 Sevim B. Bianchi1,2
Sevim B. Bianchi1,2 Laura Vilar-Ribó1
Laura Vilar-Ribó1 Abraham A. Palmer1,3
Abraham A. Palmer1,3 Daniel E. Gustavson4
Daniel E. Gustavson4 Sandra Sanchez-Roige1,3,5*
Sandra Sanchez-Roige1,3,5*- 1Department of Psychiatry, University of California San Diego, La Jolla, CA, United States
- 2College of Medicine, California Northstate University, Elk Grove, CA, United States
- 3Institute for Genomic Medicine, University of California San Diego, La Jolla, CA, United States
- 4Institute for Behavioral Genetics, University of Colorado Boulder, Boulder, CO, United States
- 5Department of Medicine, Division of Genetic Medicine, Vanderbilt University, Nashville, TN, United States
Anorexia nervosa (AN) is a heritable condition, characterized by a fear of weight gain and a distorted body image, for which treatments are only limited. AN is characterized by excessive control over feeding behaviors, which has been hypothesized to indicate that low impulsivity, including low emotional impulsivity (urgency), may place certain individuals at risk for AN; however, this has not been fully genetically evaluated. We used genomic structural equation modeling and genome-wide association studies (GWASs) based on individuals of European ancestry (n = 72,517–903,147) to examine the latent genetic architecture between AN and several measures of impulsivity. Because AN is positively genetically associated with substance use disorders (SUDs), which are also strongly associated with impulsivity, we conditioned our analyses using GWAS data from four SUDs (alcohol, tobacco, cannabis, and opioid use disorders). AN was not significantly genetically correlated with impulsivity latent factors as indices of Barratt Impulsiveness Scale (BIS) or Urgency, Premeditation, Perseverance, Sensation Seeking, and Positive Urgency (UPPS) subscales (common impulsivity, rg = −0.07; urgency-specific impulsivity, rg = 0.14; and sensation seeking, rg = −0.07) but was significantly negatively genetically correlated with delay discounting (rg = −0.19) and lack of perseverance (rg = −0.15), even after controlling for SUDs (rg = −0.32 or rg = −0.25, respectively). This work suggests that delay discounting and lack of perseverance capture genetically informative dimensions of AN; clarifying shared etiologies could inform AN diagnosis and treatment mechanisms.
Introduction
Anorexia nervosa (AN) is characterized by a fear of weight gain and a distorted body image, often accompanied by excessive self-control over restricted food intake and other weight loss-related behaviors (1). Up to 4% of female and 0.3% of male individuals are affected by AN, and the incidence among persons younger than 15 has increased in recent years (2). AN can cause serious adverse health outcomes, leading it to have the highest mortality rate of any psychiatric disorder, five times what is observed in the general population according to age and sex (3). While treatments for AN exist, their efficacy and overall recovery rates remain low (1). Elucidating risk factors contributing to AN development could illuminate the potential for novel treatment and prevention mechanisms.
Individuals with AN exhibit excessive control over feeding behavior for potential future reward (i.e., further weight loss), even when such behavior is life-threatening (4). Self-control is the opposite of impulsivity, which has been defined as thoughts or actions that are “poorly conceived, prematurely expressed, unduly risky or inappropriate to the situation, and that often result in undesirable consequences” (5). However, the construct of impulsivity is multifaceted (6). Impulsivity facets can be captured via self-reported questionnaires, such as the UPPS-P Impulsive Behavior Scale (7, 8) and Barratt Impulsiveness Scale (BIS-11) (9), and related constructs, such as delay discounting (DD), which is the tendency to favor smaller current rewards over larger future rewards and can be measured using a number of procedures (e.g (10–12)). Several studies have explored the association between AN and impulsivity/DD, often identifying excessively low levels of impulsivity/DD in patients with AN (phenotypic studies: e.g (13–18)), yet results continue to remain highly variable (15). A number of genetic studies have been conducted to evaluate this relationship as well (e.g (19–22)); however, the unique contribution of individual impulsivity facets and AN has not been explored. Therefore, the combination of high phenotypic variability and the limited number of genetic studies exploring this relationship prompts further investigation via novel genetic tools. Identifying overlapping genetic factors underpinning AN and specific impulsivity facets can offer novel insights into disease pathophysiology.
There is an extremely well-established relationship between impulsivity and propensity for various substance use disorders (SUDs) (19, 21, 23–25). The most recent study by Vilar-Ribó et al. demonstrated that both substance use and SUD traits showed distinct associations with different impulsivity facets (25). In turn, AN is also positively associated with SUDs (26–30). The systematic review by Bahji et al. reported a pooled lifetime and current prevalence of eating disorders with any comorbid SUDs of 21.9% (26). Furthermore, Mellentin et al. showed that SUDs lead to an additive effect on excess mortality in eating disorders (28). In order to begin to tease out these associations, we used multivariate statistical techniques and genetic data to further examine the relationship between AN, facets of impulsivity, DD, and SUDs.
Methods
Genome-wide association studies
All genome-wide association study (GWAS) summary statistics were based on individuals of European ancestry based on genetic similarity (31), as summarized below; a full list of sample sizes and sample types is included in Supplementary Table S1. Because GWASs map associations to a common reference panel (i.e., the human genome), this enables us to explore associations even when they were conducted in separate populations (with different ascertainment schemes).
