Abstract
Background:
The purpose of this study is to use a variety of machine learning (ML) algorithms to build a risk prediction model for nursing students’ social anxiety, select the optimal model, and identify risk factors.
Methods:
The cross-sectional survey was conducted among nursing students at 10 universities from September to December 2024. A total of 2024 nursing students were included in this study. Nine acceptable features were selected through Logistic analysis. We developed and evaluated seven ML models: Logistic regression (LR), Elastic net (EN), k-nearest neighbors (KNN), Decision tree (DT), Extreme gradient boosting (XGBoost), Support vector machine (SVM), Random forest (RF).
Results:
The area under the Area Under Curve (AUC: 0.71) of the random forest model was the highest among the 7 models that predicted nursing students’ social anxiety. The most important characteristics that predicted social anxiety in nursing students included Sleep condition, alexithymia, depression, education level, and religious belief.
Conclusion:
Our findings suggest that ML models, specifically random forests, can best predict the risk of social anxiety among nursing students.
Introduction
Social anxiety disorder is the third most common disorder in the general population (1).
Epidemiological studies have reported prevalence rates ranging between 7% and 13% in Western nations, while figures of approximately 10% and 11.7% have been documented in India and Saudi Arabia respectively (2). Social anxiety is defined as an irrational and excessive fear response elicited by interpersonal communication and social performance situations. This condition is characterized by intense affective manifestations (i.e., tension or distress) and is frequently accompanied by behavioral avoidance patterns in social contexts (3). Nursing is recognized as a profession in which significant emphasis is placed on social interaction and interpersonal relationships within clinical environments. Effective healthcare delivery in this field is dependent upon close communication and multidisciplinary collaboration being established among nurses, patients, caregivers, physicians, and allied health professionals (4). Nursing students often need to establish communication with teachers, doctors, patients, and their families during their internships, such as various operations, departmental assessment, health education for patients, and speaking in professional learning activities (5). Frequent exposure to these environments can easily lead to social anxiety. Rehab and Ahmad found in their research that the incidence of social anxiety among nursing students ranged from 28.15% to 47.5% (6, 7).
The presence of social anxiety in nursing students has been identified as a matter of particular concern due to its potential to impede the acquisition of essential clinical competencies, the establishment of therapeutic patient relationships, and effective participation in interdisciplinary healthcare teams. Furthermore, this condition has been associated with the development of multiple adverse psychological consequences, including diminished self-esteem, depressive symptoms, persistent fear responses, and feelings of social isolation (8, 9), as well as depression. The predictive validity of traditional scoring systems for social anxiety may be limited due to the multifactorial nature of its underlying mechanisms and the heterogeneity of contributing factors. This methodological constraint is attributed to the incorporation of an insufficient number of variables within conventional assessment frameworks. Machine learning (ML) algorithms are suitable for all types and sizes of data and have attracted great attention in developing patient-centered predictive/prognostic models (10). These models help optimize treatment plans and facilitate the monitoring and managing health conditions.
In our research, we chose the commonly used machine learning models: logistic regression (LR), elastic network (EN), K-nearest neighbor (KNN), decision tree (DT), extreme gradient enhancement (XGBoost), support vector Machine (SVM), and Random Forest (RF). The core of XGBoost is to adopt the integrated idea of boosting methods, generate weak learners by optimizing the structured loss function, and improve the performance of the algorithm through techniques such as pre-sorting and weighted quantiles to prevent overfitting. To improve the generalization ability of the model (11). SVM is used to construct a model for limited data, so that the model can achieve the effect of minimizing structural risk (12). During the process of model construction, the best compromise position is sought between the complexity of the function and the accuracy of data analysis, so as to obtain the best generalization ability (13). DT is a classic classification method, which is an algorithm for summarizing classification rules from the training dataset (14). This method has relatively low requirements for the data. As it divides the independent variables one by one, it has achieved remarkable results in fields such as classification, prediction, and rule extraction at present (14). EN is formed through training and learning from a large amount of source data and continuous iterative calculations. It can fit the nonlinear characteristics of the source data (15). Using this model, highly accurate predictions can be made for the characteristics of unknown data. KNN is a type of classification algorithm. It can supervise the machine to perform calculations and use Markov distance, Euclidean distance, etc., to minimize the similarity, thereby determining the classification of a certain data to be measured (16). Logistic regression is used to convert the result of a certain continuous value obtained by linear regression into a probability value with an interval, and then handle classification problems based on the obtained probability value (17). RF is an algorithm capable of fusing multiple decision trees and belongs to an ensemble algorithm (18). The operation is simple. Whether in the training process or parameter adjustment, it can be carried out quickly. The RF estimation error is combined to evaluate the fitting and prediction accuracy of the combined tree learner (19, 20). Grounded in the Health Ecological Model (21), which conceptualizes health outcomes as the product of multi-level and interacting factors, this study identified an initial set of feature variables for the ML models through a synthesis of this theoretical framework and a review of relevant literature (5, 22). We subsequently conducted a cross-sectional survey among nursing students to develop and test the applicability of ML models in predicting the risk of social anxiety. Furthermore, we analyzed and interpreted the importance of the input variables to identify the most significant predictors of social anxiety in this population.
Methods
Participants
The cross-sectional survey was conducted among nursing students at 10 universities in China from September to December 2024. Before distribution, the researchers explained the purpose of the study to all participants, informing them of the main content and confidentiality of the survey data. The nursing teachers distributed the electronic questionnaire; the informed consent statement was attached to the cover. Participants can only proceed with the survey if they agree, while those who refuse will be directed to an opt-out page. Informed consent was obtained from all participants. The study was done anonymously and voluntarily for 20 minutes. Before starting, this study was approved by the Biomedical Ethics Committee of China. We confirm that all procedures follow the relevant guidelines and regulations, including the Declaration of Helsinki. A total of 2,044 students completed the survey.
Inclusion criteria
(1) Nursing students; (2) Agree to participate in this study.
Exclusion criteria
(1) Physically disabled; (2) Those who ask for leave or are absent from classes during the investigation period;(3) Provided identical answers across all scale items; (4)Had missing data on key variables.
Sample size
Sample size was calculated based on the principle that event per variable (EPV) ≥ 10 (23). 18 variables were expected to be included in this study, considering a loss to follow-up rate of 10%-20%, so the minimum sample size for modeling was 178. Since the modeled sample size represents 70% of the total sample, the total sample size is at least 283. After applying listwise deletion to the initial 2,044 completed surveys to remove responses with missing data or uniform answering patterns, 2,024 valid cases were retained, yielding an effective response rate of 99.02%.
Ethical considerations
The Biomedical Ethics Committee approved the study of China and was conducted in accordance with the Declaration of Helsinki. All participants voluntarily agreed to participate and signed an informed consent form, and their personal information was anonymized. They were also informed of their right to refuse participation in the study at any stage.
