 Richard Morsch
Richard Morsch Tim Böckenförde2,4
Tim Böckenförde2,4 Milan Wolf
Milan Wolf Daniel J. Strauss
Daniel J. Strauss- 1Systems Neuroscience & Neurotechnology Unit, Medical Faculty, Saarland University, Homburg, Germany
- 2Medical Faculty, Saarland University, Saarbrücken, Germany
- 3Center for Digital Neurotechnologies Saar, Homburg, Germany
- 4Clinics for Orthopedics and Orthopedic Surgery, Saarland University Medical Center, Homburg, Germany
Introduction: Neuromuscular recovery after total joint arthroplasty remains insufficiently understood, and current tools for assessing muscle function lack the resolution to monitor detailed recovery dynamics. High-Density surface Electromyography (HD-sEMG) enables spatiotemporal analysis of muscle activation and may support individualized rehabilitation. However, its clinical application in orthopedic settings remains limited.
Methods: This exploratory study presents a methodological framework for applying wearable 64-channel HD-sEMG system to monitor neuromuscular recovery in patients undergoing total knee or hip arthroplasty. HD-sEMG data were recorded during standardized mobilization exercises at multiple pre- and postoperative time points. A custom signal processing pipeline was developed, encompassing artifact suppression, dimensionality reduction, feature extraction, and the derivation of five functional indices summarizing key aspects of muscle performance.
Results: Initial clinical application demonstrated the feasibility of the approach. The functional indices revealed distinct recovery dynamics across patients and showed promising alignment with patient-reported outcome measures. Individual case analyses suggested the potential of HD-sEMG to differentiate between restitution and dysfunctional compensation patterns.
Discussion: This study provides a structured, exploratory foundation for longitudinal HD-sEMG research in orthopedic rehabilitation. While not yet suited for clinical decision-making, the proposed framework offers methodological tools for future investigations of neuromuscular recovery trajectories and may contribute to the development of personalized, data-driven rehabilitation strategies.
1 Introduction
1.1 Clinical background and motivation
Recovery after total joint arthroplasty (TJA) varies greatly between individuals, and the underlying factors influencing this variability remain insufficiently understood. General muscle weakness is associated with increased surgical risk and poor functional outcomes (1, 2). However, the specific mechanisms through which muscular condition impacts recovery trajectories have yet to be clarified (3).
There is evidence of postoperative neuromuscular alterations following total knee (TKA) and hip arthroplasty (THA), including reduced quadriceps activation, asymmetrical recruitment patterns, and persistent gluteal muscle dysfunction, implying deficits in neural drive and the need for targeted rehabilitation (3, 4). Suboptimal rehabilitation can further diminish treatment outcomes and patient satisfaction, despite technically successful surgery (5–8).
1.2 High-density surface electromyography (HD-sEMG), a promising tool for objective monitoring
In recent years, HD-sEMG has emerged as a powerful tool for analyzing spatial and temporal patterns of myoelectric activity. Its two-dimensional electrode-array arrangement allows for a detailed spatiotemporal analysis of muscle activation and motor unit behavior, offering advantages over conventional bipolar EMG and invasive intramuscular techniques (9–12). Furthermore, technical innovations have made HD-sEMG systems more accessible and easier to implement in clinical practice. Recent technological advances like wearable systems, improved electrode materials, and robust decomposition algorithms have increased its usability and accuracy in dynamic, real-world settings (13, 14).
1.3 Clinical relevance and limitations
HD-sEMG has been systematically applied across a range of neuromuscular disorders, demonstrating diagnostic value in conditions such as motor neuron diseases, neuropathies, myopathies, and muscle fatigue assessment (15). Its non-invasive nature makes it particularly suitable for populations where needle electromyography is impractical, such as pediatric or longitudinal applications, while enabling detection of pathological motor unit changes (9). HD-sEMG also provides complementary biomarkers to conventional diagnostics, enhancing clinical evaluation of neuromuscular function (16). Despite its diagnostic potential and remarkable advances, HD-sEMG still faces several challenges for broader clinical adoption, including variability in electrode placement, standardization of signal processing pipelines, and the need for normative reference data across populations (17).
1.4 State of the art: a research gap in total joint arthroplasty
Despite the widespread use of surface EMG in TJA research (3, 18, 19) to name a few, HD-sEMG remains underrepresented in this context. No published longitudinal HD-sEMG studies exist for TKA or THA patients to date. Existing research primarily consists of single-time-point or methodological studies, often in healthy cohorts (20, 21). This highlights the need for longitudinal, clinically embedded HD-sEMG investigations.
1.5 Study aim
This study bridges modern neurotechnology and orthopedic rehabilitation to enhance the objectivity, treatment individualization, and efficiency of recovery. It presents a methodological framework for applying wearable HD-sEMG to monitor neuromuscular recovery after TKA and THA. A wearable 64-channel HD-sEMG system was employed to capture myoelectric activity in patients undergoing the TJA under real-world conditions. Studies of both TKA and THA demonstrate significant intraoperative and perioperative practice variability among high-volume surgeons, including differences in surgical approach, implant type, use of tourniquet, patellar resurfacing, closure technique, and perioperative medications (22, 23). However, TJA procedures at the study's clinical site are performed according to a highly standardized protocol, ensuring comparability across patients. Measurements were conducted at multiple time points pre- and post-surgery, while patients performed a standardized set of mobilization exercises supervised by a physiotherapist. This paper proposes a signal processing pipeline in order to extract key spatial, spectral, and temporal features relevant to clinical recovery monitoring. It outlines the feasibility, challenges, and diagnostic potential of HD-sEMG-based rehabilitation monitoring in a real-world clinical setting.
2 Method
Figure 1 provides a schematic overview of the measurement design and the subsequent analysis workflow.
