sufficient training in body image and weight-neutral approaches (33, 66–68). In turn, participants felt that their body image struggles were not adequately addressed, or that they were made to feel that they were at fault for not meeting beauty standards, as opposed to being encouraged to reflect on body-based systems of oppression. In two studies, participants described frustration about their need to educate their providers on weight stigma (66, 67). Three studies found that some participants preferred working with MHPs who were also fat, as this shared identity could promote a sense of trust through joint lived experiences and understanding (64, 66, 68).
Four studies (27, 65, 67, 70) inquired into participants’ recommendations for MHPs to better service higher-weight clients in therapy. Three studies included a theme that highlighted participants’ wish for providers to be aligned with fat-positive or Health at Every Size® principles, including rejecting mainstream narratives around body size and taking a holistic, person-centered approach that recognizes the person as more than their weight (27, 64, 66). Relatedly, participants in all studies described a need for providers to become educated on weight-related matters, including the common issues faced by higher-weight people (27, 64, 65), the biological determinants of size (64), and anti-fatness as a form of oppression (66).
In terms of concrete ideas for creating more inclusive practices, participants suggested providers include body-related questions in their intakes (66)—but ask about eating in the same way that they might ask a smaller-bodied client (64)—, include body-positive and inclusive signifiers in their office space (64, 66), and ensure that their office furniture accommodates larger bodies (64, 67). Participants in one study strongly recommended against MHPs making diet and exercise recommendations (66), while some participants in another study expressed a desire for therapists to help them with their weight-loss goals (27). Generally, participants agreed that MHPs should allow clients to bring up the topic of their weight and that they should not bring up weight as a problem (27, 66). Participants in three studies emphasized the importance of providers not making assumptions about a client based on their body size–especially assuming causal links between their size and their mental health issues (27, 64, 66).
3.3.2.2 Common manifestations and impacts of weight stigma in eating disorder treatment settings
Of the five studies (28, 34, 65, 69, 70) examining client experiences of weight stigma in eating disorder treatment, three studies utilized samples who had sought or received treatment for atypical anorexia nervosa (28, 34, 70), and two studies utilized samples who had received treatment for binge eating disorder (65, 69).
The three studies focused on individuals in larger bodies with atypical anorexia found evidence of widespread encounters of provider weight bias in this setting (28, 34, 70), with 90% of participants in one study (N=30) reporting that they had encountered weight stigma from an eating disorder provider (34). While one study documented participants’ direct observation of providers describing high body weight as a negative quality (34), another study found that treatment providers did not address fatphobic comments made by other clients (28). In contrast, one study among recipients of a behavioral weight loss treatment for binge eating disorder found that participants largely denied feeling stigmatized by the behavioral weight loss treatment that they received, or by their providers (69).
One of the most common manifestations in eating disorder settings—emerging across four of the five studies—was the experience of differential treatment from treatment providers because of their size (28, 34, 70) or diagnosis (e.g., binge eating disorder vs. anorexia nervosa/bulimia nervosa) (65). Participants described a sense that their illnesses were taken less seriously, and their needs were prioritized below, their peers in smaller bodies (28, 34, 65, 70). For example, participants in one study reported that their providers viewed high weight as indicating that one is not “actually sick” with an eating disorder (34). This experience was apparent even in higher levels of eating disorder care (i.e., intensive outpatient, partial hospitalization, and residential treatment), where participants reported that providers were less likely to believe the symptoms of higher-weight clients compared to lower-weight clients (28, 34). The experiences of dismissal and disbelief were even more pronounced for individuals with multiple oppressed identities (28).
Providers’ weight bias reduced the quality of care provided to higher-weight clients, skewing their clinical judgments and the treatment offered to them. Two studies focusing on participants with a history of restrictive eating disorders found that MHPs misdiagnosed their illness or missed restrictive symptoms, instead assuming that the participant was binge eating or “overeating” due to their body size (28, 34). Both studies found evidence of provider negligence, by which they failed to conduct thorough assessments for accurate diagnosis and appropriate treatment (28, 34). These biased assumptions led to suboptimal, and even harmful, treatment decisions. Despite sharing the same symptoms as their smaller-bodied peers, participants reported receiving different interventions and care recommendations (e.g., more restrictive meal plans), and not receiving the necessary care for their eating disorder (e.g., group therapy for food restriction) (28, 34, 70). Participants commonly reported providers actively encouraging eating disorder behaviors while they were in recovery from a restrictive eating disorder, including recommending or praising weight loss and restrictive eating (28, 34, 70).
