Abstract
Objectives:
Previous studies have established links between Internet addiction, life satisfaction, and post-traumatic stress symptoms (PTSS) in individuals exposed to disasters; however, the nature of longitudinal links remains uncertain. This study aimed to determine the potential associations among Internet addiction, life satisfaction and PTSS among disaster-exposed Chinese children and early adolescents.
Methods:
A three-wave longitudinal design was employed over two years and included 2354 Chinese children and early adolescents aged 6 years to 14 years who directly experienced an earthquake and COVID-19. A complete longitudinal mediation method was applied to analyze data collected in three waves from 2020 to 2022 with a one-year interlude.
Results:
Life satisfaction at Time 2 (T2) fully mediated the associations between Internet addiction at Time 1 (T1) and PTSS at Time 3 (T3). Internet addiction at T2 was a significant mediator of links between life satisfaction at T1 and PTSS at T3.
Conclusions:
These findings underscore the pivotal role of life satisfaction in mediating the impact of early Internet addiction on long-term psychological outcomes, highlighting it as a key target for interventions aimed at enhancing mental well-being after disaster exposure. Moreover, Internet addiction mediated the link between earlier life satisfaction and later PTSS, highlighting the importance of reducing problematic Internet use to prevent long-term stress symptoms.
1 Introduction
In recent years, Internet addiction (IA) has become among the most concerning adverse mental reactions among young people after experiencing stressful and traumatic life events (1). IA refers to a social problem characterized by typical symptoms such as excessive preoccupation with being online, persistent urges to use the Internet, neglect of responsibilities in real life, and intense emotional discomfort with online disconnection (2). Previous research has reported that after experiencing disasters, adolescents and young adults report an increase in IA symptoms [e.g (3–6).,]. Children and adolescents frequently used the Internet for various activities during COVID-19, such as maintaining social connections, engaging in distance learning, doing homework online, and accessing information on diverse topics (4). They are more susceptible to IA because they are in the major developmental period in terms of physiology, psychology, and socialization (1). In addition, the average time spent on the Internet increased during COVID-19, which increased IA risk among children and adolescents exposed to disasters (4). Prior studies found that 13.6% of adolescents experienced IA before the COVID-19 pandemic (7) and 24.4% of adolescents had IA during this period (8). In addition, previous research on an earthquake in Turkey indicated that survivors increased their Internet usage as a coping mechanism for stress, which could easily result in problematic use after experiencing a disaster (9).
Previous research findings indicate that IA occurrence is often accompanied by the development of psychological disorders after a disaster, such as post-traumatic stress symptoms (PTSS) (4). PTSS are defined as an individual’s adverse psychological responses and symptoms (e.g., hyperarousal, flashbacks, emotional numbness, and intrusive thoughts) after a traumatic experience, such as a disaster (10). PTSS were strongly correlated with IA in previous studies (7, 11–13). The studies noted that a more severe level of post-traumatic stress disorder (PTSD) symptoms was significantly linked with more problematic Internet use among 392 South Korean students after their experience with the Sewol ferry disaster (14, 15). Based on a sample of 776 middle-school Chinese students, one study found a strong positive association between IA symptoms and PTSS after the Wenchuan earthquake (5). Additionally, a preceding study, after controlling for age and recurring trauma exposure, reported a significant and positive relationship between PTSD and IA symptoms among 767 post-earthquake adolescents (16). A study based on a sample of 554 survivors exposed to the Turkey earthquake reported that a higher IA level was significantly associated with more severe PTSD symptoms (9).
Multiple longitudinal studies have implied a potential predictive effect of IA on PTSS following traumatic events, especially among young people with sociodemographic vulnerabilities and who have experienced severe disasters. One such study, based on a sample of 7–958 Chinese adolescents exposed to COVID-19, employed network analysis to reveal the major comorbid symptoms between IA and PTSD symptoms, suggesting IA could play a significant role in the persistence of PTSD symptoms over time (4). Another two-month longitudinal study of 811 Chinese adolescents who experienced COVID-19 applied cross-lagged panel network modeling to examine the relationships between PTSD symptoms and IA. The results revealed that high and low severity of IA strongly predicted the hyperarousal symptom from PTSD and that IA could significantly impact progression of PTSD symptoms (17).
Previous studies have suggested that increased IA in the early stages following exposure to stressful events may contribute to more severe long-term PTSS, potentially through the mediating effect of decreased life satisfaction (LS) (18, 19). LS refers to an individual’s overall evaluation of life quality and reflects how positively they generally perceive their life (20). A comprehensive meta-analysis of 18 studies found that individuals with higher IA levels tended to report significantly lower quality of life and poorer psychological well-being (21). Similarly, a global meta-analysis across 13 countries found that a higher national prevalence of IA was significantly associated with lower national levels of LS (22). In addition, a cross-cultural study involving 943 participants reported a significant negative association between PTSD symptoms and LS among young adults (23). Several other studies have also supported this negative relationship between PTSD and LS (e.g., 24, 25). Moreover, some research has suggested that the onset and persistence of IA may lead to inadequate LS (26), which could further impair mental well-being and elevate the risk of developing mental disorders such as PTSD in individuals exposed to various stressful events [e.g (27, 28)].
Several theories and studies suggest that LS may play a mediating role in the longitudinal relationship between IA and PTSS. For example, self-determination theory posits that mental well-being depends on the fulfillment of three basic psychological needs including autonomy (i.e., feeling in control and making self-determined decisions without external pressure), competence (i.e., feeling capable and effective in managing challenges), and relatedness (i.e., feeling connected, supported, and close to others) (29). IA could hinder the satisfaction of these needs, leading to decreased LS and an increased risk of negative psychological outcomes such as PTSS (30). Previous research has shown that excessive Internet use, particularly when characterized by maladaptive patterns such as escapism or social withdrawal, might compromise the fulfillment of these basic psychological needs, thereby resulting in diminished LS (31). Reduced LS may weaken psychological resilience and adaptive coping mechanisms, which could heighten individuals’ vulnerability to trauma-related symptoms (21). Accordingly, LS may serve as a mediating factor in the relationship between IA and PTSS as addictive behaviors disrupt the satisfaction of basic psychological needs, thereby reducing mental well-being and increasing susceptibility to trauma-related symptoms following disaster exposure.
The cognitive-behavioral model (CBM) has also contributed to establishing that LS may mediate the longitudinal relationship between IA and PTSS (32). CBM posits that thoughts, feelings, and behaviors are interrelated and mutually influential (32). IA is frequently characterized by maladaptive cognitive patterns (e.g., beliefs such as “being online is the only way I can unwind”) and avoidance behaviors (e.g., engaging in compulsive Internet use to avoid real-life stressors). These patterns may restrict engagement in meaningful offline activities and social relationships, thereby diminishing overall LS (33). Moreover, as individuals increasingly rely on the Internet as a coping mechanism, they may develop cognitive distortions (e.g., beliefs such as “I am only competent in online contexts”), experience reduced real-world functioning and social connectedness, and begin to neglect personal aspirations and achievements. These experiences can undermine LS, a fundamental dimension of psychological well-being (34). Previous research has indicated that lower LS is associated with reduced psychological resilience, increased vulnerability to trauma-related stress, more negative appraisals of traumatic experiences, and decreased use of adaptive coping strategies (9, 35, 36). These factors may increase individuals’ susceptibility to developing PTSS following trauma exposure induced by disaster events (24). Accordingly, LS could mediate the impact of IA at the onset on prolonged PTSS by impacting the psychological consequence of cognition and behavior adjustment and influencing coping capacity after trauma. Based on the above, we hypothesized that LS at the one-year follow-up would mediate the association between baseline IA and PTSS at the two-year follow-up among disaster-exposed children and early adolescents exposed to the disaster.
