 Rui Qiu
Rui Qiu Zhihua Guo
Zhihua Guo Xianyang Wang
Xianyang Wang Yushan Li
Yushan Li Mengze Li
Mengze Li Zhu Xia
Zhu Xia- Department of Military Medical Psychology, Air Force Medical University, Xi ‘an, China
Background: Mobile phone addiction represents a widespread concern associated with negative health consequences, influenced by various protective and risk factors. Nonetheless, two significant gaps persist in the literature: the examination of gender differences in the interplay among mobile phone addiction symptoms, and the analysis of dimension-level associations between mobile phone addiction and its determinants. These gaps motivated the current investigation. This study aimed to elucidate the interconnections among symptoms of mobile phone addiction through the development of a relational network and the identification of key central symptoms. Furthermore, it investigated the influence of fundamental psychosocial factors on mobile phone addiction, with a specific focus on gender-related differences.
Methods: The sample comprised 1,684 adults. Participants completed validated self-report instruments, including the Mobile Phone Addiction Tendency Scale (MPATS) and the Connor-Davidson Resilience Scale (CD-RISC), to assess mobile phone addiction and relevant psychosocial factors. Network analysis techniques were employed to construct two models: a standalone symptom network of mobile phone addiction and an integrated network incorporating addiction symptoms and influencing psychosocial factors. Additionally, gender-stratified analyses were conducted to compare network structures and centrality metrics between male and female groups.
Results: Across both genders, the most robust associations within the mobile phone addiction symptom network were confined to items within the same MPATS dimension. The strongest edge common to both networks connected Item 4 (“I would feel bad if I did not use my phone for a long time”) and Item 6 (“I would feel lonely without my mobile phone”), both reflecting withdrawal symptoms. The second strongest association linked Item 7 (“I feel more confident when I communicate with others using my phone”) and Item 16 (“I feel more comfortable when I communicate with others via cell phone”), which pertain to the social comfort dimension. Regarding central symptoms, Item 15 (“In class/at work, I often take the initiative to focus on my mobile phone, which affects the lesson/work”) emerged as the central node among males, whereas Item 6 (“I would feel lonely without my mobile phone”) was central among females. Within the integrated network, the strength dimension of psychological resilience served as the central node for both genders. Additionally, in the male sample, the positive reappraisal dimension of cognitive emotion regulation strategies was identified as the central node, whereas the catastrophizing dimension emerged as the central node in the female sample.
Conclusion: The results demonstrate significant gender disparities within both the isolated mobile phone addiction symptom network and the comprehensive network that includes psychosocial variables. Strong connections were observed particularly within the withdrawal and social comfort domains, accompanied by gender-specific central symptoms—namely, task-interfering phone use among males and feelings of loneliness among females. These findings contribute to a deeper comprehension of the psychopathological processes associated with mobile phone addiction. Moreover, they identify specific focal points for the formulation of gender-responsive intervention strategies designed to reduce mobile phone addiction.
1 Introduction
Due to the progress and development of science and society, smartphones, which facilitate communication, entertainment, education, and other functions, play an increasingly important role in people’s lives (1). However, as smartphones become more widely used, frequently used, and used for longer periods, the emerging smartphone use habits can increase the risk of mobile phone addiction; accordingly, many people now exhibit mobile phone addiction, which seriously affects their work and lives and poses tremendous societal challenges (2). Mobile phone addicts usually exhibit signs of relapse, withdrawal symptoms, salience, and impulsivity, which take the form of impaired social functioning due to their uncontrollable overuse of smartphones (3).
With the growing concern surrounding mobile phone addiction, researchers have extensively examined the associated risk factors and consequences, developing various theoretical frameworks to elucidate the determinants of mobile phone addiction from perspectives such as psychological needs and external pressures. Notably, among these frameworks, the Interaction of Person-Affect-Cognition-Execution (I-PACE) model has garnered significant attention and validation within the academic community.
The I-PACE model integrates multiple factors that influence mobile phone addiction and can account for the causes of mobile phone addiction effectively (4). On this basis, the I-PACE model is employed in this study, which incorporates individual psychological resilience (5), general future time perspective (6), and the need for uniqueness (7) as personal characteristic factors as well as emotion regulation (8) as an affective state factor, cognitive emotion regulation strategies (9) as a cognitive ability factor, and effortful control (10) and mind wandering as executive function factors. The aim of this study is to incorporate the factors influencing mobile phone addiction into this model in a more comprehensive way.
Psychological resilience is defined as the capacity to sustain or restore psychological well-being in the face of adversity (5). Psychological resilience is defined as the capacity to sustain or restore psychological well-being in the face of adversity. Consequently, these individuals are more likely to preserve psychological health during challenging circumstances and exhibit a decreased propensity for violent behavior, substance addiction, and other maladaptive behaviors (11–13).
For instance, when confronted with academic setbacks, resilient individuals are more likely to modify their study plans instead of engaging in prolonged social media use, thereby mitigating the likelihood of developing addictive mobile phone behaviors.
General future time perspective denotes an individual’s overarching psychological capacity to anticipate, conceptualize, and shape the future, which is primarily manifested through cognitive, affective, and behavioral orientations toward self-development (6); This perspective serves to mitigate mobile phone addiction by facilitating the prioritization of long-term goals (14, 15). Individuals possessing a strong future time perspective are inclined to perceive excessive mobile phone use as an impediment to the attainment of long-term objectives, such as career progression or academic success, and consequently engage in proactive regulation of non-essential phone activities, for instance, refraining from gaming during work hours. Such regulation diminishes the incidence of impulsive or compulsive phone use, thereby reducing the risk of addiction (16).
The need for uniqueness represents an inherent psychological drive motivating individuals to seek differentiation from others, a fundamentally adaptive trait when manifested in moderation, such as through personalized hobbies or values that reinforce self-identity. However, when this need becomes excessive, smartphones serve as an accessible and low-cost platform to fulfill intensified desires for distinctiveness. Individuals may engage in oversharing carefully curated “unique” life experiences on social media, utilize specialized applications to distinguish themselves from peers, or cultivate a distinctive online persona through compulsive interactions with their devices. This dependence on smartphones to validate uniqueness initiates a self-reinforcing cycle: increased device usage aimed at achieving distinctiveness heightens reliance on online feedback to affirm one’s sense of individuality, which in turn perpetuates compulsive use and ultimately contributes to mobile phone addiction (7).
Emotion regulation and cognitive emotion regulation strategies constitute interconnected facets of adaptive psychological functioning; however, impairments in these processes contribute to mobile phone addiction via distinct pathways. Emotion regulation refers to the capacity to modulate emotional states through deliberate strategies, such as reframing situational appraisals, to align with environmental demands. Effective emotion regulation reduces negative affective states, including anxiety and loneliness, without resorting to external distractions (8).
Cognitive emotion regulation strategies, specifically the mental processes employed to interpret and manage emotional information, further refine this capacity. Adaptive strategies, such as positive reappraisal and refocusing on planning, promote psychological well-being and prosocial development, thereby decreasing the propensity to use smartphones as an escape from distress. Conversely, maladaptive strategies, including rumination and catastrophizing, exacerbate negative emotions and drive individuals to rely on smartphones as a rapid means of alleviating emotional discomfort, reinforcing addictive behaviors over time (9).
Effortful control, a fundamental aspect of self-regulation, denotes the ability to inhibit dominant impulsive responses and engage in goal-directed behaviors, such as resisting the urge to check one’s phone during work to maintain task prioritization. This capacity is closely associated with individual adaptability; those exhibiting strong effortful control demonstrate enhanced adaptive functioning by effectively managing stressors and sustaining focus without dependence on smartphones. In contrast, deficient effortful control compromises adaptability by favoring immediate gratification, such as responding to phone notifications, over long-term objectives, resulting in frequent impulsive phone use. Over time, this impulsivity evolves into compulsive behavior, thereby increasing the risk of mobile phone addiction (10).
Mind wandering, defined as the involuntary diversion of attention toward unrelated thoughts, imaginative scenarios, or past experiences during periods of idleness or task engagement, contributes to mobile phone addiction by undermining attentional control (17).
Frequent episodes of mind wandering impair sustained concentration on ongoing activities, such as reading or working, creating attentional gaps that individuals often fill with unplanned phone use, for example, automatically reaching for their device when their mind drifts. Repeated engagement in this compensatory “attention-filling” phone use gradually consolidates into habitual and eventually addictive behavioral patterns (18). Building upon the aforementioned mechanisms, the current study posits that protective factors—such as resilience, a general future time perspective, emotion regulation, adaptive cognitive emotion regulation strategies, and effortful control—will be inversely associated with mobile phone addiction. Conversely, risk factors—including an excessive need for uniqueness and frequent mind wandering—are expected to demonstrate positive associations with mobile phone addiction. Furthermore, maladaptive cognitive emotion regulation strategies, as a subset of cognitive emotion regulation, are hypothesized to be positively correlated with mobile phone addiction, reflecting their contributory role in exacerbating distress-driven mobile phone use. Gender influences mobile phone dependency and preferences regarding internet usage, in which context men tend to view mobile phones as tool-like devices, while women use mobile phones as a medium to develop and maintain social contacts (19). Men are more proactive with regard to seeking a sense of power and fulfilling their sexual fantasies, whereas women prefer to remain anonymous online, thereby concealing their true identities and using the internet to seek intimate friendships and comfort (20). Mok and colleagues employed latent class analysis techniques in their study, which revealed that female college students are more prone to exhibit smartphone addiction than are male college students; furthermore, as dependency on smartphones increases, the individual’s anxiety index and neurotic traits also increase (21).
Improper mobile phone use can give rise to a variety of physiological and psychological discomforts in individuals, which can be divided into four categories: negative reactions on a physiological or psychological level when the individual is not engaged in mobile activities, the central state of mind and behavior associated with mobile phone use, the role of mobile phone usage in interpersonal communication, and a series of negative emotional changes resulting from mobile phones (22). These dimensions constitute the core indicators of and factors associated with mobile phone addiction disorder. The construction of a mobile phone addiction network model can also expand the extant research on issues related to addiction.
The studies referenced above demonstrated that the problem of addiction is not caused by a single factor but rather involves complex interactions among brain physiology, behavioral symptoms, the proximal environment, and distal culture (23). As a psychological disorder, mobile phone addiction can be viewed essentially as a complex and variable network system featuring feedback loops among various factors. Individuals are thus integrated into a dynamic self-organizing system, which makes it difficult to address the symptoms of mobile phone addiction disorder (24). Previous researchers have used network theory to study various psychological disorders and have developed corresponding various network analysis models (25). For example, network analysis models have been developed to investigate posttraumatic stress disorder, anxiety disorders, mood disorders, and personality disorders (26). Investigating the issue of mobile phone addiction from a dynamic system perspective can help us construct a complete risk factor model for mobile phone addiction, provide us with a framework for integrating factors at multiple levels, and help us analyze the effects of different factors on mobile phone addiction (27).
This study pursues two primary objectives: firstly, to delineate the interrelationships among symptoms of mobile phone addiction by mapping their connections and identifying the central, driving symptoms; secondly, to investigate the influence of psychosocial factors, namely resilience, cognitive emotion regulation, and effortful control. Additionally, gender-stratified analyses were conducted with two principal aims: to reveal gender-specific connectivity patterns within both the addiction symptom network and the psychosocial factor network, thereby enabling the distinct identification of core driving symptoms and key influences for each gender; and to establish a gender-sensitive empirical basis for the development of targeted interventions. By integrating gender-stratified analyses, this research provides a more nuanced and comprehensive understanding of mobile phone addiction.
