 Thairys Flores Ocasio1
Thairys Flores Ocasio1 Nicole Melendez Rivera2
Nicole Melendez Rivera2 Jorge Duconge1
Jorge Duconge1 Raman Venkataramanan3
Raman Venkataramanan3 Francisco González-Saiz4
Francisco González-Saiz4 Darlene Santiago1*
Darlene Santiago1*- 1Department of Pharmaceutical Sciences, School of Pharmacy, University of Puerto Rico, San Juan, Puerto Rico
- 2Biostatistics, Epidemiology and Research Design Core (BERD), The Hispanic Alliance for Clinical and Translational Research, University of Puerto Rico, San Juan, Puerto Rico
- 3Pharmaceutical Sciences and Pathology Department, School of Pharmacy and Medicine, University of Pittsburgh, Pittsburgh, PA, United States
- 4Unidad de Hospitalizacion de Salud Mental, Hospital Universitario de Jerez, Universidad de Cadiz, Cadiz, Spain
1 Introduction
The Opiate Dosage Adequacy Scale (ODAS) is a semi-structured clinical interview designed for estimating the adequacy of methadone or buprenorphine doses for patients with opioid use disorder (OUD) (1, 2). ODAS’s effectiveness relies on its proven ability to estimate the adequacy of a given dose based on multiple clinical parameters including continuous heroin use, cravings, narcotic blockage, objective and subjective withdrawal symptoms, and signs of overmedication (3, 4). The ODAS was originally developed and validated with Spanish-speaking European patients receiving medication for OUD (5, 6). The original validation demonstrated good reliability and construct validity, with Cronbach’s alpha coefficients ranging between 0.76 (methadone patients) and 0.92 (buprenorphine patients), with coefficients for each of the domains ranging between 0.81 and 0.93 (1, 2). ODAS scores were correlated with clinician assessments of treatment sufficiency and with patient self-reported outcomes, underscoring its clinical relevance in opioid maintenance therapy. Subsequent studies confirmed that ODAS-based dose classification is aligned with longitudinal treatment outcomes, reinforcing its clinical applicability in opioid maintenance therapy, although no Cronbach’s alpha was reported (4). Beyond European settings, the ODAS has been validated for cross-cultural use. A Persian adaptation of the ODAS demonstrated comparable psychometric properties, confirming its internal consistency (Cronbach’s α > 0.70) and convergent validity with other addiction severity measures (e.g., the Severity of Dependence Scale, SDS) (7). These findings suggest that the ODAS is a robust and adaptable instrument, capable of assessing opioid dose adequacy across diverse treatment populations. However, its applicability to other non-European Spanish-speaking populations remains unstudied.
Given the complexities of OUD pharmacotherapy, the ODAS provides a standardized approach for dose assessment that integrates both clinical symptoms and patient-reported outcomes. Previous validation studies have demonstrated its strong reliability and validity for determining whether a patient’s medication dose is sufficient to maintain clinical stabilization (2, 4). Despite the growing burden of opioid use disorder among Hispanic and Spanish-speaking individuals in the United States and across Latin America, few validated tools exist for guiding opioid dose adjustments in a linguistically and culturally relevant manner (8, 9). Given the clinical importance of ensuring appropriate buprenorphine dosing in opioid maintenance therapy, there is a critical need for validated instruments that are not only clinically sound but also tailored to the language and cultural context of diverse populations. Expanding the validation of the ODAS beyond its European origins to include Spanish-speaking populations in the Americas can contribute significantly to addressing treatment disparities and supporting individualized care strategies in these communities. Importantly, psychometric properties of clinical tools often vary across cultural and clinical contexts; hence, the ODAS measures developed in one population may not fully capture treatment adequacy in another. This gap is particularly important for Puerto Rican and other Hispanic subgroups who are disproportionally affected by opioid use disorder and who may experience distinct patterns of treatment access and retention. Validating the ODAS in these populations is therefore critical to ensure its reliability, validity, and applicability in these clinical settings, and to promote equitable assessments of treatment adequacy.
In this study, we aim to evaluate further the ODAS’s psychometric properties and its applicability to Spanish-speaking patients outside of Europe receiving buprenorphine OUD therapy evaluating the scale’s internal consistency (Cronbach’s alpha coefficient) and convergent associations with clinical stabilization variables such as severity of dependence (using the Severity of Dependence Scale [SDS]) and illicit drug use (2). We also aimed to examine the associations with patients’ buprenorphine levels (1).
2 Materials and methods
The institutional review board of the University of Puerto Rico Medical Sciences Campus approved the study before the recruitment started (#B1080320).
2.1 Participants and inclusion/exclusion criteria
This is a cross-sectional study that recruited 111 subjects. The inclusion criteria were ≥ 21 years old, being a patient under buprenorphine treatment for OUD for at least 3 months and taking a maintenance dose, and not having any changes in said buprenorphine dose during the week prior to participation in the study. The following patients were excluded: those with a social or mental incapacity (i.e., inability to understand or answer the questions on the ODAS), those who had started buprenorphine treatment less than 3 months prior to the interview, and those who were pregnant.
2.2 Recruitment sites and process
Two clinics in Puerto Rico with similar patient demographics were used to recruit participants. Both are funded by the United States Department of Health and Human Services Health Resources and Services Administration to provide care for economically disadvantaged people; at these clinics, patients receive whatever services they need, even if they cannot afford them. One clinic is located near the San Juan metropolitan area, and the other is located near the central east side of the island; their names are being kept confidential to maintain the anonymity of the recruited subjects. Both clinics primarily offer Spanish services to patients with OUD who speak Spanish. After the clinic assessed the inclusion and exclusion criteria, the study team proceeded to obtain written consent. Subjects were interviewed once to collect both data (ODAS and SDS questionnaire) and a blood sample; the researchers then collected additional information from the participant’s medical records. All the interviews and patient interactions took place face-to-face. The opiate dose adequacy scale (ODAS) and all clinical stabilization variable responses were collected during a routine appointment in a single interview based on patients’ status in the past 7 days.