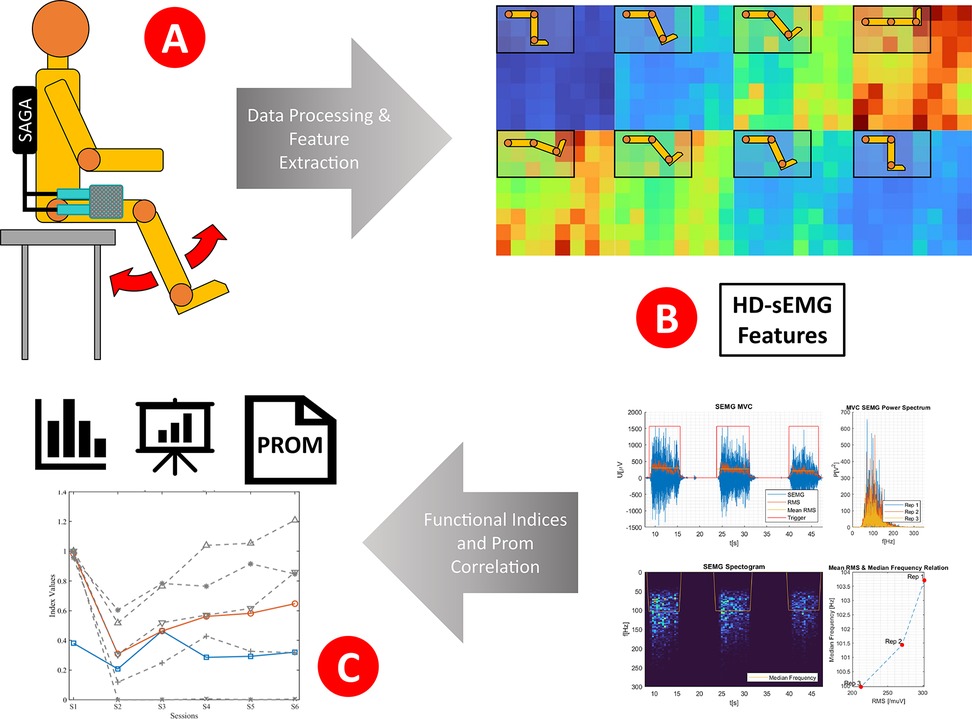
Figure 1. Conceptual overview of the HD-sEMG assessment and analysis workflow. HD-sEMG signals were recorded during functional leg movements using a wearable textile grid and the TMSi SAGA system (A). The EMG signals were processed to extract spatial, temporal, and spectral features and combined into five functional indices. Simultaneously, PROMs were collected across multiple postoperative sessions (B). Indices and PROM scores were then analyzed and compared to assess neuromuscular recovery and functional progression over time (C).
2.1 Study design and setting
This prospective observational study was designed to identify muscle-level factors, potentially predictive, influencing postoperative outcomes and patient satisfaction following TKA or THA. Measurements were conducted at Clinics for Orthopedics and Orthopedic Surgery, Saarland University Medical Center, Homburg (Saar), Germany. The study was approved by the Ethics Committee of the Medical Association of Saarland (approval number: HA273/20).
2.2 Study population
A total of 63 patients (34 M, 29 W; mean age ∼64 ± 10 years; 33 TKA and 30 THA) participated in the study. In all cases, the diagnosis was knee or hip osteoarthrosis. For this report, three exemplary patients were selected from the study population to illustrate initial trends and highlight the interpretive potential of the proposed methods. The selected cases include patient 016 (65 years, male; diagnosis: gonarthrosis; surgery: medial parapatellar approach; implant system: Persona®, Zimmer Biomet), 018 (75 years male; diagnosis: gonarthrosis; surgery: medial approach; implant system: Persona®, Zimmer Biomet) and 031 (68 years, male; diagnosis: coxarthrosis; surgery: lateral approach; implant system: AESCULAP® CoreHip®, B. Braun SE).
Patients were recruited at the day of preoperative assessment. After receiving detailed study information and providing written consent, they were enrolled in the study. Patients undergoing primary total knee or hip arthroplasty were included without restrictions on BMI or age. Eligibility required the ability to independently perform the measurement exercises and complete questionnaires, allowing for both pre- and postoperative HD-sEMG and PROMs data collection. Exclusion criteria included lack of informed consent, minor status, neurological or metabolic muscle disorders potentially affecting muscle activity, and incomplete datasets or missing follow-up assessments.
2.3 Measurement setup
2.3.1 Measurement workflow
PROMs were acquired at the beginning of each measurement session. Under supervision, the patients then performed the mobilization exercises while HD-sEMG was recorded. If feasible for the patient, both the operated and contralateral sides were assessed.
Measurements were conducted ∼5 days pre-surgery and up to five times post-surgery (∼2 days, 4–5 days, 6 weeks, 3 months, and 6 months).
2.3.2 Materials
HD-sEMG was recorded using the TMSi SAGA system (High Density Amplifier and 64-channel Ag/AgCl HD-EMG Grids; Artinis Medical Systems, Netherlands). Patient-Reported Outcome Measures (PROMs), either knee injury and osteoarthritis outcome score (KOOS) or hip disability and osteoarthritis outcome score (HOOS) served as clinically accepted measures (24, 25).
2.3.3 Electrode placement
Electrodes were positioned at m. rectus femoris (TKA) and m. gluteus medius (THA). The electrode sites were prepared by cleaning the skin with disinfectant, applying a mild abrasive gel, and using conductive electrode gel to minimize contact impedance and ensure optimal signal quality. In order to ensure consistent electrode placement and to minimize crosstalk this was done according to the SENIAM guidelines (surface EMG for a non-invasive assessment of muscles) and anatomical landmarks proposed by Hermens et al. for standardized and reproducible sEMG recording (26).
2.3.4 Exercise protocol
Two different mobilization exercise routines were used for TKA and THA patients, respectively. These exercises are well-established components of the clinic's standard rehabilitation protocol. Patients were encouraged by the supervising therapist to perform ideally ten or more repetitions per exercise and side; however, depending on individual physical condition or subjective pain levels, this could not always be achieved. The routines consisted of eight different exercises divided into two parts: Part one was performed while lying or sitting on the examination table, and part two in a standing position with optional handrail support.
The exercises for TKA included: a) foot dorsiflexion and plantarflexion in a lying position, b) knee flexion and extension with the foot sliding on the examination table, c) maximal isometric knee extension by pressing the straight leg into the examination table while lying down, d) knee flexion and extension with the foot elevated, e) knee flexion and extension while sitting upright on the examination table, f) rolling motion: upright standing in a narrow lunge position with the operated leg positioned slightly behind, performing a step-like rolling movement with the operated foot, g) loading: forward lunge with the operated leg in front, actively shifting bodyweight onto it, h) posterior stretching: backward lunge with the operated leg extended behind, shifting bodyweight onto the front leg to stretch the posterior chain.