Measures
Demographic characteristics
The general information questionnaire was developed based on the Grounded in the Health Ecological Model (21) and a comprehensive literature review (5, 22). It included key demographic and behavioral variables such as gender, age, educational level, clinical internship experience, and drinking habits, among others.
Center for epidemiological studies depression scale
Depressive symptoms among nursing students were assessed using the Center for Epidemiological Studies Depression Scale (CES-D). Developed in 1977, the CES-D is a widely used 20-item self-report instrument designed to screen for depressive symptomatology in the general population (24). Each item is rated on a 4-point Likert scale from 0 (“rarely or none of the time less than 1 day”) to 3 (“most or all of the time 5–7 days”), resulting in a total score ranging from 0 to 60. The scale encompasses four dimensions: depressed mood, positive mood, somatic complaints, and interpersonal difficulties. According to the established cutoff criteria (24), a total score of ≤ 15 indicates no significant depressive symptoms, 16–19 suggests possible mild depression, and ≥ 20 reflects specific depressive symptoms. This scale has been well-validated in Chinese university student populations, demonstrating satisfactory reliability and validity (25, 26). In the present study, the scale exhibited excellent internal consistency, with a Cronbach’s α of 0.964.
Social interaction anxiety scale
Social anxiety was assessed using the 15-item self-report scale compiled by Leary (27). This unidimensional instrument measures the subjective tendency toward social anxiety, independent of observable behavior. Items are rated on a 5-point Likert scale ranging from 1 (“not at all”) to 5 (“very consistent”), yielding a total score between 15 and 75, with a commonly used cutoff score of 45 indicating the presence of social anxiety symptoms (28). This instrument has been extensively used in Chinese university student samples, with established reliability and validity. In the present study, it showed good internal consistency, with a Cronbach’s α of 0.828.
Toronto alexithymia scale-26
This study adopted the Toronto Alexithymia Scale revised by Chinese scholar Professor Yao et al (29). The scale contains 26 questions and four dimensions: the ability to describe emotions, recognize and distinguish between emotions and body feelings, fantasy, and extroverted thinking. A 5-point scale is used, from 1 (strongly disagree) to 5 (strongly agree). A score of 26 to 51 without alexithymia, 52 to 61 with alexithymia tendency, and 62 to 130 with alexithymia (30). This instrument has been extensively used in Chinese university student samples, with established reliability and validity (29). In this study, the Cronbach’s α for the sample was 0.938.
Experimental environment
In this study, python 3.9.9 is used for all the experiments. The python dependency libraries used include: scikit-learn=1.3.2, pandas=2.1.4, numpy=1.26.3, XGBoost =2.0.3, matplotlib=3.9.4, shap=0.46.0.
Statistical analysis
Statistical analyses were performed using SPSS 27.0. Categorical variables are presented as frequencies and percentages (n, %). Between-group comparisons were conducted using Chi-square tests, while potential risk factors were identified through logistic regression analysis (P<0.05). The processing dataset split into a training set (70%) and a testing set (30%). We then use these preselected features into seven different ML models: logistic regression (LR), elastic network (EN), K-nearest neighbor (KNN), decision tree (DT), extreme gradient enhancement (XGBoost), support vector Machine (SVM), Random Forest (RF). For each model, we select a set of hyperparameters that maximize the AUC of the ROC on the training set by using a 5-fold Cross Validation and Grid Search method, thus ensuring optimal performance and efficient prediction and comparison of the test set. The models have been cross- Validated in five times to ensure robustness and reliability. Comparing the models, we select the best model based on the AUC values and create the Shapley Additive exPlanations (SHAP) interpreter to calculate the SHAP values, representing each feature’s contribution to the predicted results, and we draw a SHAP summary diagram of RF model to illustrate the effects of model features.
Results
General characteristics of the participants
A total of 2024 nursing students were investigated in this study, including 406 males and 1618 females. Among them, 25.74% were rated as socially anxious. Table 1 shows the baseline characteristics of the socially anxious group and the group without social anxiety. Two groups of patients were evaluated regarding education level, school type, Mother’s Educational Level, Single-person household, Sleep Condition, Religious Belief, Depression, and Alexithymia. The difference was statistically significant (P < 0.001). see Table 1.
Table 1
| Variables | Total | Social anxiety | χ² | P | |
|---|---|---|---|---|---|
| No | Yes | ||||
| Gender | 3.393 | 0.065 | |||
| Male | 406 | 316 | 90 | ||
| Female | 1618 | 1187 | 431 | ||
| Age(Years) | 3.017 | 0.221 | |||
| <20 | 1448 | 1061 | 387 | ||
| 20-23 | 553 | 423 | 130 | ||
| ≥24 | 23 | 19 | 4 | ||
| Ethnic Group | 0.089 | 0.776 | |||
| Han Chinese | 2003 | 1488 | 15 | ||
| Ethnic Minority | 21 | 15 | 6 | ||
| Educational Level | 6.846 | 0.009** | |||
| Associate Degree or Below | 1093 | 786 | 307 | ||
| Undergraduate Degree | 931 | 717 | 214 | ||
| School type | 8.940 | 0.003** | |||
| Public School | 962 | 685 | 277 | ||
| Private School | 1062 | 818 | 244 | ||
| Clinical Practicum | 0.130 | 0.718 | |||
| Yes | 752 | 555 | 197 | ||
| No | 1272 | 948 | 324 | ||
| Residence | 0.591 | 0.442 | |||
| Urban Area | 876 | 658 | 218 | ||
| Rural Area | 1148 | 845 | 303 | ||
| Household Monthly Income (∼) | 5.79 | 0.055 | |||
| ≥5000 | 641 | 497 | 144 | ||
| 2000-4000 | 861 | 632 | 229 | ||
| <2000 | 522 | 374 | 148 | ||
| Father’s Educational Level | 3.238 | 0.198 | |||
| Higher Education | 307 | 235 | 72 | ||
| High School | 455 | 348 | 107 | ||
| Junior High School or Below | 1262 | 920 | 342 | ||
| Mother’s Educational Level | 7.324 | 0.026* | |||
| Higher Education | 262 | 198 | 64 | ||
| High School | 336 | 268 | 68 | ||
| Junior High School or Below | 1426 | 1037 | 389 | ||
| Single-person household | 5.239 | 0.022* | |||
| Yes | 466 | 365 | 101 | ||
| No | 1558 | 1138 | 420 | ||
| Sleep Condition | 68.776 | <0.001*** | |||
| Excellent | 1222 | 977 | 245 | ||
| Fair | 627 | 432 | 195 | ||
| Poor | 175 | 94 | 81 | ||
| Smoking | 0.208 | 0.648 | |||
| Yes | 75 | 54 | 21 | ||
| No | 1949 | 1449 | 500 | ||
| Alcohol drinking | 0.029 | 0.865 | |||
| No | 1822 | 1354 | 468 | ||
| Yes | 202 | 149 | 53 | ||
| Religious Belief | 4.318 | 0.038* | |||
| Yes | 128 | 105 | 23 | ||
| No | 1896 | 1398 | 498 | ||
| Depression | 51.772 | <0.001*** | |||
| Yes | 1445 | 1137 | 308 | ||
| No | 579 | 366 | 213 | ||
| Alexithymia | 49.778 | <0.001*** | |||
| Yes | 362 | 322 | 40 | ||
| No | 1662 | 1181 | 481 | ||
| Sexual Orientation | 2.737 | 0.098 | |||
| Heterosexual | 1878 | 1403 | 475 | ||
| Sexual minority | 146 | 100 | 46 | ||
General characteristics of the participants.
