 Hai-Ying Yang1*
Hai-Ying Yang1* Li-Hong Sun2
Li-Hong Sun2- 1School of Physical Education, Southwest Jiaotong University, Chengdu, Sichuan, China
- 2School of Physical Education, Hubei Second Normal University, Wuhan, Hubei, China
Background: Adolescents faced increased psychological distress during the COVID-19 pandemic. While prior research suggests physical activity (PA) may mitigate depression and anxiety, findings have been inconsistent and rarely focus on adolescents during prolonged lockdowns. This study addresses this gap by evaluating the association between daily PA duration and mental health outcomes among Chinese adolescents during the pandemic.
Methods: A cross-sectional online survey was conducted from June 1–30, 2020, among 1,142 adolescents aged 11–18 years in Pidu District, Chengdu City, China. Depressive and anxiety symptoms were assessed using the Center for Epidemiological Studies Depression Scale for Children (CES-DC) and the Generalized Anxiety Disorder 7-item scale (GAD-7), respectively. PA was self-reported and categorized as <30, 30–60, and >60 minutes/day. Logistic regression was used to estimate odds ratios (ORs) for depression (CES-DC >15) and anxiety (GAD-7 ≥5), using ≥30 min/day as the reference.
Results: Depressive symptoms were reported by 40.7% of participants and anxiety symptoms by 24.1%. Compared to adolescents with ≥30 min/day of PA, those with <30 min/day had significantly higher odds of depression (OR = 1.722, 95% CI: 1.342–2.226) and anxiety (OR = 1.653, 95% CI: 1.299–2.521). Additional independent predictors included female sex, sleep duration <6 hours, and self-reported decline in learning efficiency.
Conclusions: Insufficient PA (<30 min/day) was independently associated with elevated depression and anxiety symptoms in adolescents during the pandemic. These findings support promoting ≥30 minutes of daily PA as a scalable, non-pharmacological strategy to protect adolescent mental health during public health emergencies.
1 Introduction
Adolescents have been particularly vulnerable to the psychological impacts of the COVID-19 pandemic, with significant increases in symptoms of depression and anxiety (1, 2). While physical activity (PA) has long been proposed as a protective factor against mental health issues, the pandemic has drastically altered the types and amounts of PA that are feasible for adolescents (3, 4). Before the pandemic, common forms of PA such as team sports, physical education, and outdoor group activities played a major role in adolescent well-being (5, 6). However, during the pandemic, restrictions limited access to gyms, sports teams, and recreational spaces, making home-based activities like bodyweight exercises, yoga, and walking crucial alternatives (7–9). These changes may have influenced the overall duration and intensity of PA, potentially altering its effects on mental health.
Recent literature underscores the mental health benefits of physical activity (PA), particularly for adolescents experiencing elevated psychological distress during the COVID-19 pandemic. Systematic reviews by Li et al. (10) and Wolf et al. (11) demonstrate that higher levels of moderate-to-vigorous PA are associated with lower rates of depression and anxiety. Samji et al. (12) further identify adolescents—especially females and older youth—as disproportionately affected by pandemic-related disruptions, highlighting PA as a potential protective factor. While intervention studies such as Erdoğan et al. (13) suggest that structured PA (e.g., yoga) may improve psychological outcomes in subgroups like obese adolescents, their findings are limited in scope and generalizability. However, several critical gaps remain. Existing studies often aggregate broad age ranges, obscuring insights specific to adolescents. Most do not differentiate between varying durations of PA or establish clear dose-response thresholds under conditions of social isolation. Additionally, few studies have examined these associations during prolonged lockdown periods, when routine PA may be severely constrained and mental health impacts intensified.
The present study addresses these gaps by focusing on a large cohort of Chinese adolescents during the early COVID-19 lockdown. By stratifying daily PA into three distinct categories and analyzing its association with depression and anxiety symptoms—while adjusting for key confounders such as gender, sleep duration, and learning efficiency—this study offers new evidence on the dose-dependent protective effects of PA. These findings contribute to a more nuanced understanding of how daily physical activity may buffer adolescent mental health during global crises.
