 Ke Zhao
Ke Zhao Yongxiao Li
Yongxiao Li Penglong Wang2
Penglong Wang2- 1Postgraduate School, University of Harbin Sport, Harbin, China
- 2College of Physical Education, Zhangjiakou University, Zhangjiakou, Hebei, China
- 3The Sports Academy, Jiangsu Ocean University, Lianyungang, Jiangsu, China
Objective: To investigate the effects of different combinations of exercise prescription variables (type, duration, frequency, period, intensity) on inhibitory control in children and adolescents with ADHD, and to provide a basis for the development of exercise prescriptions for intervening inhibitory control in children and adolescents with ADHD.
Methods: Data sources were searched up to February 1, 2025, including Scopus, PubMed, Web of Science, Embase, and Cochrane. The Cochrane Risk of Bias Assessment Tool was utilized for methodological quality assessment. Stata 17.0 software was used for net meta-analysis to compare the interventions with each other, using standardized mean difference (SMD) and 95% CI as the effect indicators. The effect differences between the interventions were compared using standardized mean difference (SMD) and 95% CI as effect indicators, and the effects of exercise prescription variables were ranked using Surface Under the Cumulative Ranking Area (SUCRA).
Results: Twenty papers with 1450 participants aged 7–18 years were finally included. Net Meta-analysis showed that the intervention duration of 70 minutes (SMD=2.15, 95% CI (1.02,3.28)) was significantly better than the control group. The intervention effect was significantly better for 2 times per week (SMD=1.27, 95% CI: (0.65,1.90)) than for the control group, and the intervention effect for at least 20 weeks (SMD=1.37, 95% CI (0.32,2.41)) was significantly better than the intervention effect for 12 weeks. moderate to high intensity (SMD = -0.14, 95% CI (-0.68, -0.40)) was significantly lower than moderate intensity (all P values < 0.05). The ranking of the SUCRA results showed that the intervention effect of Taekwondo (SUCRA=87.1), 70 minutes/repetition (SUCRA=99.0), twice per week (SUCRA=97.8), and continued for at least 20 weeks (SUCRA=92.5) and moderate intervention intensity (SUCRA=98.9) may have the best effect on inhibitory control effects in children and adolescents with ADHD.
Conclusion: This study found that for the improvement of inhibitory control in children and adolescents with ADHD, a moderate-intensity taekwondo exercise intervention model of 70 minutes twice a week for at least 20 weeks can achieve more satisfactory results, which provides a program choice with reference value for relevant clinical intervention practice.
Systematic review registration: https://www.crd.york.ac.uk/PROSPERO/, identifier CRD420251019338.
1 Introduction
Attention deficit hyperactivity disorder (ADHD) is the most common neurodevelopmental disorder among children and adolescents, with a global prevalence of ADHD of approximately 5-7% (1). The core symptoms of ADHD include inattentiveness, hyperactivity, and impulsive behaviors, which have a serious impact on children and adolescents’ academic, social, and family lives (2). One of the major functional deficits in ADHD is inhibitory control deficit, which is manifested by poor impulse control and difficulties in behavioral regulation (3, 4). Although medication is currently the mainstay of treatment for ADHD, drugs may cause side effects such as loss of appetite, insomnia, and anxiety, which has prompted researchers to look for other non-pharmacological interventions to minimize the side effects of drugs (5).
In recent years, physical activity as a non-pharmacological intervention has gradually gained widespread attention from researchers, and relevant studies have shown that physical activity can improve nerve conduction, regulate neurotransmitter levels, and enhance inhibitory control in children and adolescents with ADHD, thereby alleviating the symptoms of ADHD (6, 7). On this basis, exercise can promote the optimization of neural activity patterns by improving brain activity, especially adaptive changes in the prefrontal cortex, which has a significant effect on improving attention, impulse control, and behavioral inhibition in children and adolescents with ADHD (8). Guidelines organized by the Canadian Paediatric Society (CPS) also recommend physical activity as an effective means of ADHD treatment, emphasizing the ability of exercise to improve behavioral performance in children and adolescents with ADHD (9, 10). Hua et al. have proposed in the literature to investigate the effects of different exercise prescription variables on improving inhibitory control in patients with ADHD through a neurobiological mechanism (10). Inhibitory control effects in ADHD patients (11). While exercise prescription guidelines are based on the FITT principle (Frequency, Intensity, Time, Type), each element is interrelated and interacts with each other, and a rational design can significantly enhance the effectiveness of the intervention (12).
Although meta-studies have been conducted to show that exercise interventions have a positive effect on inhibitory control in participants with ADHD (13, 14), as Yang et al. found that cognitive-motor training was the most effective for inhibitory control in their meta-analysis (13), and Zhu et al. mentioned that open-skill activities were the most effective in improving inhibitory control in children with ADHD in their meta-analysis (15). However, systematic comparisons of the effects of factors such as exercise type, intensity, and frequency on intervention effects are still scarce. The advantage of reticulated Meta-analysis is that it can indirectly compare the effects of various interventions by using the effects of multiple interventions as a mediator, which can overcome the limitation that traditional Meta-analysis can only deal with the direct comparison of two interventions even if there is a lack of direct comparative evidence, thus improving the precision of the analysis (4). However, there is currently no review that explores the effect of the FITT variable on the inhibitory control of children with ADHD, therefore, this study aimed to provide recommendations for exercise programs to alleviate inhibitory control in children and adolescents with ADHD by conducting a reticulated Meta-analysis of randomized controlled trials of inhibitory control in children and adolescents with ADHD.
2 Methods
This systematic evaluation was conducted following the requirements of the Priority Reporting Entries for Systematic Reviews and Meta-Analyses: a PRISMA Statement and was registered on the prospective registry platform PROSPERO under the registration number CRD420251019338 (16). Also, and results were reported according to the network meta-analysis extended reporting guidelines (PRISMA-NMA) (17).
2.1 Literature search strategy
Five databases were searched: PubMed, Web of Science, Embase, Scopus, and Cochrane, with the search date ending on February 20, 2025, from the start date of each database. The following combinations of search terms were used: ①exercise, Strength Training, physical exercise, physical activity, sports, fitness, Functional Training, Exercise Therapy; ② ADHD children, ADHD children, elementary school students, adolescents, young adults, school-aged children, school-aged people; ③ executive functioning, working memory, inhibitory control, cognitive flexibility, goal-directed behavior, task switching, short-term memory, retentive retraining, impulse control, response inhibition, interference inhibition, transitive stereotyping, multitasking, RCT, experiment, trial through Boolean logical operators “AND” was used to connect the 3 groups of words, in addition to the inclusion of studies by tracking the literature in published systematic evaluations and meta-analyses to ensure the comprehensiveness of the retrieved literature. Taking Web of Science as an example, the search formula is: TS=(exercise OR “Strength Training” OR “physical exercise” OR “physical activity” OR sports OR fitness OR “Functional Training” OR ‘Exercise Therapy’) AND TS=(“ADHD children” OR ‘primary school students’ OR adolescents OR juvenile OR ‘school children’ OR “school-age population”) AND TS=(“executive functions” OR ‘working memory’ OR ‘inhibitory control’ OR ‘cognitive flexibility’ OR ‘goal - directed behavior’ OR “ task - switching” OR ‘short - term memory’ OR ‘maintenance rehearsal’ OR ‘impulse control’ OR ‘response inhibition’ OR ‘interference inhibition’ OR “ set - shifting” OR ‘multitasking’ OR RCT OR experiment OR trial). Details of the search strategy are given in Table 1.
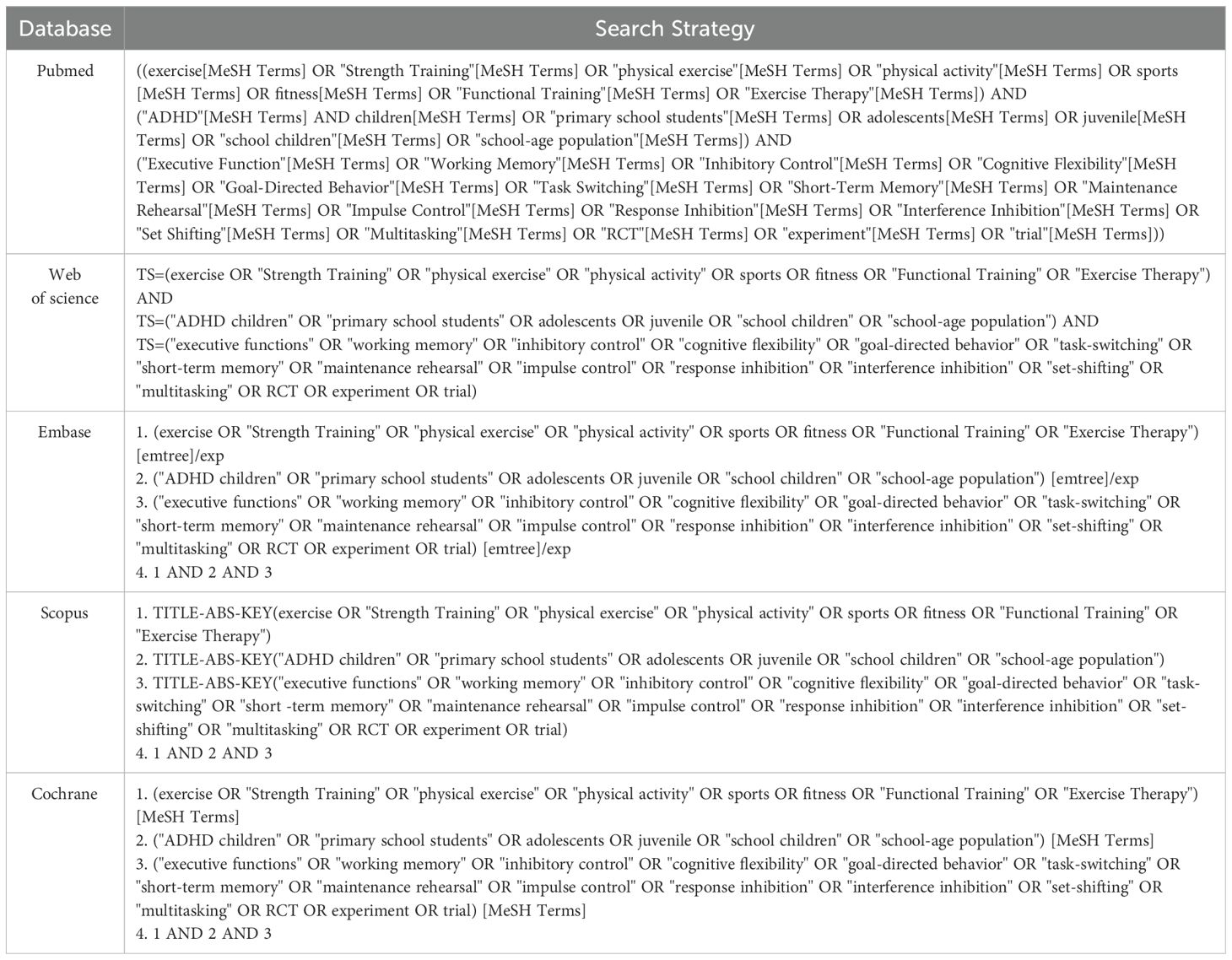
Table 1. Complete search strategy for databases.
2.2 Literature inclusion and exclusion criteria
Inclusion and exclusion criteria for the literature were developed according to the PICOS principle (18). The retrieved literature was de-duplicated by using EndNote 20 software (19). The titles and abstracts of the retrieved literature were initially screened by two independent evaluators using a double-blind approach based on the inclusion and exclusion criteria of the literature. Literature that might meet the inclusion criteria was downloaded in full text and re-screened to finalize the included literature. The inclusion criteria were as follows: (1) Population (Population): the study population was children and adolescents with attention deficit hyperactivity disorder (diagnosed according to the Diagnostic and Statistical Manual of Mental Disorders, fourth and fifth editions) under the age of 18 years. (2) Interventions: studies that included any form of exercise intervention, with no mandatory requirements for type, duration, intensity, and frequency of exercise, but with a minimum of 4 weeks of exercise intervention. (3) Control: The control group was treated in the usual way, including maintaining daily activities, health education, or routine care. (4) Outcomes: inhibitory control. (5) Study design: randomized controlled trial (RCT). Exclusion criteria were as follows: (1) studies focusing only on the physical fitness and motor skills of children and adolescents with ADHD; (2) studies using healthy children and adolescents as comparisons; (3) reviews, abstracts, letters, and commentaries that lacked a clear description of the study design; and (4) articles with incomplete data and where the required data could not be obtained by other means.
2.3 Data extraction
Literature screening and data extraction were done independently by two subject group members who are researchers with evidence-based methodology and have a long history of working with participants with ADHD (20). During the screening or data extraction process, the two researchers extracted independently, and in case of disagreement, they would discuss with the subject group members, negotiate together, and reach a consensus decision. During this process, the main focus was on extracting the following types of key information: the first author of the study, the date of publication of the article, the sample size of the participants, the type of intervention, the duration of the intervention, the frequency of the intervention, the period of the intervention, the intensity of the intervention, as well as the main outcome indicators used to assess the effectiveness of the intervention were entered into an Excel sheet and stored.