Although prior research has highlighted the impact of IA on PTSS, few longitudinal studies have explored the mediating role of LS in their relationship among disaster-exposed children and early adolescents. To address this gap, this study examined the longitudinal associations among IA, LS, and PTSS across two years. Utilizing a three-wave longitudinal design, the study involved a large sample of children and early adolescents affected by disasters. The findings should enhance our understanding of the developmental pathways linking behavioral addiction to trauma-related mental symptoms and to inform targeted interventions that support psychological well-being in post-disaster contexts.
2 Materials and methods
2.1 Participants and procedure
The study data were obtained from the Chengdu Positive Child Development project, which conducted a three-wave study among Chinese children and adolescents during the COVID-19 lockdown period (37). Chengdu was one of the worst-affected cities in China during COVID-19. Moreover, as the capital of Sichuan province in western central China, Chengdu was strongly impacted by earthquakes of different magnitude levels that occurred in China. All participants in this three-wave study experienced the most challenging and severe phase of the COVID-19 pandemic in Chengdu. While the pandemic was the primary factor, the participants may have also been secondarily affected by earthquakes of different intensities.
A random cluster sampling method was used to select five schools in Chengdu to recruit the project participants, including three high schools and two schools that provide integrated primary and middle education under unified management. A self-administered questionnaire was used to collect data. Three waves of data were collected from 2020 to 2022 with a one-year interval, including baseline (Time 1, T1: June–July 2020), first follow-up (Time 2, T2: June 2021), and second follow-up (Time 3, T3: June 2022). A total of 7–393 participants were enrolled at T1. Of these, 5–913 remained at T2 and 2–354 completed the study at T3, reflecting attrition rates of 20% from T1 to T2 and 60% from T2 to T3. Inconsistent regional lockdowns during the COVID-19 outbreak posed logistical challenges for data collection and contributed to increased participant attrition across time points.
Attrition analyses revealed that participants who dropped out were significantly more likely to be older, exhibited higher baseline IA levels, and reported lower LS (ps <.001). No significant differences were observed in sex (p = .076) or PTSS (p = .828) between those who completed all three waves and those lost to follow-up. The final sample for the current study comprised 2–354 participants who completed all three waves (50.3% females, SD = 1.77). Participants’ ages at T1 ranged from 6 years to 14 years (Mage = 9.62).
Both university and administrative departments at the data collection schools were approved by the Research Ethics Committee to conduct the research (approval no. K2020025 and KS2022913). The study’s purpose, process, participants’ rights, privacy protection, and data-retention policy were introduced to all voluntary participants. Consent was provided by participants, and the legal guardians permitted their participation in the study.
2.2 Measures
PTSS were measured using the Chinese version of the 13-item Child Revised Impact of Events Scale (38). Participants rated each item on a six-point frequency scale (0 = not at all; 5 = often). The total scores ranged from 0 to 65, with a higher score representing a higher level of PTSD symptoms. The scale has been shown to have good validity and reliability in previous studies (39). The scale showed good internal consistency in the current study. Cronbach’s alpha coefficients for PTSS at T1, T2, and T3 were 0.89, 0.87, and 0.87, respectively.
IA was measured using the Chinese version of the 20-item Young’s Internet Addiction Test (40). A five-point Likert scale was used to rate each item (1 = does not apply; 5 = always), with total scores ranging from 20 to 100. A higher total score indicates a more severe IA level. A prior study demonstrated the test’s great validity and reliability (41). The scale showed excellent internal consistency in the current study. Cronbach’s alpha coefficients for IA at T1, T2, and T3 were 0.93, 0.94, and 0.95, respectively.
LS was measured using the Chinese version of the five-item Satisfaction with Life Scale (20). Each item is rated on a six-point scale from 1 (strongly disagree) to 6 (strongly agree), with the overall score lying between 5 and 30. A higher total score represents a higher level of LS. The robust validity and reliability of this scale was demonstrated by a previous study (42). In this study, the scale showed an acceptable internal consistency. Cronbach’s alpha coefficients for LS at T1, T2, and T3 were 0.77, 0.83, and 0.86, respectively.
2.3 Statistical analysis
First, a descriptive analysis of all the study variables was conducted and a correlation matrix constructed using SPSS (Version 24). Second, a longitudinal mediation approach was applied using structural equation modeling (SEM) to examine the relationships among PTSS, IA, and LS across the three waves. This method allowed all three variables to be included in the model at each time point and enabled the analysis of all possible mediation pathways (43). It provides a robust framework for assessing whether the effect of a predictor on an outcome is mediated by variables across different time points while accounting for potential confounding factors (43). The study variables (i.e., PTSS, IA, and LS across the three waves) were modeled as latent variables, with subscales for each item as indicators. Age and sex were used as covariates that might be linked with the study variables. Furthermore, tests for common-method bias, temporal differences, measurement equivalence, and univariate normality were conducted across the three waves. AMOS (Version 23) was employed to assess the significance of mediation effects using 5–000 bootstrapped replications. Maximum likelihood estimation was applied to assess the parameters. Some suggested indexes and their standards were used to estimate the goodness-of-fit and quality-of-mediation model (44). An acceptable model required that the ratio of χ2 to degree of freedom should be smaller than 5.0. The Tucker-Lewis (TLI), normed fit (NFI), and comparative fit (CFI) indices should be higher than 0.90. The standard root mean square residual (SRMR) and root mean square error of approximation (RMSEA) should be lower than 0.08 and 0.05, respectively (44). As all participants consented to completing all the items, and no data were missing across all three waves.
3 Results
3.1 Descriptive findings
The descriptive-analysis results, including means, standard deviations, and intercorrelations among the study variables, are presented in Table 1. Significant correlations were observed among IA, LS, and PTSS across the three study waves; however, T3 PTSS did not significantly correlate with T1 IA (r = .035, p = .086), T1 LS (r = –.023, p = .275), and T2 LS (r = –.023, p = .262). All study variables were significantly intercorrelated after controlling for sex and age, excluding a nonsignificant intercorrelation between T1 LS and T3 PTSS (r = –.038, p = .066).
Table 1
| Variables | M±SD | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 |
|---|---|---|---|---|---|---|---|---|---|---|
| 1 T1 IA | 31.74±13.71 | / | -.313*** | .253*** | .468*** | -.229*** | .164*** | .173*** | -.085*** | .058** |
| 2 T1 LS | 22.90±5.72 | -.330*** | / | -.182*** | -.260*** | .391*** | -.127*** | -.065** | .113*** | -.038 |
| 3 T1 PTSS | 14.28±14.52 | .243*** | -.178*** | / | .155*** | -.123*** | .280*** | .092*** | -.058** | .119*** |
| 4 T2 IA | 32.97±14.21 | .508*** | -.293*** | .140*** | / | -.343*** | .255*** | .213*** | -.151*** | .084*** |
| 5 T2 LS | 23.03±5.81 | -.262*** | .412*** | -.116*** | -.394*** | / | -.151*** | -.119*** | .215*** | -.048* |
| 6 T2 PTSS | 13.84±12.96 | .144*** | -.119*** | .279*** | .217*** | -.137*** | / | .075*** | -.075*** | .160*** |
| 7 T3 IA | 33.77±14.48 | .230*** | -.104*** | .085*** | .300*** | -.178*** | .056** | / | -.339*** | .293*** |
| 8 T3 LS | 23.29±5.94 | -.114*** | .134*** | -.055** | -.197*** | .246*** | -.067** | -.366*** | / | -.256*** |
| 9 T3 PTSS | 11.24±11.51 | .035 | -.023 | .119*** | .042* | -.023 | .163*** | .249*** | -.235*** | / |
Means, standard deviations, and correlations among study variables (n = 2354).
