 Magdalena Buckert1*†
Magdalena Buckert1*† Carmen Streibel1
Carmen Streibel1 Mechthild Hartmann1
Mechthild Hartmann1 Nelly Monzer1
Nelly Monzer1 Stefan Kopf2
Stefan Kopf2 Julia Szendrödi2,3
Julia Szendrödi2,3 Beate Wild1*
Beate Wild1*- 1Department of General Internal Medicine and Psychosomatics, University Hospital Heidelberg, Heidelberg, Germany
- 2Department of Medicine I and Clinical Chemistry, University Hospital Heidelberg, Heidelberg, Germany
- 3German Center for Diabetes Research (DZD), Heidelberg, Germany
Introduction: Increasing evidence supports chronic psychological stress as a risk factor for the development of type 2 diabetes. Much less is known, however, about the role of chronic stress in established diabetes.
Methods: The aim of the current study was to comprehensively assess chronic stress in a sample of 73 patients with type 2 diabetes and 48 non-diabetic control participants, and to investigate associations with indicators of glycemic control (HbA1c), insulin resistance (HOMA-IR), β-cell functioning (C-peptide), illness duration, and the presence of microvascular complications. Chronic stress was measured using questionnaires [the Perceived Stress Scale (PSS), the Screening Scale of the Trier Inventory of Chronic Stress (SSCS), the Perceived Health Questionnaire (PHQ) as well as the Questionnaire on Stress in Patients with Diabetes—Revised (QSD-R)]; hair cortisol was used as a biological indicator.
Results: We found that patients with type 2 diabetes had higher levels of hair cortisol in comparison to the control group (F(1,112) = 5.3; p = 0.023). Within the diabetic group, higher hair cortisol was associated with a longer duration of the illness (r = 0.25, p = 0.04). General perceived stress did not show significant associations with metabolic outcomes in type 2 diabetes patients. In contrast, higher diabetes-related distress, as measured with the QSD-R, was associated with lower glycemic control (r = 0.28, p = 0.02), higher insulin resistance (r = 0.26, p = 0.03) and a longer duration of the illness (r = 0.30, p = 0.01).
Discussion: Our results corroborate the importance of chronic psychological stress in type 2 diabetes. It appears, however, that once type 2 diabetes has developed, diabetes-specific distress gains in importance over general subjective stress. On a biological level, increased cortisol production could be linked to the course of the illness.
1 Introduction
Psychological stress is increasingly recognized as a risk factor for the development of type 2 diabetes. On the other hand, living with a diagnosis of diabetes is also known to be stressful as it requires compliance with the treatment regimen and is related to both fear of hypoglycemia and worries about the future. These aspects are captured by the concept of diabetes distress (1). Higher levels of diabetes distress have been linked to higher HbA1c cross-sectionally [(e.g., 2, 3)], whereas results of prospective studies are mixed (4, 5). Conversely, psychological interventions that target diabetes distress were able to improve the HbA1c (6, 7). Higher levels of diabetes distress have also been found in diabetes patients with complications in some (8, 9), but not all studies (10).
Endocrine dysregulation (specifically regarding cortisol secretion) has been proposed as a biological mechanism linking chronic psychological stress and diabetes (11). For instance, elevated levels of cortisol stimulate gluconeogenesis, lipolysis with the release of free fatty acids as well as the accumulation of visceral fat (11). Hair cortisol concentration (HCC) is used to assess long-term integrated cortisol production, and thus is unbiased by circadian variations of cortisol secretion. In fact, HCC has been found to be higher among patients with diabetes compared to non-diabetic participants (12, 13).
Less is known, however, about the relationship between chronic psychological stress, HCC, and diabetic complications in established type 2 diabetes. However, illness burden in diabetes stems mainly from complications; complications increase not only morbidity, but also mortality (14). It should be noted that strict glycemic control cannot prevent the development of diabetic complications (15). It is therefore of the utmost importance that the determinants of diabetic complications be uncovered.
Diabetic complications comprise micro- and macrovascular damages. Macrovascular complications include coronary artery disease, peripheral arterial disease, and stroke (16). Microvascular damages are diabetes-specific and include diabetic nephropathy, neuropathy, and retinopathy. Endothelial dysfunction has been uncovered as a main determinant of diabetic vascular complications (17). In pre-diabetic patients, increased inflammation and oxidative stress have been reported to impair endothelial function (18). Interestingly, chronic stress also promotes a pro-inflammatory state as well as oxidative stress, and may thus affect endothelial function through the same mechanisms (19). Another mechanism affecting blood vessels involves insulin resistance, increasing cardiovascular risk even without a diagnosis of diabetes (20). Insulin resistance might also be increased by chronic psychological stress through several molecular pathways including the hypothalamus-pituitary–adrenal (HPA) axis and the autonomic nervous system, as well as other physiological systems (11, 21).
The aim of the current study was to investigate the association of both chronic psychological stress and diabetes distress with (a) diabetes-specific metabolic outcomes, and (b) the presence of diabetic microvascular complications. Psychological stress was assessed comprehensively by using questionnaire data and hair cortisol as a biological indicator of chronic stress. HbA1c, the HOMA index, and levels of C-peptide were measured as metabolic outcomes.
