 Elizabeth A. Kruse
Elizabeth A. Kruse David Dodell-Feder
David Dodell-Feder- 1Department of Psychology, University of Rochester, Rochester, NY, United States
- 2Department of Neuroscience, University of Rochester Medical Center, Rochester, NY, United States
Introduction: Within healthcare settings, schizophrenia spectrum disorder (SSD) stigma is pervasive and presents significant barriers to recovery and equitable care. Understanding the sources, nature, and moderators of such stigma among healthcare providers is essential for informing targeted interventions.
Methods: We conducted a systematic review of 44 peer-reviewed studies examining SSD-related stigma among diverse healthcare providers, including trainees, nurses, general practitioners, psychiatrists, psychologists, and community health workers. Studies were synthesized to identify common manifestations of stigma, as well as professional and demographic moderators.
Results: Stigma was observed across all healthcare professions, manifesting through stereotypes, prejudices, and discriminatory behaviors. Consistent patterns included higher stigma among generalist providers compared to mental health specialists and reduced stigma associated with greater professional experience and personal contact with individuals with SSDs. Findings regarding other moderators, such as age, gender, and etiological beliefs, were mixed.
Discussion: SSD stigma is widespread within healthcare and varies by provider type, training, and personal experience. Interventions to reduce stigma should be tailored to specific provider groups and contexts. Future research should employ longitudinal and mixed-method designs to clarify moderator effects and assess targeted anti-stigma strategies.
Introduction
Schizophrenia spectrum disorders (SSDs) are among the most stigmatized mental health disorders in the world (1–3). Affecting approximately 24 million people worldwide, SSDs represent a significant public health concern, contributing to chronic disability, reduced quality of life, and reduced life expectancy (4). The burden of disease is widespread across systems and resources, but, has the most severe impact on the affected individual, largely due to stigma—the social devaluation or disapproval of a person based on a perceived characteristic (5). Stigma among individuals with SSDs has been consistently associated with increased suicidal ideation and attempts, hopelessness and depression, and decreased quality of life, self-esteem, and social functioning (6–9). Its effects are so profound that it has been described as a “second illness” (10).
As recognition of SSD-stigma has grown, efforts have been made to understand how it forms and persists. Stigma has several dimensions: perceived stigma (belief that others hold negative views), anticipated stigma (expectation of future discrimination), experienced stigma (actual discriminatory encounters), and self-stigma (the internalization of stigma leading to a negative self-view or “illness identity”; 11). These dimensions create a multifaceted barrier to recovery, influencing individuals’ willingness to seek help, adhere to treatment, and engage with social and professional networks. Stigma manifests through stereotypes (e.g., beliefs about dangerousness or incompetence), prejudices (e.g., negative evaluations involving fear or pity), and discriminatory behaviors (e.g., avoidance or exclusion) (12–14).
The stigma surrounding SSDs has deep historical roots, shaped by centuries of fear and misunderstanding. Early conceptions portrayed individuals as dangerous and morally deficient, often invoking supernatural explanations used to justify inhumane institutionalization of affected individuals (15–17). Though contemporary views and practices have evolved, harmful attitudes persist, reinforced by cultural narratives and media depictions that associate psychosis with violence (10). Stigma may be ubiquitous, but may be particularly consequential when held by healthcare providers, who often serve as the first point of contact and are well-positioned to influence the quality and trajectory of care. Paradoxically, research increasingly shows that stigma is pervasive even within healthcare settings, manifesting as implicit biases, avoidance behaviors, and therapeutic pessimism (18). Alarmingly, these attitudes are not confined to general healthcare providers; even mental health professionals (MHPs)—those most intimately involved in supporting individuals with SSDs—may perpetuate stigma through subtle or overt behaviors, such as underestimating patients’ capabilities, adopting overly paternalistic approaches, or failing to examine their own biases (19).
This raises the question: does stigma differ across provider types in ways that meaningfully affect care? Unfortunately, studies rarely compare stigma between provider groups (e.g., psychologists versus nurses), leaving unclear how stigma manifests across professions (1, 3, 20, 21). Differences are likely, given variations in education, training, patient contact, and professional roles. For example, a provider working within a recovery-oriented framework that promotes self-efficacy, and who has observed positive patient outcomes over the years, may differ significantly from someone with little experience working with SSDs who takes a strictly biogenetic perspective. Understanding how stigma varies by provider group, and the factors that shape these differences, is critical for developing targeted, sustainable stigma-reduction efforts.
Theoretically, provider stigma can be understood through an integration of social and affective frameworks. The contact hypothesis posits that stigma may be reduced by positive, frequent interactions in equitable environments—those promoting equal status, cooperation (i.e., shared decision making), and institutional support (22). Indeed, providers who work closely with individuals with SSDs, such as psychiatrists and mental health nurses, often exhibit lower stigma (23). However, contact alone may be insufficient; without adequate training or support, challenging interactions can reinforce negative attitudes and stereotypes (24). Thus, providers lacking positive, frequent contact may be especially prone to higher stigma. Complementing the contact hypothesis, attribution theory (25) explains how casual beliefs influence emotional and behavioral responses. In clinical care, providers may attribute SSDs to internal or external, stable or unstable, and controllable or uncontrollable causes. These attributions influence emotional responses—such as pity, frustration, or fear—which then guide behavior. For example, providers who attribute SSDs to uncontrollable, biogenetic factors may experience emotions such as pity, which can reduce blame, but increase paternalistic attitudes and reduce empathy (26, 27). Conversely, when SSDs are attributed to personal failure, providers may experience anger or frustration, reinforcing avoidance or judgment. Intergroup emotion theory (28) adds a critical group-based lens, highlighting how emotional responses are shaped not only by individual appraisals but by perceived group membership. When individuals with SSDs are viewed as part of an “outgroup,” emotions like fear or disgust may intensify, particularly when tied to stereotypes of dangerousness or unpredictability, which can drive stigmatizing behaviors (29–31). These affective responses, shaped by both attributional and group-based logic, are central to understanding stigma in clinical settings. Providers who feel unprepared to manage complex symptoms may experience these emotions more intensely, increasing the risk of avoidance and disengagement.
Adopting a broader lens, the social-ecological model (32) helps illustrate how stigma, and the aforementioned social and affective processes, operates across interdependent levels. Individually, providers may internalize societal narratives that portray SSDs as dangerous or untreatable. Interpersonally, these attitudes may manifest as microaggressions or therapeutic pessimism. Structurally, stigma can be embedded in institutions, a concept referred to as “structural stigma,” manifesting through factors such as underfunded services, insufficient training opportunities, or policy barriers that limit access to care (33). These conditions both reflect and reinforce stigma, shaping provider behavior and impeding equitable care (33). The social-ecological model highlights how stigma emerges through feedback loops, e.g., how individual provider beliefs (micro) shape institutional practices (macro), and how systemic factors reinforce individual attitudes. Within this framework, attribution and intergroup emotion theories explain how providers’ causal beliefs shape affective and behavioral responses, while the contact hypothesis highlights the role of experience. This integrated, multi-level model (Figure 1) offers a comprehensive account of how stigma develops and persists among healthcare providers, and underscores the need for interventions that target these intersecting levels.
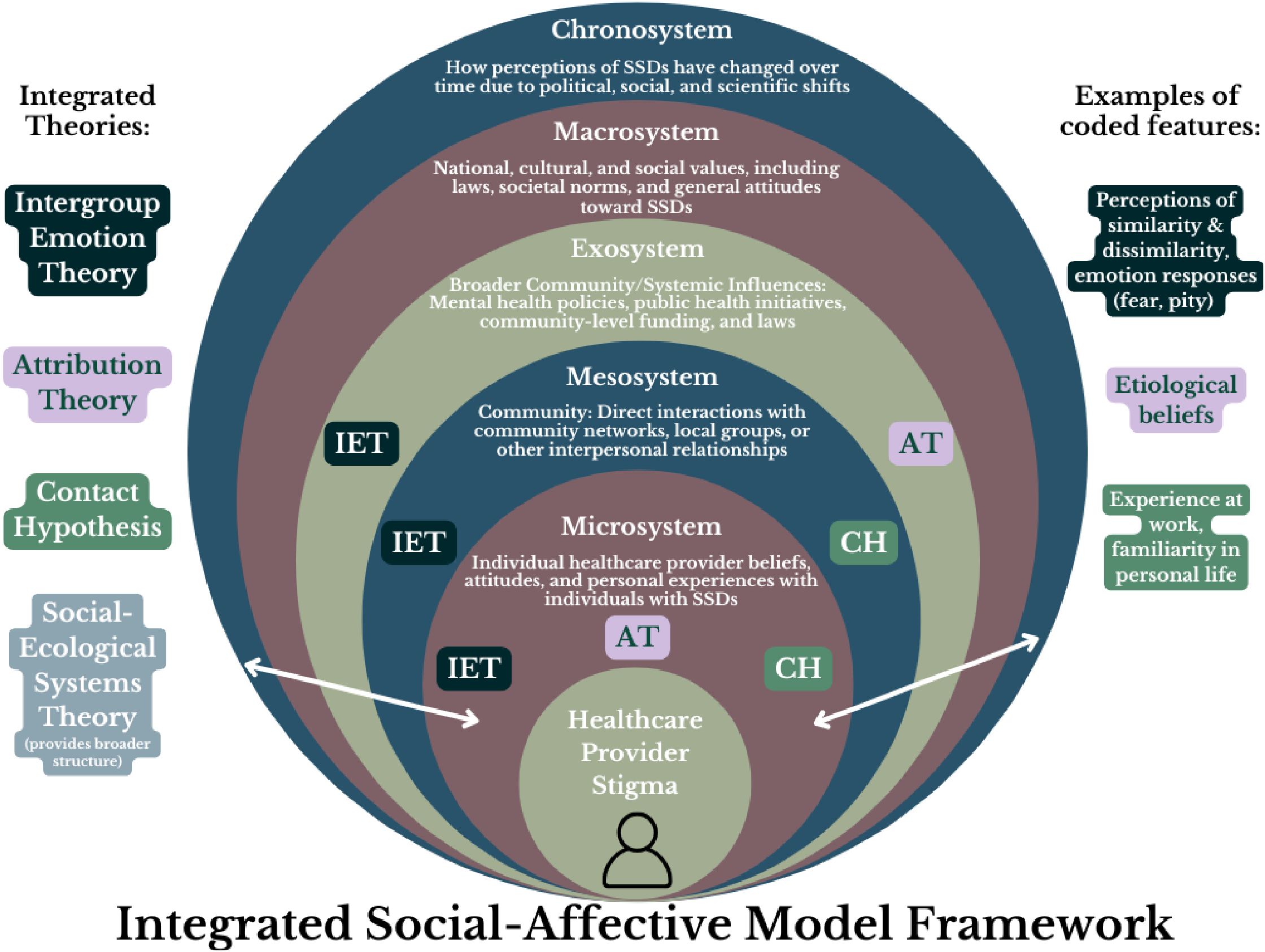
Figure 1. Visual depiction of an integrated social-affective model framework.
