Abstract
Background:
The MATRICS Consensus Cognitive Battery (MCCB) is a widely used, standardized tool for assessing cognitive impairments in schizophrenia clinical trials. However, normative data for the MCCB in healthy adolescents remain scarce. This study establishes the first regionally representative norms for the MCCB in Chinese adolescents aged 11-16 years.
Methods:
Using stratified cluster sampling, we recruited 1,244 participants from Xiaogan City, demographically matched to regional population statistics. The Chinese-adapted MCCB assessed seven cognitive domains through nine subtests. Comprehensive analyses evaluated age, gender, and education effects using ANCOVA and non-parametric tests for non-normal distributions.
Results:
Our analyses revealed distinct developmental patterns across cognitive domains. Significant age-related improvements emerged in most measures (all p<0.05 except Trail Making Test-Part A), demonstrating continuous rather than stage-like progression. Gender differences were observed, with males outperforming in cognitive domains of processing speed, reasoning and problem solving, working memory and attention/vigilance, while females showed advantages in visual learning. After adjusting for gender, age initially exhibited significant associations with all cognitive tests; however, upon further adjustment for education, the effect of age was no longer significant in eight of the nine tests.
Conclusion:
This study establishes the first locally representative normative standards for the MCCB in Chinese adolescents, addressing a crucial gap in culturally sensitive cognitive assessment tools. Our findings demonstrate the complex interplay of age, gender, and educational factors in cognitive development, providing clinically valuable benchmarks for early detection of schizophrenia in this population.
Introduction
Neurocognitive dysfunction represents a core feature of schizophrenia (1). To develop standardized methods for evaluating novel treatments aimed at mitigating these cognitive deficits, the National Institute of Mental Health (NIMH) launched the Measurement and Treatment Research to Improve Cognition in Schizophrenia (MATRICS) initiative. This endeavor culminated in the creation of the MATRICS Consensus Cognitive Battery (MCCB), a reliable and valid assessment tool for clinical trials (2, 3), which is highly sensitive to detecting cognitive dysfunction in schizophrenia (4). Although MCCB co-norms have been established for healthy adults (3, 5, 6) and adults with schizophrenia (7), norms for adolescent populations have not yet been established, particularly given that cognitive impairment often emerges during the premorbid phase of schizophrenia, which typically occurs during adolescence, and persists throughout the lifespan (8).
The MCCB comprises nine core tests that systematically evaluate six dimensions of neurocognitive impairment in schizophrenia: attention/vigilance, speed of processing, working memory, visual learning, reasoning and problem solving, and verbal learning (9). Building on emerging research highlighting the importance of social cognition in real-world functioning, a tenth test, i.e., the Managing Emotions component of the Mayer-Salovey-Caruso Emotional Intelligence Test (MSCEIT) (2), was integrated to assess the social cognition domain. Validation studies demonstrate the MCCB’s clinical utility. Performance improvements on the MCCB correlate with real-world functional gains (10, 11). Additionally, its psychometric properties have been validated through the MATRICS Psychometric and Standardization Study (7) and the Validation of Intermediate Measures studies (12). Its 44 language versions facilitate global use, though normative data vary cross-culturally. For example, Singaporean English speakers performed differently than Americans due to cultural/educational factors (13), mirroring findings in other populations (14). Such variations underscore the need for culturally-specific norms, motivating China normative data collection.
A significant proportion of individuals with schizophrenia experience illness onset or prodromal symptoms during adolescence (15–17), and evidence shows adolescents with schizophrenia-spectrum disorders exhibit consistent deficits across MCCB domains except Social Cognition compared to healthy peers (18, 19). Thus, establishing normative MCCB trajectories for healthy adolescents is critical. Current limitations in adolescent normative data hinder clinical interpretation, necessitating studies to delineate developmental patterns across age groups, genders, and education levels. Although Norwegian (20) and North American (21) studies have begun to delineate MCCB developmental trajectories in adolescents, comprehensive, directly applicable normative data for this critical age group remain scarce internationally. The absence of adolescent normative data substantially limits clinical interpretation of MCCB results, particularly considering the high incidence of schizophrenia onset and prodromal symptoms during adolescence (8).
Addressing these methodological limitations, this study establishes regionally representative normative standards for the MCCB in Chinese adolescents. Utilizing a stratified cluster sampling methodology, we identified Xiaogan City in Hubei Province as our study site - a demographically representative midsize city randomly selected from Hubei’s prefecture-level municipalities. Our sampling framework is designed with reference to China’s education system, focusing on covering three distinct educational stages: primary school (high grade), junior high school, and senior high school. From the collected samples, it randomly selects adolescents aged 11-16 (grade 5-12) in proportion to the age distribution specified in the XiaoGan Statistical Yearbook (2024). This approach captures both essential neurodevelopmental milestones and regionally specific sociodemographic characteristics. The resulting normative data will provide clinically valuable reference standards for psychiatric assessment in Central China while simultaneously establishing foundational metrics for future cross-cultural investigations of neurocognitive development.
Methods
Participants and recruitment process
Participants were adolescents aged 11 to 16 years from Xiaogan City, Hubei Province. Stratified random sampling was conducted by educational stage, based on the official school list provided by the Xiaogan Education Bureau, with 2 schools randomly selected from each stage. In each selected schools, 2 classes were randomly selected from each target grade (grades 5-12). Prior to the survey, written informed consent was obtained from all students in these classes and their guardians, with explicit notification that participants could withdraw at any time if experiencing discomfort (without adverse consequences). No withdrawals occurred, so all students in the selected classes completed the assessment. According to the XiaoGan Statistical Yearbook (2024), the sample was selected with corresponding age and gender ratios. Six age groups (11–16 years) were selected with proportional distribution: 11-year-olds (15.35%), 12-year-olds (16.24%), 13-year-olds (17.60%), 14-year-olds (18.65%), 15-year-olds (16.64%), and 16-year-olds (15.51%). The sample comprised 51.77% male and 48.23% female participants. In accordance with China’s education system, participants were categorized by educational attainment: 4 years (5.23%), 5 years (12.94%), 6 years (13.59%), 7 years (23.15%), 8 years (16.72%), 9 years (8.92%), 10 years (16.40%), and 11 years (3.05%).
Inclusion criteria: aged 11–16 years at recruitment; native Mandarin speakers with the ability to complete interviews and questionnaires in Chinese; no known chronic somatic diseases affecting brain function.
