 Joanna Mourad1,2,3,4*
Joanna Mourad1,2,3,4* Bernadette Grosjean5Nader Perroud6Katleen Bogaerts1,7
Bernadette Grosjean5Nader Perroud6Katleen Bogaerts1,7 Martin Desseilles3,4
Martin Desseilles3,4 Bruno Bonnechère1,2,8
Bruno Bonnechère1,2,8- 1REVAL Rehabilitation Research Center, Faculty of Rehabilitation Sciences, Hasselt University, Diepenbeek, Belgium
- 2Technology-Supported and Data-Driven Rehabilitation, Data Sciences Institute, Hasselt University, Diepenbeek, Belgium
- 3Department of Psychology, University of Namur, Namur, Belgium
- 4Transition Institute, University of Namur, Namur, Belgium
- 5Retired, Los Angeles, CA, United States
- 6Department of Psychiatric Specialties, Department of Psychiatry, Geneva University Hospitals, Geneva, Switzerland
- 7Health Psychology, Faculty of Psychology and Educational Sciences, University of Leuven, Leuven, Belgium
- 8Department of PXL – Healthcare, PXL University of Applied Sciences and Arts, Hasselt, Belgium
1 Body representations
Body representations (BR) refer to dynamic neural multi-layered models that integrate sensory, motor, and cognitive processes, allowing individuals to perceive and interact with their bodies (1). Traditionally, BR have been divided into two primary components: body schema, which involves unconscious, action-based representations of the body, and body image, which pertains to conscious, perception-based understandings of the body (2). More recent frameworks extend this dichotomy proposing that BR are formed by a combination of real-time multisensory inputs and an internal “offline body model” that guides actions (3). Furthermore, the role of body memory includes unique representations of the body that develop during distinct developmental periods enabling to add a temporal depth to this system (4). In essence, BR are adaptable frameworks that are continuously updated through interactions with both the environment and culture, influencing how individuals perceive and navigate the world (5). These representations play a crucial role in sensory processing, self-awareness, motor coordination, and social interactions (6, 7).
In autism, BR manifest atypically, often contributing to sensory sensitivities, altered proprioception, and difficulties with motor skills (8, 9), impacting daily tasks like personal hygiene and meal preparation. Understanding these atypicalities requires tailored assessments. However, existing questionnaires and evaluations have primarily been developed in a limited set of developed nations, including France (10, 11), Saudi Arabia (12), Japan (13), the USA (14), the UK (15), Sweden (16) and Austria (17). This concentration in developed countries restricts the applicability of these tools. Despite cultural commonalities, biased assessments overlook global BR diversity, neglecting many cultures and hindering autism diagnosis and support worldwide. Consequently, future research must prioritize developing universally adaptable assessments that accommodate cultural and linguistic diversity, enhancing both accuracy and accessibility. Because cultural norms significantly shape how BR manifest and how autism is perceived, e.g., varying norms around eye contact and social engagement (18–20), it is essential to assess BR within these contexts. This necessity extends well beyond autism, as cultural beliefs and practices shape health-seeking behaviors and the interpretation of symptoms across different populations. Culturally grounded adaptations in autism interventions improve effectiveness, as emphasized by Keehn (21), and cultural beliefs influence care practices and treatment outcomes (21, 22). A one-size-fits-all approach to autism assessment may therefore overlook critical cultural nuances, potentially leading to misdiagnosis or ineffective interventions.
Therefore, this opinion highlights the importance of integrating cultural factors in the assessment of BRs in autism.
2 Defining the landscape of BRs research in ASD
Currently, the vast majority of the studies are being conducted in high-income countries (HIC), which leads to biased understandings of autism (23), limiting the generalizability of findings to non-Western populations. While 80% of the population lives in LMICs (23), research on autism in low- and middle income countries (LMICs) is still very limited, and many individuals remain undiagnosed due to the lack of culturally appropriate diagnostic tools (24–27). For example in China, diagnostic services are still developing, resulting in lower prevalence rates 39.23 per 10,000 compared to higher-income countries like the USA and Northern Europe (1% to 2.21%); this gap can be attributed to diagnostic tools that overlook cultural differences, language barriers, and varying levels of autism awareness (23–29). This disparity is evident in epidemiological studies, where 26 of 37 surveys were from high-income countries and only 11 from middle-income countries (average prevalence 0.47%), with no studies from low-income countries (18). In Nigeria and South Africa, researchers highlight persistent barriers such as low diagnostic awareness, cultural stigma, and a lack of regionally adapted screening tools (24, 25). Similarly, in India, Dey et al. conducted an online survey followed by an in-depth conversation with parents of autistic children and autistic adults emphasizing the need for culturally grounded autism priorities and tools (26). These studies demonstrate that underdiagnosis in LMICs is not solely due to economic constraints, but also to fundamental mismatches between Western-based diagnostic models and local sociocultural frameworks.