[1] The left/bottom triangle displays the Pearson’s correlations of all study variables, and the right/top triangle displays the partial correlations of all the study variables after controlling for sex and age; [2] PTSS, post-traumatic stress symptom; IA, Internet addiction; LS, life satisfaction; [3] ***p < 0.001; **p < 0.01; and *p < 0.05.
Univariate normality was assessed by examining skewness and kurtosis values for all the study variables across the three waves (44). For LS, skewness ranged from –0.930 to –0.822 and kurtosis from 0.117 to 0.423. For IA, skewness ranged from 1.384 to 1.668 and kurtosis from 1.574 to 2.943. For PTSS, skewness ranged from 1.239 to 1.576 and kurtosis from 1.373 to 2.884. All values fell within the commonly accepted thresholds for approximate normality (i.e., |skewness| < 2 and |kurtosis| < 7), indicating that the variables exhibited acceptable levels of univariate normality (44).
To assess measurement equivalence across the three waves, a series of increasingly restrictive confirmatory-factor-analysis (CFA) models were conducted using AMOS (44). Criteria for establishing measurement invariance included the ΔCFI ≤ 0.01 and ΔRMSEA ≤ 0.015 (44). The configural invariance model (Model 1), which allowed all parameters to vary across time, demonstrated an acceptable fit (χ²/df = 2.935, CFI = 0.977, RMSEA = 0.029), indicating that the factor structure was consistent across waves. The metric invariance model (Model 2), which constrained factor loadings to be equal over time, also fit the data well (ΔCFI = 0.004, ΔRMSEA = 0.002), suggesting loading invariance. The scalar invariance model (Model 3), which added equality constraints on item intercepts, resulted in minimal change in fit relative to the metric model (ΔCFI = 0.004, ΔRMSEA = 0.001), supporting scalar invariance. Finally, the residual invariance model (Model 4), which further constrained item residual variances, showed a small but acceptable decline in fit (ΔCFI = 0.012, ΔRMSEA = 0.005), indicating partial support for strict invariance. Overall, these findings provide evidence for longitudinal measurement invariance, supporting meaningful comparisons of the latent constructs across waves.
Harman’s one-factor CFA model showed poor fit to the data (CFI = 0.322, NFI = 0.319, TLI = 0.285, SRMR = 0.141, RMSEA = 0.150), indicating that common-method bias was unlikely to be a serious concern in this study. Moreover, repeated-measures analysis of variance was used to test of temporal differences in the study variables. PTSS showed a highly significant change over time (F = 45.90, p <.001), indicating substantial variation across the three waves. IA also demonstrated a significant time effect (F = 18.72, p <.001), although the magnitude of change was smaller than that of PTSS. LS showed a modest but still statistically significant change over time (F = 3.63, p <.05). Overall, these results support the use of a longitudinal mediation model for further analysis using SEM.
3.2 The complete longitudinal mediation model
A complete longitudinal mediation model was estimated to evaluate the links among PTSS, IA, and LS across the three waves by controlling for sex and age as covariates (see Figure 1). The model demonstrated good fit (χ2/df = 4.629, CFI = 0.952, NFI = 0.940, TLI = 0.947, SRMR = 0.058, RMSEA (90% CI) = 0.039 (0.038–0.041)).
Figure 1
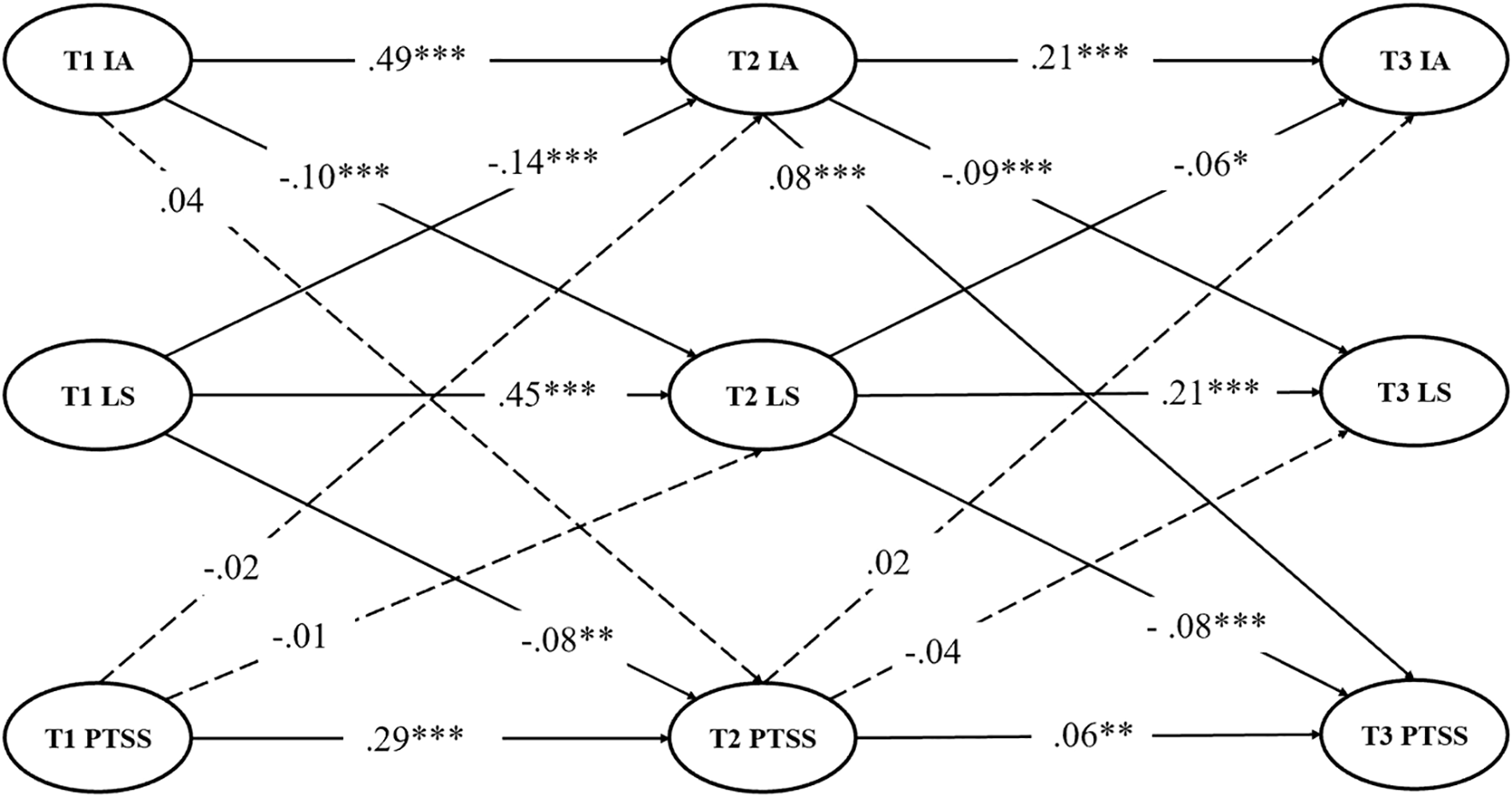
Complete longitudinal mediation model with standardized path coefficients. Dashed lines show insignificant paths. For conciseness, controlling variables (i.e., age and sex) and their factor loadings are not shown for the latent variables. IA, Internet addiction, LS, life satisfaction, PTSS, post-traumatic stress symptoms. ***p < 0.001, **p < 0.01, and *p < 0.05.