2 Method
2.1 Sample
The study sample consisted of 127 participants who were recruited within the context of a larger study through the diabetes outpatient clinic of the University Hospital of Heidelberg, announcements in libraries, pharmacies and other public places, as well as newspaper advertisements. Eligibility for participation in the study was based on the following: that participants were between 40 and 80 years of age, had sufficient speech comprehension, and reading/writing ability without assistance. Smoking more than 10 cigarettes per day, use of illegal drugs, and regular consumption of more than three alcoholic beverages per day were also exclusion criteria [for further details (see 22, 23)]. Control participants were eligible for inclusion if they reported no current or past diagnosis of diabetes and no other current chronic or acute medical condition. The control participants were matched to the patients on the basis of mean age and gender distribution, ensuring that the two groups were similar in this regard. Six persons were excluded from analysis due to non-compliance to the study requirements (n = 4) and having had bariatric surgery (n = 2). Of the remaining 121 participants, 73 had a physician-confirmed diagnosis of type 2 diabetes. Of these, 57 had microvascular complications—defined as described (Table 1 provides the characteristics of the sample).
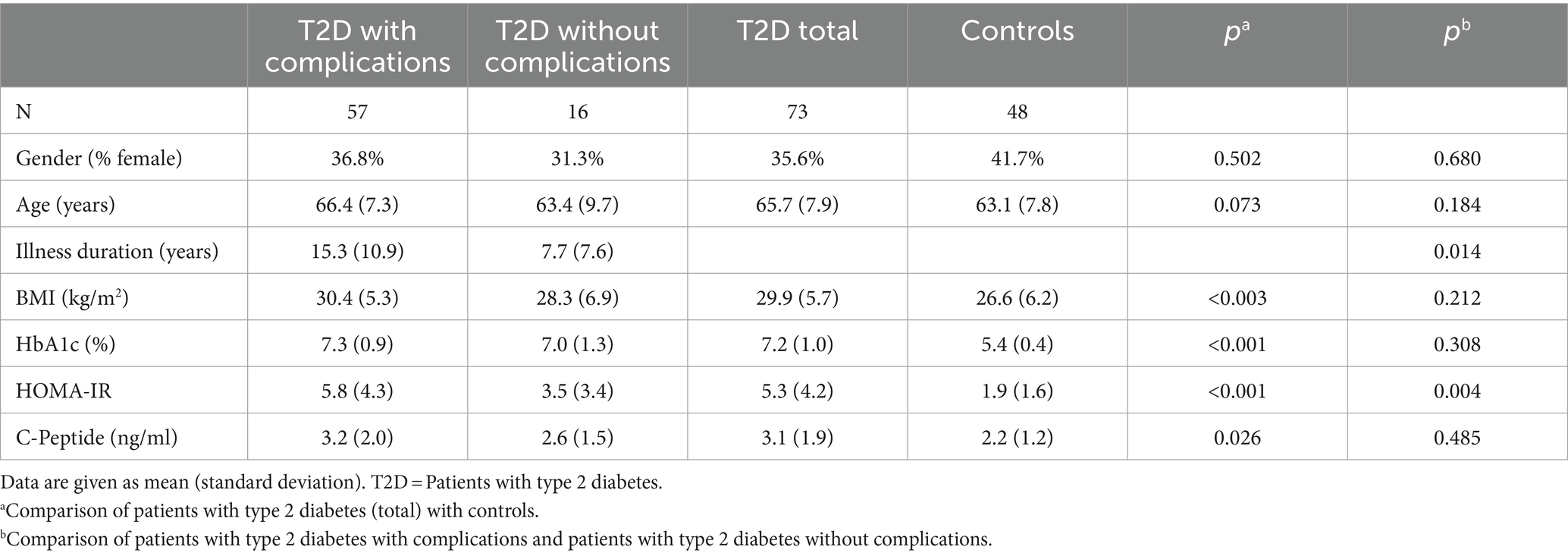
Table 1. Characteristics of the sample.
2.2 Procedure
The study was approved by the local ethics committee of the University Hospital of Heidelberg (S-019/2017). All examinations were conducted at the University Hospital of Heidelberg, starting between eight and ten a.m. Participants were examined after an overnight fast. After providing written informed consent, an indwelling catheter was inserted; they then completed several questionnaires including those assessing chronic subjective stress (please see below). Approximately one hour after the beginning of the study, blood samples were taken. Later on a hair sample was collected [additional details regarding the study protocol are described elsewhere (22)].
2.3 Definition of complications
In patients with type 2 diabetes, information regarding retinopathy, nephropathy, and peripheral neuropathy was obtained from their medical record, or if not available, by an additional medical examination performed in the diabetes outpatient clinic of the University Hospital of Heidelberg. The examination included funduscopy, assessment of the albumin-creatinine ratio in urine, and questionnaires about neuropathy [(see 22), for details].
2.4 Metabolic parameters and serum cortisol
Glycated hemoglobin (HbA1c), homeostatic model assessment of insulin resistance (HOMA-IR), C-peptide, and serum cortisol were analyzed in the accredited central laboratory of the University Hospital of Heidelberg using standard operating procedures according to the manufacturers’ instructions. Whole blood samples were centrifuged at 3,500 g for ten minutes. Plasma and serum samples were either analyzed directly or stored at −20°C before analysis. C-peptide was analyzed on a Siemens Immulite 2000 Immunoassay System (reagents kit L2KPEP2). Cortisol and insulin were analyzed on a Siemens ADVIA Centaur XPT Immunoassay System (reagents kits 04344187 and 02230141, respectively). HOMA-IR was calculated according to the formula insulin (mU/l) × glucose (mg/dl)/405. HbA1c was analyzed by HPLC (Variant II Turbo, Bio-Rad).