2.3 Opiate dosage adequacy scale
The ODAS instrument is a Spanish-validated scale used to estimate the adequacy of buprenorphine dosing (1, 2). It involves a guided clinical interview in which the interviewer asks the patient specific questions about their experiences within the last week of the use of medication for OUD. Depending on the responses provided, the interviewer will either continue with the order or skip to the next questions. The interviewer will collect the responses from the patient. The interview consists of 10 questions, and it employs a multidimensional approach that assesses frequency of heroin use (Item 1) and its effect (narcotic blockade or crossed tolerance; Item 2), objective/subjective opioid withdrawal symptoms frequency and intensity of such symptoms (Items 3 and 4), heroin cravings frequency and intensity (Item 5), and overmedication frequency and intensity of symptoms (Item 6). Questions that measure symptom frequency are coded with Likert-type scale values (none of the last seven days, two or three of the last seven days, five or six of the last seven days, one or two times a day every day, three or more times a day every day; scored 5, 4, 3, 2, 1). Questions that measure symptom intensity are coded on a visual analogue scale 1-5 (no effect, 1; the effect was extremely intense, 5). The quantitative total ODAS score is calculated by the interviewer as the sum of all item scores, ranging from 6 to 30. If a patient reports not using illicit opioids, does not experience withdrawal symptoms or heroin cravings (narcotic blockade or crossed tolerance), does not experience signs or symptoms of overmedication, then a patient is considered to be “adequately dosed; ODAS score of 30.” (2) Higher scores indicate greater dose adequacy, while lower scores suggest dose inadequacy; however, the optimal cut-off points for determining dose adequacy are limited (1). This instrument also allows for dose adequacy to be interpreted qualitatively (yes or no) by assigning an adequate dose (yes) to patients who score 4 or 5 in all six items. Those who do not meet this condition are classified as patients with inadequate doses (no) (1).
For the purpose of this analysis, the ODAS qualitative dose adequacy condition was used to determine if a participant was considered adequately dosed (yes) or not (no). (1) The quantitative total score of dose adequacy of ODAS was used to assess the convergent validity with clinical variables such as severity of dependence, toxicology (illicit opioid use) and plasma levels of buprenorphine, and to estimate a clinically meaningful ODAS threshold (cut-off score) of dose adequacy.
2.4 Clinical stabilization variables
2.4.1 Severity of dependence scale
The Severity of Dependence Scale (SDS) is a 5-item scale that assesses substance-dependence severity (including cravings and withdrawal) over the previous 12 months. The responses to each item are coded on a Likert-type scale, and the total SDS score can range from 0 to 15 points, with a higher score indicating a greater degree of drug dependence. The SDS was originally developed by Gossop et al. (10) (10) and later translated into and adapted to Spanish (11).
2.4.2 Illicit drug use (toxicology results)
On the day of the study, the data on each participant’s electronic health record pertaining to urine toxicology results for heroin, cocaine, and unprescribed use of benzodiazepines, opioids, and/or fentanyl were used as a measure of illicit drug use (by means of urine drug testing kits).
2.5 Buprenorphine and metabolite plasma analysis
A single 5 mL blood sample using lavender/purple-colored EDTA vacutainer tubes was collected. Whole blood samples were centrifuged (3000 rpm; 10 minutes) to obtain plasma (supernatant). Plasma was stored at -80 °C in cryogenic tubes for the subsequent analytical analysis. Protein precipitation of plasma samples combined with ultra-high performance liquid-chromatography-mass spectroscopy was used to quantitate buprenorphine and three of its metabolites (norbuprenorphine, buprenorphine-3-glucuronide, and norbuprenorphine-3-glucuronide) (12).
2.6 Statistical analyses
Descriptive statistics were used to assess the distribution of sociodemographic characteristics (e.g., sex, age, education) among the sample of participants, these were presented with their respective frequencies and percentages. Mann-Whitney and Chi-squared tests were employed, as appropriate, to identify potential associations between opioid dose adequacy in its categorical form (yes/no) and each of the individual symptom frequency item scores (heroin use, narcotic blockade, subjective/objective symptoms, cravings, and overmedication; Likert-type scale values). Two-sided tests were used, and the mean, standard deviation, and respective percentiles were reported. To observe the correlation between the ODAS continuous score and the different clinical stabilization measures (SDS, illicit substance use, buprenorphine dose and plasma levels), Spearman and Pearson correlations were carried out. The internal consistency of the ODAS quantitative adequacy (6 items) was estimated using Cronbach’s alpha coefficient (mean standardized). (13) All statistical analyses were conducted using STATA/MP Parallel Edition 17.0. software (14).
A receiver operating characteristic (ROC) curve analysis was conducted to estimate an optimal ODAS cut-off for classifying dose adequacy (Python 3.11 and the Scikit-learn library v1.3). Using dose adequacy (yes or no) as the classification outcome (see section 2.2), cut-off values were determined based on the maximum Youden index of the area under the ROC curve (AUC) (15).
A sample size calculation showed that at least 96 participants are needed to have 80% power to detect a medium effect size at a two-sided significance level of α = 0.05, ensuring the study is adequately powered for psychometric validation.
3 Results
3.1 Demographics, past medical history, and pharmacological treatment of sample
In our sample, 101 out of 111 (90.99%) of the participants were men, 44% (N=39.64) had a high school degree or more (55% had high school as its highest degree) and 70% (N=63.06) were employed (Table 1). The mean age of the sample was 43 ( ± 10) years. All the patients were enrolled in the health care program provided by the government of Puerto Rico. Participants self-identified as Hispanic or Latino (72%), White (2%), or other (36%).