*P<0.05, **P<0.01, ***P<0.001 .
Multivariate binary logistic regression analysis
Taking the occurrence of social anxiety among nursing students as the dependent variable (No=0, Yes=1), Educational Level (Associate Degree or Below =0, Undergraduate Degree=1), School type (Public School=0, Private School= 1), Mother’s Educational Level (Junior High School or Below =0, High school=1, Higher Education=2), Single-person household (No=0, Yes=1), Sleep Condition (Excellent=0, Fair=1, Poor=2) logistic regression analysis was conducted on Religious Belief (Yes=0, No=1), Depression (No=0, Yes=1), and Alexithymia (No=0, Yes=1). Multivariate binary logistic regression analysis found that the Undergraduate Degree (OR = 0.756, P = 0.009, 95%CI: 0.613 to 0.932) was a protective factor for social anxiety in nursing students. Poor Sleep Condition (OR = 1.637, P < 0.001, 95%CI: 1.399 to 0.916), Depression (OR = 2.093, P < 0.001, 95%CI: 1.690 to 2.592), Alexithymia (OR = 3.093, P < 0.001, 95%CI: 2.184 to 4.381) was a risk factor for social anxiety in nursing students, as shown in Table 2.
Table 2
| Risk factor | Reference factor | B | SE | Waldx2 | P | OR | 95%CI |
|---|---|---|---|---|---|---|---|
| Educational Level | Associate degree or below | ||||||
| Undergraduate Degree | -0.280 | 0.107 | 6.832 | 0.009 | 0.756 | 0.613 to 0.932 | |
| School type | Public school | ||||||
| Private School | -0.125 | 0.160 | 0.606 | 0.436 | 0.883 | 0.644 to 1.209 | |
| Mother’s Educational Level | Junior high school or below | ||||||
| Higher Education | 0.055 | 0.079 | 0.472 | 0.492 | 1.056 | 0.904 to 1.234 | |
| Single-person household | No | ||||||
| Yes | 0.172 | 0.137 | 1.587 | 0.208 | 1.188 | 0.909 to 1.553 | |
| Sleep Condition | Excellent | ||||||
| Poor | 0.493 | 0.080 | 37.686 | <0.001 | 1.637 | 1.399 to 1.916 | |
| Religious Belief | Yes | ||||||
| No | 0.486 | 0.236 | 4.243 | 0.039 | 1.626 | 1.024 to 2.583 | |
| Depression | No | ||||||
| Yes | 0.739 | 0.109 | 45.843 | <0.001 | 2.093 | 1.690 to 2.592 | |
| Alexithymia | No | ||||||
| Yes | 1.129 | 0.179 | 40.410 | <0.001 | 3.093 | 2.184 to 4.381 | |
Multivariate binary logistic regression analysis of social anxiety in nursing students.
Performance evaluation
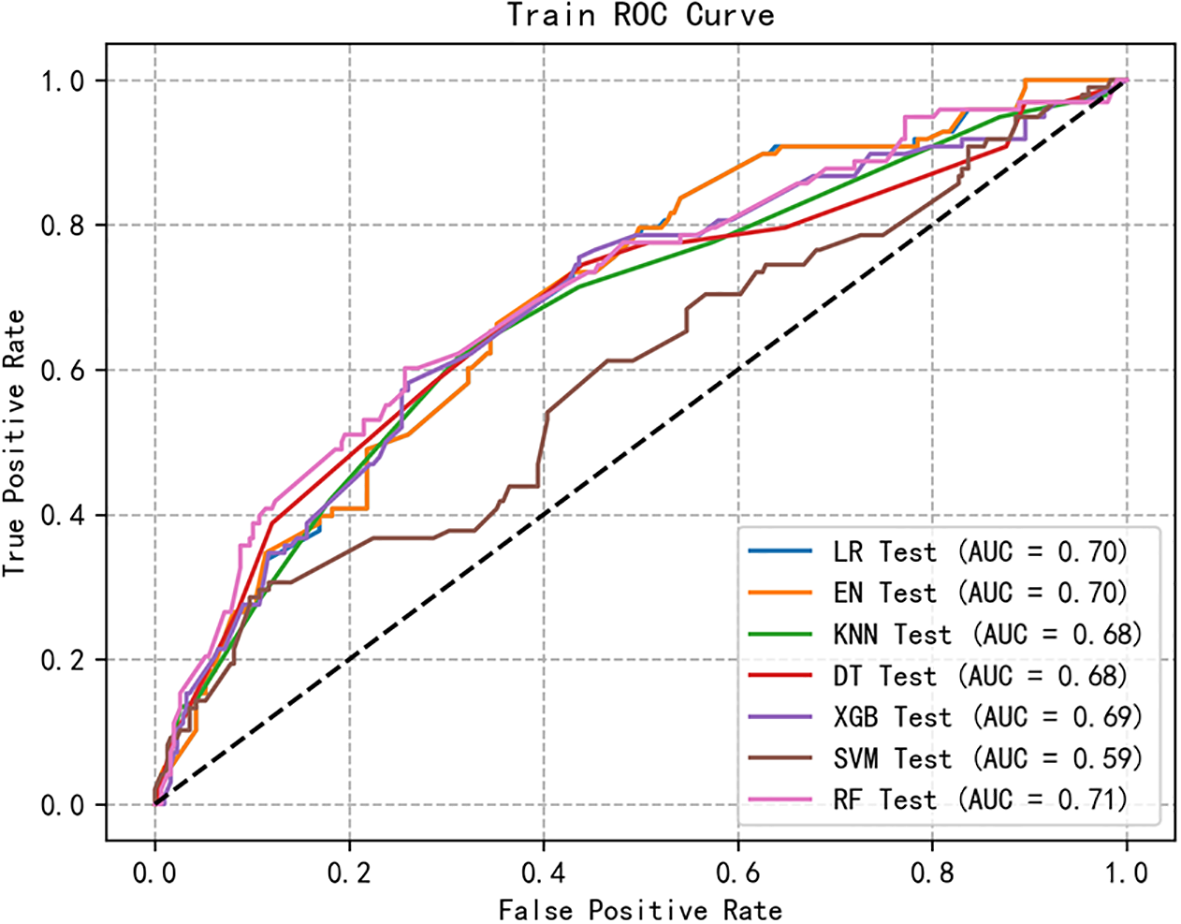
We retained five significant and highly correlated individual characteristics through Logistic correlation analysis. Using these five variables, we developed seven ML models to predict the risk of social anxiety in nursing students. Figures 1, 2 shows the ROC of all model test sets and validation sets, whose prediction and discrimination are represented by AUC. The test set RF model has the highest AUC (0.71), followed by LR (0.70), EN (0.70), XGBoost (0.69), KNN (0.68), DT (0.68), and SVM (0.59). DCA was used to evaluate the clinical applicability of all models further. DCA was used to assess the clinical efficacy of the prediction model. In most threshold ranges, RF partially or completely overlaps with other models, indicating no significant difference in net benefits, however, at about 0.2-0.4. Within the threshold range, the net benefit of the RF model is significantly higher than that of the other models (Figure 3). In addition, we calculated the accuracy, sensitivity, specificity and confusion matrices of all models (Table 3 and Appendix 1: Figures 1-7). The RF model had the highest accuracy at 0.763. Considering other indicators, the overall RF performance is better.