Participants from four of the five studies (28, 34, 65, 70) uniformly reported negative impacts of MHP weight bias on the therapeutic relationship and on the participant’s recovery. Provider weight bias diminished participants’ trust in treatment providers, harming relationships within and outside of the treatment team- including undermining general trust in eating disorder healthcare (34, 65, 70). These experiences interfered with client recovery in several ways, including heightened self-doubt, negative self-stigma, internal anguish (65), and greater difficulty developing a healthy relationship with food, eating, and their bodies and accepting their bodies’ dietary needs (34). Ultimately, provider stigma resulted in increased eating disorder symptoms and restriction (34, 65), which participants reported using as a means of self-protection from provider weight stigma (34). Participants in three studies described how provider stigma lengthened their illness trajectories and/or posed additional barriers to recovery, such as fear of seeking future treatment (28, 34, 70).
4 Discussion
Weight stigma is a known risk factor for reduced mental health and wellbeing of higher-weight individuals. The extent to which weight bias may appear in the therapeutic context—potentially posing further harm to client and therapeutic processes—was previously not well-defined. Synthesizing insights on this topic from both client and MHP perspectives, qualitative and quantitative investigations, and published journal articles and dissertations, this scoping review sought to comprehensively map this phenomenon and to answer the following questions: (1) To what extent do MHPs hold bias against higher-weight people? (2) How does provider weight bias influence clinical judgments and decisions? (3) What are the common manifestations of provider weight bias from the client perspective? And (4) What is the impact of perceived provider bias on client experiences? The findings of this scoping review highlight the exacerbating process by which higher-weight individuals may face further psychological harm when seeking mental health services due to provider weight bias.
We found conclusive evidence that MHPs hold weight bias toward larger-bodied individuals and clients, converging across observational, qualitative, experimental, and mixed methodologies. The findings suggested that MHPs may be reticent to disclose their negative attitudes toward higher-weight individuals, but they openly endorse stereotypical beliefs about higher-weight people (e.g., that they are insecure, unattractive, or have poor self-control) (42, 48, 54, 56, 57), and report high perceptions of bias among their professional colleagues (49, 54). MHPs reported having strong affective reactions to women of size, described examples of weight-based microaggressions toward clients, and demonstrated weight-centric beliefs (e.g., that weight is under one’s control) (60, 61).
Numerous experimental studies sought to examine how weight bias influences MHPs’ clinical judgments and decisions. Though findings varied across studies, general trends indicated that, compared to smaller-bodied clients with otherwise identical presentation, providers perceived higher-weight clients in general mental health settings as having greater dysfunction, more severe diagnoses, and more psychological challenges and symptoms (35–39). Most studies did not find differences in MHPs’ self-reported interest in working with the client or the clients’ predicted prognosis by clients’ body size. When examining this question in the context of eating disorders, MHPs consistently perceived larger-bodied clients’ restrictive symptomatology as less severe, less diagnosable, and in need of less medical attention compared to smaller-bodied clients (43, 44, 46).
Qualitative studies from client samples illustrate the manifestation and consistently negative impact of perceived MHP weight bias and weight-related discussions on client experiences and outcomes. The results suggested that many clients suffered from their MHPs’ reinforcement of the thin ideal, by which MHPs encouraged clients to lose weight without their asking, self-disclosed about their personal pursuits of thinness via diets and exercise, and made clients feel as though their bodies were “wrong” and not worthy of acceptance (64, 67). Clients described providers dismissing their key mental health concerns to focus instead on their weight, with some MHPs insisting that their weight was central to their psychological challenges or that their body was to blame for their mental health concerns or the trauma they had suffered (27, 66, 67). Other clients described experiences of providers’ equally hurtful subtle weight bias, by which they observed MHPs appearing less interested and engaged with higher-weight clients within a group therapy context (27). Experiences of MHP weight stigma induced shame, anxiety, and self-doubt, increased internalized weight stigma, reduced body trust among clients, and caused clients to question their journey of body/fat acceptance (67, 68). Furthermore, experiences of provider stigma made the therapeutic relationship feel unsafe, undermining trust in the provider and the mental health field at large (64, 67), and making it more difficult to bring up their body-related challenges in therapy.