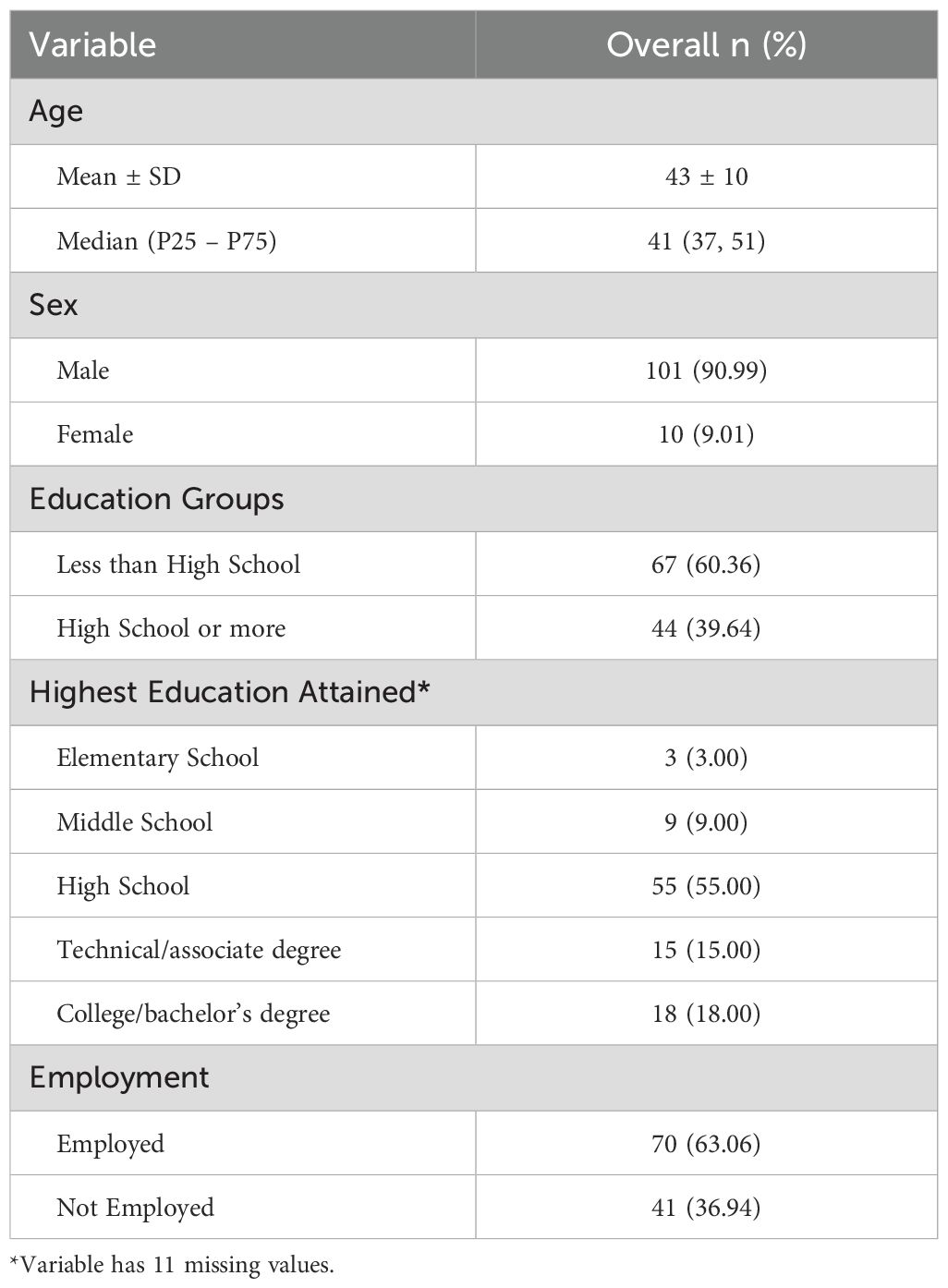
Table 1. Demographics of recruited subjects (n=111).
3.2 Opiate dosage adequacy scale
Qualitative adequacy: About 61 subjects (54.9%) of our sample were receiving an adequate dose of buprenorphine with a mean score of 29.79, as determined by the ODAS; 50 subjects had inadequate doses (45.0%; mean ODAS score of 23.60) (Table 2). Statistical analyses revealed significant differences among the dose adequacy groups for each item on the ODAS scale, as well as the total ODAS score (P-value < 0.001).