Despite growing attention to provider-based stigma (2), significant gaps remain. Much of the literature focuses on subsets of providers, such as nurses (1), MHPs (2, 21, 34), or primary care providers (35), limiting generalizability and comparison across roles. Moreover, given widespread stigma toward psychotic symptoms (2, 36, 37), and the dimensional nature of psychosis (38, 39), it is important to examine stigma across the full schizophrenia spectrum. Thus, the aim of this systematic review was to synthesize research on stigma towards the full schizophrenia spectrum (i.e., psychotic-like experiences in the general population to a SSD) among different groups of healthcare providers. These insights are essential for designing effective, context-sensitive interventions.
Methods
This review adhered to the PRISMA 2020 guidelines (40), and the study selection process is outlined in the PRISMA flowchart (Figure 2). A review protocol was not pre-registered on PROSPERO. We did not conduct a formal assessment of the strength or certainty of evidence (e.g., using GRADE; 41) due to the narrative nature of the review, the heterogeneity of measures and outcomes across studies, and the primary aim of characterizing provider-based stigma rather than evaluating intervention effects.
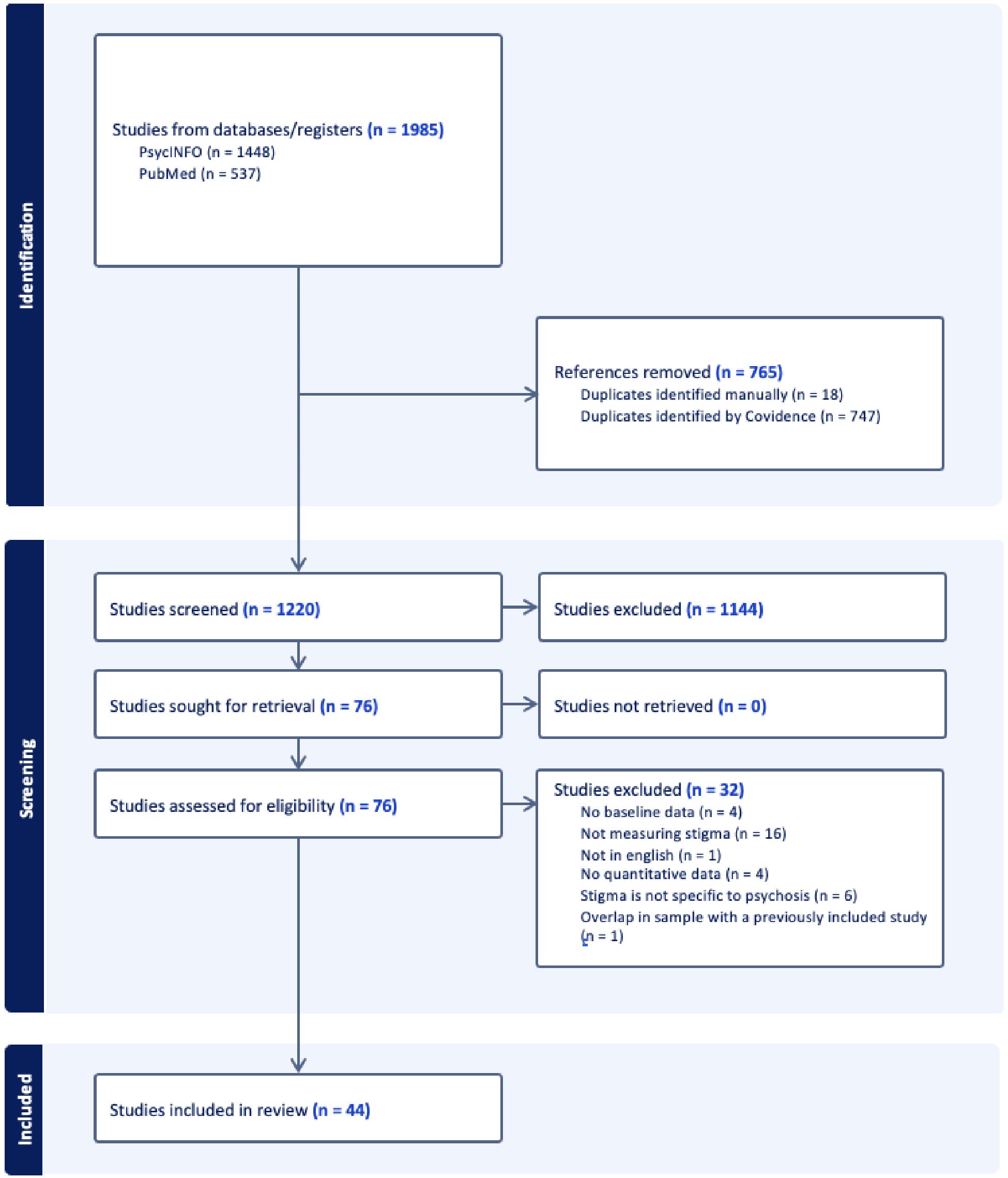
Figure 2. PRISMA flowchart for systematic search and identification of included studies.
Eligibility criteria
Studies were included for review if they were: written in English; contained original data; were published in a peer-reviewed journal; collected and reported quantitative data; investigated stigma related to the schizophrenia spectrum specifically (versus mental illness broadly); and included participants that were healthcare providers. We did not impose a publication date restriction in order to capture the full range of relevant literature on schizophrenia stigma among healthcare providers. However, we acknowledge that attitudes regarding SSDs have shifted over time, and we further address this consideration in the Limitations section.
Search strategy
The literature search was conducted in two electronic databases—PsycINFO and PubMed—using search terms for schizophrenia/psychosis, stigma, and provider: (schizo* OR psychosis OR psychotic) AND (stigma OR attitude OR stereotype OR bias OR discrimination OR prejudice) AND (professional OR provider OR doctor OR medical provider OR healthcare provider OR mental health professional OR nurse OR psychologist OR psychiatrist OR therapist OR social worker OR case manager OR paramedic OR EMT). The initial search on September 16, 2024 had the following output: 633 records (PsycINFO), 491 records (PubMed). After initial pilot screening, to capture healthcare providers in training and “physicians,” we added the following terms on October 12, 2024: (OR medical student OR graduate student OR trainee OR student OR physician). The second search had the following unique output (i.e., after removal of duplicates from initial search): 797 records (PsycINFO), 10 records (PubMed). A final update search with all search terms was conducted on April 30, 2025, and had a date constraint from 09/16/2024 to 04/30/2025 to capture only newly published records. This search had the following output: 18 records (PsycINFO), 36 records (PubMed). The first author and an undergraduate research assistant performed the initial round of screening using the title and abstract. Next, full texts were retrieved, coded by the first author (see below), and evaluated against our inclusion criteria. Discrepancies in screening decisions were discussed, and consensus was reached through adjudication by both authors.
Coding procedures
Study screening and coding were performed using Covidence, a web-based collaboration software platform that streamlines systematic reviews (42). In the initial screening phase, studies were excluded (n = 1102) if they were not original research (e.g., review papers, editorials, etc.), did not include healthcare providers as participants in their sample (e.g., measurement of experienced stigma from client perspective), did not mention stigma, did not mention SSDs, or were not written in English.
Study features were selected using a hybrid approach. Core coding categories (e.g., study design, sample characteristics, stigma measurement, the majority of the moderators) were determined a priori based on prior literature and systematic review guidelines (2, 43). However, additional features (e.g., moderator of personal experience with mental illness) emerged during the review and were incorporated into the coding framework as they became relevant. This approach ensured both theoretical rigor and responsiveness to the data.
The results are organized by key study features. First, findings are presented by provider type, the primary focus of this review. Next, results are organized by potential moderators of stigma (e.g., age, gender, workplace setting). Stigma features (e.g., social distance, perceptions of dangerousness) are highlighted throughout both sections. This structure is intended to systematically address the who, what, and why of stigma, capturing components within each aspect of the integrated social-affective model framework (Figure 1).
Results
Overview of results
N = 1985 records were identified through database searches, with 765 duplicates removed (Figure 2). After completing Title/Abstract screening and Full-Text screening, 44 articles were included in the review. The majority of articles removed during Full-Text screening were due to not measuring stigma (n = 16).
Study characteristics
The 44 studies reviewed span a wide range of countries (N = 21), reflecting diverse healthcare systems and cultural contexts (Table 1). The United States accounted for the largest percentage of the studies (20%, n = 9). Sample sizes varied considerably, ranging from small cohorts of fewer than 30 participants to larger studies exceeding 1,000 participants. The mean sample size across studies was 320 (SD = 470).

Table 1. Summary of studies investigating stigma in healthcare providers.
A wide variety of measurements were used to assess stigma among healthcare providers, with a mix of validated questionnaires, vignette and scenario-based assessments, semantic differential scales, specialized tools (e.g., Stigma Scale Toward Schizophrenia for Community Pharmacists [SSCP]), and other methods such as author-designed questionnaires. In total, 41 different measures were used, with 26 of those used only one time. The most frequently used measures were Social Distance Scales (n = 8, 18%), Attribution Questionnaires (AQ; n = 6, 13%), and Semantic Differential Scales (n = 3, 7%) (Table 1). The social distance scale measures the level of social distance individuals wish to maintain from a certain population, assessing willingness to engage in various social situations with these individuals (e.g., “How willing would you be to work closely with a person who has schizophrenia?” Not willing at all – Very willing). The AQ evaluates beliefs and attitudes that people have towards mental illness by assessing emotional reactions and discriminatory responses to a provided vignette (e.g., “How dangerous would you feel Harry is?” Not at all – Very much). The semantic differential scales assess attitudes towards individuals with mental illness by measuring participants’ perceptions along a range of bipolar adjective pairs (e.g., dangerous-safe and unpredictable-predictable). The majority of the studies included a patient vignette in their design (n = 24, 55%). However, there was considerable variation in content of the vignettes. Twenty-nine percent provided no description of the vignette used, 16% described the individual as functionally well with well controlled symptoms, 25% specify no substance use, 38% use a male vignette, and approximately 20% contain content that may indicate risk of harm. The majority of studies focused specifically on schizophrenia (n = 31, 70%) or psychosis (n = 7, 16%). One study focused on both schizophrenia and psychosis, while the remaining studies examined related conditions such as general psychotic disorders (n = 2), long-standing hallucinations and delusions (n = 1), or multiple illness stages including psychotic-like-experiences and attenuated psychosis (n = 2; Table 1). Additionally, recovery-related beliefs are frequently assessed in the literature as an indicator of stigma, with assumptions that pessimism about recovery reflects therapeutic nihilism or discriminatory attitudes. Several of the studies reviewed here take this approach. However, studies varied in how recovery-related beliefs were assessed, and many did not define “recovery” within their measures. As such, provider responses may reflect different understandings of recovery, ranging from full symptom remission to functional improvement or quality of life, limiting the interpretability of these items as straightforward indicators of stigma. This issue is further discussed in the Stigma or Realism section of the Discussion. Lastly, a small number of studies assessed perceived public stigma, that is, how providers believe the general public views individuals with SSDs, rather than their own attitudes. While this may help reduce social desirability bias, it does not directly measure providers’ personal beliefs or implicit biases, which limits interpretability. Findings from these studies are noted as such in the text (e.g., as measuring public stigma) to distinguish them from studies assessing personal attitudes.