2.5 Hair cortisol
A small, three centimeter long sample of scalp-near occipital hair was collected and sent to the laboratory of Prof. Kirschbaum (Dresden, Germany) for analysis of hair cortisol concentration (HCC). Given an average hair growth rate of 1 cm/month, this reflects an integrated retrospective measure of the cortisol output of the past three months (24). HCC was determined with a commercially available immunoassay with chemiluminescence detection (CLIA, IBL-Hamburg, Germany), employing the protocol of Davenport et al. (25) (the intraassay and interassay-coefficient of variance of this assay is below 8%). In conjunction with hair sampling, a protocol was filled in to assess hair washing frequency and hair treatment (i.e., hair dying, hair coloring, or permanent wave). For statistical analysis, a dichotomous variable for hair treatment (yes/no) was built.
2.6 Questionnaires
For the assessment of psychosocial stress, various questionnaires were applied that measure different aspects of stress. All questionnaires show a good reliability and validity (26–28). The German 14-item perceived stress scale PSS (29) was used to assess the frequency of situations such as feeling nervous and stressed, or a perception of having control over one’s life within the past month. The screening scale for chronic stress SSCS/TICS-12 (28) covers a larger time frame; it includes 12 items that assess how often situations of worry, overload, and lack of social recognition have occurred within the last three months. Furthermore, the 10-item stress module of the German version of the Prime MD Patient Health Questionnaire (PHQ) (30) was used. The extent of impairment due to problems in the areas of personal health, social as well as working life, financial status, and past burdensome experiences within the last four weeks was assessed. This stress module has proven to be sensitive to change in patients with diabetes (26).
In addition, the Questionnaire on Stress in Patients with Diabetes—Revised QSD-R (31) was sent to patients with diabetes mailed at least one week before the examination, completed at home. The daily burden of diabetes disease and therapy was assessed by 45 items constituting eight scales: leisure time, work, partner, treatment regimen, hypoglycemia, physical complaints, doctor-patient relationship, and depression/fear of the future. This questionnaire was applied to evaluate the differences between diabetes patients with and without complications in their self-perceived illness related stress.
2.7 Statistical analysis
Metabolic parameters as well as hair cortisol were positively skewed and therefore log transformed for group comparisons. Groups were compared using analysis of (co-)variance (AN(C)OVA) in two sets of analyses: First, patients with diabetes type 2 were compared to control participants. Second, within the patient group, those with microvascular complications were compared to those without such complications. To compare type 2 diabetes patients and control participants, gender was included as a second factor to investigate potential moderating effects. Potential