 André Eduardo Silva Júnior1,2*
André Eduardo Silva Júnior1,2* Mateus de Lima Macena1,2
Mateus de Lima Macena1,2 Déborah Tenório da Costa Paula1
Déborah Tenório da Costa Paula1 Délis Barbosa Soares1
Délis Barbosa Soares1 Isabelle Rodrigues de Souza Gama1
Isabelle Rodrigues de Souza Gama1 Natália Gomes da Silva Lopes1
Natália Gomes da Silva Lopes1 Maria Eduarda de Carvalho Macário da Silva3
Maria Eduarda de Carvalho Macário da Silva3 Ashley Nicole Gearhardt4
Ashley Nicole Gearhardt4 Nassib Bezerra Bueno1,2
Nassib Bezerra Bueno1,2- 1Laboratório de Nutrição e Metabolismo (LANUM), Faculdade de Nutrição, Universidade Federal de Alagoas, Maceió, Brazil
- 2Postgraduate Program in Nutrition, Escola Paulista de Medicina, Universidade Federal de São Paulo, São Paulo, Brazil
- 3Programa Associado de Pós-Graduação em Ciências de Movimento, Instituto de Educação Física e Esporte, Universidade Federal de Alagoas, Maceió, Brazil
- 4Department of Psychology, University of Michigan, Ann, Arbor, MI, United States
Introduction: The study aimed to investigate several ultra-processed food (UPF) addiction symptoms according to the weight status and to verify if there are specific symptoms of UPF addiction that differ according to the weight status in adults with a UPF addiction diagnosis.
Methods: This is a cross-sectional study that included adults (18–59 years) of both sexes with UPF addiction diagnosis. Demographic and clinical data were collected, such as body mass index (BMI), diagnosis of depression, and generalized anxiety disorder (GAD). UPF addiction was assessed using the modified Yale Food Addiction Scale 2.0.
Results: In total, 1,074 participants were included. Of this total, 83.3% (n = 895) were female, with a mean age of 23 ± 5 years, of which 36.8% (n = 395) were classified with normal weight, 31.9% (n = 343) with overweight, 19.5% (n = 209) with obesity I, 8.1% (n = 87) with obesity II, and 3.7% (n = 40) with obesity III. The prevalence of UPF addiction symptoms referring to social/interpersonal harm, cut down/quit, role interference, and physical/psychological harm increased progressively with increasing BMI, even after adjusting for age, sex, diagnosis of depression, and GAD.
Conclusion: This study showed a progressive increase in UPF addiction symptom severity with rising BMI levels. Moreover, distinct UPF addiction symptom profiles emerged across various BMI categories. Understanding these nuances can guide the development of targeted interventions and treatment strategies to address this multifaceted behavioral profile effectively. Further research across different populations is imperative to broaden our comprehension of UPF addiction’s impact and expression.
1 Introduction
The term ultra-processed food (UPF) addiction, which is defined by the excessive consumption of ultra-processed, hyperpalatable, and, commonly, energetically dense foods with characteristics that can have effects similar to addictive substances, has been drawing the attention of clinicians and researchers dealing with the global public health problem of obesity (1, 2). The latest published systematic reviews evaluating the prevalence of the diagnosis of UPF addiction using the Yale Food Addiction Scale (YFAS) tool have shown high frequencies of this phenomenon, especially in individuals with higher body mass index (BMI), which indicates overweight and obesity (2, 3). As highlighted in the study by Praxedes et al. (2), individuals without weight disorders have a pooled prevalence of UPF addiction of 13%, while individuals with overweight and obesity have 24 and 30%, respectively. Also corroborating these data, a recent systematic review showed that individuals with obesity in the preoperative period for bariatric surgery, with a mean BMI above 40kg/m², have a high prevalence of 32% (4). Such evidence suggests a strong relationship between elevated BMI and a high prevalence of UPF addiction.
Researchers debate this strong relationship between UPF addiction and obesity, but there is a consensus that consuming UPF contributes to the obesity pandemic (5, 6). Although the public health problem of obesity has already been the center of significant research, the resolution of this complex and multifactorial disease does not seem to be close. Part of the problem can be attributed to the food industry, which launches products rich in added sugar, which is considered one of the main components with the highest addictive potential (7–9). Individuals with high UPF addiction symptoms are more prone to fail in response to traditional weight loss treatment approaches, which may be associated with behavioral adaptations similar to the withdrawal and tolerance observed in individuals using addictive substances (5, 10–12).
Despite the clinical relevance of UPF addiction, little research has specifically investigated how this phenotype may exhibit a differential presentation across weight status. While UPF addiction is higher in samples with obesity, most individuals with obesity do not meet UPF addiction diagnosis (2). In addition, some individuals without weight disorders meet the UPF addiction classification and have worse quality-of-life indices in all domains (13). Thus, understanding the UPF addiction phenotype and its presence across different BMI classifications may help develop more targeted treatments to address this behavioral profile. However, we are unaware of any study evaluating the prevalence of each UPF addiction symptom in the different weight statuses (normal weight, overweight, obesity I, II, and III). Given this, the study aimed to investigate the prevalence and number of UPF addiction symptoms according to the weight status and to verify if there are specific symptoms of UPF addiction that differ according to the weight status in adults with UPF addiction.
2 Methods
2.1 Ethical aspects
The research protocol was approved by the Research Ethics Committee of the Universidade Federal de Alagoas (protocol number 4.410.403). All participants were presented with the Free and Informed Consent Form. After accessing the research link, the participants were given the Free and Informed Consent Form on the online questionnaire’s first page. It was necessary to accept it to access the questionnaire and start data collection.
2.2 Study design
This is a cross-sectional study.
2.3 Location, sample and recruitment
This study is a secondary analysis of a more extensive study that aimed to determine the prevalence of UPF addiction in Brazilian college students. The study was carried out with college students from 94 public and private universities from all units of the Brazilian federation; more details can be found in da Silva Júnior et al. (14). College students of either sex, aged between 18 and 59 years, who met the criteria for UPF addiction were included. Our study did not include underweight individuals, pregnant women, nursing mothers, or individuals after bariatric surgery. Those who sent incomplete questionnaires and improbable body weight and height values were excluded.
Participants were recruited through invitations sent by e-mail and publications on websites and institutional social networks. The participants knew the research topic (UPF addiction in Brazilian university students) and did not receive any compensation for their participation. Data collection took place between October 27 and December 11, 2020.
2.4 Demographic and clinical variables
All participants were asked to provide their age (in years), date of birth, sex, educational institution to which they were linked, and the federative unit in which they resided. In addition, participants reported whether they had received a medical diagnosis of depression.
