 Amrit Sudershan1
Amrit Sudershan1 Sumaira Rehman2Tafazul Manzoor2Basharat Shaban2Seerat Sultan3
Sumaira Rehman2Tafazul Manzoor2Basharat Shaban2Seerat Sultan3 Agar Chander Pushap4
Agar Chander Pushap4 Srishty Sudershan5Mehraj Bashir2
Srishty Sudershan5Mehraj Bashir2 Showkat Ahmad Malik2*
Showkat Ahmad Malik2*- 1Department of Human Genetics, Sri Pratap College, Cluster University Srinagar, Srinagar, Jammu & Kashmir, India
- 2Department of Zoology, Sri Pratap College, Cluster University Srinagar, Srinagar, Jammu & Kashmir, India
- 3Department of Environmental Science, Sharda University, Delhi, India
- 4Department of Education, Dakshina Bharat Hindi Prachar Sabha, Madras, Chennai, Tamil, India
- 5Department of Zoology, Central University of Jammu, Samba, Jammu, Jammu & Kashmir, India
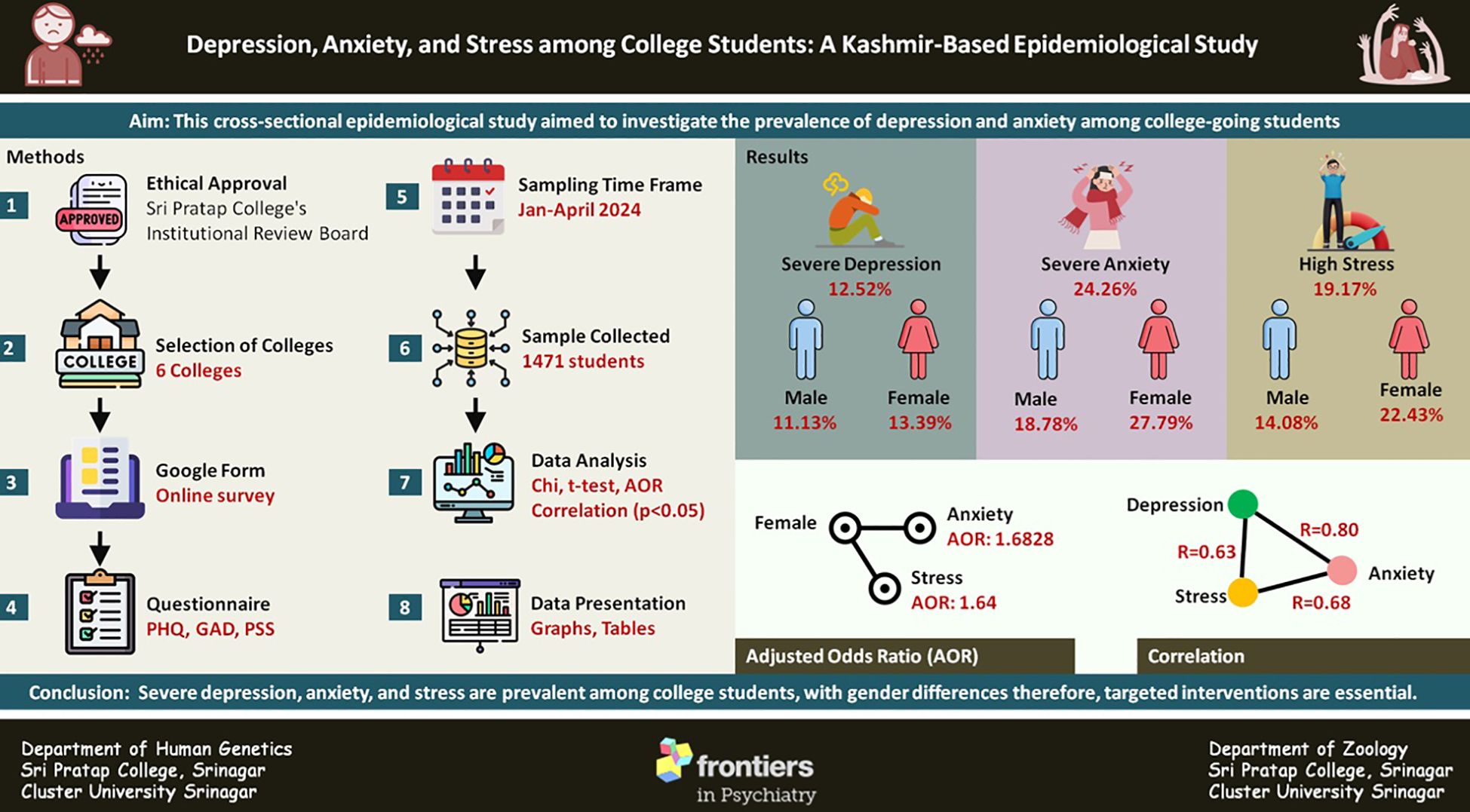
Introduction: Depression and anxiety are major public health concerns, especially among young adults. However, limited regional data exist from Kashmir, Northern India, to guide targeted mental health strategies. Therefore, the present study aimed to assess the levels of depression and anxiety among college-going students in Kashmir and examine associated demographic factors.
Methods: A cross-sectional survey was conducted from January to April 2024, involving 1,471 college students aged 18 to 26 years from institutions across the Kashmir division. Data were collected using an online Google Form after obtaining informed consent. Depression and anxiety were measured using validated scales: PHQ-9 and GAD-7. Statistical analyses included t-tests, chi-square tests, logistic regression, and Pearson correlation to explore associations and trends.
Results: Among the participants, 12.5% exhibited severe depression, with a slightly higher prevalence in females (13.39%). Severe anxiety was reported by 24.26% of students, and 19.17% reported high perceived stress levels. Gender showed notable relevance with anxiety (OR ≈ 1.68, p = 0.0001) and stress (OR ≈ 1.65, p = 0.0007). Correlation analysis revealed positive relationships between depression and stress score (r = 0.6322), anxiety and stress score (r = 0.6824), and depression and anxiety (r = 0.8064), suggesting that higher stress levels correlate with increased depression and anxiety among surveyed individuals.
Discussion: The high prevalence of depression, anxiety, and stress among college students, especially among females, highlights an urgent need for gender-sensitive, campus-based mental health interventions. The strong interrelations among these psychological conditions suggest that comprehensive stress-reduction programs may effectively mitigate multiple mental health risks. Future research should focus on designing and evaluating such targeted strategies to enhance student well-being.
Graphical Abstract.
Introduction
A nation’s progress is closely linked to the well-being of its citizens, as those who are mentally healthy are more likely to make a positive impact, engage in meaningful work, and maintain strong social connections (1). However, a significant barrier to mental well-being is Major Depressive Disorder (MDD), which is characterized by persistent symptoms such as feelings of hopelessness, difficulty concentrating, disrupted sleep, low energy, changes in appetite, and, in severe cases, suicidal thoughts or attempts. These symptoms typically last for at least two weeks and occur nearly every day, significantly impairing an individual’s ability to function (Depression-World Health Organization). According to the data of Global Burden of Diseases (GBD) 2019 identified depression and anxiety were identified as the two most disabling mental health conditions, ranking among the top 25 causes of disease burden worldwide. Around 280 million people globally suffer from depression, representing 3.8% of the population, with higher rates in adults (5.0%) and those over 60 (5.7%). The highest prevalence rates are found in Greece, Palestine, and Spain (Institute for Health Metrics and Evaluation). In India, states such as Tamil Nadu, Haryana, Andhra Pradesh, and Maharashtra report notable depression rates, with Tamil Nadu having the highest at 4.45% (Institute for Health Metrics and Evaluation | (healthdata.org).
Although adults and older populations show higher global prevalence, it is critical to study the mental health of college-going students, as they undergo significant developmental and psychosocial transitions that can heighten vulnerability to psychological distress. Academic pressure, career uncertainty, identity exploration, and changing social environments contribute to an increased risk of mental health issues in this age group (2, 3). Moreover, early identification and intervention in this formative period can prevent long-term psychological morbidity. In the Kashmir region, multiple studies have explored depression and anxiety prevalence (4–6), though none have specifically targeted the college-going population. Therefore, this study aimed to fill this gap by examining the prevalence of depression, anxiety, and perceived stress among college students in Kashmir, making it, to our knowledge, the first of its kind in the region.
Methodology
Ethical considerations and consent to participate
This study was conducted in strict adherence to ethical standards. The research methodology was reviewed and approved by the Institutional Ethical Committee (ICE) of Sri Pratap College, Srinagar, Cluster University Srinagar, and Kashmir.
Before participation, each study participant provided informed written consent electronically via an e-form or Google Form, outlining the study’s purpose, the voluntary nature of participation, and the confidentiality of their information. Data collection commenced only after obtaining informed consent from all participants (discussed below), ensuring compliance with ethical principles and regulations concerning research involving human subjects.