Anorexia nervosa
We used summary statistics from the most recent independent GWASs of AN (32). The clinical sample included 16,992 cases and 55,525 controls of European ancestry. This sample came from the Psychiatric Genomics Consortium (PGC) Eating Disorders Working Group (https://pgc.unc.edu/for-researchers/download-results/).
Impulsivity
GWASs of impulsivity were based on a sample of up to 133,517 23andMe Inc. research participants (20, 21). These included measures from the UPPS-P Impulsive Behavior Scale (7, 8) and the BIS-11 scale (9). The 20-item brief version UPPS-P Impulsive Behavior Scale consists of five subscales (“lack of premeditation”, “lack of perseverance”, “positive urgency”, “negative urgency”, and “sensation seeking”). The 30-item BIS consists of three subscales (“attentional”, “motor”, and “non-planning”).
Delay discounting
We used summary statistics from a recent GWAS of DD from 23andMe (22). Although we did not have data about the frequency of AN among these 23andMe research participants, we presumed that it was low given the low population prevalence of this diagnosis. Higher scores indicate greater valuation of short-term versus long-term rewards, or “steeper” DD.
Substance use disorders
We used summary statistics from GWASs of cannabis use disorder (CUD) (33), tobacco use disorder (TUD) (34), opioid use disorder (OUD) (35), and problematic alcohol use (PAU) (36).
Data analyses
We conducted all analyses in R version 4.1.1 (37). We used the genomic structural equation modeling (SEM) package (38), which applies SEM methods to GWAS summary statistics. Genomic SEM leverages linkage disequilibrium score regression (39) to generate a genetic correlation matrix between all traits for which summary statistics are available. Figure 1 shows the genetic correlation matrix among all study variables. We modeled impulsivity and SUD factors based on our previous genomic SEM analyses (25, 40, 41). Although some models include perseverance and sensation seeking as impulsivity facets, our prior work showed that they are not strong contributors to a common impulsivity factor and are genetically distinguishable (40). Therefore, we modeled lack of perseverance and sensation seeking as separate indicators, along with DD (25, 40, 42).

Figure 1. Genetic correlation (rg) matrix between all study variables. NU, UPPS-P Negative Urgency; PU, UPPS-P Positive Urgency; Premediation, BIS Premeditation; Attentional, BIS Attentional; Motor, BIS Motor; Nonplanning, BIS Nonplanning; Perseverance, BIS Lack of Perseverance; Sensation Seeking, BIS Sensation Seeking; DD, delay discounting; PAU, problematic alcohol use; CUD, cannabis use disorder; OUD, opioid use disorder; TUD, tobacco use disorder; AN, anorexia nervosa. The different-sized dots represent the magnitude of rg values. rg values and SE can be found in Supplementary Table S2.
Next, we fit SEMs to the data using genomic SEM, which drew on functionality from the lavaan R package (43). We fit two versions of this model: a) a correlated factor model where we estimated the genetic correlations between impulsivity, SUD, and AN factors, and b) a multiple regression, where AN was regressed on impulsivity and SUD factors. We used the default diagonally weighted least squares (DWLS) estimation method in these analyses. We determined the model fit based on chi-square tests (χ2), the comparative fit index (CFI), the Akaike information criterion (AIC), and the standardized root mean square residual (SRMR). We expected good-fitting models to have CI > 0.95 (0.90 for acceptable fit), SRMR < 0.08, and smaller AIC values compared with competing nested models (Hu & Bentler, 1998). Good-fitting models also traditionally have non-significant χ2 statistics. However, because sample sizes in GWASs are extremely large and χ2 statistics are sensitive to sample size, we focused on other fit indices. We established the significance of individual parameter estimates with standard errors (SEs) and p-values.
Data availability
GWAS summary statistics for AN and the SUD traits are publicly available. Data from 23andMe are available upon request (see https://research.23andme.com/dataset-access/). The R data files containing the genomic SEM matrices for all analyses are displayed at the following link: https://osf.io/4tjw5/. This allows for replication and analyses of competing models without obtaining the source data.
Results
Latent variable models of anorexia nervosa and impulsivity
First, a correlational model of impulsivity facets, SUD, and AN was constructed. This model included two latent factors for impulsivity, capturing common variance across impulsive urgency and lack of premeditation (common impulsivity) and variance unique to impulsive urgency (urgency-specific impulsivity). DD, SS, and lack of perseverance were modeled as separate indicators based on our prior work showing that these constructs are genetically distinguishable (25, 40, 42). The four SUDs were modeled using a single factor (substance use disorders), similar to recent studies (41, 44). AN was included as a separate indicator. This model is displayed in Figure 2 and had an acceptable fit (χ2(x) = 1,035.32, p < 9.30E−178, CFI = 0.940, SRMR = 0.074).