Results from the complete longitudinal mediation model revealed several significant pathways among the study variables across the three waves. Specifically, T1 IA positively predicted T2 IA (β = 0.492, SE = 0.031, p <.001) and negatively predicted T2 LS (β = –0.103, SE = 0.011, p <.001). T1 LS negatively predicted T2 IA (β = –0.142, SE = 0.146, p <.001) and positively predicted both T2 LS (β = 0.450, SE = 0.091, p <.001) and T2 PTSS (β = –0.081, SE = 0.214, p <.005). T1 PTSS positively predicted T2 PTSS (β = 0.285, SE = 0.022, p <.001). At the second wave, T2 IA positively predicted T3 IA (β = 0.205, SE = 0.024, p <.001), negatively predicted T3 LS (β = –0.087, SE = 0.009, p <.001), and positively predicted T3 PTSS (β = 0.083, SE = 0.016, p <.001). T2 LS negatively predicted T3 IA (β = –0.064, SE = 0.065, p <.001) and both positively predicted T3 LS (β = 0.213, SE = 0.026, p <.001) and negatively predicted T3 PTSS (β = –0.081, SE = 0.043, p <.001). T2 PTSS positively predicted T3 PTSS (β = 0.058, SE = 0.011, p <.005). Furthermore, results indicated some nonsignificant paths, including T1 IA to T2 PTSS (β = 0.043, SE = 0.046, p >.05), T1 PTSS to T2 IA (β = -0.016, SE = 0.013, p >.05) and T2 LS (β = -0.005, SE = 0.005, p >.05), and T2 PTSS to T3 IA (β = 0.020, SE = 0.017, p >.05) and T3 LS (β = -0.039, SE = 0.007, p >.05).
3.3 The clipped longitudinal mediation model
To enhance model conciseness, all nonsignificant paths were removed from the complete longitudinal mediation model, resulting in the clipped model (see Figure 2). The clipped model demonstrated a good goodness-of-fit (χ2/df = 4.587, CFI = 0.952, NFI = 0.939, TLI = 0.947, SRMR = 0.058, RMSEA (90% CI) = 0.039 (0.038–0.040)). The results revealed several significant relationships among IA, LS, and PTSS at adjacent time points. T1 IA significantly predicted T2 IA (β = 0.483, SE = 0.030, p <.001) and negatively predicted T2 LS (β = –0.10, SE = .010, p <.001). T1 LS negatively predicted T2 IA (β = –0.143, SE = 0.144, p <.001), positively predicted T2 LS (β = 0.453, SE = 0.092, p <.001), and negatively predicted T2 PTSS (β = -0.098, SE = 0.196, p <.001). T1 PTSS significantly predicted T2 PTSS (β = 0.296, SE = .021, p <.001). At the next time point, T2 IA significantly predicted T3 IA (β = 0.211, SE = .023, p <.001), negatively predicted T3 LLS (β = –0.094, SE = 0.009, p <.001), and positively predicted T3 PTSS (β = 0.081, SE = 0.015, p <.001). T2 LS negatively predicted T3 IA (β = –0.061, SE = 0.065, p = .013), positively predicted T3 LS (β = 0.218, SE = 0.026, p <.001), and negatively predicted T3 PTSS (β = –0.08, SE = 0.043, p <.001). T2 PTSS significantly predicted T3 PTSS (β = 0.045, SE = 0.009, p = .011). Overall, the results of the complete longitudinal mediation (Figure 1) and clipped (Figure 2) models revealed largely consistent findings regarding the relationships among the study variables across the three waves. Both models supported the same overall pattern of associations and underlying structure.
Figure 2
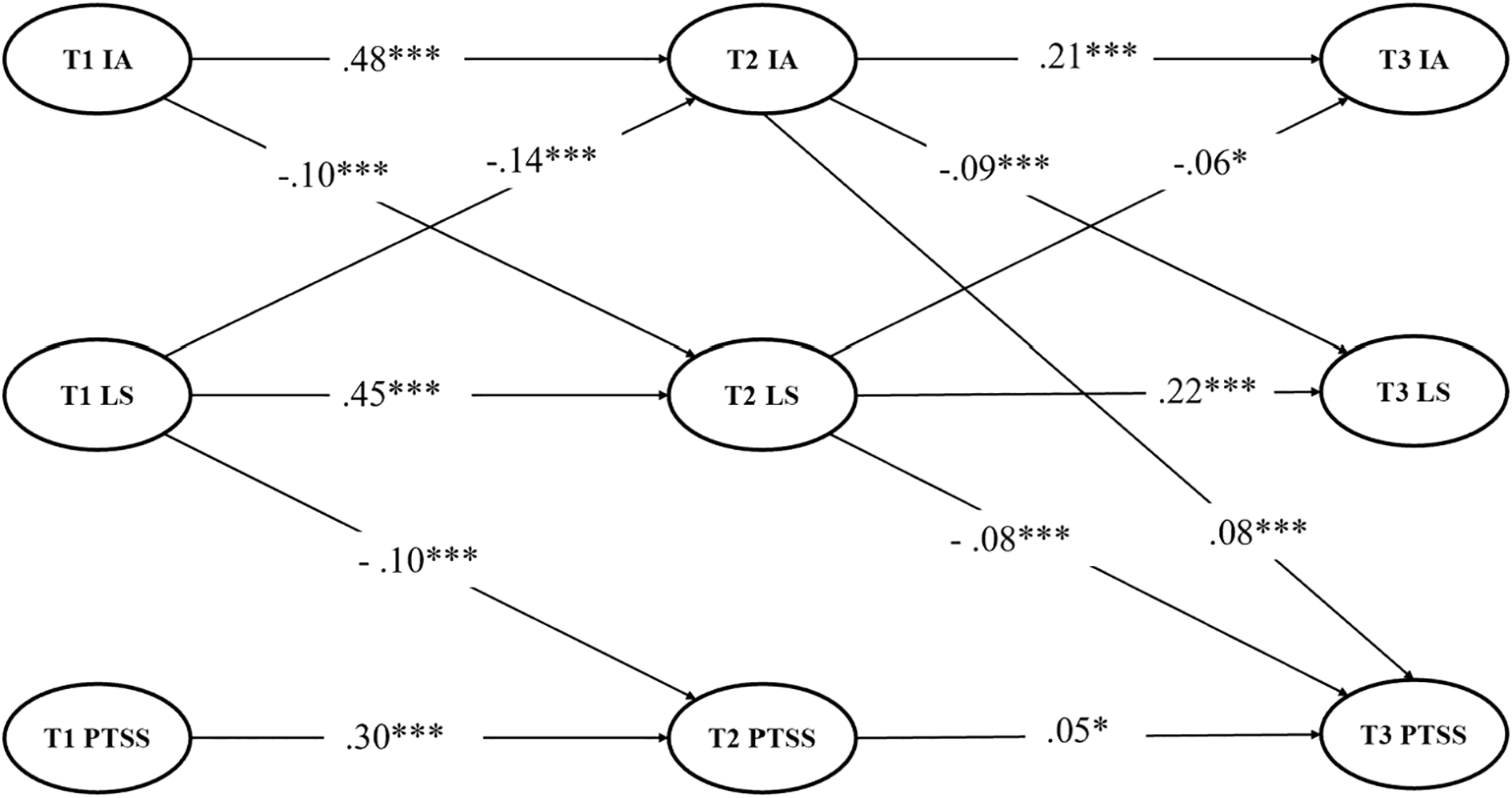
Clipped longitudinal mediation model with standardized path coefficients. Insignificant paths were removed in the model. For conciseness, controlling variables (i.e., age and sex) and their factor loadings are not shown for the latent variables. IA, Internet addiction; LS, life satisfaction; PTSS, post-traumatic stress symptoms. ***p <0.001, and *p < 0.05.