2.4 Risk of bias evaluation of included studies
In this study, the risk of bias assessment of all included studies was based on PROSPERO’s registration statement and was independently assessed using the Cochrane Risk of Bias Assessment Tool. The assessment framework covered the following seven aspects, including the validity of the randomization method, the implementation of blinding of trial participants and operators, the blinding status of the outcome assessors, the concealment of the allocation process, the completeness and accuracy of the outcome data, the presence of selective reporting of study results, and other potential bias factors. The quality risk of each study was also categorized into three categories: low risk, high risk, and uncertain risk. If any disagreement on risk of bias arises in the assessment, the assessors will reach a consensus through discussion. If consensus still cannot be reached, the corresponding author will make the final decision based on his/her judgment and taking into account the opinion of the majority of the assessors.
2.5 Statistical methods
This study was analyzed using Statа 17.0 software (21). Since the outcome indicators were continuous values and the evaluation tools and units used for individual studies were different, the standardized mean difference (SMD) was used as the effect size indicator to ensure consistency and comparability of the analyses and to accurately calculate the combined effect size. To further compare the efficacy of different interventions, we used the Surface Under the Cumulative Ranking Area (SUCRA) method to rank the interventions, with values ranging from 0 to 100; the higher the value, the better the efficacy of the effect, which further indicates the relative efficacy of the intervention in improving inhibitory control in participants with ADHD. SUCRA is a statistical method based on reticulated meta-analysis to quantify the relative efficacy of each intervention across all possible interventions. In reticulated meta-analysis, consistency reflects the similarity between the results of direct and indirect comparisons, and higher consistency indicates more reliable reticulated meta-analysis results. The global consistency test for the exercise intervention modality showed better global consistency for the type of exercise (P=0.235). Further consistency tests for closed rings showed that the lower limit of the inconsistency factor contained 0, indicating better consistency of the rings, and thus, the consistency model was used for the analysis. Single exercise time, exercise intervention frequency, exercise intervention period, and exercise intensity did not form a closed loop and therefore did not need to be tested for consistency.
2.6 Evidence certainty assessment
This study utilized the GRADE system assessment tool to evaluate the quality of evidence for all outcome indicators, and the results showed that there were 3 high-level evidence, 11 intermediate-level evidence, 5 low-level evidence, and 1 very low-level evidence (see Table 2). Among the downgrading factors, limitations were the main downgrading factor, 17 were downgraded because of limitations, most of the literature only mentioned randomization without describing the method of generating random numbers, most of the literature did not use blinding and allocation concealment, and only a few of the literature described the method of single-blind or double-blind and allocation concealment. ,
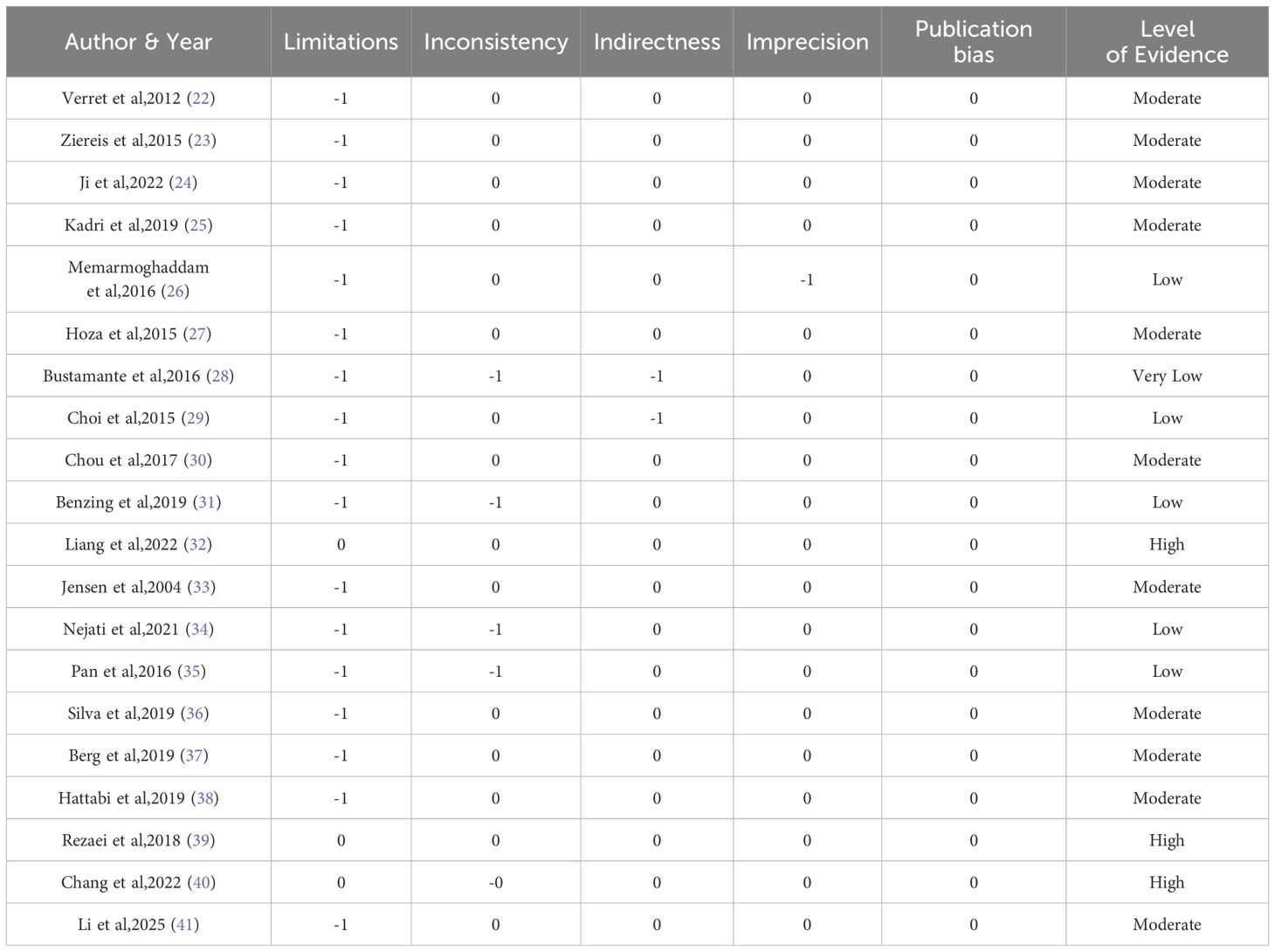
Table 2. Evaluation of the quality of evidence in the included literature.
3 Results
3.1 Results of literature search
A total of 789 documents were retrieved from various databases and other sources, 115 documents were excluded after checking, and the remaining 674 were further screened. Eventually, 20 documents were included, covering a total of 1450 subjects, and the screening process is shown in Figure 1.
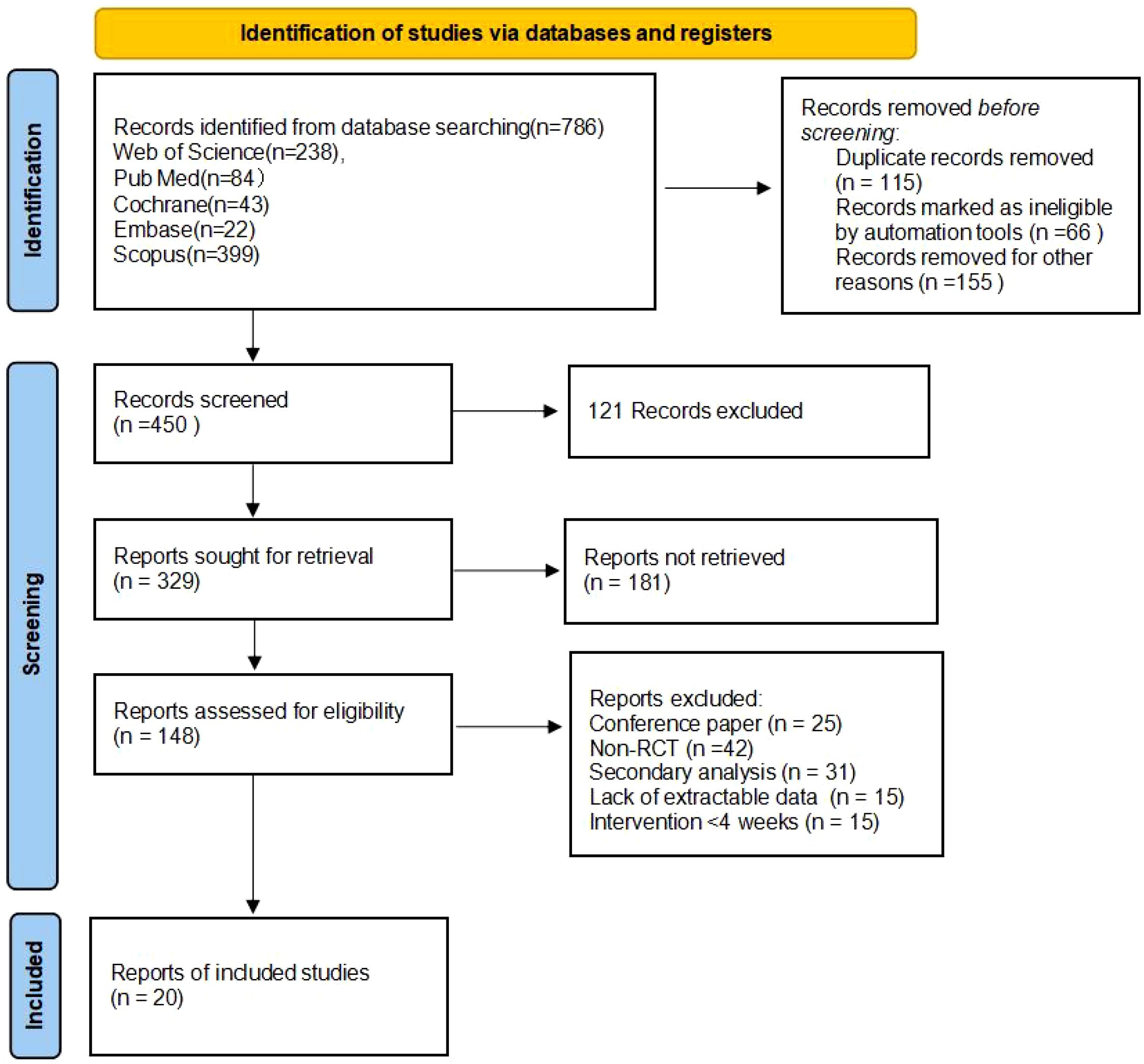
Figure 1. PRISMA flow diagram of the study process.
3.2 Basic characteristics of the included literature
In the 20 included studies, there were 1450 subjects with an age range of 7–18 years old. The main types of exercise interventions in the experimental group included aerobic exercise, sports games, Exergame, bicycle practice, Taekwondo, yoga, combination sports, table tennis, swimming, and qigong. Intervention cycles covered 4–5 weeks, 6 weeks, 8 weeks, 9–10 weeks, 12 weeks, and lasted at least 20 weeks. The frequency of interventions included 1, 2, 3, and 5 sessions. Intervention duration was 10–31 minutes, 40–50 minutes, 60 minutes, 70 bells, and ≥90 minutes. Intervention intensity was moderate intensity; medium to high intensity. Please see Table 3 for detailed basic characteristics of the included literature.
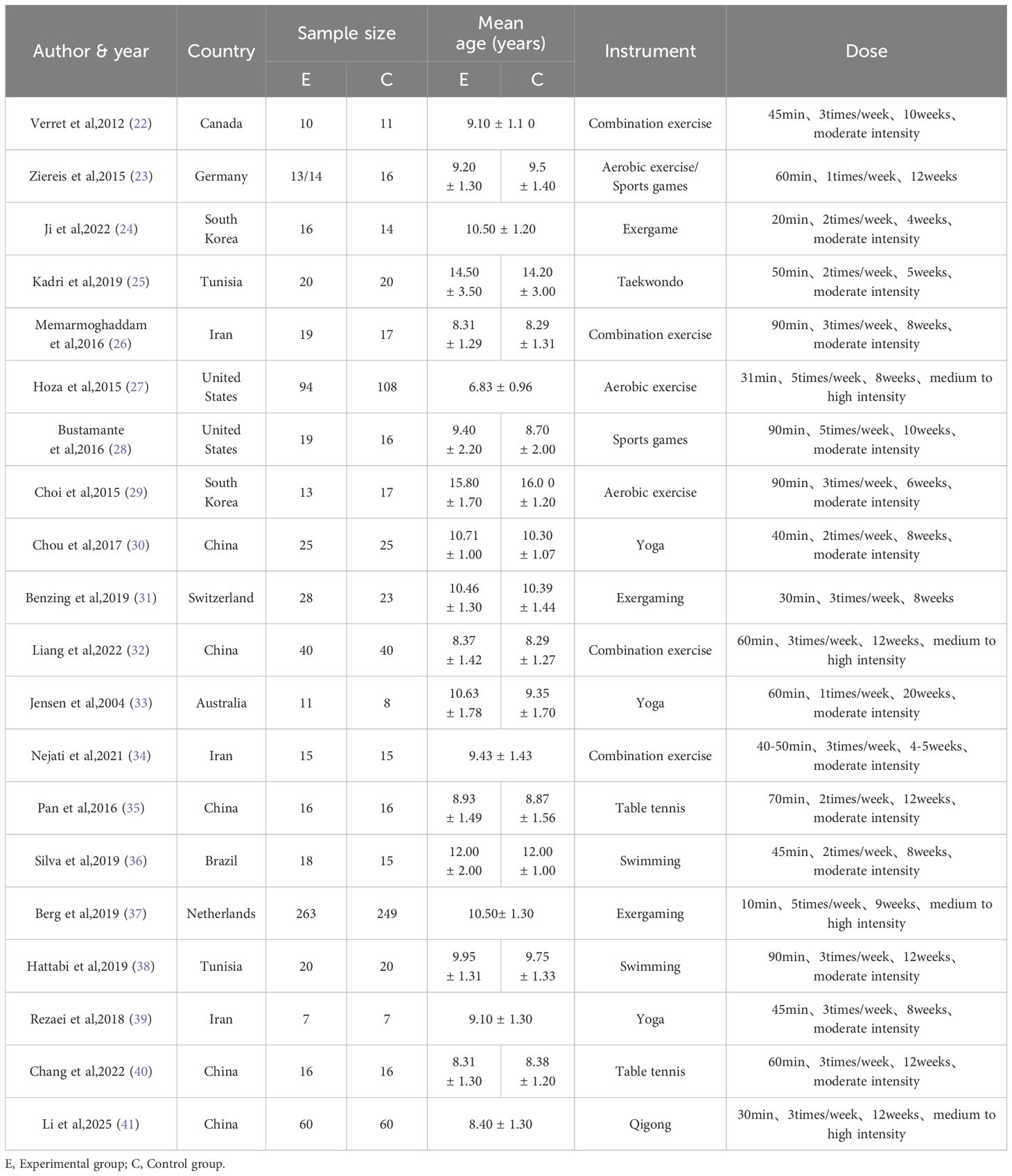
Table 3. Basic characteristics of included studies.
