 Yizhen Wu1†‡
Yizhen Wu1†‡ Yuling Qiao2†‡
Yuling Qiao2†‡ Licheng Wu1
Licheng Wu1 Minglin Gao1
Minglin Gao1 Tsz Yiu Wong1
Tsz Yiu Wong1 Jingyun Li1Zhimeng Wang3Xu Zhao3
Jingyun Li1Zhimeng Wang3Xu Zhao3 Hui Zhao1*‡
Hui Zhao1*‡ Xiwang Fan1*‡
Xiwang Fan1*‡- 1Clinical Research Center for Mental Disorders, Shanghai Pudong New Area Mental Health Center, School of Medicine, Tongji University, Shanghai, China
- 2Department of Primary Education, The New Bund School Attached to No.2 High School of East China Normal University, Shanghai, China
- 3Faculty of Psychology, Beijing Normal University, Beijing, China
Background: Major depressive disorder (MDD) in adolescents poses an increasing global health concern, yet current screening practices rely heavily on subjective reports. Virtual reality (VR), integrated with multimodal physiological sensing (EEG+ET+HRV), offers a promising pathway for more objective diagnostics.
Methods: In this case-control study, 51 adolescents diagnosed with first-episode MDD and 64 healthy controls participated in a 10-minute VR-based emotional task. Electroencephalography (EEG), eye-tracking (ET), and heart rate variability (HRV) data were collected in real-time. Key physiological differences were identified via statistical analysis, and a support vector machine (SVM) model was trained to classify MDD status based on selected features.
Results: Adolescents with MDD showed significantly higher EEG theta/beta ratios, reduced saccade counts, longer fixation durations, and elevated HRV LF/HF ratios (all p <.05). The theta/beta and LF/HF ratios were both significantly associated with depression severity. The SVM model achieved 81.7% classification accuracy with an AUC of 0.921.
Conclusions: The proposed VR-based multimodal system identified robust physiological biomarkers associated with adolescent MDD and demonstrated strong diagnostic performance. These findings support the utility of immersive, sensor-integrated platforms in early mental health screening and intervention. Future work may explore integrating the proposed multimodal system into wearable or mobile platforms for scalable, real-world mental health screening.

Graphical Abstract. Graphical abstract of the experiment.
1 Introduction
Depression is a widespread mental health disorder characterized by persistent low mood, cognitive impairments, and increased risk of suicide (1). It has become a major global public health concern (2), affecting over 300 million individuals worldwide. Experts project that depression will become the leading contributor to the global disease burden by 2030 (3, 4). Alarmingly, its prevalence among adolescents has more than doubled in recent years (5), in which one in four adolescents globally exhibit depressive symptoms—a rate that surpasses that observed in adult populations (5). In particular, the 2020 Report on National Mental Health Development in China underscores the severity of the issue, reporting a 24.6% detection rate of adolescent depression, including 7.4% classified as severe cases (6). These statistics reflect the rapidly escalating incidence of adolescent depression and its association with detrimental outcomes.
Despite the growing urgency, current diagnostic approaches for adolescent depression in China remain inadequate. They are predominantly based on symptom checklists and clinical interviews, which lack biological grounding and are susceptible to subjectivity. According to empirical research (7), over 50% of depression cases are either misdiagnosed or overlooked, significantly compromising treatment effectiveness. This underscores the urgent need for objective, biologically grounded diagnostic tools that are independent of self-report or observer bias. Such tools could serve as “emotional lie detectors,” enabling early and accurate detection of depressive states.
As advocated by an empirical study (8), the integration of artificial intelligence (AI) tools into mental health servces will significantly exhibit favorable and effective outcomes. Recent advances in AI and wearable technology offer promising avenues for more objective mental health assessments and interventions. For instance, techniques such as electroencephalography (EEG), heart rate variability (HRV), and eye-tracking (ET) have revealed distinctive neurophysiological and behavioral patterns in individuals with mental disorders compared to healthy controls (9–11). However, several challenges remain. For instance, machine learning models based on frontal EEG alpha-band asymmetry have achieved classification accuracies as high as 88.6% for depressive symptoms (12–14), yet translating these findings into clinically meaningful interpretations—such as understanding frontal lateralization—remains a hurdle (15). Similarly, while HRV-derived metrics reflect autonomic nervous system dysregulation linked to depression severity, results are often confounded by comorbidities such as cardiovascular conditions (16). Eye-tracking studies suggest that individuals with depression exhibit attentional biases toward negative stimuli; however, diagnostic accuracy is limited by inter-individual variability in smooth pursuit and saccadic eye movements (17–19). These limitations reinforce the need for novel screening paradigms that mitigate subjectivity and enhance early detection precision.
Virtual reality (VR) presents a compelling solution by enabling the integration of multimodal data within standardized, immersive environments. VR allows for the seamless collection of behavioral and physiological metrics—such as body movement, gaze patterns, and biosignals—without disrupting user engagement (20, 21). Unlike traditional media, VR’s interactive nature fosters deeper cognitive, social, and physical involvement, thereby enhancing the reliability of psychological assessments (22). Prior research (23, 24) has shown strong correlations between VR-derived metrics and established diagnostic criteria for disorders including schizophrenia, ADHD, and OCD. However, the application of VR in the context of adolescent depression remains underexplored, with no existing standardized frameworks—highlighting a crucial gap in the field.
In response to this gap, our study introduces a pioneering VR-based machine learning framework for screening adolescent depression. By synchronously capturing EEG, HRV, and ET data during user interaction within a VR environment, we aim to identify robust biomarkers of depressive states. This approach seeks to establish a more objective and scalable diagnostic model for adolescent depression, transcending the limitations of traditional methods. Ultimately, this technology-driven paradigm has the potential to transform early identification and intervention strategies for adolescent mental health.
The contributions can be listed as:
Proposes a novel VR-based multimodal framework for adolescent depression screening, integrating EEG, HRV, and eye-tracking (ET) to overcome subjectivity in traditional diagnostic methods.
Develops a machine learning model leveraging synchronized neurophysiological and behavioral data from VR immersion to identify depression biomarkers with higher objectivity than symptom-based assessments.
Addresses a critical gap in adolescent mental health diagnostics by pioneering standardized VR paradigms tailored to this population, where existing tools are scarce or reliant on self-report.
Enhances early detection accuracy by combining immersive environmental control with real-time biosignal analysis, mitigating confounders like comorbidities or inter-individual variability.
Lays groundwork for scalable, technology-driven interventions by demonstrating the clinical translatability of VR and machine learning in mental health screening.
2 Materials and methods
2.1 Study design and participants
This case-control study was conducted at Weng'an Middle School. From April 2023 to October 2024, a total of 51 adolescents diagnosed with Major Depressive Disorder (MDD) according to DSM-5 criteria (25) and free from psychiatric medications were recruited as the experimental group. While the control group comprised 64 healthy controls (HCs), who were recruited between November 6 and November 20, 2024. All controls underwent standardized psychological screening to confirm the absence of psychiatric history. Ethical approval was granted by the Shanghai Pudong New District Medical Ethics Committee (Approval No. PDJW-KY-2022-011GZ-02), and written informed consent was obtained from all adolescent participants, along with assent from their guardians as required.
The sample size for this study was determined through a power analysis - G*Power 3.1 (26) based on prior neurophysiological research in adolescent depression. Assuming a medium-to-large effect size (d = 0.6–0.8) for group differences in EEG, ET, and HRV metrics (9), a minimum of 50 participants per group was required to achieve 80% power (α = 0.05, two-tailed). Our final sample (MDD: n = 51; HC: n = 64) exceeded this threshold, aligning with recommendations for machine learning-based biomarker studies (27) and ensuring robust feature selection via RFECV. This sample size is comparable to validated VR-based psychiatric assessments (28, 29) and sufficient to detect clinically meaningful correlations (e.g., theta/beta ratio vs. CES-D: r = 0.575, p <.001) after Bonferroni correction.
Due to time and funding constraints, participants were recruited from a specific region of China. However, this does not necessarily limit the generalizability of the research. First, our study focuses on MDD, which exhibits high cross-cultural consistency in diagnosis and core symptoms (25, 30). Since DSM-5 criteria are internationally recognized, our findings may extend to other populations, though cultural variations in symptom expression warrant further investigation. Moreover, many psychological phenomena are not strongly influenced by cultural factors. Several other studies with similar participant backgrounds have demonstrated high external validity in subsequent research (31–34). Thus, our research offers a foundational contribution to this field and can guide future cross-cultural validations.
2.2 Materials
This study employed a multimodal assessment framework combining validated clinical instruments with advanced neurophysiological monitoring techniques. Depression severity was assessed using the Chinese version of the Center for Epidemiologic Studies Depression Scale (CES-D) (35). Physiological data—including electroencephalography (EEG), ocular motility, and electrocardiogram (ECG)—were recorded using the BIOPAC MP160 system and a See A8 portable telemetric ophthalmoscope.