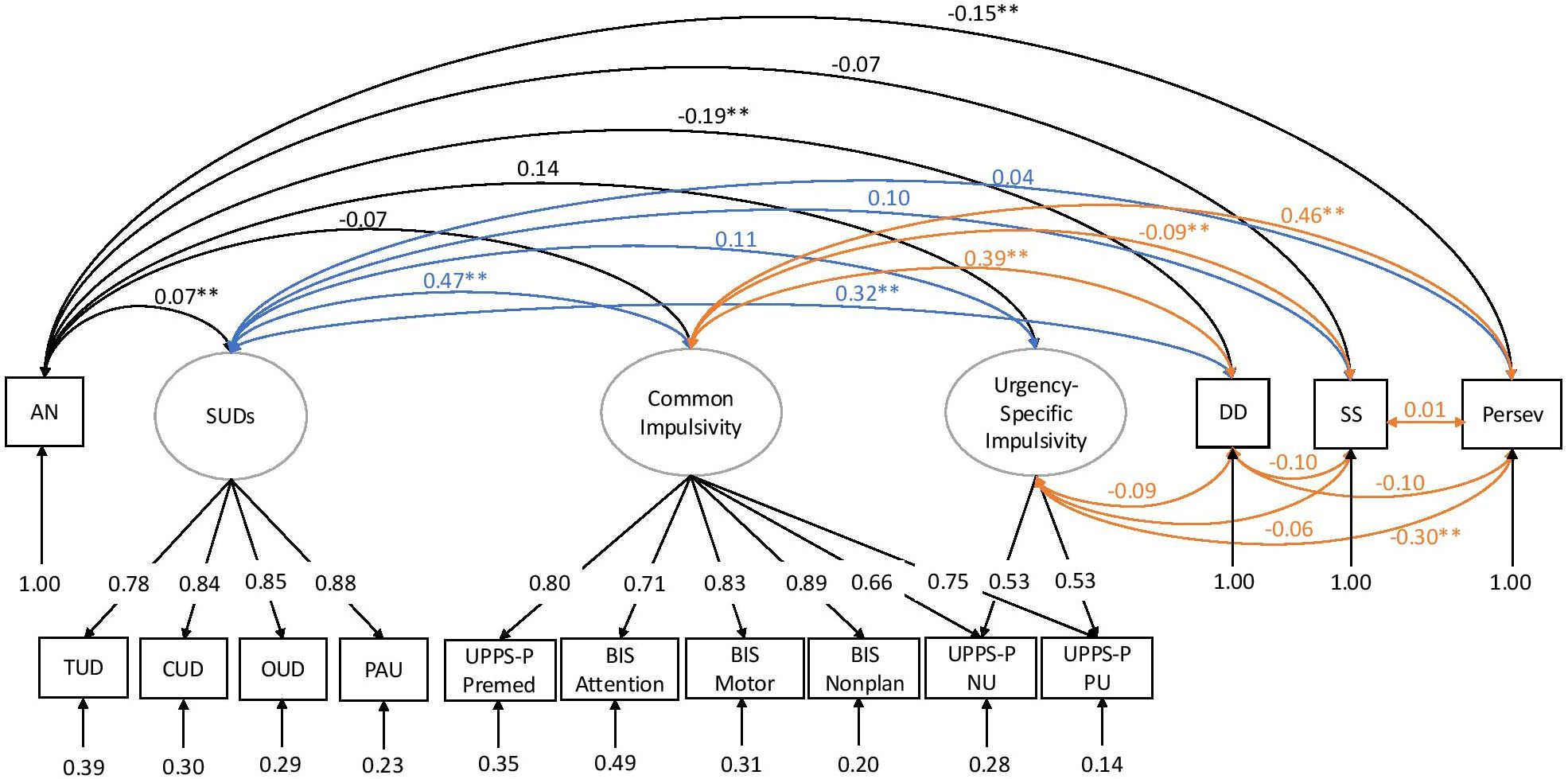
Figure 2. Genetic correlation model with AN, impulsivity facets, SUDs, delay discounting, sensation seeking, and lack of perseverance, adapted from prior studies (40). Ovals indicate latent factors, and squares indicate individual GWAS summary statistics. In this model, a “common impulsivity” factor successfully captured the shared variance across selected measures of the UPPS-P and BIS scales. To capture the particularly high correlation among UPPS-P negative urgency and UPPS-P positive urgency subscales, we included a second latent factor called “urgency-specific impulsivity”, which was fixed to be uncorrelated with genetic variance in common impulsivity. The four SUDs were modeled using a single factor (“substance use disorders”). The values under each trait represent the residual variances of the indicators. The colors are included for ease of visualization (e.g., black, correlations with AN; blue, correlations with SUDs; orange, correlations among impulsivity facets). UPPS-P NU, UPPS-P Negative Urgency; UPPS-P PU, UPPS-P Positive Urgency; UPPS-P Premed, UPPS-P Premediation; BIS Nonplan, BIS Nonplanning; SUDs, substance use disorders; PAU, problematic alcohol use; CUD, cannabis use disorder; OUD, opioid use disorder; TUD, tobacco use disorder; SS, BIS Sensation Seeking; Persev, BIS Lack of Perseverance; DD, delay discounting; AN, anorexia nervosa; GWASs, genome-wide association studies.
AN was negatively genetically correlated with DD (rg = −0.19, SE = 0.039, p = 1.63E−06) and lack of perseverance (rg = −0.15, SE = 0.045, p = 7.51E−04) but not with the common impulsivity, urgency-specific factors, or SS. AN had a modest but significant positive genetic correlation with the SUD factor (rg = 0.07, SE = 0.027, p = 7.18E−03).
After conditioning on SUDs and impulsivity (by regressing AN on all other factors), AN was still negatively genetically correlated with delay discounting (β = −0.32, p = 4.63E−05) and lack of perseverance (β = −0.25, p = 5.52E−03). In contrast, we continued to observe non-significant negative genetic correlations between AN and the common and urgency-specific impulsivity factors (β = 0.14, p = 0.203, and β = 0.01, p = 0.99, respectively). In this model, SS was also significant with AN only after conditioning for SUDs (β = −0.14, p = 8.77E−03).
