 Mónika Gálber1†
Mónika Gálber1† Szilvia Anett Nagy1,2,3,4†
Szilvia Anett Nagy1,2,3,4† Gergely Orsi2,3,4
Gergely Orsi2,3,4 Gábor Perlaki2,3,4,5
Gábor Perlaki2,3,4,5 Tamás Tényi6
Tamás Tényi6 Boldizsár Czéh1,7*
Boldizsár Czéh1,7* Maria Simon1,6
Maria Simon1,6- 1Neurobiology of Stress Research Group, Szentágothai Research Centre, University of Pécs, Pécs, Hungary
- 2HUN-REN-PTE Clinical Neuroscience MR Research Group, Pécs, Hungary
- 3Department of Neurology, Medical School, University of Pécs, Pécs, Hungary
- 4Pécs Diagnostic Centre, Pécs, Hungary
- 5Department of Neurosurgery, Medical School, University of Pécs, Pécs, Hungary
- 6Department of Psychiatry and Psychotherapy, Medical School, University of Pécs, Pécs, Hungary
- 7Department of Laboratory Medicine, Medical School, University of Pécs, Pécs, Hungary
Background: Previous studies indicate that hippocampal (subfield) and amygdala volumes may correlate with specific cognitive functions, coping strategies and emotion regulation. Here, we investigated associations between emotional processing and volumes of hippocampal subfields and amygdala. We focused on depressed patients since emotional dysregulation and hippocampal volume shrinkage are characteristic of them. Our hypothesis was that in depressed individuals, maladaptive emotional behaviors will correlate with hippocampal and amygdala volume shrinkage.
Methods: We recruited depressed patients with a history of childhood maltreatment (n=21), depressed patients without maltreatment (n=18), and matched controls (n=21). Their brains were imaged with magnetic resonance imaging and area reconstruction was performed with the FreeSurfer software. History of maltreatment was assessed with Childhood Trauma Questionnaire (CTQ). Emotion processing difficulties were evaluated using the Cognitive Emotion Regulation Questionnaire (CERQ), Difficulties in Emotion Regulation Scale (DERS), Toronto Alexithymia Scale (TAS) and Reading the Mind in the Eyes Test (RMET).
Results: Depressed patients, especially maltreated subjects had small, but nonsignificant hippocampal and amygdala volume decrease (≤10%) and displayed pronounced difficulties in emotion regulation. In maltreated individuals, we found positive correlations between CERQ–rumination and volume of the right CA3, as well as between CERQ–positive-reappraisal and volume of the left presubiculum. In maltreated individuals, CTQ–emotional-abuse scores showed positive correlation with amygdala volumes of both hemispheres. In non-maltreated depressed patients, we found negative correlations between CERQ–rumination and volumes of the right hippocampus and amygdala, as well as several subfields of the right hippocampus. Furthermore, in non-maltreated depressed patients, CTQ–emotional-neglect had a positive correlation with the volume of the right CA3. Overall, among the tests, CERQ–rumination scores had the largest number of correlations with hippocampal subfield volumes mainly in non-maltreated depressed subjects. We found no correlation between alexithymia and brain area. Amygdala volumes had very few correlations, and only with CERQ and CTQ scores.
Limitations: Relatively small sample size, cross-sectional design, retrospective self-report questionnaire to assess adverse childhood experiences and no amygdala subnuclei segmentation.
Conclusions: We could not confirm our hypothesis that maladaptive emotional behavior is associated with hippocampal volume shrinkage. Future studies should preferably focus on functional neuroimaging when examining complex emotional phenomena.
1 Introduction
The hippocampal complex plays a vital role in the formation and retrieval of declarative episodic memories, as well as in spatial learning and navigation. Besides these well-documented functions, the hippocampus has a significant role in social cognition and behavior (1, 2). In the context of emotional situations, it interacts with the amygdala (3), and together, they are key integrators of emotion and cognition, a function that is particularly vulnerable in mental disorders (4, 5). Furthermore, functional magnetic resonance imaging (MRI) studies provide direct evidence that the hippocampus is a crucial component of the emotional brain network and play a vital role in emotion processing (6).
Neuroanatomists divide the human hippocampal formation into several subfields, such as the dentate gyrus (DG), Cornu Ammonis (CA1, CA2, CA3, and CA4), and the subicular complex. Additionally, several further dimensions exist, e.g. the medial-lateral and longitudinal dimensions (7). Specific functions are attributed to each subfield, for example, numerous roles in learning and memory are accredited to the DG (8, 9), the CA3 area is important for the rapid encoding of memory (10) and in encoding of new spatial information within the short-term memory (11). Furthermore, a special role in social recognition memory is accredited to the CA2 region (12).
There has been ongoing interest in measuring the volumes of different hippocampal subfields and correlating them with disease pathology or with various aspects of cognitive and emotional regulation (e.g. 13–19). We should however emphasize that correlating brain area volumes with psychological functioning is a controversial scientific approach since experiments that aim to link morphology with complex behavior often yield ambiguous results (15). There is a widely held notion in the literature that hippocampal volume can be linked to cognition and that reduced hippocampal volume due to aging or a mental disorder such as schizophrenia, depression or post-traumatic stress disorder, results in hippocampal dependent cognitive deficits. However, there is clinical evidence that confront this notion of causality and raise the possibility that pre-determined inter-individual differences in hippocampal volume may in fact determine the vulnerability to psychopathology or age-related cognitive impairments (20, 21).
The aim of our current study was to further investigate potential correlations between the volumes of hippocampal subfields and the amygdala in relation to emotional processing. To examine these questions, we focused on patients with major depressive disorder (MDD) who have a history of childhood maltreatment (CM). We studied this population since they typically have difficulties with emotion regulation, and changes in hippocampal and amygdala volumes are often observed in these individuals (17, 22–30).
Participants of the present study completed five psychological questionnaires. Four of these assessments have been specifically developed to measure difficulties in regulating or recognizing emotions. The Difficulties in Emotion Regulation Scale (DERS) assessed the severity of emotional dysregulation. The Cognitive Emotion Regulation Questionnaire (CERQ) was used to evaluate the cognitive coping strategies employed in response to stressful life events. The presence and severity of alexithymia were assessed with the 20-item Toronto Alexithymia Scale (TAS). To assess the ability to identify facial emotional expressions, we utilized the Reading the Mind in the Eyes Test (RMET), which displays only the eye region of the face expressing complex emotions. Finally, the Childhood Trauma Questionnaire (CTQ) was employed to assess participants’ history and severity of childhood abuse and neglect.
Emotion dysregulation is a fundamental feature of mood disorders. In this study, we utilized the DERS, a widely recognized self-report questionnaire designed to assess individuals’ difficulties in recognizing and managing negative emotions (31). This scale has been proven to be reliable in research involving psychiatric patients (32). Individuals, who have experienced childhood maltreatment, often face difficulties with emotion regulation (33). Furthermore, challenges in emotion regulation have been linked to the volumes of hippocampal subfields (19, 34).
The CERQ is a widely used multidimensional tool constructed to identify the cognitive coping strategies in response to negative life events (35). Recent studies suggest that the volumes of hippocampal subfields are positively associated with the use of some specific coping strategies for cognitive emotional regulation in healthy individuals and in patients with mild cognitive impairment (19, 36).
The TAS had been specifically developed to assess alexithymia (37, 38). Although the test is not without controversy, existing evidence suggests that it is a reliable and valid instrument for measuring deficits in emotional awareness and expression (39). Several neuroimaging studies have explored the relationship between alexithymia and gray matter volume of brain areas involved in emotion processing; however, the neuroanatomical basis of alexithymia remains unclear, as previous studies yielded contradictory findings (40). For example, an early study involving healthy volunteers found that individuals with high levels of alexithymia had less gray matter volume in the amygdala and several other emotion-relevant brain areas (41). In contrast, another study indicated a positive association between alexithymia and amygdala volume (42). More recently, a study comparing depressed patients with control subjects reported that higher alexithymia scores were linked to decreased grey matter volume of the fusiform gyrus in depressed individuals, while the opposite was found in healthy controls (43). Overall, a meta-analysis of the available data concluded that individuals with high levels of alexithymia consistently exhibited smaller volumes of the left insula, left amygdala, orbital frontal cortex and striatum (40).
The Reading the Mind in the Eyes Test is a widely recognized assessment tool to evaluate theory of mind (ToM) abilities, i.e. the capacity to represent other people’s mind (“mentalizing”) (44). However, this concept has been challenged by researchers who argue that this test relies heavily on the recognition of facial emotional expression which is often impaired in individuals with alexithymia, and several studies indicate a correlation between greater levels of alexithymia and poorer performance on the RMET (45, 46). Notably, impaired performance on the RMET has been documented in abused children (47), as well as in adults with a history of childhood adversity (48), and in depressed patients with adverse childhood experiences (49–51). Furthermore, several neuroimaging studies explored the relationship between brain structure and RMET performance (52–55). Some of these studies found that larger volumes of the amygdala and/or hippocampus were associated with better performance in the RMET (52, 54).
The Childhood Trauma Questionnaire, developed by Bernstein and co-workers in 2003, is one of the most widely used and validated tools for assessing childhood maltreatment. This retrospective self-report questionnaire evaluates various types of childhood maltreatment, categorized into five dimensions: emotional, physical, sexual abuse, and emotional and physical neglect (56). Although there is a debate about the best methods to measure childhood maltreatment, a recent critical appraisal of the available 52 instruments concluded that CTQ is the only scale that has been thoroughly investigated and demonstrated a strong level of evidence with adequate internal consistency, reliability, content validity, structural validity, and convergent validity (57).
The aim of the present study was to further explore the putative associations between emotion processing and volumes of hippocampal subfields and amygdala. To address these questions, we recruited MDD patients with or without a history of childhood maltreatment and compared their data to that of healthy individuals, who had never experienced a depressive episode. We formulated three hypotheses: 1) patients with MDD, especially the maltreated individuals, will have reduced hippocampal volumes; 2) they will exhibit maladaptive emotion processing, and 3) this maladaptive emotion processing will correlate with the volume reduction of the hippocampus and/or the amygdala.
2 Materials and methods
2.1 Study design and participants
This cross-sectional study involved a total of 60 subjects (40 females). The age range of the subjects was between 18 and 54 years (mean ± SD = 33.5 ± 8.512). Participants diagnosed with MDD were recruited from the Affective Disorder Unit of the Department of Psychiatry and Psychotherapy, Clinical Centre, University of Pécs. Participants with MDD were categorized into two subgroups based on their history of childhood maltreatment (CM). The MDD+CM group included those with moderate to severe CM (N = 21; 14 females), while the non-maltreated MDD group consisted of individuals with a low incidence of childhood maltreatment (N = 18, 12 females). Additionally, a healthy control (HC) group was formed, consisting of subjects matched in age and IQ, with no history of mental disorders (N = 21, 14 females). In the HC group, the Symptom-Checklist-90-R (58, 59) was applied to rule out subthreshold psychiatric symptoms. The detailed demographic data of the three experimental groups are presented in Table 1.