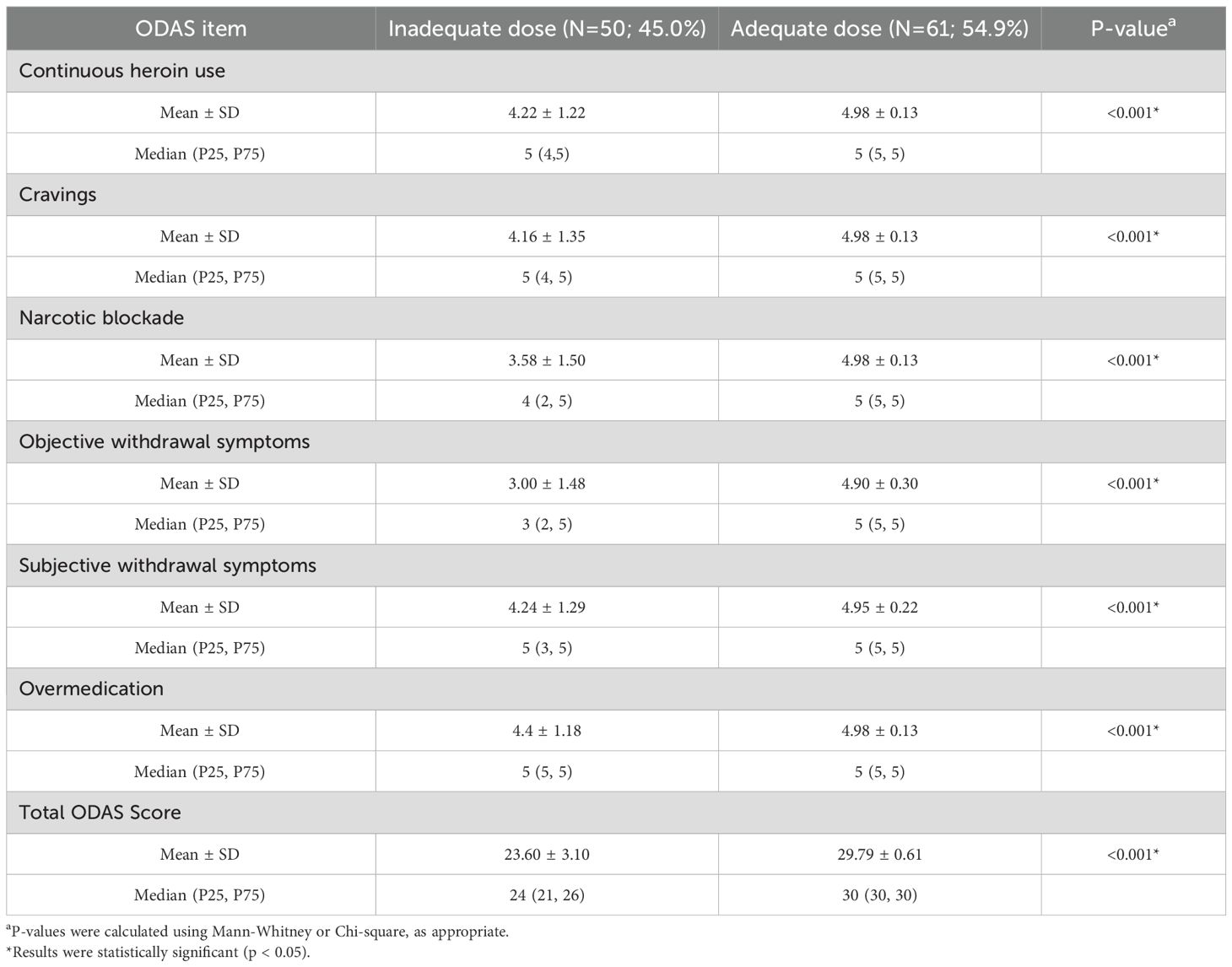
Table 2. ODAS item scores comparison with determined dose adequacy (n=111).
In this sample, the Cronbach’s alpha coefficient was 0.615, thus supporting a moderate internal consistency of the quantitative dose adequacy (16).
The ROC analysis revealed that ODAS scores ≥ 29 were highly predictive of dose adequacy, with an AUC of 0.996, demonstrating strong discriminative power.
3.3 Opiate dosage adequacy scale validity
3.3.1 ODAS adequacy scores, clinical stabilization measures, and buprenorphine plasma concentrations
Table 3 illustrates the mean and median values of the clinical stabilization measures (Severity of Dependence, illicit substance use, and buprenorphine dose and plasma levels) for the dose adequacy groups as qualitatively determined. Table 3 also shows the correlation coefficients between these clinical stabilization measures and the quantitative ODAS score, as well as its p-value. Moderately strong correlations were found between the clinical stabilization measures and dose adequacy as determined by the ODAS. The severity of dependence, illicit drug use, and buprenorphine dose all resulted in being inversely proportional with the ODAS score (all statistically significant). This means that the greater the severity of dependence, the lower the ODAS score (less adequate). The same resulted for the use of illicit opioids; more frequently reported substance use resulted in lower ODAS scores, hence less probable adequate doses. Higher buprenorphine doses were associated with lower ODAS scores (less dose adequacy). Buprenorphine plasma levels were inversely correlated to the ODAS score, meaning that increasing plasma levels correlated with a higher probability of dose adequacy.
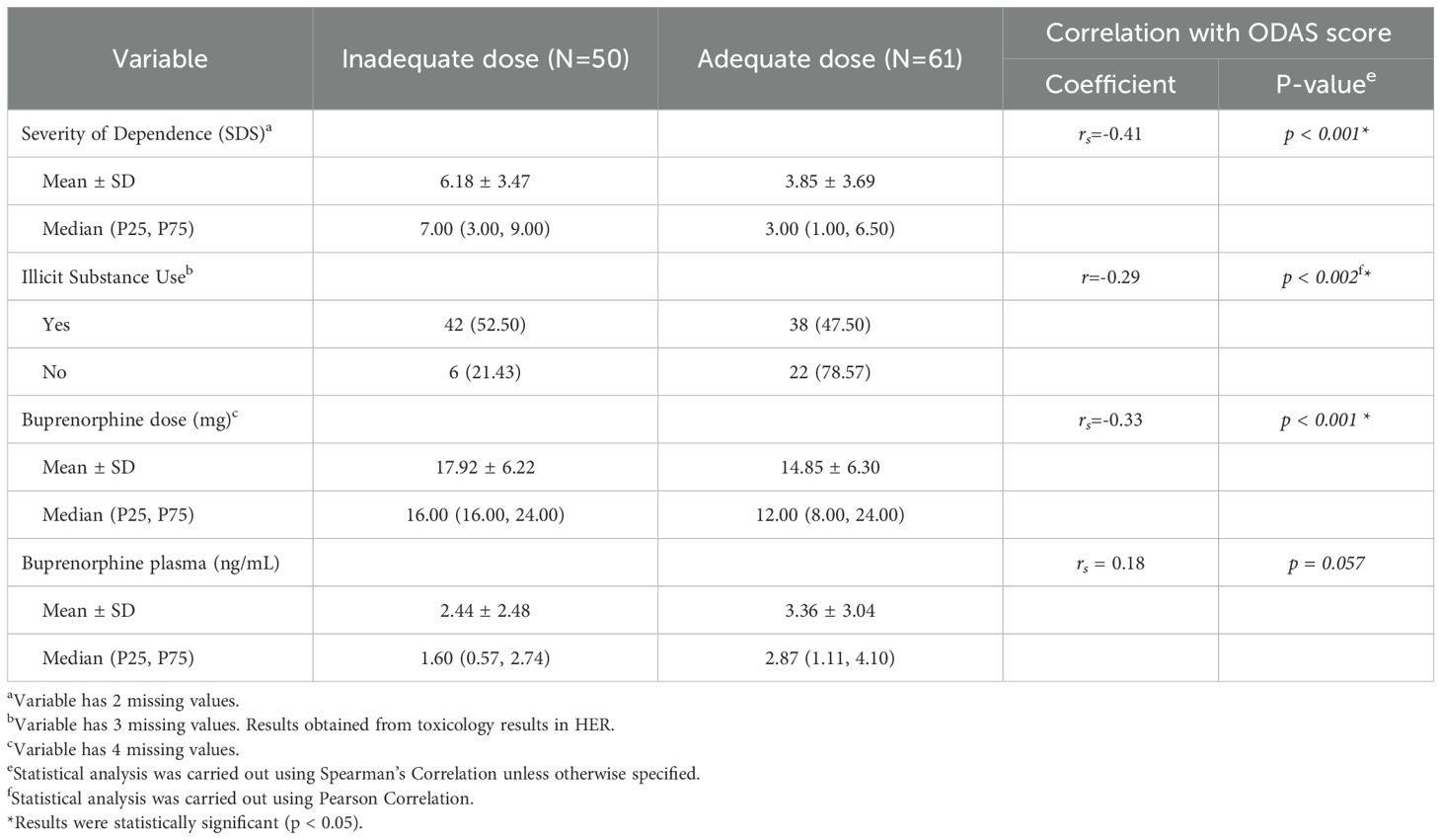
Table 3. ODAS adequacy scores and clinical stabilization measures (n=111).
