 Yuancheng Jiang1
Yuancheng Jiang1 Chuchuan Wan
Chuchuan Wan Yuankai Huang
Yuankai Huang- 1The Research Center of National Drug Policy and Ecosystem, China Pharmaceutical University, Nanjing, Jiangsu, China
- 2School of Health Policy and Management, Nanjing Medical University, Nanjing, Jiangsu, China
Introduction: Burnout is a widespread issue among physicians globally, with pronounced gender disparities observed in China. This paper aims to analyze the collaboration characteristics between clinical pharmacists and physicians in China, examine the impact of collaboration experience and frequency on physician burnout, and explore potential gender differences in these mechanisms to improve collaboration efficiency and reduce physician burnout. Collaboration experience was measured using the “Physician Experience” dimension from the Kuwait questionnaire. Collaboration frequency was assessed by asking physicians how often they collaborate with clinical pharmacists in their daily work.
Methods: A cross-sectional study was conducted between July and August 2019 across 93 urban clusters in 31 Chinese provinces. The paper examined collaboration frequency and experience between physicians and clinical pharmacists in secondary and tertiary healthcare institutions, as well as physician burnout status. Data were analyzed using ordinal logistic regression models.
Results: A total of 1,381 questionnaires were distributed and 1,322 were included in the analysis. The results indicate that both the collaboration frequency and experiences between physicians and clinical pharmacists are negatively correlated with burnout. Additionally, gender shows an interactive effect in the negative relationships among collaboration frequency, collaboration experiences, and burnout. Specifically, the inclusion of gender as a variable weakened the negative correlation between collaboration frequency and the cynicism sub-dimension of job burnout. At the same level of collaboration experience, female physicians reported higher levels of cynicism and reduced personal accomplishment in job burnout compared to their male counterparts.
Conclusion: This paper suggests that increasing collaboration frequency between physicians and clinical pharmacists, improving the collaborative experience, and paying particular attention to female physicians’ needs can better reduce physician burnout and improve healthcare service efficiency and quality.
1 Introduction
Since Freudenberger introduced the concept of burnout in 1974, the phenomenon has been extensively studied. Maslach’s three-dimensional conceptualization is now widely accepted, with the Maslach Burnout Inventory-General Survey (MBI-GS) defining burnout as a syndrome characterized by emotional exhaustion, cynicism, and reduced personal accomplishment—emotional exhaustion being the core indicator (1).
Burnout is pervasive among physicians, with prevalence rates ranging from 25% to 60% (2–7). A meta-analysis by international scholars indicates that physician burnout rates may reach 80.5% (8). Empirical evidence demonstrates that physician burnout is associated with compromised patient care quality (9) and organizational disruptions, including absenteeism and turnover (10). Given these negative consequences (11, 12), physician burnout has emerged as a global health workforce concern, prompting international organizations and national governments to develop policy responses (13, 14). Research indicates that physicians burnout in China is particularly pronounced, with those practicing in secondary and tertiary hospitals experiencing more severe symptoms than their counterparts in primary care settings (15). This underscores the importance of examining burnout among physicians in the Chinese healthcare context.
Among the various theoretical models developed to understand job burnout—such as the Job Demand-Control (JD-C) model (16), the Job Demand-Control-Support (JD-C-S) model (11), the Effort-Reward Imbalance (ERI) model (17), and the Job Demand-Resource (JD-R) model (18)—this study adopts the Person–Environment Fit (P-E Fit) model as its central framework. Unlike models that primarily emphasize external job demands or imbalances, the P-E Fit model, as introduced by Maslach and Leiter (12). This model posits that burnout results not only from individual stress but also from the interaction between the individual and their environment. It is determined by the degree of fit or misfit between the individual and six areas of their work environment: workload, control, rewards, relationships, fairness, and values (1). Therefore, rather than focusing solely on stressors or resources, the P-E Fit model emphasizes the dynamic interaction between the individual and the environment. Contemporary research has further operationalized P-E Fit along four relational dimensions: person-supervisor (PS) fit, person-organization (PO) fit, person-job (PJ) fit, and person-group (PG) fit (19, 20).
A study conducted in the United States identified social support as a critical factor in job burnout among primary healthcare providers, noting that the inclusion of clinical pharmacists in healthcare teams has a positive impact on reducing burnout. Providers working alongside pharmacists to treat complex patients may reduce emotional exhaustion and affective burden, thereby decreasing burnout (21). Further research has shown that effective teamwork in healthcare settings can alleviate physician burnout, with physicians reporting lower burnout levels when they have positive collaborative experiences (22). In light of the growing demand for pharmaceutical services, the roles and responsibilities of clinical pharmacists have expanded. Their interactions with physicians have become more frequent, positioning pharmacists as integral members of the healthcare team and essential components of physicians’ work environment and interpersonal dynamics.
In parallel, gendered dynamics within healthcare organizations merit close attention. Gendered Organization Theory (23) posits that male workers are more likely to be favored within organizational structures, and gender disparities have long persisted in workplace environments. Becker’s research (24) notes that “men have an advantage over women in the labor market.” In China, the influence of Confucian ideology has reinforced traditional gender roles, with the belief that “men work outside and women manage the household” deeply embedded in society. As a result, Chinese women often face disadvantages in the workplace compared to their male counterparts (25–28). International studies (29) mention that “women are more likely to face professional crises such as distrust in male-dominated fields.” Moreover, research indicates that “female physicians often face greater challenges in balancing work and family responsibilities compared to male physicians, leading to increased work-family conflicts and stress” (30). McMurray (31) reported that female doctors are 60% more likely to experience burnout than male doctors, while Shujuan Yang’s research found that female physicians report higher levels of burnout compared to their male counterparts (32). These findings underscore the distinct impact of gender within organizational settings, particularly in the medical profession. Building on the burnout mechanisms discussed earlier, this study argues that gender differences may serve as an important moderating factor in the relationship between physician–pharmacist collaboration and burnout, and should be taken into account in the research.
However, Thomas (33), in a review of 15 studies on resident doctors, found that only four studies identified gender as a significant factor in burnout, and none suggested that female physicians are at greater risk or experience different impacts. Research by Maslach (34) found that male physicians had significantly higher depersonalization scores than their female colleagues, potentially indicating a greater predisposition to burnout. Nathalie (35) found no clear relationship between gender and burnout. These inconclusive findings suggest that the relationship between gender and burnout may not be straightforward. While existing literature indicates that gender may influence burnout, no studies have specifically examined gender as a moderating variable in this context. This study attempts to include gender as a moderating variable, aiming to further explore its moderating effect of gender on the relationship between physician collaboration and burnout.
Building on existing literature, this study proposes two hypotheses: H1: Both collaboration frequency and experience between Chinese physicians and clinical pharmacists are negatively associated with physician burnout. H2: Gender moderates the relationship between collaboration (frequency and experience) and physician burnout, such that the strength or direction of the association varies by gender. Guided by the Person-Environment (P-E) model and focusing on person-group (PG) fit this study aims to elucidate the mechanisms through which physician-pharmacist collaboration experience and frequency influence physician burnout in healthcare institutions. Additionally, it seeks to explore the moderating role of gender in this process.