The results showed that T2 LS mediated the link between T1 IA and T3 PTSS [indirect effect (95% CI) = 0.047 (0.027–0.069)] and T2 IA mediated the relationship between T1 LS and T3 PTSS [indirect effect (95% CI) = –0.052 (–0.074 to –0.035)]. T2 LS mediated the association between T1 IA and T3 IA [indirect effect (95% CI) = 0.108 (0.080–0.141)]. T2 IA mediated the relationship between T1 LS and T3 LS [indirect effect (95% CI) = 0.112 (0.085–0.139)].
The results revealed consistent and significant bidirectional relationships among IA, LS, and PTSS across the three waves in the longitudinal mediation model. Specifically, at T1, LS was negatively correlated with both IA (r = –.445, p <.001) and PTSS (r = –.228, p <.001), while IA was positively correlated with PTSS (r = .272, p <.001). At T2, LS remained negatively correlated with IA (r = –.326, p <.001) and PTSS (r = –.133, p <.001), and IA was positively correlated with PTSS (r = .224, p <.001). Similarly, at T3, LS was negatively correlated with IA (r = –.349, p <.001) and PTSS (r = –.329, p <.001) while IA was positively correlated with PTSS (r = .321, p <.001). These findings demonstrate stable and reciprocal associations among the three study variables over time.
4 Discussion
This study employed a longitudinal mediation model to elucidate the relationships among PTSS, IA, and LS in a three-wave sample of Chinese children and young adolescents exposed to a major disaster. Our findings provided robust and large-sample evidence supporting the critical mediating role of LS as a potential mechanism linking early IA to subsequent PTSS in this population. Moreover, the results revealed that early LS significantly influenced prolonged PTSS through the mediating effect of IA following disaster exposure.
4.1 LS as a mediator between IA and PTSS
The results revealed that LS at the one-year follow-up significantly mediated the relationship between baseline IA and PTSS at the two-year follow-up. This finding supports the hypothesis and aligns with previous applications of self-determination theory (29, 30) and CBM (32, 33) in the context of IA. Specifically, higher IA levels in the early stages of a disaster may lead to reduced LS, which in turn increases the long-term risk of PTSS among Chinese children and early adolescents exposed to the disaster. This is consistent with prior research indicating an upward trend in IA among youth following traumatic events (4). Individuals with IA often experience discomfort and negative life changes, which may reduce their LS after a disaster (18). Lower LS can contribute to dissatisfaction with real life, deficits in quality of life, impaired social relationships, and disrupted life habits, ultimately heightening vulnerability to psychological problems (17). This result may also be explained by previous research showing that a higher degree of IA can impair individuals’ perceptions of LS derived from real-life social networks (45–47), thereby increasing the likelihood of long-term mental-health issues such as PTSS (48–50).
4.2 IA as a mediator between LS and PTSS
Interestingly, the findings revealed that the IA level at the one-year follow-up significantly mediated the relationship between baseline LS and PTSS at the two-year follow-up. This suggests that lower LS at the onset of a disaster might contribute to increased IA over time, which in turn heightens the risk of long-term psychological problems such as PTSS. Previous research has shown that disaster events such as the COVID-19 pandemic often disrupt daily life through factors such as social isolation, repeated testing, and regional lockdowns, all of which contribute to reduced LS (51–53). Furthermore, in the aftermath of a disaster, diminished LS may impair emotional regulation and increase vulnerability to stress, making individuals more likely to turn to the Internet as a form of avoidant coping (54). People with growing IA often rely on excessive online engagement to escape or numb distressing emotions in response to mounting real-life stressors (55–57). However, such avoidance hinders the emotional processing of trauma. When trauma remains unprocessed, it can become more deeply entrenched, leading to more severe PTSS (e.g., emotional numbing, intrusive thoughts, and hyperarousal) (58) following disasters. Additionally, although IA is frequently conceptualized as a mental-health outcome, our findings indicate that it could also function as a risk factor and mediator in the development of PTSS. This dual role aligns with prior evidence supporting the bidirectional relationships between IA and other mental-health problems (59, 60). Future research is suggested to further examine the underlying pathways through which IA longitudinally shapes psychological well-being in this dual role.
4.3 Bidirectional and mediating links involving PTSS, IA, and LS
Beyond the identified mediation pathways, the results revealed significant bidirectional associations between IA and PTSS across the three waves. These findings underscore the persistent, reciprocal relationship between IA and PTSS over time and are consistent with existing evidence highlighting strong intersections and potential comorbidity between the two [e.g (4, 14, 15).,]. Notably, no significant directed longitudinal effects were found from baseline PTSS to later LS or IA. One plausible explanation is that, within the framework of a two-year follow-up period, early PTSS may not exert a lasting impact sufficiently strong to influence long-term trajectories of subjective well-being or behavioral coping strategies, such as patterns of Internet use. Furthermore, children and early adolescents may possess greater psychological adaptability and benefit from external regulatory support (e.g., parental guidance), particularly during extended periods of home confinement and increased family time during the COVID-19 pandemic. Such support may buffer the enduring effects of trauma on daily functioning and LS (52). Additionally, both LS and Internet-use behaviors are shaped by a constellation of contextual factors, including peer relationships, academic pressures, and school dynamics, which may weaken the influence of PTSS over time (61–63). Collectively, these findings suggest that the longitudinal influence of PTSS on LS and IA may be governed by more complex and indirect mechanisms. Future research would benefit from examining potential mediators and moderators, such as personality traits, coping strategies, and family-relationship quality to further clarify these pathways (52, 64).
4.4 Strengths and limitations
Based on the large sample of disaster-exposed children and young adolescents and established measures, this three-wave study explored the associations among IA, LS, and PTSS from the perspective of a longitudinal mediation model. The different roles of LS in the mediating relationships indicated that IA and PTSS were closely linked but had independent patterns. These findings provide further evidence for the longitudinal mediated association mechanism between IA, LS, and PTSS. Notwithstanding these strengths, several limitations in the current study should be noted. First, the self-report questionnaire and assessment scales were used to evaluate the variables; this may lead to biased estimation because of social desirability, recall partiality, misinterpretation, or lack of insight (65). Future research may employ clinical diagnostic interviews (e.g., CAPS-5) or multiple-informant reports to improve measurement accuracy (66). Second, this study used a three-wave longitudinal design, which clarified temporal order and allowed tests of longitudinal mediation among IA, LS, and PTSS. The findings remain longitudinally correlational and predictive. However, since the longitudinal observational study was limited in the experimental conditions, such as manipulation and randomization, future experimental or intervention studies are needed to provide more conclusive causal evidence (67). Finally, these findings may not be generalizable to other disaster-exposed populations or to individuals who have experienced different types of trauma. Future research is recommended to investigate the causal relationships among the study variables across diverse populations and trauma exposures.