3.4 Plasma-to-dose ratio by dosing frequency
To further explore the observed variability in dose, dose adequacy and plasma levels, we examined the mean plasma concentration per mg of buprenorphine (plasma/dose ratio) across dosing frequencies. As shown in Figure 1, participants who split their daily dose more frequently did not consistently achieve higher plasma exposure per mg, and variability was notable across all frequency groups. Individual data points and standard deviations illustrate this heterogeneity in exposure efficiency.
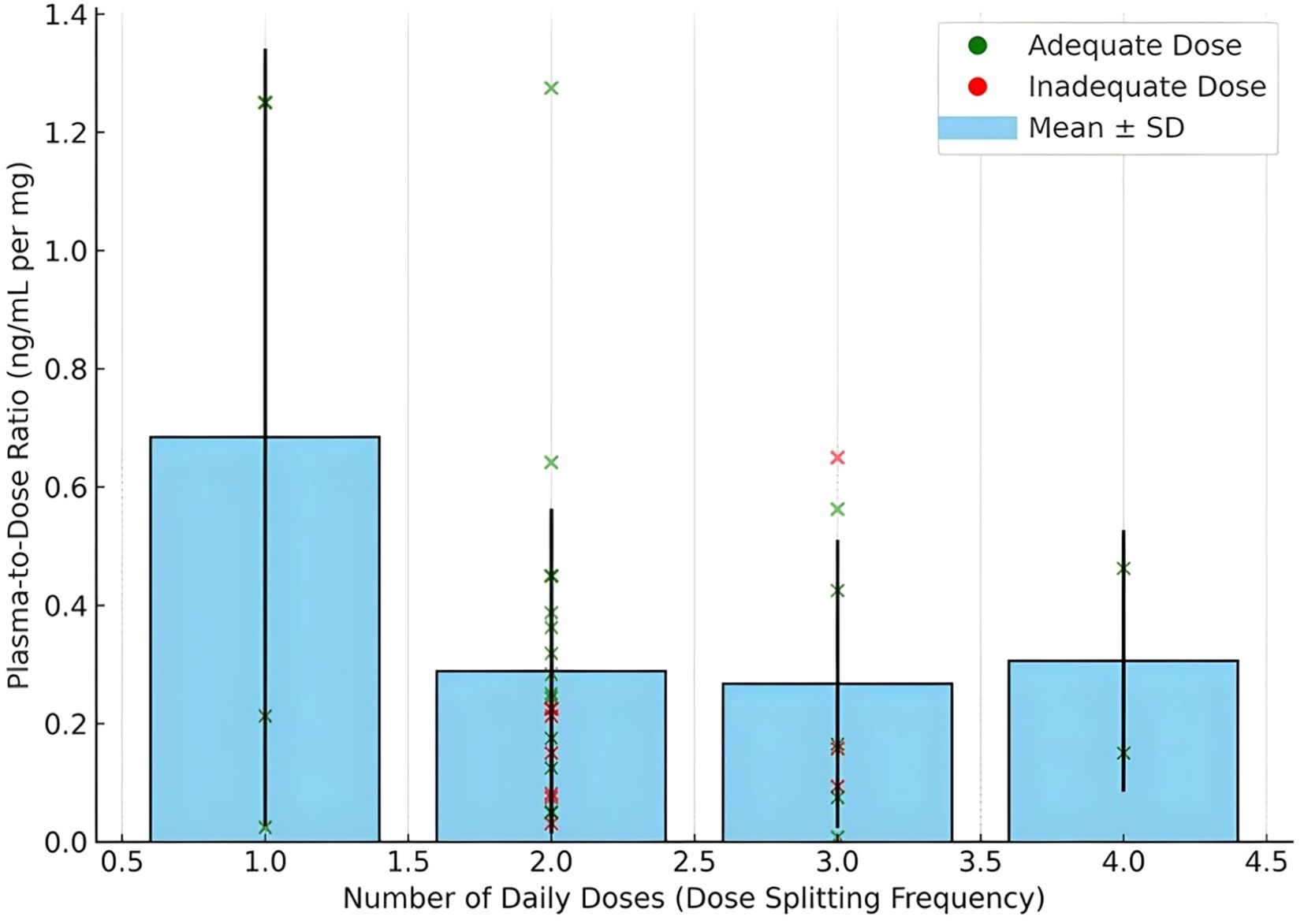
Figure 1. Plasma concentration per mg of Buprenorphine (daily dose) by dosing frequency of recruited subjects as determined by ODAS. Bars represent mean values with standard deviation error bars. Individual dots indicate observed plasma/dose values per participant. The data illustrate variability in plasma exposure efficiency across dose splitting patterns.