2.5 Economic class
To determine the economic class of the participants, the “Critério de Classificação Econômica Brasil” was used. The instrument considers ownership of goods, the number of bathrooms in the household, education of the head of the family, and access to piped water and paved streets. A score is assigned to each item, which, in the end, is added and can vary from 0 to 100 points. Participants are then classified into one of six possible economic classes: “A” (45–100 points), “B1” (38–44), “B2” (29–37), “C1” (23-28), “C2” (17-22), “D-E” (0-16) (15).
2.6 Anthropometry
Body weight (in kilograms) and height (in meters) data were self-reported. The BMI was calculated, and they were classified according to the cutoff points proposed by the World Health Organization (16): underweight (BMI < 18.5 kg/m²), normal weight (between 18.5 and 24.9 kg/m²), overweight (between 25.0 and 29.9 kg/m²), obesity I (between 30.0 and 34.9 kg/m²), obesity II (between 35.0 and 39.9 kg/m²) and obesity III (≥ 40.0 kg/m²).
2.7 Generalized anxiety disorder
To identify possible cases of generalized anxiety disorder (GAD), the validated version translated into Brazilian Portuguese of the Generalized Anxiety Disorder 7-item scale (GAD-7) was used (17). The scale consists of seven items that can be answered on a Likert scale with four points ranging from 0 to 3, where 0 represents “never” and 3 “almost every day”. The score is summed and can vary from 0 to 21 points, and participants who reached scores equal to or greater than ten were considered probable cases of GAD based on established cutoffs (18). Cronbach’s α for this sample was 0.90.
2.8 Ultra-processed food addiction
The modified Yale Food Addiction Scale 2.0 (mYFAS 2.0) was used to determine UPF addiction (19) in the translated and validated version for Brazilian Portuguese (20). The mYFAS 2.0 consists of 13 items, 11 representing symptoms related to the individual’s eating behavior that refer to aspects of substance use disorders in the DSM-5, and two referring to clinical impairment/impairment. Each question is answered according to the frequency with which it occurs, ranging from “never” to “every day”, each of which has a limit for the criterion of the symptom to be met. In the end, the 11 symptoms are added together to create a symptom count score option. Individuals with two or more symptoms that meet the threshold for any clinical distress/impairment problem are classified as having UPF addiction (21). Cronbach’s α for this sample was 0.88.
2.9 Statistical analysis
Categorical variables are presented in absolute and relative frequencies. At the same time, continuous variables are in mean and standard deviation. The ANOVA one-way test was used to test the differences in the number of symptoms between the BMI groups (normal weight, overweight, obesity I, obesity II, and obesity III). Next, a Bonferroni correction was applied to determine which groups presented differences and account for multiple comparisons.
Univariable and multivariable analyses were performed by dividing individuals by BMI classification. Poisson regressions with robust adjustment of variances were used to assess the associations between the prevalences of each symptom of UPF addiction between the different BMI classifications (1 = normal weight; 2 = overweight; 3 = obesity I; 4 = obesity II; 5 = obesity III). Linear regressions were also performed with the mYFAS 2.0 score as the outcome variable. In the multivariable analyses, the variables age (years), sex (1 = male; 2 = female), diagnosis of depression (0 = no; 1 = yes), and GAD (0 = no; 1 = yes) were used as adjustments. An alpha value of 5% was adopted, and all analyses were performed using the statistical software R v.3.6.1, with the aid of the “Rcmdr” and “ggplot2” packages (22).
3 Results
In total, 6,532 responses were received online; however, after applying the inclusion criteria, data from 1,074 participants were retained in analyses (see Figure 1 for exclusions). Of this total, 83.3% (n = 895) were female, with a mean age of 23 ± 5 years, of which 36.8% (n = 395) were classified with normal weight, 31,9% (n = 343) with overweight, 19,5% (n = 209) with obesity I, 8.1% (n = 87) with obesity II, and 3.7% (n = 40) with obesity III. The other characteristics of the total sample and according to the BMI classification can be seen in Table 1.
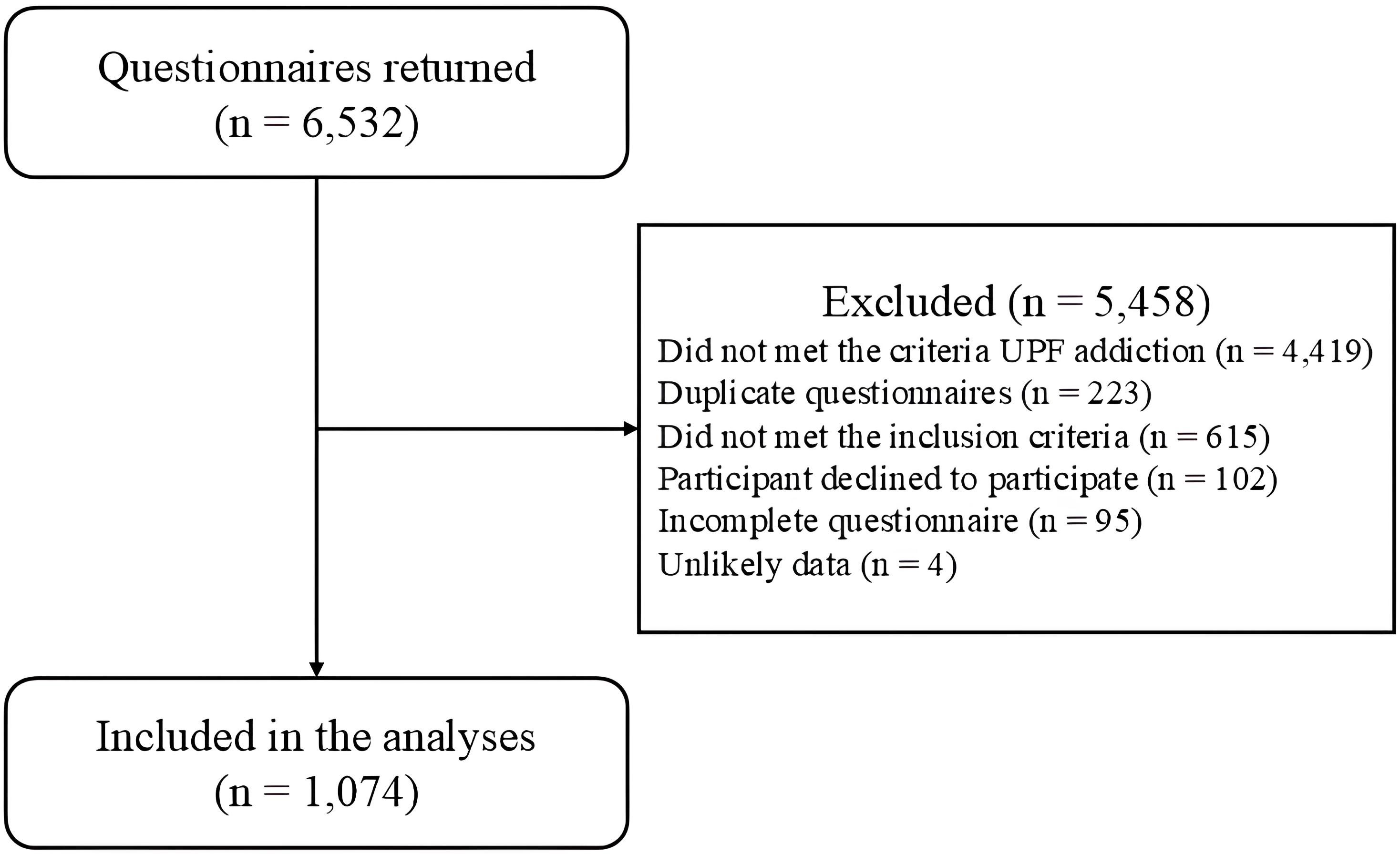
Figure 1. Flowchart of the participants selection.
