 Cássio Silveira1*†
Cássio Silveira1*† Colin Forsyth2†
Colin Forsyth2† Nivaldo Carneiro Junior1,3†
Nivaldo Carneiro Junior1,3† Alejandro Goldberg4,5†
Alejandro Goldberg4,5† Lia Maria Britto da Silva6†
Lia Maria Britto da Silva6† Rubens Antonio da Silva7†
Rubens Antonio da Silva7† Maria Aparecida Shikanai-Yasuda8,9†
Maria Aparecida Shikanai-Yasuda8,9†- 1Department of Collective Health, School of Medical Sciences of Santa Casa de São Paulo, São Paulo, Brazil
- 2Drugs for Neglected Diseases initiative – Latin America (DNDi), Rio de Janeiro, Brazil
- 3Departamento de Saúde da Coletividade, Centro Universitário Faculdade de Medicina do ABC, Santo André, São Paulo, Brazil
- 4National Council for Scientific and Technical Research of Argentina (CONICET), Institute of Anthropological Sciences, Buenos Aires, Argentina
- 5Graduate Program in Collective Health, University of Brasília, Brasília, Brasília-DF, Brazil
- 6Division of Psychology, Hospital das Clínicas, School of Medicine, University of São Paulo, São Paulo, SP, Brazil
- 7Secretaria de Estado da Saúde de São Paulo, Superintendência de Controle de Endemias, São Paulo, Brazil
- 8Department of Infectious and Parasitic Diseases, Faculdade Medicina, University of Sao Paulo, São Paulo, Brazil
- 9Laboratory of Medical Investigation in Immunology (LIM 48), Hospital das Clínicas, Faculdade de Medicina, University of Sao Paulo, São Paulo, Brazil
Background: Transnational immigrants are particularly impacted by neglected diseases, which take a heavy biological, social, and emotional toll in these marginalized communities. Chagas disease has transformed from an exclusively rural to an increasingly urban phenomenon encompassing non-endemic areas in Latin America.
Methods: Through semi-structured interviews, we investigated representations of Chagas disease in Bolivian immigrants in São Paulo, Brazil. Between August and September 2015, 27 adult migrants were interviewed, 11 of them with Chagas disease. We explored problems of access to health services and essential knowledge about the disease, as well as related conceptions and health practices.
Results: Participants constructed social representations of Chagas through interactions with family and social networks, drawing on earlier experiences in Bolivia. Diagnosis often provoked fear, and participants faced barriers to care based on language differences and uncertainties about the disease and treatment options. Healthcare personnel played an important role in alleviating concerns and facilitating access to information.
Discussion: The complex intersection of migration and neglected diseases creates challenges for local and national health programs, requiring innovative responses incorporating the perspectives and needs of the often vulnerable affected communities.
Introduction
Chagas disease, a neglected parasitic infection affecting 6-7 million people worldwide, has historically been associated with rural areas and marginalized communities (1). In a changing environmental and political scenario, the epidemiological profile and ecological pattern of the disease have transformed through efforts to control its transmission as well as social processes in Latin America, including rapid urbanization, intensified migration, and increased globalization (2). In light of these transformations, Chagas disease has ceased to be an exclusively rural problem, becoming an increasingly urban issue which has also emerged in non-endemic areas (2, 3).
Chagas disease includes multiple components making its analysis complex. Biological (T. cruzi transmission and pathology) environmental (interactions between humans, vectors, and host species), geo-economic (occupation of endemic areas and urban development), socio-cultural (knowledge, traditions, and formal education) and political aspects (policymaking, civil society participation, and the response capacity of the health system) require the combination of diverse branches of scientific knowledge into an intricate epistemological web (4–6).
Control and prevention of Chagas disease must necessarily prioritize its forms of transmission: via triatomine insect vectors, uncontrolled blood transfusion and organ transplants, and vertical and oral transmission. Public health strategies now emphasize early detection of the infection as timely treatment can achieve serological cure in the acute and early chronic phase of the disease; prevent future congenital transmission; and/or halt the progression of the disease in chronically infected individuals without severe organ involvement (7–9).
Chagas disease still represents a major public health concern in Brazil, particularly in the context of contemporary migratory flows. The estimated prevalence of T. cruzi infection in Brazil is 1% to 2.4% (7). A complex set of social and environmental factors have shaped the endemicity of the disease in Brazil, and social inequalities continue to hamper efforts to advocate for stronger interventions and control, despite over a century of study, debate, and public discourse around the disease (10, 11).