Study design, sampling approach, and sample size estimation
This study employed a cross-sectional design to investigate the prevalence of depression, anxiety, and stress among college students of Kashmiri descent, aged 18–26 years. A two-stage sampling strategy was adopted to balance representativeness and practicality, combining simple random sampling for college selection and convenience sampling for participant recruitment.
Furthermore, the sample size was estimated based on prior knowledge, considering a significance level (α) of 0.05, an expected proportion of 0.25, and a precision (margin of error) of 0.03 (Equation 1). Using these parameters, the minimum required sample size was calculated to be 801 participants.
Where: n = required sample size, Z = standard normal deviate at 95% confidence level (1.96), p = expected proportion (0.25, based on prior knowledge), and d = margin of error (0.03).
College selection & participant recruitment
In the first stage, a simple random sampling method was used to select colleges from the Kashmir region. A comprehensive list of all colleges in the region was compiled using Excel. The “RAND () function” in Excel was employed to randomly select six colleges from this list. Random sampling was chosen at this stage to ensure that every college had an equal chance of being selected, thereby minimizing selection bias and enhancing the representativeness of the sample. The decision to select six colleges was made to ensure the study maintained a manageable scope, given the logistical constraints and the available research resources. This number allowed for adequate representation of the student population while enabling in-depth analysis within a feasible timeline.
In the second stage, a convenience sampling method was used to recruit participants from the selected colleges. Convenience sampling was deemed appropriate at this stage due to the practical challenges of accessing students directly and the necessity of ensuring a sufficient sample size within the limited data collection period (January 2024 to April 2024). Furthermore, the online nature of data collection facilitated by Google Forms inherently lends itself to convenience sampling, as participants self-selected based on their willingness and availability to complete the survey. To minimize potential selection bias introduced by convenience sampling, we recruited participants from multiple colleges across various academic disciplines to improve the diversity and representativeness of the sample.
Data collection procedure
To ensure participant confidentiality and voluntary participation, data were collected via an online Google Form designed with a clear and sequential structure. The form was disseminated through official college communication channels and student groups, such as WhatsApp groups, accompanied by a briefing that explained the study’s objectives and significance. The online format allowed for greater reach, ease of participation, and flexibility for respondents. The Google Form followed a three-step structure: (a): Introductory Section: Participants were presented with an introductory page detailing the purpose of the research and requesting their consent to participate. Only those who provided informed consent could proceed. (b): Demographic Information Section: Participants were required to provide basic demographic details, including age, gender, and educational background. (c): Diagnostic Section: This section featured standardized questionnaires to assess depression, anxiety, and stress (see Diagnostic Procedure). The strategic use of a Google Form ensured participant anonymity and confidentiality while also fostering transparency and trust in the research process. To ensure data security and prevent duplicate responses, the “Limit to 1 response” feature in Google Forms was activated, allowing each participant to submit only one response. [Note: Participants were informed about the study’s purpose and provided consent before proceeding with the survey. Due to the anonymous nature of data collection, withdrawal of data post-submission was not possible.
Diagnostic procedures
Participants who agreed to take part in the study were assessed for depression, anxiety, and perceived stress using well-established tools. Depression was evaluated using the Patient Health Questionnaire-9 (PHQ-9), a widely recognized instrument designed to screen for and diagnose depressive disorders following DSM-5 criteria (7). Details of the PHQ-9 scoring method can be found in Supplementary Table 1 of the Supplementary File. To assess anxiety, we used the Generalized Anxiety Disorder Assessment (GAD-7), a trusted tool for identifying and diagnosing generalized anxiety disorder (8). The scoring method for the GAD-7 is outlined in Supplementary Table 2 of the Supplementary File. In addition to depression and anxiety, we also assessed perceived stress levels using the Perceived Stress Scale (PSS), a widely accepted measure for evaluating stress perception (NH Dept. of Administrative Services). Information about the PSS scoring method is provided in Supplementary File of the Supplementary File. All assessments were conducted in English, as all participants were fluent in the language, making it unnecessary to modify the wording of the questionnaires.
Data cleaning and analysis
Following data collection, a rigorous data-cleaning process was implemented, which was done in Microsoft Excel 2019. Exclusion criteria were established to ensure the integrity and reliability of the dataset. These criteria included (1): obtaining participant consent, (2): restricting participant age to the range of 18–26 years, (3): ensuring completion of the entire survey questionnaire, and (4): confirming that students were from the population of the Kashmir region and not from other areas. Additionally, any responses with missing data were systematically identified and excluded from the final analysis to maintain the accuracy and consistency of the dataset. By applying these criteria, unnecessary, incomplete, or inconsistent responses were identified and removed, ensuring the integrity of the dataset. In addition, the responses of the participants were then coded into a numeric form to facilitate analysis in Excel 2019.
Statistical analysis
The cleaned dataset subsequently underwent comprehensive statistical analysis to explore patterns, trends, and associations related to the prevalence of conditions among college-going students in the Kashmir population (Northern India). Descriptive data analysis of continuous and discrete variables utilized mean ± standard deviation and frequency distribution methods, respectively. To identify significant differences between continuous and discrete variables, t-tests and chi-square analyses were employed, respectively. Adjusted Odds Ratio (AOR) using Multiple Logistic Regression (MLR) was used to determine the association between dependent variables (depression and anxiety) and independent variables (Demographic variables). The Pearson correlation method is used to find the degree of linear relationship between two continuous variables. All calculations were conducted using free online statistical software, specifically the Chi-Square Calculator (2x2-5x5) from Socscistatistics.com, and MedCalc’s statistical software for Logistic Regression and correlation. A significance threshold of p< 0.05 and a 95% confidence interval were considered significant for all statistical tests.
[Note: For binary logistic regression, the response variables such as depression, anxiety, and perceived stress were dichotomized based on standard cut-off scores. For depression, individuals scoring between 15–19 (moderately severe) and 20–27 (severe) were coded as “1” (indicating high depression), while those scoring below this range were coded as “0”. For anxiety, scores of 10–14 (moderate) and 15–21 (severe) were categorized as “1”, and lower scores as “0”. Similarly, for perceived stress, scores between 27–40 were classified as “1” (high stress), while scores below 27 were coded as “0”.
Result
In the present investigation, the surveyed population comprises 1471 students (male = 575 and female=896) who were included after excluding a certain number of students (Figure 1) using exclusion criteria (see section: Data Cleaning and Analysis). The average age of participants was 21.66 ± 1.94 years, with no significant difference between males (21.63 ± 1.94) and females (21.69 ± 1.95; t = 0.577, p = 0.564). The sample was predominantly rural (61.1%), with 38.9% from urban areas (Figure 2A). Most participants were unmarried (92.2%) (Figure 2B). Gender distribution across rural and urban settings showed a higher proportion of females in urban areas and more males in rural settings. Regarding socioeconomic background, the majority of students’ guardians reported monthly incomes between ₹10,000 and ₹50,000 (Figure 2C), with 37.9% earning below ₹10,000 and 19.0% above ₹51,000. A detailed summary of demographic characteristics and gender-based comparisons is presented in Table 1.
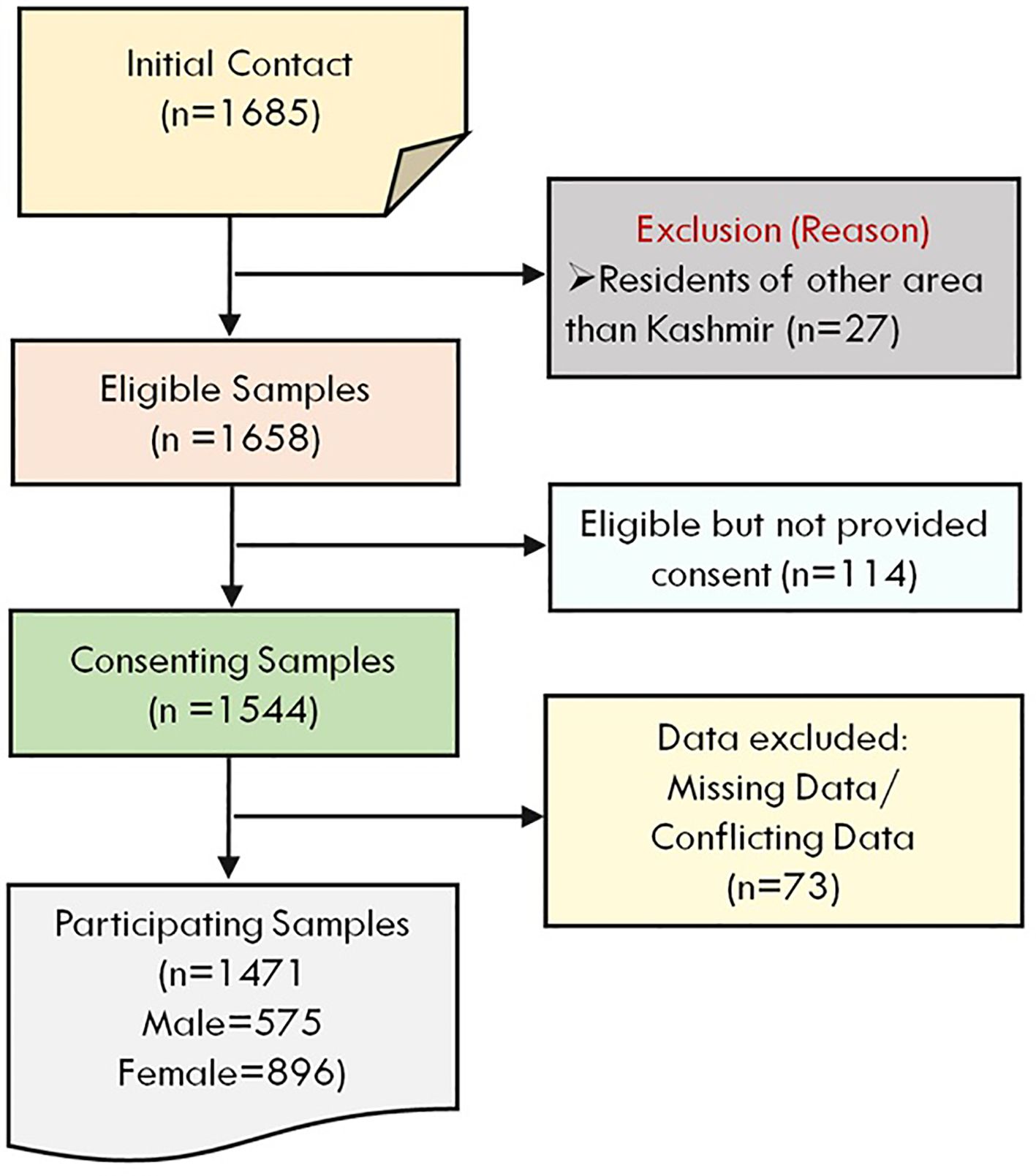
Figure 1. Flowchart illustrates the stepwise selection process of study participants, including exclusions, consent status, and final sample distribution by gender.