Currently, research on physician-pharmacist collaboration in China is limited, and the healthcare systems in international studies differ significantly from that of China, which makes their conclusions less directly applicable. Additionally, there is a research gap regarding the relationship between collaboration experience, frequency, and physician burnout. This study aims to address this gap by offering a novel perspective on enhancing collaboration between clinical pharmacists and physicians in China. Furthermore, this research specifically examines gender differences in the relationship between collaboration experience, frequency, and physician burnout, providing valuable insights for policymakers to design targeted interventions for burnout among physicians of different genders. To achieve this, the study will integrate data on the characteristics of physician-pharmacist collaboration in China, analyze microdata from secondary and tertiary healthcare institutions, and investigate the links between collaboration experience, collaboration frequency, and physician burnout, with a focus on gender differences. This research is crucial for improving collaboration efficiency between physicians and clinical pharmacists and for reducing physician burnout.
In summary, this study offers both theoretical innovation and significant practical value, providing scientific evidence and practical recommendations for enhancing collaboration efficiency between clinical pharmacists and physicians and mitigating physician burnout in China.
2 Materials and methods
2.1 Research design and sampling
A cross-sectional survey was conducted between July and August 2019, based on informed consent and voluntary participation, to investigate the collaboration frequency and experience between physicians and clinical pharmacists, as well as physician burnout in secondary and tertiary healthcare institutions in China. In China, healthcare institutions are classified into three levels: primary healthcare institutions, secondary hospitals, and tertiary hospitals. Secondary and tertiary hospitals, which are primarily municipal, provincial, or national comprehensive hospitals, provide specialized healthcare services to a wide range of regions and play a crucial role in medical education and scientific research. Studies have indicated that burnout rates are generally lower in primary healthcare institutions, and clinical pharmacy services are predominantly offered by tertiary hospitals. Therefore, to ensure greater representativeness, the study focused on physicians working in secondary and tertiary healthcare institutions.
To enhance the representativeness of the sample and accurately reflect the working conditions of physicians in China, a multistage sampling method was employed. The sampling process involved the following steps (1): All 31 provinces (including autonomous regions and municipalities) in mainland China were included. Within each province, all prefecture-level cities or districts were categorized into three clusters—high, medium, and low—based on per capita GDP in 2018, resulting in a total of 93 city clusters (2). Within each city cluster, hospitals were selected using convenience sampling from healthcare institutions with survey authorization, ensuring that at least two tertiary hospitals were included in each cluster. A total of at least 372 hospitals were eligible for inclusion in this study (3). Within each selected hospital, physicians were recruited through convenience sampling, provided that at least two eligible physicians consented to participate and completed the survey. Eligibility criteria for physicians included possession of a medical qualification certificate, active employment in a clinical department, and prescribing authority for either outpatient or inpatient care. Physicians in non-clinical roles (e.g., laboratory technicians), those without prescribing authority (e.g. physician assistants), or those not registered at the sampled hospitals were excluded. This study aimed to survey at least 744 eligible physicians who agreed to participate.
According to epidemiological research requirements, the sample size should be 5 to 10 times the number of factors. The burnout incidence rate among physician ranges from approximately 25% to 80.5%. Considering a 10% dropout rate, the estimated sample size was at least (5×13/0.665)/0.9 = 135 cases. Ultimately, a total of 1,322 eligible physicians from 372 hospitals completed the survey and were included in the final analysis.
Convenience sampling was used at the hospital and physician levels primarily due to resource constraints and access limitations. While this approach facilitates practical implementation across diverse regions, it may introduce selection bias and limit the generalizability of results. This limitation is acknowledged as a trade-off for achieving nationwide coverage within feasible resource boundaries.
2.2 Questionnaire design
2.2.1 Collaboration frequency
Collaboration frequency was assessed by asking physicians how often they collaborate with clinical pharmacists in their daily work. Responses were categorized as follows “Never or rarely,” “At least once a week,” and “Once a day or more.”
2.2.2 Collaboration experience
Collaboration experience was measured using the “Physician Experience” dimension from the Kuwait questionnaire (36). Which was originally designed to evaluate physicians’ perceptions and experiences of collaboration with pharmacists in the Kuwaiti healthcare system. The original scale was validated within hospital settings in Kuwait and demonstrated good psychometric properties, particularly in measuring interprofessional collaboration between physicians and clinical pharmacists. In this study, the instrument was translated and adapted for use in the Chinese healthcare context, with appropriate cultural and linguistic modifications to ensure relevance. Respondents rated their agreement with each item using a 5-point Likert scale (1 = “Strongly disagree” to 5 = “Strongly agree”) based on their practical collaboration experience with clinical pharmacists. The adapted version yielded a Cronbach’s α coefficient of 0.874 and a KMO value of 0.881, indicating strong internal consistency and suitability for factor analysis in the Chinese sample.
2.2.3 Burnout
The Chinese version of the 15-item Maslach Burnout Inventory General Survey (MBI-GS) was used, with permission obtained through official channels. In 2002, Li Chaoping (37) conducted an exploratory factor analysis on the 16 items of the MBI-GS using principal component extraction and orthogonal rotation, finding a high cross-load for one item. After deleting this item, a second factor analysis confirmed that the adjusted structure of the MBI-GS was identical to the original, suggesting that the instrument maintains good construct validity in China. The internal consistency coefficients for emotional exhaustion, cynicism, and reduced personal accomplishment were 0.88, 0.83, and 0.8244, respectively. The questionnaire used a 7-point Likert scale, where 0 represented “Never” and 6 represented “Very frequently.” It included 5 questions on emotional exhaustion, 4 questions on cynicism, and 6 questions on personal accomplishment. Emotional exhaustion and cynicism were scored positively, while personal accomplishment was scored negatively. The total burnout score was calculated as: Burnout Total Score = 0.4 × Average Emotional Exhaustion Score + 0.3 × Average Cynicism Score + 0.3 × Average Personal Accomplishment Score. Although not part of the original MBI-GS manual, the approach has been used in Chinese healthcare burnout research to yield more nuanced scores. The total score ranges from 0 to 1.49 (No burnout), 1.50 to 3.49 (Moderate burnout), and 3.50 to 6 (Severe burnout). The KMO value of the questionnaire was 0.910, indicating it is highly suitable for factor analysis.
Specifically, we conducted an exploratory factor analysis (EFA) using principal component extraction with varimax rotation (Kaiser normalization). The analysis yielded four factors, with acceptable factor loadings for each item. Factor 1 included 6 items related to achievement frustration (loadings ranged from 0.777 to 0.895); Factor 2 included 5 items related to emotional exhaustion (loadings from 0.744 to 0.887); Factor 3 contained 4 items representing burnout; and Factor 4 included items related to medication consultation and collaboration, with loadings above 0.522. The factor structure was consistent with theoretical expectations.
2.2.4 Control variables
To control for potential confounding factors, the study incorporated both personal variables (e.g., gender, marital status, number of children, education level, and region) and organizational factors (e.g., years of service, hospital level, hospital type, department, technical title, administrative position, and frequency of involuntary attendance). These variables were considered as they may influence the extent of physician burnout.