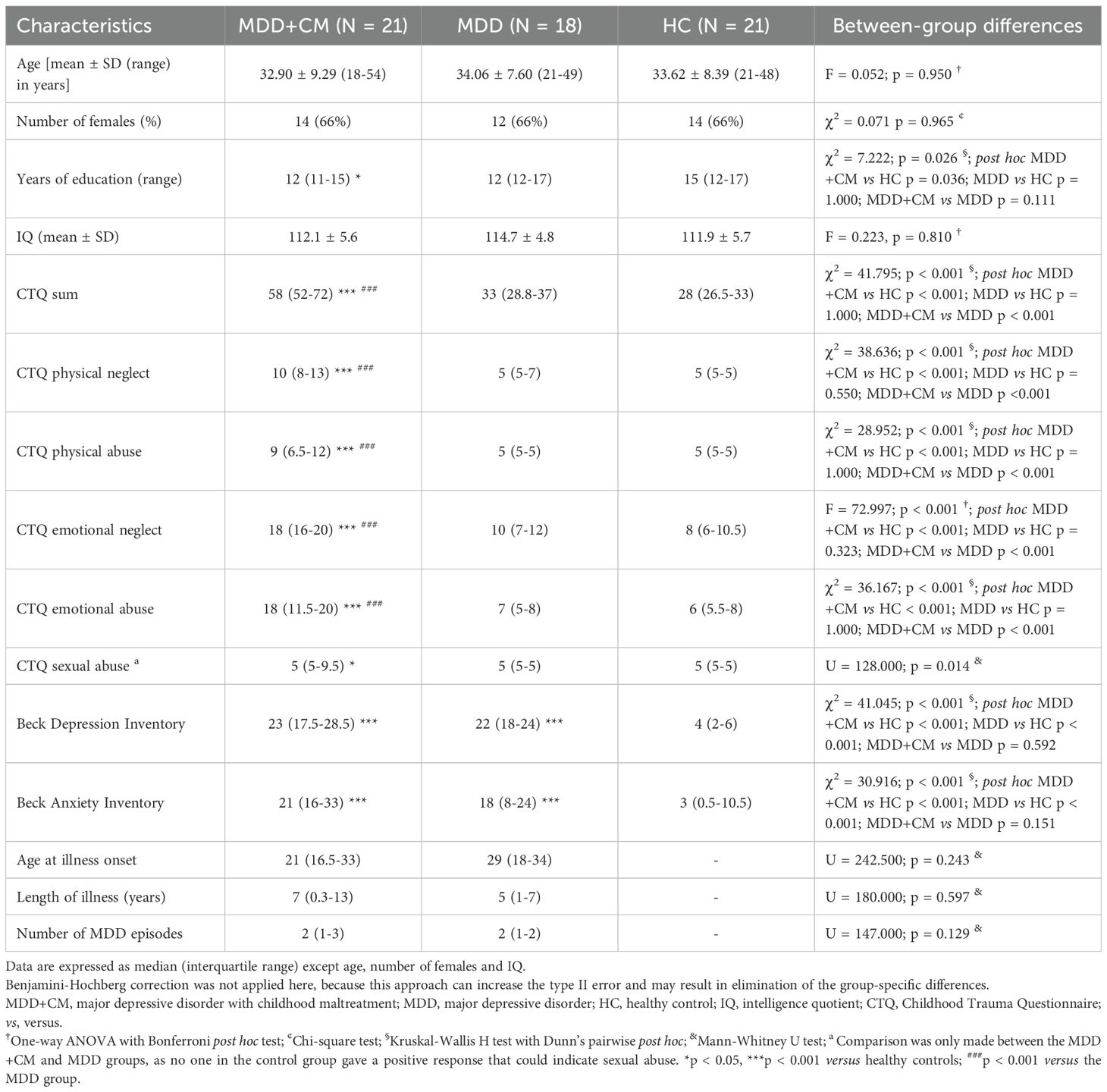
Table 1. Demographics and assessments of childhood maltreatment and neuropsychiatric status.
The exclusion criteria for participation were as follows: current substance use (abstinence for < 2 years); IQ < 85; a history of head injury; a history of any neurological or psychiatric disorders (non-excluding psychiatric disorders are summarized below); experience of traumatic life events meeting DSM-5 post-traumatic stress disorder (PTSD) criterion A; or any contraindications for MRI (i.e. claustrophobia or the presence of metal objects in the body).
In our study, non-excluding, co-morbid psychiatric disorders were: anxiety disorders (panic disorder N = 3; generalized anxiety disorder N = 3; social phobia N = 2; specific phobias N = 4); cluster C personality disorders (dependent N = 2, avoidant N = 2); obsessive-compulsive disorder in the past 6 years, and never treated when symptomatic before (N = 1); lifetime sedatives, hypnotics, and anxiolytics use disorder (N = 2) in full remission for more than 2 years; mild and non-chronic alcohol use disorder (N = 2).
In patients with MDD, the mean age of disease onset was 25.49 ± 9.47 years. The mean duration of illness was 7.15 ± 7.74 years (range 0.2–26 years). Thirty-six (97%) patients with MDD were treated with antidepressant medication: SSRIs (N = 25); SNRIs (N = 3); NaSSAs (N= 7); agomelatine (N = 4); trazodone (N= 2); combined with mood stabilizer (N = 2); combined with low-dose atypical antipsychotics (N = 5).
The local Research Ethics Committee of the University of Pécs approved the study design and protocol (Ethical Approval Nr.: 2015/5626). All participants were Hungarian speaking Caucasians, living in the urban and suburban area of Pécs, and gave written informed consent.
2.2 Neuropsychiatric assessments, psychological tests, and questionaries
All participants underwent comprehensive screening for any current or past psychiatric disorders, along with an assessment of general intelligence and emotional coping strategies and recognition using standardized neuropsychological measures.
Participants diagnosed with MDD fulfilled the DSM-5 diagnostic criteria for MDD (60), as evaluated by a trained psychiatrist (MS) using the Structured Clinical Interviews for DSM-5 disorders (SCID-5-CV and SCID-5-PD; 61, 62). The 21-item version of the Hamilton Depression Rating Scale (63) and the Beck Depression Inventory (64) were employed to evaluate the severity of depression, while the Beck Anxiety Inventory (65) was used to examine the severity of anxiety. Participants were also evaluated using the 11-item General Traumatic Experiences subscale of the 21-item Self Report Early Trauma Inventory (66) to measure causal traumatic childhood life events. Individuals with random trauma were excluded from this study. Four-subtest version of Hungarian adaptation of the Wechsler Adult Intelligence Scale-Revised was applied to test the General Intelligence Quotient (IQ; 67–69). See data for the results of the psychiatric assessments in Table 1.
2.2.1 Assessment of childhood maltreatment: Childhood Trauma Questionnaire
The history and severity of chronic and/or repeated childhood maltreatment were assessed using the self-reported, retrospective, 28-item Childhood Trauma Questionnaire (CTQ; 56). Participants had to fill out the Hungarian version of the CTQ (70, 71).
The CTQ evaluates the severity of five distinct types of maltreatment experienced prior to the age of 18: physical neglect (PN), physical abuse (PA), emotional neglect (EN), emotional abuse (EA), and sexual abuse (SA). Each subscale comprises 5 items, which participants evaluate using a 5-point Likert scale. In the present study, participants were enrolled in the MDD+CM subgroup if they obtained CTQ scores that exceeded the established cut-off values of the “low” range on any of the CTQ subscales. The cut-off values (i.e. maximum score) of the “low” range for the various subscales were as follows: physical neglect: 9; physical abuse: 9; emotional neglect: 14; emotional abuse: 12; sexual abuse: 7. For a detailed description of the assessment of childhood maltreatment see our earlier publications (50, 72, 73). A detailed summary of the CTQ results is presented in Table 1.
2.2.2 Assessment of cognitive coping strategies in response to stressful life events: Cognitive Emotion Regulation Questionnaire
CERQ is a widely used test for assessing specific emotion regulation strategies in response to threatening or stressful life events (35). We used the Hungarian version of the 36-item CERQ (74). It consists of 9 subscales, each of which represents separable emotion regulation strategies one can deploy: 1) self-blame; 2) rumination; 3) catastrophizing; 4) blaming others; 5) acceptance; 6) positive refocusing; 7) refocus on planning; 8) positive reappraisal; 9) putting into perspective, each subscale consists of 4 items.
Subscales 1, 2, 3, and 4 are categorized as maladaptive strategies because they can hinder an individual’s ability to cope effectively with stressful events. In contrast, subscales 5, 6, 7, 8, and 9 are classified as adaptive cognitive strategies that can enhance effective coping with stressful situations. Participants rated each item on a 5-point Likert scale, where 1 signifies “rarely” and 5 signifies “almost always.” Higher scores on each subscale indicate a greater tendency to use that particular emotion regulation strategy.
We calculated the “CERQ maladaptive sum” by aggregating the scores of Self-Blame, Rumination, Catastrophizing, and Blaming Others subscales. The rigid use of these maladaptive strategies may increase vulnerability to stressful life events. Therefore, they are typically associated with a range of mental health problems, including depression, and can worsen the clinical outcomes (75). Brief interpretations of these subscales are listed here. 1) Self-Blame: Frequently blaming oneself for negative events, which can lead to feelings of guilt, shame, and diminished self-esteem. 2) Rumination: The tendency to constantly dwell on negative thoughts and feelings related to a negative event. This strategy can intensify negative emotions and hinder recovery. 3) Catastrophizing: Magnifying the severity and negative consequences of an adverse event, potentially leading to heightened anxiety and distress. 4) Blaming Others: Frequently blaming others or external factors for negative events. This strategy may undermine personal responsibility and effective problem-solving. Higher scores on these maladaptive subscales suggest a greater reliance on strategies that may be detrimental to mental health.
We also calculated the “CERQ adaptive sum” which was obtained by summing the scores of Acceptance, Positive Refocusing, Refocusing on Planning, Positive Reappraisal, and Putting into Perspective subscales. The flexible implementation of adaptive emotion regulation strategies is typically associated with resilience or with a better clinical outcome. The interpretation of these adaptive strategies are as follows. Acceptance: Coming to terms with the negative event and accepting that it has happened. Positive Refocusing: Shifting attention away from negative thoughts towards more pleasant and positive thoughts. Refocus on Planning: Focusing on developing a plan of action to deal with the negative event. This can promote a sense of control and proactive problem-solving. Positive Reappraisal: Finding a positive meaning in a negative event which can promote personal growth and resilience. Putting into Perspective: Downplaying the significance of a negative event by comparing it to more significant negative events. Higher scores on adaptive subscales suggest a greater tendency to use strategies that promote positive emotional well-being.
2.2.3 Assessment of difficulties in emotion regulation: Difficulties in Emotion Regulation Scale
DERS is a widely used self-report questionnaire designed to measure challenges in emotion regulation among adults (31). Participants completed the Hungarian version of the DERS and when they reached higher scores that indicated greater difficulties (76). The scale consists of 41 items divided into six subscales: 1) Nonacceptance of Emotional Responses (DERS–nonacceptance), 2) Difficulties Engaging in Goal-Directed Behavior (DERS–goals), 3) Impulse Control Difficulties (DERS–impulse), 4) Lack of Emotional Awareness (DERS–awareness), 5) Limited Access to Emotion Regulation Strategies (DERS–strategies), and 6) Lack of Emotional Clarity (DERS–clarity).
Brief interpretations of these subscales are given here. 1) Nonacceptance of Emotional Responses: High scores on this subscale indicate that an individual may struggle with the acceptance of negative emotions, potentially leading to increased distress and difficulties in managing those emotions effectively. 2) Difficulties Engaging in Goal-Directed Behavior: Elevated scores suggest that individuals may experience challenges in maintaining focus and engaging in goal-oriented activities during periods of distress. 3) Impulse Control Difficulties: High scores suggest a tendency to impulsive actions or unconsidered reactions when experiencing emotional distress, which can increase existing challenges. 4) Lack of Emotional Awareness: This subscale measures the extent to which individuals are aware of their own emotional states. High scores indicate a deficiency in self-awareness or an unwillingness to acknowledge their emotions. 5) Limited Access to Emotion Regulation Strategies: High scores indicate a belief that few effective strategies are available to effectively manage negative emotions, leading to a diminished sense of control over emotional reactions. 6) Lack of Emotional Clarity: This subscale evaluates the extent to which individuals understand and can identify their emotions. High scores suggest that individuals may struggle to understand emotional reactions and the underlying reasons for them. Patients rated their experiences to each item on a 5-point Likert scale, where 1 indicates “rarely” and 5 “almost always”.
2.2.4 Assessment of alexithymia: Toronto Alexithymia Scale
The TAS-20 is a test designed to assess alexithymia (37, 38), although it is not without shortcomings (77). The TAS-20 has three subscales: 1) difficulty identifying feelings; 2) difficulty describing feelings; and 3) externally oriented thinking. Items are rated using 5-point Likert scales whereby 1 = strongly disagree and 5 = strongly agree. Participants completed the Hungarian version of the TAS-20 (78).
2.2.5 Assessment of face emotion recognition: Reading the Mind in the Eyes Test
All participants completed the RMET, which is widely used as a measure of social cognitive ability (79). The test comprises 36 photographs of male and female eyes illustrating emotionally charged or neutral mental states. Subjects must select which of four mental-state descriptors best matches what the person in the photograph is thinking or feeling. This test is also regarded as an advanced Theory of Mind test in which participants need to put themselves in the place of the person in the picture (44). We quantified the number of correctly identified facial expressions and classified them into emotionally charged (RMET emotional sum) and neutral expressions (RMET neutral faces). Within the emotionally charged category, we examined separately the correctly recognized negative (RMET negative emotion) and positive emotional expressions (RMET positive emotion).
2.3 Volumetric analysis with in vivo magnetic resonance imaging
2.3.1 MRI acquisition
Data were collected with a 3T Magnetom Trio TIM MRI scanner (Siemens AG, Erlangen, Germany) using a 12-channel head coil.