Chagas disease in the context of international migration
The theoretical and explanatory framework of Chagas disease has been enriched in recent decades through extensive, in-depth interpretations. Since the determination of its tropical origin in the early 20th century by Brazilian scientist Carlos Chagas, knowledge of the disease has advanced and developed an explanatory potential in the context of epidemiology. Subsequently, as the relevance of social factors became increasingly clear, the scientific community was urged to move beyond strictly biological explanations and incorporate investigation of the health-illness-care process (6, 11).
From the natural to the social context, the understanding of Chagas disease has become more comprehensive through analysis of the complex relationships that help give the disease visibility as a social issue. For instance, Briceño-León (12, 13) analyzes the role of major sociohistorical processes in the transformation of Chagas disease’s epidemiology and the subsequent development of new knowledge. Briceño-León discusses how economic development in South America shaped the epidemiology of the disease, dating back to the colonial and even Pre-Columbian era as agricultural activities expanded into lands where Chagas disease existed as a zoonosis, to the rise of the global economic system with intensified circulation of capital, commodities and workers and the ongoing expansion of agricultural boundaries and settlement in the Amazon region. In the current era of globalization, and in light of intense socioeconomic inequalities, migrants from traditional endemic areas in Latin America are often compelled to cross borders looking for work opportunities (11, 14).
Consequently, the expansion of Chagas disease to other continents has been evidenced in the last few decades. The situations of people with Chagas disease who immigrated from countries in South America, Central America and Mexico to the United States, Spain and elsewhere have evidenced the fragility and limited capacity of healthcare systems in non-endemic countries that receive migrants to provide adequate care for people infected by the disease (13, 15, 16). European and other host countries have sought to exercise enhanced control over transfusions, transplants, and the vertical transmission of the disease (17, 18).
A very common representation of Chagas disease found in the literature, particularly in epidemiological and/or biomedical approaches to the disease, personifies the immigrant as a disease carrier, that is, someone who represents a risk of illness communication and transmission. Sargent and Larchangè (19) questioned these direct correlations between infectious diseases and immigrants as risk groups. Even in relation to articles produced in the social sciences, the authors noted that the discussions prioritized South-to-North immigrants, especially to the United States and Western Europe, disregarding broader contextual analyses. This reveals a descriptive and analytical framework that places immigrant groups at the epicenter of studies on the processes of illnesses.
From this perspective, some studies also include socio-cultural aspects in the approaches to Chagas disease, contextualizing it based on the complexity of the relationships involved in the process of becoming ill. Some examples are migratory processes from rural to urban areas, social representations, awareness of the disease, healthcare providers’ ability to intervene and address the disease, and access barriers to healthcare services (20–22).
Approaches that suggest overcoming the theoretical framework of methodological nationalism in migratory analyses, particularly in the field of health, end up reinforcing the debate on notions of risks of illness and insecurity (23). Through a socio-anthropological approach, Goldberg (24) has broadened this debate by introducing a different side to the representations of Chagas disease, reconstructed with Bolivians established in Barcelona, Spain. According to the author, a factor that contributes to keeping the disease invisible is a tendency to naturalize it in the concept of the immigrants, who identify it as part of a cosmovision that incorporates elements of the forms of transmission that are naturally present in their lives and the lives of their ancestors. Alternatively, Auger (25) and Sanmartino et al. (26) associate the idea of invisibility with the creation of multiple representations by society as a whole that Chagas disease exclusively affects poor populations. This reinforces the causal notion of the disease, centered on immigrants as transmitters, but ignores many of the complexities and heterogeneities of the migratory phenomenon, e.g. people who are able to immigrate precisely because they are not subjected to the immobility caused by poverty. On the contrary, many immigrate because they are part of migratory networks based on family and/or work relationships that structure and support displacements, while others may be compelled to flee political or social violence.
Illness can be conceived as a symbolic event of human existence, in which the subject-patient reconstructs their own being in the world, subsequentially reconstructing them again by re-signifying the experience of being ill within historical, relational and socio-cultural frameworks. Thus, the disease is considered not as a mere biological fact, but as a cognitive and transformational process, a social, cultural, political, historical and economic phenomenon. The experience of the disease goes beyond identifying pathology and implementing an adequate preventative or therapeutic response. It is inscribed in the bodies of the suffering subjects, the relationships they establish, in the meanings they elaborate in their daily lives, and the knowledge they generate (27).
The experience of Chagas disease can be considered a system of relationships in which one constructs meanings and attributes causes, with knowledge and imaginary ideas, symptoms and symbols, practices and attitudes. One approach to exploring this is to examine the subjective dimension of the body (27) reconstruct the categories used to represent and define symptoms in a relational and contextual way (28), and to understand the value of people’s narratives as protagonists of their own stories and actors in their own realities (29).