The variables were measured as follows: hospital type、marital status、professional title、education level、department、administrative position、region and frequency of working with illness in the past year were treated as categorical variables, with predefined codes assigned to each category; age was treated as a continuous variable. These operational definitions were adopted to enhance measurement consistency and ensure analytical reproducibility when evaluating their potential influence on physician burnout.
2.3 Data collection
In this study, university students with professional medical backgrounds and research training were selected as interviewers. These interviewers conducted random interviews with physicians from the sample hospitals to collect relevant data. At least five doctors from each sample hospital agreed to participate in the survey. Prior to the formal survey, the interviewers identified the hospitals’ non-working hours and, with verbal permission from hospital directors or deputy directors, entered the facilities. The interviewers provided an oral explanation of the survey’s background, content, and purpose to the physicians and administered the questionnaire to those who agreed to participate and signed an informed consent form.
During the survey, the interviewers used mobile electronic devices equipped with survey software to administer the questionnaires. They explained how to answer the questions, read the items and answer choices aloud, and recorded the respondents’ verbal responses. Results from a preliminary survey indicated that this approach was feasible and that the survey demonstrated high reliability and validity. Given the relatively short length of the questionnaire, respondents did not experience survey fatigue, ensuring the quality of the data collected. All research was conducted in an undisturbed environment, and interviewers refrained from expressing any opinions or biases regarding the study content before or during the survey.
Although oral administration by trained interviewers helped ensure comprehension and data completeness, it may have introduced social desirability or interviewer bias. To minimize such effects, interviewers adhered to a standardized script, maintained neutral tone, and conducted interviews in private settings without institutional observers.
2.4 Data analysis and model testing
The electronic survey data were imported into SPSS 26.0 for initial processing, and data verification was independently conducted by two researchers. In this study, physician burnout served as the dependent variable, while collaboration frequency and collaboration experience were the primary independent variables. Demographic and work-related characteristics were included as control variables. Descriptive statistics were calculated for all relevant variables, as presented in Table 1. This study examined the relationship between physician-pharmacist collaboration frequency and experience and physician burnout, and to explore whether there were gender differences, the study investigated the interaction effects of gender on burnout and its three sub-dimensions. Ordinal logistic regression analysis was conducted using STATA 17.0, with statistical significance defined as p < 0.05. To address potential endogeneity and evaluate the robustness of the findings, the study included multicollinearity and robustness checks using STATA 17.0. A robustness test was performed by incorporating “administrative position” as an additional independent variable to determine whether the model’s results remained stable. Additionally, the study tested whether there were any multicollinearity issues among the independent variables.
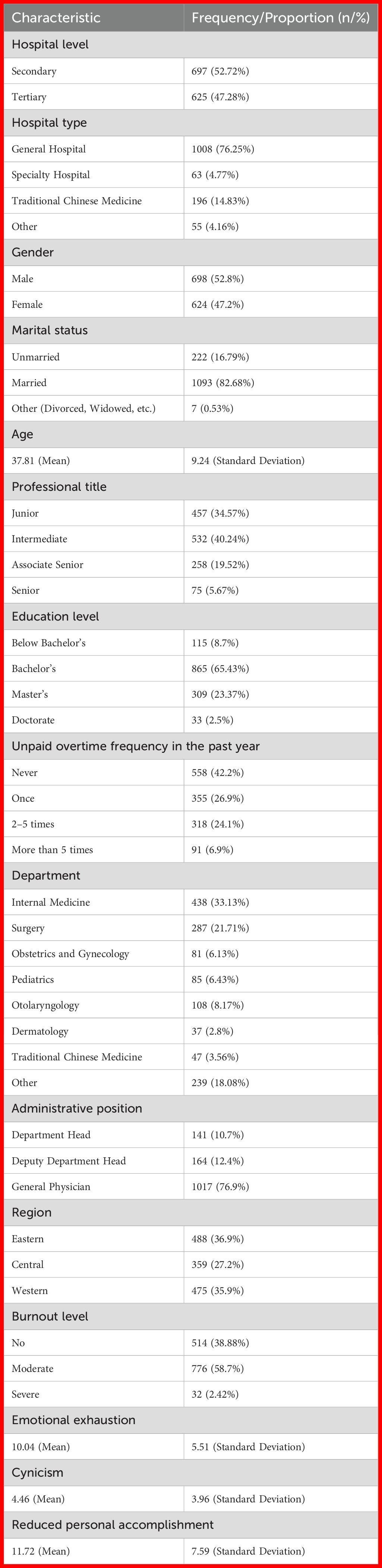
Table 1. Demographic characteristics of physicians and burnout level (n=1322).
2.5 Ethics
This study was approved by the Ethics Committee of China Pharmaceutical University (No.CPU2019015). The study was conducted after obtaining informed consent from the participants. Participants had the right to refuse to answer any questions or withdraw from the study at any time at any stage of the study. We certify that the study was performed in accordance with the 1964 declaration of HELSINKI and later amendments. To ensure confidentiality, no personally identifiable information was collected during interviews. Data were anonymized upon collection, and access was restricted to the research team. All digital data were stored in password-protected devices following institutional data protection protocols.
3 Results
3.1 Demographic characteristics of physicians and job burnout
A total of 1,500 questionnaires were distributed, and 1,381 questionnaires were returned, yielding a response rate of 92.1%. After excluding invalid questionnaires, the final valid sample size was 1,322.
As shown in Table 1, 47.28% of physicians were from tertiary hospitals, and 52.72% from secondary hospitals. Regarding professional titles, 34.57% held junior titles, 40.24% intermediate, 19.52% associate senior, and 5.67% senior titles. The majority (76.9%) had no administrative role. Physicians were primarily from internal medicine departments, and participants were distributed across the eastern, central, and western regions of China.
Over the past 12 months, more than half of the physicians reported situations where they were unable to take leave and had to work while ill. Regarding job burnout, more than half (61.12%) of the physicians exhibited signs of burnout, with 58.70% experiencing moderate burnout and 2.42% indicating severe burnout. Specifically, emotional exhaustion scored 10.04 ± 5.51, cynicism scored 4.46 ± 3.96, and reduced personal accomplishment scored 11.72 ± 7.59 (see Table 1). Burnout classification was based on the composite score derived from all three sub-dimensions (emotional exhaustion, cynicism, and reduced personal accomplishment), using the weighted formula described in the Methods section. Therefore, reported prevalence rates reflect aggregated burnout levels, not isolated dimension thresholds.