To better evaluate the research specifically performed around BR in ASD we performed a bibliometric analysis. Bibliometric analysis is a quantitative method for mapping scientific literature, allowing researchers to identify trends, collaboration networks, knowledge gaps and potential future research direction by analyzing publication metadata (30). Data for the present study was obtained from the WoS (accessed on 15 April 2025), using MeSH and title/abstract keywords related to autism spectrum disorder (e.g., “ASD,” “autism,” “Asperger’s syndrome”) and body representations (e.g., “body awareness,” “interoception,” “body schema,” “proprioception,” “sensorimotor integration,” “embodiment,” “motor imagery”). A total of 4,024 documents including research articles, review articles and book chapters formed the final dataset, with data processed using VOSviewer to visualize and map collaboration networks (31).
Before 2000 we observed that this concept was scarcely studied, but it has since experienced exponential growth. (Figure 1B). As for studies about the prevalence of ASD we observed that most, if not all the studies, are being performed in HIC (the 20 most significant contributor are presented in Figure 1C). Another important finding, potentially limiting the external validity of these studies, from a cultural point of view, is that most of the studies are being performed in one single country and that, as depicted in Figure 1A, there are almost no collaborations with LMICs.
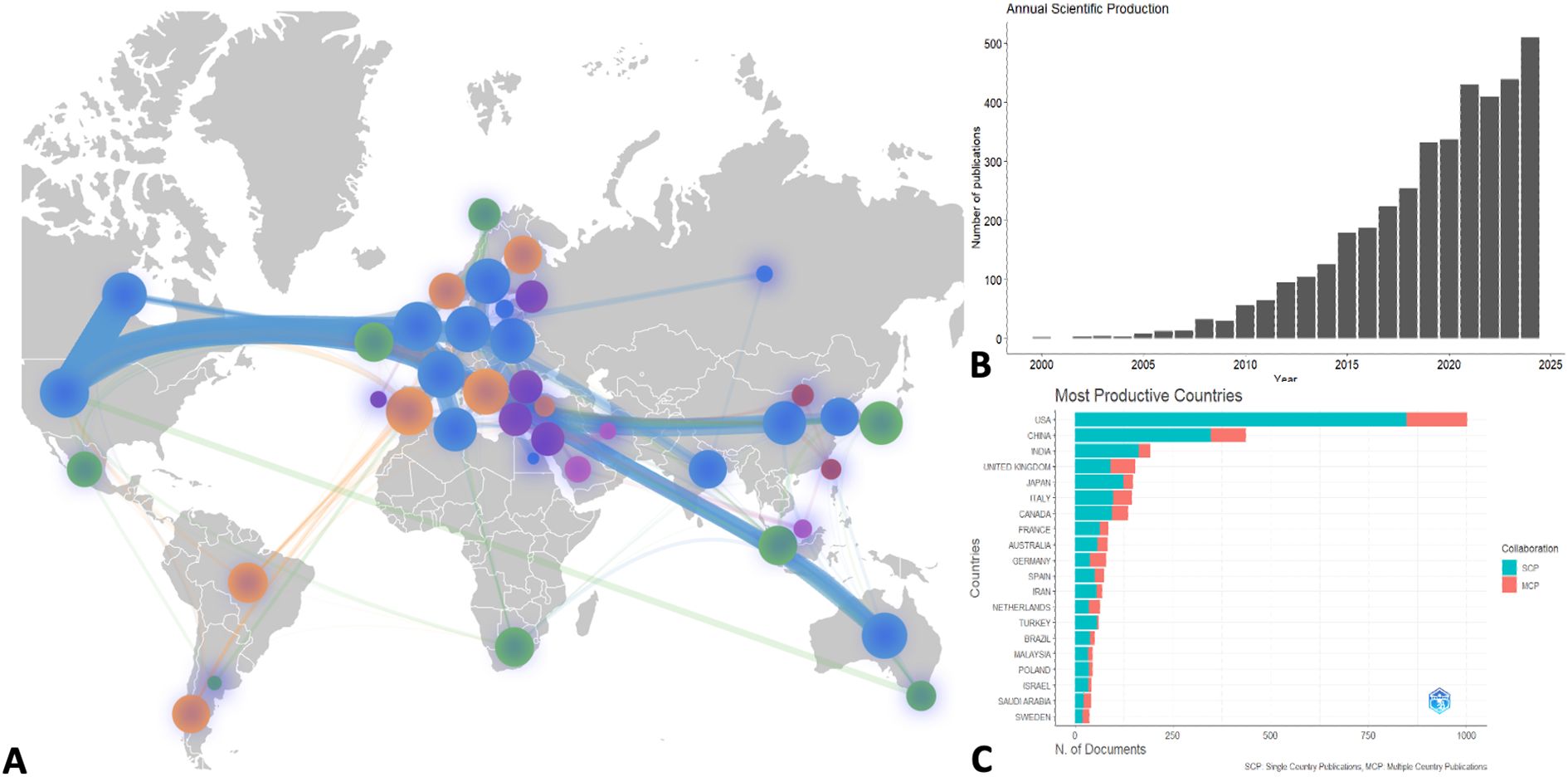
Figure 1. Bibliometric Analysis of studies on BRs in ASD. (A) Country collaboration map, the size of the bubble are proportional to the number of studies, the width of the connection is proportional to the number of collaborations, the color represents the different clusters with the most collaborations. (B) Annual scientific production; (C) Most productive countries, including single (green) and multiple country collaborations (red).