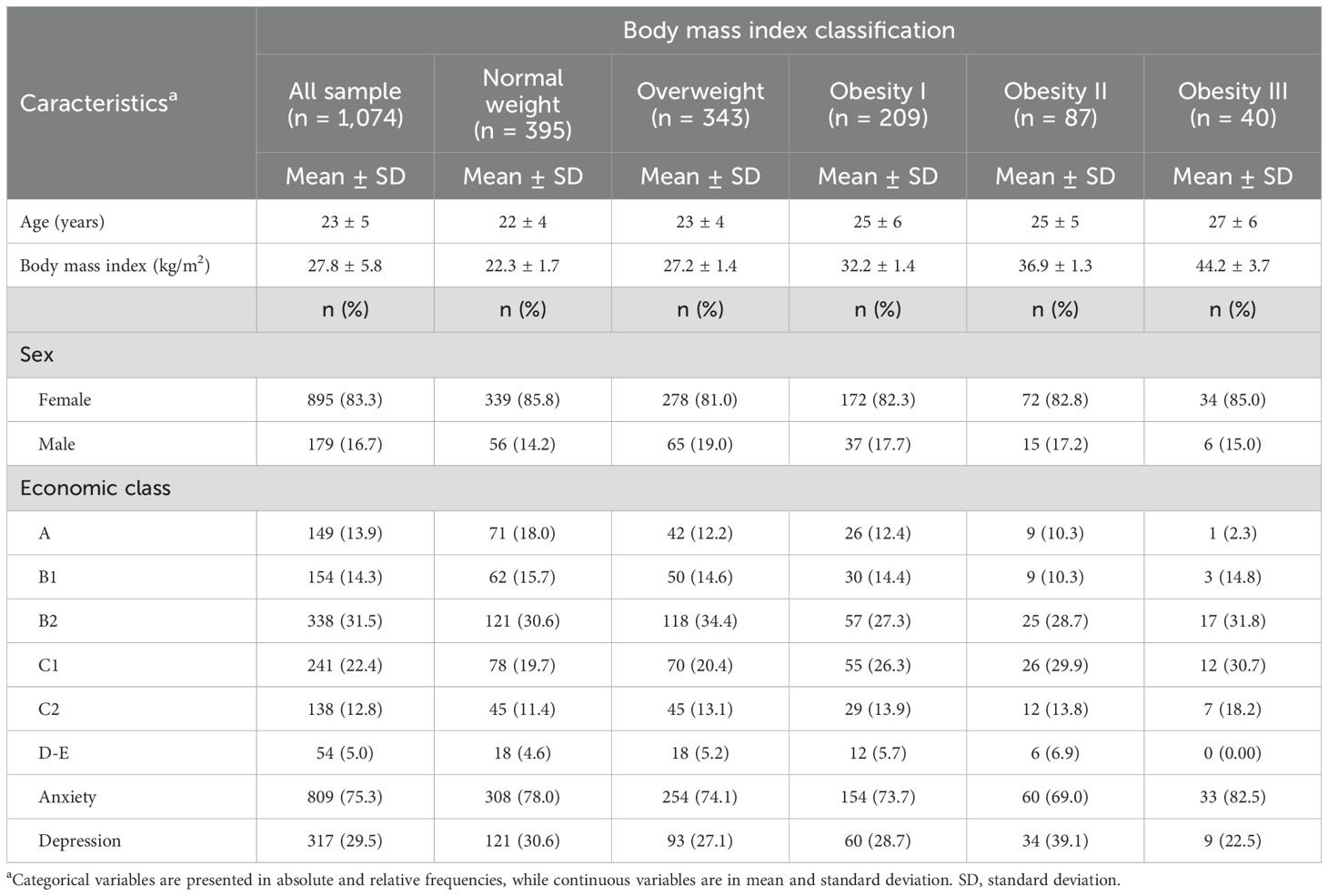
Table 1. Characteristics of the total sample and divided by body mass index classification.
For individuals with normal weight, the most prevalent UPF addiction symptoms was craving and withdrawal (69.9%, n = 276; 67.1%, n = 265, respectively), while for individuals classified with overweight, the most prevalent symptom was craving (71.7%, n = 246). For participants with obesity I, the most prevalent symptom was physical/psychological harm with prevalences of 75.6% (n = 158), and the participants with obesity II and obesity III, cut down/quit is the most prevalent (80.5%, n = 70 and 87,5%, n = 35, respectively) (Table 2). This occurs similarly between the sexes, except for the physical/psychological harm symptom, in which there are no differences between weight status and the male sex (Supplementary Table S1). The least prevalent UPF addiction symptoms for participants with normal weight, overweight, and obesity II classifications were used in hazardous situations. Those individuals classified as having obesity I and obesity III indicated giving up activities in response to use as the least prevalent symptom (22.5%, n = 47; 25%, n = 10, respectively).