3.2 Regression analysis
3.2.1 Main effects
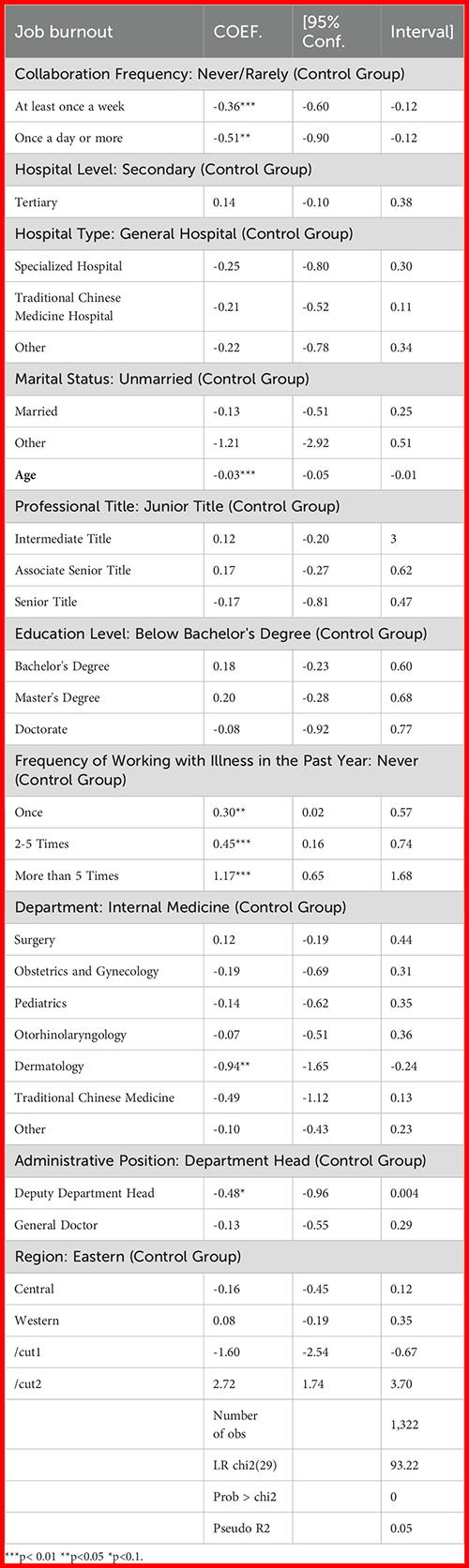
Ordinal logistic regression analysis was conducted to examine the relationship between physician-pharmacist collaboration experience and collaboration frequency (independent variables) and job burnout (dependent variable), while controlling for factors such as age, gender, marital status, and other relevant variables. The results indicated that both collaboration frequency (95% CI: -0.81 to -0.31, p < 0.001)and collaboration experience (95% CI: -0.60 to -0.12, p < 0.001) were negatively associated with job burnout (see Table 2). Additionally, control variables such as age, frequency of involuntary attendance, department, and administrative position also had significant effects on the level of physician burnout. The study employed ordinal logistic regression and tested the proportional odds assumption, collinearity, and robustness. The results indicated that the proportional odds assumption was satisfied (χ² = 101.208, df = 120, p = 0.892). The results of the collinearity test were satisfactory, with the mean Variance Inflation Factor (VIF) values being 1.56 and 1.55 (<3.25, <3.29), indicating that there were no multicollinearity issues among the independent variables. The average Variance Inflation Factor (VIF) values were 1.56 and 1.55, well below the commonly accepted threshold of 5, indicating no multicollinearity among predictors (38).” A robustness test was conducted by adding a new variable, “administrative position”, to the model. The specific administrative positions included were department head, deputy department head, and general physician. After incorporating this new variable, all key coefficients (including those of collaboration frequency and experience) retained their direction and remained statistically significant, suggesting the findings were stable.
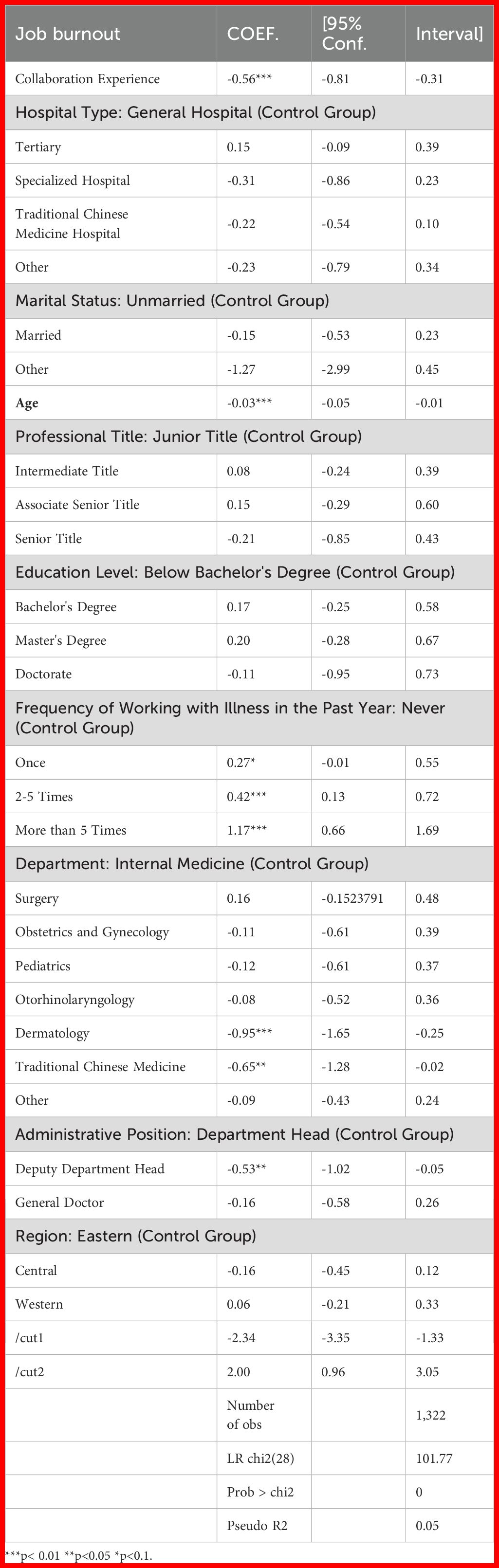
Table 2. Ordinal logistic regression results for factors related to physician burnout.
3.2.2 Interaction effects
Gender was included in the model as an interaction term to explore its potential moderating role. The interaction effects were further examined by incorporating interaction terms between gender and the key independent variables. Specifically, to assess the potential moderation effect of gender, interaction terms—collaboration experience × gender and collaboration frequency × gender—were added to the regression models. Job burnout was conceptualized as comprising three sub-dimensions: emotional exhaustion, cynicism, and reduced personal accomplishment. These dimensions were analyzed separately (see Table 3). Collaboration experience was found to be significantly associated with lower levels across all three sub-dimensions. In contrast, collaboration frequency was significantly negatively associated only with cynicism, while its associations with emotional exhaustion and reduced personal accomplishment did not reach statistical significance. The results suggest that the associations between collaboration experience and collaboration frequency with job burnout may differs by gender. Specifically, female physicians reported higher levels of burnout, cynicism, and reduced personal accomplishment compared to their male counterparts, even at the same level of collaboration experience. Furthermore, the inclusion of gender as a variable weakened the negative correlation between collaboration frequency and the cynicism sub-dimension of job burnout. These findings imply that although collaboration with clinical pharmacists is generally associated with lower levels of burnout, this association may be less pronounced among female physicians, particularly with regard to cynicism (see Table 3). Such gender differences may be partly attributable to organizational or cultural factors. For example, female physicians may encounter greater work-life conflict and experience lower levels of institutional support, which could potentially weaken the protective association between interprofessional collaboration and burnout-related outcomes.