Healthcare providers included
The review encompassed a wide spectrum of healthcare providers, categorized into six main groups: (1) medical students and trainees, including undergraduate and graduate medical students, (2) nurses, including mental health nurses, primary care nurses, and nursing students, (3) physicians, including general practitioners, psychiatrists, and specialists from various fields, (4) psychologists and mental health professionals, including clinical psychologists and other mental health workers, (5) community health workers, including village health workers and community pharmacists, (6) mixed groups, including studies that reported results combining provider types.
These categories were selected to support coherent synthesis and reflect meaningful distinctions in training, credentialing, and general proximity to mental health care. (1) Medical students and trainees were grouped separately to capture early-career attitudes and the influence of training stage. (2) Nurses were grouped together due to shared credentialing pathways and overlapping caregiving responsibilities across care settings. (3) Physicians were grouped based on common medical training, licensure routes, and clinical authority in diagnosis and treatment. (4) Psychologists and other mental health professionals were grouped due to their shared focus on behavioral and emotional functioning and their central role in mental health care delivery. (5) Community health workers, such as village health workers and pharmacists, were combined given their common roles in frontline service provision and community-based care. (6) Mixed groups were used when studies reported aggregated results across provider types that could not be meaningfully separated. We acknowledge that within-group variability exists, particularly among nurses and physicians, whose roles and degree of contact with individuals with psychotic disorders can vary substantially, but grouping was retained to ensure consistency and feasibility in synthesis.
Relatedly, we note that while psychologists are frequently included in stigma research, many studies with psychologist samples focus broadly on “mental illness” or “serious mental illness” rather than schizophrenia spectrum disorders specifically. Because the current review focused only on studies that directly assessed stigma toward SSDs, studies that did not disaggregate findings by diagnosis were excluded. As a result, the body of evidence specific to psychologists’ attitudes toward SSDs is more limited than for other provider groups.
Stigma by provider type
Medical students
Several studies demonstrated unfavorable attitudes toward SSDs within medical students; large proportions of undergraduate medical students believed individuals with schizophrenia could not marry, live at home, or work (86) and others reported high levels of fear and anger (82) and moderate levels of fear and pity (76). Psychotic disorders also received the second most negative attitudinal ratings (following conduct disorder) when compared to three other disorders, were met with authoritarian treatment approaches, and were attributed to social problems or malingering by a minority of students (54). In another sample, individuals with psychosis were rated more favorably than those with intravenous drug use or unexplained abdominal complaints but less favorably than those with pneumonia or depression (69). Beyond attitudinal stigma, medical students endorsed significantly more stereotyped beliefs, negative attitudes, and microaggressive behaviors than psychology students, licensed psychologists, and even the general public, with very large effect sizes observed across all three measures (59).
Notably, medical students consistently reported the highest desired social distance compared to psychology trainees, licensed psychologists, and community members, with very large effects (59). They also showed higher fear and anger compared to psychology trainees and psychiatrists (76) and expressed more pessimism about recovery outcomes (54, 72). Of note, medical students who hoped to become psychiatrists had significantly more positive attitudes than those with other career goals (67).
Overall, these findings align with the intergroup emotion theory and contact hypothesis domains of the integrated model (Figure 1), highlighting the role of unfamiliarity and limited patient exposure in shaping emotional and behavioral stigma.
Nurses
Nurses’ attitudes toward schizophrenia reveal significant stigma and negative perceptions, with some variation across contexts and nurse types. Compared to non-psychiatric conditions, schizophrenia was viewed as more dangerous, unpredictable, and unusual, with high levels of pessimism about recovery (46, 56). In one study, 47% of nurses in one sample believed that individuals with schizophrenia would never recover—a pessimism in the sample exceeded only by that for dementia (46). However, it is unclear whether participants interpreted “recovery” as full remission, functional improvement, or something else. Somatic nurses (i.e., physical care nurses in a somatic clinic), compared to psychiatric nurses, rated schizophrenia as more dangerous, unpredictable, and harder to talk to, with large (dangerousness and unpredictability) to small effects (hard to talk to) (46). Nurses also demonstrated lower knowledge and favorability ratings towards psychosis compared to other disorders (44). In another sample, higher overall stigma scores were associated with being nurse (81).
Nurses’ attitudes also vary between affective and social dimensions: psychiatric nurses demonstrated relatively high affective acceptance (i.e., emotional warmth, positive feelings, and affective attitude) of patients with schizophrenia but significantly lower social acceptance (i.e., behavioral intentions and desire to keep physical distance), indicating discomfort in real-life scenarios (64). Attitudes further influenced clinical care, with mental health nurses expressing reluctance to involve family in treatment planning for patients with schizophrenia, which negatively impacted the quality of family-centered care (63).
Nursing students that demonstrated more pessimistic views about prognosis had higher rates of prejudice toward individuals with schizophrenia (78), and nurses who rated the likelihood of discrimination from others against schizophrenia as high also expected more negative long-term outcomes (i.e., poor recovery, relapse, chronic impairment) (48). Nursing students in one sample demonstrated high scores in pity and help but low scores on responsibility (i.e., “perception that individuals with MHC can control their symptoms and are accountable for their condition”) and segregation (58).
Broadly, these attitudes reflect attributional and emotional pathways described in Figure 1, including perceived dangerousness, fear-based reactions, and pessimism shaped by limited recovery-oriented training.
Physicians
Physicians’ attitudes toward schizophrenia varied across disciplines but reveal elements of stigma, pessimism about recovery, and social distance. Among psychiatrists, large proportions endorsed stigmatizing beliefs. In one study, half of the psychiatrists scored in the highest stigma category (53). Another study reported that schizophrenia was associated with moderate stigma among both psychiatrists and non-psychiatrist physicians, with pediatricians showing the highest levels of social distance (84). Psychiatrists and psychiatry residents also reported a large effect of stronger desires for social distance from individuals with schizophrenia compared to a non-psychiatric condition (diabetes), despite the psychotic symptoms being described as well-controlled (52). However, in another study, being a psychiatrist was associated with better attitudes towards individuals with psychotic disorders and lower stigma scores were associated with being a psychiatry resident, compared to medical officers, nurses, medical social workers, case managers, and occupational therapists (81).
Negative attitudes toward schizophrenia were also evident among general practitioners (GPs), who perceived patients with chronic psychosis as burdensome, difficult to communicate with, and difficult to like, and held pessimistic views about prognosis and family burden (47). Likewise, compared to a vignette without schizophrenia, primary care physicians were less willing to manage the schizophrenia patient, more likely to assume they were violent, and more inclined to refer them to specialists, despite the vignette describing symptoms as being well controlled (70). However, one study found an association between greater empathy and being a general medical doctor (81).
Among medical residents, fewer than half endorsed recovery as a possibility, and many expressed attitudes of social distance, beliefs in dangerousness, and skepticism about treatment efficacy (55). Furthermore, schizophrenia elicited the second most negative attitude, following a patient with multiple inpatient admissions, among various patient vignettes (62). Emergency medicine residents demonstrated a medium effect of the most negative attitudes, while residents in their transition year were more positive, though not significantly so.
Physicians’ skepticism regarding schizophrenia recovery was a theme across studies. Fewer than one-third of general practitioners and specialists believed full recovery was possible, while a majority believed psychotropic medications were a lifelong requirement and that stopping medication would lead to dangerousness (of note, the study did not indicate what was meant by “recovery,” which poses limits to the interpretability; 72). Psychiatrists and GPs alike held more negative long-term prognostic (e.g., substance misuse, death by suicide) views for schizophrenia than for depression, with psychiatrists showing the most pessimism (65) Additional stigma was evident in general hospital settings, where patients with schizophrenia were viewed as difficult to engage, untrustworthy, and comparable to criminals due to perceived unpredictability and ulterior motives (75).
Psychologists and other MHPs (non-psychiatrist)
Clinical psychologists demonstrated mixed attitudes across studies. In one sample, clinical psychologists made ratings on semantic differential scales of effective–ineffective, understandable–incomprehensible, safe–dangerous, worthy–unworthy, desirable to be with– undesirable to be with, and similar to me–dissimilar to me; individuals with schizophrenia were rated as the least effective, least understandable, and least similar to themselves compared to individuals with depression, borderline features, or the general public (87); effects were large in magnitude. Schizophrenia was rated as the second-to-least safe and second-to-least desirable to be with (after borderline features). Notably, 69% of psychologists viewed individuals with schizophrenia as highly dissimilar to themselves, indicating persistent perceptions of otherness.
However, psychologists displayed more favorable attitudes overall compared to other healthcare providers. Psychology students and licensed psychologists endorsed significantly lower levels of social distance and stigma than medical students and community members, with very large effects (59), and lower stereotyping and discrimination compared to nurses and psychiatrists, with medium effects (19). They also demonstrated greater optimism regarding recovery outcomes compared to psychiatrists (65), although they rated likelihood of discrimination from the public as high.
It is important to note that psychologists and other mental health providers are often analyzed in combined samples, which limits the availability of findings specific to this provider group. Furthermore, many studies with psychologist participant pools focus broadly on mental illness rather than psychosis or schizophrenia. Combined sample findings and comparisons with other provider types are discussed in greater detail in the “Mixed Groups” section.
Community health workers
Community health workers had varying degrees of stigma, with some notable differences based on provider type and training background. Non-licensed rural community health workers rated psychosis as highly stigmatized, expressed a stronger desire for social distance from individuals with psychosis compared to those with depression, and associated it with dangerousness, personal weakness, and erratic behavior (50, 68).
Pharmacists and pharmacy students demonstrated similarly complex attitudes. Pharmacists linked schizophrenia with poor prognosis, violence, social and vocational difficulties, and high likelihood of discrimination from others (77). Pharmacy students expressed especially strong stigmatizing attitudes, with high unwillingness for personal interaction and perceptions of dangerousness and unpredictability (83). High social distance was strongly associated with beliefs that people with schizophrenia are difficult to talk to or are to blame for their condition. Conversely, pharmacists in one study demonstrated relatively positive attitudes toward individuals with schizophrenia, with attitudes scoring lower than the midpoint on stigma measures, suggesting less pronounced stigma among this group (57).
Mixed groups
Collapsing providers
In mixed samples of healthcare providers, stigma toward SSDs varied notably by illness stage, experience, and attitudinal factors.
Regarding illness stage, stigma beliefs and discriminatory behaviors increased progressively from psychotic-like experiences (PLEs) and at-risk mental states (ARMS), and culminated in the highest levels with schizophrenia, with large effects sizes between PLEs and schizophrenia (45). Additionally, while healthcare providers in another sample generally stigmatized schizophrenia and PLEs similarly to the public, they exhibited a large effect of lower stigma toward attenuated psychosis syndrome (71).
Two studies with combined provider groups associated SSDs with higher perceived dangerousness and preference for social distance (73); in one case these beliefs surfaced with a large effect despite the vignette describing the individual as being polite and having no history of substance use (23). However, providers in one sample demonstrated notably greater acceptance, lower social distance, and higher optimism about treatability than the public or patients’ relatives (60).