For the volumetric measurements, isotropic T1-weighted high-resolution images were obtained using a three-dimensional magnetization prepared rapid acquisition with gradient echo sequence (3D-MPRAGE) with the following parameters: repetition time/inversion time/echo time (TR/TI/TE): 2530/1100/3.37 ms; flip angle: 7°; number of averages: 1; field of view: 256 × 256 mm2; matrix size: 256 × 256; 176 sagittal slices with a thickness of 1.00 mm; bandwidth: 200 Hz/pixel.
2.3.2 Image processing
T1-weighted images underwent complex pre- and post-processing before the statistical analysis. First, visual quality control was performed to exclude data containing artifacts. In order to examine the relationship between the results of the psychological tests and the volume of hippocampal subfields and amygdala, cortical and subcortical reconstruction and segmentation were carried out using the FreeSurfer software 6.0 (https://surfer.nmr.mgh.harvard.edu/80). Technical details of the automated cortical and subcortical segmentation stream are described in a prior methodological study (81, 82). Talairach transformation and the removal of non-brain tissues were visually verified, and error correction was performed when necessary, based on the recommended workflow (https://surfer.nmr.mgh.harvard.edu/fswiki). Gray matter parcellation was estimated using an automated labelling procedure based on the Desikan-Killiany-Tourville Atlas (83). Segmentation and structure labelling were then confirmed and edited manually using standard procedures recommended by the FreeSurferWiki website, and recon-all was rerun to estimate the volumes.
The following bilateral hippocampal subfields were segmented from T1-weighted images: granule cell layer and molecular layer of the dentate gyrus (GCL-ML-DG), molecular layer, CA4, CA3, CA1, subiculum, presubiculum, parasubiculum, hippocampal-amygdaloid transition area, fimbria, hippocampal tail, and hippocampal fissure (https://surfer.nmr.mgh.harvard.edu/fswiki/HippocampalSubfields; 84). Subfield’s volume having a standard deviation greater than 10% of the mean were excluded from further analysis; therefore, the bilateral parasubiculum, the hippocampal-amygdaloid transition areas, fimbria, and the hippocampal fissures were ruled out. The volume of the entire hippocampus was calculated by the sum of all subregions except the hippocampal fissure, while the volume of the amygdala was obtained from subcortical segmentation output of the FreeSurfer file aseg.mgz (see Figure 1). Volumes are expressed in mm3.
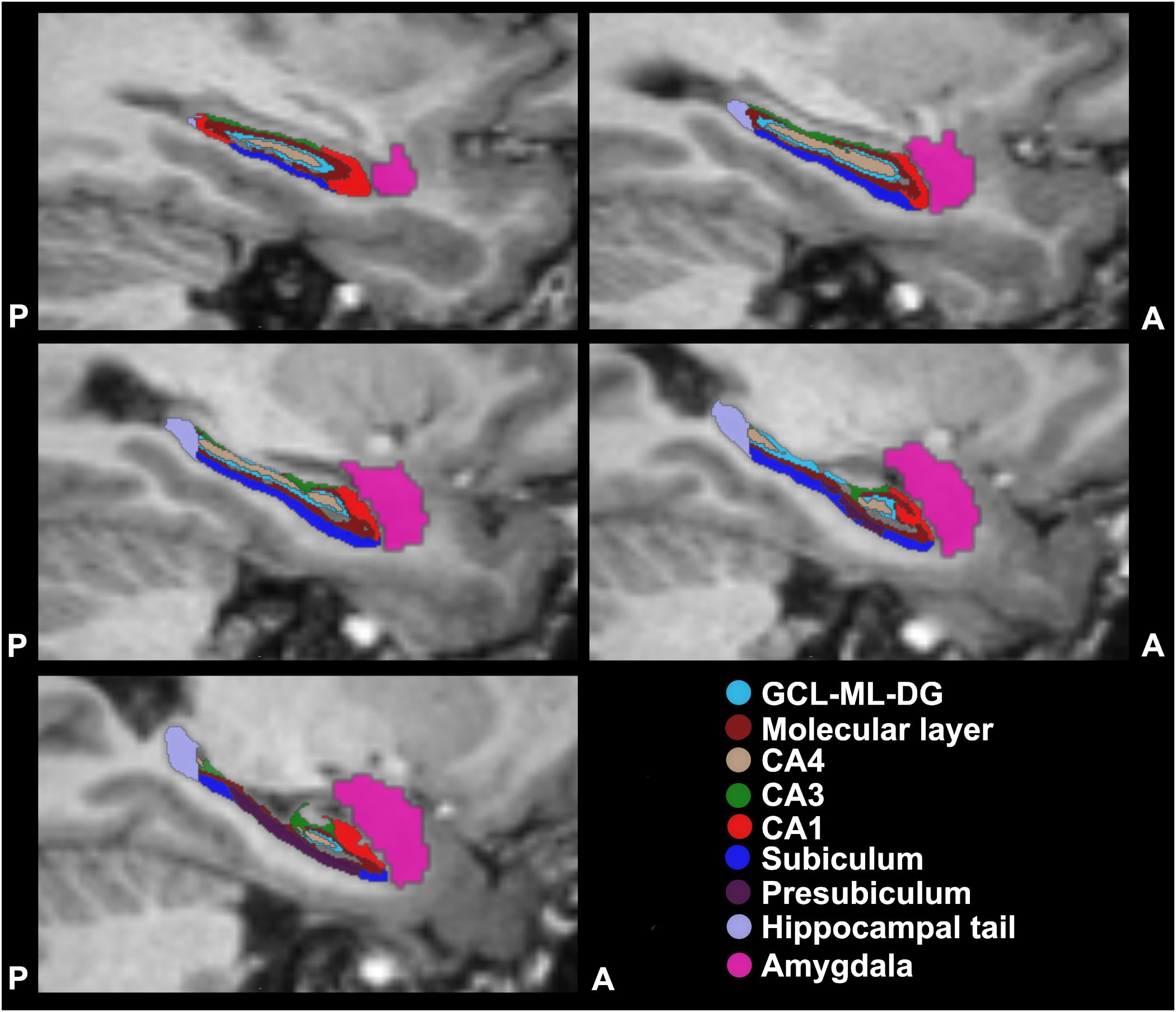
Figure 1. Reconstruction and segmentation of amygdala and hippocampal subfields. Representative T1-weighted images of reconstructed subareas from the left side of the brain. Five slices are shown here in the sagittal plane, in a direction from left to right, i.e. X = -29 to X = - 21 in the Talairach space. The segmentation was based on the ex vivo hippocampal subfield atlas described by Iglesias et al. (84). The different colours indicate different subfield areas. The reconstructed 3D volumes of the different subfields were correlated with the results of the psychological tests. A, anterior; CA, Cornu Ammonis; GCL-ML-DG, granule cell layer and molecular layer of the dentate gyrus; P, posterior.
2.4 Statistical analysis the demographic and clinical data
IBM SPSS Statistics Software version 29.0.2 was applied for data analyses. The assumptions were tested in all cases. For parametric data, one-way ANOVA with Bonferroni or Dunnett’s T3 (in case of unequal variance) post hoc test was used to compare groups for demographic, IQ and clinical variables, as well as for CERQ, DERS, TAS and RMET scores. Nonparametric data and datasets with skewed distributions were compared with the Mann-Whitney U test, as well as with the Kruskal-Wallis H test followed by Dunn’s pairwise post hoc comparison.
Given that no sexual dimorphism of hippocampal size is observed after adjusting for head size (85) and considering that the Point-Biserial Correlation revealed a relatively strong multicollinearity between estimated total intracranial volume (eTIV) and gender (rpb= -0.519, N = 60, p = 0.00002), age and eTIV were selected as regressors for subsequent statistical analyses.
Volumetric data were analyzed with one-way ANCOVA followed by Bonferroni or Dunnett’s T3 (in case of unequal variance) post hoc tests, and with Kruskal-Wallis H test followed by Dunn’s pairwise post hoc test to identify differences between groups, while controlling for age and eTIV as covariates.
The interaction effect was examined using a general linear model to determine whether there is a general between-group difference in the association of psychological parameters and brain volumes. Group, age, eTIV, psychological parameters, and the group × psychological parameter interaction term were included as independent variables. Brain volumes were used as dependent variables. If any significant findings arose, further within-group multiple linear regression analyses were conducted, while controlling for age and eTIV, to explore the relationship between volumetric data and psychological parameters. The assumptions of multiple linear regressions were satisfied, as judged by testing for linearity, normality assumptions of the residues, outliers, independence of errors, homoscedasticity, and multicollinearity (86).
The level of significance was set at two-tailed p ≤ 0.05 for all statistical tests. Uncorrected p-values are reported to facilitate comparisons with other studies. However, to address the issue of multiple comparisons, Benjamini-Hochberg correction was applied with q = 0.15 when analyzing volumetric and psychological data. P-values that survived this correction for multiple comparisons are indicated in the tables.
3 Results
3.1 Demographic data and clinical characteristics
The demographic data and the results of the psychiatric assessments are listed in Table 1. Since the individuals were carefully selected for this study, age, gender ratio, and IQ values were comparable in the three experimental groups. Maltreated MDD patients spent significantly shorter time in education compared to controls (post hoc test: p = 0.036), but they were similar to the MDD group (Table 1).
As a result of the group assignment, the CTQ scores of maltreated MDD patients (MDD+CM group) were significantly higher than those of both the non-maltreated MDD patients (MDD group) and the healthy control (HC) group across all subscales, while CTQ scores of the MDD and HC groups were very similar (Table 1). Maltreated and non-maltreated depressed patients showed much higher scores in the Beck Depression and Anxiety Inventories compared to control group. The age at illness onset, the length of illness and the number of depressed episodes were comparable in the two sub-groups of depressed patients.
3.2 Hippocampal subfield and amygdala volumes
Representative examples of T1-weighted images and the results of the automatic segmentation of the hippocampal subfields and the amygdala are depicted in Figure 1. The results of the volumetric analysis are summarized in Table 2. We observed a consistent trend for volume reduction, i.e. a shrinkage of 1-10% in nearly all hippocampal subregions of the depressed patients. However, none of these reductions were statistically significant when compared to the control group. Notably, patients who had been exposed to childhood maltreatment generally displayed smaller volumes compared to both the control group and the non-maltreated MDD group, but again, these differences did not reach statistical significance. The largest observed volume reduction (-10%) occurred in the right presubiculum, right hippocampal tail, and left amygdala of the MDD+CM group (Table 2). The least affected hippocampal region was the CA3 area of both hemispheres.
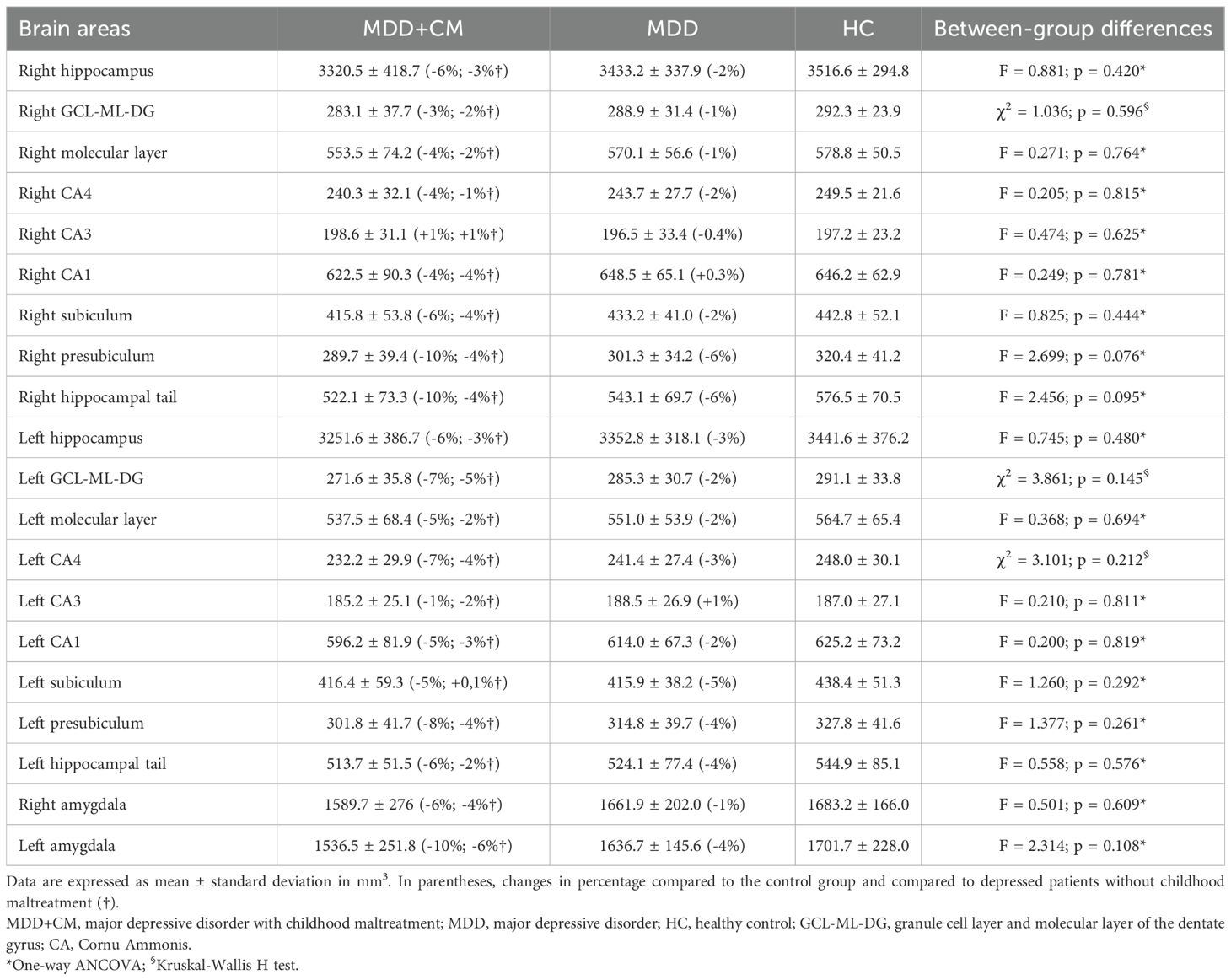
Table 2. Hippocampal subfield and amygdala volumes.