Exclusion criteria: history of past or present diagnosis of major psychiatric disorders; participants with first-degree relatives known or suspected to have major psychiatric disorders; active or recent (within the past month) substance abuse; neurological/medical comorbidities; intelligence quotient (IQ) < 70; or significant sensory/communication impairments.
All participants and guardians provided written informed consent. The study was approved by the Medical Ethics Committee of Renmin Hospital of Wuhan University (Approval No. WDRY2024-K039).
Neuropsychological measures
To evaluate cognitive functioning, the Chinese adaptation of the MATRICS Consensus Cognitive Battery (MCCB) (22, 23) was administered. This instrument measures six neurocognitive dimensions: Speed of processing [Category fluency/verbal fluency for animals (VF), Symbol coding subtest from the Brief Assessment of Cognition in Schizophrenia (SC-BACS), Trail Making Test-Part A (TMT-A); Attention/vigilance (Continuous Performance Test-Identical Pairs, CPT-IP); Working memory (Spatial Span subtest from the Wechsler Memory Scale-III, WMS-III SS); Verbal learning (Hopkins Verbal Learning Test-Revised, HVLT-R); Visual learning (Brief Visuospatial Memory Test-Revised, BVMT-R); Reasoning and problem solving (Mazes subtest from the Neuropsychological Assessment Battery, NAB Mazes); and one Social Cognition domain (Managing Emotions component of the Mayer–Salovey–Caruso Emotional Intelligence Test, MSCEIT).
The MCCB comprises 10 core tests across seven cognitive domains, nine of which were administered in this study. Due to cultural adaptation challenges as there is no corresponding alphabet system in Chinese, the Letter-Number Span (LNS) test was not adopted.
Data analysis
The distribution normality of all nine test scores was evaluated using the Lilliefors test (24), and significantly skewed distributions (p < 0.05) were subjected to transformation. Among square, logarithmic, and Box–Cox transformations, the most suitable method was selected to ensure the post-transformation p-value exceeded 0.05 and the distribution approximated normality; original scores were retained if transformation was ineffective. Raw scores of the nine MCCB subtests were converted to T-scores using the formula: T-score= 10 + 3× (raw score - Mean)/Standard Deviation. For the TMT-A, which exhibits an opposite trend of scores compared to other subtests, a specialized standardization method was employed, with the specific formula as follows: T-score = 10 - 3 × (raw score - Mean)/Standard Deviation. This transformation was based on the raw score distribution of our sample (n = 1,244). For each subtest, we first calculated the mean and standard deviation (SD) of raw scores across the entire sample. Using the formula above, T-scores were standardized such that the mean T-score for each subtest was 10 and the SD was 3. Subsequent differential analysis explored age, gender, and educational effects on nine subtest T-scores. Analysis of covariance (ANCOVA) assessed performance disparities related to age and educational attainment, while independent T-tests evaluated gender effects. For non-normally distributed data, rank sum tests (Mann-Whitney U or Kruskal-Wallis) were applied to assess group differences. To clarify the relative roles of age and years of education in performance across 10 cognitive domains, we conducted hierarchical multiple linear regression analyses. The scores of each domain served as dependent variables, with gender included as a covariate. Predictors were incorporated in three sequential steps: Model 1 included only gender; Model 2 added age to Model 1; and Model 3 further added years of education to Model 2. Standardized regression coefficients (β) were used to compare the effect magnitudes of age and education. Changes in model explanatory power (ΔR²) and significance tests were employed to evaluate the unique contribution of education relative to age.
Results
Demographic characteristics
The sample had a mean age of 13.52 years (SD = 1.66) and an average educational attainment of 7.42 years (SD = 1.88). The cohort comprised 600 females (48.23%) and 644 males (51.77%), reflecting a balanced gender distribution.
Age effects
Given the differences in educational attainments across the six age groups, education was treated as a covariate in ANCOVA models examining age-related effects. Non-parametric Kruskal–Wallis tests were employed for non-normally distributed data. Significant age effects were observed in the tests of BACS (F = 2.73, p =0.018), HVLT (H = 132.10, p < 0.001), WMS (H = 73.78, p < 0.001), NAB Mazes (H = 123.59, p < 0.001), BVMT (H = 52.06, p < 0.001), VF (H = 223.40, p < 0.001), MSCEIT (H = 58.55, p < 0.001), and CPT-IP (F = 2.23, p =0.049), except for the TMT-A test (F = 1.13, p =0.342) (see Table 1 and Figure 1).
Table 1
| AGE | 11years (n=191) | 12years (n=202) | 13years (n=219) | 14years (n=232) | 15years (n=207) | 16years (n=193) | F | p |
|---|---|---|---|---|---|---|---|---|
| TMT-A | 8.24 ± 2.67 | 9.10 ± 3.02 | 9.95 ± 2.60 | 9.99 ± 2.82 | 10.94 ± 2.99 | 11.76 ± 2.61 | 1.13 | 0.3423 |
| SC-BACS | 7.25 ± 2.39 | 8.55 ± 2.42 | 9.79 ± 2.36 | 10.04 ± 2.49 | 11.83 ± 2.56 | 12.47 ± 2.48 | 2.73 | 0.018 |
| CPT-IP | 7.16 ± 2.32 | 8.61 ± 2.37 | 9.71 ± 2.50 | 10.09 ± 2.46 | 11.82 ± 2.65 | 12.54 ± 2.22 | 2.23 | 0.049 |
| H | p | |||||||
| HVLT-R | 8.40 ± 3.16 | 9.49 ± 2.96 | 9.61 ± 2.99 | 10.11 ± 2.61 | 10.73 ± 2.81 | 11.64 ± 2.48 | 132.10 | <0.001 |
| WMS-III SS | 8.75 ± 3.14 | 9.29 ± 2.93 | 10.28 ± 2.86 | 9.95 ± 3.01 | 10.87 ± 2.74 | 10.78 ± 2.76 | 73.78 | <0.001 |
| NAB Mazes | 8.66 ± 3.49 | 9.26 ± 3.09 | 9.77 ± 2.88 | 10.13 ± 2.71 | 10.8 ± 2.64 | 11.35 ± 2.35 | 123.59 | <0.001 |
| BVMT-R | 9.07 ± 3.13 | 9.28 ± 3.19 | 10.05 ± 2.94 | 10.15 ± 3.01 | 10.84 ± 2.53 | 10.54 ± 2.8 | 52.06 | <0.001 |
| VF | 8.18 ± 2.3 | 9.12 ± 2.68 | 9.81 ± 2.55 | 9.61 ± 2.85 | 11.19 ± 3.01 | 12.13 ± 2.86 | 223.40 | <0.001 |
| MSCEIT | 9.42 ± 3.34 | 9.62 ± 2.94 | 9.58 ± 2.86 | 9.57 ± 2.96 | 10.9 ± 2.71 | 11.00 ± 2.77 | 58.55 | <0.001 |
Mean T-scores for the 9 MCCB tests, by age group.