The virtual reality (VR) environment was embedded within immersive scenarios designed to enhance ecological validity while preserving experimental rigor. A custom VR environment that was developed using the A-Frame framework (36), served as the foundation for the virtual scenes. The system integrated the Claude API (37) to enable dynamic therapeutic dialogue and was delivered through computers. This configuration created a psychologically interactive VR space that supported the detection of depressive symptoms by combining immersive virtual experiences with the natural language capabilities of large language models (LLMs) (38).
As indicated in Table 1, the VR immersive setting consisted of panoramic background representing a magical forest by a lakeside, combined with the animated appearance of an AI agent named “Xuyu.” The agent’s dialogue prompts were derived from a standardized script to ensure consistency across participants and reproducibility of the task. Besides, environmental features such as the panoramic background, ambient effects, and the agent’s visual presentation remained constant across all sessions, ensuring controlled conditions. Regarding the task details, participants engaged in interactive dialogues with the agent, who actively initiated conversations around themes of personal worries, distress, and hopes for the future. The overall experience was structured with a fixed duration of approximately 10 minutes, during which the sequence of interaction included an initial greeting, guided emotional exploration, supportive responses, and optional reflective or hopeful exchanges. By creating a secure and private context, participants could express recent emotional distress and future aspirations, which may serve as valuable diagnostic indicators for depression screening.
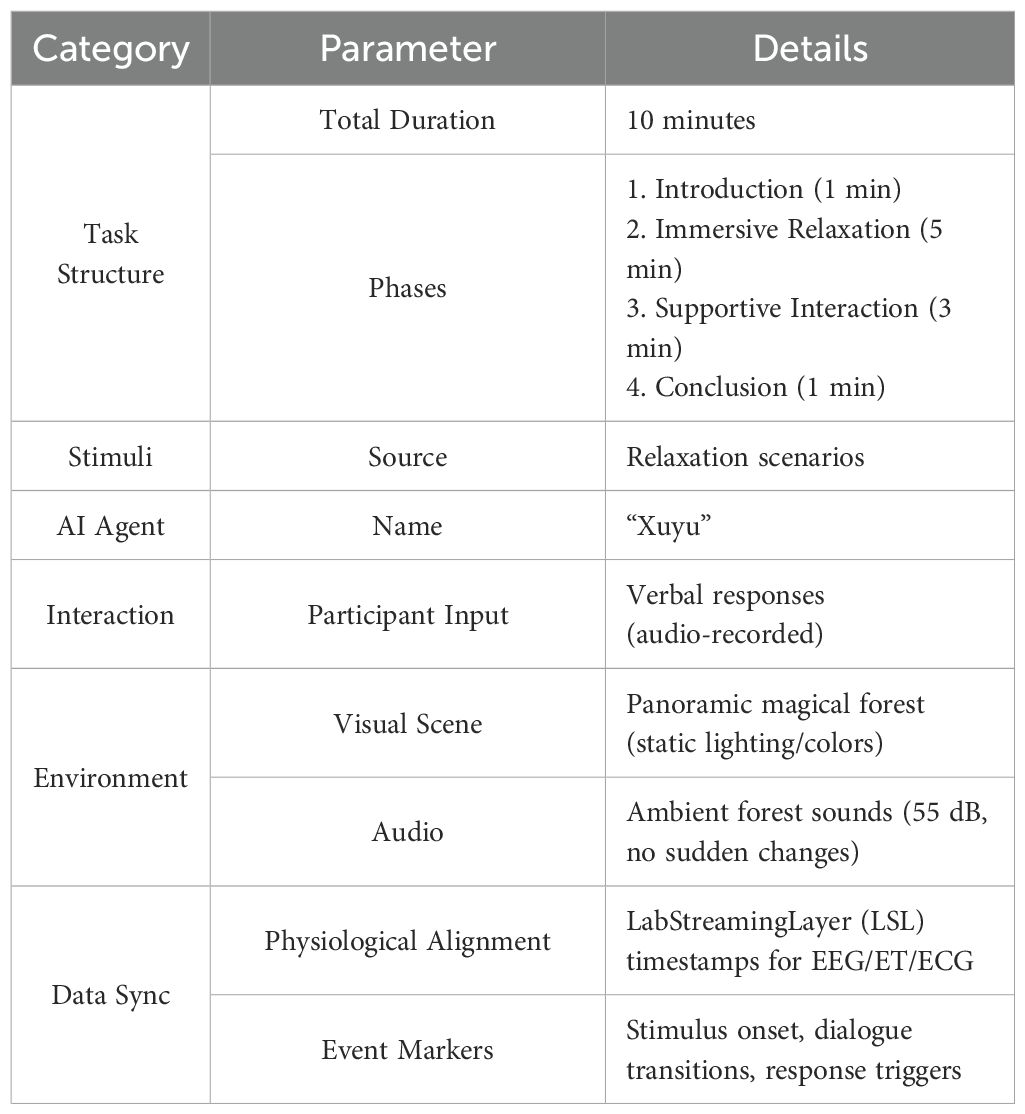
Table 1. Summary of task parameters.
2.3 Procedure
The whole procedure is presented in the graphical abstract below (Figure 1). All participants completed the experimental protocol in a sound-attenuated laboratory with standardized ambient lighting conditions. Following initial demographic and clinical assessments, participants were exposed to a 10-minute VR session during which physiological data were continuously recorded.
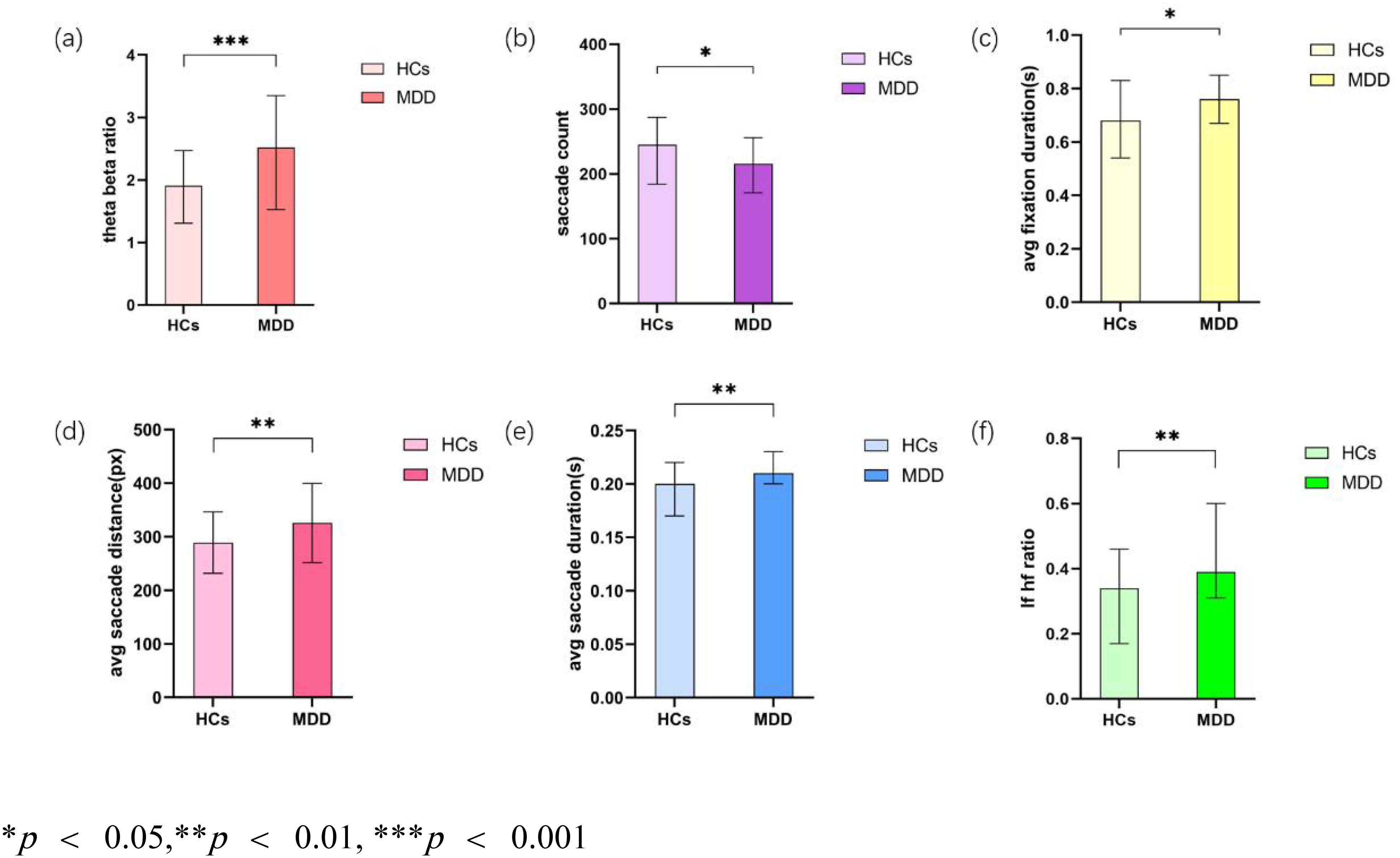
Figure 1. Analysis of key Indicators. (a) Theta beta ratio; (b) Saccade count; (c) Average fixation duration (s); (d) Average saccade distance (px); (e) Average saccade duration (s); (f) LF/HF ratio.