The present study describes part of the results of an interdisciplinary research project on Chagas disease in a population of migrant Bolivians in the city of São Paulo that showed a 4.4% prevalence of T. cruzi infection in a sample of 633 Bolivians residing in São Paulo (30). This article has been structured to problematize the socio-historical and public health interpretation of Chagas disease, discussing its socio-cultural complexity, while circumscribing the debate in the context of international migration in South America. The objective is to present the social representations of Chagas disease in the socio-cultural universe of Bolivian migrants living in the central area of São Paulo city.
Methods
This study aims to produce new knowledge on the Bolivian migrant population and their health-illness-care processes related to Chagas disease in the context of the urban social interactions in which they are inserted as immigrants. To do this, a limited number of subjective aspects (beliefs, representations, points of view, and assessments) were investigated aiming to establish relationships. Based on interpretive medical anthropology, this study emphasizes the representations, meanings and explanations the subjects produce about health, the disease and its care (31). This theoretical perspective, in close relationship with phenomenology, prioritizes the actors’ points of view, their narratives, experiences and practices, as well as the perspective of constructivism, which assumes an understanding of how people construct and reconstruct their healthcare strategies.
Participants and procedures
This was an exploratory study designed to collect qualitative data on participants’ experiences, including access to healthcare, and social representations of Chagas disease. We interviewed a convenience sample of Bolivian patients who were seen at a health center. By qualitative data we refer to patients’ own narratives about Chagas disease, which are converted to text for qualitative analysis to identify major themes.
During the second half of 2015, we asked Bolivian patients undergoing Chagas disease testing at the Barra Funda Centro de Saúde Escola (CSE, Learning Health Center) “Dr. Alexandre Vranjac,” a primary healthcare facility located in the central area of São Paulo city, to participate in an interview on Chagas disease. This disease was confirmed by two high-profile serological tests positive for IgG anti - Trypanosoma cruzi. Initially, Chagas test ELISA III (Bioschile Ingenieria Genetica SA, Santiago, Chile) and ELISA cruzi (BioMerieux Diagnostics SA, Rio de Janeiro, Brazil), containing epimastigote antigens were employed according to manufacturer instructions. In case of discordant results (one positive and one negative), confirmatory tests were performed by Tesablot anti-surface antigens of trypomastigotes (32) recombinant ELISA with trypo- and epimastigote antigens (ELISA Chagatest® Wiener Lab, Rosario, Argentina), according to manufacturer instructions.
The data collection technique used was an individual interview with a semi-structured script (Supplementary Appendix). This technique was chosen because of its potential to provide authenticity and spontaneity in the interviewee’s discourse. The scripts were developed through a discussion process between the researchers in charge of this task and the technical supervisors of the healthcare services throughout the preparation of the research protocol. Two field researchers fluent in Spanish were hired, and they translated the interview script and carried out data collection.
The interview script sought to encompass certain aspects considered critical to understanding the process of becoming ill and of care related to Chagas disease, and it includes the following topics: access to healthcare services in their country of origin; the practice of traditional medicine; diagnosing the disease; the migration process; access to healthcare services in Brazil; and social representations of Chagas disease.
Data collection included digital recording, and the interviews took place in the service provision space. The interviewees were previously invited by the CSE staff during earlier stages of the research. Everyone who agreed to participate in the interview signed an informed consent, and the project was approved by the Ethics and Research Committee of the Hospital das Clínicas from the University of São Paulo School of Medicine (protocol 196.698/2013).
Analysis of qualitative data did not distinguish between interviewees with and without Chagas disease, to fulfill the initial intention of learning about social representations of this disease (33) on the part of immigrants. After the field research, the audio files containing the interviewees’ discourse were fully transcribed as text typed in Word format, and the following process was followed: (1) analysis of the transcribed material, considering each interview in its entirety and highlighting similarities, differences, and articulations in the narratives; (2) then, portions considered essential to understand the ideas contained in the interviewees’ discourses, representing the expression of what was most important to understand their intentions were highlighted; and (3) after the empirical material was reduced through notes and systematizations, the themes considered most important in the narratives were assessed, resulting in the formulation of the analysis.
Finally, an interpretive qualitative approach was adopted, aiming to examine the meanings of the representations and issues related to Chagas disease. The investigation sought to cover an extensive, complex, and often contradictory universe, influenced by health institutions, families, information obtained from various types of media, informal information exchanges, and even more immediate perceptions that explain conceptions about Chagas disease. Through this approach, health and illness are considered to be culturally constructed notions and are articulated as a culturally constructed explanatory model. Thus, biology, social practices and meanings attributed to illness processes formed a set of interactive processes, organizing the illness as a social object and as a life experience (31, 34).