ANCOVA, education as covariance; Kruskal-Wallis test.
Figure 1

Mean T-scores of the MCCB by age group. The figure presents nine box plots showing the distribution of scores for the cognitive tests from the MCCB: TMT-A, SC-BACS, HVLT-R, WMS-III SS, NAB Mazes, BVMT-R, VF, MSCEIT and CPT-IP. Each test is represented by a separate box plot, with data points stratified into six age groups (11 to 16 years old), each denoted by a distinct color. Overall between-group differences are indicated by asterisks (* for p < 0.05; ** p < 0.001).
A consistent age effect was observed across all cognitive tests except TMT-A: later adolescent consistently outperformed younger ones, and this effect remained significant after controlling for education. Scores peaked at age 16 and showed an overall monotonic increase with age, though BVMT and WMS scores plateaued after peaking at age 15.
Gender effects
Significant gender differences were observed on several cognitive tests. In the TMT-A (t = 5.49, p < 0.001), CPT-IP (t = 2.12, df = 1242, p =0.033), WMS (U = 216913.5, p < 0.001), and NAB Mazes (U = 244081, p < 0.001), males performed better than females. Conversely, females outperformed males in BVMT (U = 178759, p =0.022). There were no statistically significant differences between male and female in the other cognitive tests (see Table 2 and Figure 2).
Table 2
| Gender | Male (n=644) | Female (n=600) | t | p | Effect size |
|---|---|---|---|---|---|
| TMT-A | 10.45 ± 2.75 | 9.52 ± 3.18 | 5.49 | <0.001 | 0.31 |
| SC-BACS | 9.84 ± 3.09 | 10.17 ± 2.89 | -1.92 | 0.055 | -0.11 |
| CPT-IP | 10.17 ± 3.06 | 9.81 ± 2.93 | 2.12 | 0.033 | 0.12 |
| U | p | ||||
| HVLT-R | 10.04 ± 2.88 | 9.96 ± 3.12 | 192783.5 | 0.948 | |
| WMS-III SS | 10.33 ± 2.86 | 9.65 ± 3.11 | 216913.5 | <0.001 | |
| NAB Mazes | 10.70 ± 2.47 | 9.25 ± 3.32 | 244081 | <0.001 | |
| BVMT-R | 9.86 ± 2.93 | 10.15 ± 3.07 | 178759 | 0.022 | |
| VF | 10.01 ± 2.98 | 9.99 ± 3.03 | 194163 | 0.879 | |
| MSCEIT | 9.96 ± 2.89 | 10.04 ± 3.11 | 188835 | 0.491 |
Mean T-scores for the nine MCCB tests, by gender.
t-test for normal data, Mann-Whitney U test.
Figure 2
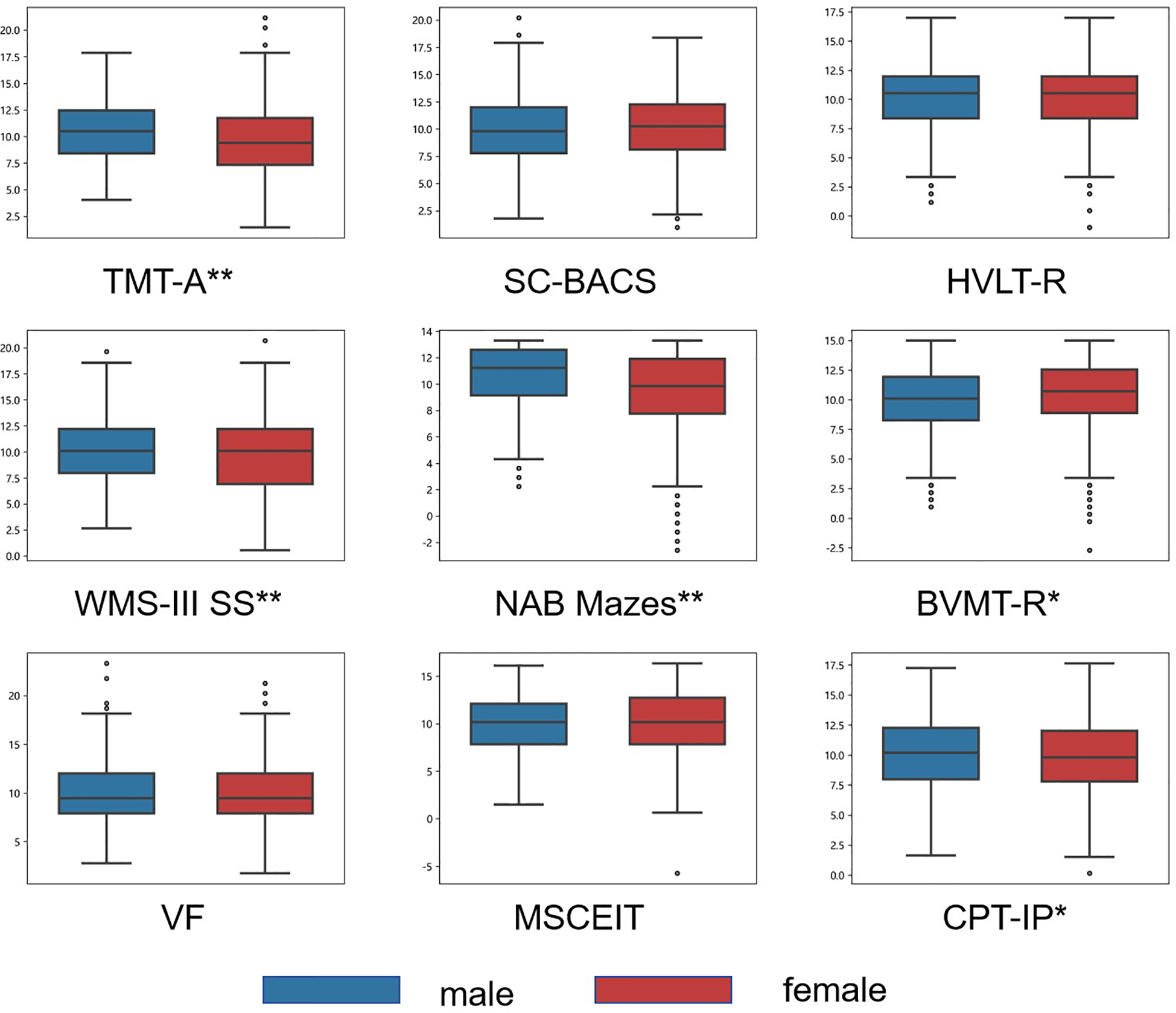
Mean T-scores of the MCCB by gender group. Box plots display the distribution of scores for males (blue) and females (red) on nine cognitive tests from the MCCB. Significant between-sex differences for each test are indicated by asterisks (* p < 0.05; ** p < 0.001).