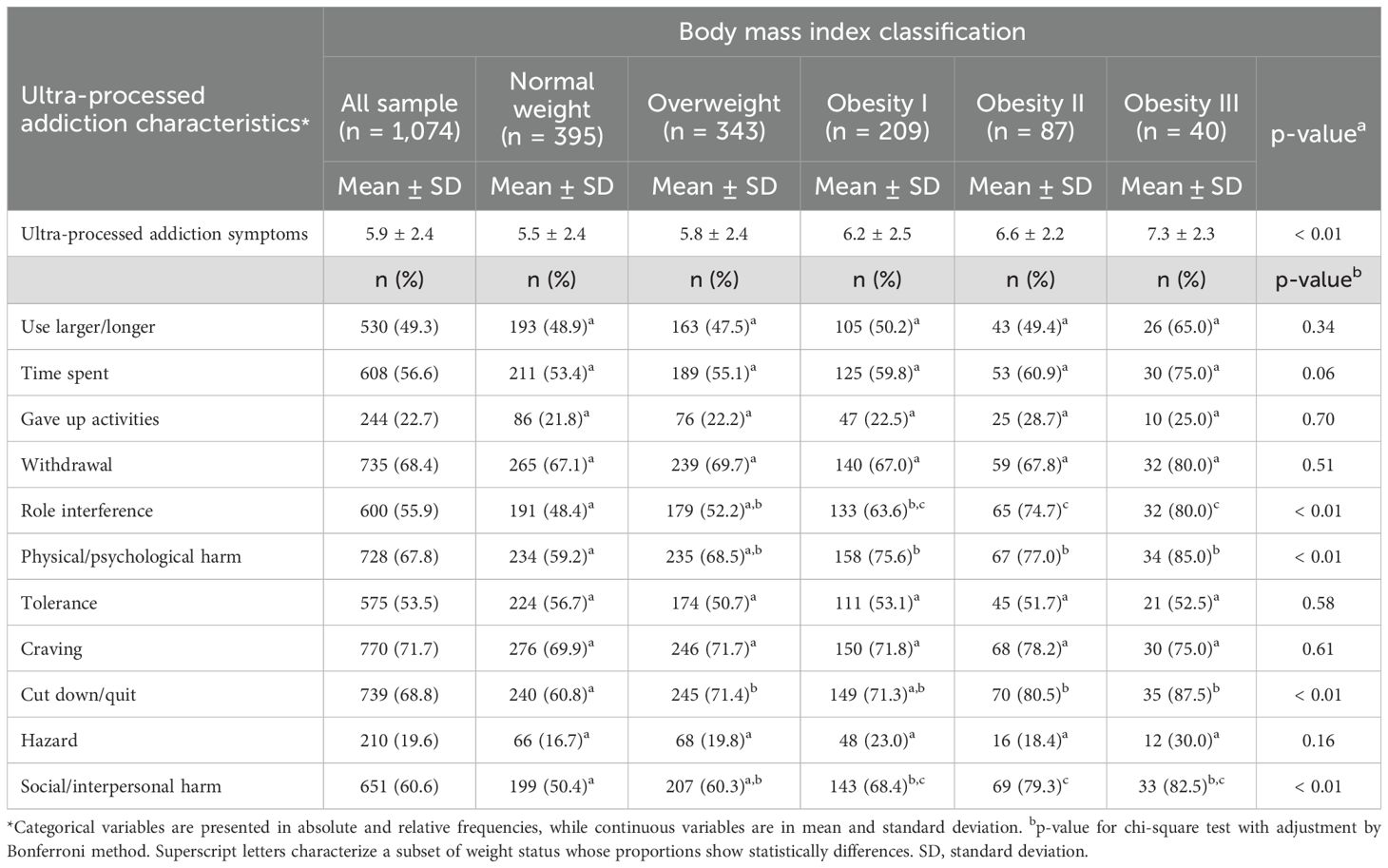
Table 2. Prevalence of symptoms of ultra-processed food addiction among body mass index classifications.
Figure 2A, Supplementary Table S2 show the positive and significant associations found in the univariable analyses between the prevalence of UPF addiction symptoms between the BMI classifications, highlighting the positive associations observed for symptoms of role interference, Physical/psychological harm, cut down/quit, and social/interpersonal harm. All associations remain positive and significant in multivariable analyses with adjustments for age, sex, diagnosis of depression, and diagnosis of GAD (Figure 2B, Supplementary Table S3).
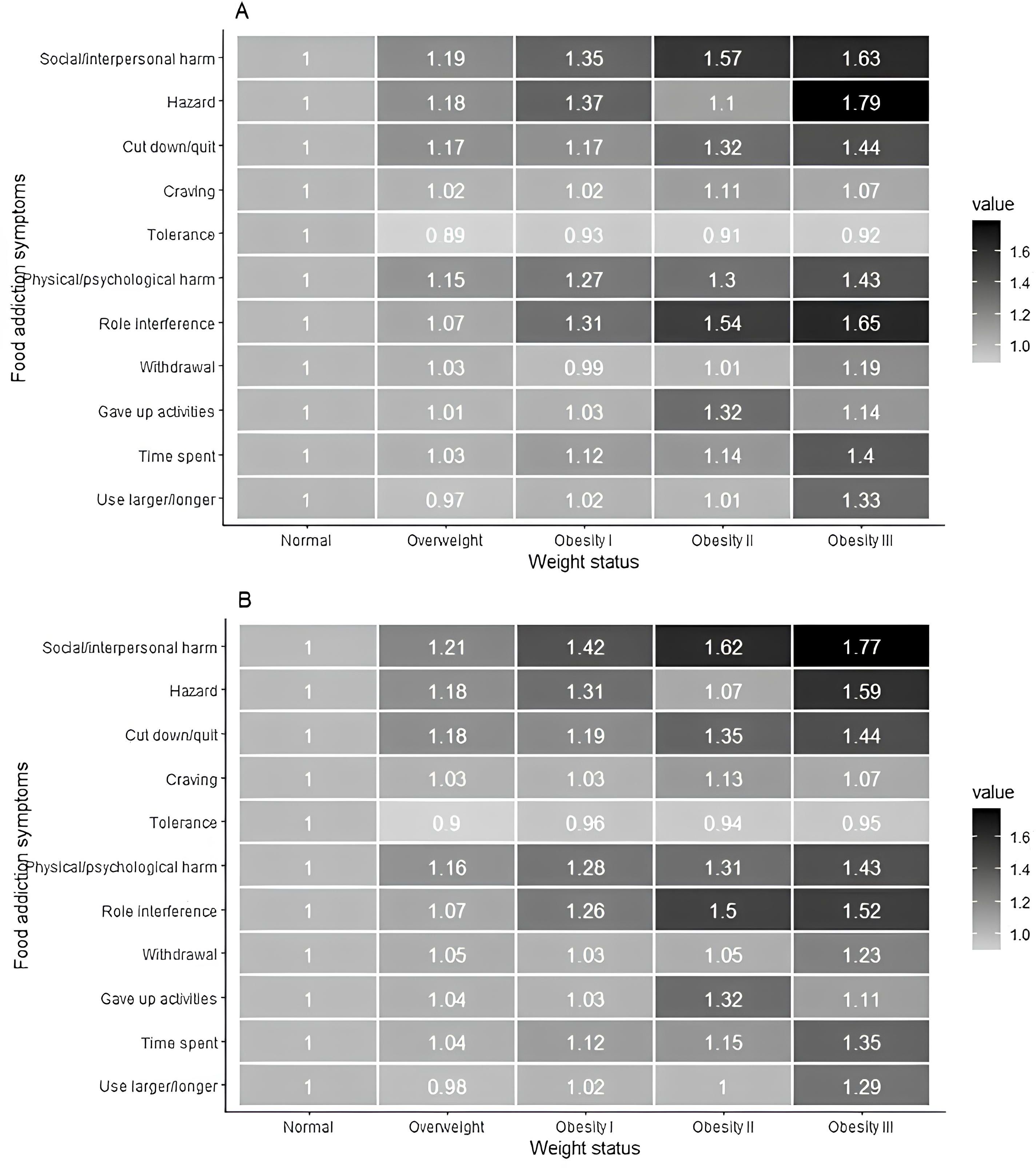
Figure 2. Heatmaps for prevalence ratios from univariable and multivariable analysis between ultra-processed food addiction symptoms and weight status. Footnote: (A) Univariable analysis between body mass index ratings and ultra-processed food addiction symptoms. (B) Multivariable analysis between body mass index classification and ultra-processed food addiction symptoms. Multivariable analysis adjusting for age, sex, diagnosis of depression and diagnosis of general anxiety disorder. Prevalence ratios by Poisson regression with robust adjustment of variance.