4.5 Practical implications
The present findings emphasize the protective role of LS in buffering the long-term negative influence of IA and PTSS, the potentially adverse effect of inchoate IA symptoms on LS, and their impact on long-term psychological health among children and young adolescents exposed to disasters. These results highlight the need for developing psychological intervention programs that strengthen positive life forces, enhance social support, and promote adaptive coping strategies in disaster-affected youth (68, 69). Customized interventions focusing on LS improvement may increase resilience and reduce excessive reliance on the virtual world following traumatic experiences. For example, mindfulness-based interventions (70), solution-focused brief therapy (71), and positive psychology interventions (72) have shown promise in boosting positive emotions, meaning, and LS in the aftermath of disasters. Policymakers and practitioners should consider incorporating these strategies into pre- or post-disaster support systems for vulnerable children and young people.
4.6 Conclusions
This exploratory study revealed that life satisfaction plays a vitally protective role by mediating the influence of early Internet addiction on long-term psychological outcomes. Moreover, Internet addiction mediated the links between earlier life satisfaction and later PTSS, indicating that both enhancing life satisfaction and reducing problematic Internet use are critical for mitigating mental symptoms among disaster-exposed youth. Future research should investigate these pathways by using longer-term dynamic tracking and multi-method approaches to elucidate causal mechanisms and aid the development of targeted interventions.
Statements
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statement
This study involving human participants was reviewed and approved by the Research Ethics Committee of Sichuan University (No. K2020025 and No. KS2022913). The studies were conducted in accordance with the local legislation and institutional requirements. Written informed consent for participation was not required from the participants or the participants’ legal guardians/next of kin in accordance with the national legislation and institutional requirements.
Author contributions
WS: Funding acquisition, Resources, Writing – review & editing, Conceptualization, Software, Writing – original draft, Data curation, Methodology, Formal Analysis, Validation, Visualization, Investigation. GY: Writing – review & editing, Investigation, Conceptualization. ZC: Investigation, Writing – review & editing, Data curation, Project administration. YT: Software, Project administration, Writing – review & editing. LJ: Project administration, Writing – review & editing, Supervision. LZ: Resources, Project administration, Writing – review & editing, Conceptualization, Methodology, Supervision.
Funding
The author(s) declare financial support was received for the research and/or publication of this article. This work was supported by the Humanities and Social Sciences Youth Foundation, Ministry of Education of the People’s Republic China (22YJC190019).
Acknowledgments
We gratefully acknowledge the support of the International Visiting Program for Excellent Young Scholars of SCU.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Generative AI statement
The author(s) declare that no Generative AI was used in the creation of this manuscript.
Any alternative text (alt text) provided alongside figures in this article has been generated by Frontiers with the support of artificial intelligence and reasonable efforts have been made to ensure accuracy, including review by the authors wherever possible. If you identify any issues, please contact us.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1
Lam LT . Risk factors of Internet addiction and the health effect of internet addiction on adolescents: a systematic review of longitudinal and prospective studies. Curr Psychiatry Rep. (2014) 16:1–9. doi: 10.1007/s11920-014-0508-2
2
Kinser PA Moyer S Jones HA Jallo N Popoola A Thacker L et al . Perceptions of the Mamma Mia program, an internet-based prevention strategy for perinatal depression symptoms. PloS Ment Health. (2025) 2:e0000138. doi: 10.1371/journal.pmen.0000138
3
Ozturk FO Ayaz-Alkaya S . Internet addiction and psychosocial problems among adolescents during the COVID-19 pandemic: A cross-sectional study. Arch Psychiatr Nurs. (2021) 35:595–601. doi: 10.1016/j.apnu.2021.08.007
4
Shi J Huang H Wang Y . Comorbidity of Internet addiction and post-traumatic stress disorder among adolescents during the COVID-19 pandemic: A network analysis. Addict Res Theory. (2024) 32:22–33. doi: 10.1080/16066359.2023.2288820
5
Yang X Wu X Qi J Zhou X . Posttraumatic stress symptoms, adversity belief, and internet addiction in adolescents who experienced a major earthquake. Curr Psychol. (2022) 41(5):3013–20. doi: 10.1007/s12144-020-00816-y
6
Kotrla Topić M Topić R Džamonja Ignjatović T . Association between problematic Internet use and specific Internet activities and COVID-19- and earthquake-related stress, anxiety, and depression symptoms among Croatian young adults. Comput Hum Behav. (2023) 140:107610. doi: 10.1016/j.chb.2022.107610
7
Fumero A Marrero RJ Voltes D Peñate W . Personal and social factors involved in internet addiction among adolescents: A meta-analysis. Comput Hum Behav. (2018) 86:387–400. doi: 10.1016/j.chb.2018.05.005
8
Dong H Yang F Lu X Hao W . Internet addiction and related psychological factors among children and adolescents in China during the coronavirus disease 2019 (COVID-19) epidemic. Front Psychiatry. (2020) 11:751. doi: 10.3389/fpsyt.2020.00751
9
Sehlikoğlu Ş Bekircan E Gündüz A . Impact of the February 6, 2023, Turkey earthquake on post-traumatic stress disorder, internet addiction and insomnia: A cross-sectional study. Int J Soc Psychiatry. (2025) 71(2):414–25. doi: 10.1177/00207640241294203
10
American Psychiatric Association, APA . Diagnostic and statistical manual of mental disorders, 5th ed. Washington, DC: American Psychiatric Association (2013). doi: 10.1176/appi.books.9780890425596.