Education effects
To account for age-related variance in cognitive performance, we included age as a covariate in our analysis of education effects. Educational attainment significantly affected performance on all nine cognitive tests of TMT-A (F = 3.54, p < 0.001), BACS (F = 9.05, p < 0.001), HVLT (H = 161.76, p < 0.001), WMS (H = 77.51, p < 0.001), NAB Mazes (H = 134.02, p < 0.001), BVMT (H = 53.78, p < 0.001), VF (H = 254.87, p < 0.001), and MSCEIT (H = 76.74, p < 0.001)(see Table 3 and Figure 3).
Table 3
| Education | 4 (n=65) | 5 (n=161) | 6 (n=169) | 7 (n=288) | 8 (n=208) | 9 (n=111) | 10 (n=204) | 11 (n=38) | F | p |
|---|---|---|---|---|---|---|---|---|---|---|
| TMT-A | 8.09 ± 2.74 | 8.35 ± 2.93 | 9.22 ± 2.66 | 10.02 ± 2.71 | 9.82 ± 2.89 | 11.29 ± 2.58 | 11.64 ± 2.91 | 11.92 ± 2.33 | 3.54 | <0.001 |
| SC-BACS | 6.64 ± 2.14 | 7.81 ± 2.46 | 8.63 ± 2.51 | 9.61 ± 2.34 | 10.25 ± 2.55 | 12.47 ± 2.14 | 12.34 ± 2.55 | 12.93 ± 1.89 | 9.05 | <0.001 |
| CPT-IP | 7.02 ± 2.08 | 7.31 ± 2.37 | 8.92 ± 2.44 | 9.62 ± 2.42 | 10.24 ± 2.67 | 11.94 ± 2.45 | 12.74 ± 2.11 | 12.41 ± 1.86 | 9.47 | <0.001 |
| H | p | |||||||||
| HVLT-R | 7.67 ± 2.91 | 8.73 ± 3.23 | 9.84 ± 2.88 | 9.66 ± 2.96 | 9.81 ± 2.54 | 11.12 ± 2.87 | 11.62 ± 2.41 | 11.76 ± 2.29 | 161.76 | <0.001 |
| WMS-III SS | 8.15 ± 3.31 | 9.02 ± 2.88 | 9.49 ± 2.87 | 10.01 ± 3.01 | 10.21 ± 2.93 | 11.16 ± 2.79 | 10.86 ± 2.75 | 10.26 ± 2.69 | 77.51 | <0.001 |
| NAB Mazes | 8.12 ± 4.21 | 8.93 ± 2.99 | 9.22 ± 2.89 | 9.82 ± 2.95 | 10.29 ± 2.75 | 11.26 ± 2.27 | 11.08 ± 2.62 | 11.49 ± 2.03 | 134.02 | <0.001 |
| BVMT-R | 8.77 ± 3.16 | 9.48 ± 3.1 | 9.1 ± 3.26 | 9.99 ± 2.97 | 10.27 ± 2.95 | 10.87 ± 2.44 | 10.58 ± 2.79 | 11.22 ± 2.04 | 53.78 | <0.001 |
| VF | 8.43 ± 2.41 | 8.08 ± 2.35 | 9.59 ± 2.63 | 9.4 ± 2.6 | 9.92 ± 2.89 | 11.1 ± 2.81 | 12.39 ± 2.93 | 11.55 ± 2.31 | 254.87 | <0.001 |
| MSCEIT | 9.54 ± 3.34 | 9.54 ± 3.2 | 9.36 ± 3.06 | 9.56 ± 2.85 | 9.75 ± 2.84 | 11.2 ± 2.54 | 11.27 ± 2.69 | 9.98 ± 3.27 | 76.74 | <0.001 |
Mean T-scores for the 9 MCCB tests, by education group.
ANCOVA, age as covariance;Kruskal-Wallis test.