2 Methods
2.1 Participants and procedures
The questionnaire used to support this study was created using the Wenjuanxing platform (https://www.wjx.cn/) in March 2023, and the questionnaires were distributed and collected via various social media platforms. A total of 1932 healthy adults participated in this study. After the exclusion of invalid questionnaires, the sample featured 1684 responses in total, including 1383 males and 301 females. Approximately 21.6% of the participants were under 20 years old, and 57.4% of the participants were between the ages of 21 to 30 years. To ensure the quality of the collected questionnaires, we used the following three criteria to exclude invalid questionnaires: ① questionnaires featuring response times of less than 900 s or more than 1800 s; ② responses featuring incorrect answers to the lie detector question;③ questionnaires on which the same option was chosen for more than 90% of the questions included in the same scale. After statistical screening, 1,684 valid samples were retained, for a validity rate of 87.16%. All the data were collected in March 2023. The participants represented 30 provincial administrative regions throughout China. The demographic information of the participants is shown in Table 1.
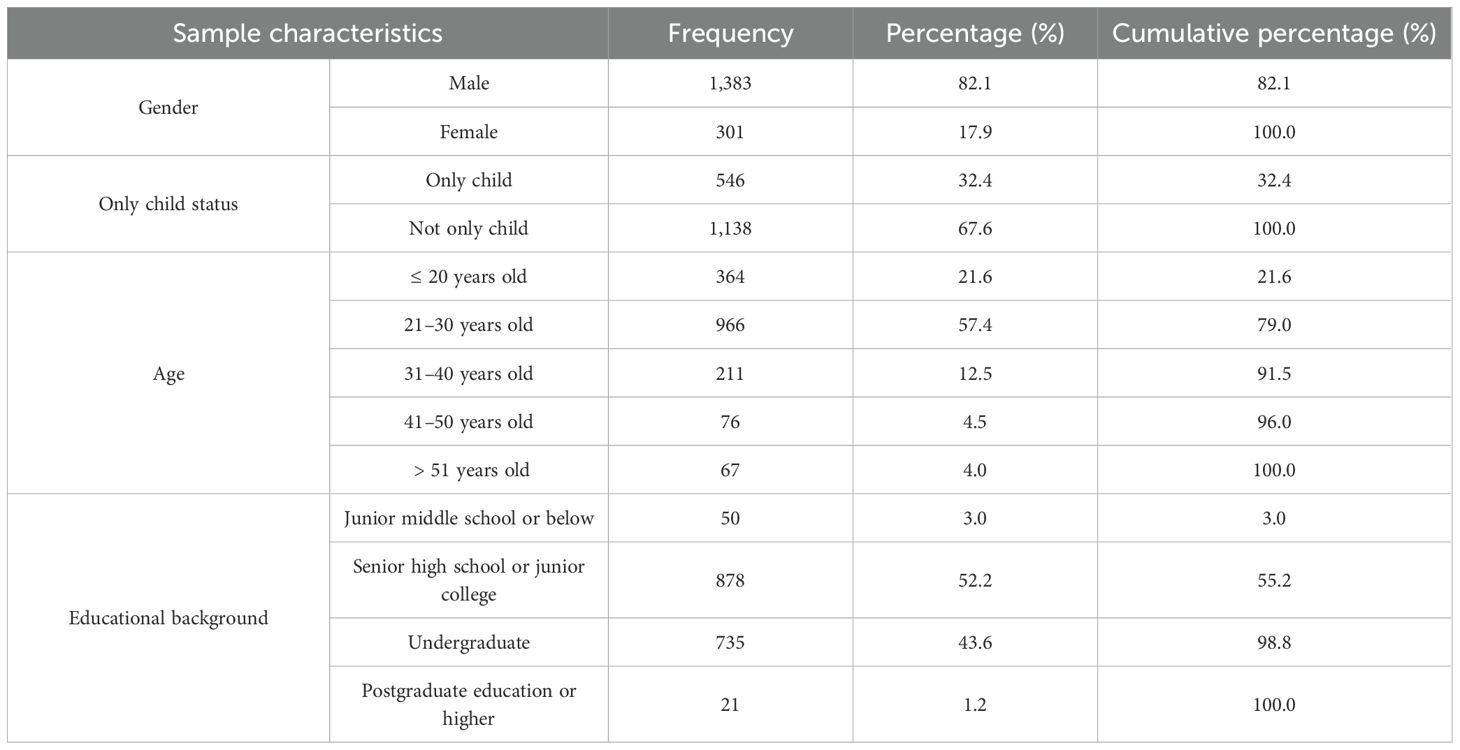
Table 1. Demographic characteristics of the research participants.
2.2 Measures
2.2.1 The mobile phone addiction tendency scale
The MPATS is a self-reported instrument that include 16 items used to assess subjects’ tendencies toward mobile phone addiction (22). The scale features four dimensions, namely, withdrawal symptoms; salience; social comfort and mood changes. All items are scored on a 5-point Likert scale ranging from 1 (completely inconsistent) to 5 (completely consistent). Higher scores indicate higher levels of mobile phone addiction. In the current study, the Cronbach’s alpha coefficients were 0.87 for withdrawal symptoms, 0.85 for salience, 0.82 for social comfort, 0.76 for mood changes and 0.94 for the total scores.
2.2.2 The cognitive emotion regulation questionnaire
The CERQ focuses on both adaptive and maladaptive cognitive strategies, which define an individual’s characteristic approach to the task of managing stress-related events (9). The Cognitive Emotion Regulation Questionnaire (CERQ) used in this study is the Chinese version developed by Zhu Xiongzhao et al. and validated through psychometric testing (28). The adaptive cognitive strategies scale includes five subscales: acceptance, refocus on planning, positive refocusing, positive reappraisal and putting into perspective. The maladaptive cognitive strategies scale includes four subscales: self-blame, blaming others, rumination or focus on thought and catastrophizing. Each subscale consists of 4 items, which are scored on a 5-point scale ranging from 1 (almost never) to 5 (almost always). In the current study, Cronbach’s alpha coefficients ranged from 0.75 (self-blame) to 0.94 (refocus on planning).
2.2.3 The general future time perspective questionnaire
The GFTPQ is a 20-item self-report scale used to measure individuals’ future time perspectives (29). It includes five factors: future efficacy, purposive consciousness, far-reaching goal orientation, future image and behavioral commitment. Each item is scored on a 4-point scale ranging from 1 (completely consistent) to 4 (completely inconsistent). In the current study, the Cronbach’s alpha coefficients ranged from 0.62 (future image) to 0.89 (behavioral commitment).
2.2.4 The emotion regulation questionnaire
The ERQ is a 10-item self-report scale used to measure emotion regulation strategies (8). This questionnaire includes two factors: reappraisal and suppression. Emotion reappraisal is defined as an antecedent-focused strategy in which a person attempts to change how they think about a situation with the goal of changing its emotional impact. Emotion suppression is defined as a response-focused strategy in which a person attempts to inhibit the behavioral expression of their emotions. Each item is scored on a 7-point Likert scale ranging from 1 (strongly disagree) to 7 (strongly agree). Higher scores indicate that emotional regulation strategies are used more frequently. In the present study, the Cronbach’s alpha coefficients were 0.89 for reappraisal and 0.80 for suppression.
2.2.5 The mind-wandering questionnaire
The MWQ is a 21-item self-report measure used to assess the frequency with which individuals engage in mind wandering (30). This questionnaire includes three subscales: spontaneous thinking, attention out of control and overall evaluation. Each item is scored on a 5-point Likert scale ranging from 1 (very rarely) to 5 (always). Higher scores indicate that individuals engage in mind wandering more frequently (22). In the current study, the Cronbach’s alpha coefficient was 0.97 for the total scale.
2.2.6 Early adolescent temperament questionnaire
Effortful control was assessed using the early adolescent temperament questionnaire–revised short form (31). In the Chinese version of this measure of effortful control, 16 items pertaining to activation control, attention and inhibitory control were used to measure effortful control (32). Each item is scored on a 6-point Likert scale ranging from 1 (almost always untrue of you) to 6 (almost always true of you). Higher scores represent higher levels of effortful control. In the current study, the Cronbach’s alpha coefficient for the total scale was 0.71.
2.2.7 The chinese version of the connor-davidson resilience scale
The original version of the CD-RISC includes 25 items (3-factor model) and is used to assess positive psychological qualities that contribute to an individual’s ability to adopt to adversity (33). The Chinese version of the CD-RISC relies on the 3-factor model (6), which includes the dimensions of tenacity, strength and optimism. Each item is scored on a 5-point Likert scale ranging from 1 (not true at all) to 5 (true all the time). Higher scores reflect greater resilience. In the current study, the Cronbach’s alpha coefficients for tenacity, strength, optimism and the total scale were 0.93, 0.94, 0.64 and 0.96, respectively.
2.2.8 The chinese version of the need for uniqueness scale
The original version of the NFU includes 8 items and is used to assess individuals’ positive striving to differentiate themselves from other people (34). The Chinese version of the NFU is a 4-item self-report scale (35). This scale exhibits a single factor structure, and each item scored on a 5-point Likert scale ranging from 1 (not at all/never) to 5 (very much/very often). In the current study, the Cronbach’s alpha coefficient for the total scale was 0.89.
2.3 Statistical analysis
First, descriptive statistics and Pearson correlations were analyzed using SPSS 29.0. Subsequently, network analysis was conducted with the assistance of R 4.2.1 software (36). The analysis conducted for this study involved four steps, each of which is described in the following sections.
2.3.1 Network estimation
The MPATS and the relationship network were estimated using the qgraph package (version 1.9.2) (37). The qgraph package uses the graphical least absolute shrinkage and selection operator (LASSO) function to produce a Gaussian graphical model. The LASSO function can omit spurious edges to produce a network model corresponding to real connections (38). In the network model, each item is represented by a node, and the associations among nodes are known as edges. The more central the nodes are within the network, the more important they are. A shorter edge between two nodes indicates a higher level of closeness between the nodes in question, and the width and color of the edges represent the strength of association and valence between nodes, respectively. Normally, green or blue lines indicate positive associations, while red lines represent negative associations.
2.3.2 Centrality indices
Two node centrality indices – strength and closeness – were calculated (using Z scored values) with the goal of quantifying the structural importance of each node within the network. The strength of a node is calculated as the sum of the weights of all edges that are directly linked to a node. A node featuring higher strength is exhibits stronger direct connections with many nodes. Closeness reflects the inverse weighted sum of the shortest distance from a node to all other connected nodes. A node that features a higher level of closeness may influence other nodes more quickly. However, certain concerns have been expressed regarding the stability of closeness (39). Therefore, the primary index used in this study was strength.
2.3.3 Network comparison
We used the Network Comparison Test (NCT) package to compare the networks obtained using the male and female datasets in terms of invariance of global strength and network structure (40). The NCT is a permutation test in which the difference between the networks associated with two groups is calculated repeatedly for randomly regrouped individuals across three stages. Tests of global strength and network structure were performed, thus generating a p value (in which context p < 0.05 indicates that the network structure differs significantly between the two samples).