Figure 1

The receiver operating characteristic curves of 7 machine learning models in training set. LR, logistic regression; XGBoost, extreme gradient boosting; DT, decision tree; SVM, support vector machine; KNN, k-nearest neighbors; RF, random forest; EN, elastic net.
Figure 2
The receiver operating characteristic curves of 7 machine learning models in testing set. LR, logistic regression; XGBoost, extreme gradient boosting; DT, decision tree; SVM, support vector machine; KNN, k-nearest neighbors; RF, random forest; EN, elastic net.
Figure 3

DCA curves for seven machine learning models. LR, logistic regression; XGBoost, extreme gradient boosting; DT, decision tree; SVM, support vector machine; KNN, k-nearest neighbors; RF, random forest; EN, elastic net.
Table 3
| Prediction model | Accuracy | Precision | F1 | Sensitivity | Specificity | Recall | Balanced accuracy | 95%CI |
|---|---|---|---|---|---|---|---|---|
| Logistic regression (LR) training group | 0.742 | 0.542 | 0.154 | 0.090 | 0.973 | 0.090 | 0.622 | 0.603,0.684 |
| Logistic regression (LR) test group | 0.758 | 0.500 | 0.093 | 0.051 | 0.984 | 0.051 | ||
| Elastic net (EN) training group | 0.742 | 0.543 | 0.154 | 0.090 | 0.973 | 0.090 | 0.615 | 0.596,0.684 |
| Elastic net (EN) test group | 0.758 | 0.500 | 0.093 | 0.051 | 0.984 | 0.051 | ||
| k-nearest neighbors (KNN) training group | 0.746 | 0.597 | 0.163 | 0.095 | 0.977 | 0.095 | 0.583 | 0.592,0.668 |
| k-nearest neighbors (KNN) test group | 0.763 | 0.600 | 0.111 | 0.061 | 0.987 | 0.061 | ||
| Decision tree (DT) training group | 0.743 | 0.541 | 0.181 | 0.109 | 0.967 | 0.109 | 0.574 | 0.660,0.689 |
| Decision tree (DT) test group | 0.765 | 0.600 | 0.159 | 0.092 | 0.981 | 0.092 | ||
| Extreme gradient boosting (XGBoost) training group | 0.746 | 0.762 | 0.072 | 0.038 | 0.996 | 0.038 | 0.618 | 0.633,0.678 |
| Extreme gradient boosting (XGBoost) test group | 0.753 | 0.250 | 0.020 | 0.010 | 0.990 | 0.010 | ||
| Support vector machine (SVM) training group | 0.748 | 0.603 | 0.167 | 0.097 | 0.977 | 0.097 | 0.574 | 0.647,0.694 |
| Support vector machine (SVM) test group |
0.768 | 0.667 | 0.146 | 0.082 | 0.987 | 0.082 | ||
| Random forest (RF) training group | 0.749 | 0.615 | 0.192 | 0.114 | 0.975 | 0.114 | 0.616 | 0.627,0.682 |
| Random forest (RF) test group | 0.763 | 0.615 | 0.192 | 0.114 | 0.975 | 0.114 |
Comparison of prediction models.
Balanced Accuracy is mean recall across categories.
Feature importance ranking
To visually present the selected variables, we employ the best feature ranking to show the importance of each factor (Figure 4). Alexithymia significantly influenced model output, followed by sleep condition, depression, educational level, and religious belief. Figure 5 provides a more detailed view of the impact of each feature on individual predictions. Alexithymia exhibited a significant positive dose-response relationship, with SHAP values continuously increasing as scores rose. The negative impact on the model output is the greatest during periods of poor sleep quality. As the quality improves, this impact tends to stabilize. However, the effect sizes of depression, educational level, and religious belief are relatively small.