Figure 3
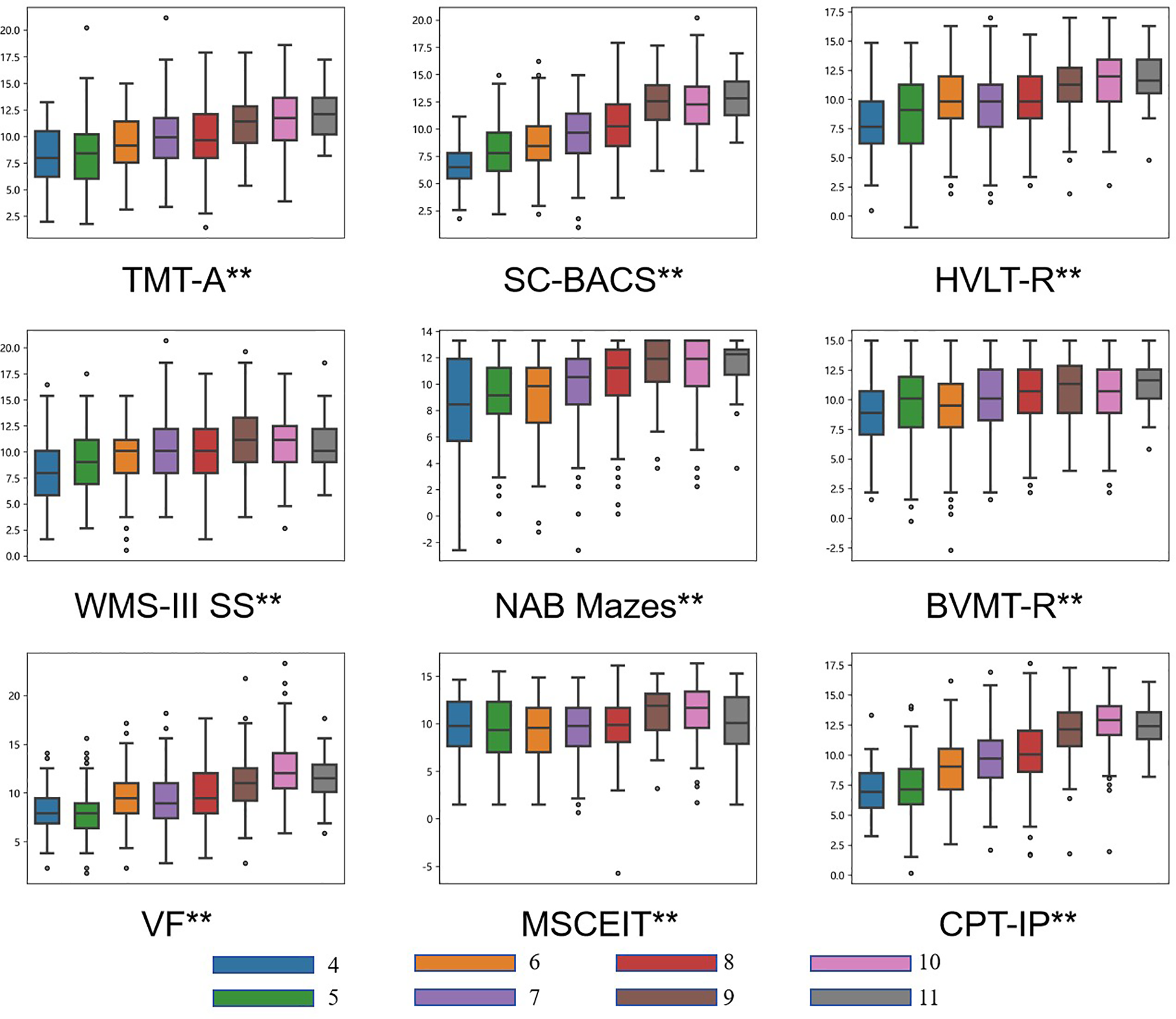
Mean T-scores of the MCCB by education level. Nine box plots display the distribution of scores for the nine cognitive tests from the MCCB. Each test is stratified by education level, categorized into groups from 4 to 11 years of schooling and represented by distinct colors. Significant overall between-group differences are indicated by asterisks (** p < 0.001).
Among the nine cognitive subtests, the CPT-IP, Category fluency, and MSCEIT Managing Emotions tests achieved their highest scores at 10 years of education. The WMS-III Spatial Span test peaked at 9 years of education, while the remaining subtests showed progressively higher scores with increasing educational attainment. Significant differences were observed across all eight educational levels for all nine cognitive subtests.
Comparisons of age and gender impact on cognitive performance
A series of multiple linear regression analyses was performed in order to evaluate the influence of age and education attainment on cognitive performance; they are summarized in Tables 4. The variables were entered in hierarchical order into a linear regression model using the enter method in order to evaluate the changes in explained variance in all tests.
Table 4
| Test | Variables | β | p | ΔR2 | Sig. F Change | Adjusted R 2 |
|---|---|---|---|---|---|---|
| TMT.A | ||||||
| 1 | gender | -0.155 | <0.001 | 0.024 | <0.001 | 0.023 |
| 2 | gender | -0.164 | <0.001 | 0.136 | <0.001 | 0.158 |
| age | 0.368 | <0.001 | ||||
| 3 | gender | -0.168 | <0.001 | 0.009 | <0.001 | 0.166 |
| age | 0.089 | 0.272 | ||||
| education | 0.295 | <0.001 | ||||
| BACS.SC | ||||||
| 1 | gender | 0.054 | 0.056 | 0.003 | 0.056 | 0.002 |
| 2 | gender | 0.04 | 0.086 | 0.325 | <0.001 | 0.327 |
| age | 0.57 | <0.001 | ||||
| 3 | gender | 0.034 | 0.14 | 0.021 | <0.001 | 0.347 |
| age | 0.144 | 0.045 | ||||
| education | 0.45 | <0.001 | ||||
| HVLT | ||||||
| 1 | gender | -0.014 | 0.622 | 0 | 0.622 | -0.001 |
| 2 | gender | -0.022 | 0.412 | 0.104 | <0.001 | 0.102 |
| age | 0.322 | <0.001 | ||||
| 3 | gender | -0.027 | 0.314 | 0.013 | <0.001 | 0.115 |
| age | -0.017 | 0.841 | ||||
| education | 0.357 | <0.001 | ||||
| WMS.III.SS | ||||||
| 1 | gender | -0.112 | <0.001 | 0.013 | <0.001 | 0.012 |
| 2 | gender | -0.118 | <0.001 | 0.054 | <0.001 | 0.065 |
| age | 0.232 | <0.001 | ||||
| 3 | gender | -0.121 | <0.001 | 0.004 | 0.021 | 0.068 |
| age | 0.044 | 0.61 | ||||
| education | 0.198 | 0.021 | ||||
| NAB.Mazes | ||||||
| 1 | gender | -0.243 | <0.001 | 0.059 | <0.001 | 0.058 |
| 2 | gender | -0.25 | <0.001 | 0.089 | <0.001 | 0.146 |
| age | 0.298 | <0.001 | ||||
| 3 | gender | -0.254 | <0.001 | 0.007 | 0.002 | 0.152 |
| age | 0.056 | 0.493 | ||||
| education | 0.255 | 0.002 | ||||
| BVMT | ||||||
| 1 | gender | 0.047 | 0.096 | 0.002 | 0.096 | 0.001 |
| 2 | gender | 0.042 | 0.128 | 0.037 | <0.001 | 0.038 |
| age | 0.192 | <0.001 | ||||
| 3 | gender | 0.041 | 0.142 | 0.001 | 0.19 | 0.038 |
| age | 0.084 | 0.334 | ||||
| education | 0.114 | 0.19 | ||||
| Fluency | ||||||
| 1 | gender | -0.004 | 0.885 | 0 | 0.885 | -0.001 |
| 2 | gender | -0.014 | 0.584 | 0.164 | <0.001 | 0.162 |
| age | 0.405 | <0.001 | ||||
| 3 | gender | -0.019 | 0.451 | 0.015 | <0.001 | 0.177 |
| age | 0.041 | 0.607 | ||||
| education | 0.383 | <0.001 | ||||
| MSCEIT.ME | ||||||
| 1 | gender | 0.014 | 0.613 | 0 | 0.613 | -0.001 |
| 2 | gender | 0.01 | 0.728 | 0.034 | <0.001 | 0.033 |
| age | 0.185 | <0.001 | ||||
| 3 | gender | 0.007 | 0.79 | 0.003 | 0.055 | 0.035 |
| age | 0.027 | 0.755 | ||||
| education | 0.167 | 0.055 | ||||
| CPT | ||||||
| 1 | gender | -0.06 | 0.034 | 0.004 | 0.034 | 0.003 |
| 2 | gender | -0.075 | 0.001 | 0.342 | <0.001 | 0.344 |
| age | 0.585 | <0.001 | ||||
| 3 | gender | -0.081 | <0.001 | 0.023 | <0.001 | 0.367 |
| age | 0.131 | 0.064 | ||||
| education | 0.479 | <0.001 | ||||
Multiple linear regression analysis: comparisons of age and gender impact on cognitive performance.