2.4 Data processing and analysis
EEG data were preprocessed through linear interpolation, band-pass filtering between 0.5–100 Hz, and 50 Hz notch filtering to remove powerline noise. Artifacts were removed using discrete wavelet transform (DWT) (39). Eye-tracking data, sampled at 60 Hz, were cleaned by removing outliers, standardizing features, and imputing missing values using either mean or median estimates, as appropriate.
Statistical comparisons between the major depressive disorder (MDD) and healthy control (HC) groups were performed using independent-sample t-tests for normally distributed variables, and Mann–Whitney U tests (40) for non-parametric data. A two-tailed significance threshold was set at p < 0.05. Effect sizes were reported using Cohen’s d (41) for parametric tests and rank-biserial correlation for non-parametric tests, along with corresponding 95% confidence intervals.
For classification analysis, a Support Vector Machine (SVM) (42) with a radial basis function (RBF) kernel was implemented using the scikit-learn library (v1.0.2). Feature selection was performed via recursive feature elimination with cross-validation (RFECV) (27) to identify the most predictive biomarkers from the multimodal dataset. Hyperparameters (C = 100, γ = 0.1) were optimized through five-fold cross-validation. Class imbalance was addressed by applying weighted training strategies. Model performance was assessed based on accuracy, the area under the receiver operating characteristic curve (AUC-ROC), and permutation testing with 1,000 iterations to establish statistical significance of the classification outcomes.
3 Results
3.1 Demographic data
As shown in Table 2, the study included 115 participants in total, comprising 64 healthy controls (HCs) and 51 adolescents with MDD. Gender distribution was similar across groups, with 35.29% males in the MDD group and 45.31% in the HC group (p = 0.278). As expected, depression severity, measured by the CES-D scale, was markedly higher in the MDD group (24.82 ± 6.16) compared to HCs (9.53 ± 4.39; p < 0.001), which confirmed the clinical validity of the group classification.
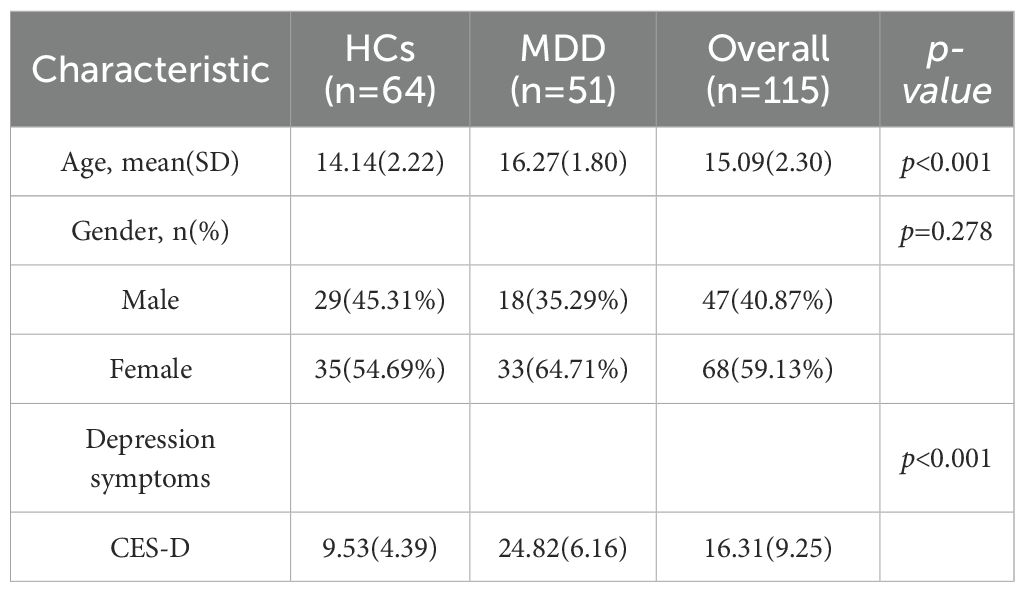
Table 2. Sample characteristics.
3.2 Multivariate analysis
In the domain of EEG measurements, the MDD group exhibited a significantly elevated theta/beta ratio compared to the control group (MDD: 2.52 [1.53, 3.35]; Control: 1.91 [1.31, 2.47]; p = .001) (Figure 1a). Regarding eye-tracking metrics, the depression group showed a notably reduced saccade count (MDD: 216 [171, 256]; Control: 245 [184.25, 287.25]; p = .046) (Figure 1b). Additionally, the mean fixation duration was significantly longer in the MDD group (0.76 [0.67, 0.85] s) relative to controls (0.68 [0.54, 0.83] s; p = .046) (Figure 1c). The average saccade distance was also greater in the depression group (325.59 ± 73.70 px) than in controls (288.82 ± 57.25 px), yielding a t-value of 9.066 (p = .003) (Figure 1d). Likewise, the mean saccade duration was significantly increased in the MDD group (0.21 [0.20, 0.23] s) compared to the control group (0.20 [0.17, 0.22] s; p = .004) (Figure 1e). In terms of autonomic nervous system activity, participants with MDD demonstrated a significantly elevated low-frequency to high-frequency (LF/HF) ratio (MDD: 0.39 [0.31, 0.60]; Control: 0.34 [0.17, 0.46]; p = .003) (Figure 1f), indicating altered heart rate variability patterns.
3.3 Correlation analysis
To mitigate the risk of Type I errors arising from multiple comparisons between physiological indicators and depression scores, a Bonferroni correction (43) was applied. The adjusted significance threshold was calculated as: α_corrected = α_original/m, where m represents the product of the number of EEG indicators, eye-tracking, HRV features, and the number of depression scales used.
In this study, depression severity was evaluated using the CES-D scale (35). Based on group-level comparisons, one EEG measure, four eye-tracking metrics, and one HRV variable were identified as significantly different between groups, yielding an adjusted alpha level of α_corrected = 0.0125. Within the MDD group, CES-D scores were positively correlated with the theta/beta ratio (r = 0.575, p <.001) (Figure 2a) and the LF/HF ratio (r = 0.575, p <.001) (Figure 2b), both exceeding the corrected significance threshold. In contrast, no significant correlations were observed between CES-D scores and average saccade distance (p = .180), saccade duration (p = .287), saccade count (p = .443), or fixation duration (p = .243).
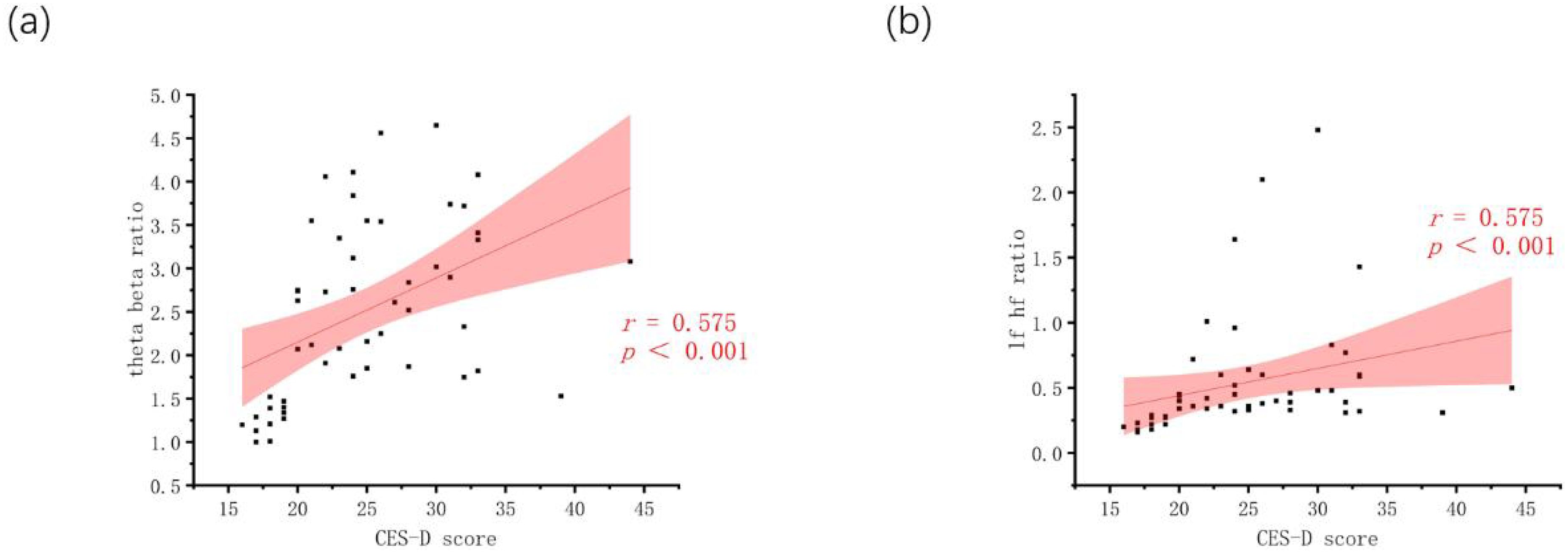
Figure 2. Correlation plots. (a) Theta beta ratio vs. CES-D; (b) LF/HF ratio vs. CES-D.