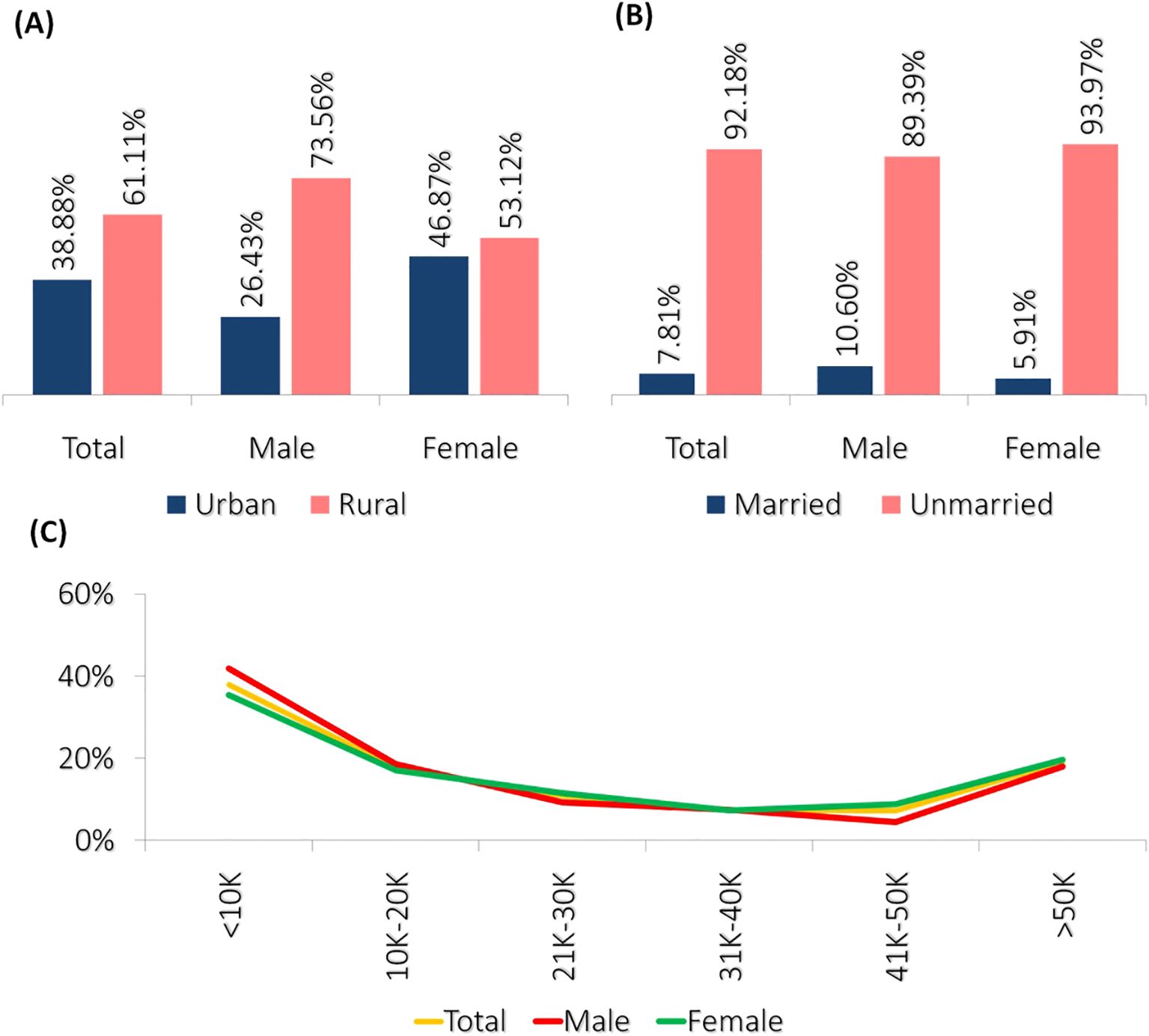
Figure 2. The presented graphs illustrate the demographic characteristics of the surveyed population. (A) The bar graph shows the distribution of participants based on their residential location, indicating a higher proportion of rural residents compared to urban residents across total, male, and female groups. (B) The bar graph represents the marital status distribution, revealing a significantly higher percentage of unmarried individuals in all categories. (C) The line graph depicts the distribution of guardian income levels, showing a declining trend as income levels increase, followed by a slight rise in the highest income category.
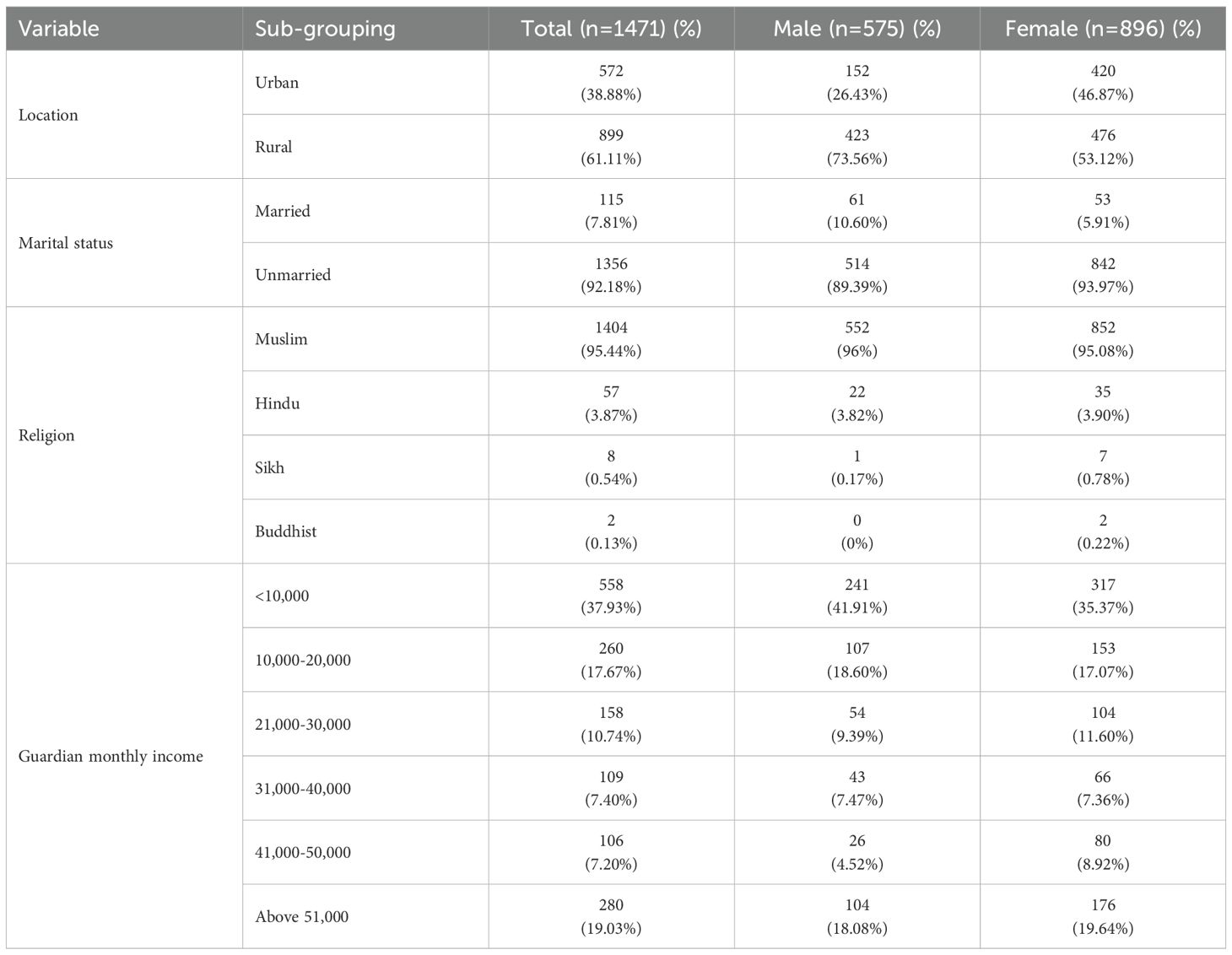
Table 1. Distribution of demographic features among study participants.