11
Contractor AA Weiss NH Tull MT Elhai JD . PTSD’s relation with problematic smartphone use: Mediating role of process-oriented smartphone use. Soc Sci Comput Rev. (2019) . 37:333–46. doi: 10.1177/0894439318770745
12
Evren B Dalbudak E Evren C Ozen S . The relationship of internet addiction symptom severity with posttraumatic stress disorder symptoms and impulsivity among Turkish university students. Psychiatry Clin Psychopharmacol. (2019) 29:83–9. doi: 10.1080/24750573.2018.1505422
13
López-Muñoz F Otero F . Social media addiction and PTSD in military veterans: A qualitative perspective. J Behav Addict Trauma. (2023) 5:45–58. doi: 10.1016/j.jbat.2023.100007
14
Lee JY Kim SW Kang HJ Kim SY Bae KY Kim JM et al . Relationship between problematic internet use and post-traumatic stress disorder symptoms among students following the Sewol ferry disaster in South Korea. Psychiatry Invest. (2017) 14:871–5. doi: 10.4306/pi.2017.14.6.871
15
Lee SY Lee HK Choi JS . The association between problematic internet use and post-traumatic stress disorder symptoms among students who survived the Sewol ferry disaster in South Korea. Psychiatry Invest. (2017) 14:198–203. doi: 10.4306/pi.2017.14.2.198
16
Zhang D Wu XC Tian YX . The relationship between posttraumatic stress disorder symptoms and internet addiction symptoms in adolescents: the mediating role of sensitivity to punishment stimuli and loneliness and the moderating role of gender. J psychol Sci. (2021) 44:1134–40. doi: 10.16719/j.cnki.issn1001-3701.2021.05.011
17
Long Y Guo B Xu Y Ren Z Newman MG Zhang L . The associations between PTSD symptom clusters, insomnia, and depressive symptoms in Chinese adolescents with low and high levels of internet addiction: A cross-lagged network analysis. psychol Trauma: Theory Research Practice Policy. (2025), 1–9. doi: 10.1037/tra0001570
18
Xiong A Liao S Luo B Luo S Tong Y Li Z . Associations between problematic internet use, life satisfaction, and deliberate self-harm among Chinese adolescents: A multi-centered longitudinal study. Addictive Behav. (2023) 147:107808. doi: 10.1016/j.addbeh.2023.107808
19
Schlechter P Hoppen TH Morina N . Associations among posttraumatic stress disorder symptoms, life satisfaction, and well-being comparisons: A longitudinal investigation. J Traumatic Stress. (2024) 37:448–59. doi: 10.1002/jts.23018
20
Diener ED Emmons RA Larsen RJ Griffin S . The satisfaction with life scale. J Pers Assess. (1985) 49:71–5. doi: 10.1207/s15327752jpa4901_13
21
Noroozi F Hassanipour S Eftekharian F Eisapareh K Kaveh MH . Internet addiction effect on quality of life: A systematic review and meta-analysis. Sci World J. (2021) 19:1–12. doi: 10.1186/s12955-021-01898-0
22
Peris M de la Barrera U Schoeps K Montoya-Castilla I . Psychological risk factors that predict social networking and internet addiction in adolescents. Int J Environ Res Public Health. (2020) 17:586–91. doi: 10.1089/cyber.2014.0326
23
Zaragoza SA Salgado S Shao Z Berntsen D . Younger adults report more distress and less well-being: A cross-cultural study of event centrality, depression, post-traumatic stress disorder and life satisfaction. Appl Cogn Psychol. (2020) 34:1180–96. doi: 10.1002/acp.3707
24
Karatzias T Chouliara Z Power K Brown K Begum M McGoldrick T et al . Life satisfaction in people with post-traumatic stress disorder. J Ment Health. (2013) 22:501–8. doi: 10.3109/09638237.2013.819418
25
Giacco D Matanov A Priebe S . Symptoms and subjective quality of life in post-traumatic stress disorder: a longitudinal study. PloS One. (2013) 8:e60991. doi: 10.1371/journal.pone.0060991
26
Ferrari Junior GJ Silva ABD Meneghetti A Leite CR Brust C Moreira GC et al . Relationships between internet addiction, quality of life and sleep problems: a structural equation modeling analysis. Jornal Pediatria. (2024) 100:283–8. doi: 10.1016/j.jped.2023.09.015
27
Luengo-González R Noriega-Matanza MC Espín-Lorite EJ García-Sastre MM Rodríguez-Rojo IC Cuesta-Lozano D et al . The role of life satisfaction in the association between problematic technology use and anxiety in children and adolescents during the COVID-19 pandemic. Int J Ment Health Nurs. (2023) 32:212–22. doi: 10.1111/inm.13077
28
Besser A Neria Y . PTSD symptoms, satisfaction with life, and prejudicial attitudes toward the adversary among Israeli civilians exposed to ongoing missile attacks. J Traumatic Stress: Off Publ Int Soc Traumatic Stress Stud. (2009) 22:268–75. doi: 10.1002/jts.20420
29
Ryan RM Deci EL . Self-determination theory and the facilitation of intrinsic motivation, social development, and well-being. Am Psychol. (2000) 55:68. doi: 10.1037/0003-066X.55.1.68
30
Li D Zhang W Li X Zhou Y Zhao L Wang Y . Stressful life events and adolescent Internet addiction: The mediating role of psychological needs satisfaction and the moderating role of coping style. Comput Hum Behav. (2016) 63:408–15. doi: 10.1016/j.chb.2016.05.070
31
Chen CY Chang SL . Moderating effects of information-oriented versus escapism-oriented motivations on the relationship between psychological well-being and problematic use of video game live-streaming services. J Behav Addict. (2019) 8:564–73. doi: 10.1556/2006.8.2019.34
32
Davis RA . A cognitive-behavioral model of pathological Internet use. Comput Hum Behav. (2001) 17:187–95. doi: 10.1016/S0747-5632(00)00041-8
33
Li R Fu W Liang Y Huang S Xu M Tu R . Exploring the relationship between resilience and internet addiction in Chinese college students: the mediating roles of life satisfaction and loneliness. Acta Psychologica. (2024) 248:104405. doi: 10.1016/j.actpsy.2024.104405
34
Baumeister RF Leary MR . The need to belong: Desire for interpersonal attachments as a fundamental human motivation. psychol Bull. (1995) 117:497–529. doi: 10.1037/0033-2909.117.3.497
35
Koivumaa-Honkanen H Honkanen R Viinamaeki H Heikkilae K Kaprio J Koskenvuo M . Life satisfaction and suicide: A 20-year follow-up study. Am J Psychiatry. (2001) 158:433–9. doi: 10.1176/appi.ajp.158.3.433
36
Sun RC Shek DT . Positive youth development, life satisfaction and problem behaviour among Chinese adolescents in Hong Kong: A replication. Soc Indic Res. (2012) 105:541–59. doi: 10.1007/s11205-011-9786-9
37
Zhao L Shek DT Zou K Lei Y Jia P . Cohort profile: Chengdu positive child development (CPCD) survey. Int J Epidemiol. (2022) 51:e95–107. doi: 10.1093/ije/dyab237
38
Deeba F Rapee RM Prvan T . Psychometric properties of the Children’s Revised Impact of Events Scale (CRIES) with Bangladeshi children and adolescents. Peer J. (2014) 2:e536. doi: 10.7717/peerj.536
39
Lau JT Yeung NC Yu XN Zhang J Mak WW Lui WW . Validation of the Chinese version of the Children's Revised Impact of Event Scale (CRIES) among Chinese adolescents in the aftermath of the Sichuan Earthquake in 2008. Compr Psychiatry. (2013) 54:83–90. doi: 10.1016/j.comppsych.2012.06.007
40
Young KS . Internet addiction test (IAT) [Database record. APA PsycTests. (1998) 1(3):237–44. doi: 10.1037/t41898-000
41
Lai CM Mak KK Watanabe H Ang RP Pang JS Ho RC . Psychometric properties of the internet addiction test in Chinese adolescents. J Pediatr Psychol. (2013) 38:794–807. doi: 10.1093/jpepsy/jst022
42
Bai X Wu C Zheng R Ren X . The psychometric evaluation of the Satisfaction with Life Scale using a nationally representative sample of China. J Happiness Stud. (2011) 12:183–97. doi: 10.1007/s10902-010-9186-x
43
Jose PE . The merits of using longitudinal mediation. Educ Psychol. (2016) 51:331–41. doi: 10.1080/00461520.2016.1207175
44
West SG Taylor AB Wu W . Model fit and modelselection in structural equation modeling. In: HoyleR, editor. Handbook of structural equation modeling. Guil-ford Press, New York (2012). p. 209–31.
45
Błachnio A Przepiorka A Benvenuti M Mazzoni E Seidman G . Relations between Facebook intrusion, Internet addiction, life satisfaction, and self-esteem: a study in Italy and the USA. Int J Ment Health Addict. (2019) 17:793–805. doi: 10.1007/s11469-018-0038-y
46
Telef BB . Investigating the relationship among internet addiction, positive and negative affects, and life satisfaction in Turkish adolescents. Int J Progressive Educ. (2016) 12:128–35.