The exercises for THA included. a) foot dorsiflexion and plantarflexion in a lying position, b) hip flexion and extension with the foot sliding on the examination table, c) hip flexion and extension with the foot elevated, d) hip abduction in a lying position, e) maximal isometric hip extension by pressing the straight leg into the examination table while lying down, f) hip flexion while standing upright by lifting the bent leg, g) hip abduction with the extended leg while standing upright, h) hip extension while standing upright by moving the straight leg posteriorly.
2.4 Signal processing
2.4.1 Data acquisition and initial inspection
HD-sEMG was recorded at a sampling rate of 1,000 Hz using the TMSi SAGA system. A manual trigger signal was acquired synchronously to the EMG data via the same system to indicate the currently performed exercise and its respective repetition (i.e., motion onset and peak). Following data acquisition, an initial manual inspection of the raw data was conducted to assess signal quality. Here, manual correction of trigger events enabled precise identification of EMG onset and offset down to the millisecond, which was crucial in this exploratory setting given the variability in patient performance during the exercises. In cases where electrode disconnection or severe motion artifacts were identified during a repetition, the affected trial was marked to be excluded from further analysis. All subsequent processing was performed using a custom MATLAB-based routine.
2.4.2 Data conditioning
2.4.2.1 Pre-processing
The raw EMG signals were bandpass-filtered within a physiological range of 20–450 Hz using sixth-order Butterworth filters. To reduce low-frequency noise such as motion artifacts and DC drift, a high-pass filter at 20 Hz was applied, while high-frequency noise was attenuated by a low-pass filter at 450 Hz (27). Additionally, a second-order IIR notch filter at 50 Hz with a quality factor of 50 was used to suppress power line interference originating from ground loops and electromagnetic noise (28).
2.4.2.2 Channel quality assessment
Channel quality was evaluated based on several criteria: a) Channel disconnects, defined as channels showing no data. b) Insufficient electrode adhesion, indicated by abnormally low signal amplitude. c) Signal-to-noise ratio, estimated as the ratio between power within the physiological frequency band (20–450 Hz) and the signal's total spectral power (27, 29).
Channels meeting one or more of these criteria were flagged as poor quality. If the number of bad channels exceeded two, they were excluded from further processing. Otherwise, affected channels were reconstructed using two-dimensional bilinear interpolation based on neighboring electrodes within the grid.
2.4.2.3 Segmenting
The recorded EMG data were segmented into individual repetitions based on manually validated trigger indices. Each trigger marked the onset of a specific exercise repetition, and segments were extracted from the onset of one repetition to the onset of the subsequent one. This approach ensured that each segment captured a full contraction cycle, independent of temporal variation across repetitions or participants. As movement speed may vary between repetitions, the resulting window lengths were inherently variable and adapted to the actual shape of the recorded activation pattern.
3.4.2.4 Signal quality enhancement
To further improve signal quality and suppress potential residual artifacts (e.g., crosstalk), blind source separation was performed via independent component analysis (ICA), using the MATLAB FastICA algorithm on each segmented repetition (10, 30–32).
Each component was evaluated based on multiple physiologically motivated criteria: spatial focus was assessed by the variance of the associated mixing vector, spectral plausibility required at least 90% of power within the 20–450 Hz band, temporal shape fidelity was evaluated by correlating rectified and smoothed (500 ms windows) components with the repetition-averaged activation profile, while also components with exceptionally low zero crossing rate, low Hoyer's sparseness in either in the component or its mixing vector, or elevated kurtosis were also considered non-physiological (31–34).
Rejected components were excluded from the inverse projection step, resulting in a denoised reconstruction of the EMG signal. The rejection logic could be flexibly adjusted to suit analysis needs—for instance, by excluding all components failing a critical criterion, or by applying thresholds requiring multiple failed metrics. This approach enabled effective noise suppression while maintaining physiologically relevant information.
2.4.3 Feature extraction
A set of temporal, spectral and spatial features was extracted for each segmented repetition in order to characterize the neuromuscular activation pattern from multiple perspectives.
Time-domain features included the integrated EMG (iEMG), root mean square (RMS), and the highest exercise-specific RMS-amplitude as maximum voluntary contraction (MVC) (35). In addition, the activation ratio (AR) was computed as the percentage of time the RMS exceeded defined thresholds (5%–30% MVC), indicating active contraction periods (36). Lastly, sample entropy for each channel was calculated (37).
Frequency-domain features comprised the median frequency (MF), zero crossing rate (ZCR), and band power (BP) distribution within 20–450 Hz, allowing assessment of spectral content, noise, and fatigue indicators (38–40).
Spatial activation was characterized using spatial RMS maps, from which Hoyer's sparseness, center of gravity (CoG), spatial dispersion (Spread), spatial entropy, and max-to-mean ratio (MMR) were derived (41–45).
2.4.4 Functional indices
To facilitate exploratory interpretation of multidimensional EMG features, five functional indices were defined to represent higher-level neuromuscular performance domains. All indices were calculated by combining physiologically related, normalized feature sets.
• Activation Intensity Index (AII): Captures the overall myoelectric activation level, based on iEMG, RMS, BP, and mean AR from 10% to 30%
• Efficiency and Focus Index (EFI): Quantifies spatial activation economy and localization, using, Hoyer's sparseness, MMR, spatial spread (inversely weighted), and spatial entropy.
• Fatigue and Performance Index (FPI): Reflects performance changes across repetitions by evaluating the trend (slope) of activation features (iEMG, RMS, MVC, BP, AR) and control-related features (MF, ZCR, Hoyer's sparseness).
• Coordination and Stability Index (CSI): Represents consistency of neuromuscular control, combining inter-repetition variance of RMS, MF, BP, and CoG.
• Spatial Correlation Index (SCI): Assesses similarity between spatial activation patterns (RMS, BP, MF two-dimensional maps) and a reference template (either mean preoperative or contralateral state), based on correlation across repetitions.
These indices were designed to summarize complex EMG activation behavior into interpretable domains and to support exploratory group comparisons, temporal progression analysis, and correlation with functional recovery markers. For all indices, higher values reflect “better” results compared to reference.