Associations of gender, age and education attainments with cognitive performance. Linear regression model. Variables entered in a hierarchical way in 3 blocks—1. gender, 2. age, 3. education attainments; The variable p, the β, adjusted R2 and ΔR2 are the values after each step.
After adjusting for gender, age emerged as a significant predictor of performance across all tests (β range = 0.185 to 0.585; all p < 0.05). However, after further adjustment for educational attainment, the effect of age was no longer significant in 8 out of the 9 tests (β range = 0.017 to 0.131; all p > 0.05), with the exception of the BACS.SC (β = 0.144; all p =0.045).
Age accounted for 3.3% to 34.4% of the variance in cognitive performance across all tests, with each model exhibiting a significant increment in ΔR² (all p < 0.001). Following additional adjustment for educational attainment, the models corresponding to 7 out of 9 tests explained 6.8% to 36.7% of the variance, accompanied by a significant ΔR² increment (all p < 0.001), the only exceptions were the models for BVMT and MSCEIT.ME.
Discussion
This study establishes the first regionally representative normative standards for the MATRICS Consensus Cognitive Battery (MCCB) among Chinese adolescents aged 11–16 years. Our results document three fundamental patterns of cognitive development: significant age-dependent trajectories, domain-specific gender differences, and education-modulated performance profiles. These findings provide critical insights for clinical assessment protocols and neurodevelopmental research.
Our study demonstrates age-related cognitive improvements across most MCCB domains in Chinese adolescents. Although we found significant overall differences between age groups, post hoc tests showed no significant pairwise differences, indicating gradual developmental changes. This continuous progression pattern contrasts with some previous studies reporting more substantial cognitive gains during adolescence (25), a discrepancy that may stem from methodological differences in age grouping, where prior work used 4-year intervals versus our 1-year stratification (25), allowing for more sensitive detection of incremental changes. Notably, our findings of progressive but decelerating cognitive maturation align with established meta-analytic evidence demonstrating a characteristic developmental sequence: rapid cognitive improvements during childhood transition to more moderated gains in adolescence, ultimately reaching a relative plateau in late adolescence and young adulthood (26). This nonlinear trajectory reflects well-documented neurodevelopmental processes, particularly the extended maturation timeline of prefrontal circuits that underlie executive functions (27). The observed pattern corresponds to initial robust neural reorganization during early adolescence, marked by intensive myelination and synaptic pruning, followed by more gradual refinement continuing through late adolescence (27, 28).
A noteworthy exception was the TMT-A, which exhibited no age effect. This is likely attributable to ceiling effects in older adolescents, as TMT-A primarily assesses visual tracking and basic motor coordination—abilities that may mature relatively early in adolescence. At this stage, most adolescents have already reached near-optimal performance on such tasks, limiting the test’s sensitivity to further age-related improvements.
Males outperformed females in psychomotor speed (TMT-A), sustained attention (CPT-IP) and spatial tasks (WMS-III SS, NAB Mazes) while females excelled in visuospatial memory (BVMT-R). Regarding males’ superior performance in NAB Mazes, our findings are consistent with those from studies on American adolescent norms and Chinese adult norms (5, 21). These findings mirror meta-analytic results (29), there is ample evidence of the influence of sex hormones on visual-spatial working memory in humans. Males demonstrated faster information processing speed, which was inconsistent with the performance observed in Norwegian norms, yet this discrepancy was not detected in studies conducted in the United States (20, 21). Additionally, no significant gender differences were identified in social cognition (MSCEIT), which might be attributed to the high homogeneity in improvements related to social cognitive abilities, which weakened the manifestation of potential gender differences.
Notable disparities in cognitive abilities were observed across levels of educational attainment. After adjusting for age, significant differences persisted in all subtests. Despite the uneven distribution of sample sizes across educational attainments due to age-based participant selection, the study still had an adequate sample size in each subgroup categorized by educational level. We found that all test performances, including the TMT-A, exhibited significant differences among the eight groups. In future comparative studies on the TMT-A, researchers are advised to analyze variations in test performance based on educational attainment rather than age, thereby enhancing the relevance and explanatory power of the results. Improvements in cognitive abilities associated with educational attainment may stem from the pivotal role of school quality and curricular depth in the cognitive development of Chinese adolescents.
After adjusting for gender, age initially exhibited significant associations with all cognitive tests; however, upon further adjustment for education, the effect of age was no longer significant in eight of the nine tests. Our findings highlight the predominant role of educational attainment over age in predicting cognitive performance. This pattern suggests that education largely cover the relationship between age and cognitive function. Moreover, the incremental variance explained by education was statistically significant in seven tests, reinforcing its stronger independent influence. These results underscore the importance of educational attainment as a key factor explain age-related cognitive differences.
