 Noemi Monika Szeifert
Noemi Monika Szeifert Barnabás Oláh
Barnabás Oláh Barbara Sebok5†
Barbara Sebok5†- 1Doctoral School of Psychology, ELTE Eötvös Lóránd University, Budapest, Hungary
- 2Department of Sports Medicine, Semmelweis University, Budapest, Hungary
- 3Department of Behavioural Sciences, Faculty of Medicine, University of Debrecen, Debrecen, Hungary
- 4Clinical Psychology Center of CC, Health Care Service Units, University of Debrecen Clinical Centre, Debrecen, Hungary
- 5Semmelweis University School of PhD Studies Workgroup for Science Management, Dr. Manninger Jenő Trauma Center, Budapest, Hungary
- 6Department of Clinical Psychology, Semmelweis University, Budapest, Hungary
- 7Department of Psychiatry and Psychotherapy, Semmelweis University, Budapest, Hungary
- 8NAP3.0-SE Neuropsychopharmacology Research Group, Hungarian Brain Research Program, Semmelweis University, Budapest, Hungary
Introduction: This Hungarian cross-sectional study examined patterns and differences in suicide risk factors across various suicidality groups, including individuals with single or multiple suicide attempts, as well as gender-specific variations. Additionally, it explored these risk factors within a biopsychosocial framework to offer a comprehensive understanding of their interconnected effects.
Materials and methods: A total of 300 psychiatric inpatients were recruited from Péterfy Sandor Hospital in Budapest, Hungary, including 146 individuals (48.67%) with a history of suicide attempts and 154 (51.33%) without such a history. Participants ranged in age from 18 to 85 years, with a mean age of 37.98 years (SD = 12.80 for suicide attempters, 13.72 for non-attempters). The overall sample comprised 83 males (27.7%) and 217 females (72.3%). Logistic regression analysis was conducted to assess the influence of demographic characteristics, life history variables, and psychiatric diagnoses on suicide risk, aiming to identify significant predictors of suicide attempts within a biopsychosocial framework.
Results: Depression was the most prevalent psychiatric diagnosis in the sample. Significant predictors of suicide attempts included family history of suicide (OR = 2.283, p = 0.015), prescription drug misuse (OR = 1.900, p = 0.047), and nicotine dependence (OR = 1.869, p = 0.035). In repeated suicide attempts, bipolar disorder (OR = 5.761, p = 0.006), borderline personality disorder (OR = 5.132, p = 0.003), depression (OR = 4.064, p = 0.004), and job loss (OR = 4.348, p = 0.031) emerged as the strongest predictors. Among men, job loss (OR = 4.074, p = 0.014) was a prominent risk factor, while among women, having two or more children (OR = 2.740, p = 0.036) and a family history of suicide (OR = 2.459, p = 0.028) significantly increased suicide risk. Relationship conflict was also associated with higher risk in women (OR = 0.382, p = 0.035).
Conclusions: Our research supports the notion that suicide risk factors interact with one another, and in certain cases, their effects may be synergistic—mutually reinforcing—rather than antagonistic. Similarly, protective factors also appear to amplify each other’s impact, suggesting a cumulative and interactive model of both risk and resilience.
Introduction
Suicide represents a significant global public health issue, ranking among the leading causes of death worldwide. According to data from the World Health Organization (WHO), over 700,000 individuals die by suicide each year, equivalent to one death every 40 seconds. Suicide is a phenomenon that affects people across all age groups and occurs throughout the lifespan (1, 2).
In Hungary, suicide has historically been a significant public health concern, with the country having had one of the highest suicide rates in the world at one point in time (3, 4). However, over the past few decades, there has been a notable decline in suicide rates. This reduction is attributed to several factors, including improved mental health services, greater access to psychiatric care, and increased public awareness surrounding mental health issues. The introduction of antidepressants, particularly SSRIs, in the 1990s, also played a role in reducing suicides. Additionally, economic improvements and social support systems have also contributed to this downward trend 5–7).
Despite these improvements, in 2023, a total of 1,593 (8) individuals died by suicide in Hungary, a rate that remains above the European average. Hungarian studies have consistently identified depression, bipolar disorder, anxiety disorders, and substance use—especially smoking and alcohol—as key risk factors for both suicide attempts and completed suicides (3, 9–15). A disadvantaged background—characterized by low socio-economic status, a history of parental suicide attempts, and exposure to psychological adversities—has also been consistently associated with an elevated risk of suicide, particularly in the presence of an untreated psychiatric disorder (16–18). These patterns are notably prevalent among middle-aged and older men, and higher suicide rates are concentrated in rural areas and the southeastern region (Rihmer et al., 2013). Continuous efforts are needed to sustain progress by improving early detection, reducing stigma, and expanding access to care (19).
Findings suggest that the COVID-19 pandemic’s socio-economic and psychological impacts may have exacerbated factors contributing to suicide in Hungary. The data underscores the importance of targeted mental health interventions and support systems, especially for the most affected demographics and regions (20, 21).
Suicide and methods
A suicide attempt is defined as a self-initiated, potentially harmful behavior undertaken with the intent to end one’s life, which does not result in death. It is influenced by a complex interplay of psychological, environmental, and biological factors (22). In suicide research, methods are often categorized as violent or non-violent based on the nature and lethality of the act (23). This classification aids in understanding the characteristics and risk factors associated with different suicide methods. Violent methods typically involve direct physical force and are associated with a high risk of immediate lethality, such as firearms/gunshots, hanging or strangulation, and blunt force injuries (e.g., jumping from a high place or stepping in front of a train). Non-violent suicide attempts typically refer to methods that do not involve physical trauma, such as overdosing on medication, poisoning, or asphyxiation (17). The risk factors for non-violent suicide attempts can overlap with general suicide risk factors, but may also have unique aspects related to method choice.
The most common and robust predictors of suicide attempts, in hierarchical order, are (24): Psychiatric and psychological disorders play a significant role in influencing suicide methods, particularly depression, bipolar disorder, and anxiety disorders (9, 11, 25). These are among the most common underlying mental health conditions associated with non-violent and violent suicide attempts, along with other serious mental illnesses (25). Personality disorders, particularly borderline personality disorder, are also strongly linked to suicidal behavior due to their association with impulsivity and self-harm (26, 27). A history of previous suicide attempts, especially non-violent ones, increases the risk of future attempts (17, 28). Substance abuse, including alcohol and drug misuse, further elevates suicide risk by impairing judgment and increasing impulsivity (11, 29, 30). Additionally, hopelessness and feelings of worthlessness are powerful psychological predictors of suicidal behavior (31). Medical and physical health factors are important contributors to suicide risk, particularly concerning method choice. Chronic illnesses such as cancer, chronic pain syndromes, and other debilitating diseases are strongly associated with increased suicidal ideation and behavior, often due to feelings of hopelessness, loss of autonomy, and perceived burden on others (32, 33). Individuals living with chronic medical conditions frequently have greater access to prescription medications, which may facilitate non-violent suicide attempts such as overdose (34, 35). The availability and familiarity with medications used for pain or symptom management can inadvertently increase the risk, especially in the context of psychological distress or comorbid mental health conditions (36, 37). Demographic factors influencing suicide methods include gender, age, and socioeconomic status. Women are more likely to attempt suicide using non-violent methods such as poisoning or overdose, while men tend to use more violent means (4, 38). Adolescents, young adults, and older adults may also favor non-violent methods (39). Additionally, individuals with higher education and socioeconomic status have sometimes been linked to non-violent methods, possibly due to better access to prescription medications (40). Social and environmental factors significantly influence suicide risk, particularly in shaping an individual’s vulnerability during times of crisis. Isolation and lack of social support have been consistently associated with increased suicidal ideation, as loneliness and the absence of close interpersonal relationships can exacerbate feelings of despair and hopelessness (41, 42). Recent life stressors, including relationship breakups, job loss, financial hardship, or involvement with the legal system, are also known to trigger suicidal behavior, especially in individuals with limited coping resources (3, 41, 43). A history of abuse or trauma, such as childhood maltreatment, sexual abuse, or exposure to violence, further compounds the risk by disrupting emotional regulation and trust in others (44–46). Cultural factors, including mental health stigma, can discourage individuals from seeking professional help or disclosing distress, a phenomenon particularly prevalent among minority populations such as the Hungarian Roma, where cultural marginalization and institutional distrust may amplify vulnerability (47, 48). Cognitive and behavioral factors play a crucial role in suicide risk, including the likelihood and method of attempts. Impulsivity is a well-established risk factor, even in cases where non-violent suicide attempts are planned, as impulsive individuals may act quickly in response to distress without fully considering the consequences (17, 49). Low problem-solving skills, particularly in managing interpersonal stressors or navigating complex emotional situations, have also been linked to an increased risk of suicidal behavior, as individuals may perceive suicide as the only escape from unsolvable problems (50). Additionally, the use of poor or maladaptive coping mechanisms—such as avoidance, denial, or substance use—can further exacerbate emotional pain and reduce resilience, increasing the likelihood of suicide attempts (51). Family and genetic factors are critical in understanding suicide risk, as both inherited traits and environmental influences can contribute. A family history of suicide or mental illness is associated with a higher likelihood of suicidal behavior, suggesting both genetic predispositions and the influence of modeled or learned behaviors within the family context (52). Additionally, family conflict and dysfunction—such as high levels of criticism, lack of emotional support, or exposure to domestic violence—can increase psychological distress and impair emotional regulation, further elevating suicide risk, particularly among adolescents and young adults (53). These factors often interact, compounding vulnerability in individuals already at risk due to mental health or cognitive challenges. The availability of means is a critical determinant of suicide risk, as access to lethal methods significantly increases the likelihood of both suicide attempts and fatalities. Easy access to medications or toxic substances, such as prescription drugs or household chemicals, raises the risk of impulsive or planned non-violent suicide attempts, particularly in individuals experiencing acute psychological distress (54). When such means are not securely stored or adequately restricted, such as unsecured medications in the home, the probability of use in a suicide attempt increases substantially (55). Restricting access to lethal means is one of the most effective strategies in suicide prevention, underscoring the importance of environmental safety measures. While numerous risk factors increase vulnerability to suicide, protective factors can buffer against these risks by enhancing resilience and reducing the likelihood of suicidal behavior. Strong social support networks serve as a critical protective element, offering emotional connection and reducing feelings of isolation (56). Access to mental health care, including early intervention and ongoing treatment, has been shown to significantly decrease suicide risk, especially when combined with effective therapeutic approaches (57, 58). Individuals with effective coping and problem-solving skills are better equipped to manage stress and emotional crises, reducing reliance on maladaptive behaviors (59). Cultural or religious beliefs that discourage suicide may provide a moral or existential framework that deters self-harm (60). Additionally, engagement in meaningful activities—such as work, regular physical activity, hobbies, or volunteering—can foster a sense of purpose and belonging, which is associated with lower suicide risk (61). These protective factors serve as crucial counterbalances to the cognitive, psychological, and social vulnerabilities associated with suicide.