2.3.4 Network robustness
We used the bootnet package (version 1.5) to test the robustness of the network structures (40). First, the bootstrapped confidence interval (CI) of each edge was estimated to test the accuracy of the edge weights. Second, the stability of centrality indices was examined by reference to subsamples featuring decreasing sample sizes. The correlation stability (CS) coefficient was also calculated to test the stability of the centrality indices. Finally, bootstrapped difference tests were used to measure the differences in node centralities.
3 Results
3.1 Preliminary analysis
Table 2 presents the means and standard deviations (SDs) for each item and dimension of the MPATS, as well as the gender differences in the dimension and total scores. The significance level α was corrected using the Bonferroni procedure. The mean scores for all dimensions exhibited significances between male and female participants. The overall level of mobile phone addiction observed in the female sample was generally higher than that observed in the male sample.
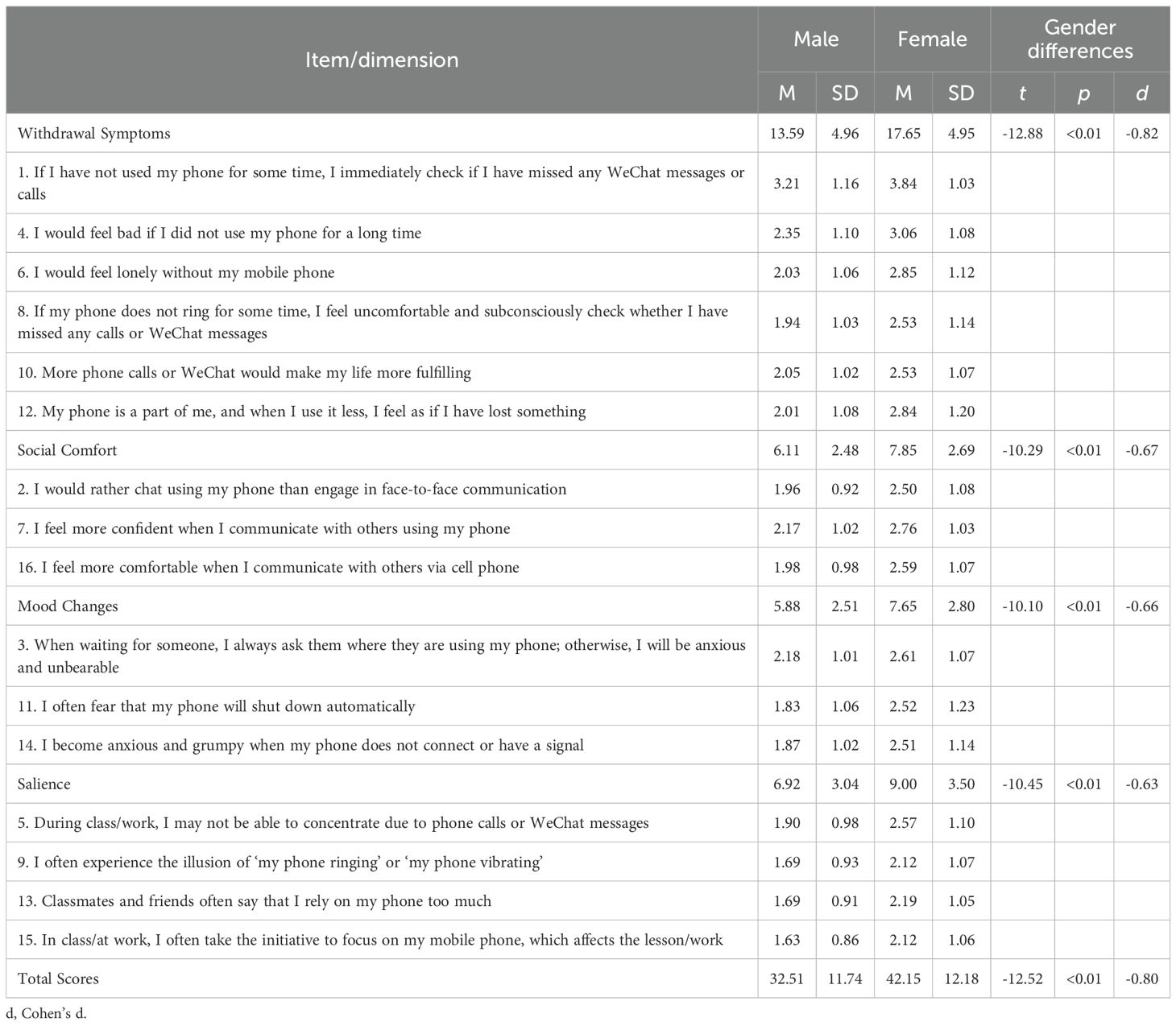
Table 2. Results of a Descriptive analysis of the items included in the MPATS-16.
3.2 Network analysis of mobile phone addiction in the male and female samples
3.2.1 Mobile phone addiction networks
Figure 1 presents the networks pertaining to both the male (Figure 1A) and female (Figure 1B) samples. With regard to the male sample, the edge between item 4 and item 6 (weight = 0.35) was the strongest among all edges and within the withdrawal symptoms dimension. The edge between item 7 and item 16 (weight = 0.32) was the second strongest within the social comfort dimension. Similarly, with regard to the female sample, the edge between item 4 and item 6 (weight = 0.34) was the strongest among all edges and within the withdrawal symptoms dimension. The edge between item 7 and item 16 (weight = 0.31) was the second strongest among all the edges in this context.
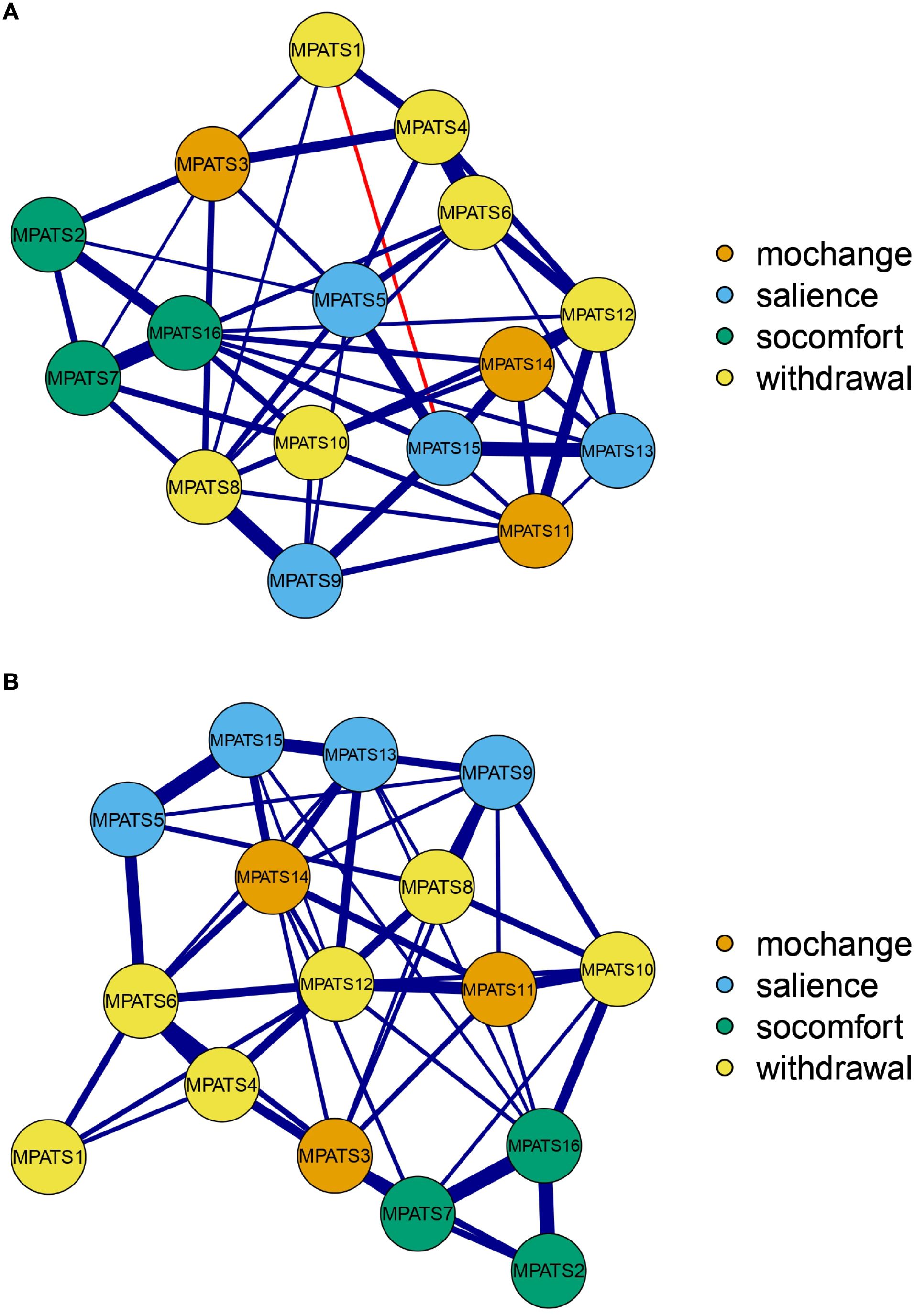
Figure 1. Network structure of mobile phone addiction. (A) Male network. (B) Female network. Note. Mochange, mood changes; socomfort, social comfort; withdrawal, withdrawal symptoms.
3.2.2 Centrality indices
The centrality indices of the nodes contained in the mobile phone addiction networks are shown in Figure 2. With regard to the male sample, item 15 exhibited the highest strength and closeness centrality indices. With respect to the female sample, item 6 exhibited the highest strength and closeness indices.