3 The main challenges in assessing BRs in various cultures
3.1 Cultural background: between similarities and differences in regional patterns
One crucial aspect to consider is that cultural similarities across certain regions or countries can result in similar patterns in the manifestation of BR and other autism-related characteristics. Countries with shared cultural, historical, or linguistic backgrounds are more likely to exhibit comparable societal norms and attitudes towards body perception. This common cultural foundation can lead to similarities in research outcomes within these regions. For example, studies conducted in countries which share cultural and linguistic resemblances, often show analogous results in terms of BRs assessments and autism prevalence (23). Countries in the Middle East, like Saudi Arabia and Egypt, may exhibit parallel outcomes due to shared cultural and religious norms (32–36). Similarly, countries influenced by Latin European and Western biomedical traditions share cultural and scientific framework, public health and educational systems, ultimately leading to alike societal attitudes toward body perceptions. In Westernized cultures, particularly among women, dissatisfaction with body weight and appearance is common and has been linked to eating disorders, depression, and anxiety (19, 37). In contrast, other cultures may emphasize different physical ideals or interpret bodily differences, for instance overweight can be associated with the norm of beauty or even considered as healthy and wealth (18, 19, 38). Western diagnostic tools, such as those based on body image dissatisfaction, may not be applicable or relevant in non-Western contexts. Moreover, behaviors seen as socially deviant in one culture may be normalized or even valued in another.
While cultural norms are acknowledged to shape body representation (BR) (19, 39) the mechanisms by which these influences operate, particularly in autism, deserve a deeper exploration. Cultural environments structure early sensorimotor experiences (40, 41), including norms around physical touch, posture, bodily autonomy, and social body use. In autistic individuals, who often show atypical sensory processing, including altered proprioception, interoception, and tactile perception (42–44), culturally mediated sensory input may exert amplified or divergent developmental effects. For example, studies have shown that self-representation and multisensory integration are modulated by cultural experiences through plasticity in regions such as the insula and temporoparietal junction (45, 46), areas that are also implicated in BR and are known to function atypically in autistic individuals (47). Taken together, these findings suggest that culturally specific experiences dynamically shape BR neurodevelopment by influencing multisensory integration and bodily self-awareness, particularly in neurodivergent populations. Therefore, a culturally sensitive approach is critical for accurate assessment in autistic individuals. It is also important to consider the nature-nurture balance in developmental disorders. This distinction underscores the need to tailor assessment tools not only to regional cultural contexts but also to the underlying nature vs nurture profile of the condition being evaluated. Acknowledging cultural similarities and differences can thus facilitate the development of more accurate and universally adaptable diagnostic tools (35, 48, 49).
3.2 Language and communication
Language and communication barriers can also play a significant role in assessing BR, especially in multilingual and culturally diverse contexts (50). Body language and social communication, both shaped by cultural and linguistic norms, can present unique challenges for autistic individuals (51). Cultural variations in non-verbal communication may further complicate the interpretation of autistic individuals’ physical expressions. For example, while typically developing children tend to display open, outward-directed movements, autistic children often exhibit inward, closed postures and lighter movements. However, these differences should not be seen merely as deficits but rather as intrinsic aspects of their identity. As Gowen and collaborators suggest, it is no longer “one big clumsy mess” but “a fundamental part of [their] character” (52). Future research should explore how cultural expectations around body language influence the perception and interpretation of autistic individuals’ movements, rather than treating these differences as barriers.
4 A more culturally sensitive healthcare model
Several culturally sensitive models have been developed to address these issues and enhance patient-centered care (53). In response to increasing diversity, healthcare professionals, and policymakers are developing culturally competent services that align communication and care with patients’ values (54). For example, the Patient-Centered Culturally Sensitive Health Care Model has demonstrated that when healthcare providers exhibit cultural sensitivity, patient adherence to treatment improves among ethnically diverse patients, particularly low-income African American and non-Hispanic White Americans, seen in community-based primary care clinics. However, a recent scoping review highlights significant heterogeneity in cultural competence models and interventions, with most focusing on racial and ethnic diversity, particularly in minority populations, overlooking cultural diversity. This underscores the need for more inclusive models suited to Europe’s superdiverse populations and beyond (55).
Another crucial initiative is the ACT Cultural Model, which provides guiding principles for culturally competent care, emphasizing the integration of cultural sensitivity training into both undergraduate and postgraduate healthcare education. A meta-ethnographic review further underscores the importance of self-awareness, cultural sensitivity, and effective collaboration with patients and families (56, 57). Keehn et al. (21) applied the Ecological Validity Framework in Kenya to co-develop a caregiver training program, emphasizing the importance of community partnership and culturally grounded design. Their approach illustrates how interventions can be meaningful and scalable when co-created with local stakeholders. Additionally, Kang-Yi et al. (22) examined how community-level cultural beliefs profoundly shape both caregiver help-seeking behaviors and professional diagnostic pathways. Despite the widespread recognition of cultural competence, research on its impact remains limited, particularly in specialized areas such as autism assessment and intervention (58). Moreover, the challenges associated with autism diagnosis in low-resource settings highlight the urgent need for culturally sensitive assessment tools. The absence of culturally appropriate diagnostic tools and a shortage of trained professionals can severely hinder autism diagnosis and treatment, especially in diverse cultural contexts (59). Similarly, it has been shown that screening tools for autism are often unavailable or poorly understood in certain cultural settings, resulting in delays in diagnosis and intervention (60). Note that these issues are not unique to autism; they extend to other mental and physical health conditions, where cultural factors significantly impact the accessibility and effectiveness of diagnostic tools and treatments, this further highlights the absolute necessity of developing more culturally adapted and less language dependent assessment tools.