Results
We interviewed 27 Bolivian immigrants: 18 women and 9 men between the ages of 18 and 30. Seventeen 17 (63%) had Chagas disease, confirmed by two positive serological tests for IgG antibodies anti-Trypanosoma cruzi while 10 (37%) tested negative (Table 1). The majority of respondents came from the departments of La Paz and Santa Cruz (9 and 6, respectively), and had lived in the city of São Paulo for at least five years. Regarding the migration process of the interviewees, only one reported passing through Argentina, a country bordering Brazil, which is also home to a large contingent of Bolivian migrants. The others went directly to São Paulo city without passing through any other city or state in Brazil.
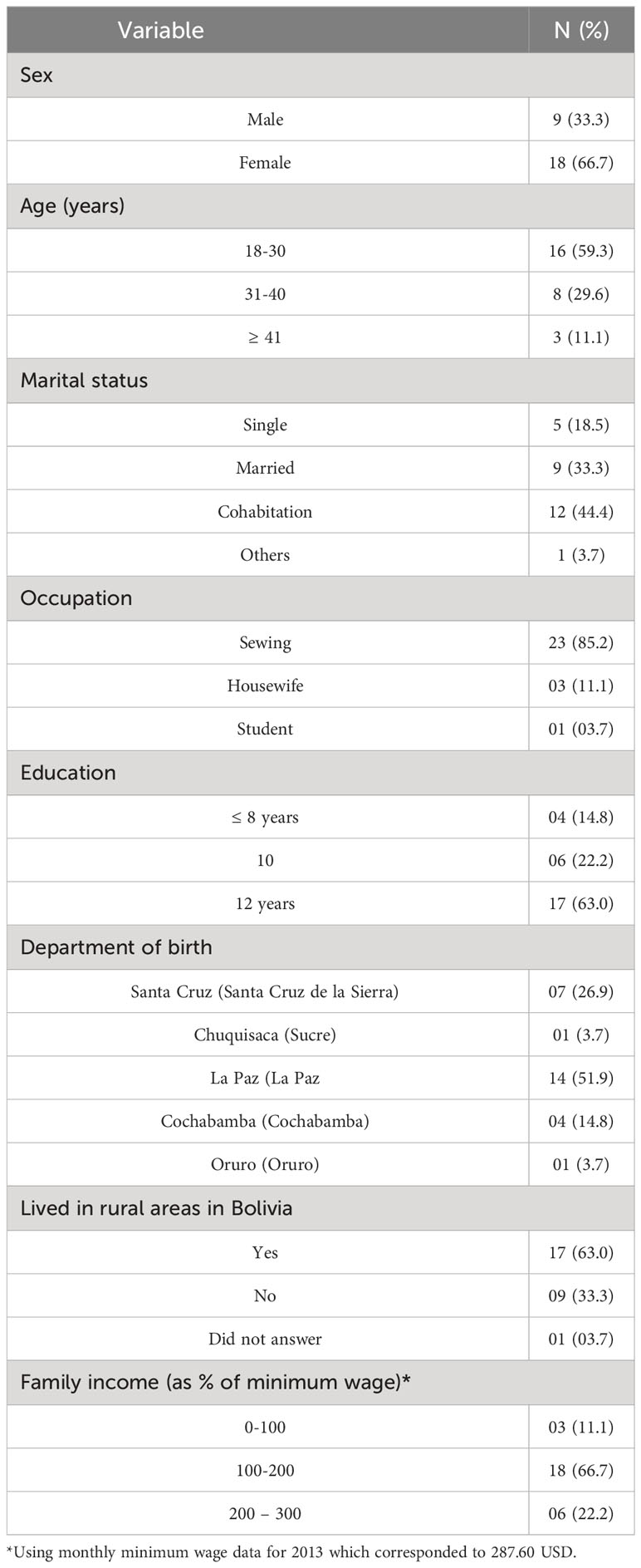
Table 1 Sociodemographic characteristics of Bolivian immigrants.
Respondents reported the availability of free or low-cost healthcare services when they had lived in Bolivia, but some access challenges, especially in rural areas:
[The] Bolivian government provides free tests, or at a lower price, to detect kidney disease, heart disease or Chagas disease in suburban or peri-urban zones. In rural zones there aren’t many health centers. (E22)
In this context, consultation of traditional Andean medicine healers and the use of medicinal plants for treatment were reported as healthcare alternatives. Respondents also mentioned receiving advice from relatives, especially elderly people, such as parents and grandparents, and in some cases sought out people known to the family to give advice or to intervene to ease suffering.