Discussion
Using existing GWAS data, we investigated genetic associations between AN and multiple impulsivity facets. We found that AN was significantly negatively genetically associated with DD and lack of perseverance, while the genetic associations with common impulsivity, urgency-specific impulsivity, and SS were non-significant. These observations held even after controlling for the shared genetic variance among SUDs. This discovery, as we elaborate below, can have important implications for our understanding of the genetic susceptibility to AN, an illness with the highest mortality rate among all psychiatric disorders (3). It also illustrates that both extremes of impulsivity are associated with psychiatric disorders: steeper DD (i.e., greater discounting of delayed rewards) has been previously associated with SUDs and ADHD, among others (23, 45, 46), whereas the current report illustrates that shallower DD is associated with AN, and prior reports have similarly shown a relationship between low DD and obsessive compulsive disorder (OCD) (47). Likewise, the negative association between lack of perseverance and AN is countered by an increase in lack of perseverance found in borderline personality disorder (48).
Identifying common genetic relationships between AN and impulsivity facets can offer novel insights into disease pathophysiology. In addition to genetic correlations of individual traits (Figure 1), we also performed a multi-factorial analysis of impulsivity that included multiple facets via two well-established questionnaires, UPPS-P and BIS-11, and DD. We identified that AN was not significantly genetically associated with the UPPS/BIS measures of impulsivity, except lack of perseverance, which distinguished our results from previous phenotypic studies that identified both positive and negative associations between AN and attentional impulsivity, negative urgency, positive urgency, motor impulsivity, and sensation seeking (positive, e.g (14, 16, 17, 49–52); negative, e.g (13, 17, 53); neither, e.g (15)). In our study, SS was correlated with AN only after controlling for shared variance among SUDs. However, these findings support our previous work showing that emotional impulsivity, specifically urgency-specific genetic influences, is much more closely tied to internalizing traits than other psychiatric conditions, such as AN (40). There are a few possibilities for this discrepancy, one being ascertainment differences, namely, higher rates of mood disorders, as described in (17, 52), or that prior positive associations are indicative of consequences of the illness. Additionally, phenotypic associations are due to both genetic and environmental contributions. The lack of significant genetic associations observed here suggests that phenotypic associations observed by prior studies may reflect environmental rather than genetic factors.
In contrast, we found a negative genetic correlation with DD, in agreement with prior phenotypic studies (4, 54, 55). This association suggests that the increased capacity to delay reward could be an endophenotype for AN (4). Our findings also suggest that DD is a significant correlate of AN (56) since the datasets used for the genetic correlations were derived from independent cohorts (i.e., individuals from the impulsivity and DD datasets were not ascertained for AN). Notably, genomic SEM does not require that AN be directly represented in the impulsivity GWAS sample. Instead, it models the genetic covariance between traits using GWAS summary statistics, regardless of phenotypic co-occurrence within cohorts. Therefore, the observed associations reflect the shared genetic architecture, not sample overlap. However, the specific biological mechanisms underlying AN and DD remain unknown; multivariate approaches combining GWASs of AN and DD may help us identify specific genetic markers that could contribute to disease pathophysiology (57).
Studying the relationship between AN with DD and lack of perseverance could lead to novel insights into potential diagnostic mechanisms (15). First, DD could be used in combination with the existing AN diagnostic criterion (18, 54). Based on the lack of significant correlations (albeit with the same negative direction) with other impulsivity facets identified in this study, or increased/decreased associations with other impulsivity traits in prior phenotypic studies, AN may be best conceptualized as a mixture of behaviors of under-and-over control in the same individual, which should be considered when formulating diagnostic approaches (15). Intriguingly, high levels of DD and impulsivity facets are transdiagnostic traits for many psychiatric conditions, particularly those on the externalizing spectrum, such as SUDs (23) and ADHD (46).
Second, modulating DD could be considered for treatment approaches because of its role in both clinical presentation and outcomes (16, 17, 58). Prior studies have suggested that increasing DD has alleviated AN symptomatology (e.g., excessive focus on maintaining a low weight over time) (4, 15, 54, 59, 60). However, it is possible that the same is not true for other eating disorders, such as bulimia nervosa and binge-eating disorder, which possess a slightly different profile of associated impulsivity facets (16, 47, 55). Furthermore, the positive associations between DD/impulsivity and SUDs suggest that substance use should also be monitored when considering impulsivity facets as modifiable factors (47).
We observed a significant negative genetic association between AN and lack of perseverance. Another phenotypic study found that lack of perseverance was associated with restraint, eating concern, and shape concern when looking at associations of the facets of impulsivity and AN within a cohort of women (61). However, the extent to which this trait could serve as an endophenotype for AN is more of an unknown. Other studies have shown that lack of perseverance is a trait less related to emotions and more specifically characterizes patients with bulimia spectrum disorders more than AN, suggesting group differences (16, 49, 50). There is a lack of studies in the literature further phenotypically exploring the specific association with AN to draw more concrete conclusions about its clinical relevance.