3.3 Evaluation of the quality of the included literature
RevMan 5.4 software and the Cochrane Risk of Bias Assessment Tool were used as criteria for a comprehensive and rigorous assessment of the quality of the literature included in the analysis (42). The results of the Cochrane risk of bias assessment for each study are displayed in Figure 2, while Figure 3 visualizes the overall distribution of risk of bias. Studies were classified as low risk in the selection bias assessment if they were assigned using randomization. In contrast, studies that did not use randomization or did not report the randomization process were labeled as high risk of bias. The results of the risk of bias assessment for each study are detailed in Table 4.
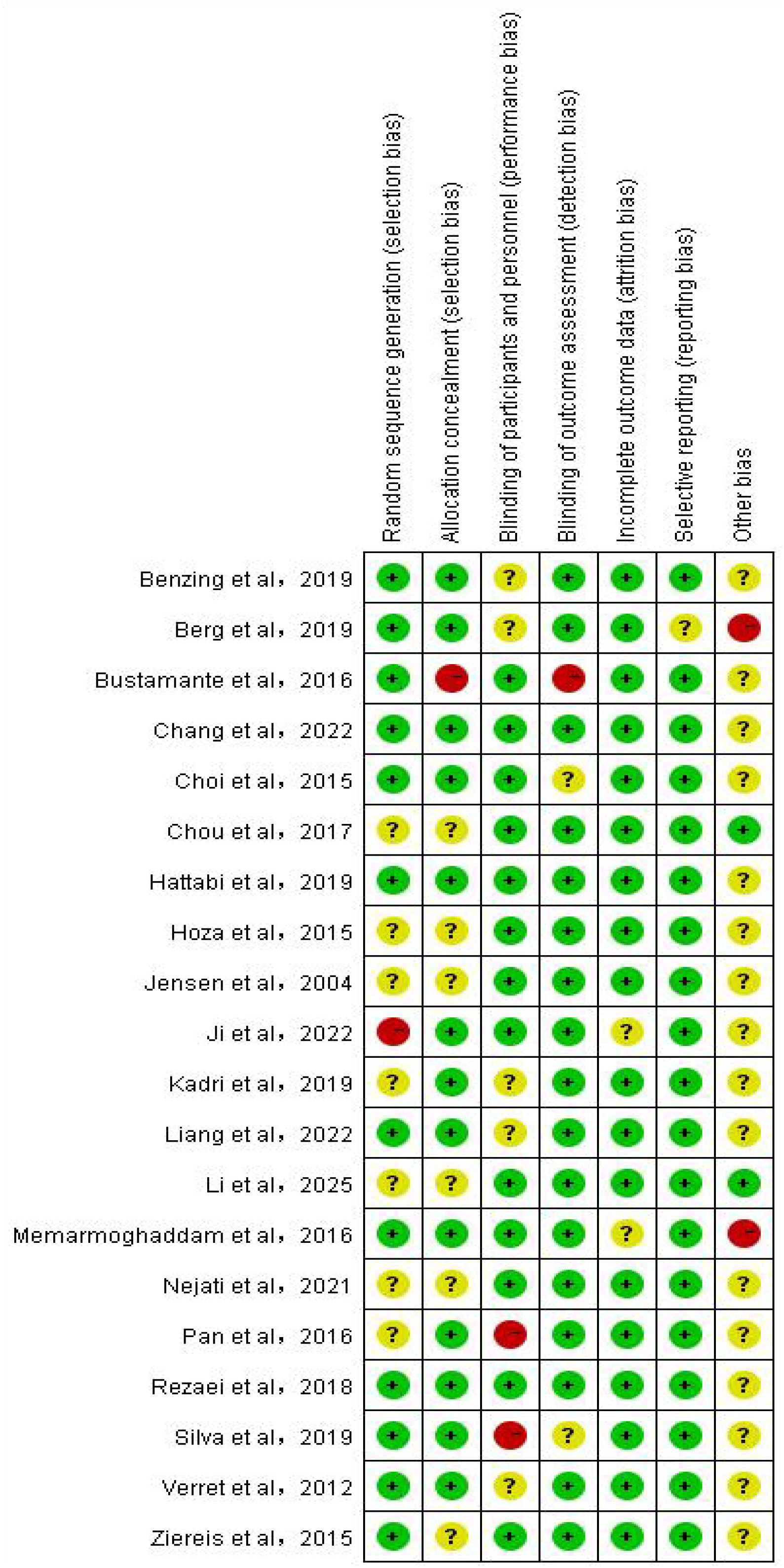
Figure 2. Bias risk diagram for each item.
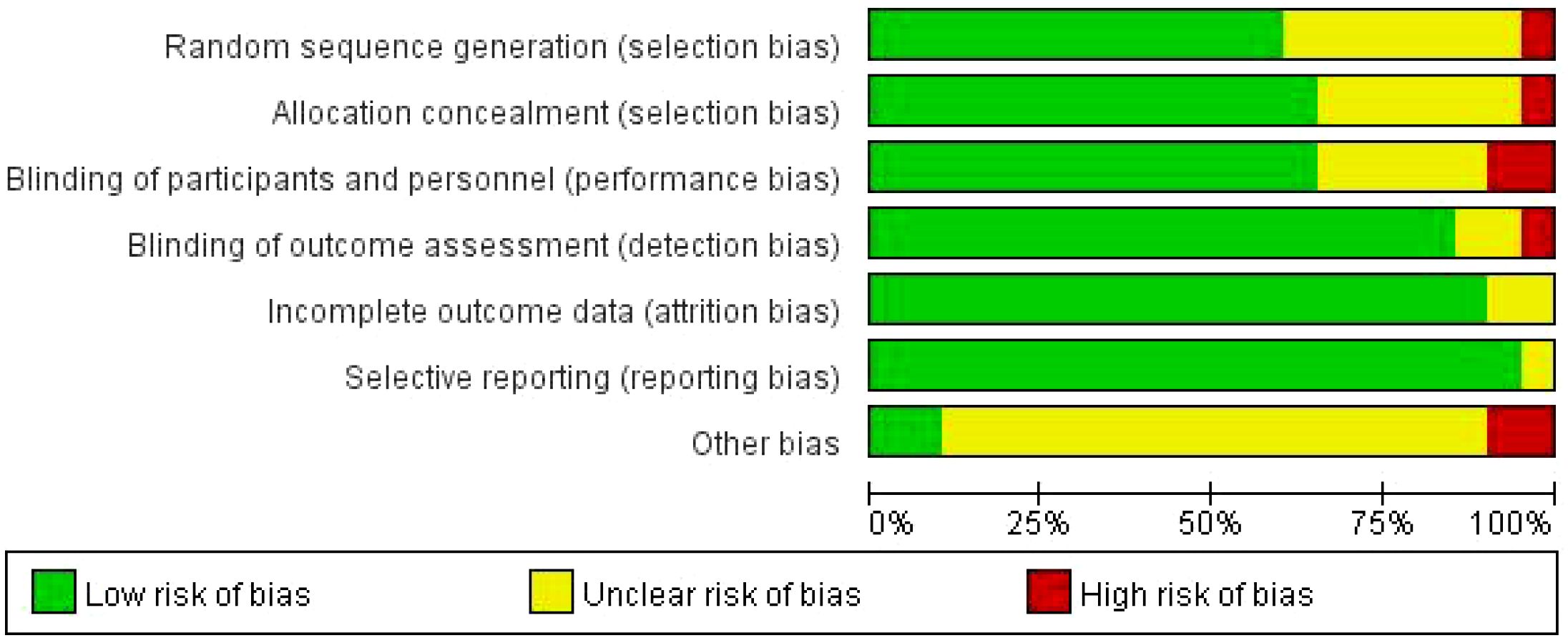
Figure 3. Overall bias risk diagram.
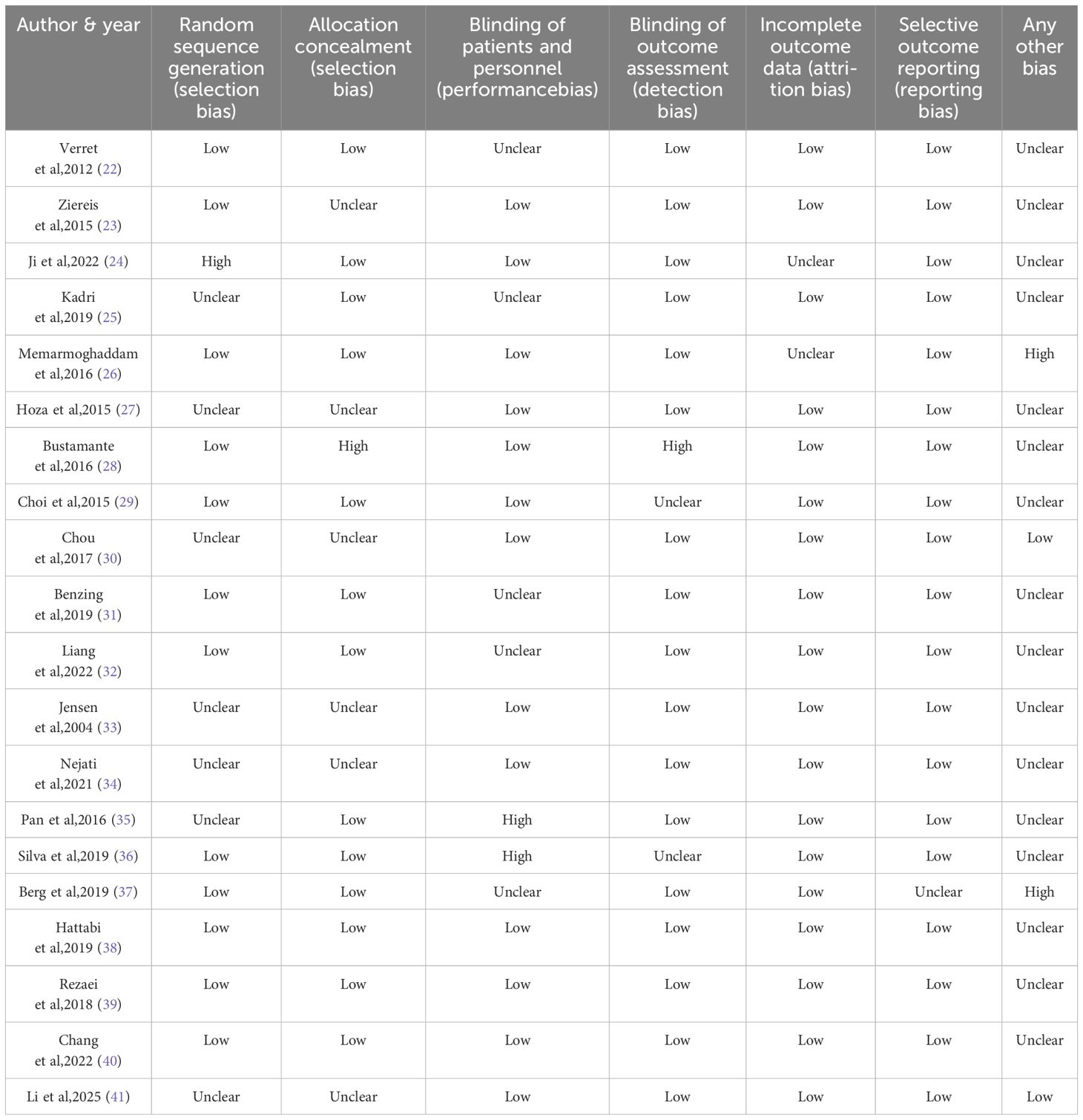
Table 4. Risk of bias assessment (n=20).
3.4 Results of reticulation meta-analysis
3.4.1 Reticulation Meta-analysis
Reticulated Meta-analysis is a method of synthesizing direct and indirect evidence that allows the effects of more than two interventions to be compared simultaneously. In a reticulation graph, each node represents an intervention, the size of the area of the node reflects the sample size, and the thickness of the lines connecting the nodes indicates the number of included studies. See Figure 4 for a specific reticulation evidence map.