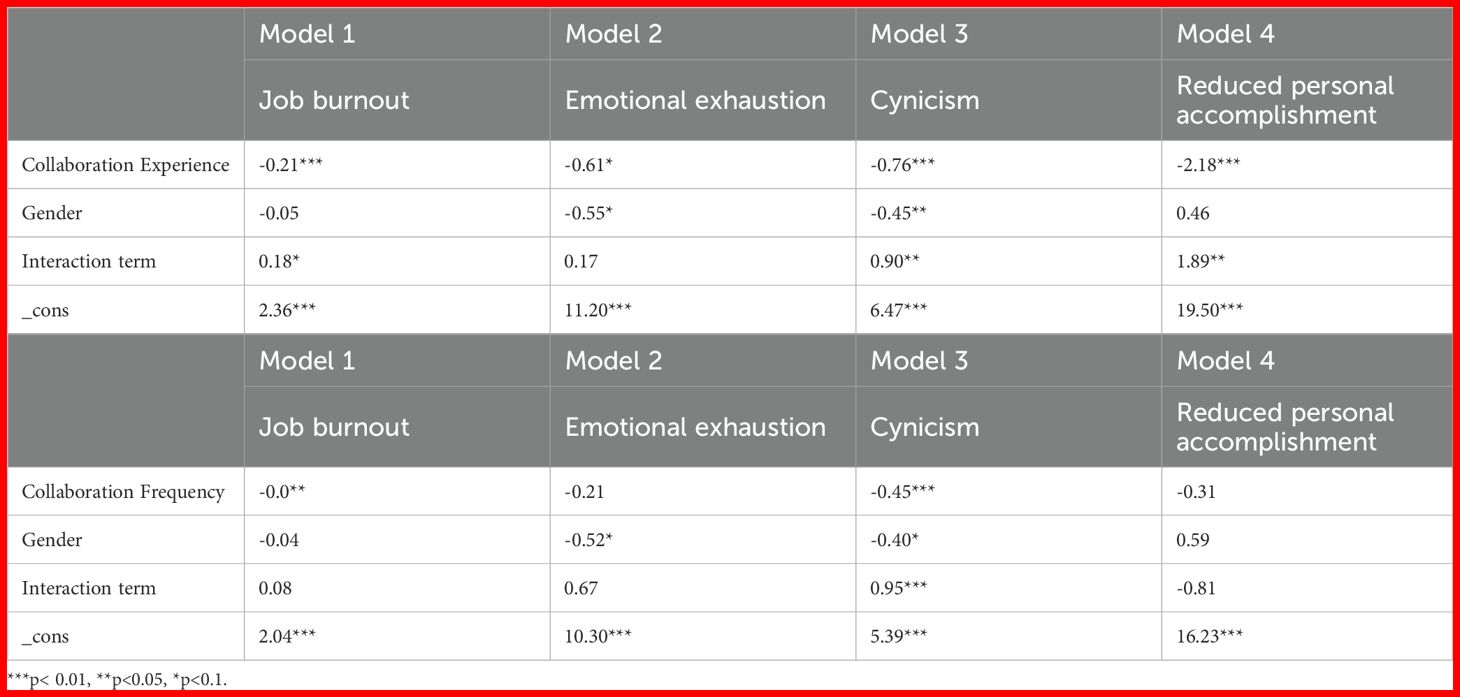
Table 3. Results for interaction effects.
However, the moderation effects were statistically significant primarily for the cynicism and emotional exhaustion dimensions, and weaker or non-significant for reduced personal accomplishment. These nuanced differences should be interpreted with caution.
4 Discussion
4.1 Demographic characteristics of physicians and job burnout levels
The study found that both collaboration frequency and collaboration experience between physicians and clinical pharmacists were significantly negatively correlated with physician burnout. Physicians who collaborated “at least once a week” or “once a day or more” reported significantly lower burnout levels than those who collaborated “never or rarely”. From the perspective of the Person-Environment Fit (PG Fit) theory (1), higher collaboration frequency may indicate better communication, clearer exchange of expectations, and fewer misunderstandings or conflicts between physicians and pharmacists (39). Higher collaboration frequency reflects better communication, clearer exchange of expectations, and fewer misunderstandings or conflicts between physicians and pharmacists (40). Additionally, shared goals and values are central to PG fit. In healthcare settings, shared goals and values may contribute to more frequent collaboration between physicians and pharmacists (41). Physicians and pharmacists working together toward high-quality patient care may foster alignment, which in turn is associated with lower burnout levels (42). Similarly, more positive collaboration experiences were associated with lower perceived burnout. Collaboration experience reflects the quality of professional interactions. Positive experiences often involve mutual respect and support (43). Mutual respect between physicians and pharmacists can serve as a psychological resource that buffers against stress (44, 45). In a positive collaboration experience, physicians and pharmacists are able to recognize and support each other’s professional roles and contributions, engage in joint decision-making (46), and establish trust and effective communication (47). These factors are linked to increased job satisfaction and reduced burnout from role disrecognition (48). Furthermore, when faced with challenges in medical work, higher collaboration frequency and positive collaboration experiences between physicians and pharmacists can form a synergistic association. The expertise of clinical pharmacists in drug management (49) helps distribute workload (50), while both parties work together to find solutions, avoid medical risks (45), and help manage work-related stress and burnout (51).
It is important to note that, due to the cross-sectional nature of this study, the observed associations between collaboration and burnout do not imply causality. Future longitudinal or experimental research designs are needed to establish the direction and causality of these effects. Our research results suggest that collaboration between physicians and clinical pharmacists in China fosters a positive work environment and enhances professional interactions, effectively reducing burnout among Chinese physicians. Therefore, policymakers and healthcare administrators can attempt to further improve the collaborative environment between physicians and clinical pharmacists in subsequent efforts, enhance the quality of their collaboration, and thus reduce the risk of physician burnout (52). Policymakers and hospital administrators can implement targeted interventions to enhance collaboration environments. These may include structured interprofessional training programs, team-based performance evaluations, and regular joint case reviews between physicians and pharmacists.
In addition, the study found that male physicians experienced lower overall burnout, particularly in the cynicism sub-dimension, compared to female physicians, largely due to more favorable collaboration experiences. Meanwhile, under the same collaboration frequency, female physicians perceived higher levels of cynicism than their male counterparts. A recent study (32) found that female doctors are more likely than male doctors to take on more work, and leadership roles are primarily held by male doctors (53). Therefore, female physicians showed higher susceptibility to cynicism and reduced personal accomplishment compared to their male colleagues, which aligns with our findings. Despite increasing independence among women, female physicians in certain healthcare environments often encounter distrust, making it more difficult for them to experience positive collaboration (54, 55). These factors may contribute to the development of burnout syndrome. These gender disparities may stem from broader sociocultural and institutional dynamics in China. For example, traditional gender norms may expect women to shoulder more family responsibilities, compounding professional stress (56). Organizational cultures in Chinese hospitals often favor male physicians in leadership and decision-making roles, further limiting female physicians’ access to influential collaborative networks (57). This social marginalization may exacerbate feelings of cynicism and reduce personal accomplishment. Given the moderating effect of gender on the negative relationship between collaboration frequency, experience, and job burnout, hospital administrators should adopt flexible strategies to provide additional care and support for female medical staff, thereby reducing the risk of burnout among female physicians. To support female physicians, institutions could establish mentorship programs, offer flexible scheduling, and ensure equal participation in leadership and decision-making forums.