covariates were tested first and included only in further analyses in the event that a significant effect was apparent. In regard to stress questionnaires and HCC, age was tested as covariate. A significant association was obtained only for the SSCS score. Regarding HCC, hair washing frequency and hair treatment were additionally considered as potential covariates, but yielded no significant influences. In addition, QSD-R score and subscales were investigated using non-parametric tests (Mann–Whitney-U) to account for deviations from normality. Further, associations between stress questionnaires, HCC, and metabolic parameters were tested by Spearman’s Rho. Due to sporadic missing data, sample size for analyses ranged between 115 and 121 for the entire sample, and between 66 and 73 for the patient sample; serum cortisol data were available for 112 participants. All analyses were carried out using IBM SPSS Statistics 26.
3 Results
3.1 Hair cortisol
HCC was significantly higher among patients with type 2 diabetes compared to control participants (F(1,112) = 5.3; p = 0.023; Figure 1). Within the patient group, the difference between those with complications compared to those without complications did not, however, reach statistical significance (F(1,68) = 3.3, p = 0.075; Figure 1).
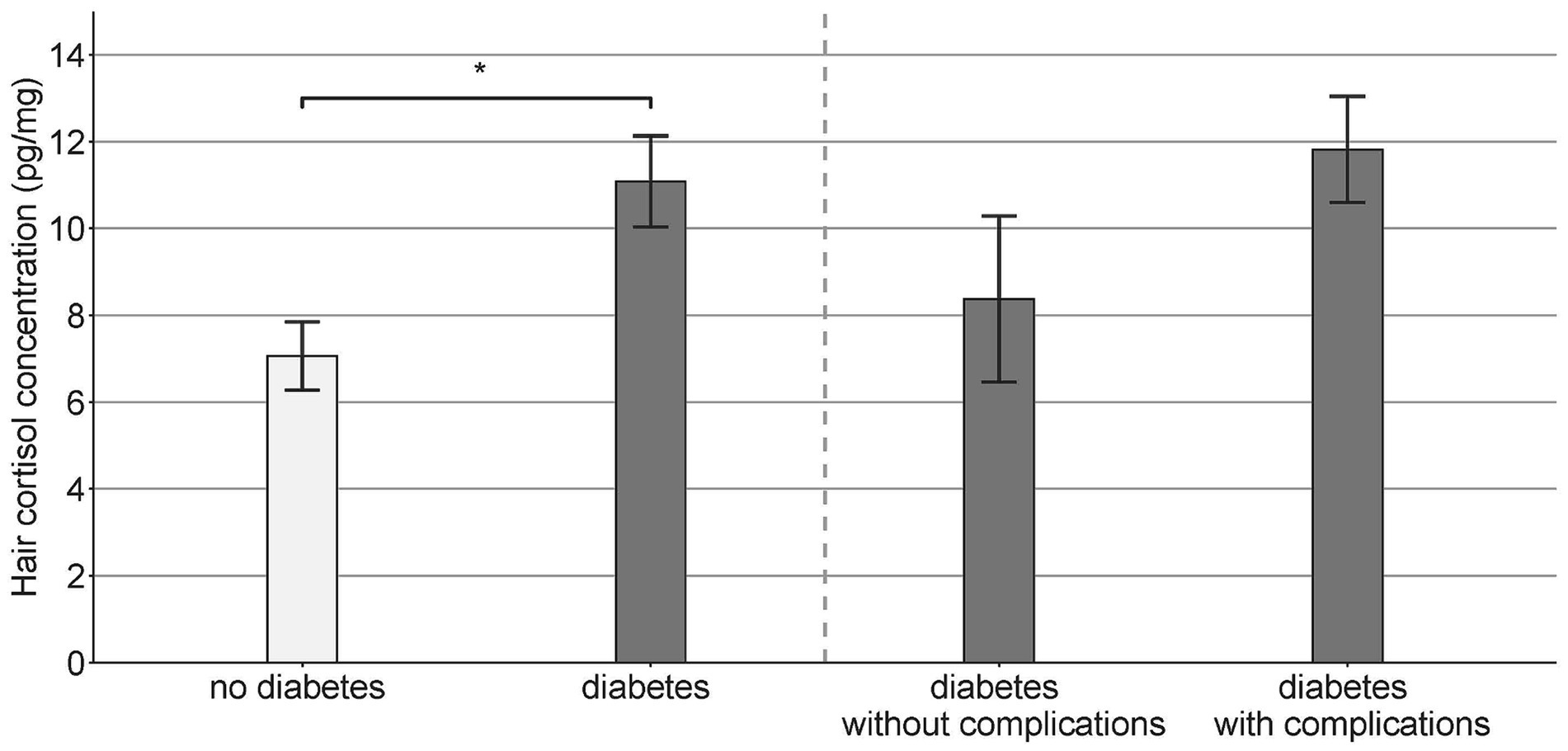
Figure 1. Hair cortisol concentration (mean ± SEM) in patients with type 2 diabetes with and without complications and in the non-diabetic control group (* p < 0.05).
3.2 Stress questionnaires
A significant interaction effect of group and gender emerged for the SSCS (F(1,115) = 9.7; p = 0.002). Women with diabetes had higher SSCS values compared to female control participants (F(1,43) = 3.9; p = 0.056), while in men the opposite pattern was observed (F(1,71) = 4.5; p = 0.037). For the PSS scores the interaction term of group and gender did not reach significance (F(1,113) = 2.9; p = 0.093).
Regarding PHQ stress scores, patients with type 2 diabetes had slightly (but not significantly) higher values than control participants, independent of gender (F(1,116) = 3.3; p = 0.071). Regarding PSS, SSCS, PHQ, or QSD-R values within the type 2 diabetes patient group, there were no differences between patients with complications and those without complications. However, regarding work (p = 0.047), and physical complaints (p = 0.029), an exploratory analysis for each of the QSD-R subscales revealed that type 2 diabetes patients with complications had significantly higher scores than those without.
3.3 Correlations
In the entire study sample HCC was not significantly related to baseline cortisol. Furthermore, HCC was not significantly associated with any of the subjective measures of chronic stress, neither in type 2 diabetes patients nor in the control group. Within type 2 diabetes patients, higher HCC was associated with longer illness duration (r = 0.25, p = 0.04) while associations with metabolic outcomes were weak (Table 2).
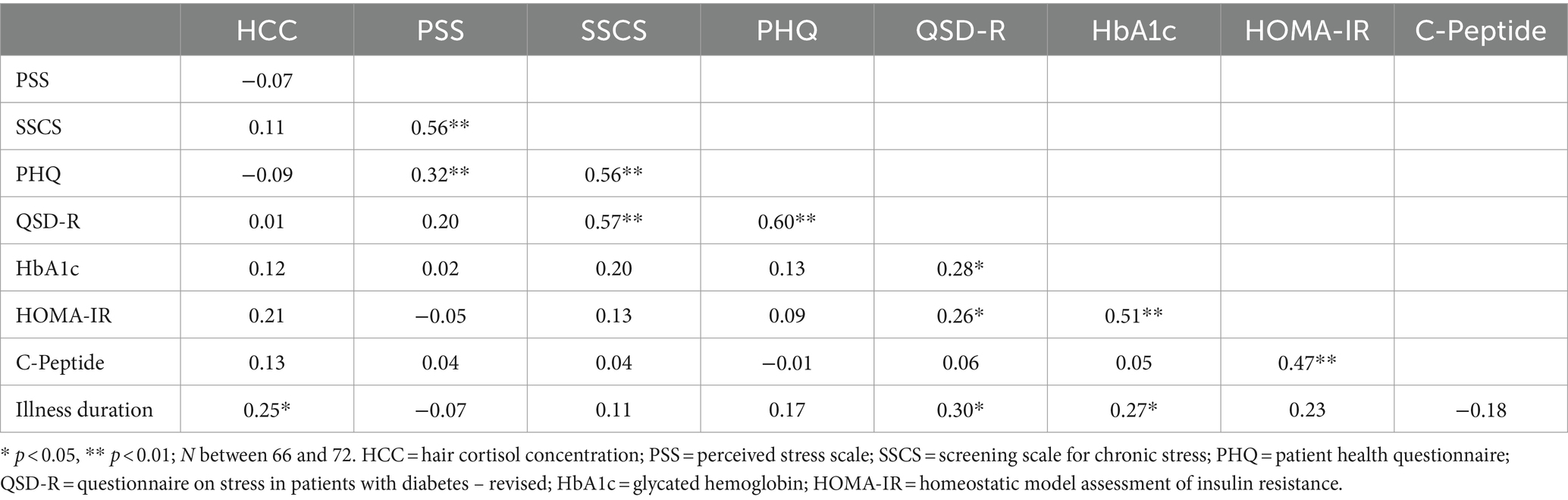
Table 2. Correlations between indicators of chronic stress and metabolic outcomes in patients with type 2 diabetes.