3.3 Emotion dysregulation, alexithymia, and emotion recognition
Results of the CERQ, DERS, TAS and RMET tests are presented in Table 3. In general, depressed patients, especially the ones with the history of childhood maltreatment, displayed numerous difficulties with emotion processing.
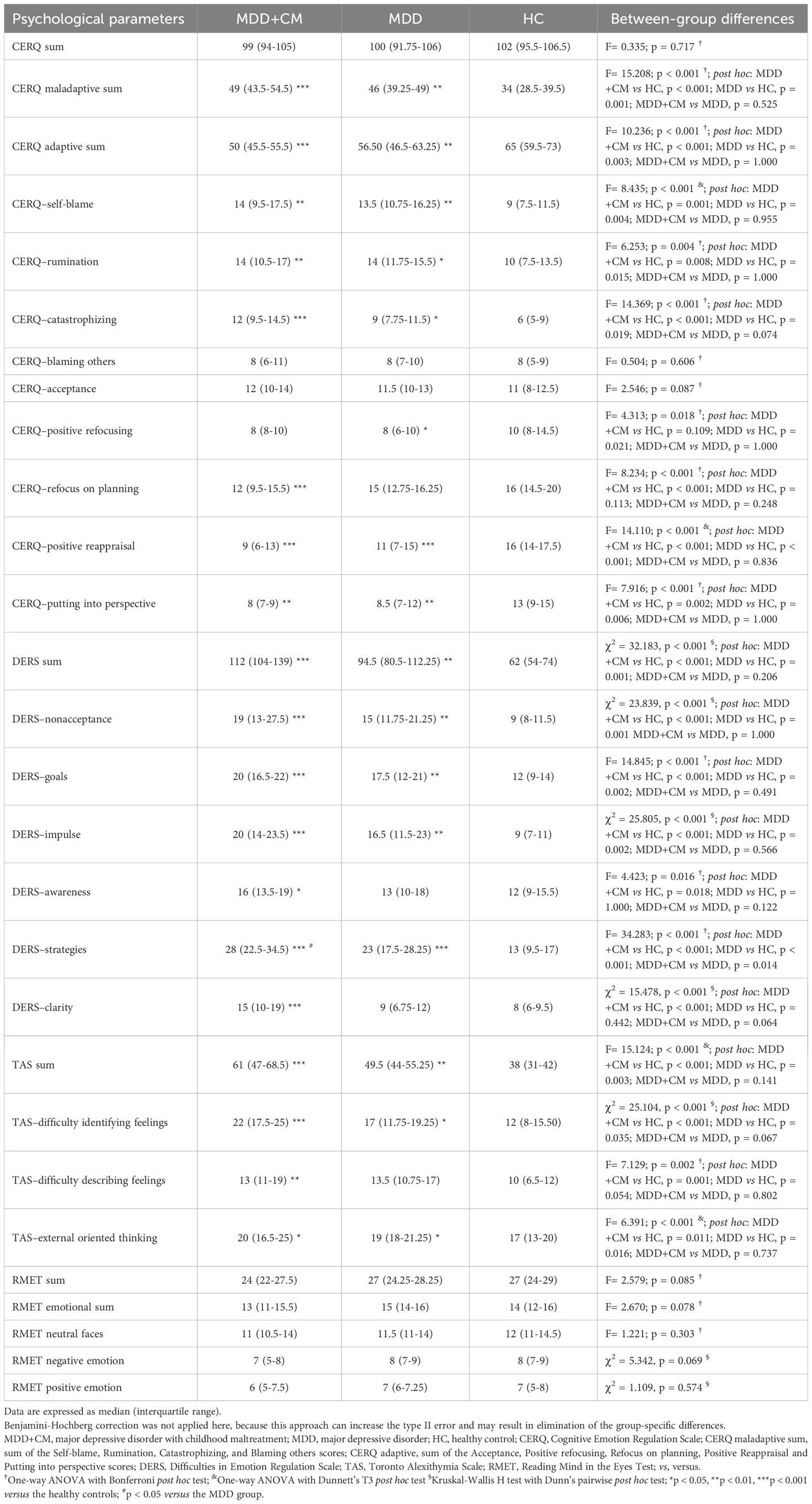
Table 3. Results of the CERQ, DERS, TAS and RMET tests.
Assessment with the Cognitive Emotion Regulation Questionnaire revealed that compared to the other two groups maltreated individuals reached the highest scores in the CERQ maladaptive sum and the lowest scores in the CERQ adaptive sum (Table 3). Maltreated patients had significantly different scores compared to controls in almost all subscales. Similarly, non-maltreated depressed individuals had significantly different scores compared to controls in most of the subscales and they also reached significantly higher scores in the CERQ maladaptive sum and significantly lower scores in the CERQ adaptive sum compared to controls (Table 3).
Results of the Difficulties in Emotion Regulation Scale indicated that maltreated individuals had the most severe difficulties with emotion regulation. They had the highest scores in DERS sum, and in all subscales, and they were always significantly different compared to controls (Table 3). Non-maltreated depressed patients also had difficulties in emotion regulation as they reached significantly higher scores in DERS sum and in most of the subscales compared to controls (Table 3).
Results of the Toronto Alexithymia Scale indicated that maltreated individuals reached the highest scores, and they were always significantly different compared to controls (Table 3). Eleven maltreated depressed individuals had equal to or greater than 61 TAS sum scores indicating alexithymia. Non-maltreated depressed patients had significantly higher TAS sum scores compared to controls and in one TAS subscale (Difficulty Identifying Feelings), they were also different compared to controls. Among the non-maltreated depressed patients, there were two subjects who had 61≤ TAS sum scores indicating alexithymia.
The Reading the Mind in the Eyes Test revealed no difference between the three experimental groups (Table 3).
3.4 Positive correlations between hippocampal subfield volumes and results of the psychological tests
The positive correlations between brain area volumes and results of the psychological tests are presented in Table 4. We report here only the statistically significant findings.
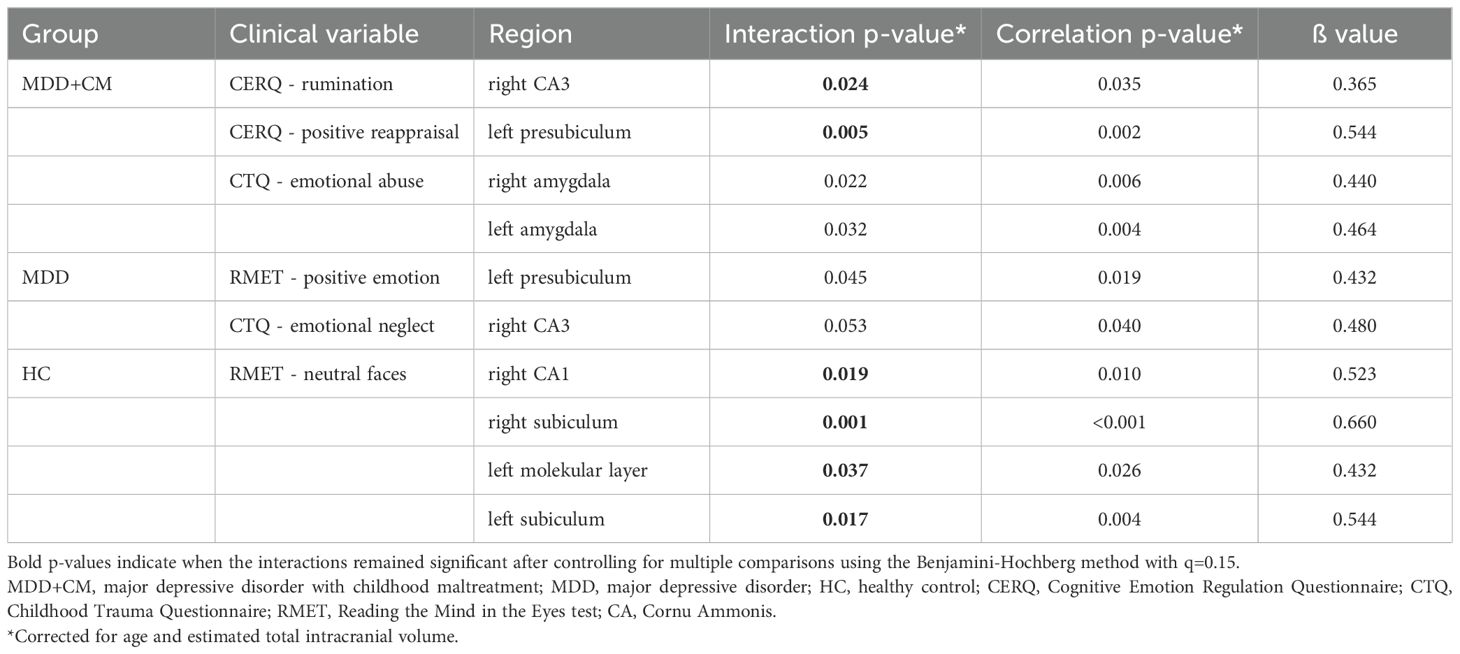
Table 4. Between-group interaction effects and positive correlations between the psychological parameters and hippocampal subfield and amygdala volumes.
In maltreated depressed patients, the scores reached in the rumination subscale of the CERQ test showed positive correlation with the volume of the right CA3 area. Notably, the right CA3 area had no volume shrinkage in these patients (Table 2). Furthermore, in maltreated patients, the low scores of the positive reappraisal subscale of the CERQ test were associated with the volume reduction of the left presubiculum (Table 4).
In non-maltreated depressed patients (MDD group), results of recognizing positive emotions in the RMET test showed positive correlation with the volume of the left presubiculum. Furthermore, results of the emotional neglect subscale of the CTQ test showed positive correlation with the volume of the right CA3 area. However, none of these two results remain significant after controlling for multiple comparisons using the Benjamini-Hochberg method with q=0.15 (Table 4).
In the control group, the results of recognizing neutral faces in the RMET test showed positive correlations with several hippocampal subfield volumes, namely with the volumes of the right CA1, right subiculum, left molecular layer, and left subiculum (Table 4).
3.5 Negative correlations between the hippocampal subfield volumes and results of the psychological tests
The negative correlations between brain area volumes and results of the psychological tests are presented in Table 5. We report here only the statistically significant findings.