Additionally, the study observed that age is negatively associated with job burnout. Several studies have concluded that burnout decreases with age (58, 59), with younger or less experienced individuals being more susceptible to burnout (15, 37, 60, 61). These studies are consistent with our findings. Younger physicians tend to experience higher levels of burnout, possibly due to a lack of experience and difficulty in developing effective coping strategies (62). As they gain experience over time, most physicians accumulate sufficient experience to manage burnout effectively.
This study shows that involuntary attendance—regardless of frequency—significantly positively affects physician burnout. Working while unwell is often referred to as presenteeism (63), which has been shown in previous studies to be associated with increased burnout (64). Van Waeyenberg (65) distinguishes between voluntary and involuntary attendance, with the latter being driven by external pressures or obligations. Involuntary attendance is positively correlated with burnout, a finding that aligns with our results. In China, clinical physicians face a severe shortage of doctors and a high number of patients, making it understandable that many physicians work while ill due to professional ethics. At the same time, physicians in China, influenced by performance evaluations, may feel obligated to work despite poor health, further contributing to burnout.
The study also found that dermatology and traditional Chinese medicine physicians in China reported lower burnout levels than physicians from other departments. Currently, there is limited research on department-specific burnout both domestically and internationally. In China, many patients are less likely to seek care in dermatology or TCM, potentially resulting in lower patient volumes and reduced work pressure, which may, in turn, decrease the risk of burnout. Apart from lower patient volume, other possible explanations include different patient expectations, lower clinical urgency, or departmental cultures that emphasize holistic care and patient rapport. These aspects may foster a more manageable work environment and reduce burnout.
Furthermore, the study that clinicians with intermediate titles were less likely to experience burnout compared to those with senior titles. In China’s healthcare system, senior physicians often shoulder greater responsibilities and pressures, such as overseeing daily operations and ensuring the quality and safety of medical services. These additional duties can increase their workload, disrupt work-life balance, and contribute to higher levels of burnout. Similarly, physicians with intermediate titles may be positioned to benefit from professional stability without the heavy administrative and supervisory burdens shouldered by senior physicians. They often have more predictable schedules and less institutional accountability, which may buffer against burnout.
4.2 Strengths and limitations
This study has three key strengths. First, it is the first to explore the interaction effect of gender on the relationship between physician-pharmacist collaboration frequency and experience and physician burnout, addressing a gap in the existing literature. Second, the large sample size enhances the statistical power of the findings, enabling a more nuanced analysis of the relationship between physician-pharmacist collaboration and burnout. Finally, the study specifically examines China’s social and cultural context, providing valuable insights into the mechanisms of collaboration and burnout among Chinese clinical physicians and pharmacists. This context-specific approach increases the applicability of the findings to China and offers valuable guidance for policy development.
Despite the significant results, there are some limitations. First, as a cross-sectional study, it is difficult to track the changes and development of the relationship between collaboration frequency, experience, and physician burnout over time, and causal inferences cannot be drawn (66). Future studies employing longitudinal designs could provide a clearer understanding of the dynamic relationships between these variables. Second, while the questionnaire used in this study represents an attempt to adapt an international tool to the Chinese context, cultural differences may still pose challenges. Thus, further research is needed to assess the generalizability of these findings across different regions or cultural settings. Third, data collection relied on self-reported recall, which may introduce bias. Lastly, although the study controlled for variables such as marital status, age, department, and involuntary attendance, the relationship between collaboration frequency, experience, and burnout is complex, and other unexamined variables may also influence these outcomes. Future research should include additional relevant variables to provide a more comprehensive and rigorous exploration of these relationships.
Future studies could benefit from longitudinal or mixed-method designs to trace the dynamic interplay of collaboration and burnout over time. Incorporating qualitative interviews would help uncover nuanced mechanisms behind physician-pharmacist interactions. Additionally, future research should explore organizational culture, leadership styles, and specific workload measures as potential mediating or moderating variables.
5 Conclusion
This study demonstrates that increasing the physician-pharmacist collaboration frequency, enhancing collaboration experience, and paying special attention to female physicians can more effectively reduce physician burnout, improve healthcare efficiency, and enhance service quality. The findings offer valuable insights into physician-pharmacist collaboration and physician burnout, providing a useful reference for policymakers and hospital administrators in China to address physician burnout and promote the development of effective physician-pharmacist team collaboration.
Data availability statement
The datasets presented in this article are not readily available because The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request. Requests to access the datasets should be directed to aHlrQGNwdS5lZHUuY24=.
Author contributions
YJ: Writing – review & editing, Data curation, Formal Analysis, Methodology, Writing – original draft. HZ: Data curation, Writing – original draft. CW: Writing – review & editing. ZW: Writing – review & editing. YH: Writing – review & editing, Project administration, Supervision. EW: Supervision, Writing – review & editing.
Funding
The author(s) declare that no financial support was received for the research and/or publication of this article.
Acknowledgments
Special thanks to primary physician who volunteered to participate in our research and the members involved in data collection and analysis.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Generative AI statement
The author(s) declare that no Generative AI was used in the creation of this manuscript.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Maslach C, Schaufeli WB, and Leiter MP. Job burnout. Annu Rev Psychol. (2001) 52:397–422. doi: 10.1146/annurev.psych.52.1.397, PMID: 11148311
2. Deckard GJ, Hicks LL, and Hamory BH. The occurrence and distribution of burnout among infectious diseases physicians. J Infect Dis. (1992) 165:224–8. doi: 10.1093/infdis/165.2.224, PMID: 1730889
3. Gallery ME, Whitley TW, Klonis LK, Anzinger RK, and Revicki DA. A study of occupational stress and depression among emergency physicians. Ann Emerg Med. (1992) 21:58–64. doi: 10.1016/s0196-0644(05)82238-3, PMID: 1539889
4. Grassi L and Magnani K. Psychiatric morbidity and burnout in the medical profession: an Italian study of general practitioners and hospital physicians. Psychother Psychosom. (2000) 69:329–34. doi: 10.1159/000012416, PMID: 11070446
5. Keller KL and Koenig WJ. Management of stress and prevention of burnout in emergency physicians. Ann Emerg Med. (1989) 18:42–7. doi: 10.1016/s0196-0644(89)80309-9, PMID: 2783361
6. Lemkau J, Rafferty J, and Gordon R Jr. Burnout and career-choice regret among family practice physicians in early practice. Fam Pract Res J. (1994) 14:213–22., PMID: 7976472
7. Ramirez AJ, Graham J, Richards MA, Cull A, Gregory WM, Leaning MS, et al. Burnout and psychiatric disorder among cancer clinicians. Br J Cancer. (1995) 71:1263–9. doi: 10.1038/bjc.1995.244, PMID: 7540037
8. Embriaco N, Azoulay E, Barrau K, Kentish N, Pochard F, Loundou A, et al. High level of burnout in intensivists: prevalence and associated factors. Am J Respir Crit Care Med. (2007) 175:686–92. doi: 10.1164/rccm.200608-1184OC, PMID: 17234905
9. Lemaire JB and Wallace JE. Burnout among doctors. Bmj. (2017) 358:j3360. doi: 10.1136/bmj.j3360, PMID: 28710272
10. Schaufeli WB and Enzmann D. The burnout companion to study and practice: A critical analysis. In: The burnout companion to study and practice: A critical analysis. Crc Press (1998).