2.4.4.1 Signal variability compensation
To account for interindividual variability and diffuseness of muscle activation, all spatially aggregated features (e.g., iEMG, RMS, BP) were computed over a variable focus area, rather than using a fixed set of channels. Specifically, channels were included if they fell within one weighted standard deviation (i.e., spatial spread) around the CoG of the activation map. This adaptive method aimed for characterization of the most physiologically relevant activation zone, while compensating for inter-session variability in spatial spread or underlying activation patterns. To our knowledge, this aspect has not yet been standardized in current HD-sEMG literature.
2.4.4.2 Index normalization
Towards inter-session and inter-subject comparability, two reference-based versions were generated, for functional indices: one normalized to the preoperative state, and one to the contralateral (non-operated) side, enabling both longitudinal and lateral asymmetry assessment. To account for physiologically plausible positive or negative deviations from reference values and to reduce the impact of outliers, a Gaussian-based normalization approach, which to our knowledge is novel in the context of HD-sEMG analysis, was explored. For each feature of CSI, the deviation from the reference value (either preoperative or contralateral) was transformed using a Gaussian similarity function centered around the reference value. A heuristically defined tolerance zone of ±20% relative to the reference value was used to define the width (i.e., σ) of the Gaussian kernel, such that values within this range were considered functionally equivalent. For FPI though the reference value was set to zero, as this should be the ideal state (i.e., constant performance, no fatigue).
2.4.4.3 Global functional index
To obtain a compact summary measure of overall neuromuscular function, a Global Functional Index (GFI) was computed by combining the five functional indices (i.e., AII, EFI, FPI, CSI, SCI). For each session, individual indices were first calculated across all exercises, then z-score normalized within the session to ensure comparability across features and movement types. The GFI was then defined as the equally weighted mean of these normalized values, reflecting an exploratory composite measure of functional muscle quality across dimensions of intensity, spatial focus, fatigue resistance, motor consistency, and pattern similarity.
2.5 PROM alignment
To evaluate the clinical relevance and interpretability of the extracted EMG features and derived functional indices, the functional indices were compared with the respective sessions PROM-results. This step aimed to explore whether objective EMG-based metrics reflect patient-experienced function and recovery, thereby supporting the potential applicability of HD-sEMG analysis in personalized rehabilitation assessment.
3 Results
Figure 2 illustrates the development of functional EMG indices over six postoperative sessions for a representative TKA patient (016), normalized to either the preoperative status (left) or the contralateral side (right). Both the KOOS score and the GFI (red) declined after surgery (S2), followed by a gradual recovery across sessions (S3–S6). Dimension-specific indices (gray) showed varying dynamics: activation- and performance-related indices (AII, EFI, FPI) improved over time, whereas coordination and pattern-based indices (CSI, SCI) remained reduced. Normalization to the contralateral side allowed detection of potential overcompensation (EFI > 1), emphasizing the added value of dual-reference visualization for nuanced interpretation of neuromuscular recovery.
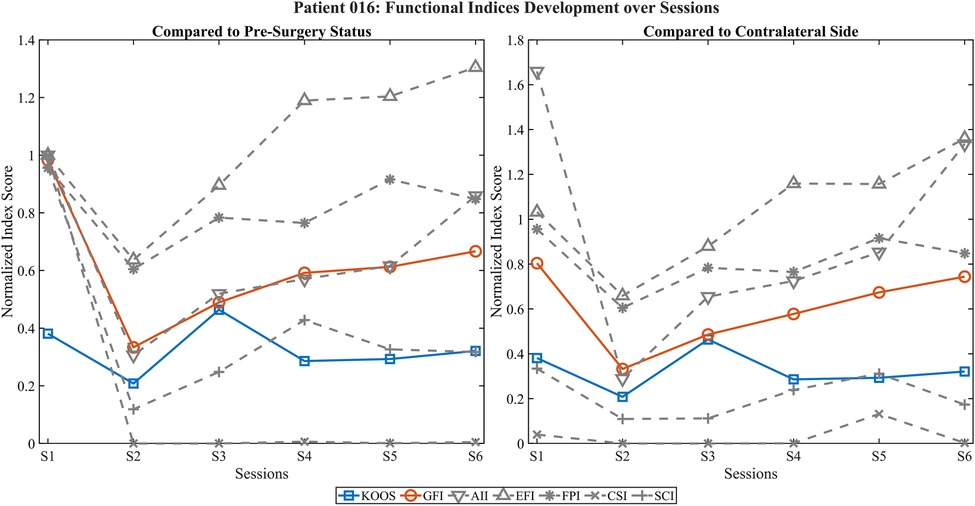
Figure 2. Development of functional EMG indices and KOOS score across postoperative sessions in patient 016. Left panel shows values normalized to the preoperative state; right panel shows normalization relative to the contralateral (non-operated) side. The GFI (red) and the KOOS score (blue) illustrate parallel recovery trends, with an initial decline after surgery (S2) followed by steady improvement across sessions. Gray lines represent individual component indices, including AII, EFI, FPI, CSI, SCI, revealing dimension-specific recovery profiles. Note that despite improving global activation and performance (AII, EFI, FPI), coordination-related indices (CSI, SCI) remain reduced, indicating potential deficits in neuromuscular control.
Figure 3 shows another TKA patient (018). While the KOOS score remained relatively stable at a low level, the GFI showed progressive improvement postoperatively. Activation indices increased strongly, particularly in comparison to the contralateral side, suggesting compensatory activation. However, low CSI and SCI values throughout all sessions indicated persistent deficits in motor coordination and spatial consistency. FPI, though offset, shows an almost similar shape as KOOS.