2 Methods
2.1 Study design
The data for this study were collected from a cross-sectional online survey conducted between June 1, 2020, and June 30, 2020, using the “Wenjuanxing” platform via WeChat. The participants were adolescents aged 11 to 18 years who were enrolled in middle or high school in our city and resided there during the COVID-19 pandemic. Each mobile phone number was permitted to participate only once in the survey. A total of 1142 middle and high school students were included in the analysis. The age range of the participants was 11 to 18 years, with a mean age of 15.3 ± 1.8 years. Prior to participation, all participants and their guardians electronically signed an informed consent form. This study was conducted in strict accordance with the ethical principles outlined in the Declaration of Helsinki and was approved by the institutional review board of our institution. The questionnaire did not collect names or other personally identifiable information and was fully anonymous. The questionnaire was anonymous, and no personally identifiable information was collected. All data were used solely for research purposes by the study team.
2.2 Survey methodology and content
his study employed an online survey to collect data on the demographic characteristics, clinical features, and lifestyle habits of adolescents, as well as to assess their levels of depression and anxiety during the COVID-19 pandemic. The survey consisted of several key sections designed to collect comprehensive data on the study participants.
1. Demographic Information: This section gathered basic demographic details, including the participant’s age, gender, residential area, grade level, and school type.
2. Study and Lifestyle Habits: The survey examined participants’ daily habits over the past week, including average sleep duration, study time, changes in study efficiency, and the time spent engaging in physical activity each day. PA was assessed with a single self-report item adapted from descriptors used in the International Physical Activity Questionnaire–Short Form (IPAQ−SF). Participants were asked: “During the past 7 days, on average how many minutes per day did you spend doing moderate−to−vigorous physical activities (e.g., brisk walking, running, cycling, ball games, or other sports) that made you breathe somewhat harder or much harder than normal?” Respondents entered a numeric value (minutes/day). To anchor intensity, examples were provided and light activities (e.g., casual walking, household chores) were explicitly excluded. Based on a priori cut−points, daily PA was categorized as <30 min, 30–60 min, and >60 min. These categories were selected to distinguish clearly insufficient PA (<30 min/day), sub−recommended levels (30–60 min/day), and meeting/exceeding the widely promoted target of ≥60 min/day for adolescents.
3. Depression Assessment: The Center for Epidemiological Studies Depression Scale for Children (CES-DC) was used to assess depressive symptoms in adolescents aged 6 to 17 years. The CES-DC is a brief, structured self-assessment tool designed to measure depressive symptoms experienced in the past week. It includes 20 items across four dimensions: depressive mood, positive mood (reverse scored), somatic symptoms, and interpersonal relationships. Each item is scored on a 0–3 scale, with 0 indicating “not at all,” 1 indicating “a little,” 2 indicating “sometimes,” and 3 indicating “most of the time.” The total score ranges from 0 to 60, with a score above 15 indicating the presence of depressive symptoms, and a score of 20 or greater suggesting significant depressive symptoms.
4. Anxiety Assessment: The Generalized Anxiety Disorder 7-Item Scale (GAD-7) was employed to assess anxiety symptoms in participants over the past two weeks. The GAD-7 is a concise self-report tool consisting of 7 items that evaluate the frequency of anxiety symptoms. A 4-point scoring system is used: 0 for “not at all,” 1 for “several days,” 2 for “more than half the days,” and 3 for “nearly every day.” A total score of 5 or higher suggests the presence of anxiety symptoms. Higher scores indicate more severe anxiety, with thresholds of 5, 10, and 15 denoting mild, moderate, and severe anxiety, respectively.
2.3 Quality control
To ensure the accuracy and reliability of the data collected, several quality control measures were implemented throughout the study process. The survey was administered via the “Wenjuanxing” platform, which provided a secure, user-friendly interface for respondents. The following quality control strategies were applied:
1. Exclusion of Inconsistent Data: To ensure data validity, responses containing obvious logical inconsistencies were excluded. This included participants whose answers to certain questions were contradictory or those who completed the survey in an abnormally short amount of time. Specifically, any survey with a completion time of less than 120 seconds was removed, as this suggested insufficient attention to the questions.
2. One Response Per Participant: Each mobile phone number was permitted to participate only once in the survey. This helped to prevent duplicate entries and ensured that the sample was representative of individual adolescents rather than repeated submissions from the same participants.