Figure 4
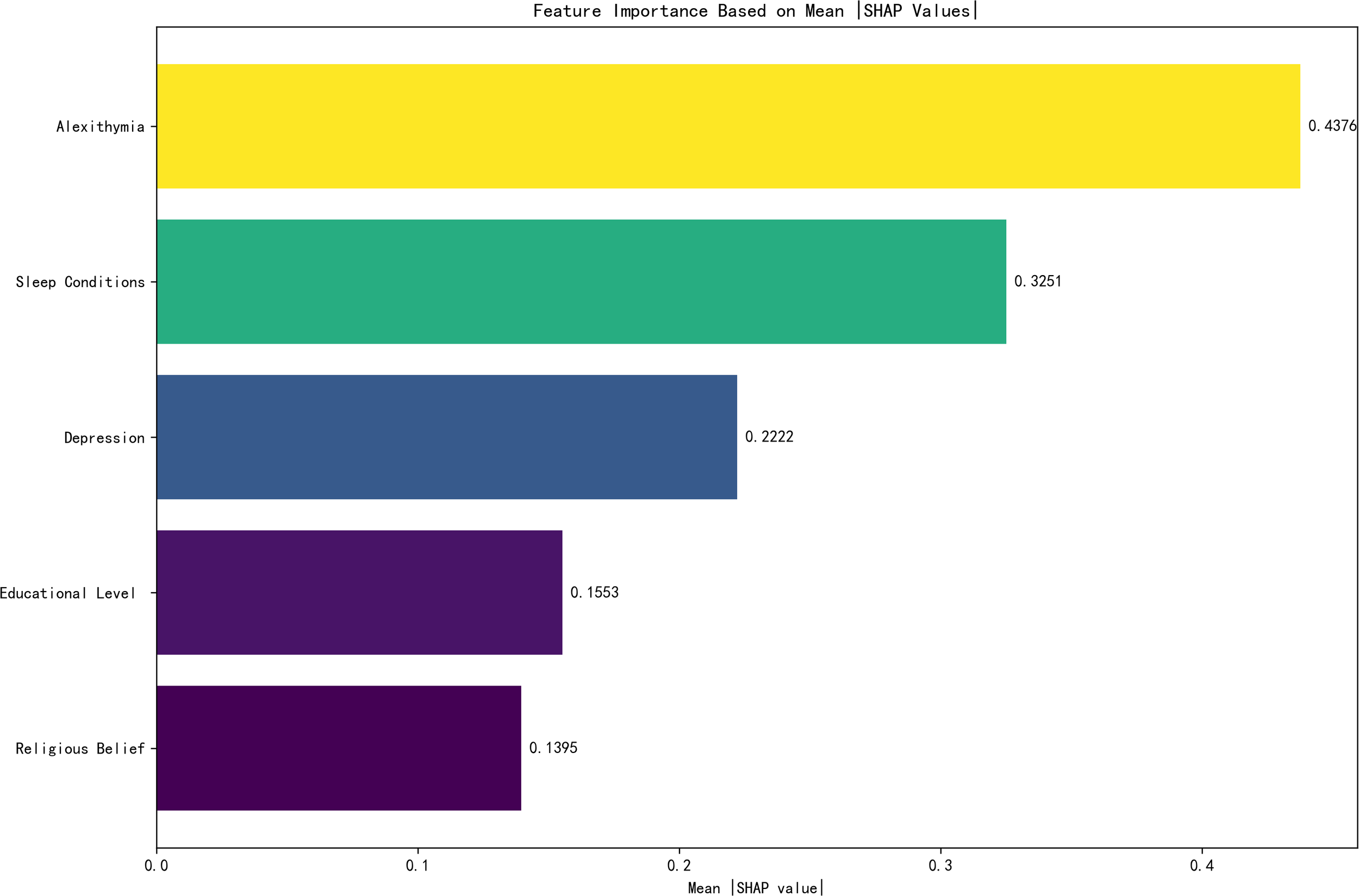
Feature importance ranking.
Figure 5
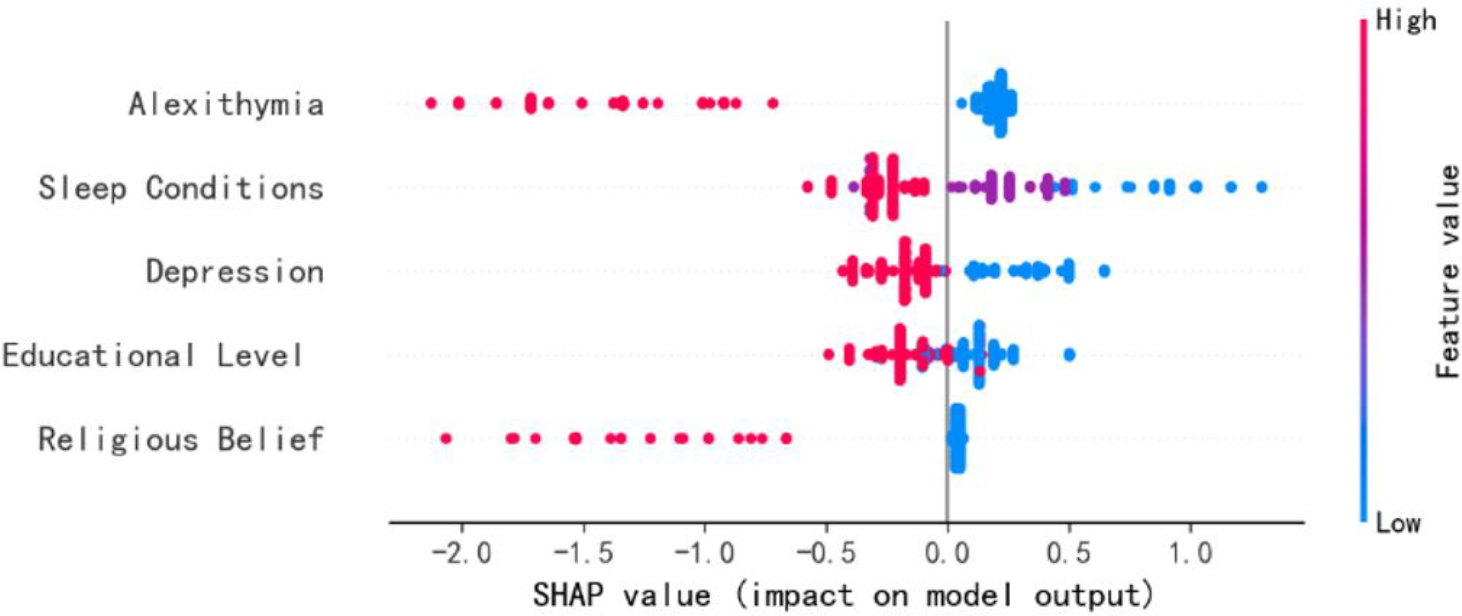
SHAP value (impact on model output).
Discussion
Our results found that the incidence of social anxiety among nursing students was 25.79%, which was lower than Wang’s (31) survey result (34.67%). However, it is still higher than Nader’s (32) meta-analysis of adolescents (17%). It shows that the social anxiety of nursing students is still at a high level. The nursing profession attaches more and more importance to the education and training of high social intelligence. Still, professional characteristics such as the imbalance of male and female ratio, traditional social concepts, low professional identity, and little emotional support lead to social anxiety. Secondly, when nursing students enter the clinical practice stage, they face a huge psychological impact, such as role identity change, and are easily exposed to different occasions and contact with other patients, so they become a group with a high incidence of social anxiety. Therefore, nursing educators and managers should conduct social anxiety assessments for nursing students in a timely manner and hold regular psychological lectures to reduce the occurrence of social anxiety among nursing students and promote their physical and mental health. In addition, in our study, we selected five acceptable traits and built seven ML models to predict the risk of social anxiety in nursing students. The RF model has the highest AUC and good clinical applicability among the seven models. The most important characteristics that predicted social anxiety in nursing students were sleep status, alexithymia, depression, education level, and religious affiliation.