After analyzing the demographic features, the prevalence of different conditions among the surveyed students was observed using various questionnaires. Depression levels were assessed using the PHQ questionnaire. It was revealed that minimal depression was observed in 22.84% of the total sample (Figure 3A). In contrast, moderately severe depression was identified in 18.83% of the sample. Notably, there was a higher prevalence of moderately severe depression among females (21.54%) compared to males (14.61%). Furthermore, it was observed that severe depression was present in 12.5% (Figure 3A) of the total sample, with a slightly elevated prevalence among females (13.39%) compared to males (11.13%) (Table 2).
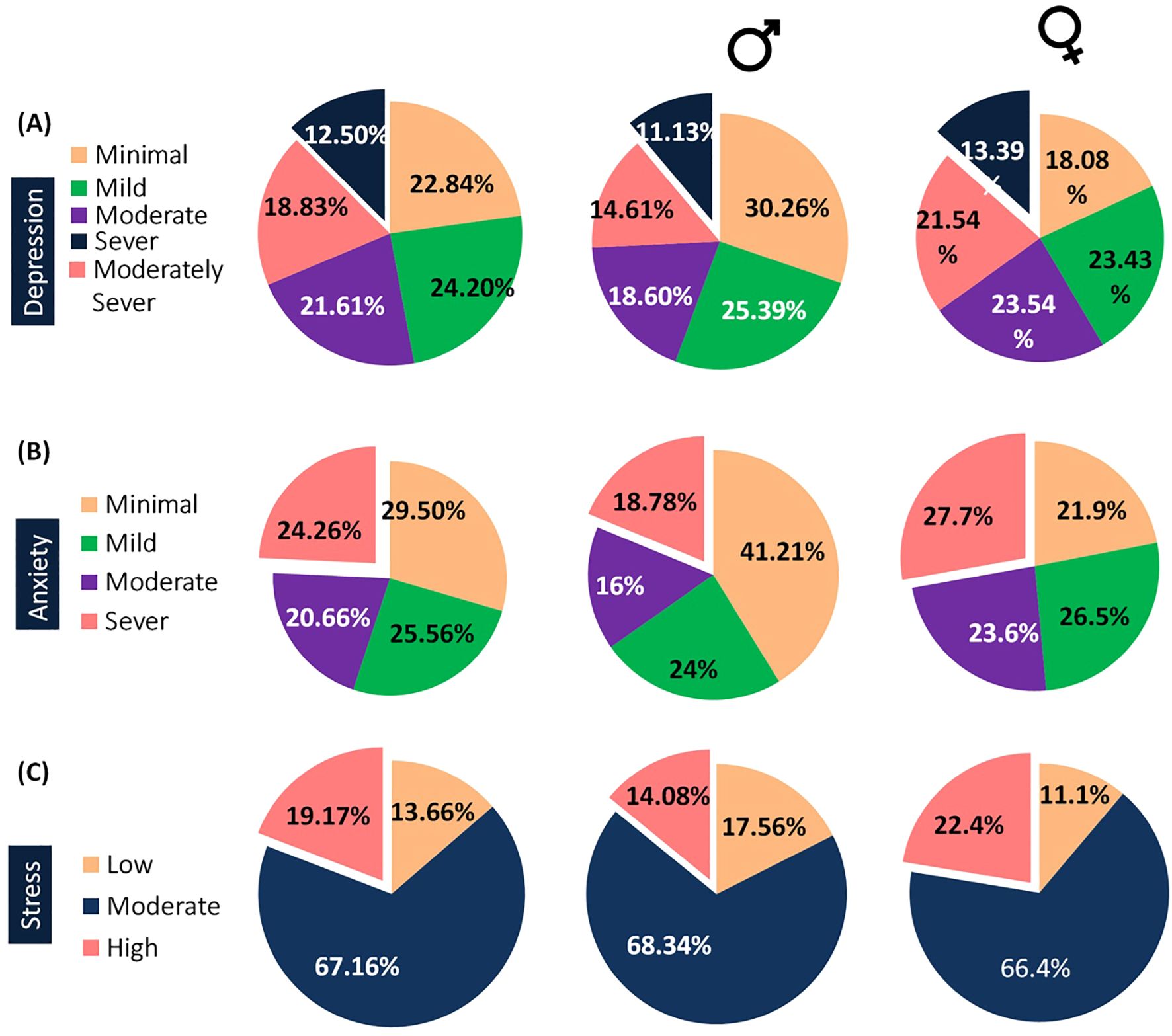
Figure 3. The presented pie charts illustrate the frequency distribution of mental health conditions among the surveyed population. (A) The pie charts display the prevalence of depression across the overall, male, and female participants, showing varying proportions across different severity levels. (B) The pie charts highlight the distribution of anxiety levels in the total population, as well as by gender. (C) The pie charts depict the prevalence of perceived stress among the overall, male, and female groups, revealing distinct trends in stress severity.
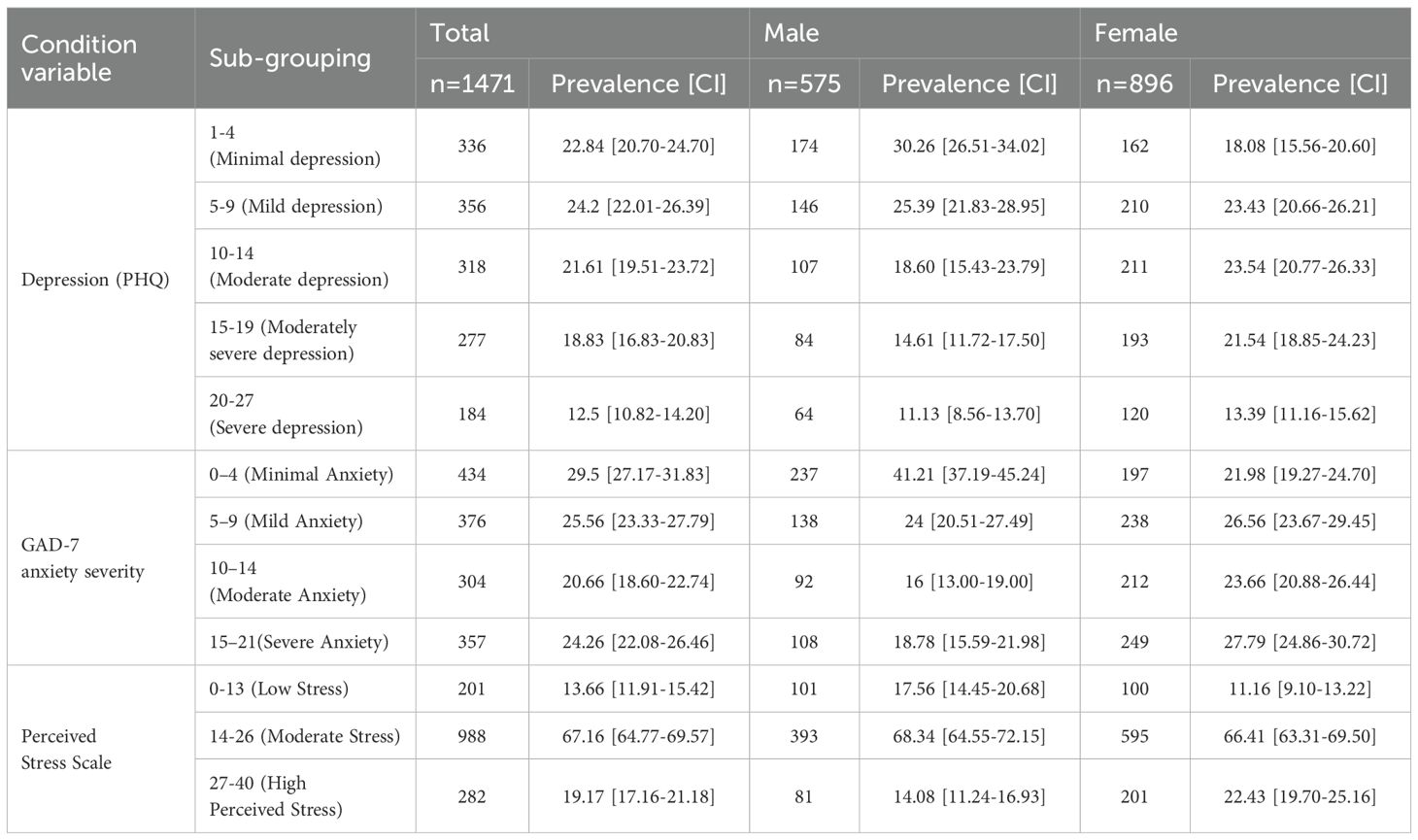
Table 2. Prevalence of depression, anxiety, and stress among student of colleges in Kashmir students.