Beyond diagnosis, the experiences of individuals with autism and their families further illustrate the critical role of cultural factors in shaping both clinical outcomes and lived experiences. For instance, research highlights how social policies and cultural narratives influence the identities of individuals with autism, underscoring the need for policies that reduce stigma and promote understanding (61). Cultural perceptions do not only affect the diagnostic process but also shape societal attitudes, access to support, and the well-being of autistic individuals and their families. These challenges parallel those faced by individuals with other health conditions, where cultural stigma may impact treatment adherence and patient outcomes. Table 1 summarizes key cultural influences on autism and outlines their implications for patients and the delivery of healthcare.
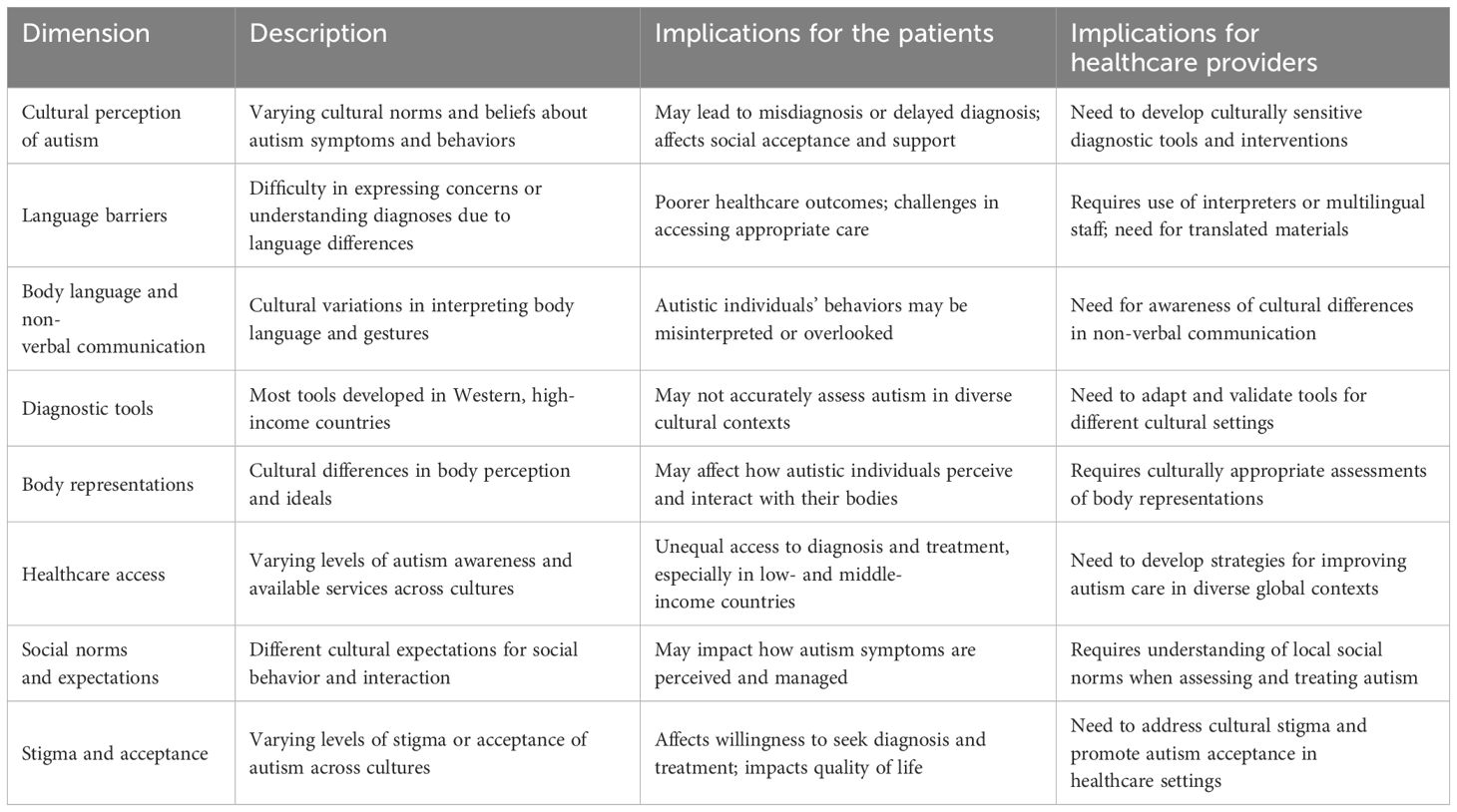
Table 1. Key aspects of autism that can be influenced by culture and language, highlighting the complexities involved in providing culturally sensitive care for autistic individuals across diverse global contexts.