Certain attitudes correlated with treatment expectations and professional behavior. Agreement with stigmatizing attitudes correlated negatively with expectations of treatment adherence, influencing clinical decisions such as referrals and prescriptions, although no significant differences were observed between professional disciplines regarding these expectations (51). Furthermore, across provider groups, perceived discrimination from others against individuals with schizophrenia was consistently high and strongly correlated with negative outcome expectations, suggesting that beliefs about societal stigma influenced providers’ recovery-related attitudes (48, 65).
Comparing providers
Finally, we evaluated stigma in studies that directly compared different healthcare providers. These studies are noteworthy in that they present an opportunity to compare provider views from samples assessed with similar measures. Medical students displayed the highest levels of stigma for negative attitudes and stereotypes with very large effects and the highest scores for social distance compared to psychology trainees, licensed psychologists, and community members (59), although they showed significantly lower stigmatizing attitudes in help, pity, and avoidance compared to non-psychiatrist doctors (76). Similarly, in another sample, medical students demonstrated stigma levels comparable to those of physicians and non-medical workers, with no apparent benefit from psychiatric education or clinical training (67). Psychiatrists displayed lower levels of stigmatizing attitudes than non-psychiatrist doctors and medical students with very large effects (76), lower discrimination and underestimation of patients’ abilities (67), and the lowest levels of fear, anger, and danger (76). However, findings on social distance varied: while one study reported lower social distance preferences among psychiatrists compared to non-psychiatrist doctors (76), another found no significant differences (84). Clinical psychology trainees and licensed psychologists demonstrated significantly lower social distance than medical students and community members (59) and were more optimistic about outcomes compared to psychiatrists and GPs (65). GPs were more likely to view patients with chronic psychosis as burdensome, difficult to communicate with, and prone to creating crises compared to psychologists and psychiatrists (47). Across all groups, there was agreement that individuals with schizophrenia were more likely to face discrimination than those with depression (65).
Summary
The results reveal that social distance is the most pronounced feature of stigma among healthcare providers, with medical students displaying the highest levels of unwillingness to engage with individuals with schizophrenia, while psychologists and psychiatrists demonstrate significantly lower levels. Nurses generally associate schizophrenia with higher levels of dangerousness and unpredictability compared to psychiatrists, who show lower levels, and psychologists endorse the lowest level of these beliefs. In terms of recovery beliefs, medical students and general practitioners are more pessimistic, while psychiatrists and psychologists show more optimism. Emotional reactions like fear and anger are highest in medical students, while psychologists and psychiatrists display more empathy and less fear. Nurses, especially psychiatric nurses, express more pity, and their social acceptance is lower. Lastly, perceptions of discrimination from others are strongest in medical students and nurses, and lower in psychologists and psychiatrists. These patterns illustrate how provider role, training, and exposure influence stigma through mechanisms captured across attributional, emotional, and experiential domains of the integrated social-affective model (Figure 1).
Moderators of stigma
Professional and contextual moderators
Etiological beliefs
Three studies reported on the effects of etiological beliefs. Two studies found associations between biogenetic beliefs and increased stigma related to pessimism about recovery and social distance with a medium effect (68, 72). However, the opposite was also observed: biological etiological beliefs predicted less stigmatization (19). Additionally in that sample, they found that continuum beliefs of schizophrenia were negatively associated with stereotypes and social distance, while categorical beliefs had a positive association.
Work setting
Providers working in independent practice reported more stereotypes beliefs and more desire for social distance compared to those working in hospital settings, with a medium effect for stereotyping and a weak effect for social distancing (19). Additionally, they found that belonging to a multidisciplinary team was associated with a lower prejudice, though the effect was weak. Lastly, they found that working in inpatient services did not predict more stigma than working in other settings. However, another sample found that providers working on inpatient psychotic disorders units perceived patients as being “too ill” due to violence, aggression, disorganization, and delusional conviction, as well as stays being too short, as barriers for effective psychosocial treatment interventions (49). Two studies found no effect of work settings on stigmatizing beliefs (48, 51).
Years in profession/experience
In one study, providers with more work experience demonstrated fewer stigmatizing attitudes (59), and less stigma regarding dangerousness, unpredictability, and blame, with medium to small effects, respectively. Another study found an association between longer work experience and better overall attitudes towards individuals with schizophrenia but higher stigma scores (81). Providers with higher education exhibited decreased social distance scores in one sample (small effect size; 60) and were associated with better attitudes and lower stigma scores in another sample (81) but had more negative attributions about patients’ responsibility for psychosis compared to providers with less education in another sample (80). Longer time since graduation was positively associated with higher stigma levels (53), and greater years in practice predicted higher stereotypes and social distance, though with weak effects (19). Similarly, doctors in their third year of residency reported significantly higher unfavorable attitudes compared to those in earlier years of residency (55), and fourth year medical students showed greater underestimation of patients’ abilities compared to third years (67). Caldwell and Jorm (48) found no significant effects of experience on discriminatory beliefs.
Professional orientation
Recovery-oriented practices and cognitive behavioral therapy theoretical orientations were associated with lower stereotypes and lower prejudices, with medium and weak effects, and recovery-oriented practice was associated with lower desire for social distance, with medium effects (19).
Contact
Providers with greater professional contact with individuals with SSDs show lower stigmatizing attitudes, higher expectations of patients with schizophrenia (74), and less negative attitudes, though with weak relationships and small effects (46). Similarly, another study found that patient contact predicted more positive implicit attitudes (52). However, three other studies reported no significant association (19, 58, 65), and one reported that staff who primarily treated individuals with psychosis held more negative attitudes compared to those treating other diagnostic groups (61).
Personal familiarity (friends/family/self)
Several studies reported that having friends, family members, or personal experience with mental illness was associated with reduced stigma. Personal familiarity significantly lowered stigmatizing attitudes (76, 81), reduced social distance (81, 83), led to fewer stereotypes (small effect) (19), increased positive attitudes (small effect) (62), and significantly increased regard for patients with schizophrenia (medium effect) (69). Providers’ comfort with seeking mental healthcare for themselves was weakly associated with reduced stigmatizing beliefs and more optimistic treatment expectations (51). However, three studies found no association (60, 67, 68). Additionally, one study reported that while higher personal contact with mental illness had a moderately large negative association with stigmatizing attitudes and beliefs, the direct relationship between personal exposure and provider expectations was not significant (74).
Demographic moderators
Age
In several studies, older providers exhibited higher stigma levels. Specifically, older age was associated with increased pity (76), less socially accepting attitudes (64), and greater stereotyping, although this was a small effect (19). In contrast, other studies found reduced stigma among older participants, with less negative attitudes about dangerousness and unpredictability (46), and negative correlations with social distance scores (55), though the effects were small in both. However, some studies found no effect of age (60, 68, 81) or mixed results, with one study finding no effect for prejudice and social distancing in spite of the greater stereotyping (19). Younger general practitioners, on the other hand, rated negative outcomes (e.g., substance misuse, death by suicide) for schizophrenia more highly than older counterparts in one study (65).
Sex
Multiple studies identified higher levels of stigma among male providers compared to female providers, including more negative attitudes (59), more stigmatizing beliefs (55, 66), and pessimism for recovery, with small to medium effects (46). One study found higher stigma scores among male providers, but the results were not statistically significant (50). Results for female providers were mixed; with one study finding that female medical students had significantly higher levels of regard for patients with schizophrenia, though the effect was small (69), less underestimation of patients’ abilities (67), greater empathy (81), and more positive attitudes toward schizophrenia than male providers, though not statistically significant (75). Conversely, some studies reported that female providers rated negative outcomes as more likely (65) had higher levels of skepticism regarding treatment (55), and had higher emotional responses for fear, anger and pity (58). Numerous studies found no effects of sex across stigma components: socially accepting attitudes (64, 81), social distance scores (68, 81), and discriminatory beliefs (48). Additionally, two studies found higher stigma amongst men for other diagnoses as well, including PTSD, eating disorders, and depression (46, 66). This is in line with previous literature finding higher stigma in men for mental illness overall (88, 89).
Discussion
This systematic review synthesized findings from 44 studies examining stigma toward SSDs among healthcare providers. Overall, findings indicate that stigma towards individuals with SSDs is more pronounced among general practitioners, community health workers, and medical students—particularly those with limited psychiatric training or exposure. In contrast, psychiatrists, psychologists, and providers with specialized training in mental health reported lower levels of stigma. Familiarity with SSDs, through training or patient contact, appears more influential than professional role alone. See Table 2 for a condensed summary of results.
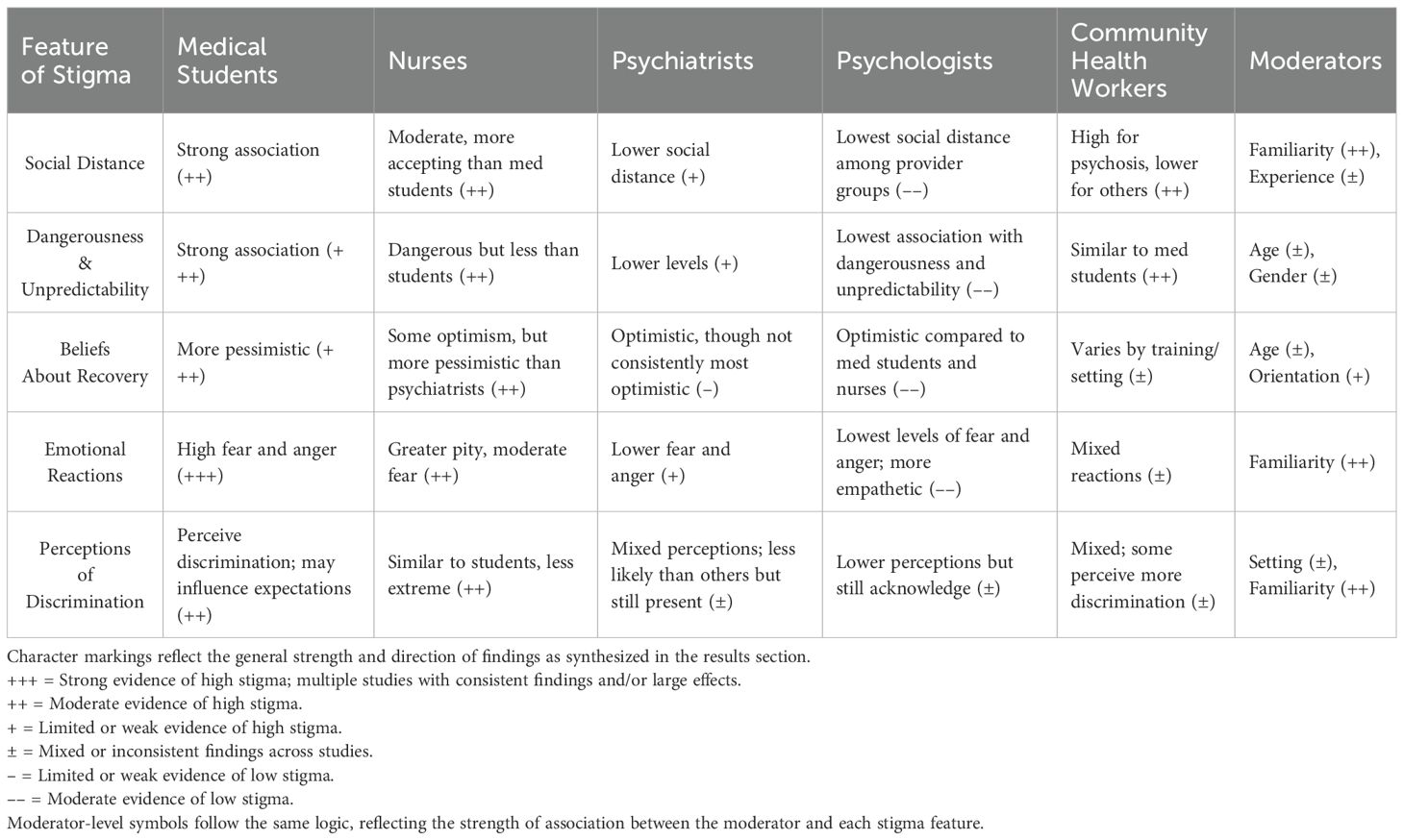
Table 2. Summary of results.