3. Age Range Verification: Only adolescents aged 11 to 18 years were included in the study. Responses from individuals outside of this age range were excluded to maintain the focus of the study on the target population. This age filter was strictly enforced during the data cleaning process.
4. Data Monitoring: Regular monitoring of survey responses was conducted throughout the data collection period to identify any potential issues with the survey or platform. This allowed for real-time corrections and ensured that data collection proceeded smoothly.
2.4 Statistical analysis
Data were analyzed using SPSS version 28.0. The data were initially categorized into quantitative and categorical variables, and normality tests were conducted to assess the distribution of quantitative data. For normally distributed quantitative data, inter-group comparisons were performed using independent sample t-tests, and the results were reported as mean ± standard deviation (SD). Categorical variables were presented as frequencies and percentages. The Chi-square (χ²) test was used to examine associations or independence between categorical variables. In cases where the assumptions for the Chi-square test were not met, Fisher’s exact test was employed as an alternative. Multivariate associations were explored using logistic regression analysis to identify factors associated with depressive or anxiety symptoms. For descriptive analyses, PA was treated as a three−level categorical variable (<30, 30–60, >60 min/day). For multivariable logistic regression, PA was dichotomized as <30 min/day versus ≥30 min/day to improve model stability and interpretability; the ≥30 min/day group served as the reference. All statistical tests were two-tailed, and a p-value of less than 0.05 was considered statistically significant.
3 Results
3.1 Demographic and clinical characteristics
Among the 1,142 adolescents included in the analysis, 465 participants (40.7%) had CES-DC scores >15, indicating depressive symptoms, while 357 (31.3%) scored ≥20, suggesting more severe depressive states. A total of 275 participants (24.1%) met the threshold for anxiety symptoms, defined as GAD-7 scores ≥5. Comparative analyses revealed several significant associations between demographic/clinical characteristics and the presence of depression and anxiety. Higher symptom prevalence was observed among older adolescents (15–18 years), females, and senior high school students (all P < 0.05). In contrast, school type and adherence to COVID-19 protective measures were not significantly associated with mental health status. Regarding behavioral factors, short sleep duration (<6 hours per night) was strongly associated with both depressive and anxiety symptoms (P < 0.001 for both). Adolescents reporting decreased learning efficiency also showed significantly higher rates of depression and anxiety compared to their peers (P < 0.001). Similarly, daily physical activity of less than 30 minutes was significantly associated with increased prevalence of both depression (P < 0.001) and anxiety (P = 0.009). No significant associations were found between daily study time and either mental health outcome (P > 0.05) (Table 1).