Univariable and multivariable analyses between UPF addiction symptom numbers and BMI classifications can be seen in Table 3. The number of UPF addiction symptoms was significantly different for individuals with overweight relative to the normal weight classification (univariable: β = 0.36; 95%CI: 0.01; 0.71; multivariable: β = 0.42; 95%CI: 0.07; 0.77). Furthermore, individuals in all obesity categories (I, II, and III) were significantly more likely to endorse UPF addiction symptoms than normal-weight individuals.
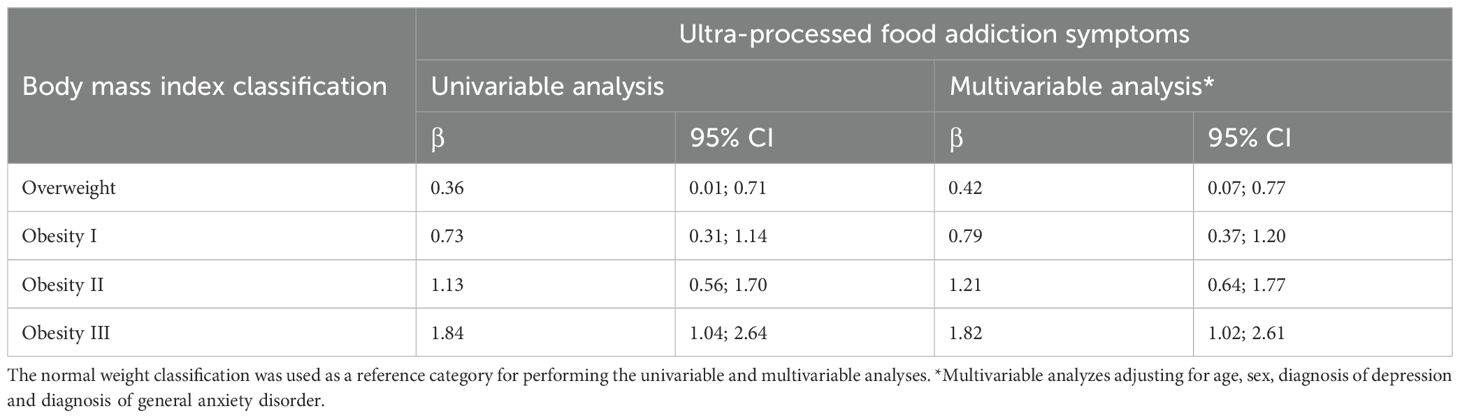
Table 3. Univariable and multivariable analysis between body mass index classification and ultra-processed food addiction symptoms (n = 1,074).
4 Discussion
In this large sample (n = 1,074) of Brazilian college students, it was possible to observe a progressive increase in the number and prevalence of role interference, Physical/psychological harm, cut down/quit, and social/interpersonal harm UPF addiction symptoms as the individuals’ BMI increased. These findings remained after statistical adjustment for age, sex, diagnosis of depression, and GAD. Regarding the number of UPF addiction symptoms, positive associations were observed with obesity classifications I, II, and III, compared to the normal weight group.
The findings that indicate that the prevalence of UPF addiction increases with the increase in BMI corroborate the results of other studies. Praxedes et al. (2) performed an extensive systematic review with meta-analysis. They observed that the prevalence of UPF addiction according to the BMI classification shows a linear growth trend. That is, as the BMI increases, the prevalence of UPF addiction also increases, as also observed in other studies (23, 24). This fact may contribute to the hypothesis that UPF addiction can present as a distinct phenotype within individuals with obesity, which may represent greater susceptibility to the reinforcing effects of highly processed foods (25). Corroborating this, as observed in our study, the magnitude of associations between UPF addiction symptoms and BMI scores appears to be greater at higher degrees of obesity.
In our study, we observed that individuals with normal weight had a high prevalence of the following UPF addiction symptoms: craving, withdrawal, and cut down/quit, while giving up activities and hazards were the least endorsed symptoms. Further, prior research has found that individuals with UPF addiction who are of normal weight also exhibit clinically relevant impairments and may require treatment as well (13). Thus, possible treatments for individuals with UPF addiction may need to be customized according to weight status.
An important aspect that should be considered in this study is the significant increase in the prevalence ratio observed for the UPF addiction symptom role interference as BMI also increases, especially when taking into account the hypothesis that UPF addiction can present as a distinct phenotype within individuals with obesity, which may represent greater susceptibility to the reinforcing effects of highly processed foods in individuals with higher BMI (25). It is known that obesity not only aggravates chronic non-communicable diseases but also plays a negative role in the quality of life and mental health of individuals. People with obesity may experience a lower quality of life, partly explained by the individuals’ mental health deterioration (26). In addition, obesity can decrease the ability to fulfill functions of daily living and, consequently, reduce aspects of overall quality of life (27). Another important point concerns mental health problems (i.e., depression), which appear to have a high prevalence in individuals with obesity and also in those with UPF addiction, so it is possible to observe a greater contribution to the higher role interference as BMI increases (28–30). In addition, another factor that seems to be linked to maladaptive eating behaviors is weight stigmatization, which is characterized by the social devaluation of people due to their body weight, causing social, economic, and psychological consequences (31, 32). The stigmatization of weight among individuals with obesity can also contribute to greater interference in the role as BMI increases (33). Thus, it is clear that the increased prevalence of the symptom “role interference” and “physical/psychological harm” as BMI increases observed in our study is closely linked to the fact that obesity, per se, decreases the quality of life and mental health with repercussions on the functional capacity of these individuals.