Our research aims to analyze the main non-violent suicide risk factors in an inpatient psychiatric sample within a biopsychosocial framework, with a focus on identifying the most significant factors and their interactions.
Methods
Sample
Participants in the patient group were recruited from the Crisis Intervention and Psychiatric Ward at Péterfy Sándor Hospital in Budapest, Hungary, between January 1, 2016, and December 31, 2021. The sample was derived from a comprehensive research project utilizing paper-and-pencil questionnaires, which inherently limited the sample size. Although approximately 4,000 to 5,000 patients were admitted to the referenced department at Péterfy Hospital during the study period, the use of detailed self-report instruments restricted the number of participants who could be feasibly included. Psychiatric diagnoses, along with assessments of suicide risk and underlying motives, were conducted using the Structured Clinical Interview for DSM-IV (SCID-IV), administered by psychiatrists and trained clinical psychologists. Diagnoses were further supported by classifications based on the International Classification of Diseases, 10th Revision (ICD-10). Diagnoses were recorded at the time of admission to the psychiatric ward. Individuals were excluded from the comprehensive study if they were experiencing an acute psychotic episode, current alcohol or substance abuse, schizophrenia, a history of traumatic brain injury or neurological disorders, severe medical conditions, or had engaged in parasuicidal behavior. Participation in the study was entirely voluntary, and all participants provided written informed consent for the extraction of relevant data from the hospital’s electronic medical record system. The study received ethical approval from the Institutional Review Board of Péterfy Sándor a Hospital and Outpatient Center (Approval No. 25/2016). The authors affirm that all procedures contributing to this research comply with the ethical standards of the relevant national and institutional committees on human experimentation, as well as with the Helsinki Declaration of 1975, as revised in 2013.
Measures
Data were collected through structured clinical interviews conducted by psychiatrists and trained clinicians, supplemented by information retrieved from the hospital’s central electronic medical record system. The analysis included a range of variables: gender, age, place of residence, educational level, marital status, number of children, employment status, financial status, psychiatric diagnosis, and various forms of substance dependence, including alcohol, medication, other substances, and nicotine. Additional data were collected on suicide motives and family history of suicide. Participants also completed a self-report questionnaire addressing whether they were born from an unintended pregnancy, whether their mother had attempted an induced abortion or suicide during pregnancy (coding was as follows: 1 = Yes, 2 = No, 3 = No information available), and whether they had undergone an induced abortion. Participants who had experienced the loss of a child were also asked to complete relevant sections of the questionnaire.
Statistical analysis
Statistical analyses were conducted using IBM SPSS Statistics, version 23. Initially, the demographic characteristics of the sample were described using means and standard deviations for continuous variables, and proportions for categorical variables, stratified by history of suicide attempts. To assess bivariate associations between suicide risk factors and history of suicide attempts, Pearson’s chi-square tests were employed. Comorbidity of psychiatric diagnoses among individuals with a history of suicide attempts was examined using Phi coefficients (φ).
Subsequently, logistic regression models were constructed to investigate the associations between various risk factors and suicidal behavior, while adjusting for demographic variables, including gender, age, place of residence, educational attainment, relationship status, number of children, employment status, and subjective financial situation. To enhance the interpretability and stability of the models, certain variables were recategorized as follows: place of residence (city, town, or village); education (primary, secondary, or tertiary); relationship status (single vs. in a relationship); and financial status (below average, average, or above average). Finally, post hoc analyses were performed using the adjusted Wald test.
Results
Descriptive statistics
Among the 300 participants, 146 individuals (48.67%) reported a history of suicide attempts, while 154 (51.33%) had no such history. Participant ages ranged from 18 to 85 years, with a mean age of 37.98 years (SD = 12.80 for those with a history of suicide attempts, and SD = 13.72 for those without). Of the total sample, 83 individuals (27.7%) were male and 217 (72.3%) were female (Table 1). Among those with a history of suicide attempts, 40 (27.5%) were male and 106 (72.6%) were female, reflecting the well-documented pattern that non-violent suicide attempts and psychiatric service utilization are more prevalent among women. This finding is consistent with existing literature indicating that females are generally more likely than males to seek psychological help.
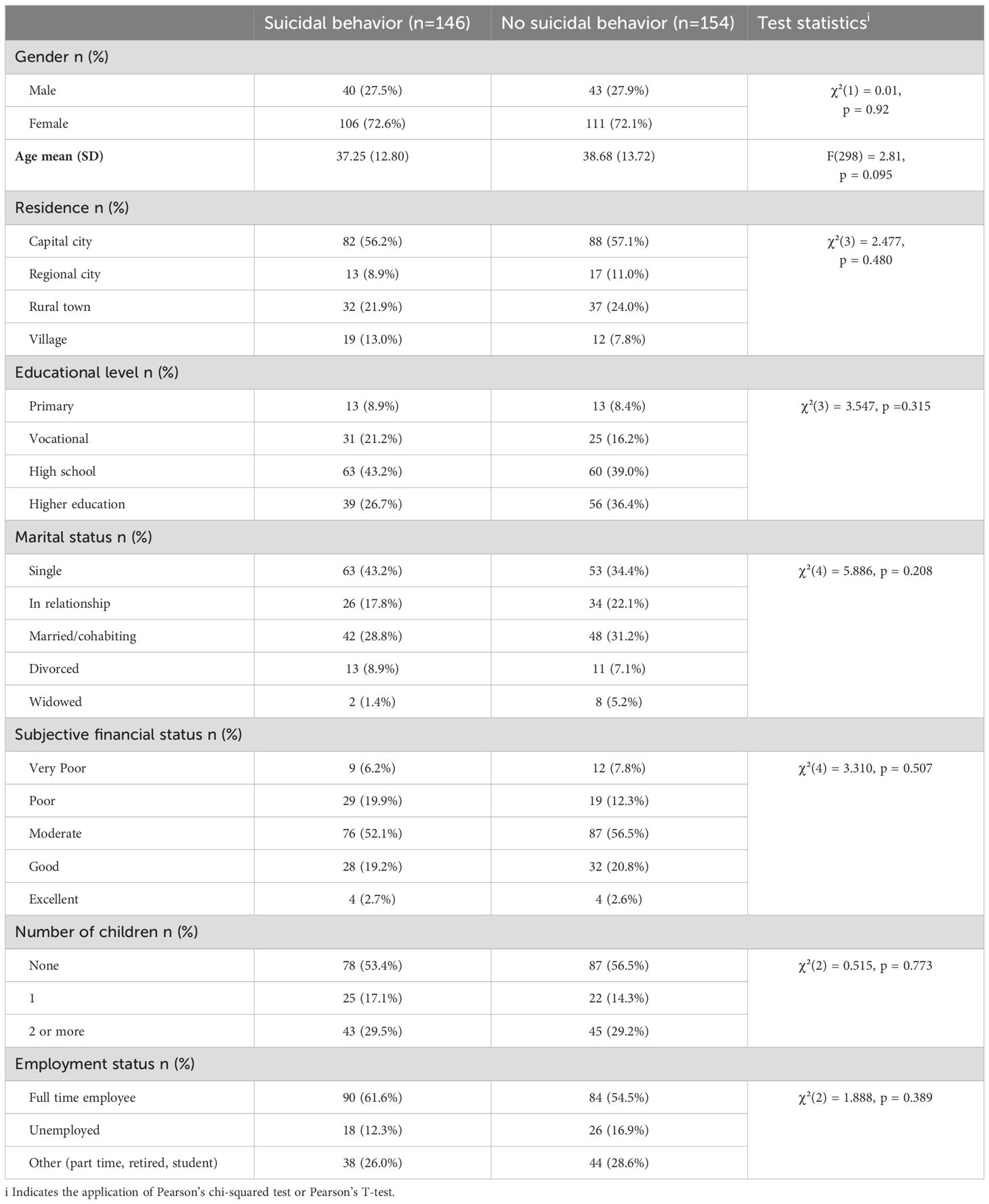
Table 1. Demographic characteristics of the samples.
Concerning the frequency of suicide attempts among attempters, 56.8% reported a single attempt, 21.2% reported two attempts, and 22.0% reported three or more. The age at first suicide attempt varied considerably: 11.0% of participants had their first attempt before the age of 18, 33.6% between the ages of 18 and 29, 28.1% between 30 and 44, 16.4% between 45 and 59, and 4.1% at age 60 or older. Post-discharge follow-up data indicated that 24.7% of individuals with a prior suicide attempt made a subsequent attempt within one month, 11.0% within three months, 5.5% within six months, and 12.3% within one year of discharge.