Regarding the anxiety disorder, insights into varying anxiety levels among surveyed students were provided by the GAD-7 questionnaire. Minimal anxiety was reported by 29.56% (n=434) of the students. Moderate anxiety was noted in 20.66% (n=304), with a higher prevalence among females (23.66%) compared to males (16.00%) (Figure 3B). Severe anxiety was experienced by 24.26% (n=357) of students, with a slightly higher prevalence among females (27.79%) compared to males (18.78%) (Table 2).
The analysis of the stress among surveyed students using the Perceived Stress Scale unveiled varying stress levels. Among the participants, 201 students (13.66%) reported low stress (0-13), with 101 males (17.56%) and 100 females (11.16%) falling within this category (Figure 3C). A majority of students, comprising 988 individuals (67.16%), experienced moderate stress (14-26), including 393 males (68.34%) and 595 females (66.40%). Additionally, 282 students (19.17%) reported high perceived stress (27-40), with 81 males (14.08%) and 201 females (22.43%) experiencing this level of stress (Table 2).
The analysis of variables linked to mental health outcomes highlighted significant associations (Table 3). Gender showed notable relevance with anxiety (OR = 1.68, p = 0.0001) and stress (OR = 1.65, p = 0.0007) (Figure 4). Additionally, correlation analysis unveiled positive relationships between depression and stress score (r = 0.6322), anxiety and stress score (r = 0.6824), and depression and anxiety (r = 0.8064), indicating that higher stress levels correlate with increased depression and anxiety among the surveyed individuals (Table 4).
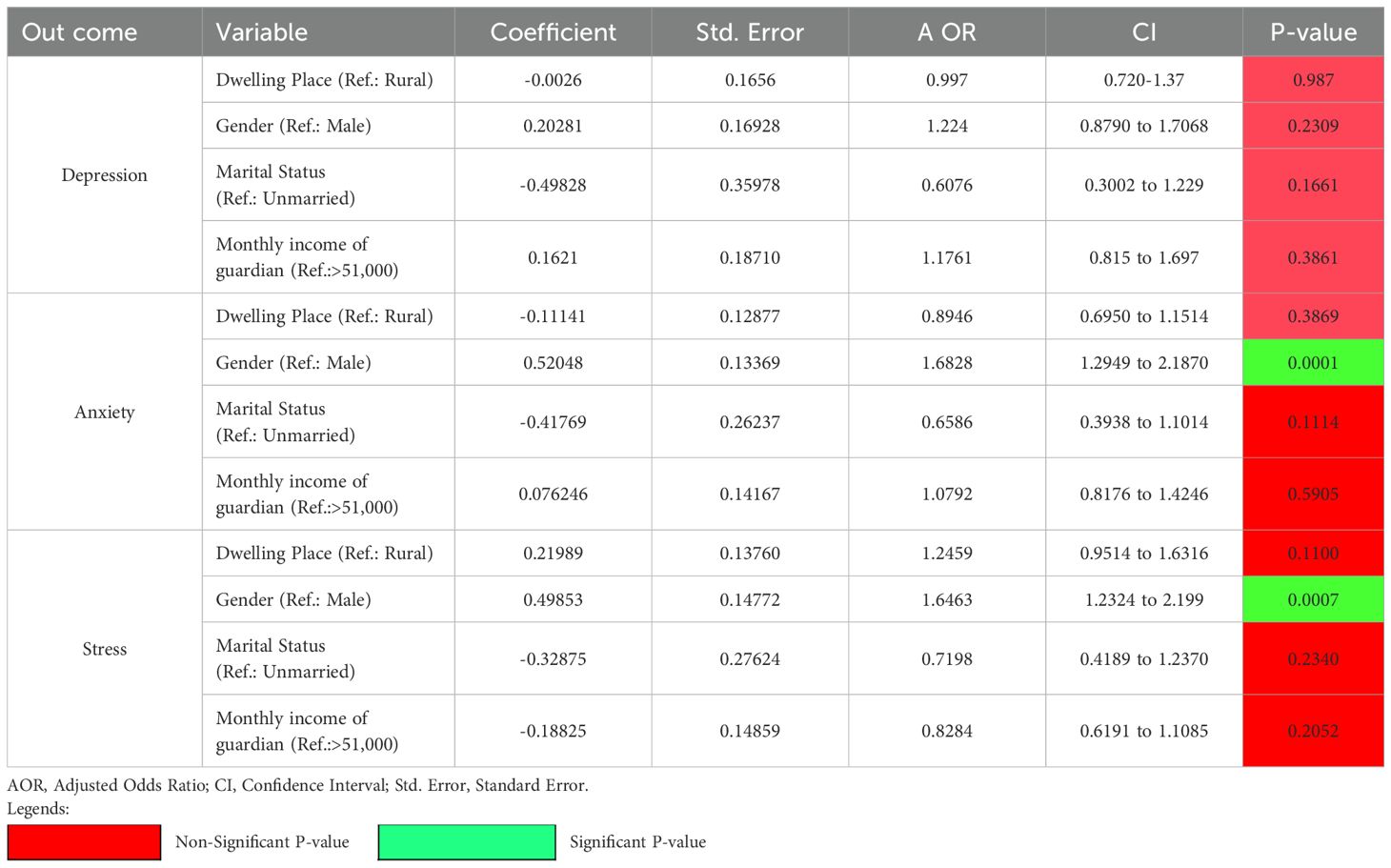
Table 3. Logistic regression analysis of factors associated with depression, anxiety, and stress among Kashmiri College students.
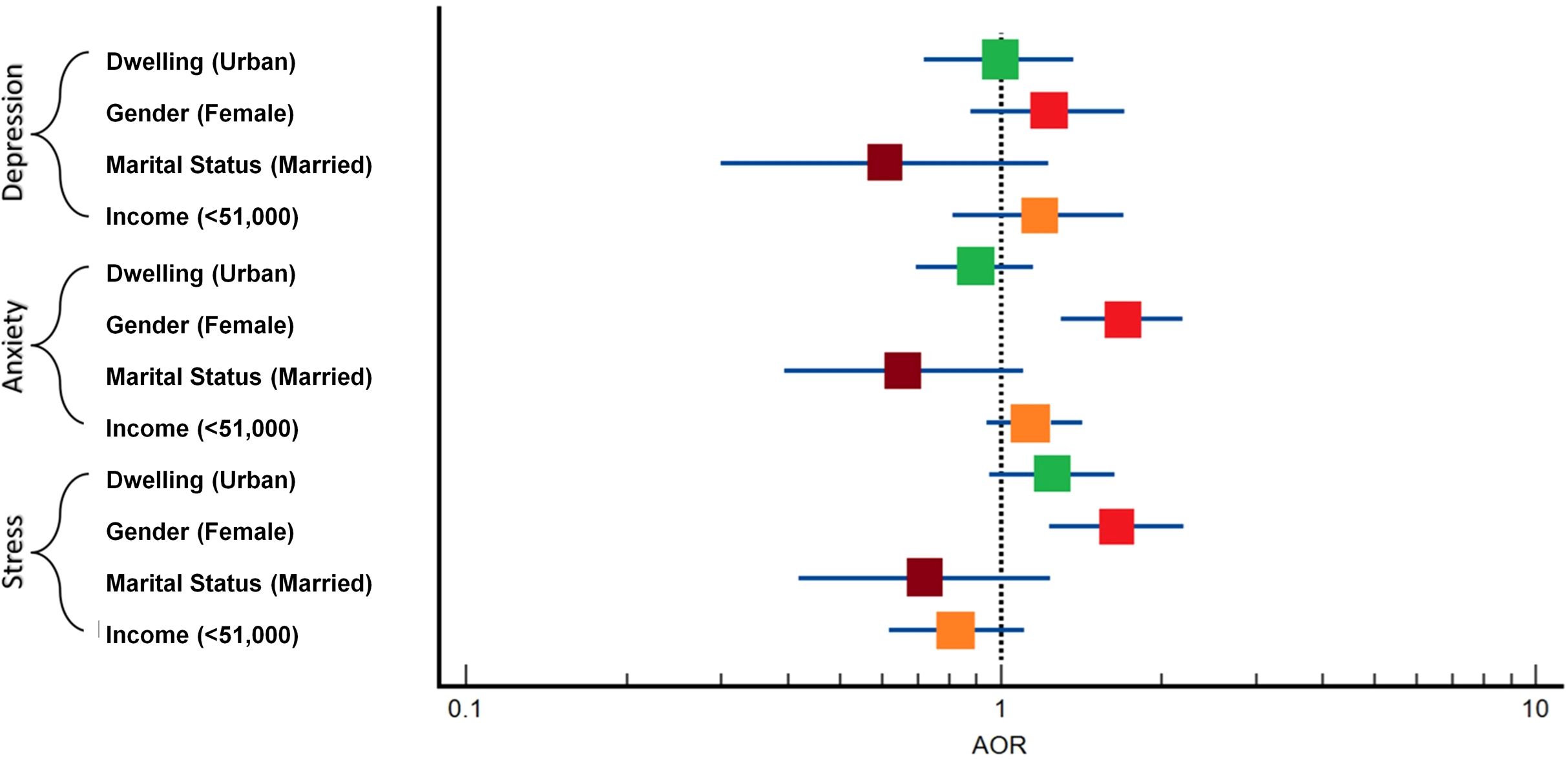
Figure 4. The forest plot shows the association between demographic factors and the risk of depression, anxiety, and stress. Each square represents the Adjusted Odds Ratio (AOR) with confidence intervals for factors such as dwelling place, gender, marital status, and guardian’s income. The dotted line (AOR = 1) indicates no effect.