4 Discussion
The results reported herein support the use of the Opiate Dose Adequacy Scale (ODAS) in Spanish-speaking, non-European individuals maintained on buprenorphine. Our study subjects closely matched the demographic profiles, including age, sex, education, and employment distributions, of those in previously reported ODAS convergent validity studies conducted in Europe (2).
The dose-adequacy distribution of recruited subjects (54.9% were adequately dosed; mean total score: 29.79 ± 0.61) was lower than that reported for Europeans (73.3%; mean total score: 28.58 ± 2.55); more patients had an inadequate dose in this study (2). Our results demonstrated the ODAS’s capability to discriminate between adequately and inadequately dosed individuals, as evidenced by statistically different ODAS total scores between groups. Item 4, objective withdrawal symptoms, had the lowest scores in both groups (which was also the case for the European subjects). This item can then be an indicator of dose inadequacy (subtotal score < 4) in this population; a major cause for dose inadequacy. The optimal ODAS cut-off score for this group has been identified as 29. Patients with scores greater than 29 are significantly more likely to receive an adequate dose, while those with scores less than 29 tend to be inadequately dosed. Further studies are essential to validate this cut-off value for a clear classification of dose adequacy within this population, particularly focusing on patients’ objective withdrawal symptoms (item 4), as these symptoms can significantly impact dose adequacy. These results, consistent with previous findings, have demonstrated that the ODAS can be used to determine dose adequacy in a group of non-European Spanish-speaking patients with OUD and, as such, can be used as a clinical assessment for providers to identify patients that require a dose adjustment and improve maintenance treatment effectiveness (1, 2, 4). Further implementation studies should be conducted to test this intervention properly.
While the internal consistency of the ODAS in this sample was moderate (Cronbach’s α = 0.615), we acknowledge that Cronbach’s alpha has certain limitations when applied to Likert-type scales. Specifically, it assumes tau-equivalence and continuous measurement, which may not fully reflect the reliability of ordinal, symptom-based responses. Future analyses should consider alternative indices such as ordinal alpha or McDonald’s omega, which are better suited for ordinal data and can provide more robust estimates of internal consistency (17). Additionally, inter-rater reliability (IRR) was not assessed in this study because all interviews were conducted by a single trained researcher. While this minimized variability in scoring, it also limits our ability to assess consistency across different raters. Future studies should evaluate IRR through standardized methods (e.g., intraclass correlation or Cohen’s kappa), particularly given the semi-structured format of the ODAS, to ensure generalizability across clinical settings.
One important finding of this study was that dose adequacy was inversely proportional to the prescribed daily dose of buprenorphine; inadequately dosed patients had higher prescribed doses than those with adequate doses. Inadequately dosed patients in this study, having mean plasma values of 2.44 ng/mL (median 1.60), can explain their low treatment effectiveness (dose inadequacy) even though having higher doses than the adequately dosed group. Plasma levels of ≥ 3 ng/mL are required for a higher (> 80%) saturation of the opioid receptors and, therefore, treatment effectiveness (18). Patients in the adequate dose group had average plasma levels of 3.36 ng/mL. The reason for patients with inadequate doses having lower plasma levels than patients with adequate doses, even though taking relatively higher doses, may be explained by a combination of patient compliance regarding dosing schedules and pharmacological characteristics in this group.
To further explore the observed results between buprenorphine dose, plasma levels, and clinical dose adequacy, we examined the plasma-to-dose ratio (ng/mL per mg of buprenorphine) across different dose splitting frequencies. As illustrated in Figure 1, mean plasma-to-dose ratios varied across dosing patterns, with high inter-individual variability evident within each group. When stratified by dose adequacy, the plot shows that adequately dosed participants (green) generally achieved higher plasma exposure efficiency than inadequately dosed participants (red), even when using similar or lower total daily doses. This suggests that higher prescribed doses in the inadequate group did not translate into proportionally higher plasma concentrations, potentially due to suboptimal adherence, metabolic differences, or pharmacokinetic fluctuations associated with irregular dosing schedules.
Notably, the majority of participants in this sample reported dividing their daily buprenorphine dose into two to six doses per day, often following asymmetric or personalized patterns. These practices, while common, may lead to variability in trough plasma levels, particularly in the inadequate group. The data underscore the importance of considering pharmacokinetic efficiency, not just total dose, in assessing and optimizing buprenorphine treatment. Incorporating both clinical assessment tools like ODAS and objective pharmacokinetic data may offer a more complete understanding of dose adequacy in diverse treatment populations. Evidenced-based dosing schemes are an alternative, even more so in the current fentanyl era within the opioid crisis where higher (>24 mg) and varied dosing schemes are proposed as treatment effectiveness increase strategies (19, 20).
Building on these findings, our team has previously developed a population pharmacokinetic (popPK) model tailored to Spanish-speaking individuals with opioid use disorder in Puerto Rico (20). This model quantitatively characterizes buprenorphine exposure and predicts steady-state plasma levels under different dosing regimens. Notably, the model suggests that standard daily dosing may be insufficient to maintain therapeutic plasma levels (>3 ng/mL) in a significant proportion of patients, particularly those with altered absorption or metabolism. In contrast, higher total daily doses administered in divided dosing schedules (e.g., 8 mg TID or 16 mg BID) were shown to better sustain receptor saturation and minimize trough concentrations.