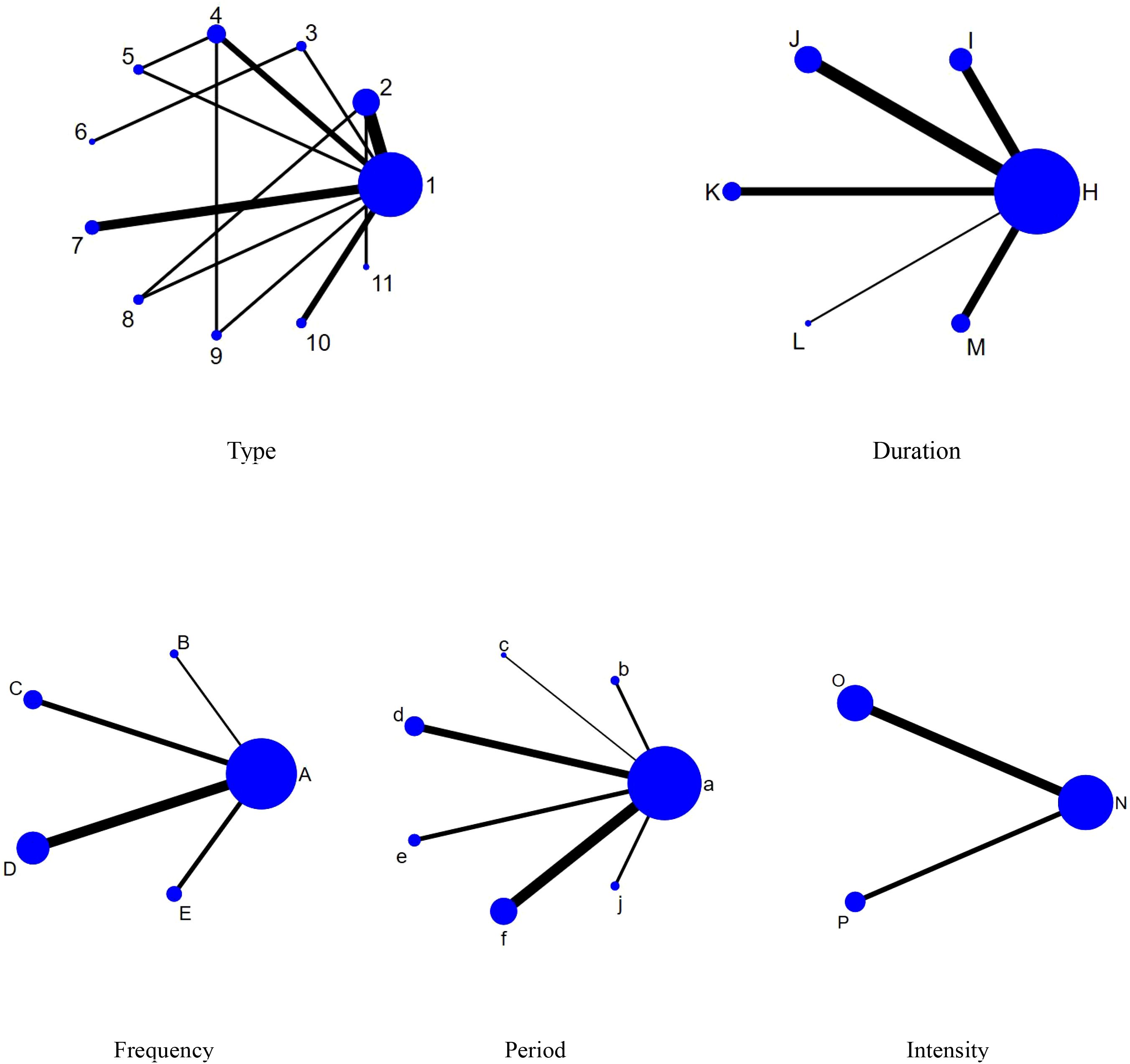
Figure 4. Network evidence diagram. 1,con;2,Aerobic exercise;3,Sports games;4,Exergame;5,Cycling exercise;6,Taekwondo;7,Yoga;8,Combination exercise;9,Table tennis;10,Swimming;11,Qigong; A,con;B,1times;C,2times;D,3times;E,5times;H,con;I,10-31min;J,40-50min;K,60min;L,70min;M,≥90min;a,con;b,4-5weeks;c,6weeks;d,8weeks;e,9-10weeks;f,12weeks;j,≥20weeks;N,con;O,Moderate intensity;P,Medium to high intensity.
3.4.2 Results of two-by-two comparisons between elements of exercise prescription
According to the data in Figure 5, swimming (SMD=1.27, 95% CI: (0.35,2.19)), p<0.05 was significantly better than the control group, while aerobic exercise (SMD=-1.39, 95% CI: (-2.49,-0.29)) was significantly less effective than swimming exercise intervention, and yoga (SMD=1.03, 95% CI: (0.04,2.02)) was significantly better than aerobic exercise intervention. According to the data in Figure 6 the intervention duration of 40–50 minutes (SMD=1.12, 95% CI: (0.69,1.56)) and 70 minutes (SMD=2.15, 95% CI (1.02,3.28)) was significantly better than the control group. Whereas the intervention effect minutes of 40–50 minutes (SMD=0.83, 95% CI: (0.26,1.40)) was significantly better than the intervention effect minutes of 10–31 minutes, the intervention effect minutes of 60 minutes (SMD=-0.87, 95% CI: (-1.53,-0.22)) was significantly lower than the intervention effect minutes of 40–50 minutes, and the intervention effect minutes of 70 minutes (SMD=1.90,95%CI: (0.67,3.13)) intervention effect was significantly better than the 60-minute intervention effect, and the ≥90-minute (SMD=-2.07,95%CI (-3.30,-0.84)) intervention effect was significantly lower than the 70-minute intervention effect and the 60-minute (SMD=-1.05,95%CI (-1.70,-0.40)) intervention Effect. According to the data in Figure 7 the intervention effect of 2 times per week (SMD=1.27, 95% CI: (0.65,1.90)) was significantly better than that of the control group, whereas the intervention effect of 3 times per week (SMD=-1.04, 95% CI (-1.81,-0.26)) was significantly lower than that of 2 times per week, and that of 5 times per week (SMD=-1.13, 95% CI (-2.00, -0.25)) was significantly lower than that of 2 times per week. 2.00, -0.25)) had a significantly lower intervention effect than 3 times. According to the data in Figure 8, the intervention effect of an intervention period of 8 weeks was significantly better than the intervention effect of 6 weeks (SMD=1.71, 95% CI: (0.45,2.98)) and 4–5 weeks (SMD=0.94, 95% CI: (0.43,1.45)), and the intervention effect of 9–10 weeks (SMD=-0.97, 95% CI (-1.77,- 0.18)) was significantly lower than the intervention effect of 8 weeks, and the intervention effect of lasting at least 20 weeks (SMD=1.37, 95% CI(0.32,2.41)) was significantly better than the intervention effect of 12 weeks, as well as the intervention effect of 6 weeks (SMD=2.11, 95% CI(0.67,3.54)) and the intervention effect of 4–5 weeks (SMD=1.33, 95% CI (0.47,2.19)) intervention effects. According to the data in Figure 9, the intervention effect of medium to high intensity was significantly lower than that of medium intensity (SMD=-0.14, 95% CI (-0.68, -0.40)), and there was no significant difference in the other two-by-two comparisons.
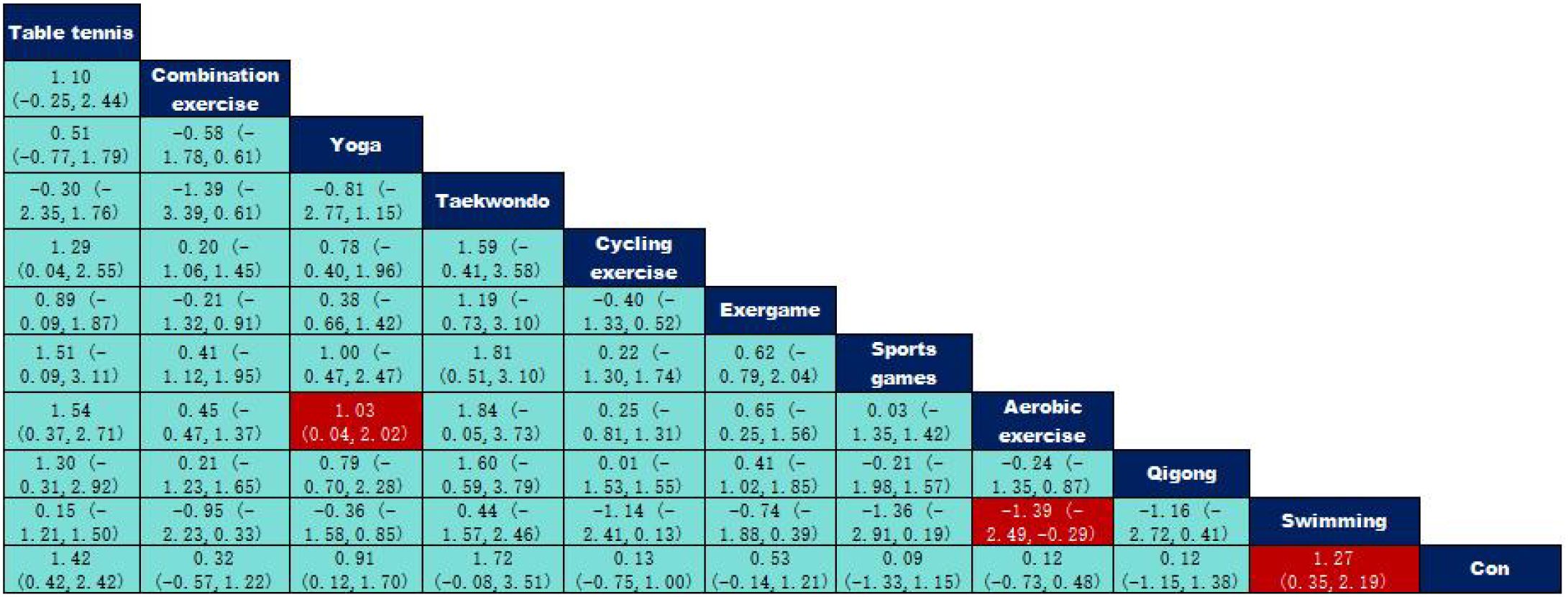
Figure 5. League table of pairwise comparisons of intervention effects among exercise type elements.
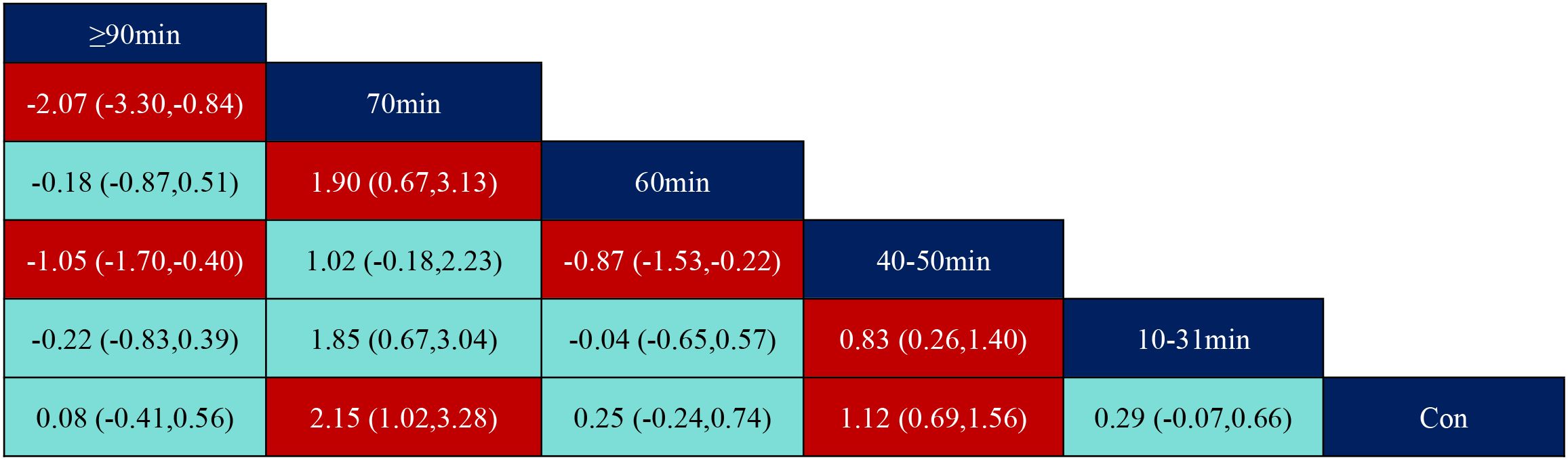
Figure 6. League table of pairwise comparisons of intervention effects among exercise duration elements.