3.4 Classification performance
An SVM-based binary classification model (Figure 3) was developed to differentiate individuals with MDD from healthy controls. The model was optimized via five-fold cross-validation, using a radial basis function (RBF) kernel with hyperparameters set to C = 100 and γ = 0.1. Only physiological features that demonstrated statistically significant differences between groups (p <.01) were included as input features. Under the equal class weight condition, Figure 3 illustrates that the model achieved an overall accuracy of 81.74% and an area under the ROC curve (AUC) of 0.921, indicating strong classification performance.
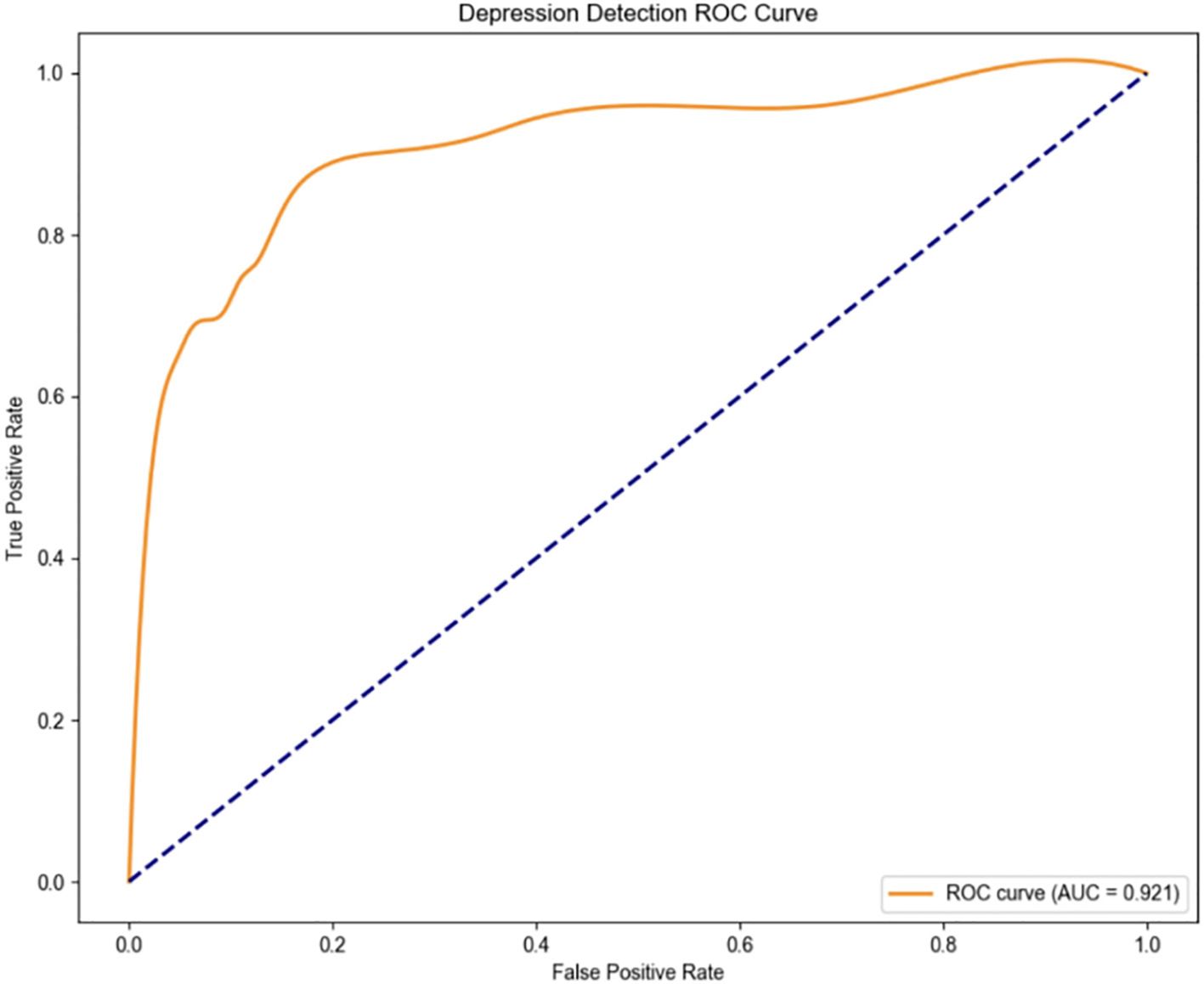
Figure 3. ROC curve (“normal” class weight = 1, “depression” class weight = 1).
The classification report and confusion matrix (Figure 4) revealed that the model performed well in identifying the control group, while the recall rate for the depression group was relatively lower (Recall = 0.65) (Figure 5), suggesting a degree of under-diagnosis.
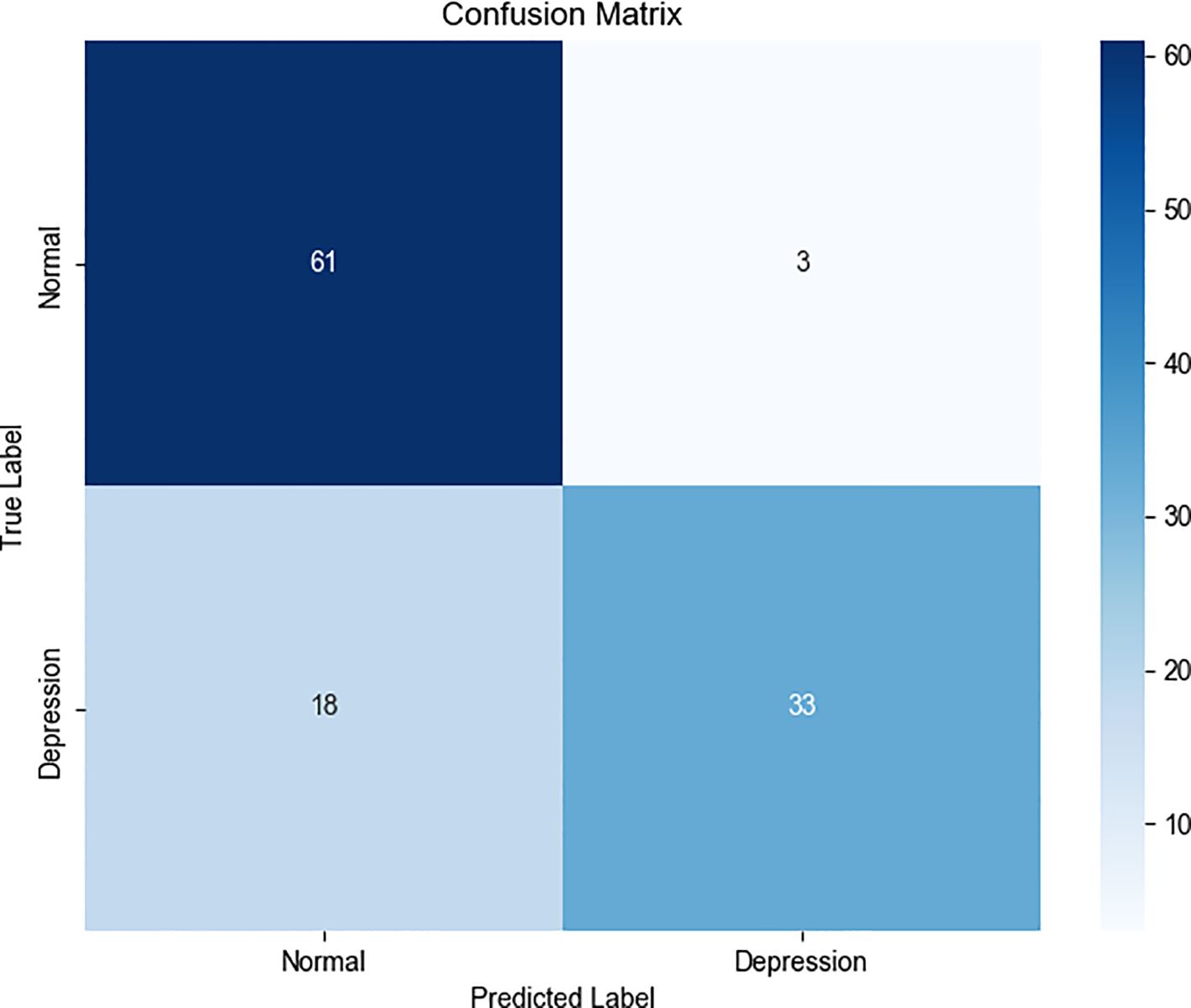
Figure 4. Confusion matrix (“normal” class weight = 1, “depression” class weight = 1).