Risk factors
Concerning familial suicide risk factors, a family history of suicide was significantly more common among individuals with a history of suicide attempts (43.8%) than among those without such a history (22.7%) (χ²(1) = 15.103, p <.001). Conversely, being born as a result of an unintended pregnancy was more frequently reported among suicide attempters (40.0%) compared to non-attempters (29.0%), although this difference did not reach statistical significance. Similarly, 10.5% of individuals with a history of suicide attempts and 7.2% of non-attempters reported that their mother had either attempted abortion or engaged in suicidal behavior during the pregnancy. The experience of losing a child was reported by 8.3% of attempters and 6.6% of non-attempters, while a personal history of abortion was noted in 24.2% and 21.3% of individuals in the respective groups (Table 2).
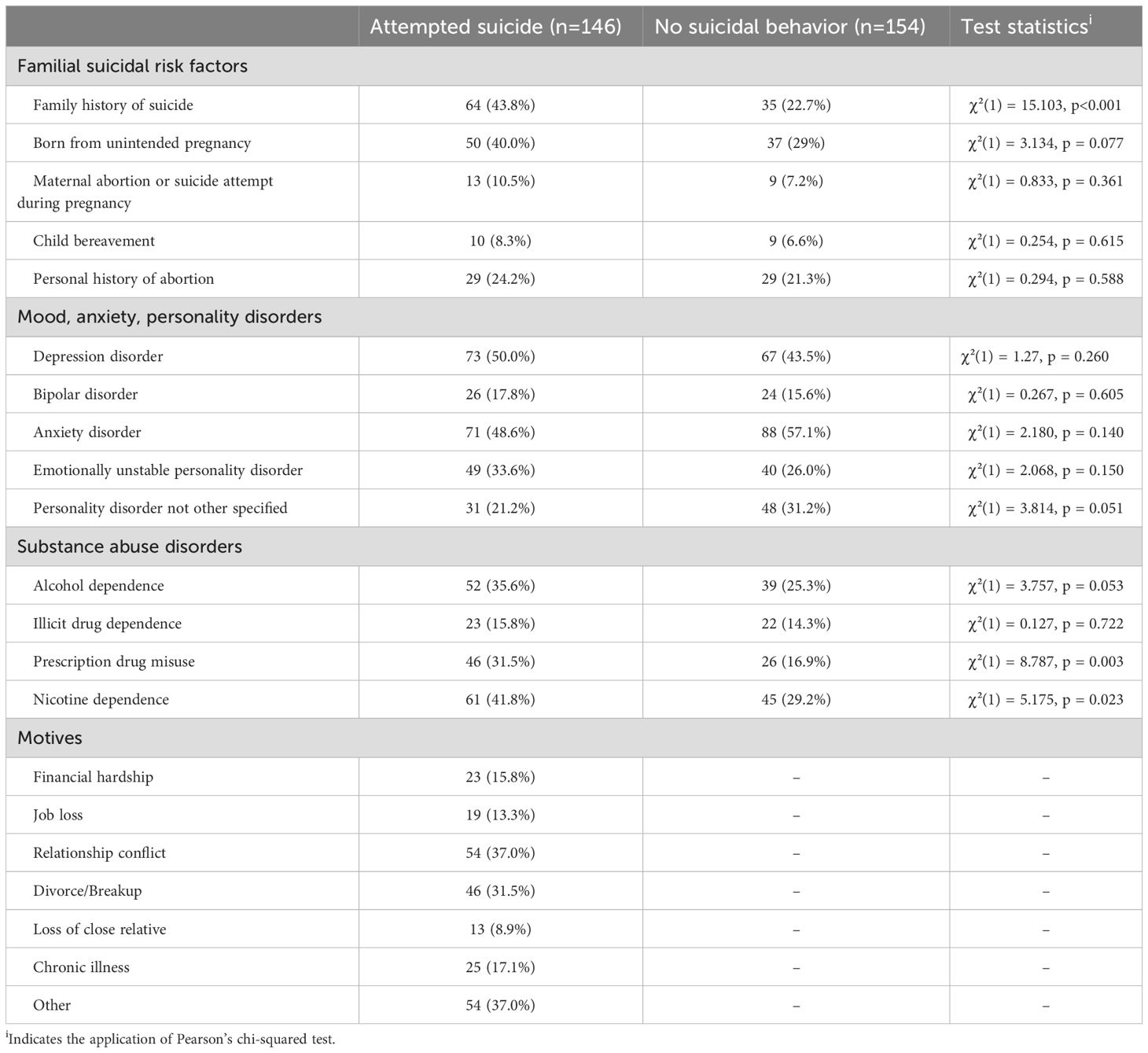
Table 2. Descriptive statistics of familial suicidal risk factors and psychiatric disorders in the samples and the motives of the latest suicide attempt.
The distribution of psychiatric diagnoses within the total sample of 300 psychiatric patients was as follows: major depressive disorders were diagnosed in 140 individuals (46.7%), bipolar disorder in 50 (16.7%), and anxiety disorders in 159 participants (53.0%). Emotionally unstable personality disorder (emotionally unstable type) was identified in 89 individuals (29.7%), while 79 participants (26.3%) met criteria for unspecified personality disorder. Substance use disorders were also prevalent: 91 individuals (30.3%) were diagnosed with alcohol use disorder, 45 (15.0%) with illicit drug use disorder, and 72 (24.0%) with prescription drug misuse. Nicotine dependence was reported by 106 individuals (35.3%). A detailed overview of psychiatric diagnoses is provided in Table 2.
Among those with a history of suicide attempts, the most frequently diagnosed psychiatric disorders included major depressive disorders (73 individuals, 50.0%), anxiety disorders (71 individuals, 48.6%), emotionally unstable personality disorder (49 individuals, 33.6%), bipolar disorder (26 individuals, 17.8%), and unspecified personality disorder (31 individuals, 21.2%). In terms of substance use, the most commonly reported conditions among suicide attempters were nicotine dependence (61 individuals, 41.8%), followed by alcohol use disorder (52 individuals, 35.6%), prescription drug misuse (46 individuals, 31.5%), and illicit drug use disorder (23 individuals, 15.8%).
Regarding the reported motivations for the most recent suicide attempt (data available only for the attempter group), the most frequently cited reasons included relationship conflict (37.0%), divorce or breakup (31.5%), and financial hardship (15.8%). Additional motives were chronic illness (17.1%), job loss (13.3%), the loss of a close relative (8.9%), and other unspecified reasons (37.0%) (Table 2).
Intercorrelations of psychiatric diagnoses among suicide attempters
Table 3 presents the correlation matrix of psychiatric diagnoses among individuals with a history of suicide attempts, utilizing Phi coefficients (φ) to quantify the strength of associations between diagnostic categories. Consistent with clinical conventions, no co-occurrence of unipolar depression and bipolar disorder was observed in the sample, reflecting their generally mutually exclusive diagnostic status. Noteworthy findings include a significant negative association between depression and emotionally unstable personality disorder (φ = -0.189, p < 0.05), which may reflect diagnostic practices wherein clinicians preferentially assign one diagnosis over the other. Similarly, emotionally unstable personality disorder and unspecified personality disorder exhibited a significant negative correlation (φ = -0.298, p < 0.001), likely due to the clinical tendency to avoid assigning a nonspecific personality disorder diagnosis when a more specific diagnosis is established. Positive associations were identified between emotionally unstable personality disorder and illicit drug dependence (φ = 0.250, p < 0.05), as well as between alcohol dependence and both prescription drug misuse (φ = 0.388, p < 0.001) and nicotine dependence (φ = 0.298, p < 0.001). The strongest correlation within the matrix was observed between illicit drug dependence and nicotine dependence (φ = 0.396, p < 0.001), indicating a particularly robust comorbidity. These findings underscore the complex interplay between psychiatric disorders and substance use within this high-risk cohort.
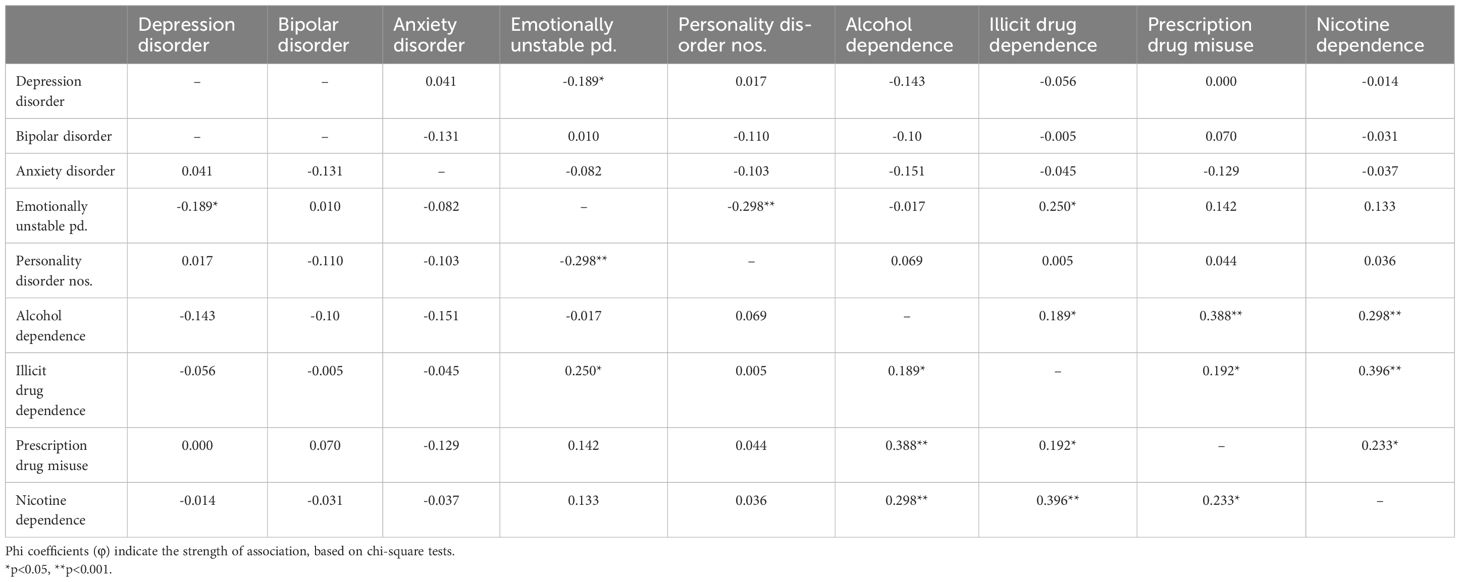
Table 3. The correlation matrix of psychiatric diagnoses among suicide attempters.