Additionally, QSD-R scores were positively associated with the HbA1c (r = 0.28, p = 0.02) and the HOMA index (r = 0.26, p = 0.03) as well as illness duration (r = 0.30, p = 0.01). No other significant correlations were seen in type 2 diabetes patients between subjective diabetes-unspecific stress scales and metabolic outcomes, including in illness duration (Table 2).
4 Discussion
Hair cortisol levels in patients with type 2 diabetes were significantly higher compared to control participants and positively associated with illness duration. Regarding questionnaire data, only diabetes distress was associated with markers of illness severity. Thus, the link between chronic stress and the course of diabetes appears to be complex, depending on diabetes outcome and the specific stress measure.
Cortisol concentrations in hair followed the expected pattern, i.e., they were highest in type 2 diabetes patients with complications, followed by type 2 diabetes patients without complications, and lowest among control participants. Higher hair cortisol concentrations in patients with type 2 diabetes compared to controls have been reported previously (12). However, previous studies have rarely used hair cortisol to investigate the relationship with markers of illness severity. Lehrer et al. (32) report a positive association of hair cortisol and HbA1c among African-American type 2 diabetes patients. Similar results were obtained by Stalder et al. (33) in a sample of Caucasian participants. However, the latter study did not focus specifically on patients with diabetes. While we did not obtain a significant association between HCC and HbA1c, HCC was related to illness duration.
To date, hair cortisol levels have not yet been investigated in relation to the presence of diabetic microvascular complications. Zhang et al. (34) found higher serum cortisol levels in T2D patients with microalbuminuria; higher serum and urinary free cortisol levels were also reported by Chiodini et al. (35) for T2D patients with chronic diabetic complications including nephropathy, neuropathy, retinopathy as well as silent macroangiopathy. In summary, we could speculate that cortisol might be causally involved in the progress of the illness including the development of diabetic complications. However, due to the correlational nature of our study, influences of other factors on hair cortisol levels cannot be excluded [cf. (36), for a meta-analysis of potential factors]. For example, the immune system and the HPA axis are strongly connected; a large study has recently shown that hair cortisol concentration was associated with markers of obesity as well as indicators of low-grade inflammation (37). Besides measurement issues associated with subjective statements such as low sensitivity, such influences might also contribute to the well-known lack of correlation between self-perceived stress and hair cortisol levels (36); this was also observed here.
In addition, it should be noted that cortisol—despite undoubtedly being an important factor— is not the sole mediator of the biological stress response in the context of diabetes (11, 21), and hair cortisol is only one indicator of HPA axis activity (38), specifically reflecting cortisol output over a longer period of time (24). Furthermore, cortisol action in the periphery is locally modulated by enzymes in the target tissue. For example, 11β-hydroxysteroid-dehydrogenase 1, which converts inactive cortisone into active cortisol, is increased in the adipose tissue of obese humans (38). Thus, the relationship between stress and diabetes is multifaceted, and each study can only investigate pieces of the complex interplay. For instance, in addition to hormonal assessments, it might be interesting in further studies to also use multimodal sensing and its integration via the Internet of Things and machine learning to continuously monitor stress in real-time (39, 40), possibly along with metabolic parameters (41).
Higher levels of subjective stress were reported by patients with type 2 diabetes compared to control participants depending on gender. This is in line with previous cohort studies which also, quite frequently, found moderating effects of gender on the association of subjective stress and diabetes incidence. Surprisingly, we found no significant differences between diabetes type 2 patients—those with and those without microvascular complications—with respect to questionnaires assessing general (i.e., diabetes-unspecific) perceived stress. In addition, diabetes-unspecific subjective stress was not related to diabetes-associated metabolic outcomes in the context of the patient sample. In contrast, diabetes-specific distress was associated with glycemic control and illness duration.
The lack of association between general perceived stress and metabolic outcomes is in line with a previous study reporting that only diabetes distress, but not the PHQ or serious psychological distress was related to the HbA1c in a sample of patients with type 2 diabetes (42). We can therefore infer that in patients with type 2 diabetes, glycemic control is not associated with the self-assessment of everyday life stress. One possible explanation is that patients with this condition may be biased in their perception of stress, making them more sensitive to disease-specific stressors. Another inference is that once diabetes has developed, general psychological stress takes a back seat whereas diabetes-specific aspects come to the fore. It should be noted, however, that longitudinal studies will be needed to test this hypothesis. In addition, causality cannot be inferred from the current results. It is conceivable that diabetes and its associated complications result in diabetes distress; on the other hand the effectiveness of psychological interventions indicates the opposite. Thus, the link between diabetes distress and diabetes (complications) is, most likely, bi-directional.