Numerous studies have established that sleep disturbances—such as insomnia, nightmares, sleepwalking, and excessive daytime sleepiness—contribute to the onset, recurrence, and persistence of mental health issues (33, 34). While prior research has identified sleep condition as a factor influencing social anxiety among nursing students (35), our study further reveals that sleep status emerged as the second most important predictor of social anxiety in this population. This finding is supported by neurocognitive explanations suggesting that sleep deprivation alters neural network activity—for instance, heightening sensitivity in brain regions associated with signaling social rejection—which may subsequently promote social withdrawal and avoidance behaviors (36). Therefore, improving sleep quality should be regarded as a crucial component in strategies aimed at alleviating anxiety symptoms among nursing students.
Our findings identified alexithymia as the primary predictor of social anxiety among nursing students. Alexithymia is characterized by deficits in emotion awareness, including difficulties in identifying feelings, distinguishing between emotions and bodily sensations, reduced imaginative capacity, and an externally oriented cognitive style (37). According to the socio-formation mechanism, alexithymia originates from early childhood experiences and is reinforced through sociocultural and relational contexts (38). As a manifestation of impaired emotional cognition and regulation (39), alexithymia is considered a risk factor for various psychological issues and maladaptive behaviors (40–42). In social situations, individuals with high levels of alexithymia often appear indifferent or detached due to their limited ability to recognize and express emotions, which impedes the formation of healthy interpersonal relationships and exacerbates social anxiety (43). Moreover, their limited imaginative and introspective capacities lead to the use of maladaptive coping strategies—such as suppression—when facing stressful events or internal conflicts (44), further increasing anxiety and impairing empathy (45, 46). In light of these results, we recommend that educational institutions implement mental health initiatives—such as psychoeducational lectures, group counseling, and psychological workshops—to disseminate knowledge on emotional health and guide students in improving emotional expression, thereby potentially reducing the prevalence and impact of alexithymia.
Our findings are consistent with previous reports by Hou (47) and Ye (48), reinforcing depression as a significant predictor of social anxiety among nursing students. In our analysis, it was ranked as the third most influential feature. Clinically defined by persistent sadness, hopelessness, and anhedonia (49), depression is theorized to drive dysfunctional social behaviors through excessive negative interpretation biases (50). The stress resulting from these impaired interactions is hypothesized to further consolidate such biased cognitive patterns, potentially creating a self-sustaining cycle of cognitive and social impairment (50). In addition, our study found that educational level is a factor affecting the social anxiety of nursing students, and the incidence of social anxiety among professional nursing students is significantly higher than that of undergraduate nursing students. On the one hand, postgraduates’ sense of social efficacy gradually increases with age, thus promoting the development of social ability. On the other hand, graduate students are more involved in social activities and work and are more exposed to social situations. Exposure itself will bring about the desensitization effect of social anxiety (51). Secondly, the junior college system is shorter than the undergraduate system. Theoretically, junior college nursing students spend less time in school than undergraduate nursing students, and their theoretical knowledge and skill levels are often slightly inferior. Moreover, junior college nursing students are younger, so they are prone to lack confidence in clinical practice, leading to social anxiety in nursing students. Our results show that whether nursing students have religious beliefs or not is a factor affecting the social anxiety of nursing students. Religious belief is a kind of “kernel” promoting factor. On the level of social relations, social support is a kind of “external” support factor, and the two work together in people’s spiritual world (52). At the same time, the concept of “being kind to others and living in harmony” in religious teachings will enable individuals to achieve harmonious coexistence between people in daily life and thus obtain more social support, thereby reducing the social anxiety of nursing students (52). In addition, the influence of faith on subjective well-being cannot be ignored. Religious belief has a guiding function on individual thoughts and behaviors, and the spiritual protection function of religious culture is conducive to making human beings perceive happiness, thus reducing the psychological pressure on nursing students in interpersonal communication (53). Therefore, school teachers or clinical teachers should pay more attention to the psychological dynamics of nursing students in practice, give psychological assessments to nursing students in time, pay attention to the characteristics of specialized nursing students, encourage the improvement of their academic qualifications, teach nursing students with different educational levels according to their aptitude, pay attention to the cultivation of their interpersonal skills, improve their ability to deal with things and their ability to withstand pressure and reduce their social anxiety.
Strengths & limitations
To our knowledge, this study is the first to construct and compare the performance of seven different social anxiety risk prediction models for nursing students. In addition, our survey was a multicenter large-sample survey of 2,024 nursing students and combined machine learning techniques with demographic characteristics to predict nursing students’ social anxiety. However, some limitations to our study should not be ignored. First, the data sets used in this study are mostly self-dependent self-reports of nursing students, and the obtained data has certain errors. Second, because this study is cross-sectional, it cannot show causality, which is different from longitudinal research. Our model ignores social and behavioral factors, such as social support and lifestyle, critical to understanding social anxiety outcomes among nursing students. Incorporating these factors in future studies could enhance the power of the model. Finally, the dataset used in this study may have a situation of class imbalance. Although we have tried various methods to alleviate this problem (such as oversampling, undersampling, SMOTE, etc.), it still limits the effective prediction of the model. Future research can attempt other models, reinforcement learning, to further clarify the results of this study. The dataset used for modeling suffered from class imbalance, meaning there was a significant disparity in the ratio between high-risk and low-risk individuals for social anxiety. This may have influenced the estimation of certain performance metrics, such as the AUC. Although we comprehensively evaluated the models using multiple metrics (including Precision, Recall, and F1-Score) to mitigate this concern, future studies should seek to validate our models in larger and more balanced samples.
Conclusion
The RF model has good clinical applicability and is expected to become an effective auxiliary tool for psychological screening of nursing students. Among the included variables, sleep state and alexithymia are the two most significant factors affecting the output of the RF model. However, the validity of this model in the external cohort and its potential to reduce social anxiety among nursing students remains to be determined.
Statements
Data availability statement
The original contributions presented in the study are included in the article/Supplementary Material. Further inquiries can be directed to the corresponding author.
Ethics statement
The studies involving humans were approved by The Biomedical Ethics Committee approved the study of Xianning Vocational Technical College (2024R051-E01) and was conducted in accordance with the Declaration of Helsinki. The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
Author contributions
FW: Writing – original draft, Methodology, Investigation, Resources, Conceptualization, Writing – review & editing. PX: Investigation, Funding acquisition, Writing – original draft, Methodology. YH: Writing – original draft, Investigation, Funding acquisition, Methodology, Writing – review & editing. LL: Writing – review & editing, Methodology, Writing – original draft, Funding acquisition, Investigation, Resources. LK: Writing – review & editing, Funding acquisition, Methodology, Software. FY: Writing – review & editing, Funding acquisition, Methodology, Writing – original draft, Investigation, Software.