The current literature describes that AN is typically characterized by low impulsivity and SUDs by high impulsivity, yet there is a positive correlation between AN and SUDs. The current study reinforces this by showing that the association between AN and SUDs persists after controlling for impulsivity. This relationship may be due to a number of factors, such as genetic risks, brain chemistry, family history, trauma, low self-esteem, depression, anxiety, and social pressures (62). However, previous phenotypic studies have reported this finding to be most prevalent in the binge eating/purging subtype of AN (26, 63). Further analysis of the different AN subtypes will further define the relationship between AN and SUDs and what populations are at the highest risk.
Our study is not without limitations. Differences between self-reported and behavioral measures of DD have been documented in AN patients (15), but our study only considered self-reported measures. In addition, there are two subtypes of AN, restrictive or binge/purge, with the binge/purge subtype showing a greater phenotypic association with impulsivity (17). However, we used summary statistics from an AN GWAS that was not subtype-specific. Additionally, there are other aspects of AN that we have not considered. Compulsivity is related to AN via behaviors of rumination thoughts toward starvation and rigidity in eating behavior (61, 64). Impulsivity and compulsivity may not be completely separable components (61); however, to date, there are no GWASs of compulsivity. Furthermore, GWASs were only conducted in individuals with European genetic similarity; therefore, it is unknown if our findings will generalize to other populations as larger non-European samples become available. Lastly, the associations examined here are based purely on genetic data, which may differ from those of an environmental nature. Longitudinal studies and more diversity in the GWASs of AN and its symptomatology could help identify sensitive periods where the role of impulsivity may be most salient in the prognosis of AN (56).
Our study has uncovered an overlapping genetic basis between AN and the impulsivity domains of DD and lack of perseverance. Based on the literature, a better understanding of the shared genetic and environmental etiologies between AN and these specific impulsivity facets could inform AN diagnostic and treatment strategies.
Data availability statement
The original contributions presented in the study are included in the article/Supplementary Material. Further inquiries can be directed to the corresponding author.
Author contributions
SBB: Data curation, Formal Analysis, Investigation, Methodology, Resources, Visualization, Writing – original draft. LVR: Formal Analysis, Investigation, Writing – review & editing. AAP: Investigation, Resources, Writing – review & editing. DEG: Conceptualization, Formal Analysis, Investigation, Methodology, Supervision, Writing – original draft. SSR: Conceptualization, Formal Analysis, Funding acquisition, Investigation, Methodology, Resources, Supervision, Writing – original draft.
Funding
The author(s) declare that financial support was received for the research and/or publication of this article. This work was supported by the National Institutes of Health DP1DA054394. SBB, AAP, and SS-R were also supported by funds from the California Tobacco-Related Disease Research Program (TRDRP; Grant Numbers 28IR-0070, T29KT0526, and T32IR5226). LVR is funded by the Interdisciplinary Research Fellowship in NeuroAIDS (5R25MH081482-18).
Acknowledgments
We would like to thank the research participants and employees of 23andMe, Inc., for making this work possible.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Generative AI statement
The author(s) declare that no Generative AI was used in the creation of this manuscript.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpsyt.2025.1613776/full#supplementary-material
References
1. Puckett L, Grayeb D, Khatri V, Cass K, and Mehler P. A comprehensive review of complications and new findings associated with anorexia nervosa. JCM. (2021) 10:2555. doi: 10.3390/jcm10122555
2. van Eeden AE, van Hoeken D, and Hoek HW. Incidence, prevalence and mortality of anorexia nervosa and bulimia nervosa. Curr Opin Psychiatry. (2021) 34:515–24. doi: 10.1097/YCO.0000000000000739
3. Edakubo S and Fushimi K. Mortality and risk assessment for anorexia nervosa in acute-care hospitals: a nationwide administrative database analysis. BMC Psychiatry. (2020) 20:19. doi: 10.1186/s12888-020-2433-8
4. Steinglass J, Figner B, Berkowitz S, Simpson HB, Weber EU, and Walsh BT. Increased capacity to delay reward in anorexia nervosa. J Int Neuropsychol Soc. (2012) 18:773–80. doi: 10.1017/S1355617712000446