5 Call for action: bridging cultural gaps in autism and BRs
It is imperative that we address the significant cultural and geographical gaps in our understanding of BR. Current research predominantly hails from developed countries, leading to skewed insights and culturally limited assessment tools. This Western-centric focus neglects the diverse manifestations of autism that occur across different global cultures, potentially resulting in misdiagnoses and ineffective interventions.
To improve this, more inclusive and adaptable diagnostic tools that reflect a multitude of cultural contexts need to be developed. Researchers and practitioners should prioritize collaborations between HICs and LMICs to ensure a broader, more comprehensive understanding of BRs and autism. However, such collaboration must consider the economic and infrastructural constraints in LMICs. Funding, staffing, and technological gaps remain key barriers. To address feasibility, we propose several cost-effective and scalable approaches. Mobile health (mHealth) tools, such as app-based screening and tablet assessments, can be delivered in local languages and administered by trained lay health workers. These tools can be integrated into existing community-based health programs and public health systems, such as those supported by the WHO’s Mental Health Gap Action Program (mhGAP). Participatory co-design involving local clinicians, families, and autistic individuals is essential to ensure cultural relevance and uptake. Open-access diagnostic protocols and public–private partnerships can help mitigate financial constraints and reduce dependency on expensive, proprietary Western tools.
Investing in local research within LMICs and fostering cross-cultural partnerships will pave the way for diagnostic advancements that are both accurate and accessible worldwide.
Furthermore, integrating cultural sensitivity into autism assessments will improve their relevance and effectiveness. This involves tailoring interventions to align with regional norms, language proficiencies, and communication styles, ensuring that all individuals receive equitable care and support.
Additionally, cross-cultural adaptation and validation of diagnostic tools are crucial to ensure they account for local languages, cultural norms, and ecological contexts. Emerging technology-based, unsupervised methods for longitudinal assessment, such as digital phenotyping, offer promising solutions, particularly in regions with limited access to healthcare professionals (62). These innovations could help integrate BR assessments into natural environments, making diagnosis and intervention more accessible and ecologic.
Taken together, these solutions represent feasible, scalable strategies to address Western-centric limitations and promote culturally informed autism diagnostics in diverse global settings.
6 Conclusion
In conclusion, integrating cultural factors into autism assessment is a broader necessity in healthcare, as cultural contexts shape the understanding, diagnosis, and treatment of various mental and physical health conditions. Failing to consider these factors presents ethical and practical challenges, particularly in evaluating body representations, a core psychomotor function linked to autonomy and quality of life.
Autism research has historically been Western-centric, overrepresenting white, cisgender, and educated individuals while underrepresenting those from diverse ethnic, cultural, religious, and socioeconomic backgrounds, particularly in LMICs. This representativity bias has distorted the global understanding of autism, leading to misdiagnosis and inadequate support.
To address these disparities, investing in culturally adapted diagnostic tools and digital phenotyping enabling unsupervised, longitudinal assessments is essential. Cross-cultural collaboration among researchers will ensure more accurate, inclusive, and context-sensitive autism assessments.
Author contributions
JM: Conceptualization, Methodology, Formal Analysis, Resources, Writing – original draft, Writing – review & editing. BG: Resources, Conceptualization, Writing – original draft. NP: Conceptualization, Resources, Writing – original draft. KB: Conceptualization, Writing – original draft, Resources. MD: Resources, Conceptualization, Writing – original draft. BB: Writing – original draft, Visualization, Resources, Methodology, Conceptualization.
Funding
The author(s) declare that financial support was received for the research and/or publication of this article. This study is supported by the University of Hasselt and University of Namur through the BOF program (R-13965).