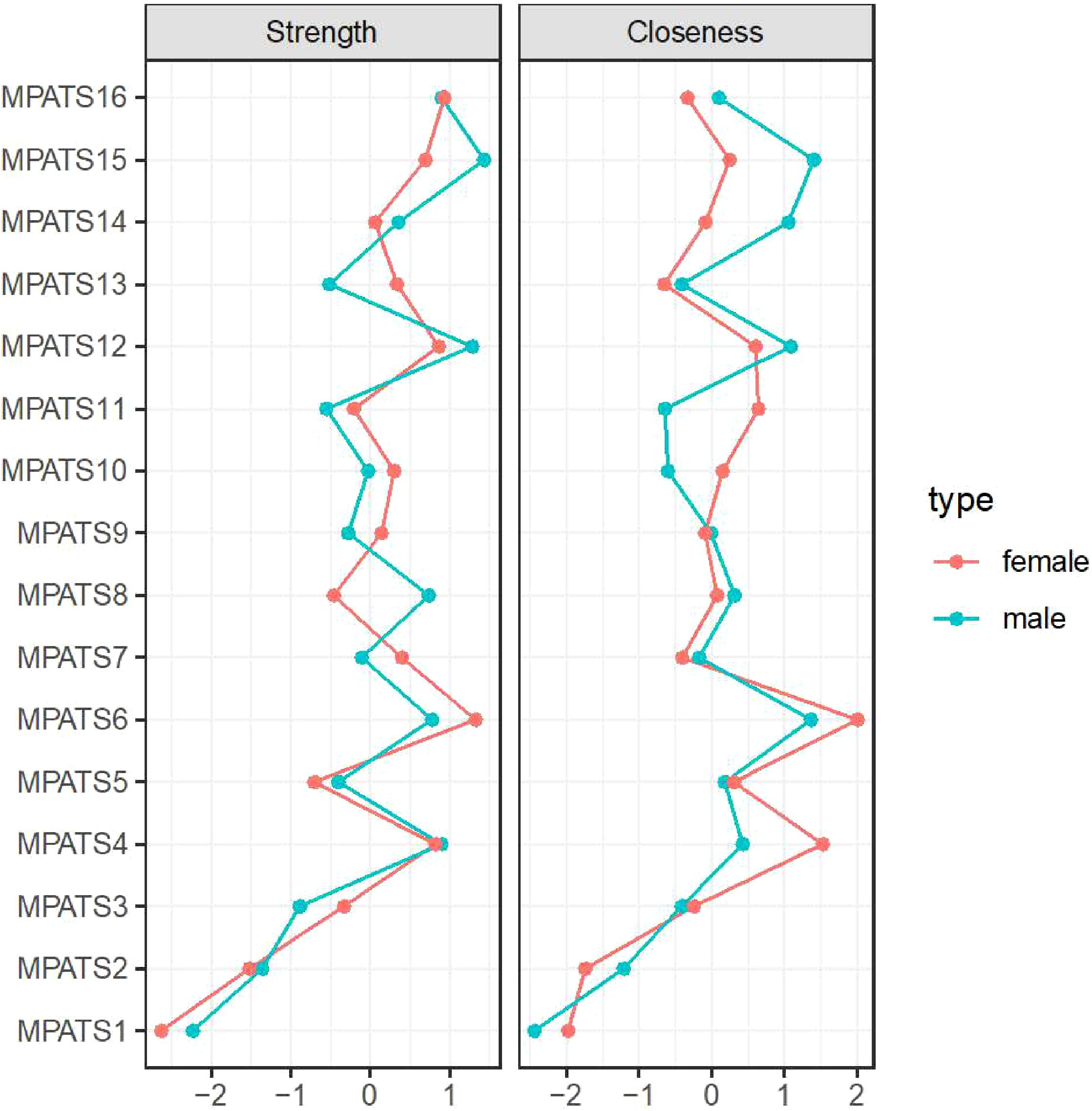
Figure 2. Centrality indices of nodes within the mobile phone addiction networks (z scores).
3.2.3 Statistical network comparison between the two samples
To compare the two networks based on the data collected regarding the two samples, global strength and network structure were compared using the NCT. The results indicated statistically significant differences in global strength (p = 0.02) but not in network structure (p = 0.52). The global strength value for the male sample was 7.419, whereas for the female sample, this value was 7.042, thus indicating that the male subgroup was associated with stronger connections throughout the whole network than was the female subgroup.
3.2.4 Network robustness
The bootstrapped 95% CIs were narrow, thus indicating that the estimated edge weights were accurate and reliable (see Supplementary Figure 1). We estimated a bootstrapped sampling distribution (n = 1000) for the networks pertaining to the male and female samples to test the stability of the inferences made regarding the network structures. Figure 3 presents the stability of the centrality indices associated with the mobile phone addiction networks. With respect to the male and female samples, strength exhibited relatively high stability despite changes in subsample size, while the closeness values exhibited a marginal decrease. In addition, the correlation stability (CS) coefficients were estimated. The CS coefficient should not be less than 0.25 and should preferably be greater than 0.5, which indicates ideal stability. The CS coefficients for strength were good in both networks (0.75 for the male network and 0.671 for the female network). However, the CS coefficient for closeness was not very good for the female network, although it was acceptable (0.672 for the male network, 0.362 for the female network). The bootstrapped difference tests for strength and closeness are shown in Supplementary Figures 2 and 3, respectively.
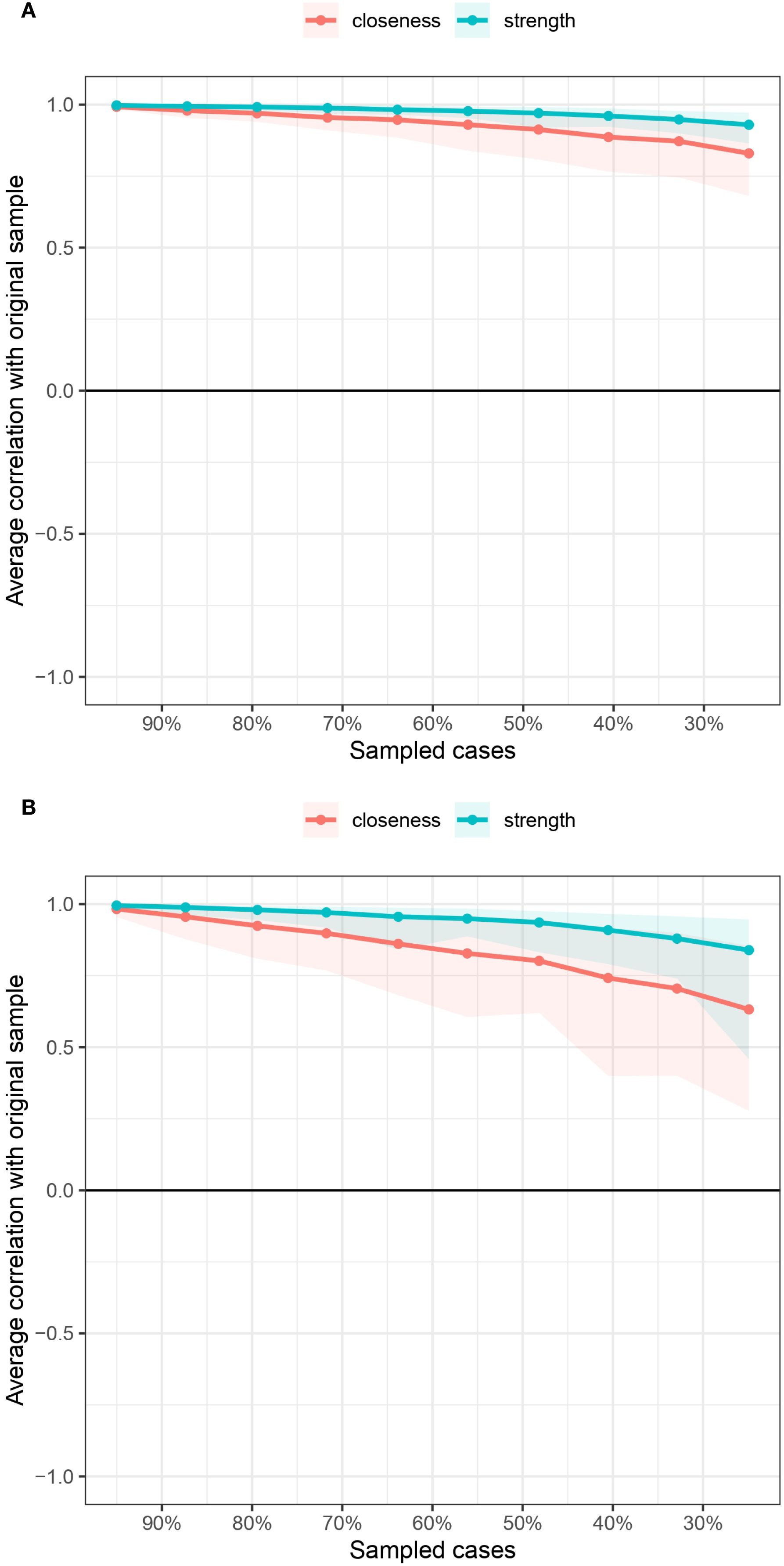
Figure 3. Centrality indices of the mobile phone addiction networks in terms of stability.
3.3 Network analysis of mobile phone addiction and relevant influencing variables
Within network models, each node corresponds to a distinct variable, which represent either a symptom of mobile phone addiction (for example, “feeling lonely without a phone”) or a psychosocial factor (such as “resilience” or “positive reappraisal”). The edges (lines connecting the nodes) indicate the strength of the association between two variables; specifically, thicker edges denote stronger relationships, implying a greater degree of mutual influence between the connected variables. A central node is characterized by having the most robust or numerous connections, functioning as a hub that significantly influences the overall structure of the network.
3.3.1 Network structure
Figure 4 presents the network structures for male (Figure 4A) and female (Figure 4B) participants. A prominent feature observed in both gender-specific networks is the strongest connection within the entire network, linking two components of psychological resilience: “tenacity,” defined as the capacity to persevere through challenging circumstances (e.g., enduring rigorous training), and “strength,” characterized as the ability to grow from adverse experiences (e.g., learning from a lost competition). This association exhibited a high magnitude in males (edge weight = 0.64) and remained substantial in females (edge weight = 0.54). This finding is theoretically coherent, as tenacity and strength function synergistically as a protective dyad that facilitates effective coping mechanisms, thereby explaining their robust interconnection.
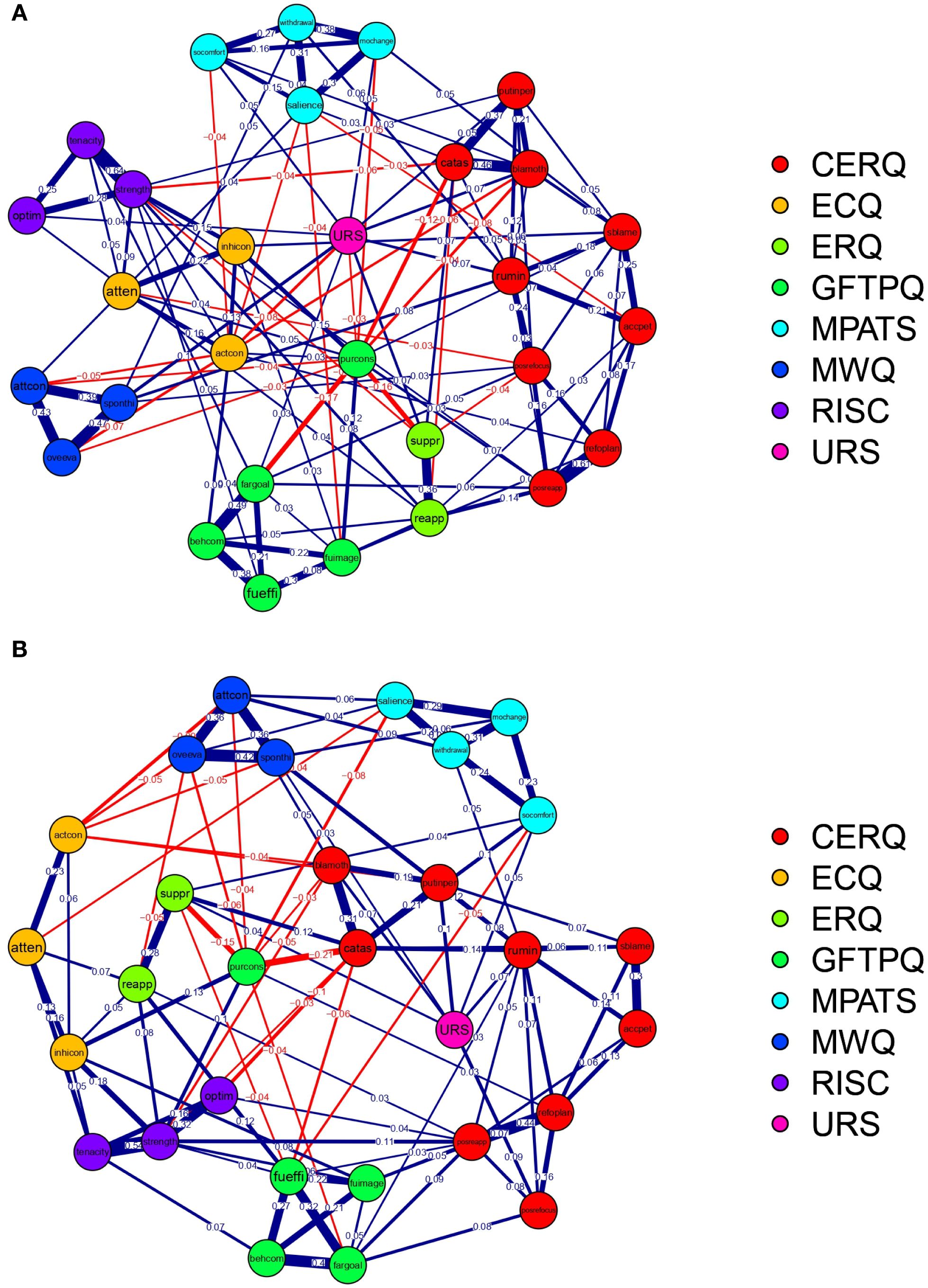
Figure 4. Network structure of mobile phone addiction and relevant influencing variables. (A) Male network; (B) Female network. CERQ, Cognitive Emotion Regulation Questionnaire; ECQ, Effortful Control Questionnaire; ERQ, Emotion Regulation Questionnaire; GFTPQ, General Future Time Perspective Questionnaire; MPATS, Mobile Phone Addiction Tendency Scale; MWQ, Mind Wandering Questionnaire; RISC, Connor-Davidson Resilience Scale; URS, Unique Requirement Scale.