The most consistent moderators linked to lower stigma were increased personal and professional contact, along with recovery-oriented frameworks. In contrast, findings for demographic (e.g., age, sex) and professional factors (e.g., years in profession, workplace setting) were mixed across studies. The variability may reflect contextual factors or interactions between moderators, but is also likely driven by methodological differences. Studies varied widely in how stigma was assessed (e.g., attitudes, behaviors, emotions) and in the tools used, including author-developed scales with unclear psychometric properties. This variability makes it difficult to make meaningful, confident comparisons across studies, even when targeting similar constructs or provider types. Vignette content also varied: over a fourth of studies using vignettes did not provide the stimuli, and those that did varied in content (e.g., some having well-controlled symptoms, others including signs of violence or substance use) which was not experimentally manipulated. These methodological inconsistencies highlight the need for more transparent and standardized approaches in future research.
Additionally, variability in moderator findings may reflect intersectionality between factors such as age, sex, workplace setting, and personal experience with mental illness. These factors may influence stigma in complex or even opposing ways; for example, older individuals may hold stigmatizing views due generational norms, but this may be offset by personal exposure to mental illness. Cultural context is another likely contributor to variability, with studies spanning 19 countries. Cultural beliefs shape how mental illness is understood, whether through a moral, supernatural, or biomedical lens (90, 91); these frameworks influence both the expression and measurement of stigma among healthcare providers.
Overall, the findings of this review align with prior research on stigma within healthcare settings, particularly in identifying misconceptions about dangerousness and poor recovery outcomes as pervasive among providers (2, 10, 21). However, this review extends the literature by systematically comparing stigma across multiple provider groups and identifying potential key moderators of stigma, such as sex and personal experience with mental illness.
Findings in theoretical context
These findings align with the contact hypothesis (22), particularly within the microsystem of provider-patient interactions (32), showing that mental health providers and providers with personal experience tend to exhibit lower stigma. Critically, this suggests that not all contact is equally beneficial—brief, task-focused interactions, more common among general healthcare providers and community health workers, may lack the relational depth needed to challenge stereotypes. In contrast, structured, supervised engagement in mental health settings likely facilitates more meaningful, stigma-reducing contact. Existing contact-based stigma interventions (92–94) may benefit from inclusion of therapeutic practices such as consistent debriefing and supervisory reflection. This may foster more constructive, compassionate, stigma-reducing contact—standard in psychology settings— and may help generalist providers process biases, foster more compassionate care, and reduce stigma.
The results also highlight the relevance of intergroup emotion theory (28) at the microsystem level, particularly in how providers view individuals with SSDs as an outgroup. For example, in one of the included studies, 69% of clinical psychologists (typically providers with the lowest levels of stigma) rated individuals with schizophrenia as highly dissimilar from themselves (87). Such perceived dissimilarity can elicit fear and discomfort, especially among trainees or provider with limited exposure, and these affective reactions often drive avoidance behaviors (95). This suggests a need for interventions that directly target emotional regulation, such as empathy-building exercises or experiential learning exercises.
Causal attributions also emerged as an important mechanism, consistent with attribution theory (25, 80). Although biogenetic explanations may reduce blame, they may simultaneously increase pessimism about recovery and reinforce perceptions of dangerousness, suggesting a dual-edged nature of how such attributions shape emotional and behavioral responses. Such effects have been documented as unintended negative consequences of anti-stigma campaigns that emphasize biogenetic frameworks (96–99). To mitigate this, interventions should promote recovery-oriented narratives alongside psychoeducation that presents a biopsychosocial framework, rather than a purely biogenetic one. These findings collectively support the integrated social-affective model (Figure 1), illustrating how stigma emerges from intersecting psychological and institutional forces.
Implications for practice and intervention
Stigma across provider types was linked to gaps in knowledge and experience with SSDs. This highlights the need for integrating comprehensive mental health training into non-specialist fields such as general medicine, nursing and pharmacy. Early, sustained clinical exposure to SSDs may challenge stereotypes and foster empathy and compassion (82, 100). For practicing providers, continuing education that combines evidence-based content with meaningful patient interactions could be particularly effective (101), especially given recent evidence that private practice providers demonstrate higher levels of stigma (19).
While many interventions target individual providers, systemic change is critical to address structural inequities that perpetuate stigma. This includes policy reforms mandating comprehensive mental health training across professions, and restructuring healthcare systems to improve access and interdisciplinary collaboration. One such model is the United States Veterans Health Administration’s PCMHI program, where integrating behavioral health into primary care supports team-based care and bridges knowledge gaps between primary and general care providers with MHPs (102–104). Workplace policies that reduce burnout and promote inclusivity also create environments conducive to stigma reduction. Drawing on the “Seed and Soil” framework (105) interventions are more effective when implemented in supportive environments with the psychological affordances for change. Reducing systemic barriers such as high workloads, inadequate funding, and limited training opportunities is thus crucial. Notably, providers in multidisciplinary settings report lower stigma (19), suggesting that fostering collaboration and shared responsibility, similar to that of the VHA PCMHI, may simultaneously reduce burnout and improve knowledge and contact (106, 107).
Stigma or realism?
Identifying and labeling providers’ perceptions as stigma is not always straightforward. In clinical practice, healthcare providers may form negative appraisals of patients with SSDs—that appear stigmatizing—based on realistic assessments of the research literature or direct clinical experience, such working with patients with aggression or impaired social functioning, which may be more pronounced in certain contexts (e.g., on psychiatric in-patient units). These appraisals may not stem from bias, but rather from the complex, challenging experiences providers face in managing signs, symptoms, and behaviors associated with a serious and complicated mental disorder. Similarly, they may reflect providers’ awareness of empirical evidence on SSDs; for example, higher rates of socio-occupational functioning are evident throughout the literature (108, 109). If, as is done in a number of the studies included here, a provider endorses the belief that individuals with an SSD may struggle in social relationships, this may reflect an evidence-based appraisal of outcome. Related concerns, such as risk of harm, poor prognostics, or likelihood of recovery, can also emerge from research on SSDs (110, 111). These negative prognostic views may not be pure reflections of stigma, but data-based views shaped by the complex etiology and associated outcomes experienced by individuals with an SSD.
Still, such negative appraisals—even those that could be said to be evidence-based—must be critically examined in terms of their clinical application and impact on individuals with SSDs. This is particularly important when such appraisals influence discriminatory and incendiary behaviors by providers. Prior research has demonstrated that provider behaviors influence patient interactions and outcomes, both positively and negatively (112–114). Staff trained in evidence-based interventions, such as social learning principles, show marked improvements in therapeutic interactions and fewer negative behaviors towards patients, which in turn improved patient compliance and social functioning (79, 115). Likewise, expressed emotion (EE) literature shows that staff who express warmth and support, while avoiding criticism or hostility, promote positive relationships and better outcomes for patients (116). Positive staff-patient relationships, where staff attribute patient difficulties to external factors internal causes, further contribute to better patient outcomes (117). Furthermore, when staff adopt a person-centered approach, emphasizing collaboration and empathy, patients demonstrate better engagement and recovery outcomes (118). These findings highlight how provider attitudes and perceptions shape behavior and how behavior, in turn, shapes patient outcomes.
Even evidence-based appraisals can inadvertently reinforce stigma when applied rigidly, especially when they stem from limited exposure to SSDs or reflect a lack of recovery-oriented training. For example, this review identified three instances in which vignettes described individuals with well-controlled symptoms, yet providers consistently expressed a desire for social distance and concerns about potential dangerousness (23, 52, 70). One likely contributor is the clinician’s illusion—provider’s tendency to overestimate overall illness severity due to primarily seeing the most severe, treatment seeking cases (119). In essence, this leads to a skewed perception of SSDs and recovery potential as a whole. Exacerbating this, providers may fall prey to the ecological fallacy: the mistaken assumption that group-level trends necessarily apply to individuals, resulting in clinical judgements that conflate statistical generalities with individual prognosis (120). Stigma-based or not, negative clinician perceptions require further empirical and applied attention.
Limitations
This review has several important limitations. First, most included studies were conducted in high-income Western countries, limiting the generalizability to non-Western and low- and middle-income countries. Sociocultural differences in stigma and healthcare systems in these underrepresented regions may yield different patterns of provider attitudes. Second, although we did not formally assess risk of bias for each included study, we note substantial methodological heterogeneity across studies, particularly in the use of measurement tools, vignette descriptions, and sample sizes. The heterogeneity in study designs may introduce inconsistencies in how stigma is defined and interpreted across studies. Most studies relied on self-report measures, which are subject to social desirability bias. This likely led to underreporting of stigmatizing attitudes, particularly given the target population is healthcare providers. While some studies attempted to reduce this by measuring perceived bias as a proxy for personal bias, such perceptions may represent realistic appraisals of public attitudes (37) rather than implicit or internalized beliefs. Third, because we only included published studies, there is a risk of publication bias. Moreover, the studies span several decades, with some published as early as the 1980s. While this allowed for a more comprehensive synthesis, it also introduces variability, as societal attitudes toward mental illness and clinical practices have likely changed over time. Findings should be interpreted within their historical context. Finally, although this review followed PRISMA guidelines, the review protocol was not pre-registered.
Future directions
Several critical gaps remain. The current literature is dominated by cross-sectional study designs; longitudinal studies are needed to assess how provider attitudes evolve over time, particularly in response to training, increased patient contact, or meaningful systemic changes (e.g., updating practice guidelines to emphasize recovery-oriented care, reducing provider caseloads). While individual-level factors like training and exposure have been well-documented, future research should examine how interdisciplinary collaboration and structural reforms contribute to stigma reduction. Mixed method approaches that integrate quantitative and qualitative data can illuminate how providers experiences, beliefs, and institutional contexts shape stigmatizing behaviors.
Additionally, future research should also explore the impact of self-stigma interventions on providers’ attitudes, as this may have the potential to influence both patient outcomes and provider perceptions. At least six established interventions target self-stigma (121), raising the interesting question: if providers work with patients actively working to reduce self-stigma and discussing their experienced stigma, might this increase providers’ awareness of their own biases? Exploring this dyadic dynamic could offer valuable insight into how patient self-empowerment and disclosure may influence provider attitudes, contributing to a reciprocal process of stigma reduction, an unexplored interpersonal feedback loop.