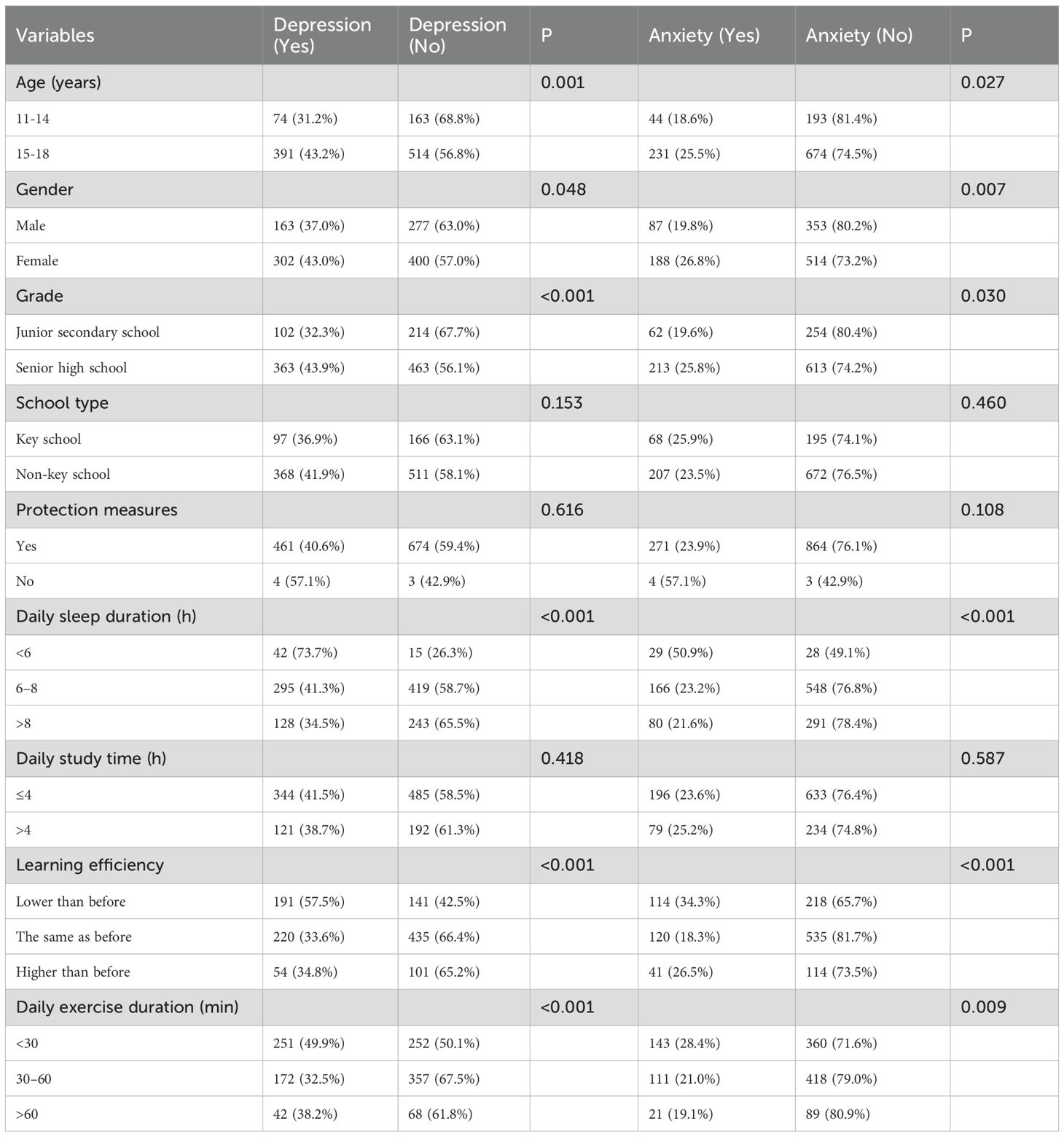
Table 1. Demographic and clinical characteristics of the study participants with depression and anxiety status.
3.2 Multivariate logistic regression analysis of correlates of depression
Multivariate logistic regression was conducted to identify independent factors associated with depression, after controlling for potential confounders. Depression was defined as a CES-DC score >15, and non-depression as a score ≤15. Several variables were significantly associated with depression. Male participants had lower odds of depression compared to females (OR = 0.765, 95% CI: 0.588–0.995, P = 0.049). Adolescents who reported sleeping less than 6 hours per night were at significantly higher risk of depression than those with longer sleep durations (OR = 4.021, 95% CI: 2.152–7.534, P < 0.001). Reduced learning efficiency was also a strong correlate of depression. Participants who perceived their learning efficiency to be lower than before the pandemic had significantly increased odds of depression (OR = 2.853, 95% CI: 2.153–3.771, P < 0.001). In addition, adolescents who engaged in <30 minutes of daily physical activity had higher odds of depression compared to those with ≥30 minutes per day (OR = 1.722, 95% CI: 1.342–2.226, P < 0.001) (Table 2).

Table 2. Multivariate logistic regression analysis of correlates of depression.
3.3 Multivariate logistic regression analysis of correlates of anxiety
Multivariate logistic regression was performed to identify independent correlates of anxiety, defined as a GAD-7 score ≥5. Scores <5 were categorized as non-anxiety. Grade level emerged as a significant predictor: junior secondary school students had lower odds of anxiety compared to senior high school students (OR = 0.438, 95% CI: 0.286–0.752, P = 0.005). School type approached statistical significance, with students from non-key schools showing a higher likelihood of anxiety than those attending key schools (OR = 0.711, 95% CI: 0.489–1.102, P = 0.063). Decreased learning efficiency was significantly associated with higher odds of anxiety (OR = 2.598, 95% CI: 1.695–3.387, P < 0.001). Physical activity was also a significant factor: adolescents engaging in <30 minutes of daily exercise had increased odds of anxiety compared to those with ≥30 minutes of activity (OR = 1.653, 95% CI: 1.299–2.521, P < 0.001) (Table 3).