Access to healthcare in São Paulo
Contact with public healthcare services in the city of São Paulo was generally considered positive by the interviewees. An important point in their narratives is availability through primary healthcare, particularly through the Family Health Strategy (Estratégia Saúde da Família, ESF) and via Community Health Agents (Agentes Comunitários de Saúde), who carry out a proactive approach to the population (35–37). However, there are still problems with access to healthcare services. Several respondents described challenges in navigating linguistic differences with healthcare personnel.
I came here when I was pregnant. It was very difficult because I didn’t know the language, I couldn’t talk. Communication was very difficult, but I received good service. (E16)
I got in contact with the service through friends. The attention is good. The problem is the Portuguese. They didn’t speak my language. There were no leaflets, but the doctor saw me. (E24n)
My mother couldn’t understand Portuguese and she didn’t know what I had. I was hospitalized. (E21)
Due to the language barrier, respondents reported relying on relatives, close friends, or other immigrants who were already familiar with the services, to accompany them to the clinic, help them obtain care, communicate health issues, and translate procedures and referrals, as in the examples below.
There was a girl who spoke Spanish. My aunt told me we had to find her. She explained everything to me. (E5)
At first, it was very difficult, because of the language. But a relative took me to the emergency clinic. (E15)
With a relative who already understood the language. It was very good. At the health clinic. When I went with my relative, it was easy. When I didn’t, it was torture. I couldn’t understand a thing. (E25)
Another challenge reported by respondents was navigating administrative and logistical barriers to obtain care. In some cases, there was limited availability of appointments or other procedures (exams, surgical interventions, etc.), or incompatibility between available appointment times and respondents’ schedules, as Carneiro Junior et al. (38) have pointed out. Some respondents reported long delays:
The service is good, but it’s a hassle, it takes too long. When you have a child with special needs, you suffer a lot. (E23)
Everything was sorted out, but it took a long time. (E2)
Sometimes it’s easy, but usually it takes a long time. (E26n)
Limitations on access to healthcare services are mostly related to how the system works and the complex, multiple barriers immigrants face.
However, other respondents reported positive experiences with the healthcare services and respectful communication from healthcare personnel, despite the potential for long waits.
The services were very good at the clinic and at AMA [Atendimento Médico Ambulatorial (Out-patient Medical Clinic), a medium-complexity emergency unit]. They care for you with respect and give you information, but it takes time, too long, for you to be seen. (E15)
[The attention is] very good. They talk to you slowly, help you understand, and they repeat it. (E6)
Respondents also described how Brazil’s system of universal care (Sistema Único de Saúde, SUS) facilitated their healthcare access.
Yes, I know this service. They give you a card with which you can be seen at the clinic or at the hospital. It’s very good. (E11)
Yes. Through SUS you can get medical care, hospitals and emergency rooms without paying anything. (E16)
Yes, it’s very good. The service is good and you don’t have to pay. (E25)
Awareness of Chagas disease
Interviewees expressed some prior awareness of Chagas disease before arriving in Brazil, outlining various elements that were sometimes in conflict with the biomedical model. Knowledge about Chagas disease was typically acquired through networks of friends and relatives, as well as television and public awareness campaigns.
Some respondents had only heard of Chagas disease but did not have personal experiences as reference points. “I had heard about it, but I didn’t know what it was,” commented one respondent (E17). Another had heard about Chagas through television and noted “In Bolivia, there are many people with the disease.” (E7) Other respondents were familiar with Chagas through fumigation or awareness campaigns in Bolivia:
Yes, people were always mentioning it in the village where I lived. The houses were always fumigated with products. (E25)
They taught about it in school. Also, doctors went where I lived to talk about Chagas, because I lived in the countryside. They went to teach about this topic. (E8)
In other cases, respondents were more closely familiar with Chagas because a neighbor or family member had had the disease. When asked if they had heard of Chagas, one respondent answered “Yes, a neighbor, as a child, was bitten by a vinchuca and died.” (E1) Others noted that their father or mother had the disease.