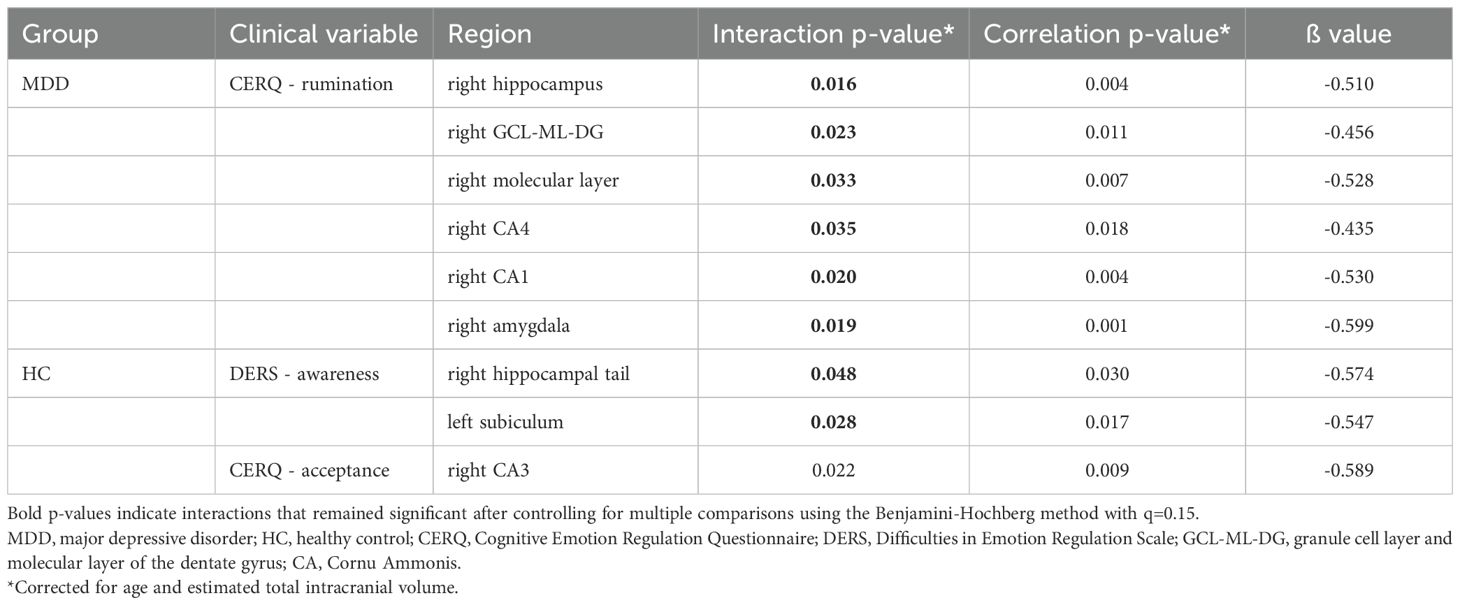
Table 5. Between-group interaction effects and negative correlations between the psychological parameters and hippocampal subfield and amygdala volumes.
In maltreated depressed patients, we did not find any negative correlations between the results of the psychological tests and brain area volumes.
In the non-maltreated MDD patients, the scores reached in the rumination subscale of the CERQ test showed negative correlations with the volumes of several subfields of the right hippocampus i.e. the GCL-ML-DG, molecular layer, CA4, CA1, and the entire right hippocampus (Table 5).
In the control group, results of the awareness subscale of the DERS test showed negative correlation with the volumes of the right hippocampal tail and left subiculum. Furthermore, in control subjects results of the acceptance subscale of the CERQ test showed negative correlation with the volume of the right CA3, but this result did not remain significant after controlling for multiple comparisons using the Benjamini-Hochberg method with q=0.15 (Table 5).
3.6 Correlations between amygdala volumes and the results of the psychological tests
In case of the amygdala, we found very few significant correlations. In maltreated individuals, the scores of the emotional abuse subscale in the CTQ test were positively associated with volume of the bilateral amygdala. However, this result did not remain significant after controlling for multiple comparisons using the Benjamini-Hochberg method with q=0.15 (Table 4). Furthermore, in non-maltreated depressed patients, the scores of the rumination subscale in the CERQ were associated with greater volume shrinkage of the right amygdala (Table 5).
4 Discussion
The present study was designed to investigate the associations between emotion processing and volumes of hippocampal subfields and amygdala. We focused on depressed patients since emotional dysregulation and hippocampal volume shrinkage are key characteristics of this population. Our first hypothesis was that depressed patients, particularly those who experienced childhood maltreatment, would demonstrate reduced hippocampal volumes. We were only able to partially confirm this. While we observed a clear trend of volume decrease in the depressed patients, this difference did not achieve statistical significance. It is noteworthy that volume shrinkage was more prominent in those with a history of maltreatment and affected both the hippocampus and the amygdala. We emphasize these non-significant volumetric differences between the groups because the absence of volumetric variation would undermine the meaningful interpretation of the volumetric correlations. Furthermore, our findings revealed that maltreated depressed subjects showed a 6% reduction in hippocampal volume across both hemispheres. In comparison, meta-analytic studies focusing on depressed patients have reported a reduction of 8% in left hippocampal volume and 10% in right hippocampal volume (87), which is to some extent comparable to our data. It is important to note, however, that the relatively low sample size of our study may have contributed to our inability to detect statistically significant differences between the groups.
Our second hypothesis was that depressed patients will exhibit maladaptive behaviors when assessed with the psychological tests and this hypothesis was clearly confirmed. Maltreated depressed patients had the most pronounced difficulties in emotion processing. Emotional dysregulation was characteristic of them as they were significantly different compared to controls in all subscales of the DERS test. Maltreated individuals also presented numerous difficulties in cognitive coping as they were significantly different compared to controls in almost all subscales of the CERQ test. Eleven maltreated depressed individuals had alexithymia, and the maltreated group was significantly different compared to controls in all subscales of the TAS test. Non-maltreated depressed patients also had severe problems with emotional regulation, coping behavior and alexithymia, because they had significantly different scores compared to controls in almost all subscales of the DERS, CERQ and TAS tests.
However, we could not confirm our third hypothesis, namely that the maladaptive behaviors will correlate with the hippocampal and/or amygdala volume shrinkage. We expected numerous negative correlations between the high scores of the psychological measures and the volume shrinkage of the hippocampal subfields, but we found only a few. In maltreated depressed patients, we did not find any negative correlations, and in the non-maltreated depressed patients, only the results of the rumination subscale of the CERQ test showed negative correlations with volumes of the right hippocampal subfields. Surprisingly, not even the results of the CTQ test had any negative correlations with brain area volumes. As a matter of fact, in maltreated individuals, the high scores of the emotional abuse subscale of the CTQ test were associated with volume of the bilateral amygdala. Furthermore, while maltreated patients had significantly higher scores in the TAS and 11 maltreated individuals had alexithymia, these abnormalities did not correlate with any brain area volumes investigated by us.
4.1 Correlation between MRI data and emotional processing
Numerous studies have used in vivo magnetic resonance imaging to examine hippocampal volume changes in subjects suffering from major depressive disorder, or in relation to adverse childhood experiences (17, 25, 30, 87–91). While the meta-analytic studies reveal a significant hippocampal volume loss of 8-10%, the results of the individual studies have been inconsistent and negative findings are not without precedent (87, 88, 92). The exact cellular changes responsible for the hippocampal volume loss are not fully understood, neuronal loss, dendritic reorganization, reduced adult neurogenesis and glial changes have all been implicated (93). A widely held view is that the stress-induced activation of the HPA-axis results in elevated glucocorticoid levels, which then initiates a cascade of neurotoxic – or at least neuroplastic – events in the brain, resulting in gross volume decrease (94–96). Based on this line of thinking, one may conclude that the hippocampal volume shrinkage is linked to the maladaptive emotional and/or cognitive behavior typical for depressed patients. Indeed, there is evidence for such a consequence, for example a study reported that in depressed patients the hippocampal volume loss correlated with executive dysfunctions (97). A more recent longitudinal study of depressed youth could also link hippocampal volume with emotion regulation and episodic memory impairment (34). Results of our present study could not however, substantiate these earlier findings.
The notion that volumetric changes in limbic structures can be linked to functional impairments has a long tradition (e.g. 15, 97, 98). Nevertheless, studies that have directly examined the structure-behavior relationship have so far yielded ambiguous results (18, 99, 100). The factors contributing to changes in brain area volume may be more complex or variable, rendering the correlation between brain structure and behavior challenging. Therefore, correlating functional neuroimaging data with complex psychological functioning may yield more consistent results.
Several factors may explain our inability to demonstrate an association between maladaptive emotional behavior and hippocampal subfield or amygdala volumes. One significant consideration is neuroplasticity, a key characteristic of the human brain. Volumetric changes may occur more rapidly and with greater variability than previously assumed (101). Furthermore, individual variability in brain development (102), hippocampal volume (21, 103), and emotional brain network topology (104) may provide another explanation. Additionally, functional reorganization (105) and structural resilience (106) following traumatic experiences may further elucidate the absence of significant results in our study.
4.2 Associations between difficulties in emotion regulation and volumes of hippocampal subfields and amygdala
Subjects of the present study were assessed with five psychological tests and the rumination subscale of the CERQ test was the one which had the largest number of correlations with hippocampal subfield volumes. This was reassuring since the hippocampus has been implicated in the regulation of stress-coping strategies (107, 108). The CERQ test has been constructed to identify the cognitive coping strategies in response to stressful life events (35). A recent study found a few positive correlations with some subscales of the CERQ test (e.g. catastrophizing, rumination, refocus on planning and positive refocusing) in healthy individuals, but none these correlations remained significant after correction for multiple analyses (19).
We also found a few negative correlations between results of the awareness subscale of the DERS test and hippocampal subfield volumes of control subjects. Only a few studies investigated the relationship between hippocampal, or amygdala volumes and emotion regulation difficulties. One study reported a strong relationship between emotion regulation and hippocampal volume (34), while another found that prolonged orphanage rearing was associated with atypically large amygdala volume and difficulties in emotion regulation (109).
In case of the RMET test, we found no difference between the groups, but within-group correlation analysis revealed that in the control group there were numerous positive correlations between hippocampal subfield volumes and scores of the RMET-neutral-faces subscale. Numerous MRI studies have been performed to relate performance in the RMET test with results of structural brain imaging and there is evidence that larger amygdala/hippocampal volumes are associated with better performance in the RMET test (52, 54).
In case of the TAS test, we could not find any correlations with brain area volumes. In the literature, there are numerous imaging studies which investigated the association between alexithymia and gray matter volumes, but most studies yielded inconsistent findings (40). Results of a recent meta-analysis indicates that the volumes of the left insula, left amygdala, orbital frontal cortex and striatum is consistently smaller in people with high levels of alexithymia (40). However, our present data could not replicate these findings.
Our present study has yielded a few counterintuitive correlations. Notably, we observed that individuals who reported higher instances of emotional abuse exhibited larger volumes of their bilateral amygdalae. Although this result did not remain significant after controlling for multiple comparisons, it stands in contrast to previous research, which typically associates childhood emotional abuse with reduced amygdala volumes (110–112). As discussed in chapter 4.1, potential explanations for these contradictory results may include individual differences in brain development, sample variability, or the presence of statistical noise.
4.3 Limitations
As with the majority of studies, the current research is subject to several limitations. A major limitation is the relatively low sample size. To circumvent this issue, participants were meticulously selected to ensure matching groups in terms of age, gender, depression severity, and IQ. The relatively small sample size is likely a contributing factor to our inability to detect statistically significant volumetric differences among the three examined groups. A formal power analysis calculated by G*Power (version 3.1.9.4) indicated that a minimum total sample size of 153 participants (51 per group) would be required to detect statistically significant volumetric differences across the three groups in hippocampal subfields and the amygdala, based on assumed effect size of 0.322 and a statistical power of 0.9508. Further limitations are the cross-sectional design of the study and the retrospective assessment of childhood maltreatment, which was conducted with a self-report questionnaire that lacks complete objectivity. The cross-sectional nature of our study coupled with the retrospective self-reporting of childhood abuse, limits our ability to establish causal relationships between childhood maltreatment, brain morphology, and emotional regulation. Longitudinal studies are necessary to clarify such causal relationships, and indeed, there have been efforts to verify such causalities. A recent longitudinal study demonstrated that childhood maltreatment is associated with a persistent reduction of hippocampal volume in children and adolescents (113). Similarly, longitudinal studies could prove that experiencing childhood maltreatment is related to emotion dysregulation (114, 115).
The segmentation of the hippocampal subfields and the amygdala was based on only T1-weighted images, as employed in previous studies (116–118). For this reason, finding related to the volumes of GCL-ML-DG, CA4 and molecular layer must be interpreted with caution. Additionally, a limitation is that the amygdala was not segmented into nuclei. This limitation arose because we began the data analysis with the latest available version of the Freesurfer software (version 6.0), which does not include the segmentation of amygdala subregions. As a result, segmentation was confined to the entire amygdala without any division into further subregions. Future studies that employ high-resolution T2-weighted images and more recent versions of FreeSurfer software (beyond version 6.0) are warranted to achieve more detailed segmentation of the amygdala. Finally, this study relied only on structural neuroimaging data, whereas correlating functional neuroimaging findings with strategies of emotion regulation in maltreated and non-maltreated patients with major depression may yield more robust and informative results.