Table 3. Multivariate logistic regression analysis of correlates of anxiety.
4 Discussion
The findings of this study have important public health implications, particularly in the context of pandemic-related crises. The association between reduced PA and increased depression and anxiety among adolescents suggests the need for public health policies that prioritize accessible PA opportunities during periods of social distancing or lockdowns. Community programs should focus on promoting home-based or low-contact physical activities, such as virtual fitness classes, outdoor walking, or cycling initiatives, to maintain mental health in youth. Policymakers could also advocate for integrating PA into virtual education platforms to ensure continuous engagement in physical activity, even during school closures. By addressing PA as a critical aspect of adolescent well-being during public health emergencies, these strategies could help mitigate the long-term mental health consequences of pandemics. The findings highlight the protective role of PA in the context of a global health crisis, providing evidence that lower levels of PA are independently associated with higher levels of depression and anxiety among youth. The results of this study underscore the importance of promoting accessible forms of physical activity as a preventive and therapeutic strategy for mental health during periods of social isolation, such as pandemics. As adolescents struggle with school closures, reduced social interaction, and uncertainty, physical activity serves as a modifiable factor that can help buffer against the psychological strain of these stressors. Clinically, these findings advocate for targeted interventions aimed at increasing PA among adolescents, particularly in environments where access to traditional sports and physical education may be limited. This study contributes to the growing body of evidence that supports PA as a cost-effective, non-pharmacological intervention to support adolescent mental health, particularly during times of crisis.
The present study examines the relationship between physical activity (PA) and depressive and anxiety symptoms in adolescents during the COVID-19 pandemic. Our findings show that lower levels of daily physical activity were significantly associated with higher risks of both depression and anxiety. Specifically, adolescents engaging in less than 30 minutes of physical activity per day exhibited markedly higher odds of developing depressive (OR = 1.722) and anxiety symptoms (OR = 1.653), even after controlling for confounding factors. These results underscore the crucial role of PA as a protective factor against mental health challenges, especially during periods of significant stress such as the COVID-19 pandemic. Physiologically, regular PA has been shown to influence several biological systems linked to mental health (14, 15). Notably, PA modulates hypothalamic-pituitary-adrenal (HPA) axis function, enhances brain-derived neurotrophic factor (BDNF) expression, and reduces systemic inflammation—mechanisms that are all implicated in the pathophysiology of depression and anxiety (16, 17). Exercise has also been associated with positive neurochemical changes, particularly increased serotonergic and dopaminergic activity, which are essential for mood regulation and anxiety reduction. This finding aligns with existing literature, which suggests that exercise-induced neuroplasticity can help buffer against the psychological toll of stress (18, 19).
Psychosocially, PA offers additional benefits. Adolescents participating in structured or group-based exercises are more likely to experience social interaction, enhanced self-efficacy, and a sense of mastery, all of which mitigate stress and enhance emotional resilience. Adolescence is a critical period for the development of self-identity and emotional regulation, making the psychological benefits of PA particularly pronounced. Furthermore, our findings suggest that adolescents who maintain regular PA routines are more likely to exhibit healthier sleep hygiene and improved academic engagement—two factors strongly linked to lower levels of depression and anxiety. These results suggest that PA can indirectly benefit adolescent mental health by promoting overall well-being and stability in other areas of life. Our study’s findings are consistent with previous research conducted both before and during the COVID-19 pandemic. For instance, Bailey et al. (20) in their meta-analysis highlighted that physical activity interventions significantly reduced depressive symptoms in adolescents, demonstrating moderate effect sizes across randomized controlled trials. Similarly, a large-scale observational study in Norway found that lower levels of sport participation were associated with higher odds of depression and anxiety. During the pandemic, disruptions in daily routines, school closures, and reduced opportunities for outdoor activity exacerbated mental health issues in adolescents, as physical activity levels significantly declined. A study by Xiang et al. (21) found that adolescents who maintained moderate-to-vigorous PA during lockdown reported fewer depressive symptoms and better overall emotional well-being, echoing the findings of our study and underscoring the importance of preserving physical activity routines even during restrictive public health measures.