The establishment of age-specific normative data enables sensitive detection of subtle cognitive impairments in adolescents at clinical risk for psychosis, particularly due to cognitive deficits that frequently emerge before overt symptom manifestation (30, 31). These robust reference standards enhance the MCCB’s clinical utility for both diagnostic assessment and intervention monitoring in adolescent populations. Findings of this study indicate that cognitive function in most domains improves continuously with age. A “high-risk” signal may also include the absence of age-expected progress in cognitive function. By acquiring data on MCCB performance in healthy adolescents, it is possible to elucidate the differential trajectories of cognitive function in early-stage psychosis, thereby facilitating the formulation of individualized cognitive rehabilitation interventions (32). Our fine-grained age stratification (1-year intervals) offers unprecedented sensitivity for tracking neurodevelopmental trajectories during this critical period, delivering clinically meaningful prognostic insights for early-onset schizophrenia cases.
The study sample was exclusively drawn from the urban area of Xiaogan, and did not include any rural populations. This limits the applicability of the local urban norm to rural areas of Xiaogan. Although the demographic and educational characteristics of Xiaogan are closely aligned with those of Hubei Province as a whole, the applicability of the norms to rural area of Xiaogan must be established through further validation. Consequently, the normative data are specific to urban Xiaogan and not generalizable to its rural areas. Furthermore, the clinical utility of these norms requires additional investigation through longitudinal studies examining their predictive validity for identifying psychosis conversion among high-risk adolescent populations.
In conclusion, by providing robust developmental norms for MCCB performance in Chinese adolescents, this study fills a critical gap in neurocognitive assessment tools. Our data underscore the interplay of age, gender, and education in shaping cognitive trajectories, offering a foundation for early identification of neurodevelopmental disorders and cross-cultural research on adolescent brain maturation.
Statements
Data availability statement
The original contributions presented in the study are included in the article/supplementary material. Further inquiries can be directed to the corresponding author.
Ethics statement
The studies involving humans were approved by Medical Ethics Committee of Renmin Hospital of Wuhan University (Approval No. WDRY2024-K039). The studies were conducted in accordance with the local legislation and institutional requirements. Written informed consent for participation in this study was provided by the participants’ legal guardians/next of kin.
Author contributions
YT: Writing – original draft. XZ: Writing – original draft, Validation. HL: Data curation, Writing – review & editing. MF: Methodology, Writing – review & editing. JH: Investigation, Writing – review & editing. XS: Data curation, Writing – review & editing. YZ: Data curation, Writing – review & editing. XW: Data curation, Writing – review & editing. JY: Data curation, Writing – review & editing. MH: Funding acquisition, Supervision, Writing – review & editing.
Funding
The author(s) declare financial support was received for the research and/or publication of this article. The study was supported by the National Natural Science Foundation of China (62576254), Fundamental Research Funds for the Central Universities (2042025YXA006), Major Project of Science and Technology Innovation of Hubei Province (2024BCA003), Hubei Provincial Natural Science Foundation (2024AFB751), Key Project of Hubei Provincial Health Commission (WJ2023Z003), and Undergraduate Training Programs for Innovation of Wuhan University (202510486145).
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Generative AI statement
The author(s) declare that no Generative AI was used in the creation of this manuscript.
Any alternative text (alt text) provided alongside figures in this article has been generated by Frontiers with the support of artificial intelligence and reasonable efforts have been made to ensure accuracy, including review by the authors wherever possible. If you identify any issues, please contact us.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1
Medalia A Thysen J . Insight into neurocognitive dysfunction in schizophrenia. Schizophr Bulletin. (2008) 34:1221–30. doi: 10.1093/schbul/sbm144
2
Nuechterlein KH Green MF Kern RS Baade LE Barch DM Cohen JD et al . The MATRICS Consensus Cognitive Battery, part 1: test selection, reliability, and validity. Am J Psychiatry. (2008) 165:203–13. doi: 10.1176/appi.ajp.2007.07010042
3
Kern RS Nuechterlein KH Green MF Baade LE Fenton WS Gold JM et al . The MATRICS Consensus Cognitive Battery, part 2: co-norming and standardization. Am J Psychiatry. (2008) 165:214–20. doi: 10.1176/appi.ajp.2007.07010043
4
Plichta P Tyburski E Bielecki M Mak M Kucharska-Mazur J Podwalski P et al . Cognitive dysfunctions measured with the MCCB in deficit and non-deficit schizophrenia. J Clin Med. (2023) 12:2257. doi: 10.3390/jcm12062257
5
Shi C Kang L Yao S Ma Y Li T Liang Y et al . The MATRICS Consensus Cognitive Battery (MCCB): co-norming and standardization in China. Schizophr Res. (2015) 169:109–15. doi: 10.1016/j.schres.2015.09.003
6
Rodriguez-Jimenez R Bagney A Garcia-Navarro C Aparicio A Lopez-Anton R Moreno-Ortega M et al . The MATRICS consensus cognitive battery (MCCB): co-norming and standardization in Spain. Schizophr Res. (2012) 134:279–84. doi: 10.1016/j.schres.2011.11.026
7
Green MF Nuechterlein KH Kern RS Baade LE Fenton WS Gold JM et al . Functional co-primary measures for clinical trials in schizophrenia: results from the MATRICS Psychometric and Standardization Study. Am J Psychiatry. (2008) 165:221–8. doi: 10.1176/appi.ajp.2007.07010089
8
Harrop C Trower P . Why does schizophrenia develop at late adolescence? Clin Psychol Rev. (2001) 21:241–65. doi: 10.1016/S0272-7358(99)00047-1
9