The negative impacts of provider bias were equally, if not more, destructive in eating disorder treatment settings. As in general outpatient settings, clients reported that providers encouraged them to lose weight and engage in restrictive eating behaviors while they were actively in recovery from restrictive eating disorders (28, 34, 62, 70). Presumably based on assumptions that higher-weight clients must “overeat,” provider bias commonly led providers to overlook or doubt restrictive symptoms in higher-weight clients, fail to conduct appropriate assessments, and misdiagnose clients (28, 34, 70). In turn, clients reported that they did not receive the level or type of care that they needed. Participants consistently reported sentiments of differential treatment on the basis of body size, in which they observed their lower-weight peers being prioritized and taken more seriously (28, 34, 65). Experiences of weight stigma in eating disorder treatment settings resulted in a breach of trust between the client and their treatment providers, diminished quality of care, heightened eating disorder symptoms and psychological distress, and a lasting negative impact on eating disorder recovery by undermining clients’ trust in eating disorder healthcare generally (28, 34, 70).
The results from the scoping review also illuminated how weight bias manifests on structural levels within the therapeutic context and confers harm on the client. One example of this structural stigma emerged in clients’ reports of the therapeutic space being unaccommodating to bodies on the higher end of the weight spectrum, including tight spaces and small or insubstantial furniture (27, 66). When therapeutic settings are not set up to comfortably service all clients, it can signal to clients that they are unwelcome and pose an immediate barrier to the therapeutic work. Another example includes findings from MHP samples that reveal a lack of graduate training and sense of discomfort supporting clients with body image issues. One study demonstrated that over 75% of participants reported that bodies (e.g., weight, size, ability state) are “rarely” or “not at all” discussed within their programs (54). The lack of training on weight- and size-related issues is likely reflective of an implicit, structural-level bias, impacting the content that graduate programs deem important or unimportant. Studies from the client perspective make clear how the omission of training harms clients’ experiences in therapy; providers’ lack of knowledge and education on pertinent topics (e.g., body-based oppression, lived experiences of higher weight people) and therapeutic techniques (e.g., weight-neutral approaches) can force clients into the educator role with their therapists (66–68). This need to educate was described as frustrating and burdensome by clients (67), and often led to clients evading discussions of weight with their MHP (27, 64, 66, 68).
Through not a primary aim, several manuscripts in this scoping review sought feedback from clients about how MHPs could cultivate more inclusive and effective practices for higher-weight individuals. Participants consistently described a need for providers to become more knowledgeable about lived experiences of higher-weight individuals, including anti-fatness as form of oppression, the politics of fatness, the biological determinants of size, and how size impacts one’s experience (27, 64, 66). Frequently, participants described a desire to work with fat-affirming providers who were aligned with weight-inclusive approaches, rejecting the mainstream narratives around body size and pressures for thinness (64, 66). Participants emphasized the need for providers to avoid making assumptions pertaining to how their body size relates to their history or presenting problems (27, 64, 66) and to focus on the client as a whole person rather than assuming that weight is a central issue (27). To create an environment in which clients feel more safe to talk about their experiences in their bodies, some clients recommended that therapists include size inclusive signifiers in their office, inquire about eating behaviors in the same way they might ask a smaller-bodied person, provide size-friendly spaces and seating, and avoid bringing up weight as a problem, recommending diets or exercise, or disclosing about their personal pursuit of weight loss (64, 66, 67).
5 Limitations and future directions
The findings of this scoping review should be considered within the context of their limitations. First, we acknowledge methodological limitations inherent in the study design and execution. While our use of search tools was deliberate and broad, it is possible that some manuscripts were not indexed by any of the search tools used, and therefore not included in this review. Additionally, the use of only published literature may skew our findings toward more significant results (i.e., reflecting publication bias (71)), though our inclusion of theses and dissertations attenuates this concern.
Another methodological limitation was the omission of search terms related to psychiatrists and psychiatric behaviors. Despite not including such terms, several studies including psychiatrist samples were returned in our search and included in this review. Still, this omission limits our ability to draw conclusions about this subgroup, and particularly the impact of clients’ weight status on physicians’ prescription decisions. A review of available experimental research in this population would provide important insights into this clinical decision-making process that is highly susceptible to weight bias.
Some limitations of this review result from limitations of the available evidence. Compared to studies examining provider bias by sampling MHPs, far fewer studies examined provider weight bias and its impacts from the client perspective, and most of these studies used qualitative methodologies. The qualitative findings provided nuanced, in-depth insights into their experiences, but have some limitations to their generalizability due to the smaller sample sizes, and they do not allow us to quantify or draw causal conclusions regarding the impact of provider bias on client outcomes and treatment decisions. Additional observational studies are needed to quantify the effect of MHPs’ perceived weight bias on the therapeutic relationship and client outcomes (e.g., psychological well-being, future mental healthcare utilization). Future research should also employ experimental methodology to examine the effect of provider weight bias on relevant client outcomes.