These findings support the use of the ODAS as a practical and psychometrically sound tool for assessing buprenorphine dose adequacy in Spanish-speaking populations outside of Europe. The scale’s ability to capture multidimensional markers of clinical stability, combined with pharmacokinetic data, highlights the complexity of dose-response relationships in opioid use disorder treatment. Notably, participants classified as inadequately dosed exhibited lower plasma-to-dose ratios despite receiving higher daily doses, suggesting suboptimal exposure efficiency. Divided or asymmetric dosing patterns, commonly observed in this sample, may contribute to these discrepancies. To address this, the integration of a population pharmacokinetic (popPK) model with ODAS-based assessment offers a translational approach for identifying patients who may benefit from optimized dosing schedules. This model may be used to guide individualized dose adjustments, aiming to maintain therapeutic plasma levels and improve treatment outcomes. In the meantime, providers can use ODAS scores in conjunction with assessments of objective withdrawal symptoms and patient-reported dosing behaviors to inform clinical decisions or reinforce buprenorphine adherence education. Ultimately, combining clinical insight with pharmacokinetic guidance represents a promising strategy to enhance treatment precision and effectiveness among Spanish-speaking individuals with opioid use disorder.
5 Conclusion
The psychometric evaluation of the ODAS in this Hispanic sample lays the groundwork for its broader application across Spanish-speaking populations in the Americas. As opioid use disorder continues to disproportionately affect underserved and linguistically diverse communities in the United States and Latin America, the availability of culturally responsive and clinically validated tools to assess treatment adequacy is increasingly critical (21, 22). The ODAS, with its multidimensional structure and adaptable interview format, offers a valuable resource to support evidence-based decision-making, guide individualized buprenorphine dose adjustments, and promote more equitable treatment outcomes in diverse care settings. The present study demonstrates that the ODAS shows acceptable psychometric properties in a non-European Hispanic population, consistent with results from the original Spanish validation and subsequent European studies. Similar to findings in Spanish and German cohorts, we observed good internal consistency and evidence of construct validity, supporting the robustness of the ODAS framework across diverse cultural contexts. However, important differences also emerged. In contrast to European samples, where higher proportions of patients achieved and sustained dose adequacy, our data reflect lower frequencies of dose adequacy, partially explained by features that are common in this population but rarely reported in European cohorts; frequent divided dosing practices. These contextual differences underscore that while the ODAS can reliably capture dose adequacy across populations, interpretation of scores must consider local patterns of treatment delivery and patient behavior.
Clinically, this work highlights the importance of validating measurement tools beyond their original populations. For non-European Hispanic groups, particularly those in high-risk communities with variable treatment adherence, the ODAS offers a structured method for assessing dose adequacy that accounts for the realities of practice. Incorporating the ODAS into care in such settings may support more precise dose adjustments and improved treatment retention. By documenting both consistencies and differences relative to European validation studies, our findings contribute to a more generalizable evidence base for the ODAS and emphasize the need to tailor implementation strategies to cultural and clinical contexts.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statement
The studies involving humans were approved by University of Puerto Rico Medical Sciences Campus Institutional Review Board. The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
Author contributions
TF: Writing – original draft, Investigation, Formal Analysis. NR: Formal Analysis, Writing – original draft. JD: Writing – review & editing, Visualization, Resources, Validation, Formal Analysis, Conceptualization. RV: Formal Analysis, Resources, Validation, Investigation, Writing – review & editing. FG: Visualization, Validation, Writing – review & editing. DS: Writing – review & editing, Funding acquisition, Visualization, Project administration, Formal Analysis, Software, Resources, Validation, Methodology, Supervision, Conceptualization, Investigation.
Funding
The author(s) declare financial support was received for the research and/or publication of this article. Funding sources: This work was supported by the National Institutes of Health, grant numbers S21MD001830, R25MD007607, and U54GM13380.
Acknowledgments
The authors gratefully acknowledge the support of the clinics and healthcare providers who facilitated participant recruitment for this study. Their collaboration and commitment to advancing care for individuals with opioid use disorder were essential to the success of this research.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Generative AI statement
The author(s) declare that Generative AI was used in the creation of this manuscript. During the preparation of this work the authors used OpenAI in order to support the editing process, figure preparation, and to improve the readability and language of the manuscript. After using this tool/service, the authors reviewed and edited the content as needed and take full responsibility for the content of the publication. The authors declare that Gen AI was used in the creation of this manuscript.
Any alternative text (alt text) provided alongside figures in this article has been generated by Frontiers with the support of artificial intelligence and reasonable efforts have been made to ensure accuracy, including review by the authors wherever possible. If you identify any issues, please contact us.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Abbreviations
ODAS, Opiate Dosage Adequacy Scale; OUD, opioid use disorder; SDS, Severity of Dependence Scale.