Our study also reinforces the concept of a dose-response relationship between PA and mental health. Global health authorities recommend at least 60 minutes of moderate-to-vigorous PA per day for adolescents, but our findings suggest that even modest reductions—specifically to less than 30 minutes—are associated with a significant increase in depression and anxiety symptoms. This finding is in line with previous studies that have suggested that the greatest protective effect occurs when adolescents transition from inactivity to regular movement, rather than simply accumulating higher levels of PA. Notably, sex- and age-specific patterns observed in our data also corroborate findings from other studies. Female adolescents consistently demonstrate higher rates of depression and anxiety, but studies, including one by Ekelund et al. (22), suggest that girls may experience equal or even greater mental health benefits from PA than boys, potentially due to differences in psychosocial stress reactivity or sociocultural factors. Similarly, our data show that older adolescents (ages 15–18) had higher rates of depression and anxiety, which may be linked to the increased academic and emotional pressures characteristic of this developmental stage. These findings support the notion that PA can be particularly beneficial during periods of heightened psychological stress, as seen in late adolescence. While some studies have focused on the role of organized sports clubs in protecting adolescent mental health, our study highlights the broader value of general physical activity, regardless of its structured form. Our results contribute to the growing body of evidence that emphasizes the positive effects of daily PA on adolescent mental health, irrespective of its specific context or organization. This broader perspective is essential for public health strategies aimed at promoting physical activity as a tool for improving mental health outcomes in adolescents, especially during periods of crisis such as the COVID-19 pandemic (23, 24).
These findings highlight the importance of clinicians, educators, and public health professionals actively promoting physical activity as part of adolescent mental health strategies. Screening for physical inactivity should be integrated into routine mental health assessments, with personalized recommendations for physical activity—tailored to individual capacities and preferences—considered as first-line preventive and adjunctive interventions for adolescents exhibiting symptoms of depression or anxiety. In particular, in post-pandemic contexts, schools and families should ensure that adolescents have regular access to safe and supportive environments for physical activity. This study has several strengths. First, it utilizes a large sample of over 1,100 adolescents, which enhances the statistical power and generalizability of the findings. Second, validated assessment tools, the CES-DC for depressive symptoms and the GAD-7 for anxiety—were used, ensuring reliable measurement of mental health status. Third, the study employed multivariate logistic regression analyses to adjust for key confounders, such as gender, age, learning efficiency, and sleep duration, thereby isolating the independent association between physical activity and mental health outcomes.
Several limitations should be acknowledged. First, the cross-sectional design limits causal inference; while significant associations were observed, it remains unclear whether low PA contributes to depression and anxiety, or whether these symptoms reduce motivation for PA. Longitudinal studies with repeated measures of PA, mental health symptoms, sleep duration, academic performance, and social engagement are needed to clarify temporal relationships. Second, PA was assessed via a single self-reported item without capturing frequency, intensity, or activity type, which may lead to exposure misclassification due to recall or social desirability bias. Future research should incorporate validated multi-item instruments or objective measures to improve measurement accuracy. Third, mental health outcomes were identified based on validated symptom thresholds rather than clinical diagnosis, which may overestimate prevalence but are appropriate for population-level screening. Fourth, the web-based survey design may introduce sampling bias, as adolescents with limited internet access or greater concern about mental health may have been overrepresented. Additionally, the study was geographically confined to Pidu District, Chengdu City in China—limiting generalizability to rural or socioeconomically diverse populations. Future studies should include more representative samples across different settings. Lastly, future research should evaluate scalable interventions—such as virtual fitness programs, outdoor activity initiatives, and integration of PA into online or hybrid school curricula—to enhance adolescent PA engagement.
5 Conclusions
In conclusion, this study identifies limited physical activity, specifically engaging in less than 30 minutes of daily exercise, as a significant independent risk factor for depressive symptoms in adolescents. Alongside female gender, reduced sleep duration, and decreased learning efficiency, insufficient physical activity emerged as a key modifiable contributor. These findings emphasize the critical role of promoting regular physical exercise in preventing adolescent depression.
Data availability statement
The original contributions presented in the study are included in the article/supplementary material. Further inquiries can be directed to the corresponding author.