Demographic, familial and psychiatric predictors of suicidal behavior
Multivariate logistic regression models (Table 4) were employed to examine the associations between demographic characteristics, familial risk factors, mood, anxiety, and personality disorder diagnoses, as well as substance use, concerning suicidal behavior. Separate models were computed for each group of variables. Models 2, 3, and 4 were adjusted for demographic covariates.
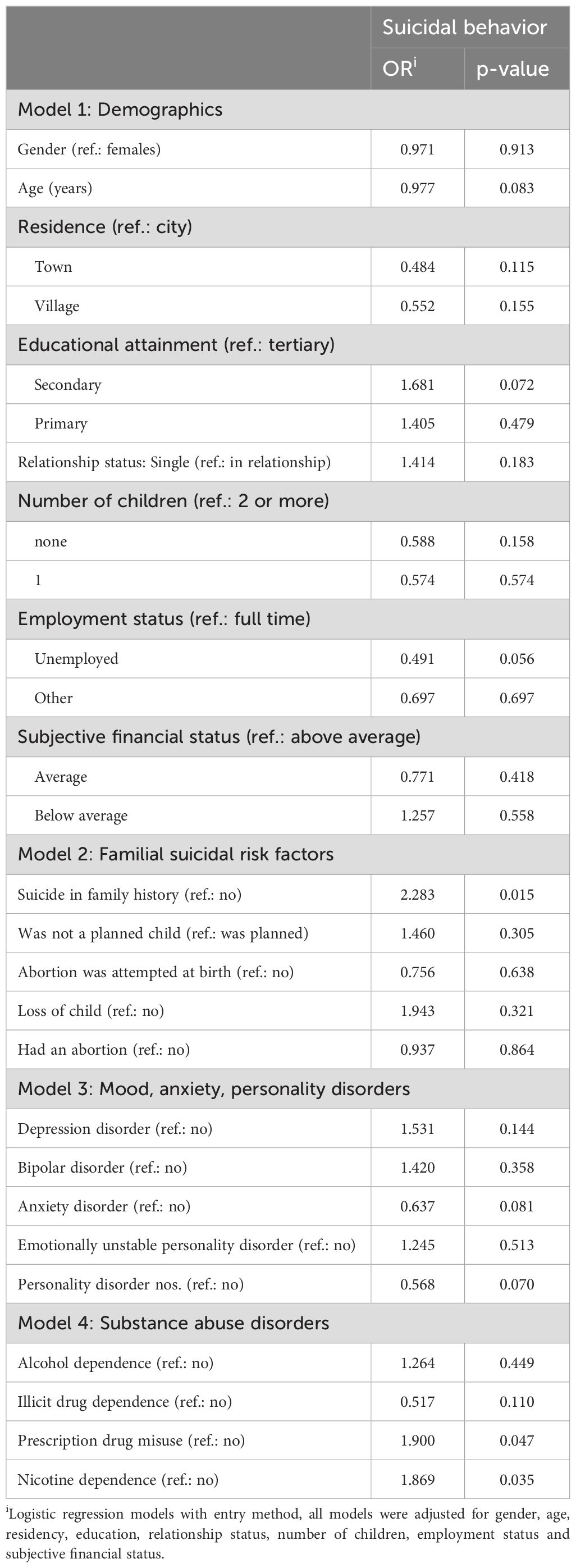
Table 4. Modelling the associations of demographic variables, familial suicidal risk factors and psychiatric diagnoses with suicidal behavior.
Among the demographic variables, no main effects reached statistical significance. However, a family history of suicide emerged as a significant predictor of suicidal behavior (OR = 2.283, p = 0.015), indicating more than a twofold increase in risk. Other familial factors were not significantly associated with suicidal behavior.
None of the mood, anxiety, or personality disorder diagnoses—including depression, bipolar disorder, anxiety disorders, emotionally unstable personality disorder, and unspecified personality disorders—significantly differentiated between individuals with and without suicidal behavior within the clinical sample. Nonetheless, non-significant trends suggesting increased risk were observed for depression, anxiety disorders, and emotionally unstable personality disorder.
In contrast, substance use variables were more predictive of suicidal behavior in this clinical population. Nicotine dependence was significantly associated with suicidal behavior (OR = 1.869, p = 0.035), corresponding to an approximately 87% increased risk. Prescription drug misuse also showed a significant association (OR = 1.900, p = 0.047), suggesting nearly double the risk. Other substance-related variables did not reach statistical significance in the sample.
Gender differences
Gender-specific differences were observed in the predictors of suicidal behavior (Table 5). Among females, increasing age was significantly associated with a reduced likelihood of suicidal behavior (OR = 0.955, p = 0.007), corresponding to a 4.5% decrease in risk for each additional year of age. Furthermore, women with two or more children exhibited significantly higher odds of suicidal behavior compared to those without children (OR = 2.740, p = 0.036). A family history of suicide was also a significant predictor among women, associated with a 2.46-fold increase in risk (OR = 2.459, p = 0.028). In contrast, none of these variables demonstrated statistically significant associations with suicidal behavior among males.
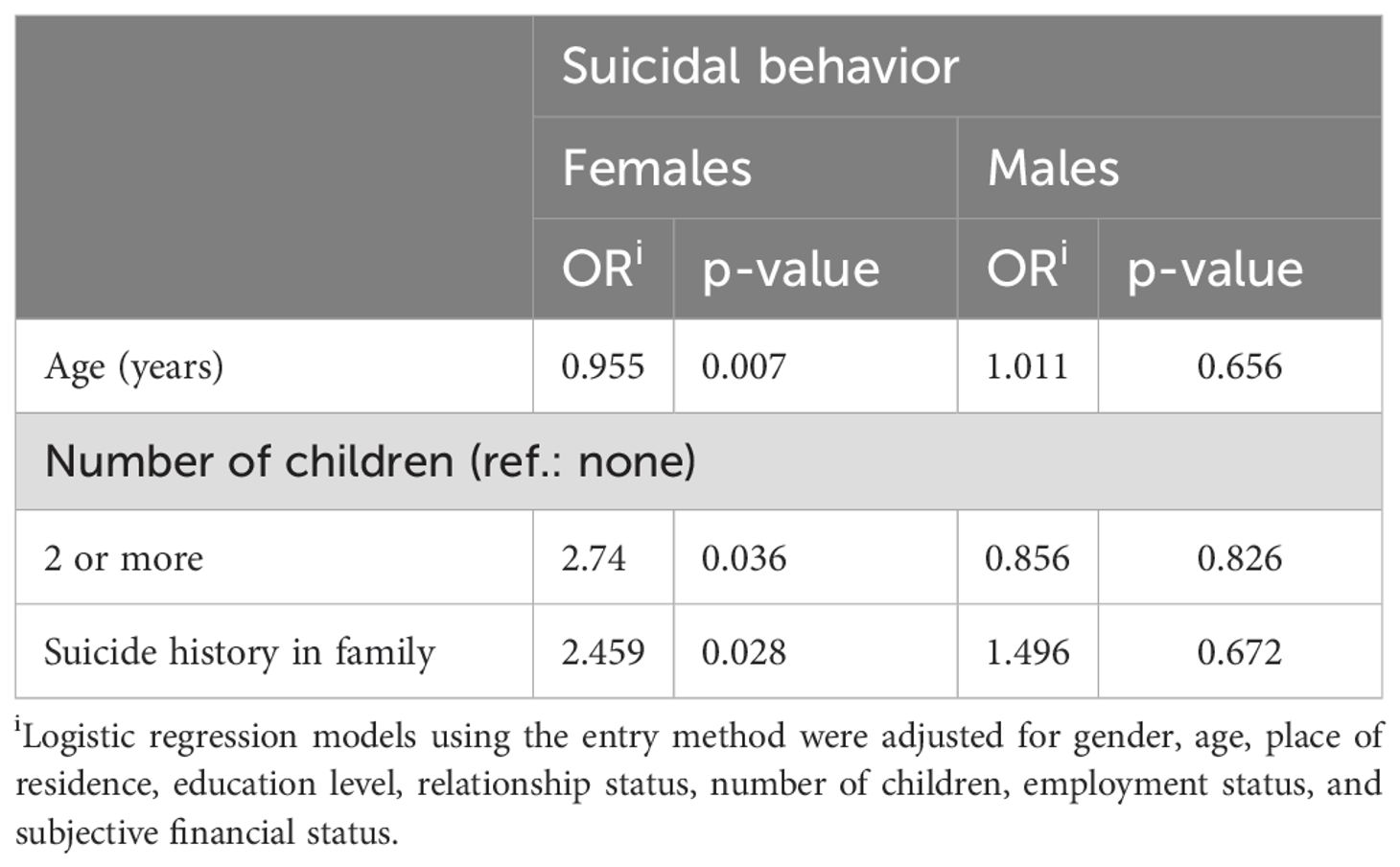
Table 5. The differences of suicide predictors between gender groups.