4.4 Conclusion
We report here that depressed patients with or without childhood maltreatment exhibit a modest reduction in hippocampal volume. Moreover, these individuals also display pronounced difficulties in emotion regulation. We demonstrate here a few associations between hippocampal subfield and amygdala volumes and disturbances in emotional processing. However, we could not detect the expected negative correlations between maladaptive behavior and hippocampal/amygdala volume shrinkage. Our present data suggest that correlating volumes of specific brain regions with complex psychological functions may not yield convincing results. Consequently, future research should prioritize functional neuroimaging methods, such as assessments of neural activity or functional connectivity, over structural data, like volumetric measurements, when investigating complex emotional phenomena.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statement
The studies involving humans were approved by Research Ethics Committee of the University of Pécs. The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
Author contributions
MG: Data curation, Formal Analysis, Investigation, Visualization, Writing – original draft. SN: Conceptualization, Data curation, Formal Analysis, Investigation, Methodology, Software, Supervision, Visualization, Writing – original draft, Writing – review & editing. GO: Methodology, Supervision, Writing – review & editing. GP: Methodology, Supervision, Writing – review & editing. TT: Resources, Supervision, Writing – review & editing. BC: Conceptualization, Funding acquisition, Project administration, Resources, Supervision, Writing – original draft, Writing – review & editing. MS: Conceptualization, Data curation, Formal Analysis, Investigation, Methodology, Resources, Supervision, Writing – original draft, Writing – review & editing.
Funding
The authors declare that financial support was received for the research and publication of this article. A major funding was granted by the National Brain Research Program 3 (NAP 3.0). Further fundings were received from the Development and Innovation Fund of Hungary’s Thematic Excellence Programs (TKP2021-EGA-16) and (TKP2021-EGA-13), and by the National Laboratory of Translational Neuroscience, within the program of “Adult Nervous System Disorders-RRF-2.3.1-21-2022-00011” framework. S.A.N. was supported by the János Bolyai Research Scholarship of the Hungarian Academy of Sciences and by the János Szolcsányi Research Fund (PTE ÁOK-KA-2025). Individual scholarships were granted to S.A.N. (EKÖP-24-4-II-PTE-250, EKÖP-25-4-II-PTE-536) and to M.G. (EKÖP-24-4-I-PTE-191) by University Research Fellowship Programme from the National Research, Development and Innovation Fund of Hungary of Ministry of Culture and Innovation. None of these funding agencies had any influence on study design, collection, analysis, and interpretation of data, the writing of this article, or the decision to submit it for publication.
Acknowledgments
We are grateful to Nándor Németh, Eszter Csernela, Flóra Elza Lakner for performing the psychological evaluation of the subjects involved in this study.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The author(s) declared that they were an editorial board member of Frontiers, at the time of submission. This had no impact on the peer review process and the final decision.
Generative AI statement
The author(s) declare that no Generative AI was used in the creation of this manuscript.
Any alternative text (alt text) provided alongside figures in this article has been generated by Frontiers with the support of artificial intelligence and reasonable efforts have been made to ensure accuracy, including review by the authors wherever possible. If you identify any issues, please contact us.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Abbreviations
CERQ, Cognitive Emotion Regulation Questionnaire; CA, Cornu Ammonis; CTQ, childhood trauma questionnaire; CM, childhood maltreatment; DERS, Difficulties in Emotion Regulation Scale; DG, dentate gyrus; GCL-ML-DG, granule cell layer and molecular layer of the dentate gyrus HC, healthy control; IQ, intelligence quotient; MDD, major depressive disorder; MRI, magnetic resonance imaging; NaSSAs, Noradrenergic and specific serotonergic antidepressants; PTSD, post-traumatic stress disorder; RMET, Reading the Mind in the Eyes Test; SNRIs, Serotonin–norepinephrine reuptake inhibitors; SSRIs, selective serotonin reuptake inhibitors; TAS, Toronto Alexithymia Scale.
References
1. Rubin RD, Watson PD, Duff MC, and Cohen NJ. The role of the hippocampus in flexible cognition and social behavior. Front Hum Neurosci. (2014) 8:742. doi: 10.3389/fnhum.2014.00742
2. Montagrin A, Saiote C, and Schiller D. The social hippocampus. Hippocampus. (2018) 28:672–9. doi: 10.1002/hipo.22797
3. Phelps EA. Human emotion and memory: interactions of the amygdala and hippocampal complex. Curr Opin Neurobiol. (2004) 14:198–202. doi: 10.1016/j.conb.2004.03.015
4. Small SA, Schobel SA, Buxton RB, Witter MP, and Barnes CA. A pathophysiological framework of hippocampal dysfunction in ageing and disease. Nat Rev Neurosci. (2011) 12:585–601. doi: 10.1038/nrn3085
5. Femenía T, Gómez-Galán M, Lindskog M, and Magara S. Dysfunctional hippocampal activity affects emotion and cognition in mood disorders. Brain Res. (2012) 1476:58–70. doi: 10.1016/j.brainres.2012.03.053
6. Zhu Y, Gao H, Tong L, Li Z, Wang L, Zhang C, et al. Emotion regulation of hippocampus using real-time fMRI neurofeedback in healthy human. Front Hum Neurosci. (2019) 13:242. doi: 10.3389/fnhum.2019.00242
7. Genon S, Bernhardt BC, La Joie R, Amunts K, and Eickhoff SB. The many dimensions of human hippocampal organization and (dys)function. Trends Neurosci. (2021) 44:977–89. doi: 10.1016/j.tins.2021.10.003
8. Hainmueller T and Bartos M. Dentate gyrus circuits for encoding, retrieval and discrimination of episodic memories. Nat Rev Neurosci. (2020) 21:153–68. doi: 10.1038/s41583-019-0260-z
9. Borzello M, Ramirez S, Treves A, Lee I, Scharfman H, Stark C, et al. Assessments of dentate gyrus function: discoveries and debates. Nat Rev Neurosci. (2023) 24:502–17. doi: 10.1038/s41583-023-00710-z
10. Rebola N, Carta M, and Mulle C. Operation and plasticity of hippocampal CA3 circuits: implications for memory encoding. Nat Rev Neurosci. (2017) 18:208–20. doi: 10.1038/nrn.2017.10
11. Kesner RP. Behavioral functions of the CA3 subregion of the hippocampus. Learn Memory (Cold Spring Harbor NY). (2007) 14:771–81. doi: 10.1101/lm.688207
12. Tzakis N and Holahan MR. Social memory and the role of the hippocampal CA2 region. Front Behav Neurosci. (2019) 13:233. doi: 10.3389/fnbeh.2019.00233
13. Foo H, Mak E, Chander RJ, Ng A, Au WL, Sitoh YY, et al. Associations of hippocampal subfields in the progression of cognitive decline related to Parkinson’s disease. NeuroImage Clin. (2016) 14:37–42. doi: 10.1016/j.nicl.2016.12.008
14. Haukvik UK, Tamnes CK, Söderman E, and Agartz I. Neuroimaging hippocampal subfields in schizophrenia and bipolar disorder: A systematic review and meta-analysis. J Psychiatr Res. (2018) 104:217–26. doi: 10.1016/j.jpsychires.2018.08.012
15. Genon S, Eickhoff SB, and Kharabian S. Linking interindividual variability in brain structure to behaviour. Nat Rev Neurosci. (2022) 23:307–18. doi: 10.1038/s41583-022-00584-7
16. Ho TC, Gutman B, Pozzi E, Grabe HJ, Hosten N, Wittfeld K, et al. Subcortical shape alterations in major depressive disorder: Findings from the ENIGMA major depressive disorder working group. Hum Brain Mapp. (2022) 43:341–51. doi: 10.1002/hbm.24988
17. Twait EL, Blom K, Koek HL, Zwartbol MHT, Ghaznawi R, Hendrikse J, et al. Psychosocial factors and hippocampal subfields: The Medea-7T study. Hum Brain Mapp. (2023) 44:1964–84. doi: 10.1002/hbm.26185
18. Zhang J, Xie L, Cheng C, Liu Y, Zhang X, Wang H, et al. Hippocampal subfield volumes in mild cognitive impairment and alzheimer’s disease: a systematic review and meta-analysis. Brain Imaging Behav. (2023) 17:778–93. doi: 10.1007/s11682-023-00804-3
19. Fallahi MS, Sahebekhtiari K, Hosseini H, Aliasin MM, Noroozi M, Moghadam Fard A, et al. Distinct patterns of hippocampal subfield volumes predict coping strategies, emotion regulation, and impulsivity in healthy adults. Brain Imaging Behav. (2024) 18:1100–20. doi: 10.1007/s11682-024-00904-8
20. Gilbertson MW, Shenton ME, Ciszewski A, Kasai K, Lasko NB, Orr SP, et al. Smaller hippocampal volume predicts pathologic vulnerability to psychological trauma. Nat Neurosci. (2002) 5:1242–7. doi: 10.1038/nn958
21. Lupien SJ, Evans A, Lord C, Miles J, Pruessner M, Pike B, et al. Hippocampal volume is as variable in young as in older adults: implications for the notion of hippocampal atrophy in humans. NeuroImage. (2007) 34:479–85. doi: 10.1016/j.neuroimage.2006.09.041
22. Teicher MH, Anderson CM, and Polcari A. Childhood maltreatment is associated with reduced volume in the hippocampal subfields CA3, dentate gyrus, and subiculum. Proc Natl Acad Sci United States America. (2012) 109:E563–72. doi: 10.1073/pnas.1115396109
23. Calem M, Bromis K, McGuire P, Morgan C, and Kempton MJ. Meta-analysis of associations between childhood adversity and hippocampus and amygdala volume in non-clinical and general population samples. NeuroImage Clin. (2017) 14:471–9. doi: 10.1016/j.nicl.2017.02.016
24. Cao B, Passos IC, Mwangi B, Amaral-Silva H, Tannous J, Wu MJ, et al. Hippocampal subfield volumes in mood disorders. Mol Psychiatry. (2017) 22:1352–8. doi: 10.1038/mp.2016.262
25. Luby JL, Tillman R, and Barch DM. Association of timing of adverse childhood experiences and caregiver support with regionally specific brain development in adolescents. JAMA Netw Open. (2019) 2:e1911426. doi: 10.1001/jamanetworkopen.2019.11426
26. Malhi GS, Das P, Outhred T, Irwin L, Gessler D, Bwabi Z, et al. The effects of childhood trauma on adolescent hippocampal subfields. Aust New Z J Psychiatry. (2019) 53:447–57. doi: 10.1177/0004867418824021
27. Yuan M, Rubin-Falcone H, Lin X, Rizk MM, Miller JM, Sublette ME, et al. Smaller left hippocampal subfield CA1 volume is associated with reported childhood physical and/or sexual abuse in major depression: A pilot study. J Affect Disord. (2020) 272:348–54. doi: 10.1016/j.jad.2020.03.169
28. Aghamohammadi-Sereshki A, Coupland NJ, Silverstone PH, Huang Y, Hegadoren KM, Carter R, et al. Effects of childhood adversity on the volumes of the amygdala subnuclei and hippocampal subfields in individuals with major depressive disorder. J Psychiatry Neurosci: JPN. (2021) 46:E186–95. doi: 10.1503/jpn.200034
29. Wang Y, Wang Y, Zhou J, Ge C, Shi Y, and Hu Z. Volumetric changes in specific neurofunctional subfields of the hippocampus in major depressive disorder. Neuroreport. (2022) 33:380–5. doi: 10.1097/WNR.0000000000001794
30. Sun Y, Hu N, Wang M, Lu L, Luo C, Tang B, et al. Hippocampal subfield alterations in schizophrenia and major depressive disorder: a systematic review and network meta-analysis of anatomic MRI studies. J Psychiatry Neurosci: JPN. (2023) 48:E34–49. doi: 10.1503/jpn.220086
31. Gratz KL and Roemer L. Multidimensional assessment of emotion regulation and dysregulation: development, factor structure, and initial validation of the difficulties in emotion regulation scale. J Psychopathol Behav Assess. (2004) 26:41–54. doi: 10.1023/B:JOBA.0000007455.08539.94
32. Fowler JC, Charak R, Elhai JD, Allen JG, Frueh BC, and Oldham JM. Construct validity and factor structure of the difficulties in Emotion Regulation Scale among adults with severe mental illness. J Psychiatr Res. (2014) 58:175–80. doi: 10.1016/j.jpsychires.2014.07.029
33. Kuo JR, Khoury JE, Metcalfe R, Fitzpatrick S, and Goodwill A. An examination of the relationship between childhood emotional abuse and borderline personality disorder features: the role of difficulties with emotion regulation. Child Abuse Negl. (2015) 39:147–55. doi: 10.1016/j.chiabu.2014.08.008
34. Barch DM, Harms MP, Tillman R, Hawkey E, and Luby JL. Early childhood depression, emotion regulation, episodic memory, and hippocampal development. J Abnormal Psychol. (2019) 128:81–95. doi: 10.1037/abn0000392
35. Garnefski N and Kraaij V. The Cognitive Emotion Regulation Questionnaire: Psychometric features and prospective relationships with depression and anxiety in adults. Eur J Psychol Assess. (2007) 23:141–9. doi: 10.1027/1015-5759.23.3.141
36. Karim HT, Lee S, Gerlach A, Stinley M, Berta R, Mahbubani R, et al. Hippocampal subfield volume in older adults with and without mild cognitive impairment: Effects of worry and cognitive reappraisal. Neurobiol Aging. (2024) 141:55–65. doi: 10.1016/j.neurobiolaging.2024.02.017
37. Bagby RM, Parker JD, and Taylor GJ. The twenty-item Toronto Alexithymia Scale–I. Item selection and cross-validation of the factor structure. J Psychosom Res. (1994) 38:23–32. doi: 10.1016/0022-3999(94)90005-1
38. Bagby RM, Taylor GJ, and Parker JD. The Twenty-item Toronto Alexithymia Scale–II. Convergent, discriminant, and concurrent validity. J Psychosom Res. (1994) 38:33–40. doi: 10.1016/0022-3999(94)90006-x
39. Bagby RM, Parker JDA, and Taylor GJ. Twenty-five years with the 20-item Toronto alexithymia scale. J Psychosom Res. (2020) 131:109940. doi: 10.1016/j.jpsychores.2020.109940
40. Xu P, Opmeer EM, van Tol MJ, Goerlich KS, and Aleman A. Structure of the alexithymic brain: A parametric coordinate-based meta-analysis. Neurosci Biobehav Rev. (2018) 87:50–5. doi: 10.1016/j.neubiorev.2018.01.004
41. Ihme K, Dannlowski U, Lichev V, Stuhrmann A, Grotegerd D, Rosenberg N, et al. Alexithymia is related to differences in gray matter volume: a voxel-based morphometry study. Brain Res. (2013) 1491:60–7. doi: 10.1016/j.brainres.2012.10.044
42. Farah T, Ling S, Raine A, Yang Y, and Schug R. Alexithymia and reactive aggression: The role of the amygdala. Psychiatry Res Neuroimaging. (2018) 281:85–91. doi: 10.1016/j.pscychresns.2018.09.003
43. Förster K, Enneking V, Dohm K, Redlich R, Meinert S, Geisler AI, et al. Brain structural correlates of alexithymia in patients with major depressive disorder. J Psychiatry Neurosci: JPN. (2020) 45:117–24. doi: 10.1503/jpn.190044
44. Baron-Cohen S, Wheelwright S, Hill J, Raste Y, and Plumb I. The “Reading the Mind in the Eyes” Test revised version: a study with normal adults, and adults with Asperger syndrome or high-functioning autism. J Child Psychol Psychiatry Allied Disciplines. (2001) 42:241–51.