The major strength of the current study is that stress was assessed comprehensively, using various questionnaires as well as hair cortisol. In addition, type 2 diabetes patients differed with respect to diabetes duration as well as the presence of microvascular diabetic complications. This allowed us to investigate associations of stress with illness severity as reflected by several diabetes-associated metabolic outcomes. However, some limitations should be noted. First, there were only a few participants without microvascular complications, thus limiting the power of the comparison tests and analyses of potentially moderating factors (43). It could be due to the insufficient power that the difference in hair cortisol between patients with and without complications narrowly failed to reach significance. However, it was particularly difficult to find diabetes patients without complications; consequently, future studies may be enhanced by allocating additional resources to the recruitment of this specific subgroup. Second, because a different measurement method was used we could not categorize individuals in groups with either high or low stress levels according to given cut-off values (44). Taking into account that associations between self-perceived stress and HCC seem to be stronger within highly stressed persons (45), it could be interesting to include a specifically selected, high-stress subsample in future studies. Third, our study may have been subject to various biases. A selection bias may have been occurred due to the recruitment of diabetes patients in a University Hospital setting. Also, the participants’ self-assessment of stress could be subject to a memory bias. However, we would rule out the reverse causality bias because all our inferences refer to possible associations and not to causal pathways.
In conclusion, our results support the importance of psychological stress in type 2 diabetes. However, diabetes-unspecific subjective stress appears not to play a major role in relation to the severity of the illness as reflected by glycemic control, insulin resistance, β-cell function, and the presence of microvascular complications. Nevertheless, on a biological level, cortisol production could be linked with diabetes outcomes. Reducing cortisol levels might therefore be important also after the diagnosis of diabetes has been received. In addition, psychological interventions could benefit from explicitly addressing diabetes-specific topics. To establish the chronological order of these associations, longitudinal studies are warranted.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statement
The studies involving humans were approved by the ethics committee of the University of Heidelberg [S-019(2017)]. The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
Author contributions
MB: Conceptualization, Formal analysis, Funding acquisition, Project administration, Writing – original draft, Writing – review & editing. CS: Formal analysis, Investigation, Visualization, Writing – review & editing. MH: Conceptualization, Funding acquisition, Supervision, Writing – review & editing, Project administration. NM: Investigation, Writing – review & editing. SK: Methodology, Resources, Writing – review & editing. JS: Resources, Writing – review & editing. BW: Conceptualization, Funding acquisition, Project administration, Supervision, Writing – review & editing.
Funding
The author(s) declare financial support was received for the research, authorship, and/or publication of this article. The study was funded by the Deutsche Forschungsgemeinschaft (DFG, German Research Foundation)–project numbers WI 4115/5-1 and 236360313 (SFB 1118). The funding sources had no role in the design of the study; the collection, analysis, and interpretation of data; writing the report; or the decision to submit the report for publication.
Acknowledgments
We would like to thank all the participants for their participation in the study, as well as Peter Nawroth, Thomas Flemming, Nikola Henningsen, and Kira Wolff for their contribution to the study.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The author(s) declared that they were an editorial board member of Frontiers, at the time of submission. This had no impact on the peer review process and the final decision.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Dennick, K, Sturt, J, and Speight, J. What is diabetes distress and how can we measure it? A narrative review and conceptual model. J Diabetes Complicat. (2017) 31:898–911. doi: 10.1016/j.jdiacomp.2016.12.018
2. Asuzu, CC, Walker, RJ, Williams, JS, and Egede, LE. Pathways for the relationship between diabetes distress, depression, fatalism and glycemic control in adults with type 2 diabetes. J Diabetes Complicat. (2017) 31:169–74. doi: 10.1016/j.jdiacomp.2016.09.013
3. Braizat, O, Feinn, R, Abbott, G, and Wagner, J. Relationship style and glycaemic control in women with type 2 diabetes: the mediating role of psychological distress. Stress Health. (2018) 34:462–7. doi: 10.1002/smi.2795
4. Fisher, L, Mullan, JT, Arean, P, Glasgow, RE, Hessler, D, and Masharani, U. Diabetes distress but not clinical depression or depressive symptoms is associated with glycemic control in both cross-sectional and longitudinal analyses. Diabetes Care. (2010) 33:23–8. doi: 10.2337/dc09-1238
5. Ismail, K, Moulton, CD, Winkley, K, Pickup, JC, Thomas, SM, Sherwood, RA, et al. The association of depressive symptoms and diabetes distress with glycaemic control and diabetes complications over 2 years in newly diagnosed type 2 diabetes: a prospective cohort study. Diabetologia. (2017) 60:2092–102. doi: 10.1007/s00125-017-4367-3