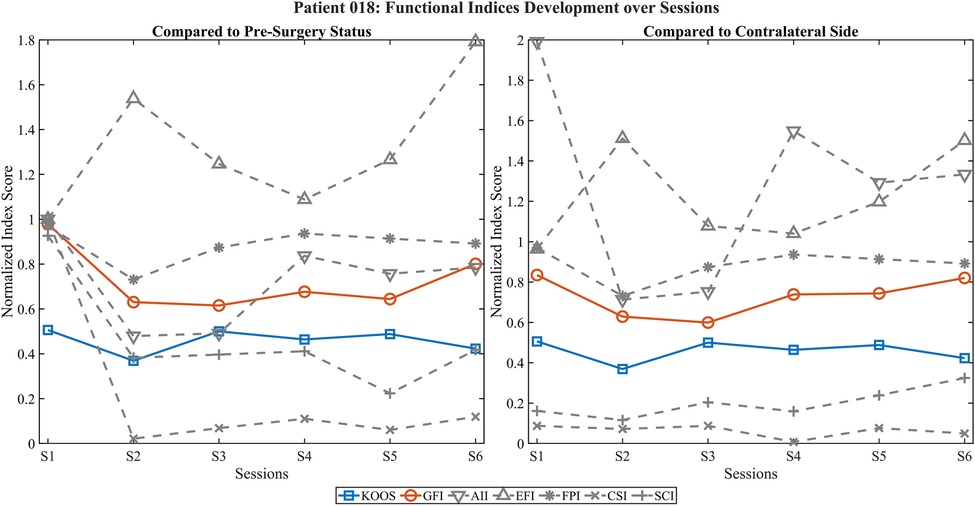
Figure 3. Development of functional EMG indices and KOOS score across postoperative sessions in patient 018. Left panel shows index values normalized to the preoperative state; right panel shows normalization relative to the contralateral side. The KOOS score (blue) remains relatively stable, while the GFI (red) shows a slight improvement across sessions. Activation-based indices (AII, EFI) increase notably, particularly when compared to the contralateral side, suggesting compensatory activation. In contrast, coordination and pattern-based indices (CSI, SCI) remain consistently low, indicating persistent deficits in neuromuscular control despite the observed increase in global activation levels. FPI behaves notably similar to KOOS.
Figure 4 depicts the results for 031, a hip arthroplasty patient. The GFI dropped sharply post-surgery and remained consistently low, whereas the HOOS score showed delayed but continuous improvement. Activation indices (AII, EFI) showed only mild recovery, while CSI and SCI remained minimal. FPI mildly increase until the last session (S6) where it drops below preoperative state. Normalization to the contralateral side revealed exaggerated index values in early sessions (e.g., AII > 30), likely due to low baseline activity on the healthy limb, underscoring the need for robust normalization methods.
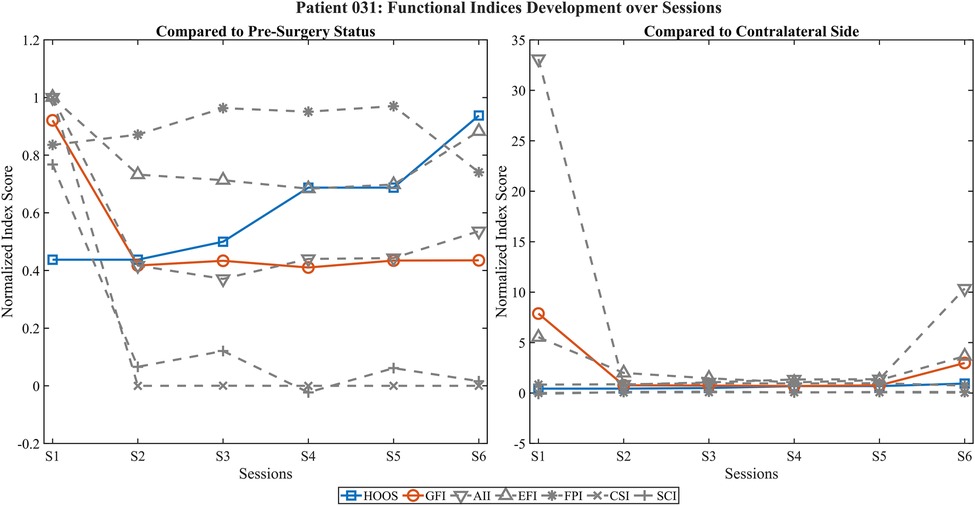
Figure 4. Development of functional EMG indices and HOOS score across postoperative sessions in patient 031. Left panel shows values normalized to the preoperative state; right panel displays normalization relative to the contralateral side. The HOOS score (blue) shows delayed but substantial improvement from session 4 onward, whereas the GFI (red) remains consistently low. Activation-related indices (AII, EFI) show minimal recovery or even exaggerated values due to low contralateral reference activity, while coordination (CSI) and pattern fidelity (SCI) indices stay markedly reduced across all sessions. Also, FPI mildly increases until the last session (S6) where it drops below preoperative state. These findings may reflect compensatory, yet inefficient, activation strategies.
4 Discussion
The visualization of functional EMG indices over multiple postoperative sessions demonstrated promising alignment with subjective functional recovery, as reflected by the PROMs. Notably, the GFI showed consistent improvements over time in several cases, suggesting that multidimensional EMG-derived metrics can capture relevant aspects of neuromuscular adaptation after joint replacement. The use of both preoperative and contralateral-side normalization enabled complementary perspectives, distinguishing between restitution of baseline function and compensatory activation strategies.
Individual case analyses highlighted the nuanced insights gained through multidimensional evaluation. In patient 016, improvements in activation-related indices (AII, EFI) contrasted with persistently low coordination and pattern-based measures (CSI, SCI), indicating incomplete motor recovery despite overall functional gains. Similarly, patient 018 demonstrated elevated activation levels but poor spatiotemporal control, emphasizing that compensatory activation alone does not equate to functional recovery. In patient 031, representing a hip arthroplasty case, PROM improvements were not mirrored by the GFI or coordination-based indices and extreme values in contralateral-side normalization suggested normalization artifacts due to very low reference activity. These findings underscore the value of integrating multiple feature domains into composite indices such as the GFI to differentiate between true recovery and dysfunctional compensation.
It has to be acknowledged that HD-sEMG decomposition and interpretation are subject to interindividual variability. Factors such as subcutaneous tissue thickness, muscle mass, training status, or patient motivation may influence signal quality and motor unit detectability (46).
Hence, certain limitations of the current index implementation became evident. Manual segmentation was adequate in this setting but remains a barrier to clinical scalability, underscoring the importance of automation in future studies. In some cases, disproportionately high activation values—particularly in AII—led to distorted GFI outcomes. This was evident especially when the contralateral reference values were low. To mitigate this, future index versions may incorporate saturation-like effects through logarithmic transformation or apply threshold-based weighting schemes to reduce outlier influence. These adaptations will require validation on a larger patient cohort before they can be meaningfully implemented.