45. Oakley BFM, Brewer R, Bird G, and Catmur C. Theory of mind is not theory of emotion: A cautionary note on the Reading the Mind in the Eyes Test. J Abnormal Psychol. (2016) 125:818–23. doi: 10.1037/abn0000182
46. Pisani S, Murphy J, Conway J, Millgate E, Catmur C, and Bird G. The relationship between alexithymia and theory of mind: A systematic review. Neurosci Biobehav Rev. (2021) 131:497–524. doi: 10.1016/j.neubiorev.2021.09.036
47. Koizumi M and Takagishi H. The relationship between child maltreatment and emotion recognition. PloS One. (2014) 9:e86093. doi: 10.1371/journal.pone.0086093
48. Schwaiger M, Heinrichs M, and Kumsta R. Oxytocin administration and emotion recognition abilities in adults with a history of childhood adversity. Psychoneuroendocrinology. (2019) 99:66–71. doi: 10.1016/j.psyneuen.2018.08.025
49. Rnic K, Sabbagh MA, Washburn D, Bagby RM, Ravindran A, Kennedy JL, et al. Childhood emotional abuse, physical abuse, and neglect are associated with theory of mind decoding accuracy in young adults with depression. Psychiatry Res. (2018) 268:501–7. doi: 10.1016/j.psychres.2018.07.045
50. Simon M, Németh N, Gálber M, Lakner E, Csernela E, Tényi T, et al. Childhood adversity impairs theory of mind abilities in adult patients with major depressive disorder. Front Psychiatry. (2019) 10:867. doi: 10.3389/fpsyt.2019.00867
51. Nilsson KK, Nygaard S, Ebsen S, and Østergård OK. Valence in the eyes: An emotion decoding profile of adults with major depressive disorder and a history of childhood maltreatment. Clin Psychol Psychother. (2023) 31:e2899. doi: 10.1002/cpp.2899. Advance online publication.
52. Rice K, Viscomi B, Riggins T, and Redcay E. Amygdala volume linked to individual differences in mental state inference in early childhood and adulthood. Dev Cogn Neurosci. (2014) 8:153–63. doi: 10.1016/j.dcn.2013.09.003
53. Sato W, Kochiyama T, Uono S, Sawada R, Kubota Y, Yoshimura S, et al. Structural neural substrates of reading the mind in the eyes. Front Hum Neurosci. (2016) 10:151. doi: 10.3389/fnhum.2016.00151
54. Baribeau DA, Dupuis A, Paton TA, Hammill C, Scherer SW, Schachar RJ, et al. Structural neuroimaging correlates of social deficits are similar in autism spectrum disorder and attention-deficit/hyperactivity disorder: analysis from the POND Network. Trans Psychiatry. (2019) 9:72. doi: 10.1038/s41398-019-0382-0
55. Otsuka Y, Nakai R, Shizawa M, Itakura S, Sato A, and Abe N. Brain structure variation and individual differences in theory of mind among older adults. Aging Brain. (2024) 5:100115. doi: 10.1016/j.nbas.2024.100115
56. Bernstein DP, Stein JA, Newcomb MD, Walker E, Pogge D, Ahluvalia T, et al. Development and validation of a brief screening version of the Childhood Trauma Questionnaire. Child Abuse Negl. (2003) 27:169–90. doi: 10.1016/s0145-2134(02)00541-0
57. Saini SM, Hoffmann CR, Pantelis C, Everall IP, and Bousman CA. Systematic review and critical appraisal of child abuse measurement instruments. Psychiatry Res. (2019) 272:106–13. doi: 10.1016/j.psychres.2018.12.068
58. Derogatis LR. Symptom Checklist-90-R: Administration. Scoring, and Procedures Manual. Minneapolis USA: MN NCS Pearson (1994).
59. Urbán R, Kun B, Farkas J, Paksi B, Kökönyei G, Unoka Z, et al. Bifactor structural model of symptom checklists: SCL-90-R and Brief Symptom Inventory (BSI) in a non-clinical community sample. Psychiatry Res. (2014) 216:146–54. doi: 10.1016/j.psychres.2014.01.027
60. American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders. Washington, D.C., USA: American Psychiatric Publishing. (2013). doi: 10.1176/appi.books.9780890425596
61. First MB, Williams JBW, Karg RS, and Spitzer RL. Structured Clinical Interview for DSM-5 Disorders - Clinician Version. Arlington, VA, USA: American Psychiatric Association Publishing (2015). [In Hungarian: First MB, Williams JBW, Karg RS, Spitzer RL. Strukturált klinikai interjú a DSM-5® zavarok felmérésére. Oriold és Társai, Budapest (2016)].
62. First MB, Williams JBW, Smith BL, and Spitzer RL. Structured Clinical Interview for DSM-5® Personality Disorders (first ed.). Arlington, VA, USA: American Psychiatric Association Publishing (2016). [In Hungarian: First MB, M.D., Williams JBW, Ph.D., Smith Benjamin L, Spitzer RL. Strukturált Klinikai Interjú a DSM-5® Személyiségzavarok Vizsgálatára. Oriold és Társai, Budapest, (2018)].
63. Hamilton M. Development of a rating scale for primary depressive illness. Br J Soc Clin Psychol. (1967) 6:278–96. doi: 10.1111/j.2044-8260.1967.tb00530.x
64. Beck AT, Ward CH, Mendelson M, Mock J, and Erbaugh J. An inventory for measuring depression. Arch Gen Psychiatry. (1961) 4:561–71. doi: 10.1001/archpsyc.1961.01710120031004
65. Beck AT, Epstein N, Brown G, and Steer RA. An inventory for measuring clinical anxiety: psychometric properties. J Consult Clin Psychol. (1988) 56:893–7. doi: 10.1037//0022-006x.56.6.893
66. Bremner JD, Bolus R, and Mayer EA. Psychometric properties of the early trauma inventory-self report. J Nervous Ment Dis. (2007) 195:211–8. doi: 10.1097/01.nmd.0000243824.84651.6c
67. Kaufman A, Ishikuma T, and Kaufman-Packer J. Amazingly short forms of the WAIS-R. J Psychoeducational Assess. (1991) 9:4–15. doi: 10.1177/073428299100900101
68. Wechsler D. Wechsler Adult Intelligence Scale–Third Edition (WAIS-III). APA PsycTests. Washington, D.C., USA: American Psychiatric Publishing. (1997) doi: 10.1037/t49755-000
69. Nagybányai Nagy O and Rózsa S. A mentális képességek tesztelése. In: Rózsa S, Nagybányai Nagy O, and Oláh A, editors. A Pszichológiai Mérés Alapjai. Elmélet, Módszer És Gyakorlati Alkalmazás. Budapest, Hungary: Bölcsész Konzorcium (2006). p. 181–98.
70. Csernela E, Németh N, Csuta C, Lakner FE, Tényi T, Czéh B, et al. An evaluation of a Hungarian questionnaire to assess childhood adversities: a pilot study. Psychiatr Hung. 36(1):26–39.
71. Kenézlői E, Csernela E, Nemoda Z, Lakatos K, Czéh B, Unoka ZS, et al. Psychometric properties of the Hungarian childhood trauma questionnaire short form and its validity in patients with adult attention-deficit hyperactivity disorder or borderline personality disorder. Borderline Pers Disord Emotion Dysregul. (2023) 10:33. doi: 10.1186/s40479-023-00239-8
72. Nagy SA, Kürtös Z, Németh N, Perlaki G, Csernela E, Lakner FE, et al. Childhood maltreatment results in altered deactivation of reward processing circuits in depressed patients: A functional magnetic resonance imaging study of a facial emotion recognition task. Neurobiol Stress. (2021) 15:100399. doi: 10.1016/j.ynstr.2021.100399
73. Gálber M, Anett Nagy S, Orsi G, Perlaki G, Simon M, and Czéh B. Depressed patients with childhood maltreatment display altered intra- and inter-network resting state functional connectivity. NeuroImage Clin. (2024) 43:103632. doi: 10.1016/j.nicl.2024.103632
74. Miklósi M, Martos T, Kocsis-Bogár K, and Perczel Forintos D. A kognitiv Erzelem-Regulació Kérdőiv magyar változatának pszichometrial jellemzői [Psychometric properties of the Hungarian version of the Cognitive Emotion Regulation Questionnaire. Psychiatria Hungarica: A Magyar Pszichiatriai Tarsasag tudomanyos folyoirata. (2011) 26:102–11.