Ethics statement
The studies involving humans were approved by School of Physical Education, Southwest Jiaotong University. The studies were conducted in accordance with the local legislation and institutional requirements. Written informed consent for participation in this study was provided by the participants’ legal guardians/next of kin.
Author contributions
H-YY: Conceptualization, Data curation, Formal Analysis, Investigation, Methodology, Resources, Software, Supervision, Writing – original draft, Writing – review & editing. L-HS: Conceptualization, Data curation, Formal Analysis, Investigation, Methodology, Project administration, Resources, Writing – original draft.
Funding
The author(s) declare financial support was received for the research and/or publication of this article. This study was supported by the General Education Project of the National Social Science Fund of China (BLA200214). The fund title is “Research on Physical Exercise and Adolescent Stress during Major Public Health Emergencies.
Acknowledgments
We would like to express our sincere gratitude to all the investigators who contributed to this study.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Generative AI statement
The author(s) declare that no Generative AI was used in the creation of this manuscript.
Any alternative text (alt text) provided alongside figures in this article has been generated by Frontiers with the support of artificial intelligence and reasonable efforts have been made to ensure accuracy, including review by the authors wherever possible. If you identify any issues, please contact us.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Philippot A, Dubois V, Lambrechts K, Grogna D, Robert A, Jonckheer U, et al. Impact of physical exercise on depression and anxiety in adolescent inpatients: A randomized controlled trial. J Affect Disord. (2022) 301:145–53. doi: 10.1016/j.jad.2022.01.011
2. Recchia F, Bernal JDK, Fong DY, Wong SHS, Chung PK, Chan DKC, et al. Physical Activity Interventions to Alleviate Depressive Symptoms in Children and Adolescents: A Systematic Review and Meta-analysis. JAMA Pediatr. (2023) 177:132–40. doi: 10.1001/jamapediatrics.2022.5090
3. McMahon EM, Corcoran P, O’Regan G, Keeley H, Cannon M, Carli V, et al. Physical activity in European adolescents and associations with anxiety, depression and well-being. Eur Child Adolesc Psychiatr. (2017) 26:111–22. doi: 10.1007/s00787-016-0875-9
4. Kim SY, Park JH, Lee MY, Oh KS, Shin DW, and Shin YC. Physical activity and the prevention of depression: A cohort study. Gen Hosp Psychiatr. (2019) 60:90–7. doi: 10.1016/j.genhosppsych.2019.07.010
5. Chen L, Liu Q, Xu F, Wang F, Luo S, An X, et al. Effect of physical activity on anxiety, depression and obesity index in children and adolescents with obesity: A meta-analysis. J Affect Disord. (2024) 354:275–85. doi: 10.1016/j.jad.2024.02.092
6. Feng Q, Zhang QL, Du Y, Ye YL, and He QQ. Associations of physical activity, screen time with depression, anxiety and sleep quality among Chinese college freshmen. PLoS One. (2014) 9:e100914. doi: 10.1371/journal.pone.0100914
7. Shen L, Gu X, Zhang T, and Lee J. Adolescents’ Physical Activity and Depressive Symptoms: A Psychosocial Mechanism. Int J Environ Res Public Health. (2022) 19:1276. doi: 10.3390/ijerph19031276
8. Velazquez B, Petresco S, Pereira R, Buchweitz C, Manfro PH, Caye A, et al. Physical activity and depressive symptoms among adolescents in a school-based sample. Braz J Psychiatr. (2022) 44:313–6. doi: 10.1590/1516-4446-2021-2235
9. Li J, Zhou X, Huang Z, and Shao T. Effect of exercise intervention on depression in children and adolescents: a systematic review and network meta-analysis. BMC Public Health. (2023) 23:1918. doi: 10.1186/s12889-023-16824-z
10. Li B, Ng K, Tong X, Zhou X, Ye J, and Yu JJ. Physical activity and mental health in children and youth during COVID-19: a systematic review and meta-analysis. Child Adolesc Psychiatry Ment Health. (2023) 17:92. doi: 10.1186/s13034-023-00629-4