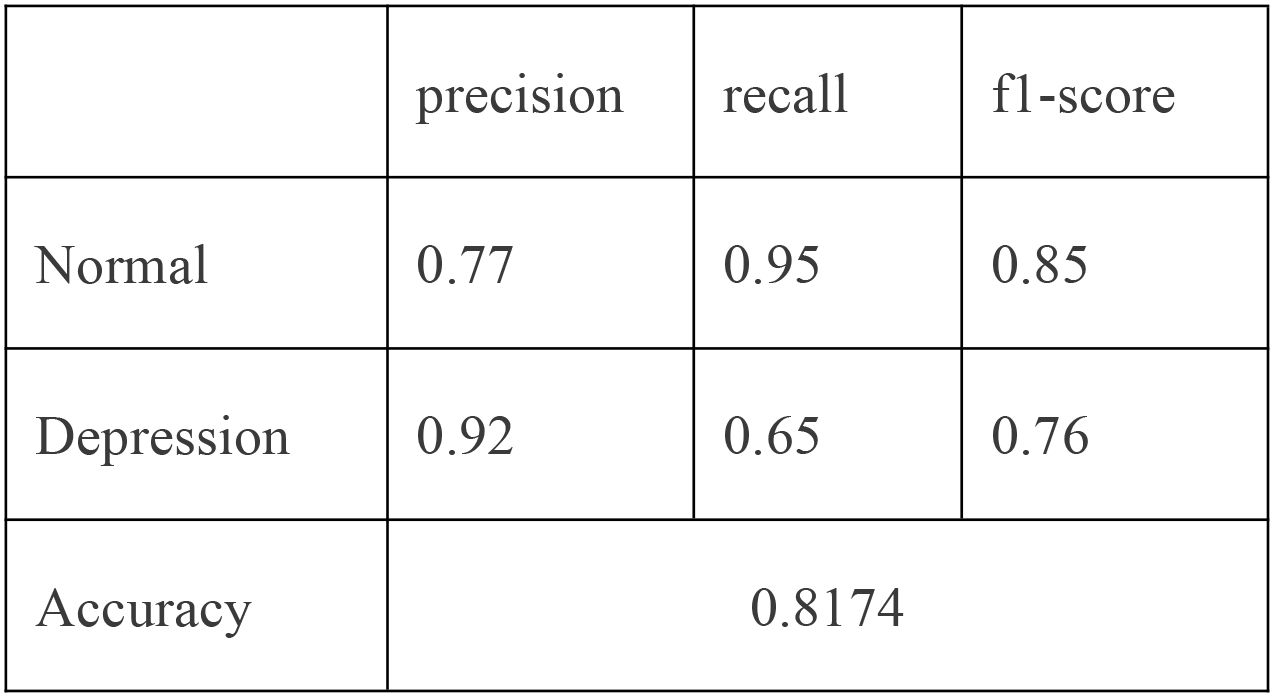
Figure 5. Classification report (“normal” class weight = 1, “depression” class weight = 1).
In practical scenarios, such as in healthcare where missing a positive case is more critical than making a false positive, we can increase the weight of the “depression” class—for example, raising its weight to 1.25 as displayed in Figure 6 - ROC curve and Figure 7 - Confusion matrix. This adjustment can improve the recall and other relevant metrics, as shown Figure 8:
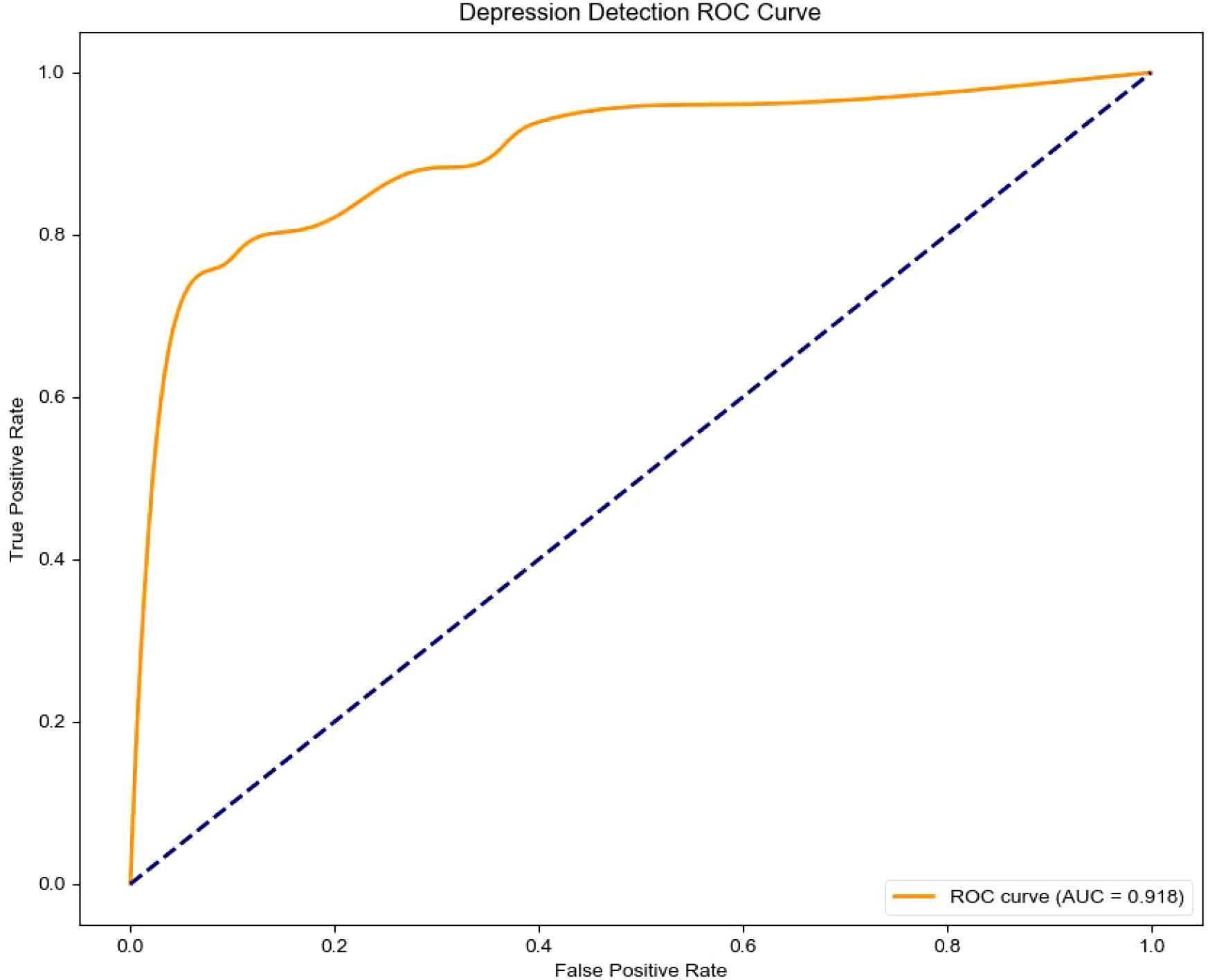
Figure 6. Confusion matrix (“normal” class weight = 1, “depression” class weight = 1.25).