Critically, more work is needed on potential mechanisms of provider stigma. These findings and the broader literature underscore that stigma is multifaceted and context-dependent. Moreover, emerging research suggests that prejudice-reduction strategies in general rarely produce meaningful and lasting effects (122). This raises the need to re-evaluate our targets: focusing on the assessment and change of provider beliefs, explicit or implicit, may be only marginally impactful for real-world change in patient care (122, 123). It is established, here and throughout the literature base, that these beliefs exist across time and among healthcare providers; beliefs are difficult to modify—discriminatory behaviors, instead, may be a more measurable and modifiable target for provider change. Using social marketing principles (122), these interventions can be designed to align with providers’ professional values, emphasizing practical benefits such as improved patient outcomes, enhanced provider efficacy, and fewer workplace barriers to implementing inclusive care.
Addressing provider-based stigma is vital for improving the outcomes of the individuals we serve. Targeted, multi-level interventions hold the potential to transform individual provider attitudes and the broader healthcare systems in which they operate. Reducing stigma among providers is essential for fostering recovery-oriented care and promoting equity for one of the most marginalized patient populations.
Data availability statement
The original contributions presented in the study are included in the article. Further inquiries can be directed to the corresponding author.
Author contributions
EK: Formal analysis, Writing – original draft, Project administration, Conceptualization, Data curation, Methodology, Investigation, Writing – review & editing. DD-F: Conceptualization, Project administration, Methodology, Supervision, Writing – review & editing.
Funding
The author(s) declare that no financial support was received for the research and/or publication of this article.
Acknowledgments
Thank you to Drs. Steven Silverstein and Christie Petrenko for serving as committee members on a prior draft of this manuscript submitted as a qualifying exam. A preprint of the article was posted on May 16, 2025, and can be found here (https://doi.org/10.31219/osf.io/qwvx2_v1).
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Generative AI statement
The author(s) declare that no Generative AI was used in the creation of this manuscript.
Any alternative text (alt text) provided alongside figures in this article has been generated by Frontiers with the support of artificial intelligence and reasonable efforts have been made to ensure accuracy, including review by the authors wherever possible. If you identify any issues, please contact us.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. de Jacq K, Norful AA, and Larson E. The variability of nursing attitudes toward mental illness: an integrative review. Arch Psychiatr Nurs. (2016) 30:788–96. doi: 10.1016/j.apnu.2016.07.004
2. Valery K-M and Prouteau A. Schizophrenia stigma in mental health professionals and associated factors: A systematic review. Psychiatry Res. (2020) 290:113068. doi: 10.1016/j.psychres.2020.113068
3. Wahl O and Aroesty-Cohen E. Attitudes of mental health professionals about mental illness: A review of the recent literature. J Community Psychol. (2010) 38:49–62. doi: 10.1002/jcop.20351
4. World Health Organization. Schizophrenia. (2022). Available at: https://www.who.int/news-room/fact-sheets/detail/schizophrenia (Accessed August 13, 2025).
5. O’Brien LT, Kulibert D, and Waldon-Lee T. Stigma and disadvantage. In: Oxford Research Encyclopedia of Psychology. Oxford, England: Oxford University Press. (2023). Available online at: https://oxfordre.com/psychology/display/10.1093/acrefore/9780190236557.001.0001/acrefore-9780190236557-e-442?d=%2F10.1093%2Facrefore%2F9780190236557.001.0001%2Facrefore-9780190236557-e-442&p=emailAktC6FaTKYi0Y (Accessed May 5, 2025).
6. Gerlinger G, Hauser M, De Hert M, Lacluyse K, Wampers M, and Correll CU. Personal stigma in schizophrenia spectrum disorders: A systematic review of prevalence rates, correlates, impact and interventions. World Psychiatry. (2013) 12:155–64. doi: 10.1002/wps.20040
7. Lysaker PH, Tsai J, Yanos P, and Roe D. Associations of multiple domains of self-esteem with four dimensions of stigma in schizophrenia. Schizophr Res. (2008) 98:194–200. doi: 10.1016/j.schres.2007.09.035
8. Lysaker PH, Vohs JL, and Tsai J. Negative symptoms and concordant impairments in attention in schizophrenia: Associations with social functioning, hope, self-esteem and internalized stigma. Schizophr Res. (2009) 110:165–72. doi: 10.1016/j.schres.2009.01.015
9. Wood L and Irons C. Experienced stigma and its impacts in psychosis: The role of social rank and external shame. Psychol Psychother: Theory Res Pract. (2017) 90:419–31. doi: 10.1111/papt.12127
10. Schulze B and Angermeyer MC. Subjective experiences of stigma. A focus group study of schizophrenic patients, their relatives and mental health professionals. Soc Sci Med. (2003) 56:299–312. doi: 10.1016/S0277-9536(02)00028-X
11. Yanos PT, Roe D, and Lysaker PH. The impact of illness identity on recovery from severe mental illness. Am J Psychiatr Rehabil. (2010) 13:73–93. doi: 10.1080/15487761003756860
12. Corrigan PW and Penn DL. Lessons from social psychology on discrediting psychiatric stigma. Am Psychol. (1999) 54:765–76. doi: 10.1037/0003-066X.54.9.765
13. Fiske ST. Stereotyping, prejudice, and discrimination. In: The handbook of social psychology, 4th, vol. 1-2. New York: McGraw-Hill. (1998). p. 357–411.
14. Goffman E. Stigma: Notes on the Management of Spoiled Identity. New York: Simon and Schuster. (2009).
15. Daugherty B, Warburton K, and Stahl SM. A social history of serious mental illness. CNS Spectrums. (2020) 25:584–92. doi: 10.1017/S1092852920001364
17. Maisel AQ. Bedlam 1946: Most US mental hospitals are a shame and a disgrace. Life Magazine. (1946) 20:102–18.
18. Corrigan PW and Nieweglowski K. How does familiarity impact the stigma of mental illness? Clin Psychol Rev. (2019) 70:40–50. doi: 10.1016/j.cpr.2019.02.001
19. Valery K-M, Violeau L, Fournier T, Yvon F, Arfeuillere S, Bonilla-Guerrero J, et al. Part of the solution yet part of the problem: Factors of schizophrenia stigma in mental health professionals. Int J Psychiatry Clin Pract. (2023) 27:134–44. doi: 10.1080/13651501.2022.2129068
20. Jauch M, Occhipinti S, and O’Donovan A. The stigmatization of mental illness by mental health professionals: Scoping review and bibliometric analysis. PloS One. (2023) 18:e0280739. doi: 10.1371/journal.pone.0280739
21. Schulze B. Stigma and mental health professionals: A review of the evidence on an intricate relationship. Int Rev Psychiatry. (2007) 19:137–55. doi: 10.1080/09540260701278929
23. Reavley NJ, Mackinnon AJ, Morgan AJ, and Jorm AF. Stigmatising attitudes towards people with mental disorders: A comparison of Australian health professionals with the general community. Aust N Z J Psychiatry. (2014) 48:433–41. doi: 10.1177/0004867413500351
24. Damsté C, Gronholm PC, de Groot T, Gurung D, Makhmud A, Peters RMH, et al. Social contact as a strategy to reduce stigma in low- and middle-income countries: A systematic review and expert perspectives. PloS Global Public Health. (2024) 4:e0003053. doi: 10.1371/journal.pgph.0003053
25. Weiner B. A cognitive (attribution)-emotion-action model of motivated behavior: An analysis of judgments of help-giving. J Pers Soc Psychol. (1980) 39:186–200. doi: 10.1037/0022-3514.39.2.186
26. Corrigan PW, River LP, Lundin RK, Penn DL, Uphoff-Wasowski K, Campion J, et al. Three strategies for changing attributions about severe mental illness. Schizophr Bull. (2001) 27:187–95. doi: 10.1093/oxfordjournals.schbul.a006865
27. Lebowitz MS and Ahn W. Effects of biological explanations for mental disorders on clinicians’ empathy. Proc Natl Acad Sci. (2014) 111:17786–90. doi: 10.1073/pnas.1414058111
28. Smith ER. Social identity and social emotions: Toward new conceptualizations of prejudice. In: Affect, cognition, and stereotyping: Interactive processes in group perception. San Diego, CA: Academic Press. (1993). p. 297–315.
29. Dovidio JF, Gaertner SL, and Saguy T. Another view of “we”: Majority and minority group perspectives on a common ingroup identity. Eur Rev Soc Psychol. (2007) 18:296–330. doi: 10.1080/10463280701726132
30. Maunder RD, White FA, and Verrelli S. Modern avenues for intergroup contact: Using E-contact and intergroup emotions to reduce stereotyping and social distancing against people with schizophrenia. Group Processes Intergroup Relations. (2019) 22:947–63. doi: 10.1177/1368430218794873
31. Tapias MP, Glaser J, Keltner D, Vasquez K, and Wickens T. Emotion and prejudice: specific emotions toward outgroups. Group Processes Intergroup Relations. (2007) 10:27–39. doi: 10.1177/1368430207071338
32. Bronfenbrenner U. Toward an experimental ecology of human development. Am Psychol. (1977) 32:513–31. doi: 10.1037/0003-066X.32.7.513
33. Hatzenbuehler ML. Structural stigma and health inequalities: research evidence and implications for psychological science. Am Psychol. (2016) 71:742–51. doi: 10.1037/amp0000068
34. Larkings JS and Brown PM. Do biogenetic causal beliefs reduce mental illness stigma in people with mental illness and in mental health professionals? A systematic review. Int J Ment Health Nurs. (2018) 27:928–41. doi: 10.1111/inm.12390
35. Vistorte AOR, Ribeiro WS, Jaen D, Jorge MR, Evans-Lacko S, and de Mari JJ. Stigmatizing attitudes of primary care professionals towards people with mental disorders: A systematic review. Int J Psychiatry Med. (2018) 53:317–38. doi: 10.1177/0091217418778620
36. Colizzi M, Ruggeri M, and Lasalvia A. Should we be concerned about stigma and discrimination in people at risk for psychosis? A systematic review. psychol Med. (2020) 50:705–26. doi: 10.1017/S0033291720000148
37. Pescosolido BA, Halpern-Manners A, Luo L, and Perry B. Trends in public stigma of mental illness in the US 1996-2018. JAMA Network Open. (2021) 4:e2140202. doi: 10.1001/jamanetworkopen.2021.40202
38. Linscott RJ and van Os J. An updated and conservative systematic review and meta-analysis of epidemiological evidence on psychotic experiences in children and adults: On the pathway from proneness to persistence to dimensional expression across mental disorders. psychol Med. (2013) 43:1133–49. doi: 10.1017/S0033291712001626
39. van Os J, Linscott RJ, Myin-Germeys I, Delespaul P, and Krabbendam L. A systematic review and meta-analysis of the psychosis continuum: Evidence for a psychosis proneness-persistence-impairment model of psychotic disorder. psychol Med. (2009) 39:179–95. doi: 10.1017/S0033291708003814
40. Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ. (2021) 372:n71. doi: 10.1136/bmj.n71
41. Owens DK, Lohr KN, Atkins D, and Treadwell JR. Grading The Strength Of A Body Of Evidence. Rockville, Maryland: Agency for Healthcare Research and Quality (AHRQ). (2009).