Additionally, our search returned few studies examining MHP bias in settings other than general outpatient and eating disorder treatment settings. The field’s understanding of this issue will be advanced by expanding the examination of weight bias to encompass a broad range of clinical settings (e.g., intensive outpatient/partial hospitalization, inpatient) and modalities (e.g., individual therapy, group therapy, couples therapy) and clinical populations (e.g., mood, anxiety, serious mental illness).
Finally, given the focus of this scoping review, we did not examine how MHPs might transition to becoming more weight-inclusive practitioners. Very few interventions to our knowledge have examined the impacts of weight bias reduction interventions in mental health trainees (56, 72), and few qualitative studies have examined the personal and professional work of MHPs specializing in body image concerns (73, 74). Generally, such providers endorsed a weight-inclusive approach, acknowledging body diversity, understanding sizeism as a form of oppression, and rejecting mainstream diet culture and weight-centric beliefs about weight and health. These studies also called attention to the need to examine one’s own relationship with their bodies to best serve their clients and for more formal training within graduate school and counseling organizations. Investigating and understanding the processes by which MHPs unlearn harmful weight-based beliefs and embody weight-inclusive, harm reduction practices represent an essential area of future research.
6 Conclusions
The results of this scoping review suggest that weight bias is a serious issue in mental health settings, in need of attention and remediation. While future research is needed, it is evident that MHPs hold stigmatizing views toward higher-weight clients and that their clinical judgments and decisions are impacted by this bias. Given the negative mental health impact of weight stigma, this is especially concerning; clients may encounter the same form of stigma from MHPs that originally contributed to the development or exacerbation of their mental health challenges. The impacts of provider bias—suggested by the findings of this review— are that clients feel less safe with their providers, experience heightened mental health symptoms, are reluctant to share their true thoughts and feelings about their bodies, and are discouraged from seeking future treatment. Increased efforts in education, training, and research are needed to promote size-inclusive beliefs and practices in mental health trainees and professionals, such that therapy can be a safe and affirming space for people of all sizes.
Data availability statement
The original contributions presented in the study are included in the article/supplementary material. Further inquiries can be directed to the corresponding author/s.
Author contributions
SaP: Writing – original draft, Investigation, Writing – review & editing, Visualization, Conceptualization, Project administration. ES: Visualization, Writing – review & editing, Conceptualization, Investigation. JS: Writing – review & editing, Investigation. SF: Investigation, Writing – review & editing. SeP: Investigation, Supervision, Conceptualization, Writing – review & editing.
Funding
The author(s) declare that no financial support was received for the research and/or publication of this article.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Generative AI statement
The author(s) declare that no Generative AI was used in the creation of this manuscript.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Daníelsdóttir S, O’Brien KS, and Ciao A. Anti-fat prejudice reduction: A review of published studies. Obes Facts. (2010) 3:47–58. doi: 10.1159/000277067
2. Puhl RM, Himmelstein MS, and Pearl RL. Weight stigma as a psychosocial contributor to obesity. Am Psychol. (2020) 75:274–89. doi: 10.1037/amp0000538
3. Vartanian LR, Pinkus RT, and Smyth JM. The phenomenology of weight stigma in everyday life. J Contextual Behav Science. (2014) 3:196–202. doi: 10.1016/j.jcbs.2014.01.003
4. Wu YK and Berry DC. Impact of weight stigma on physiological and psychological health outcomes for overweight and obese adults: A systematic review. J Adv Nurs. (2018) 74:1030–42. doi: 10.1111/jan.2018.74.issue-5
5. Brochu PM. Weight stigma as a risk factor for suicidality. Int J Obes. (2020) 44:1979–80. doi: 10.1038/s41366-020-0632-5
6. Papadopoulos S and Brennan L. Correlates of weight stigma in adults with overweight and obesity: A systematic literature review: Correlates of Stigma in Adults with Overweight and Obesity. Obesity. (2015) 23:1743–60. doi: 10.1002/oby.21187
7. Alberga AS, Edache IY, Forhan M, and Russell-Mayhew S. Weight bias and health care utilization: a scoping review. Prim Health Care Res Dev. (2019) 20:e116. doi: 10.1017/S1463423619000227
8. Sutin AR, Stephan Y, and Terracciano A. Weight discrimination and risk of mortality. Psychol Sci. (2015) 26:1803–11. doi: 10.1177/0956797615601103
9. Tomiyama AJ, Epel ES, McClatchey TM, Poelke G, Kemeny ME, McCoy SK, et al. Associations of weight stigma with cortisol and oxidative stress independent of adiposity. Health Psychol. (2014) 33:862–7. doi: 10.1037/hea0000107
10. Cullin JM. Biological normalcy and body fat: Obesity prevalence, fat stigma, and allostatic load among late adolescents and young adults. Am J Biol Anthropology. (2023) 181:575–87. doi: 10.1002/ajpa.v181.4
11. Guidi J, Lucente M, Sonino N, and Fava GA. Allostatic load and its impact on health: A systematic review. Psychother Psychosom. (2021) 90:11–27. doi: 10.1159/000510696
12. Phelan SM, Puhl RM, Burke SE, Hardeman R, Dovidio JF, Nelson DB, et al. The mixed impact of medical school on medical students’ implicit and explicit weight bias. Med Educ. (2015) 49:983–92. doi: 10.1111/medu.2015.49.issue-10
13. Meyer IH and Frost DM. Minority stress and the health of sexual minorities. In: Handbook of psychology and sexual orientation. Oxford University Press, New York, NY, US (2013). p. 252–66.