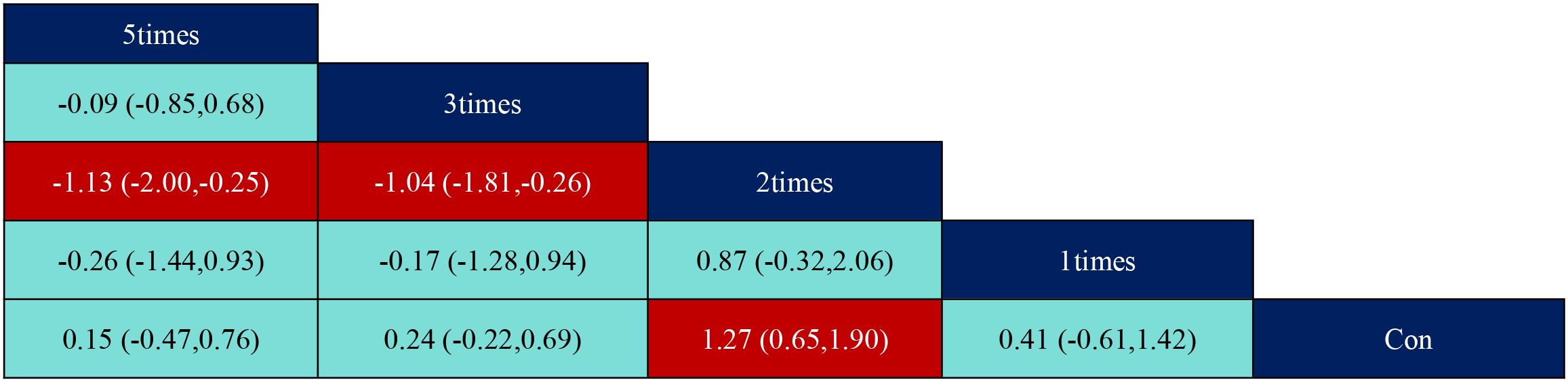
Figure 7. League table of pairwise comparisons of intervention effects among exercise frequency elements.
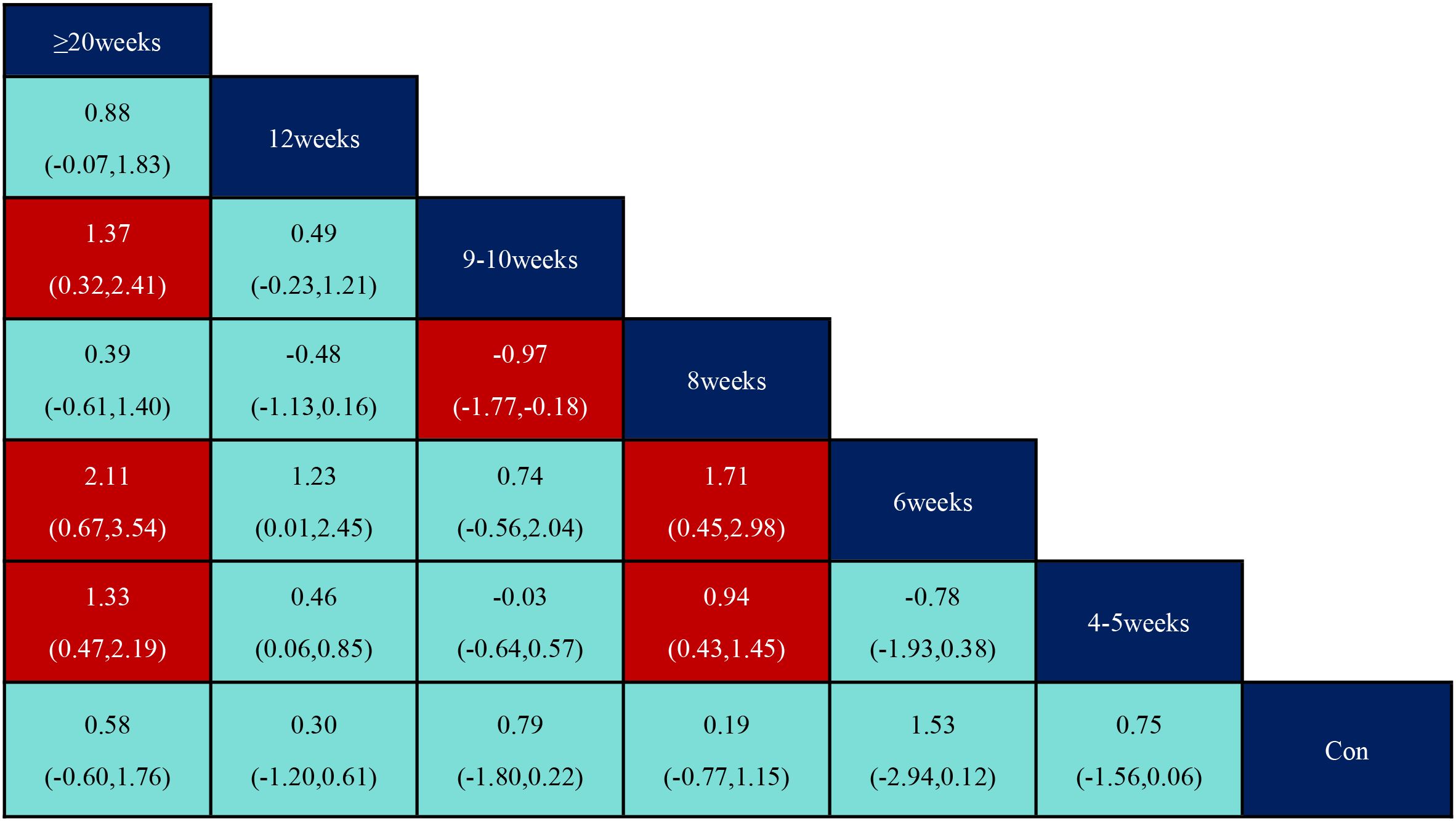
Figure 8. League table of pairwise comparisons of intervention effects among exercise period elements.
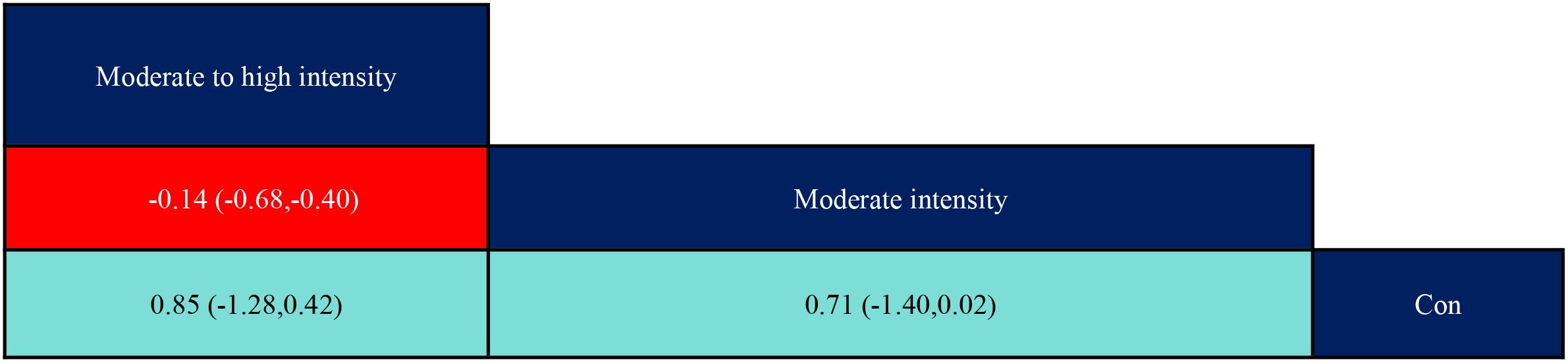
Figure 9. League table of pairwise comparisons of intervention effects among exercise intensity elements. The red numbers are statistically significant.
3.4.3 Probabilistic ranking of optimal interventions for each element of exercise prescription
According to SUCRA from Table 5 and Figure 10, the order of the effects of different types of exercise interventions on the participants with ADHD was: Taekwondo (SUCRA=87.1) > Table tennis (SUCRA=85.2) > Swimming (SUCRA=80.5) > Yoga (SUCRA=69.8) > Exergame (SUCRA=52.1) > Combination exercise (SUCRA=43.6) > Qigong (SUCRA=34.1) > Qigong (SUCRA=34.1) > Qigong (SUCRA=34.1) Swimming (SUCRA=80.5)>Yoga (SUCRA=69.8)>Exergame (SUCRA=52.1)>Combination exercise (SUCRA=43.6)>Qigong (SUCRA=34.1)>Cycling exercise (SUCRA=31.5)>Sports games (SUCRA=23.9). Aerobic exercise (SUCRA=23.8)>Con (SUCRA=18.4).
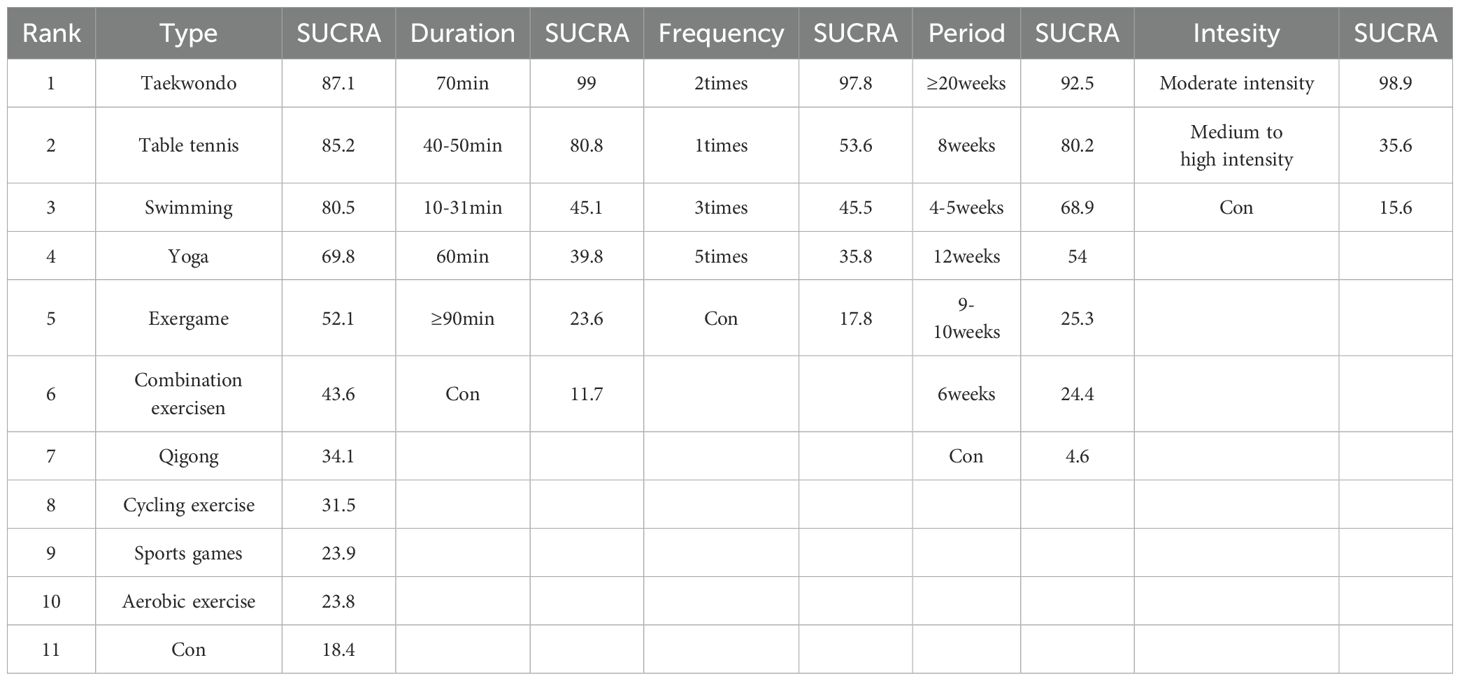
Table 5. SUCRA values for the efficacy of interventions of each element of exercise prescription.
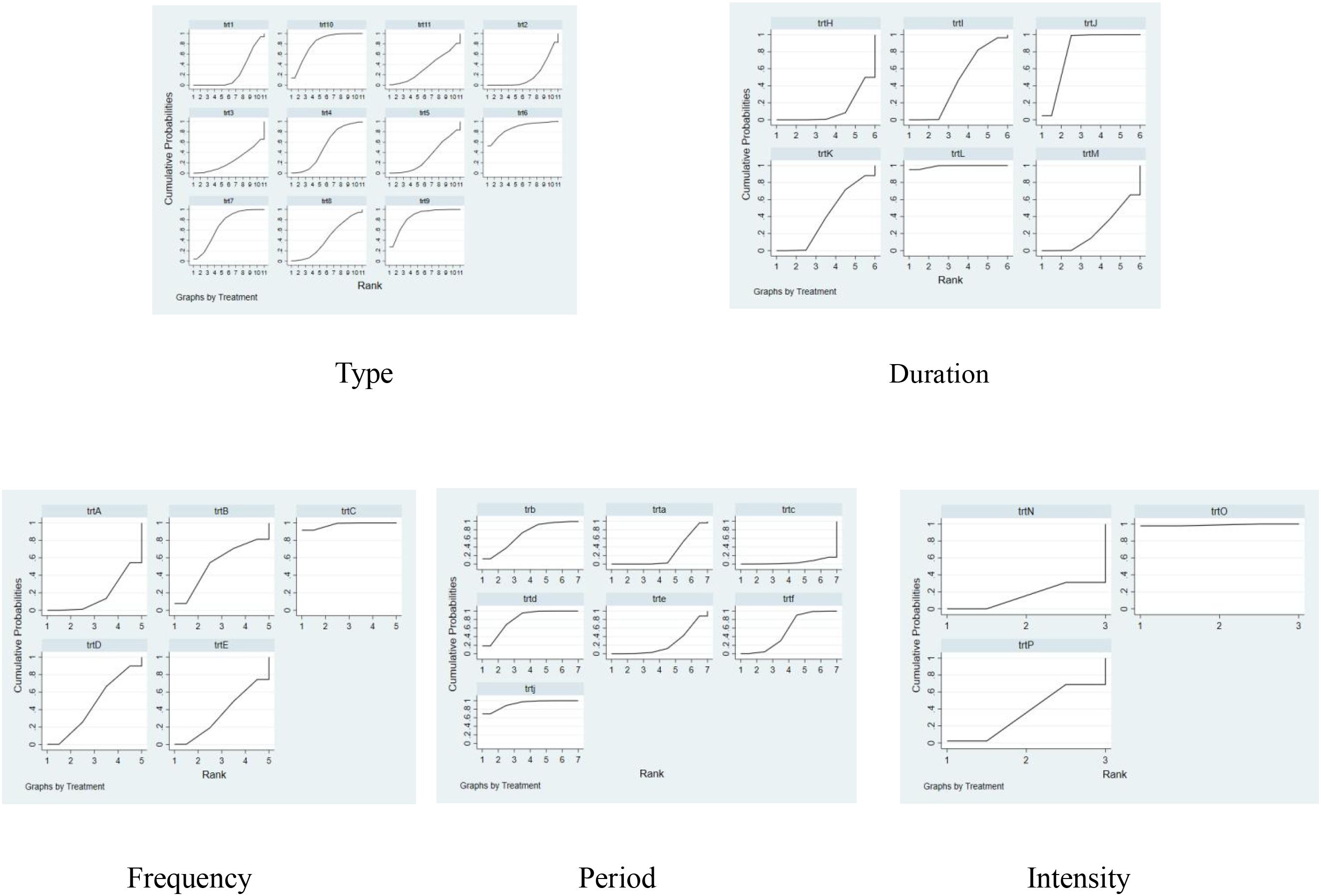
Figure 10. Probability ranking chart of dose-response effects of exercise prescription elements. 1,con;2,Aerobic exercise;3,Sports games;4,Exergame;5,Cycling exercise;6,Taekwondo;7,Yoga;8,Combination exercise;9,Table tennis;10,Swimming;11,Qigong; A,con;B,1times;C,2times;D,3times;E,5times;H,con;I,10-31min;J,40-50min;K,60min;L,70min;M,≥90min;a,con;b,4-5weeks;c,6weeks;d,8weeks;e,9-10weeks;f,12weeks;j,≥20weeks;N,con;O,Moderate intensity;P,Medium to high intensity.