It was observed that individuals with overweight and obesity also had a higher prevalence of craving and failed cut down/quit symptoms, as determined by mYFAS 2.0, than individuals with normal weight. This finding is particularly interesting in a population with overweight or obesity, where one of the central intervention goals is to promote weight loss. Individuals with UPF addiction may consume more UPF and less fresh and minimally processed foods (34). Interventions for weight loss usually involve changing the individual’s dietary pattern, increasing the consumption of fresh and whole foods, and decreasing energy-dense foods that individuals commonly identify as addictive (e.g., chocolate, French fries, baked goods) (35). Because of this, the reduction in highly processed consumption may be an agent that hinders adherence to dietary interventions for weight loss in individuals with obesity and UPF addiction, contributing to the high dropout rates evidenced in dietary interventions (11). That said, the ability to control the intake of highly processed foods seems essential for adherence to the dietary treatment of obesity. For individuals, psychobehavioral treatments and pharmacotherapy that focus on reward functioning and craving may be needed to improve weight loss treatment success for individuals with UPF addiction. Further, unsuccessful attempts to reduce highly processed food intake may be related to another symptom of UPF addiction, the characteristic withdrawal symptoms.
Withdrawal syndrome is one of the cornerstones of substance use disorders. It is defined as developing physiological and/or psychological symptoms in response to abstinence or decreased use of an addictive substance (36). Withdrawal syndrome is one of the criteria for diagnosing substance use disorders. In our study, among individuals with obesity III, withdrawal (80.0%) was one of the most endorsed symptoms of UPF addiction assessed by mYFAS 2.0. The prevalence of withdrawal is higher than that of those observed by Hauck et al. (23), in which 14.7% of overweight individuals endorsed the withdrawal criterion. Initial evidence for the plausibility of withdrawal from highly processed foods comes from the observation, in animal models, of physical and psychological symptoms of withdrawal in response to the removal of sucrose from the diet of animals (37, 38). The evidence is still early in humans and is usually measured by the YFAS 2.0 and mYFAS 2.0 items (39). Currently, there is only one tool for operationalizing withdrawal symptoms from highly processed foods, the Highly Processed Food Withdrawal Scale (ProWS) (40), which could be used in future research to investigate the response to dietary change across UPF addiction profiles and BMI classifications.
In the present study, we observed a progressive increase in the prevalence of social/interpersonal harm, and physical/psychological harm symptoms the BMI increased. In individuals with obesity class II and III, this symptom of UPF addiction becomes the most prevalent compared to other BMI classifications. This finding may be related to the stigmatization associated with obesity since the prevalence of this symptom increased as BMI increased. Individuals with obesity are often subjected to negative social stereotypes and consequences, for example, that they are lazy, unmotivated, and lack discipline or willpower, as well as limited employment opportunities, lower wages, and unfair treatment in the workplace (31, 41–43). In this regard, a qualitative study that aimed to assess participants’ interpretation of each YFAS 2.0 item and the fit with the diagnostic criteria for DSM-5 substance use disorders reported that interpersonal problems most commonly occurred when a loved one disapproved of the amount or types of food the participant ate (44). Thus, addressing the deleterious impacts of weight stigma in individuals with both UPF addiction and obesity may be a particularly important future study area.
Future research conducted across different populations, age groups, and geographical regions is essential to broaden our understanding of the impact and expression of UPF addiction. Cultural, social, nutritional, and age-related heterogeneity may influence both the prevalence and the symptomatic profile of this condition, highlighting the need for multicenter and representative investigations. Moreover, studies that take into account weight status, age, and variations in addiction symptoms can support the development of more tailored and effective intervention strategies. Such efforts are crucial for improving diagnostic and therapeutic approaches, as well as for informing public health policies aimed at preventing and managing obesity associated with UPF addiction.
This study has limitations. First, weight and height data were self-reported, which may not accurately represent the actual data of the participants. However, self-reporting body measurements is an efficient strategy for epidemiological studies, considering that there is a high concordance between the measures reported by the participants and those measured, especially in a country with continental dimensions such as Brazil (45). Another limitation concerns the use of a self-reported tool to assess UPF addiction symptoms. However, the tool used (mYFAS 2.0) is based on the criteria proposed by DSM-5 for substance use disorder, is the only validated tool, and is widely used for UPF addiction research around the world. Furthermore, there is evidence that individuals interpret the mYFAS 2.0 items in alignment with the DSM-5 diagnostic criteria for substance use disorders (44). Another limitation is the lack of systematic identification of participants with eating disorders, which are frequent comorbidities in cases of UPF addiction. Not taking these disorders into account may have influenced the results and limits the clinical usefulness of the concept evaluated, especially in contexts of diagnostic overlap. Moreover, it is important to acknowledge that behaviors such as chronic dieting, prolonged caloric restriction, and weight cycling can lead to nutrient deficiencies and mental health impacts that may mimic symptoms of UPF addiction. However, the present study did not include specific measures of dietary restraint, dieting history, or weight cycling, which limits the ability to accurately distinguish symptoms related to UPF addiction from those potentially resulting from restrictive eating behaviors. In addition, when invited to participate in the research, the participants were aware that the study aimed to evaluate UPF addiction, which may have induced the participation of individuals with some identification with the theme. Notably, underweight individuals were excluded from this study. Considering that these individuals may have UPF addiction symptoms associated with comorbid eating disorders, such as binge eating, the absence of this population limits the applicability of the findings to this group (46). Finally, our sample consisted of university students, and the results obtained may need to be more generalizable to other groups.
As for the study’s strengths, we highlight that we reached a large and representative sample of Brazilian college students from all regions of the country and public and private higher education. Therefore, we believe that we were able to capture the economic and ethnic diversity of Brazilian college students in our sample. Additionally, by identifying distinct symptom profiles of UPF addiction according to weight status, our findings contribute valuable insight to tailoring interventions, which is supported by recent longitudinal evidence demonstrating the efficacy of targeted treatments for UPF addiction symptoms over a 12-month period (47). Finally, this study was conducted in Brazil, and further research on UPF addiction in developing countries and Latin America is needed to expand global knowledge about this construct (2, 48).
5 Conclusion
The number and prevalence of UPF addiction symptoms presented increase linearly with weight status. The most frequent UPF addiction symptoms endorsed by normal-weight individuals were withdrawal, craving, and failed attempts to cut down/quit. Interestingly, the most prevalent symptoms in individuals with overweight and the degrees of obesity were related to role interference, continued use despite social/interpersonal harms, physical/psychological harms, and cut down/quit. Thus, the present study explored the unique profiles of UPF addiction symptoms in individuals by weight status, which may inform the development of interventions targeting these different behavioral profiles and strategies to improve clinical outcomes. Further research across different populations and geographical regions is imperative to broaden our comprehension of UPF addiction’s impact and expression, as well as to develop interventions considering UPF addiction profile and weight status.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statement
The studies involving humans were approved by Research Ethics Committee of the Universidade Federal de Alagoas. The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
Author contributions
AS: Investigation, Writing – review & editing, Writing – original draft, Validation, Data curation, Methodology, Visualization, Conceptualization, Formal Analysis. MM: Writing – original draft, Formal Analysis, Writing – review & editing. DT: Writing – review & editing, Writing – original draft, Formal Analysis. DS: Writing – review & editing, Writing – original draft, Formal Analysis. IG: Writing – original draft, Writing – review & editing, Formal Analysis. NL: Writing – original draft, Formal Analysis, Writing – review & editing. MS: Writing – original draft, Formal Analysis, Writing – review & editing. AG: Writing – review & editing, Writing – original draft, Formal Analysis, Visualization. NB: Validation, Formal Analysis, Writing – review & editing, Writing – original draft.