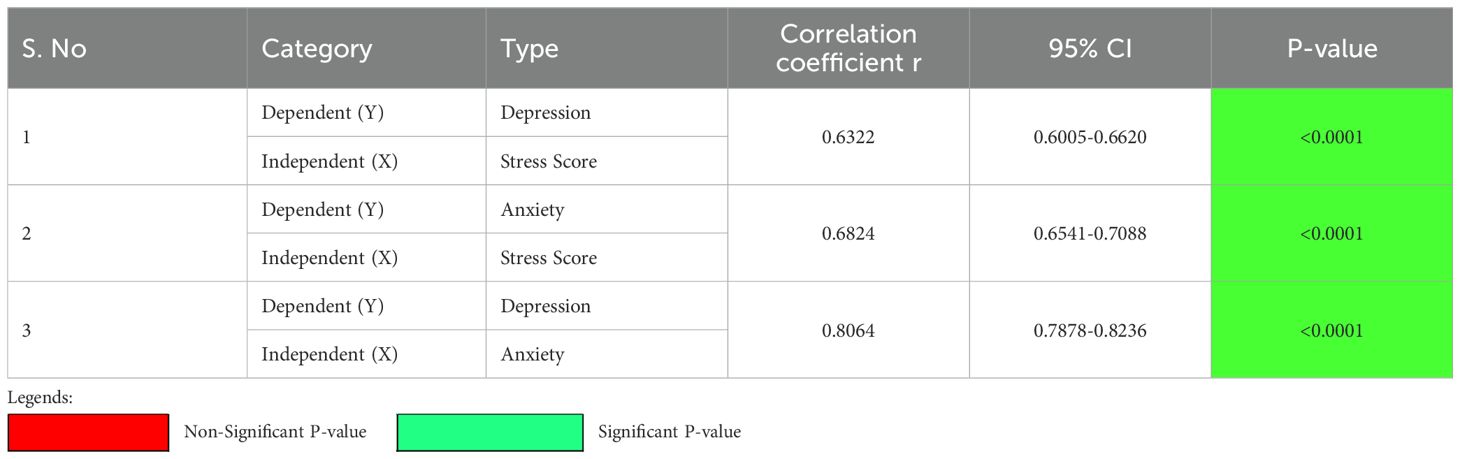
Table 4. Correlation analysis results between depression, anxiety, and stress score.
Discussion
College life represents a pivotal stage in an individual’s academic and personal development. It serves as a bridge between foundational education and professional or higher academic pursuits, promoting not only knowledge acquisition and skill enhancement but also self-awareness and identity formation. However, this transitional period is often accompanied by considerable psychological stress, which can manifest as mental health concerns, including depression, anxiety, and somatic symptoms such as headaches. Among these, anxiety has been identified as particularly prevalent among college students globally (9). In the context of Kashmir, although mental health issues have been investigated within the general population, there is a noticeable gap in research focusing specifically on college students (4–6, 10–12). Addressing this gap, the present study seeks to assess the prevalence of depression, anxiety, and perceived stress among college students in the region, contributing novel insights to an underexplored area of public mental health research.
After utilizing the cross-sectional study method, the study utilized the PHQ questionnaire to assess depression levels among college students, revealing that 18.81% (Male Vs Female: 14.61% Vs 21.53%) experienced moderately severe depression (scores 15-19) and 12.5% of students reported severe depression (scores 20-27) (Table 2). However, the present study found that 12.5% of students reported severe depression, which is somewhat similar to findings from studies conducted in various regions of India and foreign countries (13–20). For instance, in District Amritsar, 13.1% of students reported severe depression (21), while in West Bengal, 6.25% of students experienced severe depression (22). Conversely, some studies have reported contradictory results. For example, in Puducherry, only 0.7% of students were classified as having severe depression, and another 0.7% as having very severe depression (23).
In addition, the present study also revealed that severe depression was slightly more common among female students, with 13.39% affected, compared to 11.13% of male students which was consistent with research indicating higher levels of depression among females compared to males (24–34). Females are more susceptible to mental disorders and report more mental health difficulties than their male counterparts which may be due to certain factors such as academic stress, social pressures, less or no social support, body image, academic performance/stress, peer pressure, professional pressure, financial stress in home, and excessive parental expectations (25, 30, 34, 35). On the other hand, the findings are in contradiction with different studies (22, 23, 36, 37), which found that there is no significant difference between genders. Additionally, some evidence showed that a higher percentage of male students suffered varying degrees of depression than females (35, 38–42). There is a possibility that the gender differences that were found might be attributed to the cultural background of the pupils as well as the socialization process that both genders go through (41).
Anxiety levels, assessed using the GAD-7 questionnaire, indicated that 24.26% of participants reported severe anxiety, with a higher prevalence among females (27.79%) compared to males (18.78%) (Table 2). These findings align with several previous studies that have reported elevated anxiety levels among female students (24, 26, 29, 43–46). However, they also contrast with other studies that found higher anxiety levels in males (47) or reported no significant gender differences (36, 48).
Analysis of perceived stress levels showed that 19.17% of students reported high stress, with a higher prevalence observed among females (22.43%) compared to males (14.08%) (Table 2). The findings are in line with the research (29, 35, 41, 49–51) but in contrast to others (36, 52–54). Gender was found to be significantly associated with anxiety (OR = 1.68, p = 0.0001) and stress (OR =1.65, p = 0.0007), highlighting differing susceptibilities between males and females (Table 3). Furthermore, the study identified positive correlations between depression and stress (r = 0.6322), anxiety and stress (r = 0.6824), and depression and anxiety (r = 0.8064). These correlations suggest that higher stress levels were associated with increased levels of depression and anxiety among the surveyed college students (Table 4). The results were found to be consistent with previous studies (55–57); however, several studies present alternative views on the relationship between gender, stress, anxiety, and depression among college students (24, 25, 58).
One might wonder why college students, in particular, experience such high levels of stress. Kashmir has long been a region marked by political instability, prolonged conflict, and socioeconomic uncertainty, factors that have significantly impacted the psychological well-being of its population. Over the past two decades, there has been a notable rise in psychiatric morbidity, with depression emerging as a particularly widespread concern (11). Beyond the broader geopolitical context, several personal, academic, and social factors also contribute to student stress. These include academic overload, personal medical history, family background of chronic or mental illness, and dissatisfaction with body image or overall life satisfaction, all of which have been associated with increased risk of depression and anxiety (16, 59). Poor family relationships have been specifically linked to depressive symptoms. Moreover, predictors of academic stress among adolescent girls include introverted personality traits, religious affiliation, having an illiterate father, and pursuing academic streams such as commerce (60). These findings underscore that student mental health is influenced by a complex interplay of individual, familial, academic, and sociocultural factors. In a conflict-affected setting like Kashmir, such stressors are likely to be intensified, making it essential to examine the mental health of college students within this unique and sensitive context.
Strengths, limitations & future implications
Concerning the strengths of our study, firstly, to our knowledge, this is the first study to explore the prevalence of stress, anxiety, and depression among students in the Kashmiri population. Secondly, we collected data from a large number of students to accurately determine the prevalence of these conditions. Thirdly, we utilized validated and reliable measurement tools to ensure the accuracy and consistency of our findings.
This study has a few limitations that should be considered. First, we did not analyze differences across academic streams or semesters, which may influence outcomes. Secondly, although standardized tools (PHQ-9, GAD-7, and PSS) were used, reliance on self-reported data may introduce response bias. The sampling approach, combining random college selection with convenience sampling of students, may involve some selection bias, though efforts were made to ensure diversity. Since the study was cross-sectional, it cannot show cause-and-effect relationships. Additionally, online data collection may have introduced minor access or attention biases, and real-time support for distressed participants was not feasible due to anonymity. Finally, no correction for multiple comparisons (e.g., Bonferroni) was applied, which may increase the risk of Type I error.