11. Wolf S, Seiffer B, Zeibig JM, Welkerling J, Brokmeier L, Atrott B, et al. Is Physical Activity Associated with Less Depression and Anxiety During the COVID-19 Pandemic? A Rapid Systematic Review. Sports Med. (2021) 51:1771–83. doi: 10.1007/s40279-021-01468-z
12. Samji H, Wu J, Ladak A, Vossen C, Stewart E, Dove N, et al. Review: Mental health impacts of the COVID-19 pandemic on children and youth - a systematic review. Child Adolesc Ment Health. (2022) 27:173–89. doi: 10.1111/camh.12501
13. Erdoğan R. Effects of a Yoga-Based Intervention on Self-Compassion, Depression and Loneliness in Obese Adolescents. Int J Sport Stud Health. (2025) 8:1–7. doi: 10.61838/kman.intjssh.8.3.2
14. Hou J, Deng Q, Sha L, Zhu J, Xiang R, Zhao X, et al. Physical activity and risk of depression in adolescents: A systematic review and meta-analysis of prospective observational studies. J Affect Disord. (2025) 371:279–88. doi: 10.1016/j.jad.2024.11.065
15. Kandola A, Lewis G, Osborn DPJ, Stubbs B, and Hayes JF. Depressive symptoms and objectively measured physical activity and sedentary behaviour throughout adolescence: a prospective cohort study. Lancet Psychiatr. (2020) 7:262–71. doi: 10.1016/S2215-0366(20)30034-1
16. Ma R, Romano E, Vancampfort D, Firth J, Stubbs B, and Koyanagi A. Association between physical activity and comorbid anxiety/depression in 46 low- and middle-income countries. J Affect Disord. (2023) 320:544–51. doi: 10.1016/j.jad.2022.10.002
17. Glaus J, Kang SJ, Guo W, Lamers F, Strippoli MF, Leroux A, et al. Vollenweider P et al: Objectively assessed sleep and physical activity in depression subtypes and its mediating role in their association with cardiovascular risk factors. J Psychiatr Res. (2023) 163:325–36. doi: 10.1016/j.jpsychires.2023.05.042
18. Pascoe MC and Parker AG. Physical activity and exercise as a universal depression prevention in young people: A narrative review. Early Interv Psychiatr. (2019) 13:733–9. doi: 10.1111/eip.12737
19. Matias TS, Lopes MVV, da Costa BGG, Silva KS, and Schuch FB. Relationship between types of physical activity and depression among 88,522 adults. J Affect Disord. (2022) 297:415–20. doi: 10.1016/j.jad.2021.10.051
20. Bailey AP, Hetrick SE, Rosenbaum S, Purcell R, and Parker AG. Treating depression with physical activity in adolescents and young adults: a systematic review and meta-analysis of randomised controlled trials. Psychol Med. (2018) 48:1068–83. doi: 10.1017/S0033291717002653
21. Xiang M, Zhang Z, and Kuwahara K. Impact of COVID-19 pandemic on children and adolescents’ lifestyle behavior larger than expected. Prog Cardiovasc Dis. (2020) 63:531–2. doi: 10.1016/j.pcad.2020.04.013
22. Wiium N, Breivik K, and Wold B. Growth Trajectories of Health Behaviors from Adolescence through Young Adulthood. Int J Environ Res Public Health. (2015) 12:13711–29. doi: 10.3390/ijerph121113711
23. Ellis WE, Dumas TM, and Forbes L. Adolescents’ physical activity and psychological adjustment across the first year of the COVID-19 pandemic. J Phys Act Health. (2022) 19:481–9. doi: 10.1123/jpah.2022-0018
Keywords: adolescents, physical activity, depression, anxiety, COVID-19, mental health, risk factors
Citation: Yang H-Y and Sun L-H (2025) Impact of physical activity on symptoms of depression and anxiety in adolescents during the COVID-19 pandemic. Front. Psychiatry 16:1631978. doi: 10.3389/fpsyt.2025.1631978
Received: 20 May 2025; Accepted: 05 August 2025;
Published: 25 August 2025.
Edited by:
Laisa Liane Paineiras-Domingos, Federal University of Bahia (UFBA), BrazilReviewed by:
Mohsen Khosravi, Zahedan University of Medical Sciences, IranKhadijeh Irandoust, Imam Khomeini International University, Iran
Bowen Li, Zhejiang University, China
Copyright © 2025 Yang and Sun. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Hai-Ying Yang, SGFpeWluZ1kxMjNAMTYzLmNvbQ==