Gender differences also emerged in the reported motives for suicidal behavior (Table 6). Men were significantly more likely to cite job loss as a contributing factor, with a 4.07-fold increased likelihood compared to women (OR = 4.074, p = 0.014). Conversely, relationship conflict was more frequently associated with suicidal behavior among women; men were 2.6 times less likely than women to report this as a motive (male [ref.: female]: OR = 0.382, p = 0.035).
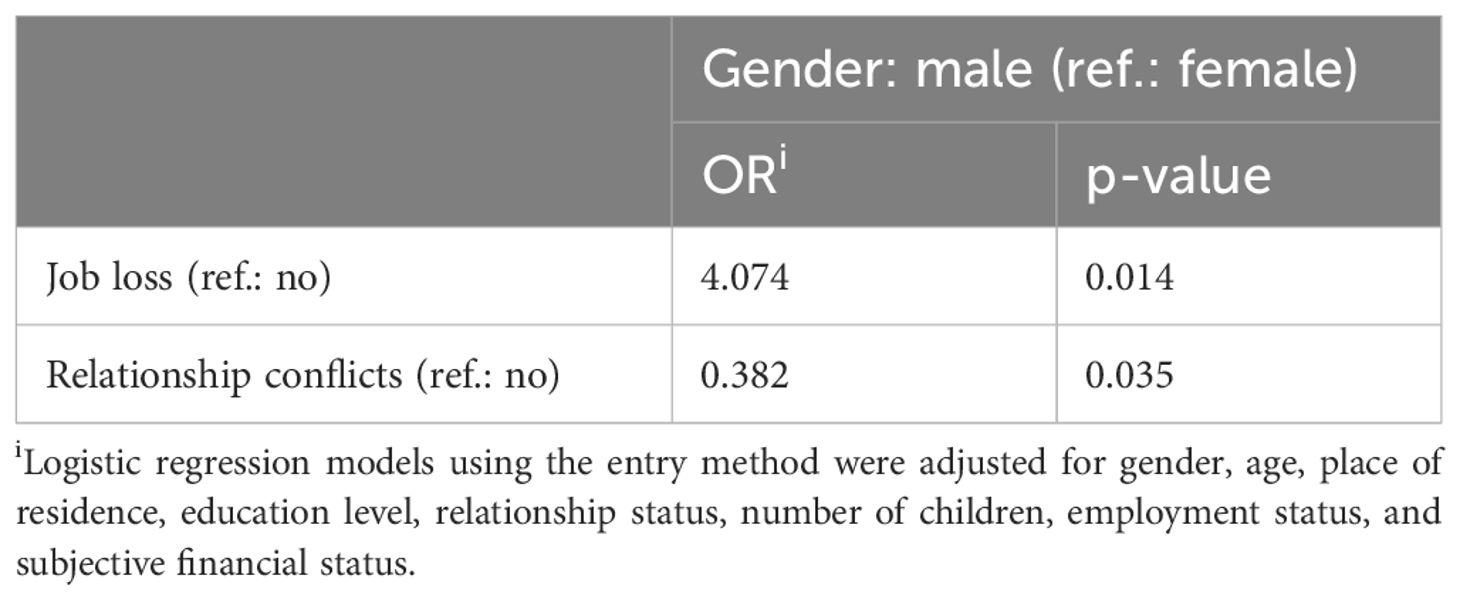
Table 6. The associations of gender with suicide motives.
These findings underscore the importance of gender-sensitive approaches to suicide prevention. For women, interventions may be more effective when addressing familial dynamics and interpersonal stressors, whereas for men, economic stressors—particularly job loss—appear to constitute a more salient risk factor. A nuanced understanding of these gender-specific patterns is critical for the development of targeted and effective prevention strategies.
Predictors of multiple suicide attempts
Table 7 illustrates that among psychiatric diagnoses, depression emerged as a strong and significant predictor of repeated suicidal behavior, with affected individuals exhibiting more than a fourfold increase in the odds of multiple suicide attempts (OR = 4.064, p = 0.004). Bipolar disorder was similarly associated with a markedly elevated risk, conferring nearly a sixfold greater likelihood of multiple attempts compared to those without the diagnosis (OR = 5.761, p = 0.006). Likewise, emotionally unstable personality disorder was a robust predictor, linked to over a fivefold increase in the probability of recurrent suicide attempts (OR = 5.132, p = 0.003). These findings suggest that mood instability, affective dysregulation, and chronic emotional distress are critical factors in the recurrence of suicidal behavior.
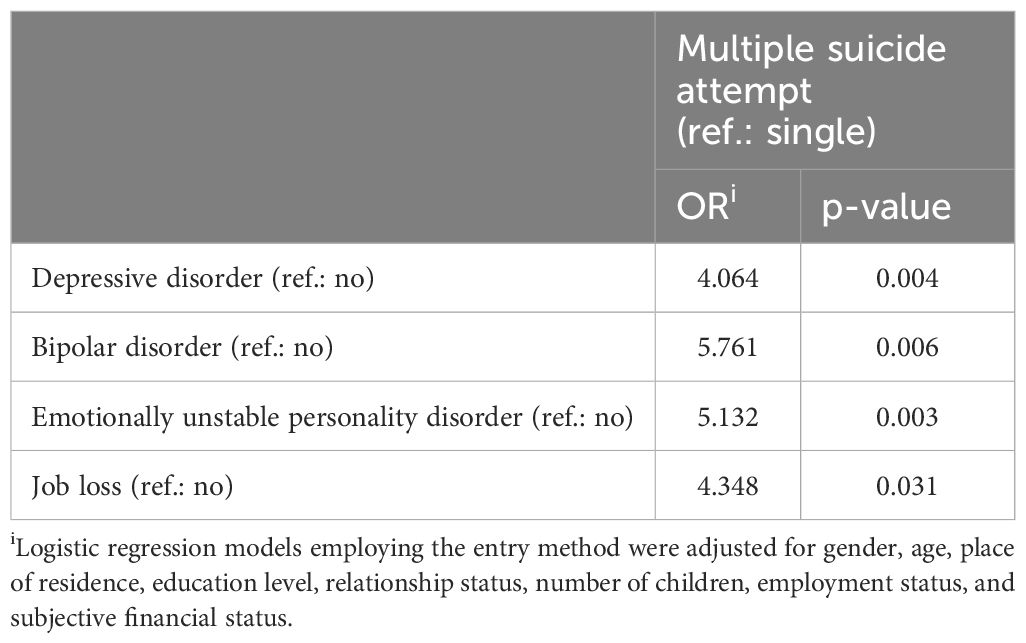
Table 7. Modelling the predictors of multiple suicide attempts.
Moreover, job loss was identified as a significant psychosocial risk factor, increasing the odds of multiple suicide attempts by more than fourfold relative to individuals without this experience (OR = 4.348, p = 0.031).
Collectively, these results underscore the necessity of prioritizing specific psychiatric diagnoses—particularly depression, bipolar disorder, and emotionally unstable personality disorder—in the assessment of risk for repeated suicide attempts. They further highlight the importance of comprehensive, individualized evaluation and intervention strategies tailored to these high-risk profiles.
Discussion
This study identified several key predictors of suicide attempts within a psychiatric inpatient population, encompassing a comprehensive range of demographic, psychiatric, and life history variables. Among all examined variables predicting suicide attempts, family history of suicide (OR = 2.283, p = 0.015) emerged as the most stable predictor. This finding supports previous research suggesting that genetic vulnerability and shared environmental stressors contribute to the intergenerational transmission of suicidal behavior (52; Rihmer et al., 2013). Consistent with a substantial body of literature, major depressive disorder also emerged as among the most robust and consistent predictors of suicidal behavior, particularly in cases involving repeated suicide attempts (OR=4.064, p=0.004). Notably, major depressive disorder diagnosis also demonstrated the highest prevalence within the sample (46.6%). This finding aligns with prior research indicating that major depressive disorder are among the most robust predictors of both suicidal ideation, intent and attempts (12, 25, 54, 62). Nicotine dependence was significantly associated with increased suicide risk (OR = 1.869, p = 0.035), supporting previous findings linking tobacco use to heightened impulsivity, psychiatric comorbidity, and suicidality (12, 14, 63, 64), while prescription drug misuse was similarly associated with elevated risk of suicide attempt (OR = 2.740, p = 0.036).
The main effects of demographic characteristics did not significantly predict suicide attempts in the overall clinical sample. However, consistent with previous literature gender-stratified analyses revealed that women were more affected by certain social determinants (65–67). Specifically, younger age was associated with a reduced likelihood of suicide attempt among women (OR = 0.955, p = 0.007), and having two or more children significantly increased the risk (OR = 2.740, p = 0.036). Additionally, a family history of suicide had a more pronounced effect among women (OR = 2.459, p = 0.028) compared to men, for whom the association was not statistically significant (OR = 1.496, p = 0.672). Notably, gender is not an independent predictor of suicidal behavior, confirming that its influence is mediated by other factors, e.g., depressive disorder or substance abuse.
The distinction between single and multiple suicide attempters further elucidated the cumulative burden of risk factors. Individuals with a history of recurrent suicide attempts exhibited higher rates of depression, bipolar disorder, nicotine dependence, and adverse life events, including a family history of suicide and being born from an unintended pregnancy. Depression emerged as a particularly strong predictor of repeated suicidal behavior (OR = 4.064, p < 0.004) and it reaffirms the central role of depression in chronic suicidality (66, 68–70). Similarly, bipolar disorder (OR = 5.761, p = 0.006) and emotionally unstable personality disorder (OR = 5.132, p = 0.003) were significant predictors of recurrent suicide risk. These findings are consistent with evidence indicating that emotional dysregulation is frequently observed in individuals at heightened risk for suicide (3, 9, 10, 71). The elevated prevalence of emotionally unstable personality disorder among multiple attempters further suggests that impulsivity and affective instability remain clinically salient features in the context of recurrent suicidality (26).