Despite these limitations, our findings offer valuable insights into the mental health status of college students in Kashmir and highlight directions for future research. Further studies are needed to explore these associations more deeply to determine whether true relationships exist or were missed due to study design. This study emphasizes the urgent need for targeted interventions addressing depression, anxiety, and stress among college students. Implementing comprehensive mental health programs within educational institutions could help reduce these conditions and enhance student well-being. In addition, longitudinal studies are recommended to monitor mental health trends over time, while qualitative research could provide a deeper understanding of students’ lived experiences and coping strategies. Future research should also assess the real-world effectiveness of such interventions and explore additional factors contributing to mental health disparities in this population.
Conclusion
This study highlights the significant mental health challenges faced by college students in Kashmir, with high prevalence rates of depression, anxiety, and stress. The findings underscore the urgent need for targeted interventions within educational institutions to support student well-being. A concrete recommendation is the implementation of on-campus mental health programs, including regular counseling services, stress management workshops, and peer support initiatives. These efforts should be integrated into the academic curriculum to reduce stigma and promote emotional well-being among students.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statement
The studies involving humans were approved by Institutional Ethical Board, Sri Pratap College. The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
Author contributions
AS: Conceptualization, Investigation, Methodology, Visualization, Writing – original draft. SR: Methodology, Writing – original draft. TM: Methodology, Writing – original draft. BS:Methodology, Writing – original draft. SeS: Methodology, Visualization, Writing – review & editing. AP: Formal analysis, Methodology, Visualization, Writing – review & editing. SrS: Formal analysis, Methodology, Writing – review & editing. MB:Investigation, Validation, Visualization, Writing – review & editing. SM: Conceptualization, Data curation, Software, Supervision, Visualization, Writing – original draft, Writing – review & editing.
Funding
The author(s) declare that no financial support was received for the research, and/or publication of this article.
Acknowledgments
The authors extend their sincere gratitude to all participants for their invaluable contribution of data, which was essential for the successful completion of this study.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Generative AI statement
The author(s) declare that no Generative AI was used in the creation of this manuscript.
Any alternative text (alt text) provided alongside figures in this article has been generated by Frontiers with the support of artificial intelligence and reasonable efforts have been made to ensure accuracy, including review by the authors wherever possible. If you identify any issues, please contact us.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpsyt.2025.1633452/full#supplementary-material
Abbreviations
MDD, Major Depressive Disorder; DSM-5, Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition; PHQ-9, Patient Health Questionnaire-9; GAD-7, Generalized Anxiety Disorder Assessment-7; IEC, Institutional Ethical Committee; SD, Standard Deviation; OR, Odds Ratio; CI, Confidence Interval; MLR, Multiple Logistic Regression; AOR, Adjusted Odds Ratio.
References
1. Pushap AC, Sudershan A, Sudershan S, Sharma A, Younis M, Bhagat S, et al. Stress among college students is linked to headache, PCOS, hypertension, and depression: A cross-sectional study. Psychol Behav Sci Int J. (2022) 20:556031. doi: 10.19080/PBSIJ.2022.20.556031
2. Pedrelli P, Nyer M, Yeung A, Zulauf C, and Wilens T. College students: mental health problems and treatment considerations. Acad psychiatry: J Am Assoc Directors Psychiatr Residency Training Assoc Acad Psychiatry. (2015) 39:503–11. doi: 10.1007/s40596-014-0205-9
3. Barbayannis G, Bandari M, Zheng X, Baquerizo H, Pecor KW, and Ming X. Academic stress and mental well-being in college students: correlations, affected groups, and COVID-19. Front Psychol. (2022) 13:886344. doi: 10.3389/fpsyg.2022.886344
4. Housen T, Lenglet A, Ariti C, Shah S, Shah H, Ara S, et al. Prevalence of anxiety, depression and post-traumatic stress disorder in the Kashmir Valley. BMJ Global Health. (2017) 2:e000419. doi: 10.1136/bmjgh-2017-000419
5. Shoib S, Islam SMS, Arafat SY, and Hakak SA. Depression and suicidal ideation among the geriatric population of Kashmir, India. Int J Soc Psychiatry. (2021) 67:651–5. doi: 10.1177/0020764020968592
6. Bashir A, Khurshid S, Altaf M, Bhatia T, Singh R, and Shoib S. Assessment of anxiety and depression among adult population of kashmir, India: A cross-sectional study. J Clin Diagn research: JCDR. (2022) 16:25–9. doi: 10.7860/jcdr/2022/53746.16649
7. Levis B, Benedetti A, Thombs BD, and DEPRESsion Screening Data (DEPRESSD) Collaboration. Accuracy of Patient Health Questionnaire-9 (PHQ-9) for screening to detect major depression: individual participant data meta-analysis. BMJ (Clinical Res ed.). (2019) 365:l1476. doi: 10.1136/bmj.l1476
8. Spitzer RL, Kroenke K, Williams JB, and Löwe B. A brief measure for assessing generalized anxiety disorder: the GAD-7. Arch Internal Med. (2006) 166:1092–7. doi: 10.1001/archinte.166.10.1092
9. Dalky HF and Gharaibeh A. Depression, anxiety, and stress among college students in Jordan and their need for mental health services. In. Nurs Forum. (2019) 54:205–12. doi: 10.1111/nuf.12316
10. Qounsar T and Parveen A. Prevalence of anxiety among adolescents in Kashmir Division. Int J Creative Res Thoughts (IJCRT). (2001) 6:32–8.
11. Amin S and Khan AW. Life in conflict: characteristics of depression in kashmir. Int J Health Sci. (2009) 3:213–23.
12. Sideeq K, Ayub T, and Nazir U. Prevalence of generalized anxiety disorder among the patients attending a peripheral health center in Kashmir Valley. Age. (2017) 20:21–30.
13. Deb S, Banu PR, Thomas S, Vardhan RV, Rao PT, and Khawaja N. Depression among Indian university students and its association with perceived university academic environment, living arrangements and personal issues. Asian J Psychiatry. (2016) 23:108–17. doi: 10.1016/j.ajp.2016.07.010
14. Shah TD and Pol T. Prevalence of depression and anxiety in college students. J Ment Health Hum Behav. (2020) 25:10–3. doi: 10.4103/jmhhb.jmhhb_16_20
15. Honnekeri BS, Goel A, Umate M, Shah N, and De Sousa A. Social anxiety and Internet socialization in Indian undergraduate students: An exploratory study. Asian J Psychiatry. (2017) 27:115–20. doi: 10.1016/j.ajp.2017.02.021
16. Taneja N, Sachdeva S, and Dwivedi N. Assessment of depression, anxiety, and stress among medical students enrolled in a medical college of New Delhi, India. Indian J Soc Psychiatry. (2018) 34:157–62. doi: 10.4103/ijsp.ijsp_114_17
17. Amaro P, Fonseca C, Afonso A, Jacinto G, Gomes L, Pereira H, et al. Depression and anxiety of Portuguese university students: A cross-sectional study about prevalence and associated factors. Depression Anxiety. (2024) 2024:5528350. doi: 10.1155/2024/5528350
18. Yan LH, Xie MY, and Yang Q. A mixed-methods study to evaluate depression and anxiety among undergraduate nursing students. J Psychiatr Ment Health Nurs. (2025) 32:364–70. doi: 10.1111/jpm.13117
19. Beshr MS, Beshr IA, and Al-Qubati H. The prevalence of depression and anxiety among medical students in Yemen: a cross-sectional study. J Affect Disord. (2024) 352:366–70. doi: 10.1016/j.jad.2024.02.080
20. Mahdavinoor SMM, Moghimi B, Mollaei A, Teimouri M, Abedi Yarandi MS, Loveneh Nasab P, et al. Prevalence and factors related with depression in Iranian university students: a large sample cross-sectional study. Middle East Curr Psychiatry. (2025) 32:24. doi: 10.1186/s43045-025-00517-x
21. Kaur S, Deepti SS, and Lal M. Prevalence and correlates of depression among college going students of district Amritsar, India. Int Res J Med Sci. (2014) 2:5–9.
22. Karmakar T and Behera SK. Depression among the college students: an empirical study. Educ Quest-An Int J Educ Appl Soc Sci. (2017) 8:163–70. doi: 10.5958/2230-7311.2017.00024.1
23. Kumar SG, Kattimani S, Sarkar S, and Kar SS. Prevalence of depression and its relation to stress level among medical students in Puducherry, India. Ind Psychiatry J. (2017) 26:86–90. doi: 10.4103/ipj.ipj_45_15
24. Eisenberg D, Gollust SE, Golberstein E, and Hefner JL. Prevalence and correlates of depression, anxiety, and suicidality among university students. Am J orthopsychiatry. (2007) 77:534–42. doi: 10.1037/0002-9432.77.4.534
25. González HM, Tarraf W, Whitfield KE, and Vega WA. The epidemiology of major depression and ethnicity in the United States. J Psychiatr Res. (2010) 44:1043–51. doi: 10.1016/j.jpsychires.2010.03.017
26. Sharma P and Kirmani MN. Exploring depression & anxiety among college going students. . Int J Sci Res. (2015) 4:528–32.