Funding
The author(s) declare that no financial support was received for the research and/or publication of this article.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Generative AI statement
The author(s) declare that no Generative AI was used in the creation of this manuscript.
Any alternative text (alt text) provided alongside figures in this article has been generated by Frontiers with the support of artificial intelligence and reasonable efforts have been made to ensure accuracy, including review by the authors wherever possible. If you identify any issues, please contact us.
Correction note
This article has been corrected with minor changes. These changes do not impact the scientific content of the article.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpsyt.2025.1721618/full#supplementary-material.
References
1
Hajure M Tariku M Abdu Z . Prevalence and associated factors of social phobia among college of health science students, mettu town, southwest Ethiopia 2019; institutional based cross-sectional study. Open Public Health J. (2020) 13:373–9. doi: 10.2174/1874944502013010373
2
Alkhalifah A Alsalameh N Majed A . Prevalence of social phobia among medical students in Saudi Arabia. Egyptian J Hosp Med. (2017) 69:2412–6. doi: 10.12816/0041685
3
Regier DA Kuhl EA Kupfer DJ . The DSM-5: Classification and criteria changes. World Psychiatry. (2013) 12:92–8. doi: 10.1002/wps.20050
4
Lau Y Wang W . Development and evaluation of a learner-centered training course on communication skills for baccalaureate nursing students. Nurse Educ Today. (2013) 33:1617–23. doi: 10.1016/j.nedt.2013.02.005
5
Ye Y Wan J Yue X Ni J . Systematie evaluation on status quo of social anxiety of nursing students in China and its characteristies. Chin Nurs Res. (2017) 31:18–21.
6
Alhazmi R . The association between social anxiety disorder and parenting style among nursing students. BMC Nurs. (2024) 23:920. doi: 10.1186/s12912-024-02584-7
7
Ayed A Abu Ejheisheh M Batran A Albashtawy M Salameh WA Obeyat AH et al . Relationship between social anxiety and self-esteem among undergraduate nursing students. Inquiry. (2024) 61:469580241276146. doi: 10.1177/00469580241276146
8
Oren-Yagoda R Melamud-Ganani I Aderka IM . All by myself: Loneliness in social anxiety disorder. J Psychopathol Clin Sci. (2022) 131:4–13. doi: 10.1037/abn0000705
9
Annoni AM Petrocchi S Camerini AL Marciano L . The relationship between social anxiety, smartphone use, dispositional trust, and problematic smartphone use: A moderated mediation model. Int J Environ Res Public Health. (2021) 18:2452. doi: 10.3390/ijerph18052452
10
Wei Z Li M Zhang C Miao J Wang W Fan H . Machine learning-based predictive model for post-stroke dementia. BMC Med Inform Decis Mak. (2024) 24:334. doi: 10.1186/s12911-024-02752-4
11
Deng X Li M Deng S Wang L . Hybrid gene selection approach using XGBoost and multi-objective genetic algorithm for cancer classification. Med Biol Eng Comput. (2022) 60:663–81. doi: 10.1007/s11517-021-02476-x
12
Cortes C Vapnik V . Support-vector networks. Mach Learning. (1995) 20:273–97. doi: 10.1023/A:1022627411411
13
Kai C Yugiong Z . A review of machine learning and its related algorithms. Stat & Inf Forum. (2007), 105–12.
14
Breiman L . Random forests. Mach Learning. (2001) 45:5–32. doi: 10.1023/A:1010933404324
15
Peng HX Luo YS Yu M . A creep constitutive model of TC11 titanium alloy based on BPNN. J Cent South Univ Forestry Technology. (2011) 31:183–6. doi: 10.14067/j.cnki.1673-923x.2011.12.007
16
Augusta G Hakim L Zainal A Tannady H . Identification of lampung script using K-neighbor, manhattan distance and population matrix algorithm. J Physics: Conf Series. (2021) 1933:012064. doi: 10.1088/1742-6596/1933/1/012064
17
Pang B Song Y Zhang C Wang H Yang R . Autonomous task allocation in a swarm of foraging robots: an approach based on response threshold sigmoid model. Int J Control Automation Systems. (2019) 17:1031–1040. doi: 10.1007/s12555-017-0585-1
18
Lei Y Tang R Xu J Zhang B Liu J Liang C et al . Construction of a novel risk model based on the random forest algorithm to distinguish pancreatic cancers with different prognoses and immune microenvironment features. Bioengineered. (2021) 12:3593–602. doi: 10.1080/21655979.2021.1951527
19
Nikolaou V Massaro S Garn W Fakhimi M Stergioulas L Price D . The cardiovascular phenotype of Chronic Obstructive Pulmonary Disease (COPD): Applying machine learning to the prediction of cardiovascular comorbidities. Respir Med. (2021) 186:106528. doi: 10.1016/j.rmed.2021.106528
20
Gomes Marques de Freitas A Almir Cavalcante Minho L Elizabeth Alves de Magalhães B Nei Lopes Dos Santos W Soares Santos L Augusto de Albuquerque Fernandes S . Infrared spectroscopy combined with random forest to determine tylosin residues in powdered milk. Food Chem. (2021) 365:130477. doi: 10.1016/j.foodchem.2021.130477
21
Qiuyu P Yinlong L Chenyao M Jinpeng Z Jun H . Research progress in health ecology. JJining Med Univ. (2022) 45:229–33.
22
Jia Y Yue Y . Influencing factors of social anxiety of undergraduate nursing students based on random forest model: A cross-sectional study. Nurs Open. (2025) 12:e70137. doi: 10.1002/nop2.70137
23
Ogundimu EO Altman DG Collins GS . Adequate sample size for developing prediction models is not simply related to events per variable. J Clin Epidemiol. (2016) 76:175–82. doi: 10.1016/j.jclinepi.2016.02.031
24
Radloff LS . The CES-D Scale: A self-report depression scale for research in the general population. Appl psychol Measurement. (1977) 1:385–401. doi: 10.1177/014662167700100306
25
Jiang L Wang Y Zhang Y Li R Wu H Li C et al . The reliability and validity of the center for epidemiologic studies depression scale (CES-D) for chinese university students. Front Psychiatry. (2019) 10:315. doi: 10.3389/fpsyt.2019.00315
26
Niu L He J Cheng C Yi J Wang X Yao S . Factor structure and measurement invariance of the Chinese version of the Center for Epidemiological Studies Depression (CES-D) scale among undergraduates and clinical patients. BMC Psychiatry. (2021) 21:463. doi: 10.1186/s12888-021-03474-x
27
Leary MR . Social anxiousness: the construct and its measurement. J Pers Assess. (1983) 47:66–75. doi: 10.1207/s15327752jpa4701_8
28
Meijia L . Secondary vocational school students interpersonal trust, social anxiety status and their relationship. ChinaJournal Health Psychol. (2014) 22:1721–3. doi: 10.13342/j.cnki.cjhp.2014.11.048
29
Ya LM . The preliminary surveying of bermond vorst alexithymia scale of Chinese version in China. Henan University. (2014).