5. Daruna JH and Barnes PA. A neurodevelopmental view of impulsivity. In: The impulsive client: Theory, research, and treatment. American Psychological Association, Washington, DC, US (1993). p. 23–37. doi: 10.1037/10500-002
6. Reynolds B, Ortengren A, Richards JB, and de Wit H. Dimensions of impulsive behavior: Personality and behavioral measures. Pers Individ Dif. (2006) 40:305–15. doi: 10.1016/j.paid.2005.03.024
7. Cyders MA, Littlefield AK, Coffey S, and Karyadi KA. Examination of a short English version of the UPPS-P Impulsive Behavior Scale. Addict Behav. (2014) 39:1372–6. doi: 10.1016/j.addbeh.2014.02.013
8. Whiteside SP and Lynam DR. The Five Factor Model and impulsivity: Using a structural model of personality to understand impulsivity. Pers Individ Dif. (2001) 30:669–89. doi: 10.1016/S0191-8869(00)00064-7
9. Patton JH, Stanford MS, and Barratt ES. Factor structure of the Barratt impulsiveness scale. J Clin Psychol. (1995) 51:768–74. doi: 10.1002/1097-4679(199511)51:6<768::aid-jclp2270510607>3.0.co;2-1
10. Ahn W-Y, Gu H, Shen Y, Haines N, Hahn HA, Teater JE, et al. Rapid, precise, and reliable measurement of delay discounting using a Bayesian learning algorithm. Sci Rep. (2020) 10:12091. doi: 10.1038/s41598-020-68587-x
11. Kirby KN, Petry NM, and Bickel WK. Heroin addicts have higher discount rates for delayed rewards than non-drug-using controls. J Exp Psychol Gen. (1999) 128:78–87. doi: 10.1037//0096-3445.128.1.78
12. Kirby KN. One-year temporal stability of delay-discount rates. Psychonomic Bull Rev. (2009) 16:457–62. doi: 10.3758/PBR.16.3.457
13. Butler GKL and Montgomery AMJ. Subjective self-control and behavioural impulsivity coexist in anorexia nervosa. Eat Behav. (2005) 6:221–7. doi: 10.1016/j.eatbeh.2004.11.002
14. Fessler DMT. Pseudoparadoxical impulsivity in restrictive anorexia nervosa: a consequence of the logic of scarcity. Int J Eat Disord. (2002) 31:376–88. doi: 10.1002/eat.10035
15. Howard M, Gregertsen EC, Hindocha C, and Serpell L. Impulsivity and compulsivity in anorexia and bulimia nervosa: A systematic review. Psychiatry Res. (2020) 293:113354. doi: 10.1016/j.psychres.2020.113354
16. Mallorquí-Bagué N, Testa G, Lozano-Madrid M, Vintró-Alcaraz C, Sánchez I, Riesco N, et al. Emotional and non-emotional facets of impulsivity in eating disorders: From anorexia nervosa to bulimic spectrum disorders. Euro Eating Disord Rev. (2020) 28:410–22. doi: 10.1002/erv.2734
17. Meneguzzo P, Todisco P, Collantoni E, Meregalli V, Dal Brun D, Tenconi E, et al. A multi-faceted evaluation of impulsivity traits and early maladaptive schemas in patients with anorexia nervosa. J Clin Med. (2021) 10:5895. doi: 10.3390/jcm10245895
18. Steward T, Mestre-Bach G, Vintró-Alcaraz C, Agüera Z, Jiménez-Murcia S, Granero R, et al. Delay discounting of reward and impulsivity in eating disorders: from anorexia nervosa to binge eating disorder. Eur Eat Disord Rev. (2017) 25:601–6. doi: 10.1002/erv.2543
19. Sanchez-Roige S, Fontanillas P, Elson SL, 23 and Me Research Team, Pandit A, Schmidt EM, et al. Genome-wide association study of delay discounting in 23,217 adult research participants of European ancestry. Nat Neurosci. (2018) 21:16–8. doi: 10.1038/s41593-017-0032-x
20. Sanchez-Roige S, Fontanillas P, Elson SL, Gray JC, de Wit H, MacKillop J, et al. Genome-Wide Association Studies of Impulsive Personality Traits (BIS-11 and UPPS-P) and Drug Experimentation in up to 22,861 Adult Research Participants Identify Loci in the CACNA1I and CADM2 genes. J Neurosci. (2019) 39:2562–72. doi: 10.1523/JNEUROSCI.2662-18.2019
21. Sanchez-Roige S, Jennings MV, Thorpe HHA, Mallari JE, van der Werf LC, Bianchi SB, et al. CADM2 is implicated in impulsive personality and numerous other traits by genome- and phenome-wide association studies in humans and mice. Transl Psychiatry. (2023) 13:1–11. doi: 10.1038/s41398-023-02453-y
22. Thorpe HH, Cupertino RB, Pakala SR, Fontanillas P, Jennings MV, Yang J, et al. Genome-wide association study of delay discounting in 134,935 individuals identifies novel loci and transdiagnostic associations across mental and physical health. medrxiv (2024). doi: 10.1101/2024.09.27.24314244
23. Kozak K, Lucatch AM, Lowe DJE, Balodis IM, MacKillop J, and George TP. The neurobiology of impulsivity and substance use disorders: implications for treatment. Ann N Y Acad Sci. (2019) 1451:71–91. doi: 10.1111/nyas.13977
24. Mitchell SH. Linking delay discounting and substance use disorders: genotypes and phenotypes. Perspect Behav Sci. (2019) 42:419–32. doi: 10.1007/s40614-019-00218-x
25. Vilar-Ribó L, Hatoum AS, Grotzinger AD, Mallard TT, 23andMe Research Team, Elson S, et al. Impulsivity facets and substance use involvement: insights from genomic structural equation modeling. psychol Med. (2025) 55:e51. doi: 10.1017/S0033291725000145
26. Bahji A, Mazhar MN, Hudson CC, Nadkarni P, MacNeil BA, and Hawken E. Prevalence of substance use disorder comorbidity among individuals with eating disorders: A systematic review and meta-analysis. Psychiatry Res. (2019) 273:58–66. doi: 10.1016/j.psychres.2019.01.007