14. Davis DE, DeBlaere C, Owen J, Hook JN, Rivera DP, Choe E, et al. The multicultural orientation framework: A narrative review. Psychotherapy. (2018) 55:89–100. doi: 10.1037/pst0000160
15. Owen J, Tao KW, Drinane JM, Hook J, Davis DE, and Kune NF. Client perceptions of therapists’ multicultural orientation: Cultural (missed) opportunities and cultural humility. Prof Psychology: Res Practice. (2016) 47:30–7. doi: 10.1037/pro0000046
16. Sue DW, Capodilupo CM, Torino GC, Bucceri JM, Holder AMB, Nadal KL, et al. Racial microaggressions in everyday life: implications for clinical practice. Am Psychol. (2007) 62:271–86. doi: 10.1037/0003-066X.62.4.271
17. Torino GC, Rivera DP, Capodilupo CM, Nadal KL, and Sue DW. Microaggression Theory: Influence and Implications. Hoboken, NJ:: John Wiley & Sons (2018). p. 400.
18. Bergen M and Mollen D. Teaching sizeism: integrating size into multicultural education and clinical training. Women Ther. (2019) 42:164–80. doi: 10.1080/02703149.2018.1524065
19. Brochu PM. Teaching clinical psychology trainees about weight bias. Women Ther. (2019) 42:191–9. doi: 10.1080/02703149.2018.1524066
20. McHugh MC and Kasardo AE. Anti-fat prejudice: the role of psychology in explication, education and eradication. Sex Roles. (2012) 66:617–27. doi: 10.1007/s11199-011-0099-x
21. Cravens JD, Pratt KJ, Palmer E, and Aamar R. Marriage and family therapy students’ Views on including weight bias training into their clinical programs. Contemp Fam Ther. (2016) 38:210–22. doi: 10.1007/s10591-015-9366-2
22. Pratt KJ, Holowacz E, and Walton NL. Marriage and family therapists’ Perspectives on treating overweight clients and their weight-related behaviors. Am J Family Ther. (2014) 42:364–85. doi: 10.1080/01926187.2013.878170
23. Kasardo AE. Size as diversity absent from multicultural textbooks. Women Ther. (2019) 42:181–90. doi: 10.1080/02703149.2018.1524069
24. McEntee ML, Philip SR, and Phelan SM. Dismantling weight stigma in eating disorder treatment: Next steps for the field. Front Psychiatry. (2023) 14:1157594. doi: 10.3389/fpsyt.2023.1157594
25. Philip SR, Fields SA, Van Ryn M, and Phelan SM. Comparisons of explicit weight bias across common clinical specialties of US resident physicians. J Gen Intern Med. (2023) 39:511–8. doi: 10.1007/s11606-023-08433-8
26. Pratt KJ, Palmer E, Cravens JD, Ferriby M, Balk E, and Cai Y. Marriage and family therapy trainees’ Reports of explicit weight bias. J Marital Family Ther. (2016) 42:288–98. doi: 10.1111/jmft.2016.42.issue-2
27. Akoury LM, Schafer KJ, and Warren CS. Fat women’s experiences in therapy: “You can’t see beyond … Unless I share it with you. Women Ther. (2019) 42:93–115. doi: 10.1080/02703149.2018.1524063
28. Harrop EN, Hutcheson R, Harner V, Mensinger JL, and Lindhorst T. You Don’t Look Anorexic”: Atypical anorexia patient experiences of weight stigma in medical care. Body Image. (2023) 46:48–61. doi: 10.1016/j.bodyim.2023.04.008
29. Puhl RM and Brownell KD. Confronting and coping with weight stigma: an investigation of overweight and obese adults. Obes (Silver Spring). (2006) 14:1802–15. doi: 10.1038/oby.2006.208
30. Phelan SM, Bauer KW, Bradley D, Bradley SM, Haller IV, Mundi MS, et al. A model of weight-based stigma in health care and utilization outcomes: Evidence from the learning health systems network. Obes Sci Practice. (2022) 8:139–46. doi: 10.1002/osp4.v8.2