Knowledge of the vector
Some respondents discussed the insect vector, known as vinchuca in Bolivia, including reporting its presence in the domestic environment and its role in disease transmission. For example, one participant described how, “In some houses, the vinchucas live in beds and mattresses.” (E1) At least one respondent had not realized the connection between vinchucas and Chagas disease: “I only knew the vinchuca, that’s all. I didn’t know what diseases it caused.” (E20) However, several other respondents described the role of the vinchuca in Chagas disease transmission:
All I knew was that it was a disease that was in the blood because of an animal bite, but in Bolivia I didn’t know I had the disease. (E12)
It was transmitted through the bite of a Chagas insect, usually in suburban zones. (E22)
Through the vinchucas, which you call barbeiros. (E3)
Yes, through a bite. You scratch yourself and it enters your blood. (E26n)
In some cases, knowledge of Chagas disease vector transmission had been acquired in Bolivia, whereas others reported learning this from healthcare personnel in Brazil.
Chagas disease pathology and impact
Respondents who had personally known someone with Chagas disease described its effects both in terms of its potential lethality and its impact on work and daily activities. One respondent recounted that her mother had died of Chagas disease in Bolivia. “She no longer worked. She was much older. She died at 82.” (E3) Another participant also described a family member who had died from Chagas heart disease. “It was someone from my family. It was their heart. It affected their heart.” (E19) In other cases, participants described relatives or friends who had been hospitalized or suffered significant morbidity from Chagas disease.
My mother. It affected her heart, which got worse, became enlarged, they had to put in a pacemaker. She was unable to work. (E12)
My father … he’s still doing treatment. He feels very tired and his body aches. (E14)
In Bolivia, the lady who worked with me, she told me. She even had this disease, but she didn’t explain it well. She was at the hospital, but she had been cured. (E6)
The person I knew couldn’t breathe, they felt very tired, nervous, couldn’t do heavy work. (E16)
Of note, two of these respondents specified the limitation Chagas disease imposed on the ability to work. However, other respondents recognized the indeterminate, asymptomatic form of Chagas disease. According to one participant, “In Bolivia I always heard about it, but I never saw a person with the disease. You can’t see who is ill.” (E7) Another mentioned their father had the indeterminate form of Chagas and was able to maintain a normal life. “My father is still alive and is well, normal. There were no changes to his work or his longevity.” (E8) Another commented “I know that the person [with Chagas disease] is able to work” (E26n).
Treatment
While some respondents were already familiar with the potential impact of Chagas disease, others became aware through interaction with healthcare personnel in São Paulo. One respondent who had not previously heard of Chagas disease commented, “What they explained to me is what it can cause some time from now. This they explained to me.” (E15) Learning of Chagas disease motivated interest in starting treatment for those with the indeterminate form. “Now that I’m aware of [the disease], I want to know if it can be treated,” said one participant (E7). “I’ve never felt anything.” Another respondent described not only learning about Chagas disease, but about the possibility of treatment after talking to healthcare personnel in São Paulo. “Now I know. I didn’t know before. As far as I know, there was no treatment before. Now I’m learning that there is.” (E8) In another case, the participant stressed the importance of seeing the results of diagnostic tests before considering treatment. “There is treatment, the doctor told me, but I want to see the results of the tests they did with me.” (E10)
However, knowledge of Chagas disease could also cause considerable worry or concern in respondents:
I was asking about this, if that’s the case, because I’m afraid. I think that it’s like AIDS, that it’s incurable. I think it’s similar, so I’m afraid. (E9)
This respondent’s concern about the availability of treatment led them to perceive Chagas disease as something “incurable” as well as lethal, similar to AIDS, provoking understandable fear.
Discussion
We sought to describe the individual experiences of Bolivian immigrants in the city of São Paulo regarding Chagas disease, including access barriers to healthcare, treatment pathways, awareness, and social representations of the disease. Various respondents reported positive experiences with local healthcare personnel and an understanding of the universal access to care provided within the SUS, yet still reported challenges navigating logistical challenges related to delays, bureaucracy, and work schedules, as well as linguistic barriers (Table 2).