27. Yadav R, Gupta S, and Malhotra AK. A cross sectional study on depression, anxiety and their associated factors among medical students in Jhansi, Uttar Pradesh, India. Int J Community Med Public Health. (2016) 3:1209–14. doi: 10.18203/2394-6040.ijcmph20161386
28. Kuehner C. Why is depression more common among women than among men? Lancet Psychiatry. (2017) 4:146–58. doi: 10.1016/S2215-0366(16)30263-2
29. Iqbal S, Gupta S, and Venkatarao E. Stress, anxiety & depression among medical undergraduate students & their socio-demographic correlates. Indian J Med Res. (2015) 141:354–7. doi: 10.4103/0971-5916.156571
30. Kumar S, Natarajan K, Yogesh B, and Chandra R. Assessment of depression and its correlates among college students in Rishikesh Uttarakhand. Indian J Community Health. (2019) 31:220–5. doi: 10.47203/IJCH.2019.v31i02.011
31. Gavurova B, Ivankova V, Rigelsky M, Mudarri T, and Miovsky M. Somatic symptoms, anxiety, and depression among college students in the Czech Republic and Slovakia: a cross-sectional study. Front Public Health. (2022) 10:859107. doi: 10.3389/fpubh.2022.859107
32. Dutta G, Rajendran N, Kumar T, Varthya SB, and Rajendran V. Prevalence of depression among undergraduate medical students in India: A systemic review and meta-analysis. Cureus. (2023) 15:e33590. doi: 10.7759/cureus.33590
33. Gupta S, Das S, Das M, Banerjee S, Neogi R, and Mukherjee S. Prevalence and correlates of depression, anxiety, and stress among high school students in a block of Hooghly district, West Bengal: Across-sectional study. J Educ Health Promotion. (2023) 12:345. doi: 10.4103/jehp.jehp_1769_22
34. Gulland A. Women have higher rates of mental disorders than men, NHS survey finds. BMJ (Clinical Res ed.). (2016) 354:i5320. doi: 10.1136/bmj.i5320
35. Gao W, Ping S, and Liu X. Gender differences in depression, anxiety, and stress among college students: a longitudinal study from China. J Affect Disord. (2020) 263:292–300. doi: 10.1016/j.jad.2019.11.121
36. Sravani A, Doshi D, Kulkarni S, Reddy P, and Reddy S. Depression, anxiety, and stress among undergraduate dental students in Hyderabad City, Telangana, India: A cross-sectional study. J Indian Assoc Public Health Dentistry. (2018) 16:26–9. doi: 10.4103/jiaphd.jiaphd_10_17
37. Bagvadiya RV and Jansari A. Depression among college students. Int J Indian Psychol. (2022) 10:1150–5.
38. Edwards MJ and Holden RR. Coping, meaning in life, and suicidal manifestations: Examining gender differences. J Clin Psychol. (2001) 57:1517–34. doi: 10.1002/jclp.1114
39. Dahlin M, Joneborg N, and Runeson B. Stress and depression among medical students: A cross-sectional study. Med Educ. (2005) 39:594–604. doi: 10.1111/j.1365-2929.2005.02176.x
40. Wong JG, Cheung EP, Chan KK, Ma KK, and Wa Tang S. Web-based survey of depression, anxiety and stress in first-year tertiary education students in Hong Kong. Aust New Z J Psychiatry. (2006) 40:777–82. doi: 10.1080/j.1440-1614.2006.01883.x
41. Al-Qaisy LM. The relation of depression and anxiety in academic achievement among group of university students. Int J Psychol counselling. (2011) 3:96–100.
42. Arora R, Kataria L, Shah S, Tanna K, Joshi D, Chhasatia AS, et al. Study of depression among Indian college youth. Journal of Evolution of Medical and Dental Sciences. 3. (2014), 416–21. doi: 10.14260/jemds/2014/1844
43. Dyrbye LN, Thomas MR, and Shanafelt TD. Systematic review of depression, anxiety, and other indicators of psychological distress among US and Canadian medical students. Acad Med. (2006) 81:354–73. doi: 10.1097/00001888-200604000-00009
44. McLean CP and Anderson ER. Brave men and timid women? A review of the gender differences in fear and anxiety. Clin Psychol Rev. (2009) 29:496–505. doi: 10.1016/j.cpr.2009.05.003
45. Eaton NR, Keyes KM, Krueger RF, Balsis S, Skodol AE, Markon KE, et al. An invariant dimensional liability model of gender differences in mental disorder prevalence: evidence from a national sample. J Abnormal Psychol. (2012) 121:282–8. doi: 10.1037/a0024780
46. Biswas S and Biswas A. Anxiety level among students of different college and universities in India during lock down in connection to the COVID-19 pandemic. J Public Health. (2021), 1–7.
47. Chapell MS, Blanding ZB, Silverstein ME, Takahashi M, Newman B, Gubi A, et al. Test anxiety and academic performance in undergraduate and graduate students. J Educ Psychol. (2005) 97:268–74. doi: 10.1037/0022-0663.97.2.268
48. Liu CH, Stevens C, Wong SH, Yasui M, and Chen JA. The prevalence and predictors of mental health diagnoses and suicide among US college students: Implications for addressing disparities in service use. Depression Anxiety. (2019) 36:8–17. doi: 10.1002/da.22830
49. Matud MP. Gender differences in stress and coping styles. Pers Individ Dif. (2004) 37:1401–15. doi: 10.1016/j.paid.2004.01.010
50. DeCesare M. Statistics anxiety” Among sociology majors: A first diagnosis and some treatment options. Teach Sociology. (2007) 35:360–7. doi: 10.1177/0092055X0703500405
51. Manjareeka M, Kanungo P, Yadav S, and Das RC. Social Risk Factors Contributing to Anxiety, Depression and Stress among Indian Healthcare Students during Lockdown. Open Public Health J. (2024) 17. doi: 10.2174/0118749445280047240108070649
52. Mandap CM. Examining gender differences in statistics anxiety among college students. Int J Educ Res. (2016) 4:358–66.
53. Baloğlu M. Individual differences in statistics anxiety among college students. Pers Individ Dif. (2003) 34:855–65. doi: 10.1016/S0191-8869(02)00076-4
54. Hsiao TY and Chiang S. Gender differences in statistics anxiety among graduate students learning English as a foreign language. Soc Behav Personality: Int J. (2011) 39:41–3. doi: 10.2224/sbp.2011.39.1.41
55. Bayram N and Bilgel N. The prevalence and socio-demographic correlations of depression, anxiety and stress among a group of university students. Soc Psychiatry Psychiatr Epidemiol. (2008) 43:667–72. doi: 10.1007/s00127-008-0345-x
56. Cummings CM, Caporino NE, and Kendall PC. Comorbidity of anxiety and depression in children and adolescents: 20 years after. psychol Bull. (2014) 140:816–45. doi: 10.1037/a0034733
57. Beiter R, Nash R, McCrady M, Rhoades D, Linscomb M, Clarahan M, et al. The prevalence and correlates of depression, anxiety, and stress in a sample of college students. J Affect Disord. (2015) 173:90–6. doi: 10.1016/j.jad.2014.10.054
58. Bewick B, Koutsopoulou G, Miles J, Slaa E, and Barkham M. Changes in undergraduate students’ psychological well-being as they progress through university. Stud higher Educ. (2010) 35:633–45. doi: 10.1080/03075070903216643
59. Jayanthi P, Thirunavukarasu M, and Rajkumar R. Academic stress and depression among adolescents: a cross-sectional study. Indian Pediatr. (2015) 52:217–9. doi: 10.1007/s13312-015-0609-y
Keywords: depression, anxiety, kashmiri population, prevalence, epidemiological study
Citation: Sudershan A, Rehman S, Manzoor T, Shaban B, Sultan S, Pushap AC, Sudershan S, Bashir M and Malik SA (2025) Depression, anxiety, and stress among college students: a Kashmir-based epidemiological study. Front. Psychiatry 16:1633452. doi: 10.3389/fpsyt.2025.1633452
Received: 22 May 2025; Accepted: 14 August 2025;
Published: 10 September 2025.
Edited by:
Tamkeen Saleem, Shifa Tameer-e-Millat University, PakistanReviewed by:
Hongyu Xu, Virginia Commonwealth University, United StatesBilal Para, Islamic University of Science and Technology Kashmir, India
Kalai Vani, Tunku Abdul Rahman University, Malaysia
Copyright © 2025 Sudershan, Rehman, Manzoor, Shaban, Sultan, Pushap, Sudershan, Bashir and Malik. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Showkat Ahmad Malik, bWFsaWsuc2hvd2thdDE5ODhAZ21haWwuY29t