Funding
The author(s) declare that financial support was received for the research and/or publication of this article. AS is supported by the Coordenação de Aperfeiçoamento de Pessoal de Nível Superior–Brazil (CAPES) research fellowships (grant number: 88887.805029/2023-00). MM is supported by the Coordenação de Aperfeiçoamento de Pessoal de Nível Superior–Brazil (CAPES) research fellowships (grant number: 88887.679721/2022-00). NB is supported by a research grant from the Conselho Nacional de Desenvolvimento Científico e Tecnológico – CNPq (grant number: 311401/2022-8). The sponsors had no role in the design and analysis of the study or the writing of this article.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Generative AI statement
The author(s) declare that no Generative AI was used in the creation of this manuscript.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpsyt.2025.1642630/full#supplementary-material
References
1. Gearhardt AN, Yokum S, Orr PT, Stice E, Corbin WR, and Brownell KD. Neural correlates of food addiction. Arch Gen Psychiatry. (2011) 68:808–16. doi: 10.1001/archgenpsychiatry.2011.32
2. Praxedes DRS, Silva-Júnior AE, Macena ML, Oliveira AD, Cardoso KS, Nunes LO, et al. Prevalence of food addiction determined by the Yale Food Addiction Scale and associated factors: A systematic review with meta-analysis. Eur Eat Disord. (2022) 30:85–95. doi: 10.1002/erv.2878
3. Oliveira J, Colombarolli MS, and Cordás TA. Prevalence and correlates of food addiction: Systematic review of studies with the YFAS 2.0. Obes Res Clin Pract. (2021) 15:191–204. doi: 10.1016/j.orcp.2021.03.014
4. Praxedes DR, Silva-Júnior AE, Macena ML, Gearhardt AN, and Bueno NB. Prevalence of food addiction among patients undergoing metabolic/bariatric surgery: A systematic review and meta-analysis. Obes Rev. (2023) 24:e13529. doi: 10.1111/obr.13529
5. Hebebrand J and Gearhardt AN. The concept of “food addiction” helps inform the understanding of overeating and obesity: NO. Am J Clin Nutr. (2021) 113:268–73. doi: 10.1093/ajcn/nqaa344
6. World Health Organization. Obesity and overweight. Geneva, Switzerland: World Health Organization (2021).
7. Chooi YC, Ding C, and Magkos F. The epidemiology of obesity. Metabolism. (2019) 92:6–10. doi: 10.1016/j.metabol.2018.09.005
8. Dent R, McPherson R, and Harper ME. Factors affecting weight loss variability in obesity. Metabolism. (2020) 113:154388. doi: 10.1016/j.metabol.2020.154388
9. Lustig RH. Ultraprocessed food: addictive, toxic, and ready for regulation. Nutrients. (2020) 12:3401. doi: 10.3390/nu12113401
10. Camanho-Barcia L, Munguía L, Gaspar-Pérez A, Jimenez-Murcia S, and Fernández-Aranda F. Impact of food addiction in therapy response in obesity and eating disorders. Curr Addict Rep. (2022) 9:268–74. doi: 10.1007/s40429-022-00421-y
11. Fielding-Singh P, Patel ML, King AC, and Gardner CD. Baseline psychosocial and demographic factors associated with study attrition and 12-month weight gain in the DIETFITS trial. Obesity. (2019) 27:1997–2004. doi: 10.1002/oby.22650
12. Parnarouskis L and Gearhardt AN. Preliminary evidence that tolerance and withdrawal occur in response to ultra-processed foods. Curr Addict Rep. (2022) 9:282–9. doi: 10.1007/s40429-022-00425-8
13. Minhas M, Murphy CM, Balodis IM, Samokhvalov AV, and MacKillop J. Food addiction in a large community sample of Canadian adults: prevalence and relationship with obesity, body composition, quality of life and impulsivity. Addiction. (2021) 116:2870–9. doi: 10.1111/add.15446
14. Silva Júnior AE, de Lima Macena M, de Oliveira ADS, Praxedes DRS, de Oliveira Maranhão Pureza IR, de Menezes Toledo Florêncio TM, et al. Prevalence of food addiction and its association with anxiety, depression, and adherence to social distancing measures in Brazilian university students during the COVID-19 pandemic: a nationwide study. Eat Weight Disord. (2022) 27:2027–35. doi: 10.1007/s40519-021-01344-9
15. ABEP. Critérios de classificação econômica Brasil (2020). Available online at: https://www.abep.org/criterio-brasil (Accessed November 15, 2023).
16. World Health Organization. Physical status: the use and interpretation of anthropometry. Geneva, Switzerland: World Health Organization (1995).