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Generative AI statement
The author(s) declare that no Generative AI was used in the creation of this manuscript.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Hoffmann M, Lanillos P, Jamone L, Pitti A, and Somogyi E. Editorial: body representations, peripersonal space, and the self: humans, animals, robots. Front Neurorobot. (2020) 14:35. doi: 10.3389/fnbot.2020.00035
2. Sattin D, Parma C, Lunetta C, Zulueta A, Lanzone J, Giani L, et al. An overview of the body schema and body image: theoretical models, methodological settings and pitfalls for rehabilitation of persons with neurological disorders. Brain Sci. (2023) 13:1410. doi: 10.3390/brainsci13101410
3. Longo M and Haggard P. An implicit body representation underlying human position sense. Proc Natl Acad Sci United States America. (2010) 107:11727–32. doi: 10.1073/pnas.1003483107
4. Riva G. The neuroscience of body memory: From the self through the space to the others. Cortex. (2018) 104:241–60. doi: 10.1016/j.cortex.2017.07.013
5. Harris L, Carnevale M, D’Amour S, Fraser L, Harrar V, Hoover A, et al. How our body influences our perception of the world. Front Psychol. (2015) 6:819. doi: 10.3389/fpsyg.2015.00819
6. Dijkerman C and Lenggenhager B. The body and cognition: The relation between body representations and higher level cognitive and social processes. Cortex. (2018) 104:133–9. doi: 10.1016/jcortex.2018.06.001
7. Möllmann A, Heinrichs N, and Herwig A A conceptual framework on body representations and their relevance for mental disorders Front Psychol. (2024) 14:1231640. doi: 10.3389/fpsyg.2023.1231640
8. Cascio CJ, Foss-Feig JH, Burnette CP, Heacock JL, and Cosby AA. The rubber hand illusion in children with autism spectrum disorders: Delayed influence of combined tactile and visual input on proprioception. Autism. (2012) 16:406–19. doi: 10.1177/1362361311430404
9. Ropar D, Greenfield K, Smith AD, Carey M, and Newport R. Body representation difficulties in children and adolescents with autism may be due to delayed development of visuo-tactile temporal binding. Dev Cogn Neurosci. (2018) 29:78–85. doi: 10.1016/j.dcn.2017.04.007
10. Haag G, Botbol M, Graignic R, Perez-Diaz F, Bronsard G, Kermarrec S, et al. The Autism Psychodynamic Evaluation of Changes (APEC) scale: A reliability and validity study on a newly developed standardized psychodynamic assessment for youth with Pervasive Developmental Disorders. J Physiology-Paris. (2010) 104:323–36. doi: 10.1016/j.jphysparis.2010.10.002
11. Le Menn-Tripi C, Vachaud A, Defas N, Malvy J, Roux S, and Bonnet-Brilhault F. L’évaluation sensori-psychomotrice dans l’autisme: un nouvel outil d’aide au diagnostic fonctionnel. L’Encéphale. (2019) 45:312–9. doi: 10.1016/j.encep.2018.12.003
12. Alkhalifah SM, AlArifi H, AlHeizan M, Aldhalaan H, and Fombonne E. Validation of the arabic version of the two sensory processing measure questionnaires. Res Autism Spectr Disord. (2020) 78:101652. doi: 10.1016/j.rasd.2020.101652
13. Itoi C, Ujiie Y, Matsushima K, Takahashi K, and Ide M. Validation of the Japanese version of the Interoception Sensory Questionnaire for individuals with autism spectrum disorder. Sci Rep. (2022) 12:21722. doi: 10.1038/s41598-022-25883-y
14. Suzman E, Williams ZJ, Feldman JI, Failla M, Cascio CJ, Wallace MT, et al. Psychometric validation and refinement of the Interoception Sensory Questionnaire (ISQ) in adolescents and adults on the autism spectrum. Mol Autism. (2021) 12:42. doi: 10.1186/s13229-021-00440-y
15. Longhurst P, Todd J, Aspell JE, and Swami V. Psychometric evaluation of a revised version of the body appreciation scale-2 for autistic adults (BAS-2A). Body Image. (2024) 49:101706. doi: 10.1016/j.bodyim.2024.101706
16. Bertilsson I, Melin J, Brogårdh C, Opheim A, Gyllensten AL, Björksell E, et al. Measurement properties of the Body Awareness Scale Movement Quality (BAS MQ) in persons on the autism spectrum: A preliminary Rasch analysis. J Bodywork Movement Therapies. (2024) 38:464–73. doi: 10.1016/j.jbmt.2024.01.004
17. Söchting E, Hartl J, Riederer M, Schönauer C, Kaufmann H, and Lamm C. Development of tests to evaluate the sensory abilities of children with autism spectrum disorder. Proc Comput Sci. (2015) 67:193–203. doi: 10.1016/j.procs.2015.09.263
18. Merino M, Tornero-Aguilera JF, Rubio-Zarapuz A, Villanueva-Tobaldo CV, Martín-Rodríguez A, and Clemente-Suárez VJ. Body perceptions and psychological well-being: A review of the impact of social media and physical measurements on self-esteem and mental health with a focus on body image satisfaction and its relationship with cultural and gender factors. Healthcare. (2024) 12:1396. doi: 10.3390/healthcare12141396