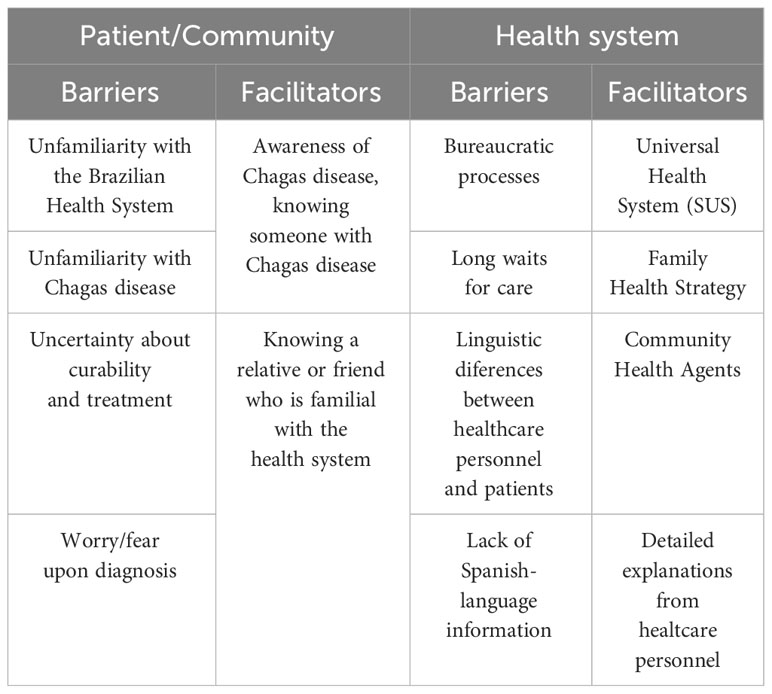
Table 2 Barriers and facilitators for patient/community and of the healthcare system.
Participants’ social representations of Chagas disease are constructed primarily through interactions with social networks – through stories of friends, neighbors, and relatives who suffered from the impacts of the disease, as well as healthcare personnel. Chagas was described as a debilitating disease which impacts the heart, in many cases limiting essential functions such as work or family life. Chagas was linked with past experiences of encountering the vector earlier in life in rural Bolivia. Some participants described the importance of being able to initiate treatment, yet faced important access barriers linked with daily life challenges (39–44). Ultimately, Bolivian immigrants’ health-seeking strategies and opportunities for accessing care in São Paulo depend on diverse factors, including migration policies, possibilities to join the workforce, and social representations about the use of healthcare services by non-natives, among other examples (45).
Similar to previous studies, we found that previously knowing someone with Chagas disease played a critical role in shaping participants’ social representations. In some cases, this may also increase fears about the implications of the disease; however, other participants did not express major concerns about their Chagas diagnosis as long as the illness was asymptomatic. Just as Sanmartino (46) observed in Bolivian and rural-to-urban migrants in Buenos Aires, Chagas disease did not have precedence over other types of problems faced in their day-to-day lives (46). To some of the interviewees in our study, nothing changed in their lives after learning about their health status, even when T. cruzi infection was confirmed. Things could remain in a state of normalcy “porque no es algo que te duele” (“because it’s not something that hurts”) (E15) – a clear allusion to the invisibility of the disease until symptoms can be detected, and the body expresses the need for healthcare measures because of the symptoms (24). Nonetheless, for others, a positive diagnosis led to considerable concern, as observed in other studies. For instance, Valdez-Tah describes how a positive diagnosis disrupts the sense of normalcy in the lives of immigrants in California (47). The phenomenon of indeterminate T. cruzi infection as a latent risk, and its impact on emotions and health-seeking, is discussed in-depth in Ventura-Garcia’s study among Bolivian women in Catalonia, Spain (48).
Chagas disease, as a phenomenon that is invisible and cannot be perceived through the senses, is related to its asymptomatic nature and, along with limited healthcare access, perpetuates its underdiagnosis (24). Respondents reported uncertainties about the meaning of test results or potential health impacts of the disease, indicating a greater need for communication and education strategies targeted to this population (49). Such interventions can help promote immigrant health, reconfiguring notions, customs and practices, as long as they are carried out with the involvement and agreement of the immigrants themselves.
Prior studies have reported limited awareness of Chagas disease among Bolivian migrants, despite the high prevalence of the disease in Bolivia. A study by Silva et al. (14) examining knowledge of Chagas disease among Bolivians in São Paulo reports that 47.7% of those interviewed were familiar with the vector, 22.5% had noticed the vector in their homes, and 35.8% were aware of Chagas disease (14). Another study among Bolivian migrants in Madrid also found that knowledge of symptoms and biomedical diagnosis and treatment of Chagas disease was limited (50).]. Our study suggests that word-of-mouth communication in social networks and interactions with healthcare providers play an important role in strengthening awareness of Chagas disease and the available biomedical care options.
Our study adds to the growing literature on Chagas disease in the context of transnational migration. Migration of people with Chagas disease highlights inequities in healthcare processes, as well as the lack of articulation between national programs to address the needs of this population (6, 10, 11, 15, 43, 47). For Bolivians residing in São Paulo, social inequities rooted in historical processes in their home country continue to be relevant in Brazil, although the migratory context presents both new challenges (such as linguistic barriers) and new opportunities (the possibility of universal health coverage)
Indeed, perspectives for obtaining healthcare may be reinforced through regular access to healthcare services (35, 38). Even so, barriers to healthcare services are still observed. The language barrier creates obstacles to effective communication between affected people, their families, and healthcare services, impacting the healthcare process from screening and consultation to care and follow-up (38, 47, 51, 52). This poses a major challenge in facing the disease’s complexity and navigating the different ocial representations of Chagas on the part of healthcare providers and transnational immigrants affected by the disease.