42. Covidence systematic review software. Melbourne, Australia: Veritas Health Innovation. (2024). Available at: https://www.covidence.org/ (Accessed August 13, 2025).
43. Villiger J, Schweiger SA, and Baldauf A. Making the invisible visible: guidelines for the coding process in meta-analyses. Organizational Res Methods. (2022) 25:716–40. doi: 10.1177/10944281211046312
44. Ayano G, Assefa D, Haile K, Chaka A, Haile K, Solomon M, et al. Mental health training for primary health care workers and implication for success of integration of mental health into primary care: Evaluation of effect on knowledge, attitude and practices (KAP)”: Correction. Int J Ment Health Syst. (2017) 11:1–8. Available online at: https://ezp.lib.rochester.edu/login?url=https://www.proquest.com/docview/1968546084?accountid=13567&bdid=80108&_bd=6zT8KGdHR%2BCBkhnTYaZ9lpcuT5s%3D (Accessed December 20, 2024).
45. Baba Y, Nemoto T, Tsujino N, Yamaguchi T, Katagiri N, and Mizuno M. Stigma toward psychosis and its formulation process: prejudice and discrimination against early stages of schizophrenia. Compr Psychiatry. (2017) 73:181–6. doi: 10.1016/j.comppsych.2016.11.005
46. Björkman T, Angelman T, and Jönsson M. Attitudes towards people with mental illness: A cross-sectional study among nursing staff in psychiatric and somatic care. Scand J Caring Sci. (2008) 22:170–7. doi: 10.1111/j.1471-6712.2007.00509.x
47. Burns T, Greenwood N, Kendrick T, and Garland C. Attitudes of general practitioners and community mental health team staff towards the locus of care for people with chronic psychotic disorders. Primary Care Psychiatry. (2000) 6:67–71. doi: 10.1185/135525700543253
48. Caldwell TM and Jorm AF. Mental health nurses’ beliefs about likely outcomes for people with schizophrenia or depression: A comparison with the public and other healthcare professionals. Aust N Z J Ment Health Nurs. (2001) 10:42–54. doi: 10.1046/j.1440-0979.2001.00190.x
49. Chang NA, Grant PM, Luther L, and Beck AT. Effects of a recovery-oriented cognitive therapy training program on inpatient staff attitudes and incidents of seclusion and restraint. Community Ment Health J. (2014) 50:415–21. doi: 10.1007/s10597-013-9675-6
50. Chowdhury AN, Sanyal D, Dutta SK, Banerjee S, De R, Bhattacharya K, et al. Stigma and mental illness: Pilot study of laypersons and health care providers with the EMIC in rural West Bengal, India. Int Med J. (2000) 7:257–60.
51. Corrigan PW, Mittal D, Reaves CM, Haynes TF, Han X, Morris S, et al. Mental health stigma and primary health care decisions. Psychiatry Res. (2014) 218:35–8. doi: 10.1016/j.psychres.2014.04.028
52. Dabby L, Tranulis C, and Kirmayer LJ. Explicit and implicit attitudes of canadian psychiatrists toward people with mental illness. Can J Psychiatry. (2015) 60:451–9. doi: 10.1177/070674371506001006
53. da Silva AG, Loch AA, Leal VP, da Silva PR, Rosa MM, Bomfim O, et al. Stigma toward individuals with mental disorders among Brazilian psychiatrists: A latent class analysis. Braz J Psychiatry. (2021) 43:262–8. doi: 10.1590/1516-4446-2020-0864
54. Elizur A, Neumann M, and Bawer A. Interdependency of attitudes, diagnostic assessments and therapeutic recommendations of medical students towards mental patients. Int J Soc Psychiatry. (1986) 32:31–40. doi: 10.1177/002076408603200305
55. Fekih-Romdhane F, Hamdi F, Jahrami H, and Cheour M. Attitudes toward schizophrenia among Tunisian family medicine residents and non-medical students. Psychosis: Psychol Soc Integr Approaches. (2022) 15(2): 168–80. doi: 10.1080/17522439.2022.2032291
56. Fontesse S, Rimez X, and Maurage P. Stigmatization and dehumanization perceptions towards psychiatric patients among nurses: A path-analysis approach. Arch Psychiatr Nurs. (2021) 35:153–61. doi: 10.1016/j.apnu.2020.12.005
57. Fujii T, Hanya M, Murotani K, and Kamei H. Scale development and an educational program to reduce the stigma of schizophrenia among community pharmacists: A randomized controlled trial. BMC Psychiatry. (2021) 21:211. doi: 10.1186/s12888-021-03208-z
58. García-Carpintero Blas E, Vélez-Vélez E, Gómez-Moreno C, Martínez-Arce A, Tovar-Reinoso A, Rodriguez-Gómez P, et al. Simulation with a standardised patient to reduce stigma towards people with schizophrenia spectrum disorder among nursing students: A quasi-experimental study. Arch Psychiatr Nurs. (2024) 52:24–30. doi: 10.1016/j.apnu.2024.07.015
59. Gonzales L, López-Aybar L, and McCullough B. Variation in provider attitudes and treatment recommendations for individuals with schizophrenia and additional marginalized identities: A mixed-method study. Psychiatr Rehabil J. (2021) 44:107–17. doi: 10.1037/prj0000461
60. Grausgruber A, Meise U, Katschnig H, Schöny W, and Fleischhacker WW. Patterns of social distance towards people suffering from schizophrenia in Austria: A comparison between the general public, relatives and mental health staff. Acta Psychiatr Scand. (2007) 115:310–9. doi: 10.1111/j.1600-0447.2006.00882.x
61. Hansson L, Jormfeldt H, Svedberg P, and Svensson B. Mental health professionals’ attitudes towards people with mental illness: Do they differ from attitudes held by people with mental illness? Int J Soc Psychiatry. (2013) 59:48–54. doi: 10.1177/0020764011423176
62. Hemingway J, Kunz J, Draney D, Martin DE, and Sukpraprut-Braaten S. Evaluating stigmatization toward mental illnesses among resident physicians. Cureus. (2024) 16:e61648. doi: 10.7759/cureus.61648
63. Hsiao CY, Lu HL, and Tsai YF. Factors associated with primary family caregivers’ Perceptions on quality of family-centered care in mental health practice. J Nurs Scholarsh. (2019) 51:680–8. doi: 10.1111/jnu.12526
64. Ishige N and Hayashi N. Occupation and social experience: Factors influencing attitude towards people with schizophrenia. Psychiatry Clin Neurosci. (2005) 59:89–95. doi: 10.1111/j.1440-1819.2005.01337.x
65. Jorm AF, Korten AE, Jacomb PA, Christensen H, and Henderson S. Attitudes towards people with a mental disorder: A survey of the Australian public and health professionals. Aust N Z J Psychiatry. (1999) 33:77–83. doi: 10.1046/j.1440-1614.1999.00513.x
66. Kaitz JE, Steinhilber KM, and Harris JI. Influence of provider gender on mental health stigma. Community Ment Health J. (2022) 58:536–40. doi: 10.1007/s10597-021-00849-y
67. Kataoka M, Ohira T, Tsuboi S, Miura I, and Yabe H. Comparison of attitudes toward schizophrenia among medical students and health professionals in Japan and their associated factorsamong medical students: A cross-sectional study. Fukushima J Med Sci. (2024) 70:219–28. doi: 10.5387/fms.23-00012
68. Kermode M, Bowen K, Arole S, Pathare S, and Jorm AF. Attitudes to people with mental disorders: A mental health literacy survey in a rural area of Maharashtra, India. Soc Psychiatry Psychiatr Epidemiol: Int J Res Soc Genet Epidemiol Ment Health Serv. (2009) 44:1087–96. doi: 10.1007/s00127-009-0031-7
69. Korszun A, Dinos S, Ahmed K, and Bhui K. Medical students attitudes about mental illness: Does medical-school education reduce stigma? Acad Psychiatry. (2012) 36:197–204. doi: 10.1176/appi.ap.10110159
70. Lawrie SM, Parsons C, Patrick J, Masson S, Sussmann J, Cumming D, et al. A controlled trial of general practitioners’ attitudes to patients with schizophrenia. Health Bull (Edinb). (1996) 54:201–3.
71. Lee EH-M, Hui CL-M, Ching EY-N, Lin J, Chang W-C, Chan SK-W, et al. Public stigma in China associated with schizophrenia, depression, attenuated psychosis syndrome, and psychosis-like experiences. Psychiatr Serv. (2016) 67:766–70. doi: 10.1176/appi.ps.201500156
72. Magliano L, Citarelli G, and Read J. The beliefs of non-psychiatric doctors about the causes, treatments, and prognosis of schizophrenia. Psychol Psychother. (2020) 93:674–89. doi: 10.1111/papt.12252
73. Mannarini S, Rossi A, and Munari C. How do education and experience with mental illness interact with causal beliefs, eligible treatments and stigmatising attitudes towards schizophrenia? A comparison between mental health professionals, psychology students, relatives and patients. BMC Psychiatry. (2020) 20:167. doi: 10.1186/s12888-020-02580-6
74. Mittal D, Ounpraseuth ST, Reaves C, Chekuri L, Han X, Corrigan P, et al. Providers’ Personal and professional contact with persons with mental illness: relationship to clinical expectations. Psychiatr Serv. (2016) 67:55–61. doi: 10.1176/appi.ps.201400455
75. Noblett JE, Lawrence R, and Smith JG. The attitudes of general hospital doctors toward patients with comorbid mental illness. Int J Psychiatry Med. (2015) 50:370–82. doi: 10.1177/0091217415612721
76. Oliveira AM, MaChado D, Fonseca JB, Palha F, Silva Moreira P, Sousa N, et al. Stigmatizing attitudes toward patients with psychiatric disorders among medical students and professionals. Front Psychiatry. (2020) 11:326. doi: 10.3389/fpsyt.2020.00326
77. O’Reilly CL, Bell JS, and Chen TF. Pharmacists’ beliefs about treatments and outcomes of mental disorders: A mental health literacy survey. Aust New Z J Psychiatry. (2010) 44:1089–96. doi: 10.3109/00048674.2010.512864
78. Richards SJ, O’Connell KA, and Dickinson JK. A Missed Opportunity to Cultivate Positive Attitudes about Mental Health Recovery among Undergraduate Nursing Students—A Quasi-Experimental Controlled Study. Issues Ment Health Nurs. (2024) 45:391–8. doi: 10.1080/01612840.2023.2291653
79. Silverstein SM, Hatashita-Wong M, Wilkniss S, Bloch A, Smith T, Savitz A, et al. Behavioral rehabilitation of the “treatment-refractory” schizophrenia patient: Conceptual foundations, interventions, and outcome data. psychol Serv. (2006) 3:145–69. doi: 10.1037/1541-1559.3.3.145
80. Strauser DR, Ciftci A, and O’Sullivan D. Using attribution theory to examine community rehabilitation provider stigma. Int J Rehabil Res. (2009) 32:41–7. doi: 10.1097/MRR.0b013e328307f5b0
81. Tay JL, Qu Y, Lim L, Puthran R, Tan CLR, Rajendran R, et al. Impact of a virtual reality intervention on stigma, empathy, and attitudes toward patients with psychotic disorders among mental health care professionals: randomized controlled trial. JMIR Ment Health. (2025) 12:e66925. doi: 10.2196/66925
82. Tsoi OYY, Chan SKW, Chui AHC, Hui CLM, Chang WC, Lee EHM, et al. Effect of brief social contact video compared with expert information video in changing knowledge and attitude towards psychosis patients among medical students. Early Intervention Psychiatry. (2021) 15:278–85. doi: 10.1111/eip.12938
83. Volmer D, Mäesalu M, and Bell JS. Pharmacy students’ attitudes toward and professional interactions with people with mental disorders. Int J Soc Psychiatry. (2008) 54:402–13. doi: 10.1177/0020764008090427
84. Yashikhina A, Romanov D, Strelnik S, Gradinar A, Markina E, Kuvshinova N, et al. Non-psychiatrist healthcare professionals? Attitudes toward patients with mental disorders: lower scores in social distance as a fragile facet of public stigma against depression. Psychiatr Danub. (2022) 34:238–45.