Analysis of suicide motives revealed that relationship conflicts were significantly more frequently cited as reasons for suicide attempts among women compared to men (OR = 2.60, p = 0.035). These findings are consistent with prior research indicating that interpersonal stressors, particularly within intimate relationships, serve as potent emotional triggers for acute suicidal crises (21, 43, 72). Job loss also emerged as a prominent motive, especially among men (OR = 4.074, p = 0.014) and individuals with a history of multiple suicide attempts (OR = 0.438, p = 0.031), suggesting distinct psychosocial risk profiles based on both gender and suicide attempt history (65).
Interestingly, although chronic alcohol abuse was highly prevalent within the sample, it did not significantly predict suicide attempts in the multivariate models (OR = 1.264, p = 0.449). This finding may reflect the role of alcohol as a mediating or exacerbating factor within the context of mood disorders, rather than functioning as an independent predictor of suicidal behavior. Additionally, the high baseline prevalence of alcohol use in psychiatric populations may diminish its discriminatory power in distinguishing between those with and without suicide attempts (29, 73).
Strengths and limitations
This study offers several important strengths that contribute meaningfully to the existing literature on suicide risk factors within psychiatric populations. First, it adopts a comprehensive biopsychosocial approach, examining a wide range of psychological, social, demographic, familial, and early-life variables, including less frequently studied factors such as being born from an unintended pregnancy, maternal abortion and suicide attempts. The integration of both clinical assessments and self-reported data provides a multidimensional view of suicide risk. Second, the study utilizes a relatively large inpatient sample, allowing for meaningful subgroup comparisons (e.g., single vs. multiple attempters, gender-specific patterns). Third, the statistical analysis is robust, including logistic regression models that adjust for multiple covariates, enabling the identification of key predictors such as depression, nicotine dependence, bipolar disorder, and family history of suicide. Importantly, the study also highlights gender differences and recurrent suicide attempts, offering clinically relevant insights for targeted prevention and intervention strategies.
However, several limitations should be considered when interpreting the findings. Most notably, the cross-sectional design limits the ability to establish causal relationships between the identified risk factors and suicide attempts. Longitudinal studies would be required to confirm temporal dynamics and the potential cumulative impact of these factors. Additionally, reliance on self-reported data may introduce recall bias or social desirability bias, particularly in relation to sensitive topics such as substance use, psychiatric history, and early-life experiences. The sample was drawn primarily from psychiatric inpatients, which, while appropriate for exploring high-risk populations, may restrict the generalizability of the results to non-clinical or community samples. Furthermore, cultural and societal factors specific to the Hungarian context—such as stigmatization of mental illness and social attitudes toward abortion and suicide—may influence participant responses and limit the applicability of the findings to other populations.
Conclusions
Our findings replicate and support previous international (25, 54, 71, 74, 75) and Hungarian studies (3, 4, 9, 11, 72, 73, 76, 77), reinforcing the significance of affective disorders and nicotine dependence in predicting suicide attempts. Previous literature also emphasizes that suicide attempts are frequently associated not only with diagnosable psychiatric disorders as defined by DSM-IV criteria, but also with a high prevalence of subthreshold mental disorders. These subclinical conditions, although not meeting the full diagnostic threshold, warrant serious consideration in the context of suicide prevention strategies. These findings, along with evidence from cited previous studies examining the relationship between smoking and individual-level risk of suicidal behavior, suggest that initiatives aimed at preventing tobacco use and improving the recognition and treatment of depression may contribute to the prevention of suicidality. This study underscores the multifactorial nature of suicidal behavior, integrating psychiatric, sociodemographic, substance-related, and early developmental risk factors. Our research also supports the notion that suicide risk factors interact with one another, and in certain cases, their effects may be synergistic—mutually reinforcing—rather than antagonistic. Similarly, protective factors also appear to amplify each other’s impact, suggesting a cumulative and interactive model of both risk and resilience. Depression emerged as the most robust and consistent predictor of suicide attempts, highlighting the critical importance of early detection and comprehensive treatment of depressive disorders. Nicotine dependence, bipolar disorder, anxiety disorders, and adverse early-life experiences—such as being born from an unintended pregnancy or maternal abortion attempts—also significantly contributed to suicide vulnerability. Socioeconomic stressors, particularly lower educational attainment and financial difficulties were especially relevant among women, while substance use factors were more pronounced among men. Although gender, in itself, was not identified as an independent predictor of suicide attempts—being mediated by other risk factors such as untreated psychiatric disorders—the distinct patterns observed underscore the importance of implementing gender-sensitive prevention strategies. Furthermore, individuals with multiple suicide attempts displayed elevated rates of psychiatric comorbidities and life stressors, emphasizing the need for intensive, long-term post-attempt care. Motivational factors such as interpersonal distress, chronic illness, and existential difficulties were commonly cited, indicating the importance of addressing both psychological symptoms and the psychosocial context of individuals at risk. Despite the study’s limitations, including its cross-sectional design, reliance on self-reported data, and a primarily psychiatric inpatient sample, the findings offer valuable insights into the complex interplay of psychiatric, psychosocial, and developmental contributors to suicide risk. Importantly, this study provides a foundation for practical suicide prevention efforts. Targeted mental health interventions should prioritize depression and include substance use programs—particularly for nicotine cessation—as integral components of care. Addressing socioeconomic disparities through educational and financial support programs is essential, especially for women. Family-based interventions that address intergenerational trauma and a history of suicide within families can play a preventive role, while motivation-specific interventions can provide tailored support for those facing relationship difficulties, chronic illness, or existential distress. Women with a history of abortion also represent a sensitive subgroup requiring specialized counseling and psychological support. Our study also underscores the significance of suicidal behavior among adolescents and youth, emphasizing the need to strengthen prevention efforts within schools and other secondary social settings (e.g., sports clubs). Lastly, robust post-attempt care for individuals with a history of repeated suicide attempts remains a cornerstone of prevention. Future research should expand upon these findings using longitudinal designs, objective clinical assessments, and more culturally diverse samples to enhance the generalizability and impact of suicide prevention strategies. Overall, the study highlights the need for integrated, personalized, and gender-informed interventions that address the diverse and interacting dimensions of suicide risk to reduce the incidence and recurrence of suicidal behavior effectively.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statement
The study received ethical approval from the Institutional Review Board of Péterfy Alexander Hospital and Outpatient Center (Approval No. 25/2016). The authors affirm that all procedures contributing to this research comply with the ethical standards of the relevant national and institutional committees on human experimentation, as well as with the Helsinki Declaration of 1975, as revised in 2013. The participants provided their written informed consent to participate in this study.
Author contributions
NS: Conceptualization, Investigation, Writing – original draft. BO: Formal analysis, Methodology, Software, Writing – review & editing. BS: Data curation, Formal analysis, Writing – review & editing. XG: Supervision, Writing – review & editing.
Funding
The author(s) declare that no financial support was received for the research and/or publication of this article.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Generative AI statement
The author(s) declare that no Generative AI was used in the creation of this manuscript.
Any alternative text (alt text) provided alongside figures in this article has been generated by Frontiers with the support of artificial intelligence and reasonable efforts have been made to ensure accuracy, including review by the authors wherever possible. If you identify any issues, please contact us.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. World Health Organization. Suicide data . Available online at: https://www.who.int/teams/mental-health-and-substance-use/data-research/suicide-data (Accessed 22 January 2025).
2. World Health Organization. Suicide worldwide in 2019 . Available online at: https://iris.who.int/bitstream/handle/10665/341728/9789240026643-eng.pdf?sequence=1 (Accessed 22 January 2025).
3. Almasi K, Belso N, Kapur N, Webb R, Cooper J, Hadley S, et al. Risk factors for suicide in Hungary: a case-control study. BMC Psychiatry. (2009) 9:45. doi: 10.1186/1471-244X-9-45, PMID: 19638202
4. Balint L, Dome P, and Osvath P. Long-term gender differences in completed suicide in Hungary 1955–2022: trends in absolute and relative inequalities. Hung Stat Rev. (2025) 103:517–44. doi: 10.20311/stat2025.06.hu0517
5. Rihmer Z, Gonda X, Kapitany B, and Dome P. Suicide in Hungary-epidemiological and clinical perspectives. Ann Gen Psychiatry. (2013) 12:21. doi: 10.1186/1744-859X-12-21, PMID: 23803500
6. Rihmer Z, Gonda X, Torzsa P, Kalabay L, Akiskal HS, and Eory A. Affective temperament, history of suicide attempt and family history of suicide in general practice patients. J Affect Disord. (2013) 149:350–4. doi: 10.1016/j.jad.2013.02.010, PMID: 23477849
7. Rihmer Z. Suicide in Hungary - The role of depression in regional differences and in decreasing suicide mortality. Neuropsychopharmacol Hung. (2023) 25:36–46., PMID: 37262341
8. Hungarian Central Statistical Office. (2025). Available online at: https://www.ksh.hu/stadat_files/nep/hu/nep0010.html (Accessed April 5 2025).