3.3.2 Centrality indices
This study prioritized node strength—defined as the aggregate strength of a node’s connections to other variables—to identify the most influential factors within the network. The centrality indices of nodes within the mobile phone addiction and relevant influencing variables networks (z scores) are shown in Figure 5.
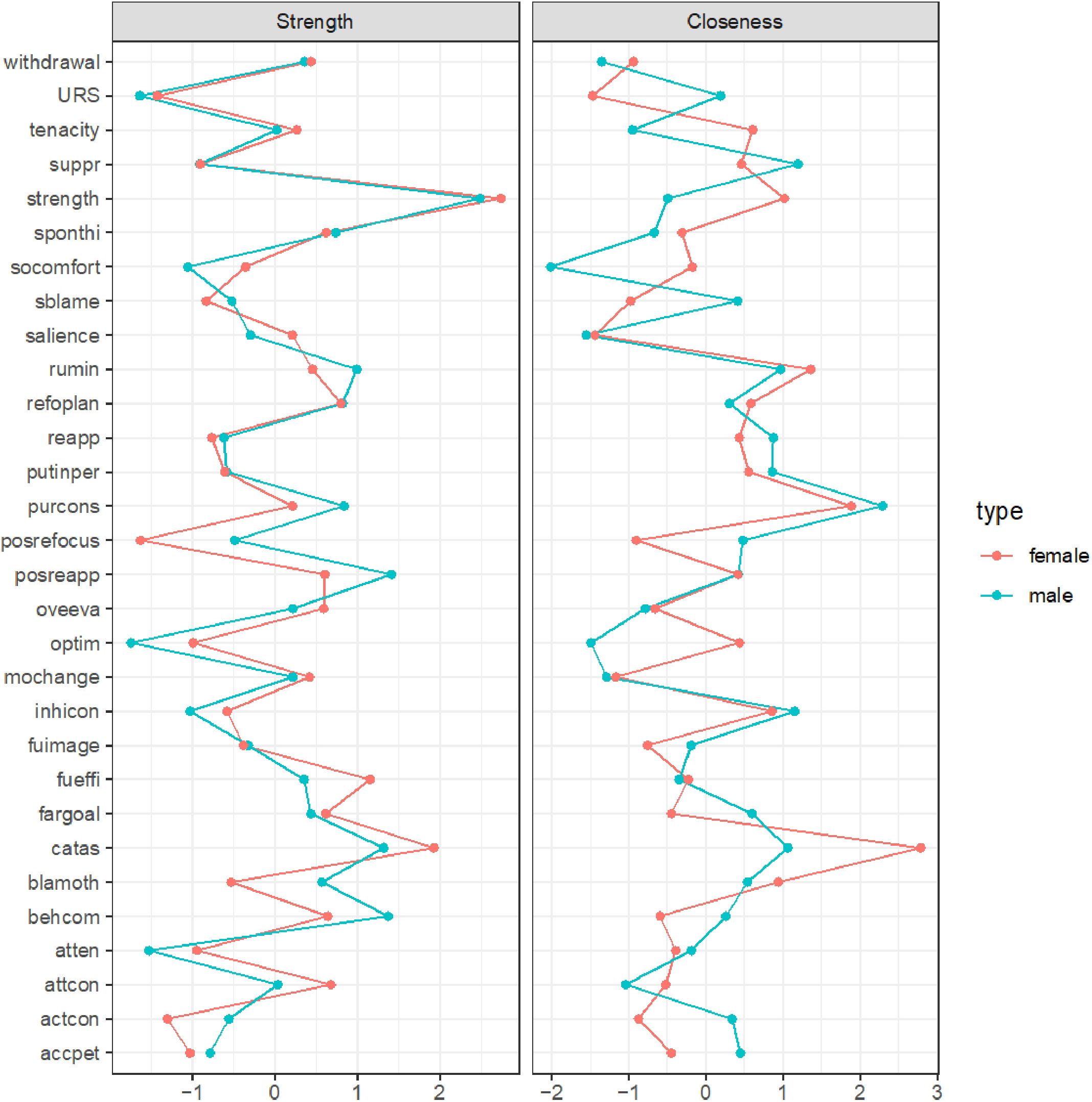
Figure 5. Centrality indices of nodes within the mobile phone addiction and relevant influencing variables networks (z scores).
For both genders, the most central node corresponded to the “strength” dimension of psychological resilience, as assessed by the Connor-Davidson Resilience Scale (CD-RISC). This indicates that the capacity to recover and grow from setbacks constitutes the single most pivotal variable within the network. It exhibits extensive connections to various addiction symptoms and related factors, including the mitigation of withdrawal symptoms and the reduction of impulsive phone use, thereby playing a critical role in the development of addictive behaviors.
Among males exclusively, the second most central node was identified as “positive reappraisal,” a cognitive strategy involving the reframing of negative experiences. This node functions as a protective hub by attenuating the association between stressors—such as training pressure—and problematic phone use.
Conversely, for females, the second most central node was “catastrophizing,” characterized by excessive worry. This node serves as a risk hub by amplifying the relationship between anxiety—such as pre-competition stress—and addictive phone use, thereby complicating efforts to reduce such behaviors.
3.3.3 Statistical network comparison between the two samples
The Network Comparison Test (NCT) results reveal statistically significant differences in global strength (p = 0.01), whereas no significant differences were observed in network structure (p = 0.22). Specifically, the global strength metric for the male cohort was 15.615, compared to 13.607 for the female cohort, suggesting that the male subgroup exhibited stronger overall connectivity within the network relative to the female subgroup.
3.4 Network robustness
The bootstrapped 95% confidence intervals (CIs) were narrow, indicating that the estimated edge weights were both precise and reliable (refer to Supplementary Figure 4). Figure 6 illustrates the stability of centrality indices within the networks. In the male sample, strength demonstrated a relatively high degree of stability despite variations in subsample size, whereas closeness values showed a slight decline. Conversely, in the female sample, both strength and closeness exhibited a pronounced decrease as subsample size changed, with closeness being particularly affected. Furthermore, the correlation stability (CS) coefficient for strength was robust in both networks (0.750 for the male network and 0.672 for the female network). In contrast, the CS coefficient for closeness was acceptable but comparatively lower, especially in the female network (0.595 for the male network and 0.362 for the female network). The results of the bootstrapped difference tests for strength and closeness are presented in Supplementary Figures 5 and 6, respectively.
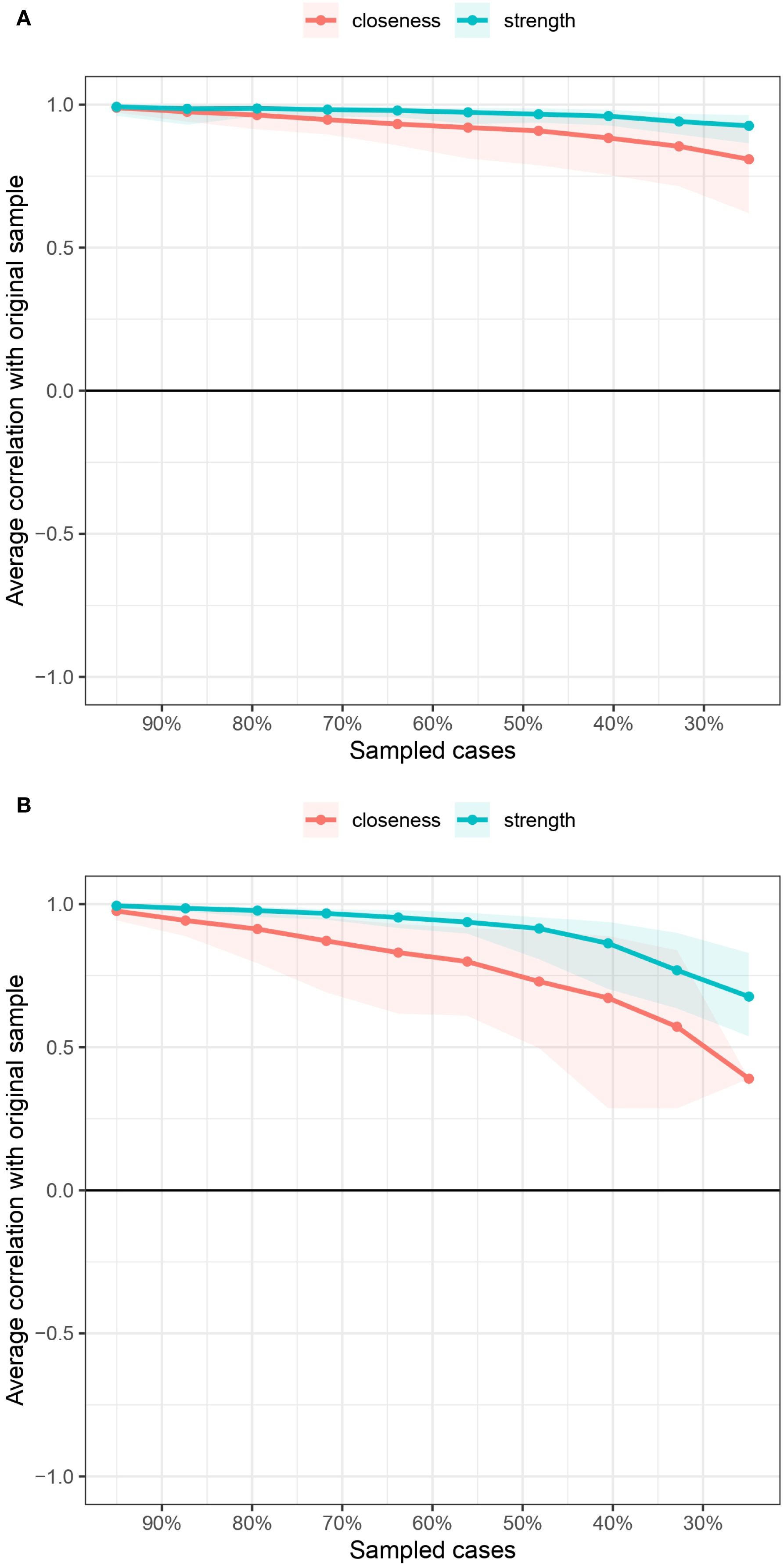
Figure 6. Centrality indices of the mobile phone addiction and relevant influencing variables networks in terms of stability.