The ranking of the effects of different exercise intervention durations on the intervention effects on participants with ADHD was: 70min (SUCRA=99.0) > 40- 50min (SUCRA=80.8) > 10- 31min (SUCRA=45.1) > 60min (SUCRA=39.8) > ≥90min (SUCRA=23.6) > Con (SUCRA=11.7).
The effects of different exercise intervention frequencies on participants with ADHD were ranked as follows: 2 times (SUCRA=97.8) > 1 time (SUCRA=53.6) > 3 times (SUCRA=45.5) > 5 times (SUCRA=35.8) > Con (SUCRA=17.8).
The rank order of the effect of different exercise intervention cycles on the effect of intervention on participants with ADHD was: ≥ 20 weeks (SUCRA=92.5) > 8 weeks (SUCRA=80.2) > 4–5 weeks (SUCRA=68.9) > 12 weeks (SUCRA=54) > 9–10 weeks (SUCRA=25.3) > 6 weeks (SUCRA=24.4) > Con (SUCRA=4.6).
The ranking of the effects of different exercise intervention intensities on the effects of the intervention on participants with ADHD was Moderate intensity (SUCRA=98.9) > Medium to high intensity (SUCRA=35.6) > Con (SUCRA=15.6).
3.5 Sensitivity analysis
In this study, a sensitivity analysis was conducted to investigate the sources of heterogeneity using the leave-one-out method (43). The results of the analysis showed that the fluctuation range of the combined effect value remained between 0.05 and 0.95 after the removal of any single literature. This indicates that the deletion of each piece of literature has a more limited impact on the overall combined effect value, suggesting that the analytical results of this study have a high degree of stability and reliability. Therefore, it can be confirmed that the conclusions obtained are highly robust.
3.6 Publication bias test
As can be observed from Figure 11, the funnel plot of each indicator is roughly symmetrically distributed, and most of the data points are located in the inner part of the funnel plot, while only a few data points are located in the outer part of the funnel. Overall, the distribution pattern of the funnel plot suggests that there may be a small publication bias in this study. To further verify this, this study assessed publication bias using the Egger test, which showed a p-value of 0.119. This result suggests that no significant publication bias was found (44). However, even though the statistical analysis failed to reveal significant bias, the results of the study need to be interpreted with caution because publication bias may not have been completely ruled out, and other potential factors may still affect the reliability of the results.
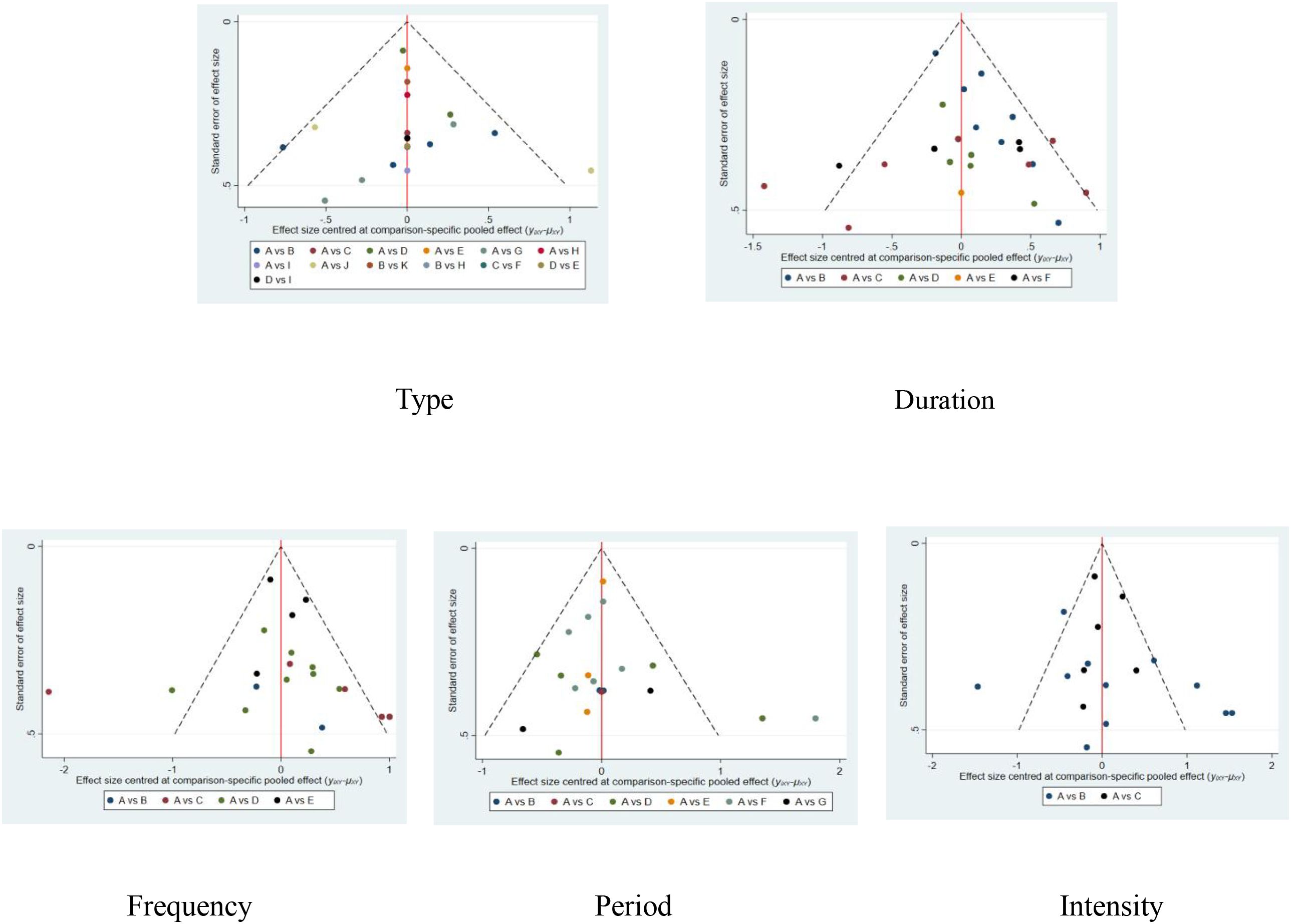
Figure 11. Funnel plot of dose-response effects of exercise prescription elements. 1,con;2,Aerobic exercise;3,Sports games;4,Exergame;5,Cycling exercise;6,Taekwondo;7,Yoga;8,Combination exercise;9,Table tennis;10,Swimming;11,Qigong; A,con;B,1times;C,2times;D,3times;E,5times;H,con;I,10-31min;J,40-50min;K,60min;L,70min;M,≥90min;a,con;b,4-5weeks;c,6weeks;d,8weeks;e,9-10weeks;f,12weeks;j,≥20weeks;N,con;O,Moderate intensity;P,Medium to high intensity.
4 Discussion
Although several systematic reviews and meta-analyses have recently discussed the effects of exercise on interventions for individuals with ADHD (45, 46), our reticulated meta-analysis is the first to discuss the effects of exercise on inhibitory control in individuals with ADHD concerning the components of exercise prescription. In addition, we ranked the magnitude of the effect of different exercise types, exercise frequency, exercise duration, exercise period, and exercise intensity on inhibitory control in children and adolescents with ADHD, which will help to further identify the most effective exercise intervention prescriptions in the population of children and adolescents with ADHD.
The present study found through a net meta-analysis that the best type of exercise to improve inhibitory control in children and adolescents with ADHD may be taekwondo; the best duration of intervention may be 70 min; the best frequency of intervention may be 2 times/week; the best cycle of intervention may be one that lasts for at least 20 weeks; and the best intensity of intervention may be of moderate intensity. The possible reasons for this lie in the theory of brain plasticity, which has been explored by academics in terms of neurophysiological mechanisms (47). This theory suggests that prolonged exercise triggers structural and functional changes in the brain, increasing the capacity of the prefrontal cortex, which in turn affects cognitively active areas of the brain. Notably, inhibitory neurons are heavily distributed in these regions (48). In addition, related studies have also shown that long-term participation in sports has a more significant intervention effect on children and adolescents with ADHD (49).
Taekwondo may be the best type of exercise to improve inhibitory control in youth with ADHD, but given the limited sample size and literature, taekwondo needs to be promoted with caution despite its potential to be the best exercise. This result is somewhat different from the existing Meta-analysis. The results of the established Meta-analysis suggest that ball games may be the type of intervention that has the best impact on youth with ADHD (11). From a neurophysiological perspective, physical activity can directly affect the release of neurotransmitters in the brain, which in turn alters neural circuits (50), especially in populations with ADHD, where brain regions such as the prefrontal cortex and the basal ganglia are often underfunctioning and accompanied by deficiencies of neurotransmitters, such as dopamine and norepinephrine, which are essential for inhibitory control (51), and the effect of different types of exercise on the neurotransmission systems vary (52, 53). Taekwondo, on the other hand, as an offensive and defensive sport, involves body coordination, concentration, and self-control, which not only provides a physical exercise effect, but also an exercise for the brain (54). Taekwondo training requires children and adolescents to be highly concentrated in executing movements, especially when performing precise kicking, fighting, and defending, which requires the participants’ brains to make quick judgments and decisions in a short period of time (55). At this time, increased activity in the prefrontal cortex promotes the release of dopamine and norepinephrine, which in turn improves the brain’s ability to control attention and inhibit impulses (56).
In addition, the present study also explored the effect of intervention duration on inhibitory control in youth with ADHD, and the duration of 70 minutes per intervention may be optimal, a finding that is consistent with the results of an existing meta-analysis, which also pointed out that a prolonged exercise intervention each time had a positive effect on improving inhibitory control in youth with ADHD (57). According to research, interventions of moderate exercise duration can help children and adolescents maintain high levels of attention and help to improve self-control after exercise (58). 70-minute exercise interventions may have the best intervention effect on inhibitory control in youth with ADHD, which may be closely related to the temporal characteristics of neurotransmitter release in the brain (59). Studies have shown that exercise lasts 45 to 60 minutes to significantly increase dopamine and norepinephrine neurotransmitter release (60). And concentrations of these neurotransmitters peak between 15 and 30 minutes after exercise (61). Thus, the 70-minute exercise duration coincides with two critical periods of neurotransmitter release: the first 60 minutes of exercise activate transmitter release, and the next 10 minutes is the period of peak transmitter concentration when training maximizes the effects of inhibitory control (62, 63). In contrast, short durations of 40 to 50 min of exercise, while capable of triggering neurotransmitter release, release relatively small amounts that are insufficient to fully activate relevant receptor pathways in the prefrontal cortex of the brain (64). Although a 60-minute exercise duration can satisfy the demand for neurotransmitter release, the lack of a maintenance phase of peak transmitter concentration can lead to a reduced neuroplasticity effect, while on the other hand, it has been shown that a prolonged 90-minute exercise period may have led to a significant increase in cortisol concentration, a change that inhibits the efficiency of dopamine synthesis through a negative feedback mechanism (65).
Regarding intervention frequency, the present study found that an intervention frequency of 2 times per week was the most effective, which is consistent with the results of existing studies (57, 66, 67). Multiple studies have shown that appropriate intervention frequency is critical for inhibitory control in children with ADHD; in other words, regular exercise twice a week is most effective in improving executive functioning (e.g., intervening to inhibit impulses) in children and adolescents with ADHD (28, 57). Too high a frequency of intervention may lead to overexertion and low energy, whereas too low a frequency may lead to a lag in the effects of the intervention and affect the adaptive response of the nervous system. Another study showed that an intervention frequency of 2 times per week was effective in balancing neurostimulation and the physical load of children and adolescents, ensuring that they did not react negatively to overtraining, and avoiding physical fatigue and psychological overstress (68). At the same time, the frequency of 2 times per week provides sufficient time for children and adolescents with ADHD to recover and consolidate the last training session (69).