9. Balázs J, Lecrubier Y, Csiszér N, Koszták J, and Bitter I. Prevalence and comorbidity of affective disorders in persons making suicide attempts in Hungary: importance of the first depressive episodes and of bipolar II diagnoses. J Affect Disord. (2003) 76:113–9. doi: 10.1016/s0165-0327(02)00084-8, PMID: 12943940
10. Balázs J, Benazzi F, Rihmer Z, Rihmer A, Akiskal KK, and Akiskal HS. The close link between suicide attempts and mixed (bipolar) depression: implications for suicide prevention. J Affect Disord. (2006) 91:133–8. doi: 10.1016/j.jad.2005.12.049, PMID: 16458364
11. Rihmer A, Rihmer Z, Jekkel E, Kárteszi M, Csiszér N, and Farkas A. Psychiatric characteristics of 100 nonviolent suicide attempters in Hungary. Int J Psychiatry Clin Pract. (2006) 10:69–72. doi: 10.1080/13651500500443365, PMID: 24926772
12. Rihmer Z, Döme P, Gonda X, Kiss HG, Kovács D, Seregi K, et al. Cigarette smoking and suicide attempts in psychiatric outpatients in Hungary. Neuropsychopharmacol Hung. (2007) 9:63–7., PMID: 17970528
13. Rihmer Z, Döme P, and Gonda X. 30 years against suicide: a summary of our research on depression and suicide prevention between 1985 and 2015. Neuropsychopharmacol Hung. (2015) 17:113–9., PMID: 26485741
14. Döme P, Kapitány B, Ignits G, Porkoláb L, and Rihmer Z. Tobacco consumption and antidepressant use are associated with the rate of completed suicide in Hungary: an ecological study. J Psychiatr Res. (2011) 45:488–94. doi: 10.1016/j.jpsychires.2010.08.011, PMID: 20863518
15. Grucza RA, Plunk AD, Krauss MJ, Cavazos-Rehg PA, Deak J, Gebhardt K, et al. Probing the smoking-suicide association: do smoking policy interventions affect suicide risk? Nicotine Tob Res. (2014) 16:1487–94. doi: 10.1093/ntr/ntu106, PMID: 25031313
16. Pitchot W, Paquay C, and Ansseau M. Le comportement suicidaire: facteurs de risque psychosociaux et psychiatriques [Suicidal behaviour: psycho-social and psycho-pathological risk factor. Rev Med Liege. (2008) 63:396–403.
17. Stenbacka M and Jokinen J. Violent and non-violent methods of attempted and completed suicide in Swedish young men: the role of early risk factors. BMC Psychiatry. (2015) 15:196. doi: 10.1186/s12888-015-0570-2, PMID: 26271258
18. Rihmer Z, Rihmer A, and Beltezcki Z. Psycho-social correlates of suicidal behaviour. Neuropsychopharmacol Hung. (2022) 24:162–9., PMID: 36776017
19. Lantos T, McNally RJQ, and Nyári TA. Patterns of suicide deaths in Hungary between 1995 and 2017. SSM Popul Health. (2021) 16:100958. doi: 10.1016/j.ssmph.2021.100958, PMID: 34815998
20. Balint L, Osvath P, Kapitany B, Rihmer Z, Nemeth A, and Dome P. Suicide in Hungary during the first year of the COVID-19 pandemic: Subgroup investigations. J Affect Disord. (2023) 325:453–8. doi: 10.1016/j.jad.2023.01.046, PMID: 36642307
21. Szeifert NM, Szilágyi S, Sebők B, and Bérdi M. Changes of violent suicide attempts during the first two years of COVID-19 pandemic in Dr. Manninger Jenő National Traumatology Center, Hungary. Orv Hetil. (2023) 164:1003–11. doi: 10.1556/650.2023.32786, PMID: 37738110
22. Silverman MM, Berman AL, Sanddal ND, O’Carroll PW, and Joiner TE. Rebuilding the tower of Babel: A revised nomenclature for the study of suicide and suicidal behaviors. Part 1: Background, rationale, and methodology. Suicide Life-Threatening Behav. (2007) 37:248–63. doi: 10.1521/suli.2007.37.3.248, PMID: 17579538
23. Rydin E, Asberg M, Edman G, and Schalling D. Violent and nonviolent suicide attempts–a controlled Rorschach study. Acta Psychiatr Scand. (1990) 82:30–9. doi: 10.1111/j.1600-0447.1990.tb01351.x, PMID: 2399818
24. Rihmer Z, Dome P, Gonda X, and Belteczki Z. Assessing suicide risk based on a hierarchical classification of risk factors. Neuropsychopharmacol Hung. (2017) 19:131–6., PMID: 29306904
25. Hawton K, Saunders KEA, and O’Connor RC. Self-harm and suicide in adolescents. Lancet. (2013) 379:2373–82. doi: 10.1016/S0140-6736(12)60322-5, PMID: 22726518
26. Linehan MM, Comtois KA, Murray AM, Brown MZ, Gallop RJ, Heard HL, et al. Two-year randomized controlled trial and follow-up of dialectical behavior therapy vs therapy by experts for suicidal behaviors and borderline personality disorder. Arch Gen Psychiatry. (2006) 63:757–66. doi: 10.1001/archpsyc.63.7.757, PMID: 16818865
27. Martin A, Oehlman M, Hawgood J, and O’Gorman J. The role of impulsivity and self-control in suicidal ideation and suicide attempt. Int J Environ Res Public Health. (2023) 20:5012. doi: 10.3390/ijerph20065012, PMID: 36981922
28. Owens D, Horrocks J, and House A. Fatal and non-fatal repetition of self-harm: Systematic review. Br J Psychiatry. (2002) 181:193–9. doi: 10.1192/bjp.181.3.193, PMID: 12204922
29. Wilcox HC, Conner KR, and Caine ED. Association of alcohol and drug use disorders and completed suicide: An empirical review of cohort studies. Drug Alcohol Depend. (2004) 76:S11–9. doi: 10.1016/j.drugalcdep.2004.08.003, PMID: 15555812
30. Elbogen EB and Johnson SC. The intricate link between violence and mental disorder: results from the National Epidemiologic Survey on Alcohol and Related Conditions. Arch Gen Psychiatry. (2009) 66:152–61. doi: 10.1001/archgenpsychiatry.2008.537, PMID: 19188537
31. Beck AT, Steer RA, Kovacs M, and Garrison B. Hopelessness and eventual suicide: A 10-year prospective study of patients hospitalized with suicidal ideation. Am J Psychiatry. (1985) 142:559–63. doi: 10.1176/ajp.142.5.559, PMID: 3985195
32. Fishbain DA, Goldberg M, Meagher BR, Steele R, and Rosomoff RS. Male and female chronic pain patients categorized by DSM-III psychiatric diagnostic criteria. Pain. (1997) 73:305–17. doi: 10.1016/S0304-3959(97)00118-8, PMID: 3763232
33. Mystakidou K, Parpa E, Tsilika E, Katsouda E, Galanos A, and Vlahos L. Desire for death near the end of life: The role of depression, anxiety and pain. Gen Hosp Psychiatry. (2005) 27:258–62. doi: 10.1016/j.genhosppsych.2005.02.006, PMID: 15993258
34. Osváth P, Fekete S, and Abrahám I. Physical illness and suicidal behavior. Review of results at the Pécs Center of the WHO/EURO Multicenter Study of Parasuicide. Orv Hetil. (2001) 142:127–31., PMID: 11217161
35. Ilgen MA, Zivin K, Austin KL, Bohnert AS, Czyz EK, Valenstein M, et al. Severe pain predicts greater likelihood of subsequent suicide. Suicide Life-Threatening Behav. (2010) 40:597–608. doi: 10.1521/suli.2010.40.6.597, PMID: 21198328
36. Racine M. Chronic pain and suicide risk: A comprehensive review. Prog Neuropsychopharmacol Biol Psychiatry. (2018) 87:269–80. doi: 10.1016/j.pnpbp.2017.08.020, PMID: 28847525
37. Chen C, Pettersson E, Summit AG, Boersma K, Chang Z, Kuja-Halkola R, et al. Chronic pain conditions and risk of suicidal behavior: a 10-year longitudinal co-twin control study. BMC Med. (2023) 21:9. doi: 10.1186/s12916-022-02703-8, PMID: 36600296
38. Schrijvers DL, Bollen J, and Sabbe BG. The gender paradox in suicidal behavior and its impact on the suicidal process. J Affect Disord. (2012) 138:19–26. doi: 10.1016/j.jad.2011.03.050, PMID: 21529962
39. Kim JW, Jung HY, Won DY, Noh JH, Shin YS, and Kang TI. Suicide trends according to age, gender, and marital status in South Korea. Omega (Westport). (2019) 79:90–105. doi: 10.1177/0030222817715756, PMID: 28622733
40. Kim MH, Jung-Choi K, Jun HJ, and Kawachi I. Socioeconomic inequalities in suicidal ideation, parasuicides, and completed suicides in South Korea. Soc Sci Med. (2010) 70:1254–61. doi: 10.1016/j.socscimed.2010.01.004, PMID: 20163900
41. Osvath P, Vörös V, and Fekete S. Life events and psychopathology in a group of suicide attempters. Psychopathology. (2004) 37:36–40. doi: 10.1159/000077018, PMID: 14988649
42. Calati R, Ferrari C, Brittner M, Oasi O, Olié E, Carvalho AF, et al. Suicidal thoughts and behaviors and social isolation: A narrative review of the literature. J Affect Disord. (2019) 245:653–67. doi: 10.1016/j.jad.2018.11.022, PMID: 30445391
43. Foster T. Adverse life events proximal to adult suicide: A synthesis of findings from psychological autopsy studies. Arch Suicide Res. (2011) 15:1–15. doi: 10.1080/13811118.2011.540213, PMID: 21293996
44. Afifi TO, Enns MW, Cox BJ, Asmundson GJ, Stein MB, and Sareen J. Population attributable fractions of psychiatric disorders and suicide ideation and attempts associated with adverse childhood experiences. Am J Public Health. (2008) 98:946–52. doi: 10.2105/AJPH.2007.120253, PMID: 18381992
45. Rihmer A, Szilágyi S, Rózsa S, Gonda X, Faludi G, and Rihmer Z. The role of childhood abuse in adult suicidal behaviour. Neuropsychopharmacol Hung. (2009) 11:237–46.