31. Phelan SM, Burgess DJ, Yeazel MW, Hellerstedt WL, Griffin JM, and Ryn M. Impact of weight bias and stigma on quality of care and outcomes for patients with obesity. Obes Rev. (2015) 16:319–26. doi: 10.1111/obr.2015.16.issue-4
32. Arksey H and O’Malley L. Scoping studies: towards a methodological framework. Int J Soc Res Methodology. (2005) 8:19–32. doi: 10.1080/1364557032000119616
33. Raves DM, Brewis A, Trainer S, Han SY, and Wutich A. Bariatric surgery patients’ Perceptions of weight-related stigma in healthcare settings impair post-surgery dietary adherence. Front Psychol. (2016) 7:1497. doi: 10.3389/fpsyg.2016.01497
34. Gilbert K. Atypical Anorexia Nervosa: Examining the Impact of Weight Stigma on Weight Bias Internalization and Eating Disorder Symptoms. United States – Connecticut: University of Hartford (2024). Available at: https://www.proquest.com/pqdtglobal/docview/3014023430/abstract/4DF385D04CC04B5CPQ/1 (Accessed January 7, 2025).
35. Young LM and Powell B. The effects of obesity on the clinical judgments of mental health professionals. J Health Soc Behav. (1985) 26:233–46. doi: 10.2307/2136755
36. Agell G and Rothblum ED. Effects of clients’ obesity and gender on the therapy judgments of psychologists. Prof Psychology: Res Practice. (1991) 22:223–9. doi: 10.1037/0735-7028.22.3.223
37. Davis-Coelho K, Waltz J, and Davis-Coelho B. Awareness and prevention of bias against fat clients in psychotherapy. Prof Psychology: Res Practice. (2000) 31:682–4. doi: 10.1037/0735-7028.31.6.682
38. Hassel TD, Amici CJ, Thurston NS, and Gorsuch RL. Client weight as a barrier to non-biased clinical judgment. J Psychol Christianity. (2001) 20:145–61.
39. Adams LG. Weight bias among counselors-in-training: A qualitative inquiry. United States – Alabama: Auburn University (2008). Available at: https://www.proquest.com/pqdtglobal/docview/304688851/abstract/8AD529F5220F4DC9PQ/1 (Accessed January 7, 2025).
40. Hightower LA. A mixed methods survey of fat bias in marriage and family therapists. United States – Texas: St. Mary’s University (Texas (2014). Available at: https://www.proquest.com/pqdtglobal/docview/1686814966/abstract/CC9BE8CB8F6A46C6PQ/1 (Accessed January 7, 2025).
41. Kasardo AE. Fat bias in the field of psychology: Examining diversity counseling texts and clinical judgment across college counseling centers. United States – Pennsylvania: Indiana University of Pennsylvania (2015). Available at: https://www.proquest.com/pqdtglobal/docview/1678895935/abstract/9FFC70B9F8D745D9PQ/1 (Accessed January 7, 2025).
42. Forristal KM. Fatphobia and Clinical Counseling Decision Making in Counselor Education Students. United States – Ohio: The University of Toledo (2018). Available at: https://www.proquest.com/pqdtglobal/docview/2243061279/abstract/56CB30EC3DFF4498PQ/1 (Accessed January 7, 2025).
43. Veillette LAS, Serrano JM, and Brochu PM. What’s weight got to do with it? Mental health trainees’ Perceptions of a client with anorexia nervosa symptoms. Front Psychol. (2018) 9:2574. doi: 10.3389/fpsyg.2018.02574
44. McAshan M. The Impact of Client Weight and Ethnicity on Counselors’ Evaluation of Eating Disorders Symptoms: A Vignette Study. United States – Texas: Texas Woman’s University (2018). Available at: https://www.proquest.com/pqdtglobal/docview/2120950698/abstract/E4DCF0F9BB74229PQ/1 (Accessed January 7, 2025).