Nuechterlein KH Barch DM Gold JM Goldberg TE Green MF Heaton RK . Identification of separable cognitive factors in schizophrenia. Schizophr Res. (2004) 72:29–39. doi: 10.1016/j.schres.2004.09.007
10
Buchanan RW Davis M Goff D Green MF Keefe RS Leon AC et al . A summary of the FDA-NIMH-MATRICS workshop on clinical trial design for neurocognitive drugs for schizophrenia. Schizophr bulletin. (2005) 31:5–19. doi: 10.1093/schbul/sbi020
11
Buchanan RW Keefe RS Umbricht D Green MF Laughren T Marder SR . The FDA-NIMH-MATRICS guidelines for clinical trial design of cognitive-enhancing drugs: what do we know 5 years later? Schizophr Bull. (2011) 37:1209–17. doi: 10.1093/schbul/sbq038
12
Green MF Schooler NR Kern RS Frese FJ Granberry W Harvey PD et al . Evaluation of functionally meaningful measures for clinical trials of cognition enhancement in schizophrenia. Am J Psychiatry. (2011) 168:400–7. doi: 10.1176/appi.ajp.2010.10030414
13
Rapisarda A Lim TF Lim M Collinson SL Kraus MS Keefe RS . Applicability of the MATRICS consensus cognitive battery in Singapore. Clin Neuropsychologist. (2013) 27:455–69. doi: 10.1080/13854046.2012.762120
14
Shadlen MF Larson EB Gibbons LE Rice MM McCormick WC Bowen J et al . Ethnicity and cognitive performance among older African Americans, Japanese Americans, and Caucasians: The role of education. J Am Geriatrics Society. (2001) 49:1371–8. doi: 10.1046/j.1532-5415.2001.49269.x
15
Cannon M Jones P Huttunen MO Tanskanen A Huttunen T Rabe-Hesketh S et al . School performance in Finnish children and later development of schizophrenia: a population-based longitudinal study. Arch Gen Psychiatry. (1999) 56:457–63. doi: 10.1001/archpsyc.56.5.457
16
Juuhl-Langseth M Holmén A Thormodsen R Øie M Rund BR . Relative stability of neurocognitive deficits in early onset schizophrenia spectrum patients. Schizophr Res. (2014) 156:241–7. doi: 10.1016/j.schres.2014.04.014
17
Thomsen P . Schizophrenia with childhood and adolescent onset—a nationwide register-based study. Acta Psychiatrica Scandinavica. (1996) 94:187–93. doi: 10.1111/j.1600-0447.1996.tb09847.x
18
Holmén A Juuhl-Langseth M Thormodsen R Melle I Rund BR . Neuropsychological profile in early-onset schizophrenia-spectrum disorders: measured with the MATRICS battery. Schizophr bulletin. (2010) 36:852–9. doi: 10.1093/schbul/sbn174
19
Kelleher I Clarke MC Rawdon C Murphy J Cannon M . Neurocognition in the extended psychosis phenotype: performance of a community sample of adolescents with psychotic symptoms on the MATRICS neurocognitive battery. Schizophr bulletin. (2013) 39:1018–26. doi: 10.1093/schbul/sbs086
20
Mohn C Sundet K Rund BR . The Norwegian standardization of the MATRICS (measurement and treatment research to improve cognition in schizophrenia) consensus cognitive battery. J Clin Exp neuropsychology. (2012) 34:667–77. doi: 10.1080/13803395.2012.667792
21
Stone WS Mesholam-Gately RI Giuliano AJ Woodberry KA Addington J Bearden CE et al . Healthy adolescent performance on the MATRICS Consensus Cognitive Battery (MCCB): developmental data from two samples of volunteers. Schizophr Res. (2016) 172:106–13. doi: 10.1016/j.schres.2016.02.003
22
Lai S Zhong S Wang Y Zhang Y Xue Y Zhao H et al . The prevalence and characteristics of MCCB cognitive impairment in unmedicated patients with bipolar II depression and major depressive disorder. J Affect Disord. (2022) 310:369–76. doi: 10.1016/j.jad.2022.04.153
23
Liang S Yu W Ma X Luo S Zhang J Sun X et al . Psychometric properties of the MATRICS Consensus Cognitive Battery (MCCB) in Chinese patients with major depressive disorder. J Affect Disord. (2020) 265:132–8. doi: 10.1016/j.jad.2020.01.052
24
Abdi H Molin P . Lilliefors/Van Soest’s test of normality. Thousand Oaks, CA: Sage (2007) p. 540–4.
25
Nitzburg GC DeRosse P Burdick KE Peters BD Gopin CB Malhotra AK . MATRICS cognitive consensus battery (MCCB) performance in children, adolescents, and young adults. Schizophr Res. (2014) 152:223–8. doi: 10.1016/j.schres.2013.11.023
26
Romine CB Reynolds CR . A model of the development of frontal lobe functioning: findings from a meta-analysis. Appl neuropsychology. (2005) 12:190–201. doi: 10.1207/s15324826an1204_2
27
Sowell ER Thompson PM Leonard CM Welcome SE Kan E Toga AW . Longitudinal mapping of cortical thickness and brain growth in normal children. J Neurosci. (2004) 24:8223–31. doi: 10.1523/JNEUROSCI.1798-04.2004
28
Sowell ER Thompson PM Toga AW . Mapping changes in the human cortex throughout the span of life. Neuroscientist. (2004) 10:372–92. doi: 10.1177/1073858404263960
29
Voyer D Voyer SD Saint-Aubin J . Sex differences in visual-spatial working memory: A meta-analysis. Psychonomic Bull review. (2017) 24:307–34. doi: 10.3758/s13423-016-1085-7
30
Catalan A De Pablo GS Aymerich C Damiani S Sordi V Radua J et al . Neurocognitive functioning in individuals at clinical high risk for psychosis: a systematic review and meta-analysis. JAMA Psychiatry. (2021) 78:859–67. doi: 10.1001/jamapsychiatry.2021.1290
31
Jonas K Lian W Callahan J Ruggero CJ Clouston S Reichenberg A et al . The course of general cognitive ability in individuals with psychotic disorders. JAMA Psychiatry. (2022) 79:659–66. doi: 10.1001/jamapsychiatry.2022.1142
32
Zhang T Wei Y Cui H Tang X Xu L Hu Y et al . Associations between age and neurocognition in individuals at clinical high risk and first-episode psychosis. Psychiatry Res. (2023) 327:115385. doi: 10.1016/j.psychres.2023.115385
Summary
Keywords
MCCB, adolescents, norms, schizophrenia, Chinese
Citation
Tan Y, Zong X, Li H, Feng M, He J, Sun X, Zhang Y, Wang X, Yao J and Hu M (2025) Establishment of local norms and standardization of the MATRICS consensus cognitive battery in Chinese adolescents. Front. Psychiatry 16:1675079. doi: 10.3389/fpsyt.2025.1675079
Received
28 July 2025
Accepted
02 September 2025
Published
17 September 2025
Volume
16 - 2025
Edited by
Tianhong Zhang, Shanghai Jiao Tong University, China
Reviewed by
Weiqing Liu, Tongji University, China
Lian Du, First Affiliated Hospital of Chongqing Medical University, China
Updates
Copyright
© 2025 Tan, Zong, Li, Feng, He, Sun, Zhang, Wang, Yao and Hu.
This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Maolin Hu, humaolin@whu.edu.cn
†These authors have contributed equally to this work
Disclaimer
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.