4 Discussion
To investigate the specific interrelations among the symptoms of mobile phone addiction and identify risk-increasing and protective factors related to mobile phone addiction, this study examined the network structure of mobile phone addiction as well as the corresponding network structure including relevant influencing factors. The results revealed that the strongest edges were observed within the community in all the networks. This study also identified central nodes that played important roles in these networks. Additionally, we identified gender differences in network characteristics pertaining to both the mobile phone addiction network and the corresponding network including relevant influencing factors.
The results revealed that the specific nodes in the networks of mobile phone addiction were intensively connected in both male and female samples. Item 4 (“I would feel bad if I did not use my phone for a long time”) was closely associated with item 6 (“I would feel lonely without my mobile phone”) for both samples. Both items belong to the withdrawal dimension and reflect negative emotional states arising from restricted phone access, which explains their robust connection. This finding is consistent with previous network studies indicating that the strongest edges often occur within, rather than between, theoretical dimensions (41, 42), underscoring the conceptual and empirical coherence of the withdrawal construct. Similarly, a strong edge was identified between item 7 (“I feel more confident when I communicate with others using my phone”) and item 16 (“I feel more comfortable when I communicate with others via cell phone”), both of which load on the social comfort dimension. This relationship is theoretically plausible, as confidence and comfort in social contexts are closely related psychological experiences (43–45). Our network results empirically support that these two aspects are intertwined in the context of mobile phone use: feeling comfortable in phone-mediated communication may enhance self-confidence, and vice versa, forming a reinforcing cycle that may contribute to the development and maintenance of problematic use patterns. This reciprocity highlights the affective reinforcement mechanisms underlying this dimension of phone addiction.
The networks integrating mobile phone addiction and psychological factors revealed a consistently strong edge between the psychological resilience subcomponents—tenacity and strength—in both genders. This robust connection is conceptually intuitive, as both attributes reflect closely related aspects of resilience: the capacity to persist through challenges (tenacity) and the ability to not only recover from setbacks but also achieve growth and development (strength). This finding aligns with network theory and prior research (35, 46, 47), where the strongest connections typically occur within, not between, conceptual domains. It also resonates with prior work that similarly identified tenacity and strength as strongly connected nodes in a network involving emotion regulation, affect, and resilience (48). What makes this replication noteworthy, however, is its emergence in the specific context of mobile phone addiction. The tight linkage suggests that tenacity and strength function as an interdependent protective unit, potentially enhancing an individual’s capacity to regulate behavior and resist compulsive phone use. The recurrence of this pattern in our study underscores the structural coherence of psychological resilience and highlights its potential role as a buffer in the context of behavioral addiction.
To identify the most influential nodes, we calculated centrality indices, prioritizing the strength metric due to the relatively low stability of closeness estimates—a common finding in network psychometrics (49–51). Interestingly, distinct central nodes emerged across genders in the mobile phone addiction network: for males, the most central symptom was item 15 (“In class/at work, I often take the initiative to focus on my mobile phone, which affects the lesson/work”), whereas for females, it was item 6 (“I would feel lonely without my mobile phone”). The prominence of item 15 among males aligns with prior work highlighting impaired focus as a core feature of mobile phone addiction (52). However, this result contrasts with studies emphasizing loss of control and continued overuse as central (53)—a discrepancy that may stem from cultural or methodological differences in sampling and measurement. For females, the centrality of loneliness without the phone reinforces earlier findings that withdrawal symptoms, particularly affective ones, play a critical role in sustaining problematic smartphone use (52). This divergent pattern invites a meaningful interpretation rooted in potential gender-specific drivers of use. The male network may be primarily driven by a behavioral impulse—a difficulty inhibiting phone use even in situations demanding focus. In contrast, the female network appears centrally organized around an affective state—the fear of isolation and the phone’s role as a social lifeline.
With respect to the network including mobile phone addiction and relevant influencing factors, this study revealed that the strength dimension of psychological resilience was the central node for both males and females. This is a noteworthy finding, as it suggests that strength serves as a common protective factor against addictive phone use across genders. This aligns with previous studies strength buffers against mental health problems such as depression and anxiety (54, 55). This finding is also consistent with a previous network analysis that focused on problematic smartphone use and relevant factors, which reported that resilience was a central node (56). Many studies have demonstrated that psychological resilience has protective effects with regard to mobile phone addiction in either a direct or indirect manner (57–60). What makes this insight particularly compelling is the specific role played by strength. We speculate that strength—as a subcomponent of resilience—equips individuals to adapt to adversity and buffer risk factors of mobile phone addiction such as academic burnout or fear of missing out (57, 61, 62), thereby reducing reliance on phones for emotional regulation or escape. By highlighting strength of resilience specifically, our study clarifies a key malleable target for interventions aimed at fostering healthier digital behaviors.
Additionally, our analysis revealed a striking gender-specific divergence in the cognitive emotion regulation strategies: positive reappraisal served as the central node for males, while catastrophizing was central for females. For males, the prominence of positive reappraisal—a strategy oriented toward reframing negative experiences in constructive terms (63)—aligns with its well-established role as a protective factor for mental health (64–69). Its close functional relationship with resilience (70), which also emerged as highly central in our networks, suggests a reinforcing cycle whereby adaptive coping supports emotional stability and may reduce reliance on mobile devices for mood regulation. In contrast, for females, the centrality of catastrophizing—a pattern of exaggerated negative interpretation—highlights a vulnerability pathway. This finding is consistent with prior work linking catastrophizing to alexithymia and other mental disorders (66, 71–74), particularly in predominantly female samples74. We propose that a tendency toward catastrophizing may lead individuals to seek immediate emotional relief through mobile phone use. Furthermore, this process is self-reinforcing: the individual consequently engages in mobile phone use whenever that individual experiences the negative emotional state induced by catastrophizing, resulting in addictive use. This pattern underscores the value of tailoring interventions to gender-specific cognitive-emotional profiles—promoting cognitive reappraisal skills in males and targeting catastrophic thinking in females.
The NCT analysis revealed a notable gender difference in network structure. Despite females reporting higher average levels of mobile phone addiction, the male network exhibited significantly greater global strength. This suggests that while women may have more symptoms, the interactions between these symptoms are more tightly coupled in men. This finding appears to contrast with earlier studies suggesting that stronger network connectivity is associated with greater symptom severity (40, 75), highlighting a potential gender-specific patterning in how mobile phone addiction manifests. One possible interpretation is that for males, addictive phone use may be driven by a more self-reinforcing and interdependent set of behaviors, whereas for females, higher scores may reflect broader—but less reciprocally activated—patterns of use. Although previous studies have reported no gender differences in global strength in networks involving mobile phone addiction and anxiety or internet addiction and depression (76, 77), our results underscore the need to look beyond mean scores and consider structural differences in psychological networks. Future research should further explore what drives these structural divergences and whether they reflect differing motivational or behavioral pathways into mobile phone addiction across genders.
The findings of this study have important implications. Theoretically, by mapping the interactions among specific symptoms, we move beyond aggregate scores to reveal how certain symptoms may activate others—offering a more dynamic understanding of how mobile phone addiction develops and sustains itself. Clinically, the identification of central nodes provides actionable targets for intervention. In line with network theory (78–80), focusing on these highly influential symptoms or factors may produce cascading benefits across the entire symptom network. Crucially, our findings underscore the necessity of gender-sensitive interventions. For males, strategies should prioritize reducing distraction in goal-directed settings (item 15: “In class/at work…”) while bolstering resilience and the use of positive reappraisal. For females, interventions may be more effective if they address emotional dependence (item 6: “I would feel lonely…”), mitigate tendencies toward catastrophizing, and simultaneously strengthen psychological resilience. These tailored approaches acknowledge that the pathways into—and out of—problematic phone use are gendered, and thus demand nuanced clinical responses.
Despite the contributions of our study, several limitations must be considered. First, the cross-sectional design precludes causal inference; longitudinal or experimental studies are needed to examine how symptom networks evolve or respond to intervention over time. Second, we collected data using self-report scales, which may have been subject to recall bias. Future work would benefit from incorporating objective measures of phone use or behavioral assessments. Third, although we included several key factors, other relevant variables such as personality traits and intolerance of uncertainty were not considered87-88; their inclusion in future network analyses may yield a more comprehensive understanding. Fourth, although central nodes suggest potential intervention targets, their clinical efficacy must be tested through rigorous experimental or longitudinal designs. Fifth, the use of a convenience sampling and moderate sample size may limit generalizability; future replication in larger and more diverse populations is necessary to enhance the robustness and applicability of our findings. Another notable limitation lies in the pronounced gender imbalance in the sample, which is an inherent outcome of the study’s sampling context—all participants were recruited from military academies. As a structural feature of military academies in China, the student and staff population is predominantly male, and our convenience sampling (designed to access individuals with regular mobile phone use within this specific institutional setting) naturally reflected this inherent gender distribution: of the 1,684 participants, 1,383 (82.1%) were male and 301 (17.9%) were female. This imbalance was not a deliberate design choice but a practical constraint tied to the study’s focus on military academy populations. This gender imbalance may impact the robustness and interpretation of our findings in two key ways. First, it weakens the statistical power of gender-stratified network analyses for female participants. While the larger male sample enabled reliable detection of even weak but meaningful associations (e.g., the link between “phone use during military training breaks” and “effortful control”), the smaller female sample may lack sufficient power to capture such subtle connectivity patterns—potentially leading to underestimation of gender-specific mechanisms unique to military academy women (e.g., how the pressure of balancing military training with daily life interacts with addiction symptoms). Second, it limits the generalizability of female-specific results: the small female subsample not only prevents broad inferences to the wider group of military academy women but also rules out extrapolation to civilian female populations, as military academy women may face context-specific stressors (e.g., gendered expectations in military training) that differ from those of civilian women. Future research should employ longitudinal designs and include a wider range of psychological and social variables to move beyond superficial comparisons and truly explain why and for whom these gendered pathways to mobile phone addiction emerge.