11. Johnson JV and Hall EM. Job strain, work place social support, and cardiovascular disease: a cross-sectional study of a random sample of the Swedish working population. Am J Public Health. (1988) 78:1336–42. doi: 10.2105/ajph.78.10.1336, PMID: 3421392
12. Maslach C, Jackson SE, and Leiter MP. The maslach burnout inventory manual. In: Evaluating stress: A book of resources (1997).
13. Cescatto Bobroff MC, Trevisan Martins J, and Montezeli JH. Stress prevention at work checkpoints: practical improvements for stress prevention in the workplace. J Nurs Ufpe. (2012) 90–9.
14. Executive GBHaS. How to tackle work-related stress: A guide for employers on making the management standards work. (2009).
15. Mengming L, Zhong W, and Jiangmei Q. Analysis on factors affecting job burn-out of public hospital doctors. Chin Med Rec. (2012) 13:47–8. doi: 10.3969/j.issn.1672-2566.2012.03.029
16. Karasek R. Job decision latitude, job demands and mental strain: Implications for job redesign. (1979). STOR in Administrative Science Quarterly. doi: 10.2307/2392498, PMID: 30315367
17. Siegrist J. Adverse health effects of high-effort/low-reward conditions. J Occup Health Psychol. (1996) 1:27–41. doi: 10.1037//1076-8998.1.1.27, PMID: 9547031
18. Demerouti E, Bakker AB, Nachreiner F, and Schaufeli WB. The job demands-resources model of burnout. J Appl Psychol. (2001) 86:499–512. doi: 10.1037/0021-9010.86.3.499
19. Kristof AL. Person-organization fit: an integrative review of its conceptualizations, measurement, and implications. Personnel Psychol. (2010) 49:1–49. doi: 10.1111/j.1744-6570.1996.tb01790.x
20. Seong JY, Kristof-Brown AL, Park WW, Hong DS, and Shin Y. Person-group fit: diversity antecedents, proximal outcomes, and performance at the group level. J Manage. (2015) 41:1184–213. doi: 10.1177/0149206312453738
21. Haag J, Yost KJ, Tarpenning KAK, Umbreit A, Mcgill SA, Rantala AL, et al. Effect of an integrated clinical pharmacist on the drivers of provider burnout in the primary care setting. J Am Board Family Med. (2021) 34:553–560. doi: 10.3122/jabfm.2021.03.200597, PMID: 34088815
22. Maslach C and Leiter MP. New insights into burnout and health care: Strategies for improving civility and alleviating burnout. Med Teacher. (2017) 39:160–3. doi: 10.1080/0142159x.2016.1248918, PMID: 27841065
23. Acker J. Hierarchies, jobs, bodies: A theory of gendered organizations. Gender Soc. (1990) 139–58. doi: 10.2307/189609
24. Becker GS. Human capital, effort, and the sexual division of labor. J Labor Economics. (1985) 3:S33–58. http://www.jstor.org/stable/2534997
25. CDYZZ LIANG. Crops,Cooperation and trust pattern: empirical evidence from chain. China Economic Quarterly. (2018) 17:579–608. doi: 10.13821/j.cnki.ceq.2018.01.06
26. Ya’na XJH. Gender identity, marriage and labor behavior within households. Economic Res J. (2018) 53:136–50. doi: 10.1016/j.chieco.2021.101741
27. Ying ZXYZT. Digi talEconomy, household laborDivision,and gender equality. China Economic Quarterly. (2023) 23:125–41. doi: 10.13821/j.cnki.ceq.2023.01.08
28. Yueyao DCDSY. Rice theory, housework division and female labour force participation. J World Economy. (2020) 43:3–25. doi: 10.19985/j.cnki.cassjwe.2020.07.002
29. Li Z, Liu J, Li H, Huang Y, and Xi X. Primary healthcare pharmacists’ Perceived organizational support and turnover intention: do gender differences exist? Psychol Res Behav Manag. (2023) 16:1181–93. doi: 10.2147/prbm.S406942, PMID: 37082527
30. Robinson J. Postcolonialising geography: tactics and pitfalls. Singapore J Trop Geography. (2003) 24:273–89. doi: 10.1111/1467-9493.00159
31. Julia E, McMurray M, Linzer TR, and Konrad JD. The work lives of women physicians: results from the physician work life study. J Gen Internal Med. (2000) 273–89. doi: 10.1111/j.1525-1497.2000.im9908009.x, PMID: 10886471
32. Shujuan Y, Danping L, Hongbo L, Juying Z, Zhanqi D, and Dongmei L. Relationship of work-family conflict, self-reported social support and job satisfaction to burnout syndrome among medical workers in southwest China: A cross-sectional study. PloS One. (2017) 12:e0171679. doi: 10.1371/journal.pone.0171679, PMID: 28207821
33. Thomas NK. Resident burnout. Jama. (2004) 292:698. doi: 10.7326/0003-4819-137-8-200210150-00021, PMID: 12379076
34. Maslach C. Job burnout: new directions in research and intervention. Curr Dir psychol Sci. (2003) 12:189–92. doi: 10.1111/1467-8721.01258
35. Embriaco N and Papazian L. Erratum: high level of burnout in intensivists—Prevalence and associated factors. Am J Respir Crit Care Med. (2007) 175:1209a–1210. doi: 10.1164/ajrccm.175.11.1209a
36. Xiao-yu L. Introduction of and experience draws on the measurement methods aboard for clinical pharmaoeutical care requirement of physicians. Chin J Hosp Pharm. (2020) 40:1607–11. doi: 10.13286/j.1001-5213.2020.15.02
37. Li CP and Shi K. The influence of distributive justice and procedural justi ce on job burnout. Acta Psychologica Sinica. (2003) 35:677–84. doi: 10.1023/A:1022289509702
38. O’brien RM. A caution regarding rules of thumb for variance inflation factors. Qual Quantity. (2007) 41:673–90. doi: 10.1007/s11135-006-9018-6
39. Dyrbye LN, Shanafelt TD, Balch CM, Satele D, and Freischlag J. Relationship between work-home conflicts and burnout among american surgeons: A comparison by sex. Arch Surgery. (2011) 146:211. doi: 10.1001/archsurg.2010.310, PMID: 21339435
40. Morgantini LA, Naha U, Wang H, Francavilla S, Acar M, Flores JM, et al. Factors contributing to healthcare professional burnout during the COVID-19 pandemic: A rapid turnaround global survey. PloS One. (2020) 15:1–11. doi: 10.1371/journal.pone.0238217, PMID: 32881887
41. Xiaoyu ZQYCLMX. Construction of collaborative relationship model between clinical pharmacists and physicians in China. China Pharmacy. (2019) 30:711–6. doi: 10.13286/j.1001-5213.2020.15.02
42. Garrosa E, Moreno-Jiménez B, Rodríguez-Munoz A, and Rodríguez-Carvajal R. Role stress and personal resources in nursing: A cross-sectional study of burnout and engagement. Int J Nurs Stud. (2011) 48:479–89. doi: 10.1016/j.ijnurstu.2010.08.004, PMID: 20828694