17. Sousa TV, Viveiros V, Chai MV, Vicente FL, Jesus G, Carnot MJ, et al. Reliability and validity of the Portuguese version of the Generalized Anxiety Disorder (GAD-7) scale. Health Qual Life Outcomes. (2015) 13:50. doi: 10.1186/s12955-015-0244-2
18. Spitzer RL, Kroenke K, Williams JB, and Löwe B. A brief measure for assessing generalized anxiety disorder: the GAD-7. Arch Intern Med. (2006) 166:1092–7. doi: 10.1001/archinte.166.10.1092
19. Schulte EM and Gearhardt AN. Development of the modified yale food addiction scale version 2.0. Eur Eat Disord Rev. (2017) 25:302–8. doi: 10.1002/erv.2515
20. Nunes-Neto PR, Köhler CA, Schuch FB, Quevedo J, Solmi M, Murru A, et al. Psychometric properties of the modified Yale Food Addiction Scale 2.0 in a large Brazilian sample. Braz J Psychiatry. (2018) 40:444–8. doi: 10.1590/1516-4446-2017-2432
21. Silva Júnior AED and Bueno NB. Comments on the translated version of the modified Yale Food Addiction Scale 2.0 into Brazilian Portuguese. Braz J Psychiatry. (2022) 45:189–99. doi: 10.47626/1516-4446-2022-2917
22. Fox J. The R commander: A basic statistics graphical user interface to R. J Stat Softw. (2005) 14:1–42. doi: 10.18637/jss.v014.i09
23. Hauck C, Weiß A, Schulte EM, Meule A, and Ellrott T. Prevalence of ‘Food addiction’ as measured with the yale food addiction scale 2.0 in a representative german sample and its association with sex, age and weight categories. Obes Facts. (2017) 10:12–24. doi: 10.1159/000456013
24. Schulte EM and Gearhardt AN. Associations of food addiction in a sample recruited to be nationally representative of the United States. Eur Eat Disord Rev. (2018) 26:112–9. doi: 10.1002/erv.2575
25. LaFata EM and Gearhardt AN. Ultra-processed food addiction: an epidemic? Psychother Psychosom. (2022) 91:363–72. doi: 10.1159/000527322
26. Taylor VH, Forhan M, Vigod SN, McIntyre RS, and Morrison KM. The impact of obesity on quality of life. Best Pract Res Clin Endocrinol Metab. (2013) 27:139–46. doi: 10.1016/j.beem.2013.04.004
27. Forhan M and Gill SV. Obesity, functional mobility and quality of life. Best Pract Res Clin Endocrinol Metab. (2013) 27:129–37. doi: 10.1016/j.beem.2013.01.003
28. Blasco BV, García-Jiménez J, Bodoano I, and Gutiérrez-Rojas L. Obesity and depression: its prevalence and influence as a prognostic factor: A systematic review. Psychiatry Investig. (2020) 17:715–24. doi: 10.30773/pi.2020.0099
29. Burrows T, Kay-Lambkin F, Pursey K, Skinner J, and Dayas C. Food addiction and associations with mental health symptoms: a systematic review with meta-analysis. J Hum Nutr Diet. (2018) 31:544–72. doi: 10.1111/jhn.12532
30. Schachter J, Martel J, Lin CS, Chang CJ, Wu TR, Lu CC, et al. Effects of obesity on depression: A role for inflammation and the gut microbiota. Brain Behav Immun. (2018) 69:1–8. doi: 10.1016/j.bbi.2017.08.026
31. Puhl RM and Heuer CA. The stigma of obesity: a review and update. Obesity. (2009) 17:941–64. doi: 10.1038/oby.2008.636
32. Vartanian LR and Porter AM. Weight stigma and eating behavior: A review of the literature. Appetite. (2016) 102:3–14. doi: 10.1016/j.appet.2016.01.034
33. Puhl RM, Himmelstein MS, and Pearl RL. Weight stigma as a psychosocial contributor to obesity. Am Psychol. (2020) 75:274–89. doi: 10.1037/amp0000538
34. Silva Júnior AED, Gearhardt AN, and Bueno NB. Association between food addiction with ultra-processed food consumption and eating patterns in a Brazilian sample. Appetite. (2023) 186:106572. doi: 10.1016/j.appet.2023.106572
35. Schulte EM, Avena NM, and Gearhardt AN. Which foods may be addictive? The roles of processing, fat content, and glycemic load. PloS One. (2015) 10:e0117959. doi: 10.1371/journal.pone.0117959
36. American Psychiatric Association. Diagnostic and statistical manual of mental disorders, 5th ed. (Arlington, VA: American Psychiatric Association). (2013).
37. Colantuoni C, Rada P, McCarthy J, Patten C, Avena NM, Chadeayne A, et al. Evidence that intermittent, excessive sugar intake causes endogenous opioid dependence. Obes Res. (2002) 10:478–88. doi: 10.1038/oby.2002.66
38. Avena NM, Bocarsly ME, Rada P, Kim A, and Hoebel BG. After daily bingeing on a sucrose solution, food deprivation induces anxiety and accumbens dopamine/acetylcholine imbalance. Physiol Behav. (2008) 94:309–15. doi: 10.1016/j.physbeh.2008.01.008
39. Parnarouskis L, Leventhal AM, Ferguson SG, and Gearhardt AN. Withdrawal: A key consideration in evaluating whether highly processed foods are addictive. Obes Rev. (2022) 23:e13507. doi: 10.1111/obr.13507
40. Schulte EM, Smeal JK, Lewis J, and Gearhardt AN. Development of the highly processed food withdrawal scale. Appetite. (2018) 131:148–54. doi: 10.1016/j.appet.2018.09.013
41. O’Brien KS, Latner JD, Halberstadt J, Hunter JA, Anderson J, and Caputi P. Do antifat attitudes predict antifat behaviors? Obes (Silver Spring). (2008) 16:S87–92. doi: 10.1038/oby.2008.456
42. O’Brien KS, Latner JD, Ebneter D, and Hunter JA. Obesity discrimination: the role of physical appearance, personal ideology, and anti-fat prejudice. Int J Obes. (2013) 37:455–60. doi: 10.1038/ijo.2012.52
43. Roehling MV, Roehling PV, and Pichler S. The relationship between body weight and perceived weight-related employment discrimination: the role of sex and race. J Vocat Behav. (2007) 71:300–18. doi: 10.1016/j.jvb.2007.04.008
44. Schiestl ET, Wolfson JA, and Gearhardt AN. The qualitative evaluation of the Yale Food addiction scale 2.0. Appetite. (2022) 175:106077. doi: 10.1016/j.appet.2022.106077
45. Davies A, Wellard-Cole L, Rangan A, and Allman-Farinelli M. Validity of self-reported weight and height for BMI classification: A cross-sectional study among young adults. Nutrition. (2020) 71:110622. doi: 10.1016/j.nut.2019.110622
46. Unwin J, Giaever H, Avena N, Kennedy C, Painschab M, and LaFata EM. Toward consensus: using the Delphi method to form an international expert consensus statement on ultra-processed food addiction. Front Psychiatry. (2025) 16:1542905. doi: 10.3389/fpsyt.2025.1542905
47. Unwin J, Delon C, Giæver H, Kennedy C, Painschab M, Sandin F, et al. Low carbohydrate and psychoeducational programs show promise for the treatment of ultra-processed food addiction. Front Psychiatry. (2022) 13:1005523. doi: 10.3389/fpsyt.2022.1005523
Keywords: eating addiction, behavioral profile, weight status, obesity, food addiction
Citation: Silva Júnior AE, Macena MdL, Paula DTdC, Soares DB, Gama IRdS, Lopes NGdS, da Silva MEdCM, Gearhardt AN and Bueno NB (2025) Ultra-processed food addiction symptoms profile according to weight status among Brazilian adults. Front. Psychiatry 16:1642630. doi: 10.3389/fpsyt.2025.1642630
Received: 06 June 2025; Accepted: 30 June 2025;
Published: 29 July 2025.
Edited by:
Jen Unwin, The Collaborative Health Community, United KingdomReviewed by:
Tro Kalayjian, Dr. Tro’s Medical Weight Loss, United StatesVera I. Tarman, University of Toronto, Canada
Copyright © 2025 Silva Júnior, Macena, Paula, Soares, Gama, Lopes, da Silva, Gearhardt and Bueno. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: André Eduardo Silva Júnior, YW5kcmVlZHVhcmRvanJAaG90bWFpbC5jb20=