47
Sayili U Pirdal BZ Kara B Acar N Camcioglu E Yilmaz E et al . Internet addiction and social media addiction in medical faculty students: prevalence, related factors, and association with life satisfaction. J Community Health. (2023) 48:189–98. doi: 10.1007/s10900-022-01153-w
48
Deng AP Wang C Cai J Deng ZY Mu YF Song HJ et al . Effects of internet addiction and academic satisfaction on mental health among college students after the lifting of COVID-19 restrictions in China. Front Psychiatry. (2023) 14:1243619. doi: 10.3389/fpsyt.2023.1243619
49
Cao H Sun Y Wan Y Hao J Tao F . Problematic Internet use in Chinese adolescents and its relation to psychosomatic symptoms and life satisfaction. BMC Public Health. (2011) 11:1–8. doi: 10.1186/1471-2458-11-802
50
Veisani Y Jalilian Z Mohamadian F . Relationship between internet addiction and mental health in adolescents. J Educ Health Promotion. (2020) 9:303. doi: 10.4103/jehp.jehp_362_20
51
Shi W Yuan GF Hall BJ Liu X Su Y Zhao L et al . Mental disorders and emotional competence among Chinese adolescents before and during COVID-19 Pandemic: A longitudinal mediation model. Front Public Health. (2021) 9:767004. doi: 10.3389/fpubh.2021.767004
52
Shi W Yuan GF Hall BJ Jia P Zhao L . Chinese adolescents’ depression, anxiety, and family mutuality before and after COVID-19 lockdowns: Longitudinal cross-lagged relations. Family Relations. (2022) 72:77–91. doi: 10.1111/fare.12761
53
Von Soest T Bakken A Pedersen W Sletten MA . Life satisfaction among adolescents before and during the COVID-19 pandemic. Tidsskrift Den norske legeforening. (2020) 140(10):1–13. doi: 10.4045/tidsskr.20.0437
54
Gao W Chen Z . Pathological psychological mechanism and comprehensive psychological intervention of Internet addiction. Adv psychol Sci. (2006) 14:596–603. Available at: https://journal.psych.ac.cn/adps/EN/.
55
Hsieh YP Shen ACT Wei HS Feng JY Huang SCY Hwa HL . Associations between child maltreatment, PTSD, and internet addiction among Taiwanese students. Comput Hum Behav. (2016) 56:209–14. doi: 10.1016/j.chb.2015.11.048
56
Bozoglan B Demirer V Sahin I . Loneliness, self-esteem, and life satisfaction as predictors of Internet addiction: A cross-sectional study among Turkish university students. Scandinavian J Psychol. (2013) 54:313–9. doi: 10.1111/sjop.12049
57
Şahin C . Examination of the relationship between life satisfaction level and internet addiction of the students in guidance and psychological counseling department. Int J Contemp Educ Stud. (2016) . 2:1–13.
58
Shi W Hall BJ . Trajectories of posttraumatic stress symptoms among young adults exposed to a typhoon: a three-wave longitudinal study. Int J Public Health. (2023) 67:1605380. doi: 10.3389/ijph.2023.1605380
59
Lam LT . Risk factors of internet addiction and the health effect of internet addiction on adolescents: a systematic review of longitudinal and prospective studies. Curr Psychiatry Rep. (2014) 16:508. doi: 10.1007/s11920-014-0508-2
60
Wartberg L Kriston L Zieglmeier M Lincoln T Kammerl R . A longitudinal study on psychosocial causes and consequences of internet gaming disorder in adolescence. psychol Med. (2019) 49:287–94. doi: 10.1017/S003329171800082X
61
Servidio R Gentile A Boca S . The mediational role of coping strategies in the relationship between self-esteem and risk of internet addiction. Europe's J Psychol. (2018) 14:176–87. doi: 10.5964/ejop.v14i1.1449
62
Wu XS Zhang ZH Zhao F Wang WJ Li YF Bi L . Prevalence of Internet addiction and its association with social support and other related factors among adolescents in China. J Adolescence. (2016) 52:103–11. doi: 10.1016/j.adolescence.2016.07.012
63
Woodward MJ Eddinger J Henschel AV Dodson TS Tran HN Beck JG . Social support, posttraumatic cognitions, and PTSD: The influence of family, friends, and a close other in an interpersonal and non-interpersonal trauma group. J Anxiety Disord. (2015) 35:60–7. doi: 10.1016/j.janxdis.2015.09.002
64
Yuan G Shi W Lowe S Chang K Jackson T Hall BJ . Associations between posttraumatic stress symptoms, perceived social support and psychological distress among disaster-exposed Chinese young adults: A three-wave longitudinal mediation model. J Psychiatr Res. (2021) 137:491–7. doi: 10.1016/j.jpsychires.2021.03.036
65
Paulhus DL Vazire S . The self-report method. In: RobinsRWFraleyRCKruegerRF, editors. Handbook of research methods in personality psychology. Guilford Press, New York (2007). p. 224–39.
66
Weather FF Blake DD Schnurr PP Kaloupek DG Marx BP Keane TM . The Clinician-administered PTSD scale for DSM-5 (CAPS-5). Boston, MA: National Center for PTSD, U.S. Department of Veterans Affairs. (2013).
67
Hayes AF . Introduction to mediation, moderation, and conditional process analysis: A regression-based approach. 2nd ed. New York: The Guilford Press (2017).
68
Meule A Voderholzer U . Life satisfaction in persons with mental disorders. Qual Life Res. (2020) . 29:3043–52. doi: 10.1007/s11136-020-02556-9
69
Wu Z Shi W Chen Y Lowe SR Liu J . Help-seeking preferences and influencing factors among Chinese nurses exposed to COVID-19: a person-centered approach. J Community Health Nurs. (2024) 41:273–85. doi: 10.1080/07370016.2024.2314076
70
Müller L Rapoport O Rahe M . Mindfulness meditation improves mental health in flood survivors and disaster volunteers: A randomized wait-list controlled trial. Mindfulness. (2024) 15(11):2750–64. doi: 10.1007/s12671-024-02467-7
71
Steinbrecher E Jordan SS Turns B . Providing immediate hope to survivors of natural disasters: A miracle question intervention. Am J Family Ther. (2020) 49:204–19. doi: 10.1080/01926187.2020.1789899
72
Lotzin A Franc de Pommereau A Laskowsky I . Promoting recovery from disasters, pandemics, and trauma: a systematic review of brief psychological interventions to reduce distress in adults, children, and adolescents. Int J Environ Res Public Health. (2023) 20:5339. doi: 10.3390/ijerph20075339
Summary
Keywords
Internet addiction, life satisfaction, post-traumatic stress symptoms, children, young adolescents
Citation
Shi W, Yuan G, Chen Z, Tan Y, Jiang L and Zhao L (2025) Associations between Internet addiction, life satisfaction, and post-traumatic stress symptoms among disaster-exposed children and early adolescents: a three-wave longitudinal study. Front. Psychiatry 16:1628873. doi: 10.3389/fpsyt.2025.1628873
Received
14 May 2025
Accepted
30 September 2025
Published
24 October 2025
Volume
16 - 2025
Edited by
Yu Tian, Qingdao University of Science and Technology, China
Reviewed by
Peng Wang, Shandong Normal University, China
Chang Peng, Chongqing Medical University, China
Updates
Copyright
© 2025 Shi, Yuan, Chen, Tan, Jiang and Zhao.
This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Li Zhao, zhaoli@scu.edu.cn
Disclaimer
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.