27. Devoe DJ, Dimitropoulos G, Anderson A, Bahji A, Flanagan J, Soumbasis A, et al. The prevalence of substance use disorders and substance use in anorexia nervosa: a systematic review and meta-analysis. J Eat Disord. (2021) 9:161. doi: 10.1186/s40337-021-00516-3
28. Mellentin AI, Nielsen DG, Skøt L, Støving RK, Guala MM, Nielsen AS, et al. Risk of somatic diseases in patients with eating disorders: the role of comorbid substance use disorders. Epidemiol Psychiatr Sci. (2022) 31:e73. doi: 10.1017/S204579602200052X
29. Mellentin AI, Mejldal A, Guala MM, Støving RK, Eriksen LS, Stenager E, et al. The impact of alcohol and other substance use disorders on mortality in patients with eating disorders: A nationwide register-based retrospective cohort study. Am J Psychiatry. (2022) 179:46–57. doi: 10.1176/appi.ajp.2021.21030274
30. Munn-Chernoff MA, Johnson EC, Chou Y-L, Coleman JRI, Thornton LM, Walters RK, et al. Shared genetic risk between eating disorder- and substance-use-related phenotypes: Evidence from genome-wide association studies. Addict Biol. (2021) 26:e12880. doi: 10.1111/adb.12880
31. Wilson MR, Beachy SH, and Schumm SN eds. Rethinking Race and Ethnicity in Biomedical Research. Washington, D.C: National Academies Press (2025). doi: 10.17226/27913
32. Watson HJ, Yilmaz Z, Thornton LM, Hübel C, Coleman JRI, Gaspar HA, et al. Genome-wide association study identifies eight risk loci and implicates metabo-psychiatric origins for anorexia nervosa. Nat Genet. (2019) 51:1207–14. doi: 10.1038/s41588-019-0439-2
33. Levey DF, Galimberti M, Deak JD, Wendt FR, Bhattacharya A, Koller D, et al. Multi-ancestry genome-wide association study of cannabis use disorder yields insight into disease biology and public health implications. Nat Genet. (2023) 55:2094–103. doi: 10.1038/s41588-023-01563-z
34. Toikumo S, Jennings MV, Pham BK, Lee H, Mallard TT, Bianchi SB, et al. Multi-ancestry meta-analysis of tobacco use disorder identifies 461 potential risk genes and reveals associations with multiple health outcomes. Nat Hum Behav. (2024) 8:1177–93. doi: 10.1038/s41562-024-01851-6
35. Zhou H, Rentsch CT, Cheng Z, Kember RL, Nunez YZ, Sherva RM, et al. Association of OPRM1 functional coding variant with opioid use disorder: A genome-wide association study. JAMA Psychiatry. (2020) 77:1072–80. doi: 10.1001/jamapsychiatry.2020.1206
36. Zhou H, Kember RL, Deak JD, Xu H, Toikumo S, Yuan K, et al. Multi-ancestry study of the genetics of problematic alcohol use in over 1 million individuals. Nat Med. (2023) 29:3184–92. doi: 10.1038/s41591-023-02653-5
37. R: The R Project for Statistical Computing. (2022). Available online at: https://www.r-project.org/ (Accessed April 10, 2025).
38. Grotzinger AD, Rhemtulla M, de Vlaming R, Ritchie SJ, Mallard TT, Hill WD, et al. Genomic structural equation modelling provides insights into the multivariate genetic architecture of complex traits. Nat Hum Behav. (2019) 3:513–25. doi: 10.1038/s41562-019-0566-x
39. Bulik-Sullivan BK, Loh P-R, Finucane HK, Ripke S, Yang J, Schizophrenia Working Group of the Psychiatric Genomics Consortium, et al. LD Score regression distinguishes confounding from polygenicity in genome-wide association studies. Nat Genet. (2015) 47:291–5. doi: 10.1038/ng.3211
40. Gustavson DE, Morrison CL, Mallard TT, Jennings MV, Fontanillas P, Elson SL, et al. Executive function and impulsivity predict distinct genetic variance in internalizing problems, externalizing problems, thought disorders, and compulsive disorders: A genomic structural equation modeling study. Clin Psychol Sci. (2024) 12:865–81. doi: 10.1177/21677026231207845
41. Hatoum AS, Johnson EC, Colbert SMC, Polimanti R, Zhou H, Walters RK, et al. The addiction risk factor: A unitary genetic vulnerability characterizes substance use disorders and their associations with common correlates. Neuropsychopharmacology. (2022) 47:1739–45. doi: 10.1038/s41386-021-01209-w
42. Gustavson DE, Friedman NP, Fontanillas P, Elson SL, Palmer AA, and Sanchez-Roige S. The latent genetic structure of impulsivity and its relation to internalizing psychopathology. Psychol Sci. (2020) 31:1025–35. doi: 10.1177/0956797620938160
43. Rosseel Y. lavaan: an R package for structural equation modeling. J Stat Softw. (2012) 48:1–36. doi: 10.18637/jss.v048.i02
44. Hatoum AS, Colbert SMC, Johnson EC, Huggett SB, Deak JD, Pathak G, et al. Multivariate genome-wide association meta-analysis of over 1 million subjects identifies loci underlying multiple substance use disorders. Nat Ment Health. (2023) 1:210–23. doi: 10.1038/s44220-023-00034-y
45. Kulacaoglu F and Kose S. Singing under the impulsiveness: Impulsivity in psychiatric disorders. Psychiatry Clin Psychopharmacol. (2018) 28:205–10. doi: 10.1080/24750573.2017.1410329