45. Ryland SC. The Effect of Anti-Fat Bias on Therapists’ Perception of Client Motivation, Prognosis, Severity of Mental Illness, and Working Alliance. United States – Pennsylvania: Carlow University (2020). Available at: https://www.proquest.com/docview/2451414011/abstract/5A74E7B525854EA6PQ/1 (Accessed January 7, 2025).
46. Silbiger K. Mental health providers’ perceptions of restrictive eating disorders: Relationship with client body weight. Intl J Eating Disord. (2024) 57:916–23. doi: 10.1002/eat.24154
47. O’Loughlin MK. Therapists’ preferences to provide treatment based on clients’ body size and gender. United States – New York: New York University (1994). Available at: https://www.proquest.com/pqdtglobal/docview/304123573/abstract/EFB3F0FEC2B44679PQ/1 (Accessed January 7, 2025).
48. McCardle M. Weight bias and social work practice: An empirical exploration. United States – New York: City University of New York (2008). Available at: https://www.proquest.com/pqdtglobal/docview/304676171/abstract/2431BD4FBFFE4BBAPQ/1 (Accessed January 7, 2025).
49. Puhl RM, Latner JD, King KM, and Luedicke J. Weight bias among professionals treating eating disorders: Attitudes about treatment and perceived patient outcomes. Intl J Eating Disord. (2014) 47:65–75. doi: 10.1002/eat.22186
50. Puhl RM, Luedicke J, and Grilo CM. Obesity bias in training: attitudes, beliefs, and observations among advanced trainees in professional health disciplines. Obes (Silver Spring). (2014) 22:1008–15. doi: 10.1002/oby.20637
51. Stokes JA. Stigma in Clinical Psychology Trainees: Bias Towards Eating Disorders on the Basis of Weight Variance and the Mediating Influence of Personal Psychological Traits. Illinois, United States: The Chicago School of Professional Psychology (2015). Available at: https://www.proquest.com/pqdtglobal/docview/1559203860/abstract/8ED59758DDB74F11PQ/1 (Accessed January 7, 2025).
52. Soto L, Armendariz-Anguiano AL, Bacardí-Gascón M, and Jiménez Cruz A. Beliefs, attitudes and phobias among Mexican medical and psychology students towards people with obesity. Nutr Hosp. (2014) 30:37–41. doi: 10.3305/nh.2014.30.1.7512
53. Darling R and Atav AS. Attitudes toward obese people: A comparative study of nursing, education, and social work students. J Prof Nurs. (2019) 35:138–46. doi: 10.1016/j.profnurs.2018.07.009
54. Lee SR. Graduate Training in Body Image Complexity: Evolving Competence to Meet Emerging Research. United States – Texas: Texas Woman’s University (2019). Available at: https://www.proquest.com/pqdtglobal/docview/2391990319/abstract/AF64CDA56DD44067PQ/1 (Accessed January 7, 2025).
55. Christensen KN. Factors Related to Weight-Bias among Counselors. United States – North Carolina: The University of North Carolina at Charlotte (2021). Available at: https://www.proquest.com/pqdtglobal/docview/2562239518/abstract/B1AD212A96914F1DPQ/1 (Accessed January 7, 2025).
56. Brochu PM. Testing the effectiveness of a weight bias educational intervention among clinical psychology trainees. J Appl Soc Psychol. (2023) 53:231–41. doi: 10.1111/jasp.12653
57. Franko I. The Correlates of Explicit Weight Bias Among Mental Health Providers in Training. United States – New Jersey: Rutgers The State University of New Jersey, Graduate School of Applied and Professional Psychology (2023). Available at: https://www.proquest.com/docview/2835793739/abstract/3DAD0E0C5C7E4E97PQ/1 (Accessed January 7, 2025).
58. van der Voorn B, Camfferman R, Seidell JC, Puhl RM, and Halberstadt J. Weight-biased attitudes about pediatric patients with obesity in Dutch healthcare professionals from seven different professions. J Child Health Care. (2023) 27:243–52. doi: 10.1177/13674935221133953
59. Sohier L, Ravet MS, Berger-Vergiat A, and Iceta S. Bias related to overweight and obesity among French psychiatrists: Results of a national survey (2024). Available online at: https://www.sciencedirect.com/science/article/pii/S001370062400188X (Accessed January 7, 2025).
60. Aza MN. What’s the skinny on fat women in psychotherapy: mental health clinicians’ countertransference with women of size. Smith College School for Social Work (2009).