5 Conclusion
This research utilized network analysis to systematically investigate the internal interaction patterns among symptoms of mobile phone addiction, as well as the interrelationships at the dimensional level between mobile phone addiction and psychosocial influencing factors. The findings not only support the applicability of the I-PACE model to mobile phone addiction but also highlight resilience, emotion regulation strategies, and effortful control as pivotal nodes within the addiction network. These results further substantiate the model’s focus on dynamic interactions among personal, affective, cognitive, and executive components. Additionally, the study challenges the traditional single-factor causation paradigm of addiction by demonstrating that mobile phone addiction arises from complex reciprocal interactions between symptoms and psychosocial variables. Ultimately, this investigation elucidates the dynamic network structure of mobile phone addiction and its associated factors, offering gender-specific theoretical insights and practical implications for addressing this significant public health issue.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statement
This study was conducted with the approval of the relevant ethics committee at Tangdu Hospital Ethics Committee (No. 202103–129). All procedures were carried out in accordance with ethical standards. All participants provided informed consent prior to their inclusion in the study. The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study. Written informed consent was obtained from the individual(s) for the publication of any potentially identifiable images or data included in this article.
Author contributions
RQ: Investigation, Methodology, Software, Visualization, Writing – original draft, Writing – review & editing. ZG: Data curation, Investigation, Software, Supervision, Validation, Writing – original draft, Writing – review & editing. XW: Conceptualization, Data curation, Investigation, Software, Supervision, Validation, Writing – original draft. YL: Conceptualization, Data curation, Formal Analysis, Methodology, Project administration, Writing – original draft. ML: Conceptualization, Formal Analysis, Methodology, Writing – original draft, Writing – review & editing. XZ: Funding acquisition, Investigation, Resources, Supervision, Validation, Visualization, Writing – original draft, Writing – review & editing.
Funding
The author(s) declare financial support was received for the research and/or publication of this article. The work was supported by the Logistics scientific research project (AKJWS221) and the Doctoral Dissertation Research Fund of Air Force Medical University (2024D10). The support from this project was crucial in enabling the conduct of this research. It provided the necessary resources, including but not limited to research materials, access to relevant data, and partial funding for research activities. There were no potential conflicts of interest associated with the funding source. The authors were able to carry out the research objectively and report the findings without any undue influence. We would like to express our gratitude to the Logistics scientific research project for its support in facilitating this research endeavor.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Generative AI statement
The author(s) declare that no Generative AI was used in the creation of this manuscript.
Any alternative text (alt text) provided alongside figures in this article has been generated by Frontiers with the support of artificial intelligence and reasonable efforts have been made to ensure accuracy, including review by the authors wherever possible. If you identify any issues, please contact us.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpsyt.2025.1665673/full#supplementary-material
References
1. James RJE, Grace D, Mariagabriela D, Edie T, and Lucy H. Understanding the construction of 'behavior' in smartphone addiction: a scoping review. Addict Behav. (2022) 137:107503. doi: 10.1016/j.addbeh.2022.107503
2. Lenamarie P, Franziska M, S BD, J KR, Jürgen M, Jan S, et al. Engaging in physical activity instead of (over)using the smartphone: an experimental investigation of lifestyle interventions to prevent problematic smartphone use and to promote mental health. J Public Health (Oxf). (2024) 32:589–607. doi: 10.1093/pubmed/fdae024
3. Pop-Jordanova N and Loleska S. Neuropsychological correlates of internet addiction. Prilozi (Makedonska akademija na naukite i umetnostite. Oddelenie za medicinski nauki). (2021) 42:17–28. doi: 10.2478/prilozi-2021-0031
4. Brand M, Young KS, Laier C, Wölfling K, and Potenza MN. Integrating psychological and neurobiological considerations regarding the development and maintenance of specific internet-use disorders: an interaction of person-affect-cognition-execution (i-pace) model. Neurosci Biobehav Rev. (2016) 71:252–66. doi: 10.1016/j.neubiorev.2016.08.033
5. Aburn M. What is resilience? An integrative review of the empirical literature. J Adv Nurs. (2016) 72:980–1000. doi: 10.1111/jan.12888
6. Yeung DY, FH H, and R LF. Gender differences in social network characteristics and psychological well-being among hong kong chinese: the role of future time perspective and adherence to renqing. Aging Ment Health. (2007) 11:45–56. doi: 10.1080/13607860600735820
7. Geng L, Yang Y, and Xu Y. To pursue personality or conformity: a study on the impact of face view on consumers’ need for uniqueness. Psychol Mark. (2008) 36(3):188–97. doi: 10.1002/mar.21169
8. Gross JJ and John OP. Individual differences in two emotion regulation processes: implications for affect, relationships, and well-being. J Pers Soc Psychol. (2003) 85:348–62. doi: 10.1037/0022-3514.85.2.348
9. Garnefski N, Legerstee J, Kraaij VV, Kommer T, and Teerds J. Cognitive coping strategies and symptoms of depression and anxiety: a comparison between adolescents and adults. J Adolesc. (2002) 25:603–11. doi: 10.1006/jado.2002.0507
10. Vaughan TJ, Ward JT, Jeff B, and Piquero AR. The general factor of self-control and cost consideration: a critical test of the general theory of crime. Crime Delinq. (2018) 65:475347957. doi: 10.1177/0011128718776213
11. Kelly C. Leveraging longitudinal pre-pandemic data to understand mental health vulnerability and resilience among young people during the early pandemic. Biol Psychiatry Global Open science. (2021) 1:244–5. doi: 10.1016/j.bpsgos.2021.10.005
12. Canale N, Marino C, Griffiths MD, Scacchi L, Monaci MG, and Vieno A. The association between problematic online gaming and perceived stress: the moderating effect of psychological resilience. J Behav Addict. (2019) 8:174–80. doi: 10.1556/2006.8.2019.01
13. Hou X, Wang H, Guo C, Gaskin J, and H. D. Psychological resilience can help combat the effect of stress on problematic social networking site usage. Pers Individ Differences. (2017) 109:61–6. doi: 10.1016/j.paid.2016.12.048
14. Yang X, Cuiying F, Zongkui Z, Qingqi L, and Shuailei L. The relationship between mindfulness and mobile phone addiction tendency: the role of boredom tendency and future time insight. psychol Dev education. (2021) 37:419–28. doi: 10.16187/j.cnki.issn1001-4918.2021.03.13
15. Tingting Y and Liu Y. Study on the relationship among college students' cell phone addiction, learning burnout and future time insight —— taking yangzhou university as an example. Educ Teach Forum. (2019) 6:68–73. doi: 10.16400/j.cnki.kjdks.2019.06.032
16. Julia M, J. LR, Ilke B, and R. MZ. An examination of multidimensional time perspective and mental health outcomes. Int J Environ Res Public Health. (2023) 20:4688. doi: 10.3390/ijerph20064688
17. Xiaolan S and Xiao W. Mind wandering in chinese daily lives–an experience sampling study. PloS One. (2012) 7:e44423. doi: 10.1371/journal.pone.0044423
18. Shuyan L, Ruihua L, Luisa W, Chuanning H, HM N, SD J, et al. High-mind wandering correlates with high risk for problematic alcohol use in China and Germany. Eur Arch Psychiatry Clin Neurosci. (2023) 274:335–41. doi: 10.1007/s00406-023-01555-4
19. Busch PA and Mccarthy S. Antecedents and consequences of problematic smartphone use: a systematic literature review of an emerging research area. Comput Hum Behav. (2021) 114:106414. doi: 10.1016/j.chb.2020.106414
20. Young KS. Internet sex addiction risk factors, stages of development, and treatment. Am Behav Sci. (2008) 52:21–37. doi: 10.1177/0002764208321339
21. Mok J, Choi S, Kim D, Choi J, Lee J, Ahn H, et al. Latent class analysis on internet and smartphone addiction in college students. Neuropsychiatr Dis Treat. (2014) 10:817–27. doi: 10.2147/NDT.S59293
22. Jie X, Zongkui Z, Chen W, Youzhiqi, and Ziyan Z. Development of mobile phone addiction tendency scale for college students. Chin Ment Health J. (2012) 26:222–5. doi: 10.3969/j.issn.1000-6729.2012.03.011
23. Borsboom D and Cramer AOJ. Network analysis: an integrative approach to the structure of psychopathology. Annual Review of Clinical Psychology (2013) 9:91–121. doi: 10.1146/annurev-clinpsy-050212-185608
24. Cramer AOJ, van Borkulo CD, Giltay EJ, van der Maas HLJ, Kendler KS, Scheffer M, et al. Major depression as a complex dynamic system. PloS One. (2016) 11:e167490. doi: 10.1371/journal.pone.0167490
25. Contreras A, Nieto I, Valiente C, Espinosa R, and Vazquez C. The study of psychopathology from the network analysis perspective: a systematic review. Psychother Psychosom. (2019) 88:71–83. doi: 10.1159/000497425
26. Price M, Legrand A, Brier Z, and Hébert-Dufresne L. The symptoms at the center: examining the comorbidity of posttraumatic stress disorder, generalized anxiety disorder, and depression with network analysis. J Psychiatr Res. (2018) 109:52–8. doi: 10.1016/j.jpsychires.2018.11.016
27. Griffiths M. A components model of addiction within a biopsychosocial framework. J Subst Use. (2009) 10:191–7. doi: 10.1080/14659890500114359
28. Xiongzhao Z, Fusheng L, Yaoshuqiao, Auerbach RP, and Abela JZ. Reliability and validity of cognitive emotion regulation questionnaire chinese version (cerq-c). Chin J Clin Psychol. (2007) 15:121–4. doi: 10.16128/j.cnki.1005-3611.2007.02.005
29. Qizheng S. Theoretical and empirical research on college students' future time insight. Southwest normal Univ. (2004), 45–68.