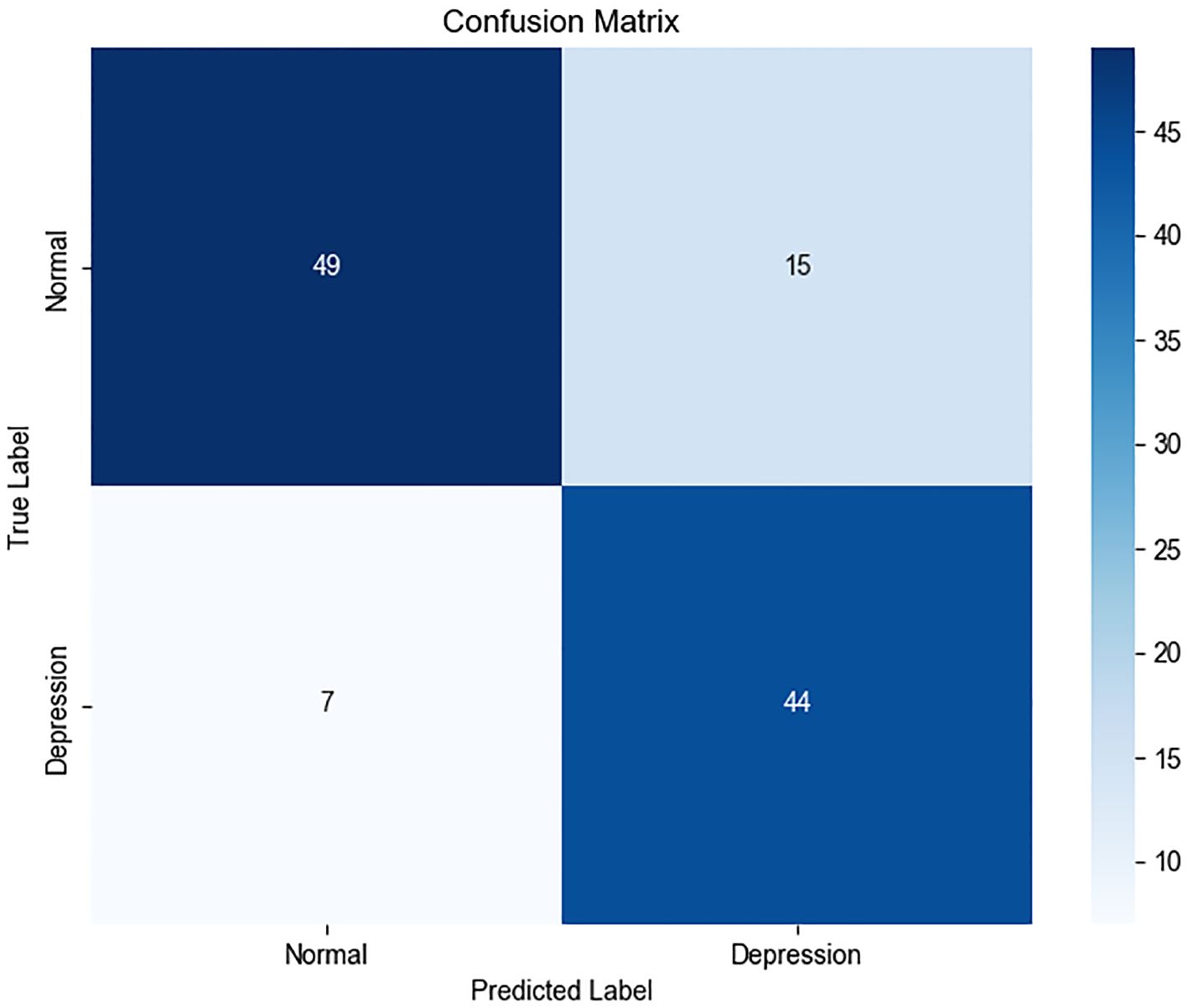
Figure 7. Confusion matrix (“normal” class weight = 1, “depression” class weight = 1.25).
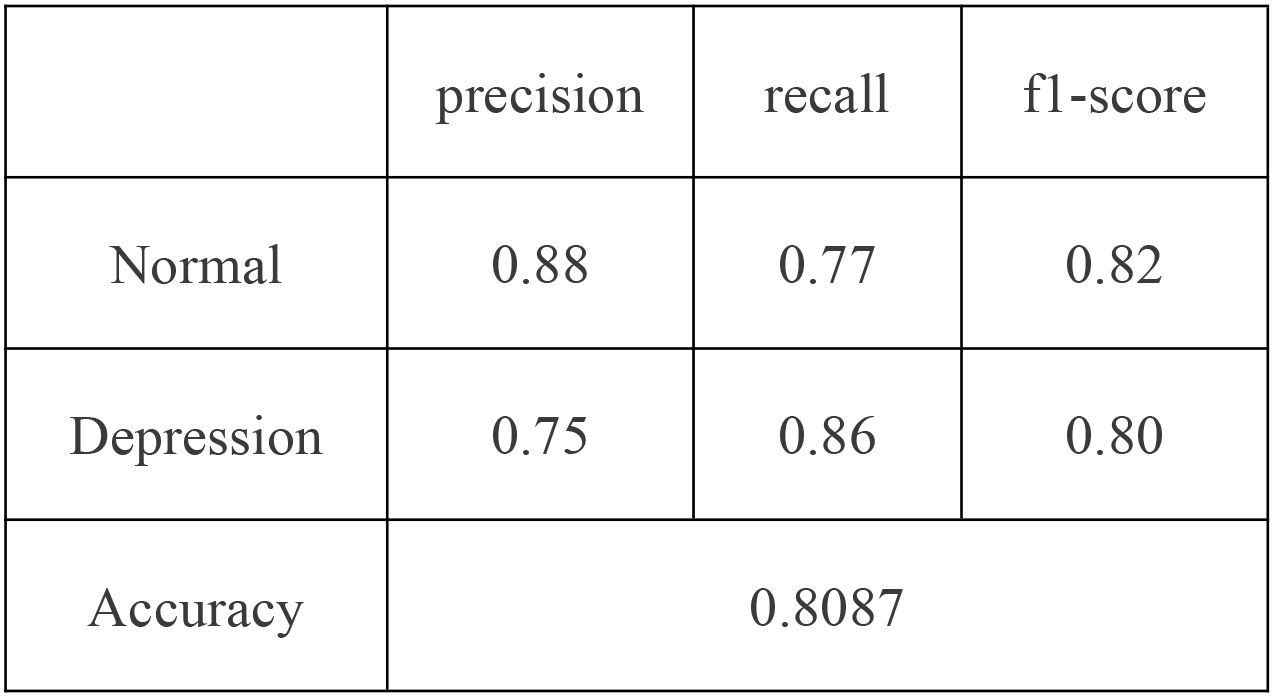
Figure 8. Classification report (“normal” class weight = 1, “depression” class weight = 1.25).
In summary, the proposed model demonstrates robust performance in identifying individuals with depression. For practical deployment, the classification strategy can be flexibly adjusted by tuning class weights according to application-specific risk preferences.
4 Discussion
4.1 Key findings
This study identified robust physiological markers of adolescent MDD through a novel, VR-integrated multimodal assessment framework. Compared to healthy controls, adolescents with MDD exhibited elevated theta/beta EEG ratios, altered ocular motility patterns—characterized by reduced saccade counts but increased fixation duration and saccade distance/duration—and heightened LF/HF ratios in HRV. Among these, four features—theta/beta ratio, LF/HF ratio, saccade distance, and saccade duration—demonstrated significant correlations with depression severity (p <.0125, Bonferroni-corrected). When integrated into a SVM model, these physiological indicators yielded an overall classification accuracy of 81.7% (AUC = 0.921), underscoring their potential as objective biomarkers for MDD. These findings are consistent with established neurophysiological models of depression implicating impaired cortical arousal regulation and autonomic dysfunction. Importantly, this work advances previous studies by incorporating multimodal signals within an ecologically valid, immersive environment (44).
4.2 Comparison with prior works
Recent advances in machine learning have led to substantial progress in the objective identification of major depressive disorder (MDD), particularly through the use of multimodal physiological data such as EEG, eye-tracking, and autonomic indicators. Multiple studies have shown that classification models achieving over 80% accuracy are not only feasible but also meet current expectations for psychiatric screening tools. For instance, a systematic review and meta-analysis of resting-state functional MRI-based machine learning models reported classification accuracies ranging from approximately 75% to 89%, depending on data modality and model configuration, supporting the reliability of accuracies within this range for MDD diagnosis (45). In addition, research leveraging eye-tracking features within virtual reality environments has demonstrated high diagnostic precision; one study reported an accuracy of 86% and an F1 score of 0.92 in distinguishing individuals with depression from controls using eye movement features alone (46). Furthermore, the inclusion of eye-tracking biomarkers has been shown to significantly improve the diagnostic performance of models identifying depression with mixed symptom presentations (47). Beyond behavioral signals, multimodal physiological studies integrating EEG, eye-tracking, and galvanic skin response (GSR) have consistently demonstrated robust performance, with classification accuracies close to 80% (48). A broader synthesis of machine learning applications in psychiatry also highlights that diagnostic models in this field commonly operate within the 80–90% accuracy range, reaffirming this threshold as a credible benchmark (49).
As a consequence, these collective findings reinforce the validity of the current study’s classification results. Our model’s accuracy of 81.7% aligns well with prior research and demonstrates that a performance level above 80% is both empirically grounded and clinically acceptable for MDD identification. Moreover, our results highlight the added screening value of combining heterogeneous physiological markers for adolescent depression detection, extending beyond the limitations of unimodal approaches. While prior machine learning models have reported classification accuracies as high as 88.6% (28), these typically relied on static, resting-state data with limited real-world applicability. By contrast, our VR-based protocol captures physiological reactivity during interactive, emotionally salient tasks, thereby enhancing ecological validity and reflecting dynamic, task-evoked psychopathology. Moreover, the performance of our classification model aligns with recent trends in the use of VR-based diagnostics for other psychiatric conditions, such as schizophrenia (50), suggesting broader applicability of immersive digital tools for mental health evaluation. The integration of VR and physiological monitoring thus represents a meaningful evolution in adolescent depression screening.