The present study found that intervention cycles lasting at least 20 weeks may be the best option for the treatment of attention deficit hyperactivity disorder (ADHD), which is consistent with existing meta-analyses that have found that long-term interventions can help to consolidate the treatment effects and increase the degree of neuroadaptation and behavioral improvement in children (70). Longer interventions provide more opportunities for neuroadaptation, allowing for gradual neurological improvements over a longer period, and the positive effects that long-term exercise interventions can have on children and adolescents with ADHD (71). It has also been shown that exercise interventions lasting more than 6 months can significantly improve attention, impulse control, and task performance in children and adolescents with ADHD (40). Long-term exercise intervention improves the efficiency of signaling in neural circuits, particularly in the prefrontal cortex, a key region of the brain responsible for higher cognitive functions, and its improved functioning significantly enhances self-control and concentration in children and adolescents (7).
The present study found that a moderate-intensity intervention may be most beneficial for improving inhibitory control in children and adolescents with attention deficit hyperactivity disorder (ADHD). This finding differs from a previous meta-analysis, which concluded that high-intensity sports training is more appropriate for improving inhibitory control in children and adolescents with ADHD (72). In contrast, studies have shown that moderate-intensity sport significantly improves core symptoms, including inhibitory control, attentional focus, and executive functioning, in children and adolescents with ADHD (73). Moderate-intensity exercise is typically defined as an activity between light and high intensity, characterized by a significant increase in heart rate and respiratory rate, but not yet at a vigorous level. As defined by the American College of Sports Medicine (ACSM), moderate-intensity exercise typically corresponds to exercise intensities in the range of 40% to 59% of maximal oxygen uptake reserve (VO2R) (74). Although exercise interventions are overall beneficial for children and adolescents with ADHD, too much high-intensity exercise may be counterproductive. Studies have found that improvements in cognitive performance are reduced after vigorous exercise compared to moderate-intensity exercise in children and adolescents with ADHD (73). Another experiment on the effects of acute aerobic exercise at different intensities showed that only after low- and moderate-intensity exercise, the response rate of executive functions (e.g., Flanker inhibition task) was significantly faster in children and adolescents with ADHD than after vigorous exercise (73). In addition, the psychological dimension cannot be ignored. High-intensity training is often taxing and even frustrating for children and adolescents and may lead to decreased self-efficacy, meaning that children feel less confident in their ability to complete the training and control their behavior. Children and adolescents with ADHD are inherently characterized by inattention and poor control, and if the intensity and complexity of exercise exceeds the ability of the child or adolescent, the child is likely to be resistant, which is not conducive to long-term adherence (6). Therefore, moderate-intensity exercise interventions are gaining attention and can be used to help children and adolescents with ADHD improve their symptoms.
5 Limitations
Firstly, the included literature mainly focused on exercise intervention without strict control of daily diet and other activities, and the influence of potential moderating factors (e.g., age, ADHD subtype, medication use, etc.) on the relationship between exercise and inhibitory control was not sufficiently considered; secondly, no distinction was made between genders, and children and adolescents with ADHD of different genders may respond differently to intervention due to the developmental characteristics of puberty; the issue of potential publication bias that would The issue of potential publication bias affecting the credibility of the results was also not explored in depth; finally, the literature search was limited to English, and other languages were not searched, and the inclusion of less literature on qigong, taekwondo, and sports games affected the comprehensiveness of the included literature to a certain extent.
6 Implications for research
This study provides important theoretical support for exercise interventions for children and adolescents with ADHD, revealing the effectiveness of exercise interventions in improving behavioral regulation. The findings suggest that exercise type, duration, frequency, periodization, and intensity have a significant effect on inhibitory control in children and adolescents with ADHD, particularly in terms of the neurophysiological mechanisms at play. This provides an intervention framework for future research.
7 Implications for clinical practice
This study demonstrates the importance of exercise interventions in the treatment of children and adolescents with ADHD, particularly the need to tailor the selection of exercise type and intervention duration to individual patient differences. Based on the results of this study, clinical staff can develop a personalized exercise treatment plan that takes into account the individual characteristics of children and adolescents with ADHD (e.g., age, gender, and interest in exercise). At the same time, studies have shown that exercise is not only physical exercise, but its effect on the neural function of the brain cannot be ignored, which provides a new perspective for the integrated treatment of ADHD in clinical practice. In addition, future clinical studies could combine exercise intervention with medication to improve treatment effects and reduce the risk of drug dependence.
8 Conclusion
This study assessed the impact of different exercise prescriptions on the effectiveness of ADHD interventions by including 20 studies and using network Meta-analysis. The available evidence suggests that specific exercise prescriptions, such as taekwondo intervention, 70 minutes per intervention duration, 2 times per week intervention frequency, intervention cycles longer than 20 weeks, and moderate-intensity exercise, may have the best effect on improving inhibitory control in children and adolescents with ADHD. However, we should also be concerned about individual differences in children’s expression of ADHD symptoms, and each child’s specific symptoms need to be accurately assessed before the intervention is implemented. Meanwhile, due to the relatively limited number of included studies, the generalizability and reliability of these findings still need to be further verified. Nevertheless, this study provides a valuable reference for the clinical development of individualized exercise intervention programs. Future studies should expand the sample size, explore the effects of different exercise prescriptions on different ADHD subtypes, and enhance the evaluation of long-term intervention effects. At the same time, when implementing exercise interventions in the clinic or in the school, it is necessary to pay attention to potential barriers such as resource constraints, adherence challenges, and the need for training in specific sports (e.g., taekwondo), and to address them appropriately to ensure that the interventions are carried out smoothly and achieve good results.
Data availability statement
The original contributions presented in the study are included in the article/supplementary material. Further inquiries can be directed to the corresponding author.
Author contributions
KZ: Writing – original draft, Methodology, Conceptualization, Writing – review & editing. YL: Writing – original draft, Software. PW: Validation, Supervision, Writing – review & editing. PZ: Writing – original draft, Writing – review & editing, Methodology.
Funding
The author(s) declare that no financial support was received for the research and/or publication of this article.
Acknowledgments
The authors would like to express sincere gratitude to those who provided data.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Generative AI statement
The author(s) declare that no Generative AI was used in the creation of this manuscript.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Raman SR, Man KK, Bahmanyar S, Berard A, Bilder S, Boukhris T, et al. Trends in attention-deficit hyperactivity disorder medication use: A retrospective observational study using population-based databases. Lancet Psychiatry. (2018) 5:824–35. doi: 10.1016/S2215-0366(18)30293-1
2. Wilens TE, Biederman J, Faraone SV, Martelon M, Westerberg D, and Spencer TJ. Presenting adhd symptoms, subtypes, and comorbid disorders in clinically referred adults with adhd. J Clin Psychiatry. (2009) 70:15333. doi: 10.4088/JCP.08m04785pur
3. Schachar RJ, Tannock R, and Logan G. Inhibitory control, impulsiveness, and attention deficit hyperactivity disorder. Clin Psychol Rev. (1993) 13:721–39. doi: 10.1016/S0272-7358(05)80003-0
4. Roselló B, Berenguer C, Baixauli I, Mira Á, Martinez-Raga J, and Miranda A. Empirical examination of executive functioning, adhd associated behaviors, and functional impairments in adults with persistent adhd, remittent adhd, and without adhd. BMC Psychiatry. (2020) 20:1–12. doi: 10.1186/s12888-020-02542-y
5. Graham J, Banaschewski T, Buitelaar J, Coghill D, Danckaerts M, Dittmann RW, et al. European guidelines on managing adverse effects of medication for adhd. Eur Child Adolesc Psychiatry. (2011) 20:17–37. doi: 10.1007/s00787-010-0140-6
6. Chan Y-S, Jang J-T, and Ho C-S. Effects of physical exercise on children with attention deficit hyperactivity disorder. Biomed J. (2022) 45:265–70. doi: 10.1016/j.bj.2021.11.011
7. Christiansen L, Beck MM, Bilenberg N, Wienecke J, Astrup A, and Lundbye-Jensen J. Effects of exercise on cognitive performance in children and adolescents with adhd: potential mechanisms and evidence-based recommendations. J Clin Med. (2019) 8:841. doi: 10.3390/jcm8060841
8. Radel R, Brisswalter J, and Perrey S. Saving mental effort to maintain physical effort: A shift of activity within the prefrontal cortex in anticipation of prolonged exercise. Cognitive Affective Behav Neurosci. (2017) 17:305–14. doi: 10.3758/s13415-016-0480-x
9. Subcommittee on Attention-Deficit/Hyperactivity Disorder SCoQI, Management. Adhd: Clinical Practice Guideline for the Diagnosis, Evaluation, and Treatment of Attention-Deficit/Hyperactivity Disorder in Children and Adolescents. IL, USA: American Academy of Pediatrics Elk Grove Village (2011) p. 1007–22.
10. Tremblay MS, Chaput J-P, Adamo KB, Aubert S, Barnes JD, Choquette L, et al. Canadian 24-hour movement guidelines for the early years (0–4 years): an integration of physical activity, sedentary behaviour, and sleep. BMC Public Health. (2017) 17:1–32. doi: 10.1186/s12889-017-4859-6
11. Li H, Zhang P, and Yan B. Does type of exercise matter? Network meta-analysis of the effects of different exercise modalities on inhibitory control in children with attention deficit hyperactivity disorder. Curr Psychol. (2024) 17:1–10. doi: 10.1007/s12144-023-04703-0
12. Billinger SA, Boyne P, Coughenour E, Dunning K, and Mattlage A. Does aerobic exercise and the fitt principle fit into stroke recovery? Curr Neurol Neurosci Rep. (2015) 15:1–8. doi: 10.1007/s11910-014-0519-8
13. Yang Y, Wu C-H, Sun L, Zhang T-R, and Luo J. The impact of physical activity on inhibitory control of adult adhd: A systematic review and meta-analysis. J Global Health. (2025) 15:04025. doi: 10.7189/jogh.15.04025
14. Amatriain-Fernández S, Ezquerro García-Noblejas M, and Budde H. Effects of chronic exercise on the inhibitory control of children and adolescents: A systematic review and meta-analysis. Scandinavian J Med Sci Sports. (2021) 31:1196–208. doi: 10.1111/sms.13934
15. Zhu F, Zhu X, Bi X, Kuang D, Liu B, Zhou J, et al. Comparative effectiveness of various physical exercise interventions on executive functions and related symptoms in children and adolescents with attention deficit hyperactivity disorder: A systematic review and network meta-analysis. Front Public Health. (2023) 11:1133727. doi: 10.3389/fpubh.2023.1133727
16. Gianola S, Castellini G, Andreano A, Corbetta D, Frigerio P, Pecoraro V, et al. Effectiveness of treatments for acute and sub-acute mechanical non-specific low back pain: protocol for a systematic review and network meta-analysis. Systematic Rev. (2019) 8:1–8. doi: 10.1186/s13643-019-1116-3
17. Hutton B, Salanti G, Caldwell DM, Chaimani A, Schmid CH, Cameron C, et al. The prisma extension statement for reporting of systematic reviews incorporating network meta-analyses of health care interventions: checklist and explanations. Ann Internal Med. (2015) 162:777–84. doi: 10.7326/M14-2385
18. Munn Z, Stern C, Aromataris E, Lockwood C, and Jordan Z. What kind of systematic review should I conduct? A proposed typology and guidance for systematic reviewers in the medical and health sciences. BMC Med Res Method. (2018) 18:1–9. doi: 10.1186/s12874-017-0468-4