While the study's longitudinal design included repeated measurements across up to six sessions per patient, these reflect dynamic recovery trajectories rather than stable baselines. Hence, only intra session-consistency-tests and no formal test-retest reliability analysis was conducted. Future studies should incorporate repeated baseline sessions in stable conditions to evaluate inter-session reliability of the proposed indices.
Moreover, some extreme index values (both high and low) suggest the need for further refinement of index construction. As additional datasets become available, statistical approaches such as multivariate regression, principal component analysis, or feature importance analysis (e.g., via random forest models) will be explored to optimize feature selection and weighting. This may allow for more robust, interpretable, and condition-specific indices. Adaptive weighting, outlier-resistant normalization, and clinically grounded interpretation thresholds are potential enhancements to improve sensitivity and generalizability.
4.1 Conclusion & future implications
This study demonstrated the feasibility of applying wearable HD-sEMG to assess neuromuscular recovery after total joint replacement in a clinical setting. Electrode array placement and data-acquisition could be performed reliably by a trained assistant physician after a short learning period, suggesting improved accessibility compared to earlier generations of technology. The GFI and its component metrics provided structured, interpretable insights into multidimensional aspects of recovery, capturing changes in activation, coordination, and signal quality. Preliminary trends indicated a potential alignment between EMG-based indices and PROM outcomes, though with subject-specific variability, highlighting the value of objective muscle monitoring alongside subjective measures.
With an aging population and rising rates of orthopedic surgeries, there is a growing need for precise, personalized, and data-driven rehabilitation strategies to improve patient outcomes and reduce long-term healthcare burdens (47–49). HD-sEMG offers a promising modality for non-invasive muscular assessment, and ongoing advances in electrode technology, signal processing, and real-time analytics are likely to further enhance its clinical applicability (17).
Despite promising capabilities, the broader clinical adoption of HD-sEMG is currently limited by several practical hurdles, including data processing complexity, lack of standardized interpretation frameworks, and integration with conventional instrumentation and existing rehabilitation protocols. However, the increasing availability of more accessible and more user-friendly hardware, clinician-oriented software tools (e.g., iSpin, MUedit), and open-source toolboxes (e.g., openhdemg) is expected to lower the entry threshold for clinical researchers and practitioners. Furthermore, as HD-sEMG captures activation patterns that are not accessible through conventional methods, it may contribute to more nuanced understanding of functional compensation, fatigue, or neural drive – especially in longitudinal, therapy-guided applications. Future studies should continue to evaluate the added value of HD-sEMG in complementing established clinical assessments and its potential role in personalized, data-driven rehabilitation strategies.
Current findings are exploratory and limited by sample size and variability in electrode placement. Due to the heterogeneous nature of the population and signal sources, no inferential group statistics were conducted yet. Rather, individual cases were used to illustrate the interpretive potential of the proposed framework. Future work will focus on validating the indices across broader cohorts, refining feature selection and weighting schemes using statistical methods such as multivariate regression and clustering, and exploring HD-sEMG's potential for pre-surgical outcome prediction. Additionally, novel methodological approaches like the Gaussian-based normalization with tolerance zones and the CoG-centered adaptive channel selection will be further investigated in future work to evaluate their robustness, optimize parameter settings and assess their impact on index stability and interpretability across broader datasets. Statistical group comparisons are also subject of future validation studies. Ultimately, this research may support individualized monitoring of recovery trajectories and enable adaptive rehabilitation strategies tailored to patient-specific neuromuscular profiles.
Data availability statement
The raw data supporting the conclusions of this article are available from the corresponding author upon reasonable request. Due to ethical and data protection regulations (GDPR), only pseudonymized data can be shared and within the limits approved by the local ethics committee.
Ethics statement
The studies involving humans were approved by Ethics Committee of the Medical Association of Saarland (approval number: HA273/20). The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
Author contributions
RM: Software, Visualization, Data curation, Formal analysis, Writing – review & editing, Methodology, Writing – original draft, Conceptualization. TB: Writing – review & editing, Methodology, Validation, Conceptualization, Data curation. MW: Conceptualization, Validation, Resources, Supervision, Writing – review & editing, Project administration. SL: Resources, Funding acquisition, Project administration, Supervision, Conceptualization, Writing – review & editing. DS: Supervision, Methodology, Conceptualization, Writing – review & editing, Formal analysis, Funding acquisition, Project administration, Resources.
Funding
The author(s) declare that financial support was received for the research and/or publication of this article. This project is funded by the European Union (Europäischer Fonds für regionale Entwicklung, EFRE), as part of the joint project CDNS: Center for Digital Neurotechnologies Saar.
Acknowledgments
The authors would like to thank the clinical staff involved in the study, particularly the physiotherapists at the orthopedic department, for their support during patient recruitment and data collection. Special thanks are also extended to all study participants for their valuable contributions.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Generative AI statement
The author(s) declare that Generative AI was used in the creation of this manuscript. Generative AI technologies were used to support the refinement of scientific text and the organization of methodological content. Specifically, ChatGPT (GPT-4; OpenAI, 2025) and Perplexity (model mixture using GPT-4, Claude, and other large language models; Perplexity AI, Inc., 2025) were employed to assist in language editing, structure suggestions, and phrasing improvements. All content has been critically reviewed and edited by the authors to ensure accuracy and integrity.