4.3 Implications
The results of this study underscore the potential utility of VR-enhanced multimodal assessment as a novel strategy for early identification of adolescent MDD. First, the model’s high classification accuracy (81.7%) supports its feasibility for implementation in school-based screenings or primary care settings, particularly for populations reluctant to disclose symptoms through self-report. Second, the reliance on objective physiological indicators enhances diagnostic reliability and may prove useful for longitudinal monitoring during treatment. Third, the approach may help disambiguate MDD from clinically overlapping disorders such as ADHD by leveraging distinct neurophysiological signatures. Finally, the use of VR represents a significant technological advancement, providing a controlled yet immersive environment that encourages naturalistic behavioral expression while maintaining experimental rigor. This balance between ecological validity and standardization positions the method as a promising adjunct to traditional diagnostic protocols.
4.4 Limitations and future directions
Despite its promising results, this study has several limitations. First, the sample was demographically limited to Chinese adolescents in a specific region. Even though MDD demonstrates high cross-cultural consistency in both core symptoms and DSM-5 diagnostic criteria (25, 30), future studies should include more diverse populations to evaluate cross-cultural validity and increase applicability. Second, the modest sample size (n=115) may increase the risk of overfitting. To further validate the model, it is necessary to obtain independent datasets from various sites and cohorts to confirm robustness across populations and recording conditions. Third, although the SVM model demonstrated strong performance, interpretability remains a concern. Like many machine learning-based methods, the current approach functions as a “black box,” which may hinder clinical acceptance (51). In the future, scientists or researchers can incorporate explainable AI methods such as SHAP or LIME to enhance transparency and improve clinical adoption. In addition, expanding the feature set to include task-based behavioral or cognitive metrics may further improve predictive performance and offer richer insights into depressive symptomatology.
5 Conclusion
This study developed a VR-based multimodal framework combining EEG, HRV, and eye-tracking to identify objective biomarkers of adolescent depression. Key features—such as elevated theta/beta and LF/HF ratios—enabled an SVM classifier to achieve 81.7% accuracy (AUC = 0.921), demonstrating strong diagnostic potential. The integration of immersive environments and physiological signals offers a promising, scalable approach for early depression screening, which also has the potential to be implemented in schools or primary healthcare settings. Future work should improve model interpretability and validate the framework across diverse populations.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statement
The studies involving humans were approved in accordance with the Declaration of Helsinki and approved by Shanghai Pudong New District Medical Ethics Committee (No. pDJW-KY-2022-011GZ-02). The studies were conducted in accordance with the local legislation and institutional requirements. Written informed consent for participation in this study was provided by the participants’ legal guardians/next of kin.
Author contributions
YW: Conceptualization, Investigation, Methodology, Writing – original draft, Writing – review & editing. YQ: Conceptualization, Investigation, Methodology, Project administration, Resources, Writing – review & editing. LW: Formal analysis, Writing – original draft, Writing – review & editing. MG: Writing – original draft. TW: Formal analysis, Writing – original draft. JL: Formal analysis, Writing – original draft. ZW: Data curation, Writing – original draft. XZ: Data curation, Writing – original draft. HZ: Funding acquisition, Supervision, Writing – review & editing. XF: Funding acquisition, Supervision, Writing – review & editing.
Funding
The author(s) declare financial support was received for the research and/or publication of this article. This study was supported by the Medical Discipline Construction program of Shanghai Pudong New Area Health Commission (the Specialty program) (No.: pWZzb2022-09), Tongji University Medicine-X Interdisciplinary Research Initiative (2025-0708-YB-02), and the New Quality Clinical Specialty program of High-end Medical Disciplinary Construction in Shanghai Pudong New Area (Grant No.: 2025-pWXZ-08).
Acknowledgments
We extend our sincere gratitude to the adolescents and their families who participated in this study, as well as the staff at the Mental Health Center of Pudong New District, Shanghai, and Junnan Middle School in Guizhou province for their invaluable support in participant recruitment and data collection.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Generative AI statement
The author(s) declare that no Generative AI was used in the creation of this manuscript.
Any alternative text (alt text) provided alongside figures in this article has been generated by Frontiers with the support of artificial intelligence and reasonable efforts have been made to ensure accuracy, including review by the authors wherever possible. If you identify any issues, please contact us.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Wang C, Tong Y, Tang T, Wang XH, Fang L.L, Wen X, et al. Association between adolescent depression and adult suicidal behavior: A systematic review and meta-analysis. Asian J Psychiatry. (2024) 100:104185. doi: 10.1016/j.ajp.2024.104185
2. Malhi GS and Mann JJ. Depression. Lancet. (2018) 392:2299–312. doi: 10.1016/s0140-6736(18)31948-2
3. Huang Y, Wang Y, Wang H, Liu ZR, Yu X, Yan J, et al. Prevalence of mental disorders in China: a cross-sectional epidemiological study. Lancet Psychiatry. (2019) 6:211–24. doi: 10.1016/S2215-0366(18)30511-X
4. Ettman CK, Abdalla SM, Cohen GH, Sampson L, Vivier PM, and Galea S. Prevalence of depression symptoms in US adults before and during the COVID-19 pandemic. JAMA Netw Open. (2020) 3:e2019686. doi: 10.1001/jamanetworkopen.2020.19686
5. Miller L and Campo JV. Depression in adolescents. Ropper AH Ed New Engl J Med. (2021) 385:445–9. doi: 10.1056/nejmra2033475
6. Zhou J, Liu Y, Ma J, Feng ZZ, Hu J, Hu J, et al. Prevalence of depressive symptoms among children and adolescents in China: a systematic review and meta-analysis. Child Adolesc Psychiatry Ment Health. (2024) 18(150). doi: 10.1186/s13034-024-00841-w
7. Sampson M. Diagnosis, misdiagnosis, and becoming better: An investigation into epistemic injustice and mental health. repository.uwtsd.ac.uk (2021). Available online at: https://repository.uwtsd.ac.uk/id/eprint/1849/ (Accessed May 1, 2025).
8. Husain W, Pandi-Perumal SR, and Jahrami H. Artificial intelligence-assisted adjunct therapy: advocating the need for valid and reliable AI tools in mental healthcare. ALPHA Psychiatry. (2024) 25:667–8. doi: 10.5152/alphapsychiatry.2024.241827
9. Kaiser AK, Gnjezda MT, Knasmüller S, and Aichhorn W. Electroencephalogram alpha asymmetry in patients with depressive disorders: current perspectives. Neuropsychiatr Dis Treat. (2018) 14:1493–504. doi: 10.2147/ndt.s137776
10. Aslan IH and Baldwin DS. Ruminations and their correlates in depressive episodes: Between-group comparison in patients with unipolar or bipolar depression and healthy controls. J Affect Disord. (2021) 280:1–6. doi: 10.1016/j.jad.2020.10.064
11. Cont C, Stute N, Galli A, Schulte C, and Wojtecki L. Eye tracking as biomarker compared to neuropsychological tests in parkinson syndromes: an exploratory pilot study before and after deep transcranial magnetic stimulation. Brain Sci. (2025) 15:180. doi: 10.3390/brainsci15020180
12. Reznik SJ and Allen JJB. Frontal asymmetry as a mediator and moderator of emotion: An updated review. Psychophysiology. (2017) 55:e12965. doi: 10.1111/psyp.12965
13. Lacey MF and Gable PA. Frontal Asymmetry in an approach–avoidance conflict paradigm. Psychophysiology. (2021) 58(5):e13780. doi: 10.1111/psyp.13780
14. Sacks DD, Schwenn PE, McLoughlin LT, Lagopoulos J, and Hermens DF. Phase–amplitude coupling, mental health and cognition: implications for adolescence. Front Hum Neurosci. (2021) 15:622313. doi: 10.3389/fnhum.2021.622313
15. Noda Y, Zomorrodi R, Saeki T, Rajji TK, Blumberger DM, Daskalakis ZJ, et al. Resting-state EEG gamma power and theta–gamma coupling enhancement following high-frequency left dorsolateral prefrontal rTMS in patients with depression. Clin Neurophysiol. (2017) 128:424–32. doi: 10.1016/j.clinph.2016.12.023
16. Jia Z and Li S. Risk of cardiovascular disease mortality in relation to depression and 14 common risk factors. Int J Gen Med. (2021) 14:441–9. doi: 10.2147/ijgm.s292140
17. Suslow T, Hußlack A, Kersting A, and Bodenschatz CM. Attentional biases to emotional information in clinical depression: A systematic and meta-analytic review of eye tracking findings. J Affect Disord. (2020) 274:632–42. doi: 10.1016/j.jad.2020.05.140
18. Bodenschatz CM, Skopinceva M, Ruß T, and Suslow T. Attentional bias and childhood maltreatment in clinical depression - An eye-tracking study. J Psychiatr Res. (2019) 112:83–8. doi: 10.1016/j.jpsychires.2019.02.025
19. Clementz BA, Sweeney JA, Hamm JP, Ivleva EI, Ethridge LE, Pearlson GD, et al. Identification of distinct psychosis biotypes using brain-based biomarkers. Am J Psychiatry. (2016) 173:373–84. doi: 10.1176/appi.ajp.2015.14091200
20. Bodenschatz CM, Skopinceva M, Kersting A, Quirin M, and Suslow T. Implicit negative affect predicts attention to sad faces beyond self-reported depressive symptoms in healthy individuals: An eye-tracking study. Psychiatry Res. (2018) 265:48–54. doi: 10.1016/j.psychres.2018.04.007
21. Cattarinussi G, Delvecchio G, Sambataro F, and Brambilla P. The effect of polygenic risk scores for major depressive disorder, bipolar disorder and schizophrenia on morphological brain measures: A systematic review of the evidence. J Affect Disord. (2022) 310:213–22. doi: 10.1016/j.jad.2022.05.007
22. Petrakis A, Koumakis L, Kazantzaki E, and Kondylakis H. Transforming healthcare: A comprehensive review of augmented and virtual reality interventions. Sensors. (2025) 25:3748. doi: 10.3390/s25123748
23. Li L, Yu F, Shi D, Shi JP, Tian ZJ, Yang JQ, et al. Application of virtual reality technology in clinical medicine. Am J Trans Res. (2017) 9:3867. doi: PMC5622235
24. Wiebe A, Kannen K, Li M, Aslan B, Anders D, Selaskowski B, et al. Multimodal virtual reality-based assessment of adult ADHD: A feasibility study in healthy subjects. Assessment. (2022) 30(5):1435–53. doi: 10.1177/10731911221089193
25. American Psychiatric Association, DSM Task Force. Diagnostic and statistical manual of mental disorders: DSM-5TM. 5th ed. psycnet.apa.org (2022). Available online at: https://psycnet.apa.org/record/2013-14907-000 (Accessed May 1, 2025).