19. Abdoli M, Scotto Rosato M, Desousa A, and Cotrufo P. Cultural differences in body image: A systematic review. Soc Sci. (2024) 13:305. doi: 10.3390/socsci13060305
20. Bernier R, Mao A, and Yen J. Psychopathology, families, and culture: autism. Child Adolesc Psychiatr Clinics North America. (2010) 19:855–67. doi: 10.1016/j.chc.2010.07.005
21. McNally Keehn R, Rispoli M, Saina C, Nafiseh A, Oyungu E, Omari FW, et al. Pepea Pamoja:† Applying the Ecological Validity Framework to co-develop a wellbeing and behavioural training program for caregivers of young children with autism in low-resource settings of Kenya and the United States. Child Care Health Dev. (2024) 50:e13299. doi: 10.1111/cch.13299
22. Kang-Yi CD, Grinker RR, Beidas R, Agha A, Russell R, Shah SB, et al. Influence of community-level cultural beliefs about autism on families’ and professionals’ Care for children. Transcult Psychiatry. (2018) 55:623–47. doi: 10.1177/1363461518779831
23. Leeuw A, Happe F, and Hoekstra R. A conceptual framework for understanding the cultural and contextual factors on autism across the globe. Autism research: Off J Int Soc Autism Res. (2020) 13. doi: 10.1002/aur.2276
24. Adams S. The unmasking of autism in South Africa and Nigeria. NDT. (2024) 20:947–55. doi: 10.2147/NDT.S461650
25. Aderinto N, Olatunji G, and Oluwatobi I. Autism in africa: prevalence, diagnosis, treatment, and the impact of social and cultural factors on families and caregivers; A review and wirral partnership NHS foundation trust A C C E P T E D. Ann Med Surg. (2012) 2023):85. doi: 10.1097/MS9.0000000000001107
26. Dey I, Chakrabarty S, Nandi R, Shekhar R, Singhi S, Nayar S, et al. Autism community priorities in diverse low-resource settings: A country-wide scoping exercise in India. Autism. (2023) 28:187. doi: 10.1177/13623613231154067
27. Samadi SA. Overview of services for autism spectrum disorders (ASD) in low- and middle-income countries (LMICs) and among immigrants and minority groups in high-income countries (HICs). Brain Sci. (2022) 12:1682. doi: 10.3390/brainsci12121682
28. Wang F, Lu L, Wang S-B, Zhang L, Ng CH, Ungvari GS, et al. The prevalence of autism spectrum disorders in China: a comprehensive meta-analysis. Int J Biol Sci. (2018) 14:717–25. doi: 10.7150/ijbs.24063
29. Elsabbagh M, Divan G, Koh Y-J, Kim YS, Kauchali S, Marcín C, et al. Global prevalence of autism and other pervasive developmental disorders. Autism Res. (2012) 5:160–79. doi: 10.1002/aur.239
30. Donthu N, Kumar S, Mukherjee D, Pandey N, and Lim WM. How to conduct a bibliometric analysis: An overview and guidelines. J Business Res. (2021) 133:285–96. doi: 10.1016/j.jbusres.2021.04.070
31. van Eck NJ and Waltman L. Software survey: VOSviewer, a computer program for bibliometric mapping. Scientometrics. (2010) 84:523–38. doi: 10.1007/s11192-009-0146-3
32. Alallawi B, Hastings RP, and Gray G. A systematic scoping review of social, educational, and psychological research on individuals with autism spectrum disorder and their family members in arab countries and cultures. Rev J Autism Dev Disord. (2020) 7:364–82. doi: 10.1007/s40489-020-00198-8
33. Alkhateeb JM, Hadidi MS, and Alkhateeb AJ. Inclusion of children with developmental disabilities in Arab countries: A review of the research literature from 1990 to 2014. Res Dev Disabil. (2016) 49–50:60–75. doi: 10.1016/j.ridd.2015.11.005
34. Taha GRA, Hussein H, and Almanasef A. Two years’ outcome of autism in a sample of Egyptian and Saudi children: a comparative prospective naturalistic study. Middle East Curr Psychiatry. (2013) 20:122–30. doi: 10.1097/01.XME.0000430434.74114.01
35. Hussein H and Taha GRA. Autism spectrum disorders: a review of the literature from Arab countries. Middle East Curr Psychiatry. (2013) 20:106–16. doi: 10.1097/01.XME.0000430433.49160.a4
36. Yang B, Liao J, Tang X, and Wang M. Loving body loving life: body image and life satisfaction in different cultures. Curr Psychol. (2025) 44:3643–51. doi: 10.1007/s12144-025-07386-x
37. Rodgers RF, Laveway K, Campos P, and de Carvalho PHB. Body image as a global mental health concern. Glob Ment Health (Camb). (2023) 10:e9. doi: 10.1017/gmh.2023.2
38. Naigaga DA, Jahanlu D, Claudius HM, Gjerlaug AK, Barikmo I, and Henjum S. Body size perceptions and preferences favor overweight in adult Saharawi refugees. Nutr J. (2018) 17:17. doi: 10.1186/s12937-018-0330-5
39. Fuchs T. Chapter 1. “The phenomenology of body memory”. In: Koch SC, Fuchs T, Summa M, and Müller C, editors. Body memory, metaphor and movement. Amsterdam, The Netherlands: John Benjamins Publishing Company, (2012). p. 9–22. Available online at: https://www.degruyterbrill.com/document/doi/10.1075/aicr.84.03fuc/pdf.