85. Corrigan PW, River LP, Lundin RK, Wasowski KU, Campion J, Mathisen J, et al. Stigmatizing attributions about mental illness. J Community Psychol. (2000) 28:91–102. doi: 10.1002/(SICI)1520-6629(200001)28:1<91::AID-JCOP9>3.0.CO;2-M
86. Khandel Wal SK and Workneh F. Change in perception of mental illnesses by undergraduate medical students of Addis Ababa following psychiatric attachment. Indian J Psychiatry. (1987) 29:57–62.
87. Servais LM and Saunders SM. Clinical psychologists’ perceptions of persons with mental illness. Prof Psychol: Res Pract. (2007) 38:214–9. doi: 10.1037/0735-7028.38.2.214
88. Parcesepe AM and Cabassa LJ. Public stigma of mental illness in the United States: A systematic literature review. Administration Policy Ment Health Ment Health Serv Res. (2013) 40:384–99. doi: 10.1007/s10488-012-0430-z
89. Pascucci M, La Montagna M, Di Sabatino D, Stella E, Nicastro R, Grandinetti P, et al. Stigma and attitudes towards mental illness: Gender differences in a sample of Italian medical students. Eur Psychiatry. (2017) 41:S739. doi: 10.1016/j.eurpsy.2017.01.1359
90. Kudva KG, El Hayek S, Gupta AK, Kurokawa S, Bangshan L, Armas-Villavicencio MVC, et al. Stigma in mental illness: Perspective from eight Asian nations. Asia-Pacific Psychiatry. (2020) 12:e12380. doi: 10.1111/appy.12380
91. Corrigan PW and Watson AC. Understanding the impact of stigma on people with mental illness. World Psychiatry. (2002) 1:16–20.
92. Amsalem D, Markowitz JC, Jankowski SE, Yang LH, Valeri L, Lieff SA, et al. Sustained effect of a brief video in reducing public stigma toward individuals with psychosis: A randomized controlled trial of young adults. Am J Psychiatry. (2021) 178:635–42. doi: 10.1176/appi.ajp.2020.20091293
93. Jankowski SE, Yanos P, Dixon LB, and Amsalem D. Reducing public stigma towards psychosis: A conceptual framework for understanding the effects of social contact based brief video interventions. Schizophr Bull. (2023) 49:99–107. doi: 10.1093/schbul/sbac143
94. Jorm AF. Effect of contact-based interventions on stigma and discrimination: A critical examination of the evidence. Psychiatr Serv. (2020) 71:735–7. doi: 10.1176/appi.ps.201900587
95. Carver CS. Approach, avoidance, and the self-regulation of affect and action. Motivation Emotion. (2006) 30:105–10. doi: 10.1007/s11031-006-9044-7
96. Corrigan PW. Lessons learned from unintended consequences about erasing the stigma of mental illness. World Psychiatry. (2016) 15:67–73. doi: 10.1002/wps.20295
97. Harré JRN. The role of biological and genetic causal beliefs in the stigmatisation of “mental patients. J Ment Health. (2001) 10:223–35. doi: 10.1080/09638230123129
98. Phelan JC, Cruz-rojas R, and Reiff M. Genes and stigma: the connection between perceived genetic etiology and attitudes and beliefs about mental illness. Psychiatr Rehabil Skills. (2002) 6:159–85. doi: 10.1080/10973430208408431
99. Read J. Why promoting biological ideology increases prejudice against people labelled “schizophrenic. Aust Psychol. (2007) 42:118–28. doi: 10.1080/00050060701280607
100. Thornicroft G, Mehta N, Clement S, Evans-Lacko S, Doherty M, Rose D, et al. Evidence for effective interventions to reduce mental-health-related stigma and discrimination. Lancet (London England). (2016) 387:1123–32. doi: 10.1016/S0140-6736(15)00298-6
101. Corrigan PW and Shapiro JR. Measuring the impact of programs that challenge the public stigma of mental illness. Clin Psychol Rev. (2010) 30:907–22. doi: 10.1016/j.cpr.2010.06.004
102. Davis MJ, Moore KM, Meyers K, Mathews J, and Zerth EO. Engagement in mental health treatment following primary care mental health integration contact. psychol Serv. (2016) 13:333–40. doi: 10.1037/ser0000089
103. Levine DS, McCarthy JF, Cornwell B, Brockmann L, and Pfeiffer PN. Primary care–mental health integration in the VA health system: associations between provider staffing and quality of depression care. Psychiatr Serv. (2017) 68:476–81. doi: 10.1176/appi.ps.201600186
104. Possis E, Skroch B, Hintz S, Bronars C, Mallen M, Crowl H, et al. Examining and improving provider adherence to the primary care mental health integration model. Military Med. (2020) 185:e1411–6. doi: 10.1093/milmed/usaa140
105. Walton GM and Yeager DS. Seed and soil: psychological affordances in contexts help to explain where wise interventions succeed or fail. Curr Dir Psychol Sci. (2020) 29(3):219–26. doi: 10.1177/0963721420904453
106. Au M, Kehn M, Ireys H, Blyler C, and Brown J. Care coordinators in integrated care: burnout risk, perceived supports, and job satisfaction. Am J Prev Med. (2018) 54:S250–7. doi: 10.1016/j.amepre.2018.01.044
107. Zubatsky M, Runyan C, Gulotta S, Knight JR, and Pettinelli JD. Burnout among behavioral health providers in integrated care settings. Families Syst Health. (2020) 38:74–82. doi: 10.1037/fsh0000456
108. Jablensky A. Epidemiology of schizophrenia: The global burden of disease and disability. Eur Arch Psychiatry Clin Neurosci. (2000) 250:274–85. doi: 10.1007/s004060070002
109. Mueser KT, Bellack AS, Douglas MS, and Morrison RL. Prevalence and stability of social skill deficits in schizophrenia. Schizophr Res. (1991) 5:167–76. doi: 10.1016/0920-9964(91)90044-r
110. Kotov R, Fochtmann L, Li K, Tanenberg-Karant M, Constantino EA, Rubinstein J, et al. Declining clinical course of psychotic disorders over the two decades following first hospitalization: evidence from the suffolk county mental health project. Am J Psychiatry. (2017) 174:1064–74. doi: 10.1176/appi.ajp.2017.16101191
111. Velthorst E, Fett A-KJ, Reichenberg A, Perlman G, van Os J, Bromet EJ, et al. The 20-year longitudinal trajectories of social functioning in individuals with psychotic disorders. Am J Psychiatry. (2017) 174:1075–85. doi: 10.1176/appi.ajp.2016.15111419
112. Browne J, Wright AC, Berry K, Mueser KT, Cather C, Penn DL, et al. The alliance-outcome relationship in individual psychosocial treatment for schizophrenia and early psychosis: A meta-analysis. Schizophr Res. (2021) 231:154–63. doi: 10.1016/j.schres.2021.04.002
113. Harangozo J, Reneses B, Brohan E, Sebes J, Csukly G, López-Ibor J, et al. Stigma and discrimination against people with schizophrenia related to medical services. Int J Soc Psychiatry. (2014) 60:359–66. doi: 10.1177/0020764013490263
114. Mucci A, Kawohl W, Maria C, and Wooller A. Treating schizophrenia: open conversations and stronger relationships through psychoeducation and shared decision-making. Front Psychiatry. (2020) 11:761. doi: 10.3389/fpsyt.2020.00761
115. Schenkel LS, Wilkniss SM, Savitz A, Spaulding WD, and Silverstein SM. The effects of a staff-training program in behavior management and social-learning principles on staff–patient interactions within a psychiatric rehabilitation inpatient unit. Am J Orthopsychiatry. (2020) 90:419–31. doi: 10.1037/ort0000443
116. Berry K, Barrowclough C, and Haddock G. The role of expressed emotion in relationships between psychiatric staff and people with a diagnosis of psychosis: A review of the literature. Schizophr Bull. (2011) 37:958–72. doi: 10.1093/schbul/sbp162
117. Berry K, Gregg L, Vasconcelos e Sa D, Haddock G, and Barrowclough C. Staff–patient relationships and outcomes in schizophrenia: The role of staff attributions. Behav Res Ther. (2012) 50:210–4. doi: 10.1016/j.brat.2012.01.004
118. Allerby K, Goulding A, Ali L, and Waern M. Increasing person-centeredness in psychosis inpatient care: Staff experiences from the Person-Centered Psychosis Care (PCPC) project. BMC Health Serv Res. (2022) 22:596. doi: 10.1186/s12913-022-08008-z
119. Cohen P and Cohen J. The clinician’s illusion. Arch Gen Psychiatry. (1984) 41:1178–82. doi: 10.1001/archpsyc.1984.01790230064010
120. Winzar H. The ecological fallacy: how to spot one and tips on how to use one to your advantage. Australas Marketing J. (2015) 23:86–92. doi: 10.1016/j.ausmj.2014.12.002
121. Yanos PT, Lucksted A, Drapalski AL, Roe D, and Lysaker P. Interventions targeting mental health self-stigma: A review and comparison. Psychiatr Rehabil J. (2015) 38:171–8. doi: 10.1037/prj0000100
122. Campbell MR and Brauer M. Incorporating social-marketing insights into prejudice research: advancing theory and demonstrating real-world applications. Perspect psychol Sci. (2020) 15:608–29. doi: 10.1177/1745691619896622
Keywords: schizophrenia, stigma, healthcare, providers, bias
Citation: Kruse EA and Dodell-Feder D (2025) Schizophrenia spectrum stigma in healthcare: a systematic review. Front. Psychiatry 16:1648957. doi: 10.3389/fpsyt.2025.1648957
Received: 17 June 2025; Accepted: 01 August 2025;
Published: 25 August 2025.
Edited by:
Massimo Tusconi, University of Cagliari, ItalyReviewed by:
Helene Speyer, Psychiatric Center Copenhagen, DenmarkJill Laquidara, Case Western Reserve University, United States
Copyright © 2025 Kruse and Dodell-Feder. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Elizabeth A. Kruse, ZS5rcnVzZUByb2NoZXN0ZXIuZWR1