46. Miller DJ, Derefinko KJ, Lynam DR, Milich R, and Fillmore MT. Impulsivity and attention deficit-hyperactivity disorder: subtype classification using the UPPS impulsive behavior scale. J Psychopathol Behav Assess. (2010) 32:323–32. doi: 10.1007/s10862-009-9155-z
47. Amlung M, Marsden E, Holshausen K, Morris V, Patel H, Vedelago L, et al. Delay discounting as a transdiagnostic process in psychiatric disorders: A meta-analysis. JAMA Psychiatry. (2019) 76:1176–86. doi: 10.1001/jamapsychiatry.2019.2102
48. Hahn AM, Simons RM, and Tirabassi CK. Five factors of impulsivity: unique pathways to borderline and antisocial personality features and subsequent alcohol problems. Pers Individ Dif. (2016) 99:313–9. doi: 10.1016/j.paid.2016.05.035
49. Bardone-Cone AM, Butler RM, Balk MR, and Koller KA. Dimensions of impulsivity in relation to eating disorder recovery. Int J Eat Disord. (2016) 49:1027–31. doi: 10.1002/eat.22579
50. Claes L, Islam MA, Fagundo AB, Jimenez-Murcia S, Granero R, Agüera Z, et al. The relationship between non-suicidal self-injury and the UPPS-P impulsivity facets in eating disorders and healthy controls. PloS One. (2015) 10:e0126083. doi: 10.1371/journal.pone.0126083
51. Lavender JM and Mitchell JE. Eating disorders and their relationship to impulsivity. Curr Treat Options Psych. (2015) 2:394–401. doi: 10.1007/s40501-015-0061-6
52. Phillipou A, Abel LA, Castle DJ, Gurvich C, Hughes ME, and Rossell SL. Self-reported and behavioural impulsivity in anorexia nervosa. World J Psychiatry. (2016) 6:345–50. doi: 10.5498/wjp.v6.i3.345
53. Wade TD, Tiggemann M, Bulik CM, Fairburn CG, Wray NR, and Martin NG. Shared temperament risk factors for anorexia nervosa: a twin study. Psychosom Med. (2008) 70:239–44. doi: 10.1097/PSY.0b013e31815c40f1
54. Decker JH, Figner B, and Steinglass JE. On weight and waiting: delay discounting in anorexia nervosa pretreatment and posttreatment. Biol Psychiatry. (2015) 78:606–14. doi: 10.1016/j.biopsych.2014.12.016
55. Foldi CJ, Morris MJ, and Oldfield BJ. Executive function in obesity and anorexia nervosa: Opposite ends of a spectrum of disordered feeding behaviour? Prog Neuropsychopharmacol Biol Psychiatry. (2021) 111:110395. doi: 10.1016/j.pnpbp.2021.110395
56. Waxman SE. A systematic review of impulsivity in eating disorders. Eur Eat Disord Rev. (2009) 17:408–25. doi: 10.1002/erv.952
57. Himmerich H, Bentley J, Kan C, and Treasure J. Genetic risk factors for eating disorders: an update and insights into pathophysiology. Ther Adv Psychopharmacol. (2019) 9:2045125318814734. doi: 10.1177/2045125318814734
58. Hoffman ER, Gagne DA, Thornton LM, Klump KL, Brandt H, Crawford S, et al. Understanding the association of impulsivity, obsessions, and compulsions with binge eating and purging behaviours in anorexia nervosa. Eur Eating Disord Rev. (2012) 20:e129–36. doi: 10.1002/erv.2161
59. Lindvall Dahlgren C and Rø O. A systematic review of cognitive remediation therapy for anorexia nervosa - development, current state and implications for future research and clinical practice. J Eat Disord. (2014) 2:26. doi: 10.1186/s40337-014-0026-y
60. Lynch TR, Gray KL, Hempel RJ, Titley M, Chen EY, and O’Mahen HA. Radically open-dialectical behavior therapy for adult anorexia nervosa: feasibility and outcomes from an inpatient program. BMC Psychiatry. (2013) 13:293. doi: 10.1186/1471-244X-13-293
61. Lavender JM, Goodman EL, Culbert KM, Wonderlich SA, Crosby RD, Engel SG, et al. Facets of impulsivity and compulsivity in women with anorexia nervosa. Eur Eat Disord Rev. (2017) 25:309–13. doi: 10.1002/erv.2516
62. Substance Use and Eating Disorders - NEDA. National Eating Disorders Association . Available online at: https://www.nationaleatingdisorders.org/substance-use-and-eating-disorders/ (Accessed May 27, 2025).
63. Root T, Pinheiro AP, Thornton L, Strober M, Fernandez-Aranda F, Brandt H, et al. Substance use disorders in women with anorexia nervosa. Int J Eat Disord. (2010) 43:14–21. doi: 10.1002/eat.20670
Keywords: genomic structural equation modeling, GWAS, eating disorders, anorexia, delay discounting, BIS, UPPS, impulsivity
Citation: Bianchi SB, Vilar-Ribó L, Palmer AA, Gustavson DE and Sanchez-Roige S (2025) Genomic structural equation study reveals links between anorexia nervosa and delay discounting and lack of perseverance but not other facets of impulsivity. Front. Psychiatry 16:1613776. doi: 10.3389/fpsyt.2025.1613776
Received: 17 April 2025; Accepted: 11 June 2025;
Published: 04 July 2025.
Edited by:
Matthew J. Hoptman, Nathan S. Kline Institute for Psychiatric Research, United StatesReviewed by:
Jun Li, Ruijin Hospital, Shanghai Jiao Tong University, ChinaPhilip Szeszko, Icahn School of Medicine at Mount Sinai, United States
Copyright © 2025 Bianchi, Vilar-Ribó, Palmer, Gustavson and Sanchez-Roige. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Sandra Sanchez-Roige, c2FuY2hlenJvaWdlQHVjc2QuZWR1