30
Xiaoxu C Maoxin H Dimu T Fengli X . Assessment of alexithymia, anxiety and the impact on quality of life in patients with chronic eczema. Chin J Derm Venereol. (2023) 37:1378–84. doi: 10.13735/j.cjdv.1001-7089.202305010
31
Zixuan W Yijun Z Ying W Zhenqing Y Chujie L Feifei H . Mediating effect of social anxiety on relationship between social network addiction and sleep quality among undergraduate nursing students. Occup Health. (2024) 40:381–4. doi: 10.13329/j.cnki.zyyjk.2024.0055
32
Salari N Heidarian P Hassanabadi M Babajani F Abdoli N Aminian M et al . Global prevalence of social anxiety disorder in children, adolescents and youth: A systematic review and meta-analysis. J Prev (2022). (2024) 45:795–813. doi: 10.1007/s10935-024-00789-9
33
Baglioni C Battagliese G Feige B Spiegelhalder K Nissen C Voderholzer U et al . Insomnia as a predictor of depression: a meta-analytic evaluation of longitudinal epidemiological studies. J Affect Disord. (2011) 135:10–9. doi: 10.1016/j.jad.2011.01.011
34
Reeve S Sheaves B Freeman D . The role of sleep dysfunction in the occurrence of delusions and hallucinations: A systematic review. Clin Psychol Rev. (2015) 42:96–115. doi: 10.1016/j.cpr.2015.09.001
35
Yuan W Chen L Wu Y Su B Liu J Zhang Y et al . Sleep time and quality associated with depression and social anxiety among children and adolescents aged 6–18 years, stratified by body composition. J Affect Disord. (2023) 338:321–8. doi: 10.1016/j.jad.2023.06.029
36
Ben Simon E Walker MP . Sleep loss causes social withdrawal and loneliness. Nat Commun. (2018) 9:3146. doi: 10.1038/s41467-018-05377-0
37
Taylor GJ Bagby RM Parker JD . The alexithymia construct. A potential paradigm psychosomatic Med Psychosomatics. (1991) 32:153–64. doi: 10.1016/s0033-3182(91)72086-0
38
Chunyu Z Jinfu Z Jingqiu Z Pingping Z . Cognitive and social mechanisms of Alexithymia. Adv psychol Sci. (2011) 19:398–409.
39
Taylor GJ Bagby RM Parker JDA . Disorders of affect regulation: Alexithymia in medical and psychiatric illness. New York, NY, US: Cambridge University Press (1997) p. 359–xxii.
40
Bankier B Aigner M Bach M . Alexithymia in DSM-IV disorder: comparative evaluation of somatoform disorder, panic disorder, obsessive-compulsive disorder, and depression. Psychosomatics. (2001) 42:235–40. doi: 10.1176/appi.psy.42.3.235
41
De Gucht V Heiser W . Alexithymia and somatisation: quantitative review of the literature. J Psychosom Res. (2003) 54:425–34. doi: 10.1016/S0022-3999(02)00467-1
42
Luminet O Rimé B Bagby RM Taylor GJ . A multimodal investigation of emotional responding in alexithymia. Cogn Emotion. (2004) 18:741–66. doi: 10.1080/02699930341000275
43
Jingjing H Shanshan Z lianhuan X . Latent classes of alexithymia in college students and depressive symptoms, social interaction anxiety. Chin J Sch Health. (2021) 42:1838–41. doi: 10.16835/j.cnki.1000-9817.2021.12.019
44
Lulu X Yuan J Ping F . Alexithymia and interpersonal relations in middle school students: a moderated mediation model. psychol Dev Education. (2021) 37:92–100. doi: 10.16187/j.cnki.issn1001-4918.2021.01.12
45
Chen J Xu T Jing J Chan RCK . Alexithymia and emotional regulation: A cluster analytical approach. BMC Psychiatry. (2011) 11:33. doi: 10.1186/1471-244X-11-33
46
Nicolò G Semerari A Lysaker PH Dimaggio G Conti L D’Angerio S et al . Alexithymia in personality disorders: correlations with symptoms and interpersonal functioning. Psychiatry Res. (2011) 190:37–42. doi: 10.1016/j.psychres.2010.07.046
47
Hou J Juinge Xiaoyi F . Mobile phone addiction and depression: the multi-mediating role of social anxiety and attentional bias of negative emotional information. Acta Psychologica Sin. (2021) 53:362–73. doi: 10.3724/SP.J.1041.2021.00362
48
Baojuan Y Tingting M . The relationship between social support and depression in college students: a moderated mediating model. Psychol Exploration. (2020) 40:465–71. doi: 10.1017/S0033291715002044
49
WHO . Depressive disorder (depression) (2023). Available online at: https://www.who.int/news-room/fact-sheets/detail/depression (Accessed May 2, 2025).
50
Wittenborn AK Rahmandad H Rick J Hosseinichimeh N . Depression as a systemic syndrome: mapping the feedback loops of major depressive disorder. Psychol Med. (2016) 46:551–62. doi: 10.1017/S0033291715002044
51
Jing X Houcan Z . A study on interpersonal efficacy of college students. psychol Res. (2008) 1:67–71.
52
Shuang Z Dawa Ruoyu Y . Religious belief, social support and residents’ happiness: An empirical study based on CGSS2015 data. THE World RELIGIOUS CULTURES. (2018), 83–7.
53
Wei L . Religious belief, economic income and subjective well-being of urban and rural residents. Agrotechnical economy. (2016), 98–110. doi: 10.13246/j.cnki.jae.2016.07.010
Summary
Keywords
nursing students, social anxiety, machine learning, prediction model, random forest
Citation
Wang F, Xu P, Huang Y, Liu L, Kong L and Yang F (2025) Social anxiety prediction model for nursing students based on machine learning: a cross-sectional survey. Front. Psychiatry 16:1721618. doi: 10.3389/fpsyt.2025.1721618
Received
09 October 2025
Revised
11 November 2025
Accepted
21 November 2025
Published
12 December 2025
Corrected
23 December 2025
Volume
16 - 2025
Edited by
Yang Sun, Shenyang Normal University, China
Reviewed by
Ikram E. Khuda, Iqra University, Pakistan
Cheng Liu, Jiangsu Vocational Institute of Commerce, China
Updates
Copyright
© 2025 Wang, Xu, Huang, Liu, Kong and Yang.
This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Liuliu Kong , 2646706150@qq.com
Disclaimer
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.