6. Schmidt, C, van Loon, BP, Vergouwen, A, Snoek, F, and Honig, A. Systematic review and meta-analysis of psychological interventions in people with diabetes and elevated diabetes-distress. Diabetic Med. (2018) 35:1157–72. doi: 10.1111/dme.13709
7. Zagarins, SE, Allen, NA, Garb, JL, and Welch, G. Improvement in glycemic control following a diabetes education intervention is associated with change in diabetes distress but not change in depressive symptoms. J Behav Med. (2012) 35:299–304. doi: 10.1007/s10865-011-9359-z
8. Fisher, L, Mullan, JT, Skaff, MM, Glasgow, RE, Arean, P, and Hessler, D. Predicting diabetes distress in patients with type 2 diabetes: a longitudinal study. Diab Med. (2009) 26:622–7. doi: 10.1111/j.1464-5491.2009.02730.x
9. Kasteleyn, M, de Vries, L, Van Puffelen, A, Schellevis, F, Rijken, M, Vos, R, et al. Diabetes-related distress over the course of illness: results from the diacourse study. Diab Med. (2015) 32:1617–24. doi: 10.1111/dme.12743
10. Baek, RN, Tanenbaum, ML, and Gonzalez, JS. Diabetes burden and diabetes distress: the buffering effect of social support. Ann Behav Med. (2014) 48:145–55. doi: 10.1007/s12160-013-9585-4
11. Joseph, JJ, and Golden, SH. Cortisol dysregulation: the bidirectional link between stress, depression, and type 2 diabetes mellitus. Ann N Y Acad Sci. (2017) 1391:20–34. doi: 10.1111/nyas.13217
12. Abell, JG, Stalder, T, Ferrie, JE, Shipley, MJ, Kirschbaum, C, Kivimäki, M, et al. Assessing cortisol from hair samples in a large observational cohort: the Whitehall ii study. Psychoneuroendocrinology. (2016) 73:148–56. doi: 10.1016/j.psyneuen.2016.07.214
13. Jackson, SE, Kirschbaum, C, and Steptoe, A. Hair cortisol and adiposity in a population-based sample of 2,527 men and women aged 54 to 87 years. Obesity. (2017) 25:539–44. doi: 10.1002/oby.21733
14. Cusick, M, Meleth, AD, Agrón, E, Fisher, MR, Reed, GF, Knatterud, GL, et al. Associations of mortality and diabetes complications in patients with type 1 and type 2 diabetes: early treatment diabetic retinopathy study report no. 27. Diabetes Care. (2005) 28:617–25. doi: 10.2337/diacare.28.3.617
15. Rodríguez-Gutiérrez, R, and Montori, VM. Glycemic control for patients with type 2 diabetes mellitus: our evolving faith in the face of evidence. Circ Cardiovasc Qual Outcomes. (2016) 9:504–12. doi: 10.1161/CIRCOUTCOMES.116.002901
16. Fowler, MJ. Microvascular and macrovascular complications of diabetes. Clin Diabetes. (2008) 26:77–82. doi: 10.2337/diaclin.26.2.77
17. Carrizzo, A, Izzo, C, Oliveti, M, Alfano, A, Virtuoso, N, Capunzo, M, et al. The main determinants of diabetes mellitus vascular complications: endothelial dysfunction and platelet hyperaggregation. Int J Mol Sci. (2018) 19:2968. doi: 10.3390/ijms19102968
18. Sardu, C, Paolisso, P, Sacra, C, Mauro, C, Minicucci, F, Portoghese, M, et al. Effects of metformin therapy on coronary endothelial dysfunction in patients with prediabetes with stable angina and nonobstructive coronary artery stenosis: the codyce multicenter prospective study. Diabetes Care. (2019) 42:1946–55. doi: 10.2337/dc18-2356
19. Sher, LD, Geddie, H, Olivier, L, Cairns, M, Truter, N, Beselaar, L, et al. Chronic stress and endothelial dysfunction: mechanisms, experimental challenges, and the way ahead. Am J Phys Heart Circ Phys. (2020) 319:H488–506. doi: 10.1152/ajpheart.00244.2020
20. Sasso, FC, Pafundi, PC, Marfella, R, Calabrò, P, Piscione, F, Furbatto, F, et al. Adiponectin and insulin resistance are related to restenosis and overall new PCI in subjects with normal glucose tolerance: the prospective AIRE study. Cardiovasc Diabetol. (2019) 18:1–13. doi: 10.1186/s12933-019-0826-0
21. Yaribeygi, H, Maleki, M, Butler, AE, Jamialahmadi, T, and Sahebkar, A. Molecular mechanisms linking stress and insulin resistance. EXCLI J. (2022) 21:317–34. doi: 10.17179/excli2021-4382
22. Buckert, M, Hartmann, M, Monzer, N, Wolff, K, Nawroth, P, Fleming, T, et al. Pronounced cortisol response to acute psychosocial stress in type 2 diabetes patients with and without complications. Horm Behav. (2022) 141:105120. doi: 10.1016/j.yhbeh.2022.105120
23. Monzer, N, Hartmann, M, Buckert, M, Wolff, K, Nawroth, P, Kopf, S, et al. Associations of childhood neglect with the acth and plasma cortisol stress response in patients with type 2 diabetes. Front Psych. (2021) 12:986. doi: 10.3389/fpsyt.2021.679693
24. Stalder, T, and Kirschbaum, C. Analysis of cortisol in hair – state of the art and future directions. Brain Behav Immun. (2012) 26:1019–29. doi: 10.1016/j.bbi.2012.02.002
25. Davenport, MD, Tiefenbacher, S, Lutz, CK, Novak, MA, and Meyer, JS. Analysis of endogenous cortisol concentrations in the hair of rhesus macaques. Gen Comp Endocrinol. (2006) 147:255–61. doi: 10.1016/j.ygcen.2006.01.005
26. Hartmann, M, Kopf, S, Kircher, C, Faude-Lang, V, Djuric, Z, Augstein, F, et al. Sustained effects of a mindfulness-based stress-reduction intervention in type 2 diabetic patients: design and first results of a randomized controlled trial (Heidelberger Diabetes and Stress Study). Diabetes Care. (2012) 35:945–7. doi: 10.2337/dc11-1343
27. Klein, EM, Brähler, E, Dreier, M, Reinecke, L, Müller, KW, Schmutzer, G, et al. The german version of the perceived stress scale–psychometric characteristics in a representative german community sample. BMC Psychiatry. (2016) 16:1–10. doi: 10.1186/s12888-016-0875-9
28. Schulz, P, Schlotz, W, and Becker, P. Trierer Inventar zum chronischen Stress. Göttingen: Hogrefe (2004).
29. Cohen, S, Kamarck, T, and Mermelstein, R. A global measure of perceived stress. J Health Soc Behav. (1983) 24:385–96. doi: 10.2307/2136404
30. Löwe, B, Spitzer, RL, Zipfel, S, and Herzog, W. Gesundheitsfragebogen für Patienten (PHQ-D). Manual und Testunterlagen. 2nd ed. Karlsruhe: Pfizer (2002).