19. Idris SA, Qureshi AG, Elkhair IS, Idris TA, Adam AM, and Mohammed NK. Usefulness of endnote software for writing scientific manuscripts: A comparative study. Health Res. (2019) 7:6–10. doi: 10.4314/sjms.v4i1.44876
20. Sterne JA, Savović J, Page MJ, Elbers RG, Blencowe NS, Boutron I, et al. Rob 2: A revised tool for assessing risk of bias in randomised trials. bmj. (2019) 28:366. doi: 10.1136/bmj.l4898
21. Shim S, Yoon B-H, Shin I-S, and Bae J-M. Network meta-analysis: application and practice using stata. Epidemiol Health. (2017) 39:e2017047. doi: 10.4178/epih.e2017047
22. Verret C, Guay M-C, Berthiaume C, Gardiner P, and Béliveau L. A physical activity program improves behavior and cognitive functions in children with adhd: an exploratory study. J attention Disord. (2012) 16:71–80. doi: 10.1177/1087054710379735
23. Ziereis S and Jansen P. Effects of physical activity on executive function and motor performance in children with adhd. Res Dev Disabil. (2015) 38:181–91. doi: 10.1016/j.ridd.2014.12.005
24. Ji H, Wu S, Won J, Weng S, Lee S, Seo S, et al. The effects of exergaming on attention in children with attention deficit/hyperactivity disorder: randomized controlled trial. JMIR Serious Games. (2023) 11:e40438. doi: 10.2196/40438
25. Kadri A, Slimani M, Bragazzi NL, Tod D, and Azaiez F. Effect of taekwondo practice on cognitive function in adolescents with attention deficit hyperactivity disorder. Int J Environ Res Public Health. (2019) 16:204. doi: 10.3390/ijerph16020204
26. Memarmoghaddam M, Torbati H, Sohrabi M, Mashhadi A, and Kashi A. Effects of a selected exercise programon executive function of children with attention deficit hyperactivity disorder. J Med Life. (2016) 9:373. doi: 10.17918/00002792
27. Hoza B, Smith AL, Shoulberg EK, Linnea KS, Dorsch TE, Blazo JA, et al. A randomized trial examining the effects of aerobic physical activity on attention-deficit/hyperactivity disorder symptoms in young children. J Abnormal Child Psychol. (2015) 43:655–67. doi: 10.1007/s10802-014-9929-y
28. Bustamante EE, Davis CL, Frazier SL, Rusch D, Fogg LF, Atkins MS, et al. Randomized controlled trial of exercise for adhd and disruptive behavior disorders. Med Sci sports Exercise. (2016) 48:1397. doi: 10.1249/MSS.0000000000000891
29. Choi JW, Han DH, Kang KD, Jung HY, and Renshaw PF. Aerobic exercise and attention deficit hyperactivity disorder: brain research. Med Sci sports Exercise. (2015) 47:33. doi: 10.1249/MSS.0000000000000373
30. Chou C-C and Huang C-J. Effects of an 8-week yoga program on sustained attention and discrimination function in children with attention deficit hyperactivity disorder. PeerJ. (2017) 5:e2883. doi: 10.7717/peerj.2883
31. Benzing V and Schmidt M. The effect of exergaming on executive functions in children with adhd: A randomized clinical trial. Scandinavian J Med Sci sports. (2019) 29:1243–53. doi: 10.1111/sms.13446
32. Liang X, Qiu H, Wang P, and Sit CH. The impacts of a combined exercise on executive function in children with adhd: A randomized controlled trial. Scandinavian J Med Sci sports. (2022) 32:1297–312. doi: 10.1111/sms.14192
33. Jensen PS and Kenny DT. The effects of yoga on the attention and behavior of boys with attention-deficit/hyperactivity disorder (Adhd). J attention Disord. (2004) 7:205–16. doi: 10.1177/108705470400700403
34. Nejati V and Derakhshan Z. The effect of physical activity with and without cognitive demand on the improvement of executive functions and behavioral symptoms in children with adhd. Expert Rev Neurother. (2021) 21:607–14. doi: 10.1080/14737175.2021.1912600
35. Pan C-Y, Chu C-H, Tsai C-L, Lo S-Y, Cheng Y-W, and Liu Y-J. A racket-sport intervention improves behavioral and cognitive performance in children with attention-deficit/hyperactivity disorder. Res Dev Disabil. (2016) 57:1–10. doi: 10.1016/j.ridd.2016.06.009
36. Silva LAD, Doyenart R, Henrique Salvan P, Rodrigues W, Felipe Lopes J, Gomes K, et al. Swimming training improves mental health parameters, cognition and motor coordination in children with attention deficit hyperactivity disorder. Int J Environ Health Res. (2020) 30:584–92. doi: 10.1080/09603123.2019.1612041
37. van den Berg V, Saliasi E, de Groot RH, Chinapaw MJ, and Singh AS. Improving cognitive performance of 9–12 years old children: just dance? A randomized controlled trial. Front Psychol. (2019) 10:174. doi: 10.3389/fpsyg.2019.00174
38. Hattabi S, Bouallegue M, Yahya HB, and Bouden A. Rehabilitation of adhd children by sport intervention: A Tunisian experience réhabilitation des enfants tdah par le sport: une expérience tunisienne. La Tunisie medicale. (2019) 97:874–81. doi: 10.5812/intjssh.118756
39. Rezaei M, Salarpor Kamarzard T, and Najafian Razavi M. The effects of neurofeedback, yoga interventions on memory and cognitive activity in children with attention deficit/hyperactivity disorder: A randomized controlled trial. Ann Appl Sport Sci. (2018) 6:17–27. doi: 10.29252/aassjournal.6.4.17
40. Chang S-H, Shie J-J, and Yu N-Y. Enhancing executive functions and handwriting with a concentrative coordination exercise in children with adhd: A randomized clinical trial. Perceptual Motor Skills. (2022) 129:1014–35. doi: 10.1177/00315125221098324
41. Li Y, He Y-C, Wang Y, He J-W, Li M-Y, Wang W-Q, et al. Effects of qigong vs. Routine physical exercise in school-aged children with attention-deficit hyperactivity disorder: A randomized controlled trial. World J Pediatr. (2025) 10:1–11. doi: 10.1007/s12519-025-00890-x
42. Higgins JPT and Thompson SG. Quantifying heterogeneity in a meta-analysis. Stat Med. (2002) 21:1539–58. doi: 10.1002/sim.1186
43. Balshem H, Helfand M, Schünemann HJ, Oxman AD, Kunz R, Brozek J, et al. Grade guidelines: 3. Rating the quality of evidence. J Clin Epidemiol. (2011) 64:401–6. doi: 10.1016/j.jclinepi.2010.07.015
44. Lin L, Chu H, Murad MH, Hong C, Qu Z, Cole SR, et al. Empirical comparison of publication bias tests in meta-analysis. J Gen Internal Med. (2018) 33:1260–7. doi: 10.1007/s11606-018-4425-7
45. Huang H, Jin Z, He C, Guo S, Zhang Y, and Quan M. Chronic exercise for core symptoms and executive functions in adhd: A meta-analysis. Pediatrics. (2023) 151:e2022057745. doi: 10.1542/peds.2022-057745
46. Vysniauske R, Verburgh L, Oosterlaan J, and Molendijk ML. The effects of physical exercise on functional outcomes in the treatment of adhd: A meta-analysis. J attention Disord. (2020) 24:644–54. doi: 10.1177/1087054715627489
47. Zhang ZY, Shi P, Zhang K, Li CY, and Feng XS. The frontal association area: exercise-induced brain plasticity in children and adolescents and implications for cognitive intervention practice. Front Hum Neurosci. (2024) 18:1418803. doi: 10.3389/fnhum.2024.1418803
48. Chen C and Nakagawa S. Recent advances in the study of the neurobiological mechanisms behind the effects of physical activity on mood, resilience and emotional disorders. Adv Clin Exp Med. (2023) 32:937–42. doi: 10.17219/acem/171565
49. Feng LL, Li BW, Yong SS, and Tian ZJ. Effects of exercise intervention on physical and mental health of children and adolescents with attention-deficit/hyperactivity disorder: A systematic review and meta-analysis based on icf-cy. J Sci Sport Exercise. (2024) 8:1–8. doi: 10.1007/s42978-024-00295-8
50. Di Liegro CM, Schiera G, Proia P, and Di Liegro I. Physical activity and brain health. Genes. (2019) 10:720. doi: 10.3390/genes10090720
51. Shaw P, De Rossi P, Watson B, Wharton A, Greenstein D, Raznahan A, et al. Mapping the development of the basal ganglia in children with attention-deficit/hyperactivity disorder. J Am Acad Child Adolesc Psychiatry. (2014) 53:780–9.e11. doi: 10.1016/j.jaac.2014.05.003
52. Mueller PJ. Exercise training and sympathetic nervous system activity: evidence for physical activity dependent neural plasticity. Clin Exp Pharmacol Physiol. (2007) 34:377–84. doi: 10.1111/j.1440-1681.2007.04590.x
53. Daniela M, Catalina L, Ilie O, Paula M, Daniel-Andrei I, and Ioana B. Effects of exercise training on the autonomic nervous system with a focus on anti-inflammatory and antioxidants effects. Antioxidants. (2022) 11:350. doi: 10.3390/antiox11020350
54. Kim J-S. Effects of Taekwondo Exercise on the Psychological Well-Being of School Children and Young Adults. UNSW Sydney (2001).
55. Adams DB. Brain mechanisms for offense, defense, and submission. Behav Brain Sci. (1979) 2:201–13. doi: 10.1017/S0140525X00061926
56. Berridge CW and Devilbiss DM. Psychostimulants as cognitive enhancers: the prefrontal cortex, catecholamines, and attention-deficit/hyperactivity disorder. Biol Psychiatry. (2011) 69:e101–e11. doi: 10.1016/j.biopsych.2010.06.023
57. Wang M, Yang X, Yu J, Zhu J, Kim H-D, and Cruz A. Effects of physical activity on inhibitory function in children with attention deficit hyperactivity disorder: A systematic review and meta-analysis. Int J Environ Res Public Health. (2023) 20:1032. doi: 10.3390/ijerph20021032
58. Dobbins M, Husson H, DeCorby K, and LaRocca RL. School-based physical activity programs for promoting physical activity and fitness in children and adolescents aged 6 to 18. Cochrane Database systematic Rev. (2013) 2:1–10. doi: 10.1002/14651858.CD007651.pub2
59. Gilbert C. Optimal physical performance in athletes: key roles of dopamine in a specific neurotransmitter/hormonal mechanism. Mech Ageing Dev. (1995) 84:83–102. doi: 10.1016/0047-6374(95)01635-X
60. Kruk J, Kotarska K, and Aboul-Enein BH. Physical exercise and catecholamines response: benefits and health risk: possible mechanisms. Free Radical Res. (2020) 54:105–25. doi: 10.1080/10715762.2020.1726343
61. McMorris T and Hale BJ. Is there an acute exercise-induced physiological/biochemical threshold which triggers increased speed of cognitive functioning? A meta-analytic investigation. J Sport Health Sci. (2015) 4:4–13. doi: 10.1016/j.jshs.2014.08.003
62. Meeusen R, Piacentini MF, and Meirleir KD. Brain microdialysis in exercise research. Sports Med. (2001) 31:965–83. doi: 10.2165/00007256-200131140-00002
63. Lin T-W and Kuo Y-M. Exercise benefits brain function: the monoamine connection. Brain Sci. (2013) 3:39–53. doi: 10.3390/brainsci3010039
64. Breitbach S, Tug S, and Simon P. Circulating cell-free DNA: an up-coming molecular marker in exercise physiology. Sports Med. (2012) 42:565–86. doi: 10.2165/11631380-000000000-00000
65. Tremblay MS, Copeland JL, and Van Helder W. Influence of exercise duration on post-exercise steroid hormone responses in trained males. Eur J Appl Physiol. (2005) 94:505–13. doi: 10.1007/s00421-005-1380-x
66. Qiu C, Zhai Q, and Chen S. Effects of practicing closed-vs. Open-skill exercises on executive functions in individuals with attention deficit hyperactivity disorder (Adhd)—a meta-analysis and systematic review. Behav Sci. (2024) 14:499. doi: 10.3390/bs14060499
67. Ye Y, Ning K, Wan B, and Shangguan C. The effects of the exercise intervention on fundamental movement skills in children with attention deficit hyperactivity disorder and/or autism spectrum disorder: A meta-analysis. Sustainability. (2023) 15:5206. doi: 10.3390/su15065206
68. Liang X, Li R, Wong SH, Sum RK, and Sit CH. The impact of exercise interventions concerning executive functions of children and adolescents with attention-deficit/hyperactive disorder: A systematic review and meta-analysis. Int J Behav Nutr Phys Activity. (2021) 18:68. doi: 10.1186/s12966-021-01135-6
69. Jiang K, Xu Y, Li Y, Li L, Yang M, and Xue P. How aerobic exercise improves executive function in adhd children: A resting-state fmri study. Int J Dev Neurosci. (2022) 82:295–302. doi: 10.1002/jdn.10177
70. Cerrillo-Urbina AJ, García-Hermoso A, Sánchez-López M, Pardo-Guijarro MJ, Santos Gómez J, and Martínez-Vizcaíno V. The effects of physical exercise in children with attention deficit hyperactivity disorder: A systematic review and meta-analysis of randomized control trials. Child: care Health Dev. (2015) 41:779–88. doi: 10.1111/cch.12255
71. Berwid OG and Halperin JM. Emerging support for a role of exercise in attention-deficit/hyperactivity disorder intervention planning. Curr Psychiatry Rep. (2012) 14:543–51. doi: 10.1007/s11920-012-0297-4
72. Chen J-W, Du W-Q, and Zhu K. Optimal exercise intensity for improving executive function in patients with attention deficit hyperactivity disorder: systematic review and network meta-analysis. Eur Child Adolesc Psychiatry. (2024) 26:1–22. doi: 10.1007/s00787-024-02507-6
73. Tsai Y-J, Hsieh S-S, Huang C-J, and Hung T-M. Dose-response effects of acute aerobic exercise intensity on inhibitory control in children with attention deficit/hyperactivity disorder. Front Hum Neurosci. (2021) 15:617596. doi: 10.3389/fnhum.2021.617596
Keywords: exercise prescription, inhibitory control, ADHD, children and adolescents, meta-analysis
Citation: Zhao K, Li Y, Wang P and Zhang P (2025) Exercise prescription to improve inhibitory control in children and adolescents with ADHD: a network meta-analysis. Front. Psychiatry 16:1601765. doi: 10.3389/fpsyt.2025.1601765
Received: 03 April 2025; Accepted: 10 June 2025;
Published: 30 June 2025.
Edited by:
Miguel Jacinto, Polytechnic Institute of Leiria, PortugalReviewed by:
Marcos Bella-Fernández, UNIE Universidad, SpainHakan Öğütlü, Cognitive Behavioral Psychotherapies Association, Türkiye
Soukaina Hattabi, University of Jendouba, Tunisia
Maria Theodoratou, Neapolis University, Cyprus
Copyright © 2025 Zhao, Li, Wang and Zhang. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Ping Zhang, emhhbmdwaW5nQGhyYmlwZS5lZHUuY24=