26. Faul F, Erdfelder E, Buchner A, and Lang AG. (2009) Statistical power analyses using G*Power 3.1: tests for correlation and regression analyses. Behav Res Methods. 41(4):1149–60 doi: 10.3758/brm.41.4.1149
27. Awad M and Fraihat S. Recursive feature elimination with cross-validation with decision tree: feature selection method for machine learning-based intrusion detection systems. J Sens Actuator Netw. (2023) 12:67. doi: 10.3390/jsan12050067
28. Silva de RD C, Albuquerque SGC, Muniz de A V, Filho PPR, Ribeiro S, Pinheiro PR, et al. Reducing the schizophrenia stigma: A new approach based on augmented reality. Comput Intell Neurosci. (2017) 2017:1–10. doi: 10.1155/2017/2721846
29. Wiebe A, Kannen K, Selaskowski B, Mehren A, Thöne AK, Pramme L, et al. Virtual reality in the diagnostic and therapy for mental disorders: A systematic review. Clin Psychol Rev. (2022) 98:102213. doi: 10.1016/j.cpr.2022.102213
30. Ye Q, Liu Y, Zhang S, Ni K, Fu SF, Dou WJ, et al. Cross-cultural adaptation and clinical application of the Perth Empathy Scale. J Clin Psychol. (2024) 80(7):1473–89. doi: 10.1002/jclp.23643
31. Doliński D, Grzyb T, Folwarczny M, Grzybała P, Krzyszycha K, Martynowska K, et al. Would you deliver an electric shock in 2015? Obedience in the experimental paradigm developed by stanley milgram in the 50 years following the original studies. Soc psychol Pers Sci. (2017) 8:927–33. doi: 10.1177/1948550617693060
32. Milgram S. Behavioral study of obedience. J Abnormal Soc Psychol. (1963) 67:371–8. doi: 10.1037/h0040525
33. Tversky A and Kahneman D. Advances in prospect theory: Cumulative representation of uncertainty. J Risk Uncertain. (1992) 5:297–323. doi: 10.1007/BF00122574
34. West R, Michie S, Rubin GJ, and Amlôt R. Applying principles of behaviour change to reduce SARS-CoV-2 transmission. Nat Hum Behav. (2020) 4:451–9. doi: 10.1038/s41562-020-0887-9
35. Radloff LS. The CES-D scale: A self-report depression scale for research in the general population. Appl Psychol Meas (1977). Available online at: https://nida.nih.gov/sites/default/files/Mental_HealthV.pdf. (Accessed May 1, 2025).
36. GitHub. A-Frame - A Web framework for building virtual reality experiences. github.com. (2021). Available online at: https://github.com/aframevr/aframe (Accessed May 1, 2025).
37. Postman. Postman. Postman.com (2025). Available online at: https://www.postman.com/postman/anthropic-apis/documentation/dhus72s/claude-api.
38. IBM. What are large language models (LLMs)? Ibm.com (2023). Available online at: https://www.ibm.com/think/topics/large-language-models (Accessed May 1, 2025).
39. ScienceDirect. Discrete Wavelet Transform - an overview | ScienceDirect Topics. www.sciencedirect.com (2020). Available online at: https://www.sciencedirect.com/topics/mathematics/discrete-wavelet-transform (Accessed May 1, 2025).
40. Social Science Statistics. Mann-Whitney U Test Calculator. Socscistatistics.com (2024). Available online at: https://www.socscistatistics.com/tests/mannwhitney/.
41. Maher JM, Markey JC, and Ebert-May D. The other half of the story: effect size analysis in quantitative research. CBE—Life Sci Educ. (2013) 12:345–51. doi: 10.1187/cbe.13-04-0082
42. IBM. Support Vector Machine. ibm.com. (2023). Available online at: https://www.ibm.com/think/topics/support-vector-machine (Accessed May 1, 2025).
43. Kenton W. Bonferroni Test. investopedia.com. (2021). Available online at: https://www.investopedia.com/terms/b/bonferroni-test.asp (Accessed May 1, 2025).
44. Banerjee D. Speech Based Machine Learning Models for Emotional State Recognition and PTSD Detection - ProQuest. Proquest.com (2017). Available online at: https://www.proquest.com/docview/2054023094?pq-origsite=gscholar&fromopenview=true&sourcetype=Dissertations%20&%20Theses (Accessed May 1, 2025).
45. Chen Y, Wang Z, Yi S, and Li J. The diagnostic performance of machine learning based on resting-state functional magnetic resonance imaging data for major depressive disorders: a systematic review and meta-analysis. Front Neurosci. (2023) 17:2023.1174080. doi: 10.3389/fnins.2023.1174080
46. Zheng Z, Liang L, Luo X, Chen J, Lin MR, Wang GJ, et al. Diagnosing and tracking depression based on eye movement in response to virtual reality. Front Psychiatry. (2024) 15:1280935. doi: 10.3389/fpsyt.2024.1280935
47. Liu XC, Chen M, Ji YJ, Chen HB, Lin YQ, Xiao Z, et al. Identifying depression with mixed features: the potential value of eye-tracking features. Front Neurol. (2025) 16:1555630. doi: 10.3389/fneur.2025.1555630
48. Ding X, Yue X, Zheng R, Bi C, Li D, and Yao G. Classifying major depression patients and healthy controls using EEG, eye tracking and galvanic skin response data. J Affect Disord. (2019) 251:156–61. doi: 10.1016/j.jad.2019.03.058
49. Liu X, Xu Z, Li W, Zhou Z, and Jia X. Editorial: Clinical application of machine learning methods in psychiatric disorders. Front Psychiatry. (2023) 14:2023.1209615. doi: 10.3389/fpsyt.2023.1209615
50. GeeksforGeeks. Why Deep Learning is Black Box. geeksforgeeks.org (2024). Available online at: https://www.geeksforgeeks.org/why-deep-learning-is-black-box/ (Accessed May 1, 2025).
Keywords: virtual reality, multimodal sensing, adolescent depression, EEG, eye tracking, heart rate variability, machine learning, support vector machine
Citation: Wu Y, Qiao Y, Wu L, Gao M, Wong TY, Li J, Wang Z, Zhao X, Zhao H and Fan X (2025) A virtual reality-based multimodal framework for adolescent depression screening using machine learning. Front. Psychiatry 16:1655554. doi: 10.3389/fpsyt.2025.1655554
Received: 28 June 2025; Accepted: 20 August 2025;
Published: 17 September 2025.
Edited by:
Francesco Monaco, Azienda Sanitaria Locale Salerno, ItalyReviewed by:
Azeemuddin Syed, Penn State University Erie, United StatesStefania Landi, ASL Salerno, Italy
Copyright © 2025 Wu, Qiao, Wu, Gao, Wong, Li, Wang, Zhao, Zhao and Fan. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Hui Zhao, cGR4cWhkc3F3c0AxMjYuY29t; Xiwang Fan, ZmFueGl3YW5nMjAyMEAxNjMuY29t
†These authors have contributed equally to this work
‡ORCID: Yizhen Wu, orcid.org/0009-0001-5007-0336
Yuling Qiao, orcid.org/0009-0004-2522-1085
Hui Zhao, orcid.org/0009-0007-4100-0655
Xiwang Fan, orcid.org/0000-0003-4180-0496