75. McKinnon A, Kuyken W, Hayes R, Werner-Seidler A, Watson P, Dalgleish T, et al. The psychometric properties of the cognitive emotion regulation questionnaire (CERQ) in a clinical sample of adults with recurrent depression. J Affect Disord. (2020) 276:212–9. doi: 10.1016/j.jad.2020.06.061
76. Kökönyei G, Urbán R, Reinhardt M, Józan A, and Demetrovics Z. The difficulties in emotion regulation scale: factor structure in chronic pain patients. J Clin Psychol. (2014) 70:589–600. doi: 10.1002/jclp.22036
77. Kooiman CG, Spinhoven P, and Trijsburg RW. The assessment of alexithymia: a critical review of the literature and a psychometric study of the Toronto Alexithymia Scale-20. J Psychosom Res. (2002) 53:1083–90. doi: 10.1016/s0022-3999(02)00348-3
78. Cserjési R, Luminet O, and Lénárd L. A Torontói Alexitímia Skála (TAS-20) magyar változata: megbízhatósága és faktorvaliditása egyetemista mintán. Magyar Psychol Szemle. (2007) 62:355–68. doi: 10.1556/mpszle.62.2007.3.4
79. Baron-Cohen S. Adult “Reading the Mind in the Eyes” Test–Revised [Database record]. APA PsycTests. Washington, D.C., USA: American Psychiatric Publishing (2001). doi: 10.1037/t00387-000
80. Reuter M, Schmansky NJ, Rosas HD, and Fischl B. Within-subject template estimation for unbiased longitudinal image analysis. NeuroImage. (2012) 61:1402–18. doi: 10.1016/j.neuroimage.2012.02.084
81. Fischl B, Salat DH, Busa E, Albert M, Dieterich M, Haselgrove C, et al. Whole brain segmentation: automated labeling of neuroanatomical structures in the human brain. Neuron. (2002) 33:341–55. doi: 10.1016/s0896-6273(02)00569-x
82. Fischl B, Salat DH, van der Kouwe AJ, Makris N, Ségonne F, Quinn BT, et al. Sequence-independent segmentation of magnetic resonance images. NeuroImage. (2004) 23 Suppl 1:S69–84. doi: 10.1016/j.neuroimage.2004.07.016
83. Desikan RS, Ségonne F, Fischl B, Quinn BT, Dickerson BC, Blacker D, et al. An automated labeling system for subdividing the human cerebral cortex on MRI scans into gyral based regions of interest. NeuroImage. (2006) 31:968–80. doi: 10.1016/j.neuroimage.2006.01.021
84. Iglesias JE, Augustinack JC, Nguyen K, Player CM, Player A, Wright M, et al. A computational atlas of the hippocampal formation using ex vivo, ultra-high resolution MRI: Application to adaptive segmentation of in vivo MRI. NeuroImage. (2015) 115:117–37. doi: 10.1016/j.neuroimage.2015.04.042
85. Perlaki G, Orsi G, Plozer E, Altbacker A, Darnai G, Nagy S, et al. Are there any gender differences in the hippocampus volume after head-size correction? A volumetric and voxel-based morphometric study. Neuroscience Letters. (2014) 570:119–23. doi: 10.1016/j.neulet.2014.04.013
87. Videbech P and Ravnkilde B. Hippocampal volume and depression: a meta-analysis of MRI studies. Am J Psychiatry. (2004) 161:1957–66. doi: 10.1176/appi.ajp.161.11.1957
88. Campbell S, Marriott M, Nahmias C, and MacQueen GM. Lower hippocampal volume in patients suffering from depression: a meta-analysis. Am J Psychiatry. (2004) 161:598–607. doi: 10.1176/appi.ajp.161.4.598
89. Kempton MJ, Salvador Z, Munafò MR, Geddes JR, Simmons A, Frangou S, et al. Structural neuroimaging studies in major depressive disorder. Meta-analysis and comparison with bipolar disorder. Arch Gen Psychiatry. (2011) 68:675–90. doi: 10.1001/archgenpsychiatry.2011.60
90. Opel N, Redlich R, Zwanzger P, Grotegerd D, Arolt V, Heindel W, et al. Hippocampal atrophy in major depression: a function of childhood maltreatment rather than diagnosis? Neuropsychopharmacol: Off Publ Am Coll Neuropsychopharmacol. (2014) 39:2723–31. doi: 10.1038/npp.2014.145
91. Schmaal L, Veltman DJ, van Erp TG, Sämann PG, Frodl T, Jahanshad N, et al. Subcortical brain alterations in major depressive disorder: findings from the ENIGMA Major Depressive Disorder working group. Mol Psychiatry. (2016) 21:806–12. doi: 10.1038/mp.2015.69
92. McKinnon MC, Yucel K, Nazarov A, and MacQueen GM. A meta-analysis examining clinical predictors of hippocampal volume in patients with major depressive disorder. J Psychiatry Neurosci: JPN. (2009) 34:41–54.
93. Czéh B and Lucassen PJ. What causes the hippocampal volume decrease in depression? Are neurogenesis, glial changes and apoptosis implicated? Eur Arch Psychiatry Clin Neurosci. (2007) 257:250–60. doi: 10.1007/s00406-007-0728-0
94. Pittenger C and Duman RS. Stress, depression, and neuroplasticity: a convergence of mechanisms. Neuropsychopharmacol: Off Publ Am Coll Neuropsychopharmacol. (2008) 33:88–109. doi: 10.1038/sj.npp.1301574
95. Lucassen PJ, Pruessner J, Sousa N, Almeida OF, Van Dam AM, Rajkowska G, et al. Neuropathology of stress. Acta Neuropathol. (2014) 127:109–35. doi: 10.1007/s00401-013-1223-5
96. McEwen BS, Nasca C, and Gray JD. Stress effects on neuronal structure: hippocampus, amygdala, and prefrontal cortex. Neuropsychopharmacol: Off Publ Am Coll Neuropsychopharmacol. (2016) 41:3–23. doi: 10.1038/npp.2015.171
97. Frodl T, Schaub A, Banac S, Charypar M, Jäger M, Kümmler P, et al. Reduced hippocampal volume correlates with executive dysfunctioning in major depression. J Psychiatry Neurosci: JPN. (2006) 31:316–23.
98. Hickie I, Naismith S, Ward PB, Turner K, Scott E, Mitchell P, et al. Reduced hippocampal volumes and memory loss in patients with early- and late-onset depression. Br J Psychiatry: J Ment Sci. (2005) 186:197–202. doi: 10.1192/bjp.186.3.197
99. Clark IA, Monk AM, Hotchin V, Pizzamiglio G, Liefgreen A, Callaghan MF, et al. Does hippocampal volume explain performance differences on hippocampal-dependant tasks? NeuroImage. (2020) 221:117211. doi: 10.1016/j.neuroimage.2020.117211
100. Scheepens DS, van Waarde JA, Lok A, de Vries G, Denys DAJP, and van Wingen GA. The link between structural and functional brain abnormalities in depression: A systematic review of multimodal neuroimaging studies. Front Psychiatry. (2020) 11:485. doi: 10.3389/fpsyt.2020.00485
101. Zsido RG, Williams AN, Barth C, Serio B, Kurth L, Mildner T, et al. Ultra-high-field 7T MRI reveals changes in human medial temporal lobe volume in female adults during menstrual cycle. Nat Ment Health. (2023) 1:761–71. doi: 10.1038/s44220-023-00125-w
102. Mills KL, Siegmund KD, Tamnes CK, Ferschmann L, Wierenga LM, Bos MGN, et al. Inter-individual variability in structural brain development from late childhood to young adulthood. NeuroImage. (2021) 242:118450. doi: 10.1016/j.neuroimage.2021.118450
103. Decker AL, Duncan K, Finn AS, and Mabbott DJ. Children’s family income is associated with cognitive function and volume of anterior not posterior hippocampus. Nat Commun. (2020) 11:4040. doi: 10.1038/s41467-020-17854-6
104. Ling G, Lee I, Guimond S, Lutz O, Tandon N, Nawaz U, et al. Individual variation in brain network topology is linked to emotional intelligence. NeuroImage. (2019) 189:214–23. doi: 10.1016/j.neuroimage.2019.01.013
105. Bremner JD, Elzinga B, Schmahl C, and Vermetten E. Structural and functional plasticity of the human brain in posttraumatic stress disorder. Prog Brain Res. (2008) 167:171–86. doi: 10.1016/S0079-6123(07)67012-5
106. Bonne O, Brandes D, Gilboa A, Gomori JM, Shenton ME, Pitman RK, et al. Longitudinal MRI study of hippocampal volume in trauma survivors with PTSD. Am J Psychiatry. (2001) 158:1248–51. doi: 10.1176/appi.ajp.158.8.1248
107. Lyons DM, Buckmaster PS, Lee AG, Wu C, Mitra R, Duffey LM, et al. Stress coping stimulates hippocampal neurogenesis in adult monkeys. Proc Natl Acad Sci United States America. (2010) 107:14823–7. doi: 10.1073/pnas.0914568107
108. Yoon SH, Song WS, Chung G, Kim SJ, and Kim MH. Activity in the dorsal hippocampus-mPFC circuit modulates stress-coping strategies during inescapable stress. Exp Mol Med. (2024) 56:1921–35. doi: 10.1038/s12276-024-01294-z
109. Tottenham N, Hare TA, Quinn BT, McCarry TW, Nurse M, Gilhooly T, et al. Prolonged institutional rearing is associated with atypically large amygdala volume and difficulties in emotion regulation. Dev Sci. (2010) 13:46–61. doi: 10.1111/j.1467-7687.2009.00852.x
110. Schmahl CG, Vermetten E, Elzinga BM, and Douglas Bremner J. Magnetic resonance imaging of hippocampal and amygdala volume in women with childhood abuse and borderline personality disorder. Psychiatry Res. (2003) 122:193–8. doi: 10.1016/s0925-4927(03)00023-4
111. Ahmed-Leitao F, Spies G, van den Heuvel L, and Seedat S. Hippocampal and amygdala volumes in adults with posttraumatic stress disorder secondary to childhood abuse or maltreatment: A systematic review. Psychiatry Res Neuroimaging. (2016) 256:33–43. doi: 10.1016/j.pscychresns.2016.09.008
112. Nogovitsyn N, Addington J, Souza R, Placsko TJ, Stowkowy J, Wang J, et al. Childhood trauma and amygdala nuclei volumes in youth at risk for mental illness. Psychol Med. (2022) 52:1192–9. doi: 10.1017/S0033291720003177
113. Doretto VF, Salto ABR, Schivoletto S, Zugman A, Oliveira MC, Brañas M, et al. Childhood maltreatment and the structural development of hippocampus across childhood and adolescence. psychol Med. (2025) 54:1–9. doi: 10.1017/S0033291724001636. Advance online publication.
114. Kim J and Cicchetti D. Longitudinal pathways linking child maltreatment, emotion regulation, peer relations, and psychopathology. Journal of. Child Psychol Psychiatry Allied Disciplines. (2010) 51:706–16. doi: 10.1111/j.1469-7610.2009.02202.x
115. Kim-Spoon J, Cicchetti D, and Rogosch FA. A longitudinal study of emotion regulation, emotion lability-negativity, and internalizing symptomatology in maltreated and nonmaltreated children. Child Dev. (2013) 84:512–27. doi: 10.1111/j.1467-8624.2012.01857.x
116. Baglivo V, Cao B, Mwangi B, Bellani M, Perlini C, Lasalvia A, et al. Hippocampal subfield volumes in patients with first-episode psychosis. Schizophr Bull. (2018) 44:552–9. doi: 10.1093/schbul/sbx108
117. Ho NF, Holt DJ, Cheung M, Iglesias JE, Goh A, Wang M, et al. Progressive Decline in Hippocampal CA1 Volume in Individuals at Ultra-High-Risk for Psychosis Who Do Not Remit: Findings from the Longitudinal Youth at Risk Study. Neuropsychopharmacol: Off Publ Am Coll Neuropsychopharmacol. (2017) 42:1361–70. doi: 10.1038/npp.2017.5
Keywords: adverse childhood experiences, child abuse, emotional processing, hippocampus, magnetic resonance imaging, MRI, major depressive disorder, volumetry
Citation: Gálber M, Nagy SA, Orsi G, Perlaki G, Tényi T, Czéh B and Simon M (2025) Hippocampal subfield and amygdala volumes are associated with difficulties in emotion regulation of depressed patients with a history of childhood maltreatment. Front. Psychiatry 16:1641745. doi: 10.3389/fpsyt.2025.1641745
Received: 05 June 2025; Accepted: 28 July 2025;
Published: 25 August 2025.
Edited by:
Gustavo E Tafet, Texas A and M University, United StatesReviewed by:
Carlos Hesed Virto Farfan, Andean University of Cusco, PeruSonia Tabares, Institución Universitaria de Envigado, Colombia
Copyright © 2025 Gálber, Nagy, Orsi, Perlaki, Tényi, Czéh and Simon. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Boldizsár Czéh, Y3plaC5ib2xkaXpzYXJAcHRlLmh1
†These authors have contributed equally to this work and share first authorship