Any alternative text (alt text) provided alongside figures in this article has been generated by Frontiers with the support of artificial intelligence and reasonable efforts have been made to ensure accuracy, including review by the authors wherever possible. If you identify any issues, please contact us.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Stevens-Lapsley JE, Balter JE, Wolfe P, Eckhoff DG, Kohrt WM. Early neuromuscular electrical stimulation to improve quadriceps muscle strength after total knee arthroplasty: a randomized controlled trial. Phys Ther. (2012) 92:210–26. doi: 10.2522/ptj.20110124
2. Bohannon RW. Muscle strength: clinical and prognostic value of hand-grip dynamometry. Curr Opin Clin Nutr Metab Care. (2015) 18:465–70. doi: 10.1097/MCO.0000000000000202
3. Mizner RL, Petterson SC, Stevens JE, Vandenborne K, Snyder-Mackler L. Early quadriceps strength loss after total knee arthroplasty: the contributions of muscle atrophy and failure of voluntary muscle activation. J Bone Joint Surg. (2005) 87:1047–53. doi: 10.2106/JBJS.D.01992
4. Chopra S, Taunton M, Kaufman K. Muscle activation pattern during gait and stair activities following total hip arthroplasty with a direct anterior approach: a comprehensive case study. Arthroplasty Today. (2018) 4:27–32. doi: 10.1016/j.artd.2017.06.006
5. Flanigan DC, Everhart JS, Glassman AH. Psychological factors affecting rehabilitation and outcomes following elective orthopaedic surgery. J Am Acad Orthop Sur. (2015) 23:563–70. doi: 10.5435/JAAOS-D-14-00225
6. Lowe CJM, Barker KL, Dewey M, Sackley CM. Effectiveness of physiotherapy exercise after knee arthroplasty for osteoarthritis: systematic review and meta-analysis of randomised controlled trials. Br Med J. (2007) 335:812. doi: 10.1136/bmj.39311.460093.BE
7. Wang D, Hu Y, Liu K, Liu Z, Chen X, Cao L, et al. Issues in patients’ experiences of enhanced recovery after surgery (ERAS): a systematic review of qualitative evidence. BMJ Open. (2023) 13:e068910. doi: 10.1136/bmjopen-2022-068910
8. Tedesco D, Gibertoni D, Rucci P, Hernandez-Boussard T, Rosa S, Bianciardi L, et al. Impact of rehabilitation on mortality and readmissions after surgery for hip fracture. BMC Health Serv Res. (2018) 18:701. doi: 10.1186/s12913-018-3523-x
9. Merletti R, Holobar A, Farina D. Analysis of motor units with high-density surface electromyography. J Electromyogr Kinesiol. (2008) 18:879–90. doi: 10.1016/j.jelekin.2008.09.002
10. Holobar A, Farina D. Blind source identification from the multichannel surface electromyogram. Physiol Meas. (2014) 35:R143–65. doi: 10.1088/0967-3334/35/7/R143
11. Rojas-Martínez M, Serna LY, Jordanic M, Marateb HR, Merletti R, Mañanas MÁ. High-density surface electromyography signals during isometric contractions of elbow muscles of healthy humans. Sci Data. (2020) 7:397. doi: 10.1038/s41597-020-00717-6
12. Vieira TM, Botter A. The accurate assessment of muscle excitation requires the detection of multiple surface electromyograms. Exerc Sport Sci Rev. (2021) 49:23–34. doi: 10.1249/JES.0000000000000240
13. Bradford JC, Tweedell A, Leahy L. High-density surface and intramuscular EMG data from the Tibialis anterior during dynamic contractions. Sci Data. (2023) 10:434. doi: 10.1038/s41597-023-02114-1
14. Grison A, Guerra IM, Clarke AK, Muceli S, Pereda JI, Farina D. Unlocking the full potential of high-density surface EMG: novel non-invasive high-yield motor unit decomposition. J Physiol. (2024) 603(8):2281–300. doi: 10.48550/ARXIV.2410.14800
15. Drost G, Stegeman DF, Van Engelen BGM, Zwarts MJ. Clinical applications of high-density surface EMG: a systematic review. J Electromyogr Kinesiol. (2006) 16:586–602. doi: 10.1016/j.jelekin.2006.09.005
16. Merletti R, Temporiti F, Gatti R, Gupta S, Sandrini G, Serrao M. Translation of surface electromyography to clinical and motor rehabilitation applications: the need for new clinical figures. Transl Neurosci. (2023) 14:20220279. doi: 10.1515/tnsci-2022-0279
17. Farina D, Merletti R, Enoka RM. The extraction of neural strategies from the surface EMG: 2004–2024. J Appl Physiol. (2025) 138:121–35. doi: 10.1152/japplphysiol.00453.2024
18. Bernard J, Razanabola F, Beldame J, Van Driessche S, Brunel H, Poirier T, et al. Electromyographic study of hip muscles involved in total hip arthroplasty: surprising results using the direct anterior minimally invasive approach. Orthop Traumatol Surg Res. (2018) 104:1137–42. doi: 10.1016/j.otsr.2018.03.013
19. Wang Y-C, Wu S-H, Chen C-A, Liang J-M, Yang C-C, Chen C-H, et al. Compare the quadriceps activity between Mini-midvastus and Mini-medial parapatellar approach in total knee arthroplasty with electromyography. JCM. (2024) 13:2736. doi: 10.3390/jcm13102736
20. Tanzarella S, Muceli S, Del Vecchio A, Casolo A, Farina D. A high-density surface EMG framework for the study of motor neurons controlling the intrinsic and extrinsic muscles of the hand. 2019 41st Annual International Conference of the IEEE Engineering in Medicine and Biology Society (EMBC); Berlin, Germany: IEEE (2019). p. 2307–10 doi: 10.1109/EMBC.2019.8856825
21. Bedoy EH, Diaz G, Dalrymple EA, Levy AN, Hyatt I, Griffin T, et al. Improving localization and measurements of M-waves using high-density surface electromyography. J Neurophysiol. (2025) 133:299–309. doi: 10.1152/jn.00354.2024
22. Bosch LC, Beger SB, Duncan ST, Rossi SMP, Sculco PK, Barnes CL, et al. Intraoperative practice variability in total knee arthroplasty. J Arthroplasty. (2020) 35:725–31. doi: 10.1016/j.arth.2019.10.014
23. Pincus D, Jenkinson R, Paterson M, Leroux T, Ravi B. Association between surgical approach and Major surgical complications in patients undergoing total hip arthroplasty. JAMA. (2020) 323:1070. doi: 10.1001/jama.2020.0785
24. Roos EM, Lohmander LS. The knee injury and osteoarthritis outcome score (KOOS): from joint injury to osteoarthritis. Health Qual Life Outcomes. (2003) 1:64. doi: 10.1186/1477-7525-1-64