43. Xiaoyu WCHYX. Discussion on the concept of collaboration between clinical pharmacists and physicians in China. China Pharmacy. (2023) 34:487–92. doi: 10.6039/j.issn.1001-0408.2023.04.20
44. Bottiani JH, Duran CAK, Pas ET, and Bradshaw CP. Teacher stress and burnout in urban middle schools: Associations with job demands, resources, and effective classroom practices. J School Psychol. (2019) 77:36–51. doi: 10.1016/j.jsp.2019.10.002, PMID: 31837727
45. West CP, Dyrbye LN, and Shanafelt TD. Physician burnout: contributors, consequences and solutions. J Internal Med. (2018) 283:516–29. doi: 10.1111/joim.12752, PMID: 29505159
46. Xiaoyu WCHYX. Exploration of influential factors for collaboration between clinical pharmacists and physicians in China based on literature review. China Pharmacy. (2022) 33:2791–6. doi: 10.6039/j.issn.1001-0408.2022.22.21
47. Jennie B, Jarrett PD, MedEd M, Bcacp MQ, and Pharm. D. Pharmacist burnout: The real dilemma and missing pieces. Am J Health-System Pharmacy. (2019) 76:2. doi: 10.1093/ajhp/zxz131, PMID: 31369119
48. Alrawashdeh HM, Al-Tammemi AB, Alzawahreh MK, Al-Tamimi A, and Ghoul I. Occupational burnout and job satisfaction among physicians in times of COVID-19 crisis: a convergent parallel mixed-method study. BMC Public Health. (2021) 21:811. doi: 10.1186/s12889-021-10897-4, PMID: 33906619
49. Shi-kun H-j. Discussion on the service strategies of clinical pharmacists in the process of pharmacy services in medical institutions. . Chin J Rational Drug Use. (2020) 17:19–22. doi: 10.3760/CMA.J.CN112137-20220221-00350
50. Waszyk-Nowaczyk M, Guzenda W, Kamasa K, Pawlak K, Bałtruszewicz N, Artyszuk K, et al. Cooperation between pharmacists and physicians - whether it was before and is it still ongoing during the pandemic? J Multidiscip Healthc. (2021) 14:2101–10. doi: 10.2147/jmdh.S318480, PMID: 34393489
51. Tucker SJ, Weymiller AJ, Cutshall SM, Rhudy LM, and Lohse CM. Stress ratings and health promotion practices among RNs: a case for action. J Nurs Administration. (2012) 42:282–92. doi: 10.1097/NNA.0b013e318253585f, PMID: 22525292
52. Welp A, Meier LL, and Manser T. The interplay between teamwork, clinicians’ emotional exhaustion, and clinician-rated patient safety: a longitudinal study. Crit Care. (2016) 20:110. doi: 10.1186/s13054-016-1282-9, PMID: 27095501
53. Beschoner P, Braun M, Schoenfeldt-Lecuona CF, and von Wietersheim J. Gender aspects in female and male physicians. Occupational and psychosocial stress. Bundesgesundheitsblatt, Gesundheitsforschung. Gesundheitsschutz. (2016) 59:1343–50. doi: 10.1007/s00103-016-2431-7, PMID: 27631321
54. Beibei Y. Current status of gender differences in the working environment and work experience of female medical staff and measures to improve them. Chin Med J. (2022) 102:5. doi: 10.3969/j.issn.2096-3327.2020.11.005
55. Dutta N, Giddings L, and Maggino F. Does trust always help gender role attitudes? Role Individualism Collectivism. (2022) 324. doi: 10.1007/s11205-021-02755-y, PMID: 34276121
56. Wang T and Zeng R. Addressing inequalities in China’s health service. Lancet. (2015) 386:1441. doi: 10.1016/S0140-6736(15)00402-X, PMID: 26466037
57. Li M, Raven J, and Liu X. Feminization of the health workforce in China: exploring gendered composition from 2002 to 2020. Hum Resour Health. (2024) 22:15. doi: 10.1186/s12960-024-00898-w, PMID: 38373975
58. Alacacioglu A, Yavuzsen T, Dirioz M, Oztop I, and Yilmaz U. Burnout in nurses and physicians working at an oncology department. Psychooncology. (2009) 18:543–8. doi: 10.1002/pon.1432, PMID: 18942658
59. Kanai-Pak M, Aiken LH, Sloane DM, and Poghosyan L. Poor work environments and nurse inexperience are associated with burnout, job dissatisfaction and quality deficits in Japanese hospitals. J Clin Nurs. (2008) 17:3324–9. doi: 10.1111/j.1365-2702.2008.02639.x, PMID: 19146591
60. Erickson RJ and Grove WJC. Why emotions matter: age, agitation, and burnout among registered nurses. Online J Issues Nursing. (2008) 13:1–13. doi: 10.3912/ojin.vol13no01ppt01
61. Johnson SJ, Holdsworth L, Hoel H, and Zapf D. Customer stressors in service organizations: The impact of age on stress management and burnout. Eur J Work Organizational Psychol. (2013) 22:318–30. doi: 10.1080/1359432X.2013.772581
62. Bilge F. Examining the burnout of academics in relation to job satisfaction and other factors. Soc Behav Pers Int J. (2006) 34:1151–60. doi: 10.2224/sbp.2006.34.9.1151
63. Ruhle S, Breitsohl H, Aboagye E, Baba VV, and Muschalla B. To work, or not to work, that is the question” -Recent trends and avenues for research on presenteeism. Eur J Work Organizational Psychol. (2020) 29:344–63. doi: 10.1080/1359432x.2019.1704734
64. Demerouti E, Blanc PML, Bakker AB, Schaufeli WB, and Hox J. Present but sick: a three-wave study on job demands, presenteeism and burnout. Career Dev Int. (2009) 14:50–68. doi: 10.1108/13620430910933574
65. Vanwaeyenberg T. Why do employees attend work sick? The assessment and relevance of opposite presenteeism motivations. J Occup Organizational Psychol. (2024) 97:536–54. doi: 10.1111/joop.12481
Keywords: burnout, collaboration, pharmacists, physicians, gender equity
Citation: Jiang Y, Zhang H, Wan C, Wu Z, Huang Y and Wang E (2025) The association of physician-clinical pharmacist collaboration frequency and experience on physician burnout: are there gender differences. Front. Psychiatry 16:1627734. doi: 10.3389/fpsyt.2025.1627734
Received: 13 May 2025; Accepted: 09 July 2025;
Published: 28 July 2025.
Edited by:
Virtudes Pérez-Jover, Miguel Hernández University, SpainReviewed by:
Dragana Jocic, Faculty of Pharmacy, SerbiaVanessa Neves, Universidade Federal de Sao Paulo, Brazil
Copyright © 2025 Jiang, Zhang, Wan, Wu, Huang and Wang. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Yuankai Huang, aHlrQGNwdS5lZHUuY24=; Ennan Wang, d2VuQG5qbXUuZWR1LmNu