46. Szeifert NM, Oláh B, and Gonda X. The mediating role of adult attachment styles between early traumas and suicidal behaviour. Sci Rep. (2025) 15:15855. doi: 10.1038/s41598-025-00831-8, PMID: 40328875
47. Kósa K, Daragó L, and Ádány R. Environmental survey of segregated habitats of Roma in Hungary: A way to be empowering and reliable in minority research. Eur J Public Health. (2007) 17:433–8. doi: 10.1093/eurpub/ckl261, PMID: 19617380
48. Tóth MD, Ádám S, Zonda T, Birkás E, and Purebl G. Risk factors for multiple suicide attempts among Roma in Hungary. Transcult Psychiatry. (2018) 55:55–72. doi: 10.1177/1363461517731703, PMID: 29035144
49. Anestis MD, Soberay KA, Gutierrez PM, Hernandez TD, and Joiner TE. Reconsidering the link between impulsivity and suicidal behavior. Pers Soc Psychol Rev. (2014) 18:366–86. doi: 10.1177/1088868314535988, PMID: 24969696
50. Schotte DE and Clum GA. Problem-solving skills in suicidal psychiatric patients. J Consult Clin Psychol. (1987) 55:49–54. doi: 10.1037/0022-006X.55.1.49, PMID: 3571658
51. Wagner BM, Cole RE, Schwartzman P, and Band EB. Psychological correlates of suicide attempts among adolescents and young adults: A 3-year longitudinal study. J Am Acad Child Adolesc Psychiatry. (2000) 39:411–9. doi: 10.1097/00004583-200004000-00010, PMID: 10761343
52. Brent DA and Mann JJ. Family genetic studies, suicide, and suicidal behavior. Am J Med Genet Part C: Semin Med Genet. (2005) 133C:13–24. doi: 10.1002/ajmg.c.30042, PMID: 15648081
53. Johnson JG, Cohen P, Gould MS, Kasen S, Brown J, and Brook JS. Childhood adversities, interpersonal difficulties, and risk for suicide attempts during late adolescence and early adulthood. Arch Gen Psychiatry. (2002) 59:741–9. doi: 10.1001/archpsyc.59.8.741, PMID: 12150651
54. Mann JJ, Apter A, Bertolote J, Beautrais A, Currier D, Haas A, et al. Suicide prevention strategies: A systematic review. JAMA. (2005) 294:2064–74. doi: 10.1001/jama.294.16.2064, PMID: 16249421
55. Yip PSF, Caine E, Yousuf S, Chang SS, Wu KCC, and Chen YY. Means restriction for suicide prevention. Lancet. (2012) 379:2393–9. doi: 10.1016/S0140-6736(12)60521-2, PMID: 22726520
56. Kleiman EM and Liu RT. Social support as a protective factor in suicide: Findings from two nationally representative samples. J Affect Disord. (2013) 150:540–5. doi: 10.1016/j.jad.2013.01.033, PMID: 23466401
57. Rihmer Z, Dome P, and Gonda X. The role of general practitioners in prevention of depression-related suicides. Neuropsychopharmacol Hung. (2012) 14:245–51.
58. Zalsman G, Hawton K, Wasserman D, van Heeringen K, Arensman E, Sarchiapone M, et al. Suicide prevention strategies revisited: 10-year systematic review. Lancet Psychiatry. (2016) 3:646–59. doi: 10.1016/S2215-0366(16)30030-X, PMID: 27289303
59. Johnson J, Gooding PA, Wood AM, and Tarrier N. Resilience to suicidality: The buffering hypothesis. Clin Psychol Rev. (2011) 31:563–91. doi: 10.1016/j.cpr.2010.12.007, PMID: 21276646
60. Stack S and Kposowa AJ. Religion and suicide acceptability: A cross-national analysis. J Sci Study Religion. (2011) 50:289–306. doi: 10.1111/j.1468-5906.2011.01568.x, PMID: 21969937
61. Heisel MJ and Flett GL. Purpose in life, satisfaction with life, and suicide ideation in a clinical sample. J Psychopathol Behav Assess. (2004) 26:127–35. doi: 10.1023/B:JOBA.0000013660.22413.e0
62. Rihmer Z. Can better recognition and treatment of depression reduce suicide rates? A brief review. Eur Psychiatry. (2001) 16(7):406–9. doi: 10.1016/s0924-9338(01)00598-3, PMID: 11728853
63. Edwards AC and Kendler KS. A twin study of depression and nicotine dependence: shared liability or causal relationship?. J Affect Disord. (2012) 142(1-3):90–7. doi: 10.1016/j.jad.2012.03.048, PMID: 22901332
64. Bohnert KM, Ilgen MA, Louzon S, McCarthy JF, and Katz IR. Substance use disorders and the risk of suicide mortality among men and women in the US Veterans Health Administration. Addiction. (2014) 112:1193–201. doi: 10.1111/add.13774, PMID: 28301070
65. Fekete S, Voros V, and Osvath P. Gender differences in suicide attempters in Hungary: retrospective epidemiological study. Croat Med J. (2005) 46:288–93., PMID: 15849852
66. Tóth MD, Ádám S, Birkás E, Székely A, Stauder A, and Purebl G. Gender differences in deliberate self-poisoning in Hungary: analyzing the effect of precipitating factors and their relation to depression. Crisis. (2014) 35:145–53. doi: 10.1027/0227-5910/a000245, PMID: 24491825
67. Bálint L, Osváth P, Rihmer Z, and Döme P. Associations between marital and educational status and risk of completed suicide in Hungary. J Affect Disord. (2016) 190:777–83. doi: 10.1016/j.jad.2015.11.011, PMID: 26625089
68. Gonda X, Fountoulakis KN, Kaprinis G, and Rihmer Z. Prediction and prevention of suicide in patients with unipolar depression and anxiety. Ann Gen Psychiatry. (2007) :6:23. doi: 10.1186/1744-859X-6-23, PMID: 17803824
69. Nock MK, Hwang I, Sampson N, and Kessler RC. Mental disorders, comorbidity and suicidal behavior: Results from the National Comorbidity Survey Replication. Mol Psychiatry. (2008) 15:868–76. doi: 10.1038/mp.2009.29, PMID: 19337207
70. Ezquerra B, Alacreu-Crespo A, Peñuelas-Calvo I, Abascal-Peiró S, Jiménez-Muñoz L, Nicholls D, et al. Characteristics of single vs. multiple suicide attempters among adolescents: a systematic review and meta-analysis. Eur Child Adolesc Psychiatry. (2024) 33:3405–18. doi: 10.1007/s00787-023-02260-2, PMID: 37470845
71. Sareen J, Cox BJ, Afifi TO, de Graaf R, Asmundson GJ, ten Have M, et al. Anxiety disorders and risk for suicidal ideation and suicide attempts: A population-based longitudinal study of adults. Arch Gen Psychiatry. (2005) 62:1249–57. doi: 10.1001/archpsyc.62.11.1249, PMID: 16275812
72. Bálint L, Osváth P, Rihmer Z, and Döme P. Associations between marital and educational status and risk of completed suicide in Hungary. J Affect Disord. (2016 Jan 15) 190:777–83. doi: 10.1016/j.jad.2015.11.011, PMID: 26625089
73. Döme P, Kapitány B, Ignits G, Porkoláb L, and Rihmer Z. Tobacco consumption and antidepressant use are associated with the rate of completed suicide in Hungary: an ecological study. J Psychiatr Res. (2011) 45(4):488–94. doi: 10.1016/j.jpsychires.2010.08.011, PMID: 20863518
74. Lorant V, Kunst AE, Huisman M, Bopp M, and Mackenbach J. Socio-economic inequalities in suicide: A European comparative study. Br J Psychiatry. (2005) 187:49–54. doi: 10.1192/bjp.187.1.49, PMID: 15994571
75. Sher L and Oquendo MA. Suicide: an overview for clinicians. Med Clin North Am. (2023) 107:119–30. doi: 10.1016/j.mcna.2022.03.008, PMID: 36402494
76. Balázs J, Bitter I, Lecrubier Y, Csiszér N, and Ostorharics G. Prevalence of subthreshold forms of psychiatric disorders in persons making suicide attempts in Hungary. Eur Psychiatry. (2000) 15:354–61. doi: 10.1016/s0924-9338(00)00503-4, PMID: 11004730
Keywords: suicide risk, psychiatric disorders, gender differences, single and multiple attempters, suicide prevention
Citation: Szeifert NM, Oláh B, Sebok B and Gonda X (2025) Uncovering key biopsychosocial risk factors in non-violent suicide attempts: evidence from a Hungarian cross-sectional study. Front. Psychiatry 16:1626808. doi: 10.3389/fpsyt.2025.1626808
Received: 11 May 2025; Accepted: 16 July 2025;
Published: 20 August 2025.
Edited by:
Fabio Sambataro, University of Padua, ItalyReviewed by:
Zoltán – Rihmer, Semmelweis University, HungaryPeter Osvath, University of Pécs, Hungary
Copyright © 2025 Szeifert, Oláh, Sebok and Gonda. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Noemi Monika Szeifert, c3plaWZlcnQubm9lbWlAc2VtbWVsd2Vpcy5odQ==
†ORCID: Noemi Monika Szeifert, orcid.org/0000-0002-3141-5116
Barnabás Oláh, orcid.org/0000-0001-9259-5272
Barbara Sebok, orcid.org/0000-0003-2358-307X
Xenia Gonda, orcid.org/0000-0001-9015-4203