References
1. González-Saiz F, Rojas OL, Gómez RB, Acedos IB, Martínez JG, Collantes MAG, et al. Evidence of reliability and validity of the opiate dosage adequacy scale (ODAS) in a sample of methadone maintenance patients. Heroin Addict Relat Clin Probl. (2008) 10:25–38. doi: 10.1016/j.drugalcdep.2017.10.035
2. González-Saiz F, Lozano Rojas O, Trujols J, Alcaraz S, Siñol N, Pérez de Los Cobos J, et al. Evidence of validity and reliability of the Opiate Dosage Adequacy Scale (ODAS) in a sample of heroin addicted patients in buprenorphine/naloxone maintenance treatment. Drug Alcohol Depend. (2018) 183:127–33. doi: 10.1016/j.drugalcdep.2017.10.035
3. González-Saiz F. Escala de Adecuación de Dosis de Opiáceos (EADO): un nuevo instrumento para la evaluación clínica del ajuste de las dosis de metadona. Trastornos Adictivos. (2009) 11:24–34. doi: 10.1016/S1575-0973(09)71376-5
4. Walcher S, Koc J, Reichel V, Schlote F, Verthein U, and Reimer J. The opiate dosage adequacy scale for identification of the right methadone dose–a prospective cohort study. BMC Pharmacol Toxicol. (2016) 17:15. doi: 10.1186/s40360-016-0058-9
5. D’Egidio PF, Bignamini E, De Vivo E, Leonardi C, Pieri MC, González-Saiz F, et al. METODO, A prospective observational study to assess the efficacy and tolerability of methadone in heroin-addicted patients undergoing a methadone maintenance treatment: preliminary results at baseline evaluation. Subst Use Misuse. (2013) 48:1530–40. doi: 10.3109/10826084.2013.800886
6. Dematteis M, Auriacombe M, D’Agnone O, Somaini L, Szerman N, Littlewood R, et al. Recommendations for buprenorphine and methadone therapy in opioid use disorder: a European consensus. Expert Opin Pharmacotherapy. (2017) 18:1987–99. doi: 10.1080/14656566.2017.1409722
7. Golnezhad A, Torkaman-Boutorabi A, Mohammad Razaghi E, Zarrindast MR, Yadollahi S, Dousti Kataj P, et al. Psychometric characteristics of the Persian version of the opiate dosage adequacy scale (ODAS). Basic Clin Neurosci. (2023) 14:471–8. doi: 10.32598/bcn.2023.2756.1
8. Esteve R, Reyes-Pérez Á, Ramírez-Maestre C, Gutiérrez-Extremera A, Fuentes-Bravo R, de la Vega R, et al. Diagnostic and predictive capacity of the Spanish versions of the Opioid Risk Tool and the Screener and Opioid Assessment for patients with pain-Revised: A preliminary investigation in a sample of people with noncancer chronic pain. Pain Ther. (2022) 11:493–510. doi: 10.1007/s40122-022-00356-2
9. Opioid and Illicit Drug Use Among the Hispanic/Latino Populations (2019). Available online at: https://www.samhsa.gov/blog/opioid-illicit-drug-use-among-hispaniclatino-populations (Accessed April 28, 2025).
10. Gossop M, Darke S, Griffiths P, Hando J, Powis B, Hall W, et al. The Severity of Dependence Scale (SDS): psychometric properties of the SDS in English and Australian samples of heroin, cocaine and amphetamine users. Addiction. (1995) 90:607–14. doi: 10.1046/j.1360-0443.1995.9056072.x
11. González-Saiz F, de Las Cuevas C, Barrio G, and Domingo-Salvany A. Spanish version of the severity of dependence scale (SDS). Med clinica. (2008) 131:797–8. doi: 10.1016/s0025-7753(08)75509-x
12. Bastian JR, Chen H, Zhang H, Rothenberger S, Tarter R, English D, et al. Dose-adjusted plasma concentrations of sublingual buprenorphine are lower during than after pregnancy. Am J Obstetrics Gynecology. (2017) 216:64.e1–7. doi: 10.1016/j.ajog.2016.09.095
13. Cronbach LJ. Coefficient alpha and the internal structure of tests. Psychometrika. (1951) 16:297–334. doi: 10.1007/BF02310555
15. Mandrekar JN. Receiver operating characteristic curve in diagnostic test assessment. J Thorac Oncol. (2010) 5:1315–6. doi: 10.1097/JTO.0b013e3181ec173d
16. Taber KS. The use of cronbach’s alpha when developing and reporting research instruments in science education. Res Sci Educ. (2018) 48:1273–96. doi: 10.1007/s11165-016-9602-2
17. Gadermann Anne M, Martin G, and Zumbo BD. Estimating ordinal reliability for Likert-type andordinal item response data: A conceptual, empirical, and practical guide. Practical Assessment, Research & Evaluation, (2012) 17. Available online at: http://pareonline.net/getvn.asp?v=17&n=3 (Accessed February 20, 2025).
18. Greenwald MK, Comer SD, and Fiellin DA. Buprenorphine maintenance and mu-opioid receptor availability in the treatment of opioid use disorder: implications for clinical use and policy. Drug Alcohol Depend. (2014) 144:1–11. doi: 10.1016/j.drugalcdep.2014.07.035
19. Grande LA, Cundiff D, Greenwald MK, Murray M, Wright TE, and Martin SA. Evidence on buprenorphine dose limits: A review. J Addict Med. (2023) 17:509–16. doi: 10.1097/ADM.0000000000001189
20. Santiago D, Mangas-SanJuan V, Melin K, Duconge J, Zhao W, and Venkataramanan R. Pharmacokinetic characterization and external evaluation of a quantitative framework of sublingual buprenorphine in patients with an opioid disorder in Puerto Rico. Pharmaceutics. (2020) 12:1226. doi: 10.3390/pharmaceutics12121226
21. Paul NB, Lopez LA, Strong MN, and Donohue B. Cultural Considerations in the Behavioral And Treatment ofSubstance-Related Disorders. In: Benuto, L.T., Gonzalez, F.R., Singer, J. (eds) Handbook of Cultural Factors in Behavioral Health. (2020). (Cham: Springer). doi: 10.1007/978-3-030-32229-8_28
Keywords: opiate dosage adequacy scale, ODAS, opioid use disorder, buprenorphine, convergent validity, realiability
Citation: Flores Ocasio T, Rivera NM, Duconge J, Venkataramanan R, González-Saiz F and Santiago D (2025) Psychometric evaluation of the opiate dosage adequacy scale: reliability and convergent validity among non-European Spanish-speaking buprenorphine patients. Front. Psychiatry 16:1644076. doi: 10.3389/fpsyt.2025.1644076
Received: 09 June 2025; Accepted: 13 October 2025;
Published: 14 November 2025.
Edited by:
Yukiko Washio, RTI International, United StatesReviewed by:
Anastasio Tini, Marche Polytechnic University, ItalyMariana Campello De Oliveira, Department of Health, Brazil
Copyright © 2025 Flores Ocasio, Rivera, Duconge, Venkataramanan, González-Saiz and Santiago. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Darlene Santiago, ZGFybGVuZS5zYW50aWFnb0B1cHIuZWR1