61. Hedden LE. Novice Counselors’ Weight and Body Image Beliefs: An Exploratory Q Study. United States – Georgia: University of Georgia (2023). Available at: https://www.proquest.com/pqdtglobal/docview/2917438381/abstract/435568C33E72442CPQ/1 (Accessed January 7, 2025).
62. Chen C and Gonzales L. Understanding weight stigma in eating disorder treatment: Development and initial validation of a treatment-based stigma scale. J Health Psychol. (2022) 27:3028–45. doi: 10.1177/13591053221079177
63. Puhl RM, Lessard LM, Pearl RL, Himmelstein MS, and Foster GD. International comparisons of weight stigma: addressing a void in the field. Int J Obes. (2021) 45:1976–85. doi: 10.1038/s41366-021-00860-z
64. Downes AM. What do fat women want? An exploratory investigation of the influences of psychotherapy on the process by which fat women work toward acceptance of their size and weight. United States – Massachusetts: University of Massachusetts Amherst (2001). Available at: https://www.proquest.com/pqdtglobal/docview/304699803/abstract/B47962898A0B4DCBPQ/1 (Accessed January 7, 2025).
65. Ciepcielinski E. Client perceptions of weight stigma among eating disorder professionals (2016). Available online at: https://hdl.handle.net/20.500.12588/3239 (Accessed January 7, 2025).
66. Abel SA. Let’s talk about your weight”: How fatphobia manifests in therapy (2020). Available online at: http://hdl.handle.net/10315/37782 (Accessed January 7, 2025).
67. Moore M. Exploring Higher Weight Women’s Experiences of Provider Weight Stigma (2022). Available online at: https://scholarworks.uark.edu/etd/4507 (Accessed January 7, 2025).
68. Goehner HJ. Finding Body Appreciation Through the Weight-Neutral Framework. United States – Ohio: Antioch University (2023). Available at: https://www.proquest.com/pqdtglobal/docview/2869208320/abstract/6377EBB75F0A4F4APQ/1 (Accessed January 7, 2025).
69. Sonnenblick RM, Liu J, Riddle DR, Manasse SM, Forman EM, and Juarascio AS. Behavioral weight loss treatment for adults with binge-eating disorder: A qualitative analysis of patients’ perspectives and experiences. Int J Eat Disord. (2024) 57:1854–67. doi: 10.1002/eat.24234
70. Talbert P. An Examination of the Lived Experiences of Those Who Have Received or Attempted to Receive Treatment and/or Recovery from Atypical Anorexia in a Higher Weight Body. United States – California: Alliant International University (2024). Available at: https://www.proquest.com/pqdtglobal/docview/3055877473/abstract/C2A831A4930D4E0DPQ/2 (Accessed January 7, 2025).
71. DeVito NJ and Goldacre B. Catalogue of bias: publication bias. BMJ Evid Based Med. (2019) 24:53–4. doi: 10.1136/bmjebm-2018-111107
72. Gerringer BP. Training Competent Counselors for EveryBODY: The Impact of a Health at Every Size Training on Weight Bias and Its Relationship to Multicultural Competence. United States – North Carolina: The University of North Carolina at Greensboro (2022). Available at: https://www.proquest.com/pqdtglobal/docview/2719399449/abstract/F0C63FC4134343CAPQ/1 (Accessed January 7, 2025).
73. Ali SA. A Qualitative Exploration of Licensed Professional Counselors’ Therapeutic Relationships Working with Clients with Body Image Concerns. United States – Texas: Sam Houston State University (2022). Available at: https://www.proquest.com/docview/2778883706/abstract/FCFDE9F3848E4DA0PQ/1 (Accessed January 7, 2025).
Keywords: weight bias, weight stigma, weight inclusive care, mental health professional, mental health care, cultural competence, mental health equity, scoping review
Citation: Philip SR, Standen EC, Schueler J, Fields SA and Phelan SM (2025) Weight bias in mental health settings: a scoping review. Front. Psychiatry 16:1596625. doi: 10.3389/fpsyt.2025.1596625
Received: 19 March 2025; Accepted: 19 June 2025;
Published: 15 July 2025.
Edited by:
Lily O’Hara, Griffith University, AustraliaReviewed by:
Mussie Msghina, Örebro University, SwedenMohsen Khosravi, Zahedan University of Medical Sciences, Iran
Copyright © 2025 Philip, Standen, Schueler, Fields and Phelan. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Samantha R. Philip, c3JwaGlsaXBAdGFtdS5lZHU=