40. Waterman A, Giles O, Jelena H, Ali S, Culmer P, Wilkie R, et al. Sensorimotor control dynamics and cultural biases: Learning to move in the right (or left) direction. R Soc Open Sci. (2017) 4:160806. doi: 10.1098/rsos.160806
41. Wang S and Basch S. “Chapter Six - A cultural perspective of action-based learning by infants and young children”. In: Lockman JJ, editor. Advances in child development and behavior. London, United Kingdom (Elsevier’s primary editorial office): JAI (an imprint of Elsevier), (2024). p. 164–99. doi: 10.1016/bs.acdb.2024.07.003
42. Cascio CJ, Moana-Filho EJ, Guest S, Nebel MB, Weisner J, Baranek GT, et al. Perceptual and neural response to affective tactile texture stimulation in adults with autism spectrum disorders. Autism research: Off J Int Soc Autism Res. (2012) 5:231. doi: 10.1002/aur.1224
43. Schauder KB, Mash LE, Bryant LK, and Cascio CJ. Interoceptive ability and body awareness in autism spectrum disorder. J Exp Child Psychol. (2015) 131:193–200. doi: 10.1016/j.jecp.2014.11.002
44. Izawa J, Pekny SE, Marko MK, Haswell CC, Shadmehr R, and Mostofsky SH. Motor learning relies on integrated sensory inputs in ADHD, but over-selectively on proprioception in autism spectrum conditions. Autism Res. (2012) 5:124. doi: 10.1002/aur.1222
45. Han S and Northoff G. Culture-sensitive neural substrates of human cognition: a transcultural neuroimaging approach. Nat Rev Neurosci. (2008) 9:646–54. doi: 10.1038/nrn2456
46. Kitayama S and Huff S. “Cultural neuroscience: connecting culture, brain, and genes”. In: Scott RA and Kosslyn SM, editors. Emerging trends in the social and behavioral sciences. Hoboken, NJ, USA: Wiley (2015). p. 1–16. doi: 10.1002/9781118900772.etrds0062
47. Hao Z, Shi Y, Huang L, Sun J, Li M, Gao Y, et al. The atypical effective connectivity of right temporoparietal junction in autism spectrum disorder: A multi-site study. Front Neurosci. (2022) 16:927556. doi: 10.3389/fnins.2022.927556
48. Misic-Ilic B. Language and culture studies - wonderland through the linguistic looking glass. In: Facta universitatis: series linguistics and literature. Niš, Serbia: University of Niš (2004). p. 1–15.
49. Alnahdi GH. Variations in perceptions of well-being within families of youths with intellectual disabilities in Saudi Arabia. Children (Basel). (2024) 11:644. doi: 10.3390/children11060644
50. Stefani ED and Marco DD. Language, gesture, and emotional communication: an embodied view of social interaction. Front Psychol. (2019) 10:2063. doi: 10.3389/fpsyg.2019.02063
51. Safira I, Rangkuti R, Nasution E, and Harefa Y. Non-verbal communication by autistic children. ELS J Interdiscip Stud Humanities. (2020) 3:492–505. doi: 10.34050/elsjish.v3i4.8065
52. Gowen E, Earley L, Waheed A, and Poliakoff E. From “one big clumsy mess” to “a fundamental part of my character.” Autistic adults’ experiences of motor coordination. PloS One. (2023) 18. doi: 10.1371/journal.pone.0286753
53. Tucker CM, Marsiske M, Rice KG, Nielson JJ, and Herman K. Patient-centered culturally sensitive health care: Model testing and refinement. Health Psychol. (2011) 30:342–50. doi: 10.1037/a0022967
54. Hickson SV. Assessment of cultural competency. Clinics Integrated Care. (2023) 21:100173. doi: 10.1016/j.intcar.2023.100173
55. De-María B, Topa G, and López-González MA. Cultural competence interventions in european healthcare: A scoping review. Healthcare. (2024) 12:1040. doi: 10.3390/healthcare12101040
56. Li S, Miles K, George RE, Ertubey C, Pype P, and Liu J. A critical review of cultural competence frameworks and models in medical and health professional education: A meta-ethnographic synthesis: BEME Guide No. 79. Med Teacher. (2023) 45:1085–107. doi: 10.1080/0142159X.2023.2174419
57. Brooks LA, Manias E, and Bloomer MJ. Culturally sensitive communication in healthcare: A concept analysis. Collegian. (2019) 26:383–91. doi: 10.1016/j.colegn.2018.09.007
58. Rukadikar C, Mali S, Bajpai R, Rukadikar A, and Singh AK. A review on cultural competency in medical education. J Family Med Primary Care. (2022) 11:4319. doi: 10.4103/jfmpc.jfmpc_2503_21
59. Durkin MS, Elsabbagh M, Barbaro J, Gladstone M, Happe F, Hoekstra RA, et al. Autism screening and diagnosis in low resource settings: Challenges and opportunities to enhance research and services worldwide. Autism Res. (2015) 8:473–6. doi: 10.1002/aur.1575
60. Al-Beltagi M. Pre-autism: What a paediatrician should know about early diagnosis of autism. World J Clin Pediatr. (2023) 12:273–94. doi: 10.5409/wjcp.v12.i5.273
61. Mogensen L and Mason J. The meaning of a label for teenagers negotiating identity: experiences with autism spectrum disorder. Sociology Health Illness. (2015) 37:255–69. doi: 10.1111/1467-9566.12208
Keywords: body representations, body image, body schema, culture, autism
Citation: Mourad J, Grosjean B, Perroud N, Bogaerts K, Desseilles M and Bonnechère B (2025) Rethinking body representations in autism across cultures. Front. Psychiatry 16:1612219. doi: 10.3389/fpsyt.2025.1612219
Received: 15 April 2025; Accepted: 11 July 2025;
Published: 04 August 2025.
Edited by:
Jonna Bobzien, Old Dominion University, United StatesReviewed by:
Christianna Blanchard-Alworth, Old Dominion University, United StatesCopyright © 2025 Mourad, Grosjean, Perroud, Bogaerts, Desseilles and Bonnechère. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Joanna Mourad, Sm9hbm5hLm1vdXJhZEB1aGFzc2VsdC5iZQ==