25. Nilsdotter AK, Lohmander LS, Klässbo M, Roos EM. Hip disability and osteoarthritis outcome score (HOOS) – validity and responsiveness in total hip replacement. BMC Musculoskelet Disord. (2003) 4:10. doi: 10.1186/1471-2474-4-10
26. Hermens HJ, Freriks B, Disselhorst-Klug C, Rau G. Development of recommendations for SEMG sensors and sensor placement procedures. J Electromyogr Kinesiol. (2000) 10:361–74. doi: 10.1016/S1050-6411(00)00027-4
27. De Luca CJ, Donald Gilmore L, Kuznetsov M, Roy SH. Filtering the surface EMG signal: movement artifact and baseline noise contamination. J Biomech. (2010) 43:1573–9. doi: 10.1016/j.jbiomech.2010.01.027
28. Mewett DT, Reynolds KJ, Nazeran H. Reducing power line interference in digitised electromyogram recordings by spectrum interpolation. Med Biol Eng Comput. (2004) 42:524–31. doi: 10.1007/BF02350994
29. Boyer M, Bouyer L, Roy J-S, Campeau-Lecours A. Reducing noise, artifacts and interference in single-channel EMG signals: a review. Sensors. (2023) 23:2927. doi: 10.3390/s23062927
30. Merletti R, Farina D, editors. Surface Electromyography: Physiology, Engineering, and Applications. 1st ed. Hoboken, NJ: Wiley. (2016). doi: 10.1002/9781119082934
31. Hyvarinen A. Fast and robust fixed-point algorithms for independent component analysis. IEEE Trans Neural Netw. (1999) 10:626–34. doi: 10.1109/72.761722
32. Sato W, Kochiyama T. Crosstalk in facial EMG and its reduction using ICA. Sensors. (2023) 23:2720. doi: 10.3390/s23052720
33. Winkler I, Haufe S, Tangermann M. Automatic classification of artifactual ICA-components for artifact removal in EEG signals. Behav Brain Funct. (2011) 7:30. doi: 10.1186/1744-9081-7-30
34. Fitzgibbon SP, DeLosAngeles D, Lewis TW, Powers DMW, Grummett TS, Whitham EM, et al. Automatic determination of EMG-contaminated components and validation of independent component analysis using EEG during pharmacologic paralysis. Clin Neurophysiol. (2016) 127:1781–93. doi: 10.1016/j.clinph.2015.12.009
35. Basmajian JV, DeLuca CJ. Muscles Alive: Their Functions Revealed by Electromyography. 5th ed., 2. print. Baltimore: Williams & Wilkins. (1986). p. 561.
36. Ozgünen KT, Celik U, Kurdak SS. Determination of an optimal threshold value for muscle activity detection in EMG analysis. J Sports Sci Med. (2010) 9:620–8. PMID: 24149789.
37. Zhang X, Zhou P. Sample entropy analysis of surface EMG for improved muscle activity onset detection against spurious background spikes. J Electromyogr Kinesiol. (2012) 22:901–7. doi: 10.1016/j.jelekin.2012.06.005
38. Stulen FB, De Luca CJ. Frequency parameters of the myoelectric signal as a measure of muscle conduction velocity. IEEE Trans Biomed Eng. (1981) BME-28:515–23. doi: 10.1109/TBME.1981.324738
39. Hägg GM. Comparison of different estimators of electromyographic spectral shifts during work when applied on short test contractions. Med Biol Eng Comput. (1991) 29:511–6. doi: 10.1007/BF02442323
40. Hägg GM. Zero crossing rate of electromyograms during occupational work and endurance tests as predictors for work related myalgia in the shoulder/neck region. Europ J Appl Physiol. (1991) 62:436–44. doi: 10.1007/BF00626617
41. Madeleine P, Leclerc F, Arendt-Nielsen L, Ravier P, Farina D. Experimental muscle pain changes the spatial distribution of upper trapezius muscle activity during sustained contraction. Clin Neurophysiol. (2006) 117:2436–45. doi: 10.1016/j.clinph.2006.06.753
42. Sanderson A, Martinez-Valdes E, Heneghan NR, Murillo C, Rushton A, Falla D. Variation in the spatial distribution of erector spinae activity during a lumbar endurance task in people with low back pain. J Anat. (2019) 234:532–42. doi: 10.1111/joa.12935
43. Kuruganti U, Pradhan A, Toner J. High-Density electromyography provides improved understanding of muscle function for those with amputation. Front Med Technol. (2021) 3:690285. doi: 10.3389/fmedt.2021.690285
44. De La Fuente C, Weinstein A, Neira A, Valencia O, Cruz-Montecinos C, Silvestre R, et al. Biased instantaneous regional muscle activation maps: embedded fuzzy topology and image feature analysis. Front Bioeng Biotechnol. (2022) 10:934041. doi: 10.3389/fbioe.2022.934041
45. Corvini G, Arvanitidis M, Falla D, Conforto S. Novel metrics for high-density sEMG analysis in the time–space domain during sustained isometric contractions. IEEE Open J Eng Med Biol. (2024) 5:760–8. doi: 10.1109/OJEMB.2024.3449548
46. De Oliveira DS, Casolo A, Balshaw TG, Maeo S, Lanza MB, Martin NRW, et al. Neural decoding from surface high-density EMG signals: influence of anatomy and synchronization on the number of identified motor units. J Neural Eng. (2022) 19(4):046029. doi: 10.1101/2022.02.05.479100
47. Aronson S. Moving toward preoperative optimization and value-based perioperative care. Tech Orthop. (2020) 35:2. doi: 10.1097/BTO.0000000000000436
48. Di Martino A, Keating C, Butsick MJ, Platano D, Berti L, Hunter LN, et al. Enhancing recovery: surgical techniques and rehabilitation strategies after direct anterior hip arthroplasty. J Orthop Traumatol. (2024) 25:45. doi: 10.1186/s10195-024-00786-y
Keywords: HD-sEMG, electromyography (EMG), rehabilitation, TJA, wearable EMG system, neuromuscular recovery, rehabilitation monitoring, functional indices
Citation: Morsch R, Böckenförde T, Wolf M, Landgraeber S and Strauss DJ (2025) Enhanced rehabilitation after total joint replacement using a wearable high-density surface electromyography system. Front. Rehabil. Sci. 6:1657543. doi: 10.3389/fresc.2025.1657543
Received: 11 July 2025; Accepted: 29 September 2025;
Published: 16 October 2025.
Edited by:
Björn Krüger, University of Bonn, GermanyReviewed by:
Robert LeMoyne, Northern Arizona University, United StatesNelson Azevedo, Instituto Superior de Saúde do Alto Ave, Portugal
Copyright: © 2025 Morsch, Böckenförde, Wolf, Landgraeber and Strauss. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Richard Morsch, cmljaGFyZF9hbGV4YW5kZXIubW9yc2NoQHVuaS1zYWFybGFuZC5kZQ==