30. Xiaolan S, Xiao W, and Xiaowei T. Mental wandering: phenomenon, mechanism and significance. Adv psychol science. (2011) 19:499–509. doi: 10.3724/SP.J.1042.2011.00499
31. Ellis L and Rothbart M. Revision of the early adolescent temperament questionnaire. Poster presented at 2001 Biennal Meeting Soc Res Child Dev. (2001). doi: 10.1037/t07624-000
32. Li D, Zhang W, Li X, Zhen S, and Wang Y. Stressful life events and problematic internet use by adolescent females and males: a mediated moderation model. Comput Hum Behav. (2010) 26:1199–207. doi: 10.1016/j.chb.2010.03.031
33. Connor KM and Davidson JRT. Development of a new resilience scale: the connor-davidson resilience scale (cd-risc). Depress Anxiety. (2003) 18:76–82. doi: 10.1002/da.10113
34. Lynn M and Harris J. The desire for unique consumer products: a new individual differences scale. Psychol Mark. (1997) 14:601–16. doi: 10.1002/(SICI)1520-6793(199709)14:6<601::AID-MAR5>3.0.CO;2-B
35. Cai H, Zou X, Feng Y, Liu Y, and Jing Y. Increasing need for uniqueness in contemporary China: empirical evidence. Front Psychol. (2018) 9:554. doi: 10.3389/fpsyg.2018.00554
36. Team R. A language and environment for statistical computing. Computing. (2006) 1:5–24. doi: 10.1890/0012-9658(2002)083[3097:CFHIWS]2.0.CO;2
37. Epskamp S, Cramer AOJ, Waldorp LJ, Schmittmann VD, and Borsboom D. Qgraph: network visualizations of relationships in psychometric data. J Stat Software. (2012) 48:1–18. doi: 10.18637/jss.v048.i04
38. Epskamp S and Fried EI. A tutorial on regularized partial correlation networks. Psychol Methods. (2018) 23:617–34. doi: 10.1037/met0000167
40. van Rooijen G, Isvoranu A, Kruijt OH, van Borkulo CD, Meijer CJ, Wigman JTW, et al. A state-independent network of depressive, negative and positive symptoms in male patients with schizophrenia spectrum disorders. Schizophr Res. (2018) 193:232–9. doi: 10.1016/j.schres.2017.07.035
41. Gong Y, Guo Z, Lu H, Wang X, Zhang Y, Ren L, et al. Network analysis of acute stress reaction in a sample of chinese male military college students. Front Psychiatry. (2023) 14:1082549. doi: 10.3389/fpsyt.2023.1082549
42. Yuan H, Ren L, Ma Z, Li F, Liu J, Jin Y, et al. Network structure of ptsd symptoms in chinese male firefighters. Asian J Psychiatr. (2022) 72:103062. doi: 10.1016/j.ajp.2022.103062
43. Curran K. Building relationships: the impact of explicitly teaching social emotional learning standards and implementing restorative practices. Journal of School Health (2022) 92:89–102. doi: 10.1111/josh.13124
44. Peng N, Liu H, Wang T, Chang Y, Lee H, and Liang H. Evaluation of comfort and confidence of neonatal clinicians in providing palliative care. J Palliat Med. (2018) 21:1558–65. doi: 10.1089/jpm.2018.0102
45. Politis M, El Brown M, Huser CA, Crawford L, and Pope L. 'i wouldn't know what to do with the breasts': the impact of patient gender on medical student confidence and comfort in clinical skills. Educ primary care: an Off Publ Assoc Course Organisers Natl Assoc GP Tutors World Organisation Family Doctors. (2022) 33:316–26. doi: 10.1080/14739879.2022.2129460
46. Guo Z, He Y, Yang T, Ren L, Qiu R, Zhu X, et al. The roles of behavioral inhibition/activation systems and impulsivity in problematic smartphone use: a network analysis. Front Public Health. (2022) 10:1014548. doi: 10.3389/fpubh.2022.1014548
47. Haws JK, Brockdorf AN, Gratz KL, Messman TL, Tull MT, and Dilillo D. Examining the associations between ptsd symptoms and aspects of emotion dysregulation through network analysis. J Anxiety Disord. (2022) 86:102536. doi: 10.1016/j.janxdis.2022.102536
48. Guo Z, Cui Y, Yang T, Liu X, Lu H, Zhang Y, et al. Network analysis of affect, emotion regulation, psychological capital, and resilience among chinese males during the late stage of the covid-19 pandemic. Front Public Health. (2023) 11:1144420. doi: 10.3389/fpubh.2023.1144420
49. Bai W, Xi H, Zhu Q, Ji M, Zhang H, Yang B, et al. Network analysis of anxiety and depressive symptoms among nursing students during the covid-19 pandemic*. J Affect Disord. (2021) 294:753–60. doi: 10.1016/j.jad.2021.07.072
50. Bringmann LF, Elmer T, Epskamp S, Krause RW, Schoch D, Wichers M, et al. What do centrality measures measure in psychological networks? J Abnorm Psychol. (2019) 128:892–903. doi: 10.1037/abn0000446
51. Gijzen MWM, Rasing SPA, Creemers DHM, Smit F, Engels RCME, and De Beurs D. Suicide ideation as a symptom of adolescent depression. A network analysis. J Affect Disord. (2021) 278:68–77. doi: 10.1016/j.jad.2020.09.029
52. Tateno M, Kato TA, Shirasaka T, Kanazawa J, Ukai W, and Hirota T. A network analysis of problematic smartphone use in Japanese young adults. PloS One. (2022) 17:e0272803. doi: 10.1371/journal.pone.0272803
53. Huang S, Lai X, Xue Y, Zhang C, and Wang Y. A network analysis of problematic smartphone use symptoms in a student sample. J Behav Addict. (2020) 9:1032–43. doi: 10.1556/2006.2020.00098
54. Ran L, Wang W, Ai M, Kong Y, Chen J, and Kuang L. Psychological resilience, depression, anxiety, and somatization symptoms in response to covid-19: a study of the general population in China at the peak of its epidemic. Soc Sci Med. (2020) 262:113261. doi: 10.1016/j.socscimed.2020.113261
55. Wang Y, Chen Y, Xu J, Chen H, and Gao J. Association between resilience and frailty among chinese older adults. Front Psychiatry. (2022) 13:948958. doi: 10.3389/fpsyt.2022.948958
56. Rozgonjuk D, Blinka L, Loechner N, Faltynkova A, Husarova D, and Montag C. Differences between problematic internet and smartphone use and their psychological risk factors in boys and girls: a network analysis. Child Adolesc Psychiatry Ment Health. (2023) 17:62. doi: 10.1186/s13034-023-00620-z
57. Gong Z, Lv Y, Jiao X, Liu J, Sun Y, and Qu Q. The relationship between covid-19-related restrictions and fear of missing out, problematic smartphone use, and mental health in college students: the moderated moderation effect of resilience and social support. Front Public Health. (2022) 10:986498. doi: 10.3389/fpubh.2022.986498
58. Hao Z, Jin L, Huang J, Akram HR, and Cui Q. Resilience and problematic smartphone use: a moderated mediation model. BMC Psychiatry. (2023) 23:454. doi: 10.1186/s12888-023-04541-1
59. Ma A, Yang Y, Guo S, Li X, Zhang S, and Chang H. Adolescent resilience and mobile phone addiction in henan province of China: impacts of chain mediating, coping style. PloS One. (2022) 17:e0278182. doi: 10.1371/journal.pone.0278182
60. Ma A, Yang Y, Guo S, Li X, Zhang S, and Chang H. The impact of adolescent resilience on mobile phone addiction during covid-19 normalization and flooding in China: a chain mediating. Front Psychol. (2022) 13:865306. doi: 10.3389/fpsyg.2022.865306
61. Hao Z, Jin L, Huang J, and Wu H. Stress, academic burnout, smartphone use types and problematic smartphone use: the moderation effects of resilience. J Psychiatr Res. (2022) 150:324–31. doi: 10.1016/j.jpsychires.2022.03.019
62. Southwick SM and Charney DS. The science of resilience: implications for the prevention and treatment of depression. Science. (2012) 338:79–82. doi: 10.1126/science.1222942
63. Nowlan JS, Wuthrich VM, and Rapee RM. Self-report measures of positive reappraisal with a focus on older adults: a systematic review. Clin Gerontol. (2015) 38:302–24. doi: 10.1080/07317115.2015.1032468
64. Barberis N, Cernaro V, Costa S, Montalto G, Lucisano S, Larcan R, et al. The relationship between coping, emotion regulation, and quality of life of patients on dialysis. Int J Psychiatry Med. (2017) 52:111–23. doi: 10.1177/0091217417720893
65. Hauber K, Boon A, and Vermeiren R. Non-suicidal self-injury in clinical practice. Front Psychol. (2019) 10:502. doi: 10.3389/fpsyg.2019.00502
66. Li Y, Xu Y, and Chen Z. Effects of the behavioral inhibition system (bis), behavioral activation system (bas), and emotion regulation on depression: a one-year follow-up study in chinese adolescents. Psychiatry Res. (2015) 230:287–93. doi: 10.1016/j.psychres.2015.09.007
67. Liu C, Chen L, and Chen S. Influence of neuroticism on depressive symptoms among chinese adolescents: the mediation effects of cognitive emotion regulation strategies. Front Psychiatry. (2020) 11:420. doi: 10.3389/fpsyt.2020.00420
68. Orgiles M, Morales A, Fernandez-Martinez I, Melero S, and Espada JP. Validation of the short version of the cognitive emotion regulation questionnaire for spanish children. J Child Health Care. (2019) 23:87–101. doi: 10.1177/1367493518777306
69. Quan L, Lu B, Sun J, Zhao X, and Sang Q. The relationship between childhood trauma and post-traumatic growth among college students: the role of acceptance and positive reappraisal. Front Psychol. (2022) 13:921362. doi: 10.3389/fpsyg.2022.921362
70. Min J, Yu JJ, Lee C, and Chae J. Cognitive emotion regulation strategies contributing to resilience in patients with depression and/or anxiety disorders. Compr Psychiatry. (2013) 54:1190–7. doi: 10.1016/j.comppsych.2013.05.008
71. Mao C, Li Y, Zhang Y, Xie Z, and Li P. The relationship between alexithymia and cognitive emotion regulation strategies in nursing college students: a network analysis model. Chin J Clin Psychol. (2021) 29:753–7. doi: 10.16128/j.cnki.1005-3611.2021.04.015
72. Amone-P'Olak K, Boitumelo V, and Mberengwa DS. Cognitive emotion regulation strategies and mental health problems in war-affected youth in northern Uganda: findings from the ways study. J Ment Health (Abingdon England). (2019) 28:125–31. doi: 10.1080/09638237.2017.1385745
73. Extremera N and Rey L. Health-related quality of life and cognitive emotion regulation strategies in the unemployed: a cross-sectional survey. Health Qual Life Outcomes. (2014) 12:172. doi: 10.1186/s12955-014-0172-6
74. Yang X, Xu Y, Tan R, and Zhou X. Event centrality and post-traumatic stress symptoms among college students during the covid-19 pandemic: the roles of attention to negative information, catastrophizing, and rumination. Eur J Psychotraumatol. (2022) 13:2078563. doi: 10.1080/20008198.2022.2078563
75. Huang Y, Hu H, Wang L, Zhang Y, Wang X, Wang Y, et al. Relationships between childhood trauma and dimensional schizotypy: a network analysis and replication. Asian J Psychiatr. (2023) 85:103598. doi: 10.1016/j.ajp.2023.103598
76. Wang J, Luo Y, Yan N, Wang Y, Shiferaw BD, Tang J, et al. Network structure of mobile phone addiction and anxiety symptoms among rural chinese adolescents. BMC Psychiatry. (2023) 23:971. doi: 10.1186/s12888-023-04971-x
77. Cai H, Bai W, Sha S, Zhang L, Chow IHI, Lei S, et al. Identification of central symptoms in internet addictions and depression among adolescents in macau: a network analysis. J Affect Disord. (2022) 302:415–23. doi: 10.1016/j.jad.2022.01.068
78. Borsboom D. A network theory of mental disorders. World Psychiatry. (2017) 16:5–13. doi: 10.1002/wps.20375
79. Robinaugh DJ, Millner AJ, and Mcnally RJ. Identifying highly influential nodes in the complicated grief network. J Abnorm Psychol. (2016) 125:747–57. doi: 10.1037/abn0000181
Keywords: mobile phone addiction, network comparison test, central node, network analysis, effortful control
Citation: Qiu R, Guo Z, Wang X, Li Y, Li M and Xia Z (2025) New perspectives on mobile phone addiction based on network analysis. Front. Psychiatry 16:1665673. doi: 10.3389/fpsyt.2025.1665673
Received: 14 July 2025; Accepted: 25 September 2025;
Published: 13 October 2025.
Edited by:
Juan Sebastian Izquierdo-Condoy, University of the Americas, EcuadorReviewed by:
Tour Liu, Tianjin Normal University, ChinaBerkan Celik, Van Yuzuncu Yil University, Türkiye
Copyright © 2025 Qiu, Guo, Wang, Li, Li and Xia. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Zhu Xia, emh1eGlhQGZtbXUuZWR1LmNu
†These authors have contributed equally to this work and share first authorship