31. Herschbach, P, Duran, G, Waadt, S, Zettler, A, Amm, C, Marten-Mittag, B, et al. Psychometric properties of the questionnaire on stress in patients with diabetes—revised (QSD-R). Health Psychol. (1997) 16:171–4. doi: 10.1037/0278-6133.16.2.171
32. Lehrer, HM, Dubois, SK, Maslowsky, J, Laudenslager, ML, and Steinhardt, MA. Hair cortisol concentration and glycated hemoglobin in african american adults. Psychoneuroendocrinology. (2016) 72:212–8. doi: 10.1016/j.psyneuen.2016.06.018
33. Stalder, T, Kirschbaum, C, Alexander, N, Bornstein, SR, Gao, W, Miller, R, et al. Cortisol in hair and the metabolic syndrome. J Clin Endoc Metabol. (2013) 98:2573–80. doi: 10.1210/jc.2013-1056
34. Zhang, X, Deng, X, Zhou, J, Qiu, K, Deng, M, Lin, Z, et al. The association of serum cortisol level with microalbuminuria in patients with type 2 diabetes and prediabetes. Int J Med Sci. (2020) 17:2998–3004. doi: 10.7150/ijms.48742
35. Chiodini, I, Adda, G, Scillitani, A, Coletti, F, Morelli, V, Di Lembo, S, et al. Cortisol secretion in patients with type 2 diabetes: relationship with chronic complications. Diabetes Care. (2007) 30:83–8. doi: 10.2337/dc06-1267
36. Stalder, T, Steudte-Schmiedgen, S, Alexander, N, Klucken, T, Vater, A, Wichmann, S, et al. Stress-related and basic determinants of hair cortisol in humans: a meta-analysis. Psychoneuroendocrinology. (2017) 77:261–74. doi: 10.1016/j.psyneuen.2016.12.017
37. van der Valk, ES, van der Voorn, B, Iyer, AM, Mohseni, M, Leenen, PJM, Dik, WA, et al. Hair cortisol, obesity and the immune system: results from a 3 year longitudinal study. Psychoneuroendocrinology. (2021) 134:105422. doi: 10.1016/j.psyneuen.2021.105422
38. Rodriguez, ACI, Epel, ES, White, ML, Standen, EC, Seckl, JR, and Tomiyama, AJ. Hypothalamic-pituitary-adrenal axis dysregulation and cortisol activity in obesity: a systematic review. Psychoneuroendocrinology. (2015) 62:301–18. doi: 10.1016/j.psyneuen.2015.08.014
39. Garcia-Ceja, E, Riegler, M, Nordgreen, T, Jakobsen, P, Oedegaard, KJ, and Tørresen, J. Mental health monitoring with multimodal sensing and machine learning: a survey. Perv Mobile Comput. (2018) 51:1–26. doi: 10.1016/j.pmcj.2018.09.003
40. Nath, RK, Thapliyal, H, Caban-Holt, A, and Mohanty, SP. Machine learning based solutions for real-time stress monitoring. IEEE Cons Electron Magaz. (2020) 9:34–41. doi: 10.1109/MCE.2020.2993427
41. Maqbool, S, Bajwa, IS, Maqbool, S, Ramzan, S, and Chishty, MJ. A smart sensing technologies-based intelligent healthcare system for diabetes patients. Sensors. (2023) 23:9558. doi: 10.3390/s23239558
42. Winchester, RJ, Williams, JS, Wolfman, TE, and Egede, LE. Depressive symptoms, serious psychological distress, diabetes distress and cardiovascular risk factor control in patients with type 2 diabetes. J Diabetes Complicat. (2016) 30:312–7. doi: 10.1016/j.jdiacomp.2015.11.010
43. Stoop, C, Nefs, G, Pop, V, Wijnands-van Gent, C, Tack, C, Geelhoed-Duijvestijn, P, et al. Diabetes-specific emotional distress in people with type 2 diabetes: a comparison between primary and secondary care. Diabetic Med. (2014) 31:1252–9. doi: 10.1111/dme.12472
44. Gonzalez, D, Jacobsen, D, Ibar, C, Pavan, C, Monti, J, Fernandez Machulsky, N, et al. Hair cortisol measurement by an automated method. Sci Rep. (2019) 9:8213. doi: 10.1038/s41598-019-44693-3
Keywords: psychological stress, hair cortisol, type 2 diabetes, microvascular complications, HbA1c
Citation: Buckert M, Streibel C, Hartmann M, Monzer N, Kopf S, Szendrödi J and Wild B (2024) Cross-sectional associations of self-perceived stress and hair cortisol with metabolic outcomes and microvascular complications in type 2 diabetes. Front. Public Health. 12:1289689. doi: 10.3389/fpubh.2024.1289689
Edited by:
Khalid Siddiqui, King Saud University, Saudi ArabiaReviewed by:
Sridhar R. Gumpeny, Endocrine and Diabetes Centre, IndiaYun Shen, Pennington Biomedical Research Center, United States
Copyright © 2024 Buckert, Streibel, Hartmann, Monzer, Kopf, Szendrödi and Wild. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Magdalena Buckert, magdalena.buckert@iu.org; Beate Wild, beate.wild@med.uni-heidelberg.de
†Present address: Magdalena Buckert, IU International University of Applied Sciences, Mannheim, Germany