Adding to the difficulties in overcoming the limitations created by the different socio-cultural perspectives in the context of healthcare services, there are the distant and often isolated relationships of immigrants’ life experiences in the city where they now live, particularly in terms of healthcare services, a space where different notions of health and illness meet. Even if the participants of this study have access to healthcare services and consider this situation positive, it can still represent a significant investment in terms of travel time, the implications of potential indirect costs due to lost work time, as well as challenges related to transportation, childcare and other logistical aspects of their daily lives. These factors were also mentioned as important barriers to the diagnosis and treatment of Chagas disease in Bolivia (21), Colombia (22), Italy (51) and the United States (52).
An important limitation of our study is the small sample size, and the fact that we rely on a convenience sample, which largely prevents us from making subgroup comparisons. Finding seropositive participants from within this population, given the underdiagnosis of T. cruzi infection and the challenges in accessing healthcare, was one factor limiting our sample size. However, we considered the final sample size adequate to reach saturation where new themes in qualitative data analysis were no longer emerging (53). Further, we relied on semi-structured interviews and did not incorporate other methods which could have provided additional insights into participants’ social representations of Chagas. Another limitation is that our data collection took place in 2015, and major events such as the COVID-19 pandemic have occurred since then. New research could help shed light on how representations of Chagas disease in this community might have changed during this period. Our results may not be generalizable to other groups in different geographic and sociocultural contexts.
Our study focused on collection of qualitative data and was part of a larger multidisciplinary study examining Chagas disease in the Bolivian community of Sao Paulo from various perspectives (5, 14, 30). Qualitative research provides an important complement to quantitative studies, as it can highlight concepts and processes that would be lost in a pure analysis of numerical data. However, quantitative methods from the social sciences could also be employed to gain insight into this and other communities’ social representations of Chagas disease (21), which could be a fruitful direction for future research.
Obstacles to diagnosis and treatment of Chagas disease have been described as multidimensional, encompassing social, biological, psychological and other areas (15, 54–56) For immigrants, the social and economic inequalities that increase the risk of contracting Chagas disease also hinder access to healthcare, while in many cases also placing a significant burden on emotional well-being. As a result, solutions to approach this neglected disease require a multidisciplinary framework that addresses the structural factors that contribute to creating the access barriers, while considering the social and emotional impact created by the disease (56). Communication strategies must consider common representations of Chagas disease among the population as well as the influence of immigration, gender, age and other factors on access to healthcare and strategies for looking for these services.
This debate can be expanded by creating and practicing healthcare strategies that recognize and incorporate the cosmovision of the diverse ethnic and/or national groups in the healthcare system, considering as well the socio-cultural diversity that shapes the thoughts and practices of immigrants, and the social inequalities that hinder their healthcare access. Improving access to information about relevant diseases, forms of prevention, and management is an excellent start to expanding the protection and promotion of the health of immigrating people and families. This can help overcome inequities that subject immigrants and other vulnerable individuals, including children and elderly people, to illness and suffering processes that cannot easily be addressed through the support provided by family and social networks. The particular healthcare barriers affecting this population, and others impacted by Chagas and other neglected diseases, are shaped both by local contexts and broader structural inequalities. While there are no quick fixes to these longstanding issues, safeguarding the universal human right to health and incorporating the perspective of immigrant communities in the design of programs and materials to address relevant health concerns is a promising way forward.
Data availability statement
Because of the sensitive nature of the underlying data, requests for access to the raw data will be evaluated on a case-by-case basis. Further queries can be directed to the corresponding author.
Ethics statement
The studies involving humans were approved by the Ethics and Research Committee of the Hospital das Clínicas da Faculdade de Medicina, University of São Paulo, Brazil (protocol# 196.698/2013). The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
Author contributions
CS: Conceptualization, Data curation, Formal analysis, Investigation, Methodology, Project administration, Supervision, Validation, Visualization, Writing – original draft, Writing – review & editing. AG: Writing – review & editing. NCJ: Conceptualization, Formal analysis, Project administration, Validation, Writing – review & editing. LB: Formal analysis, Writing – review & editing. CF: Writing – original draft, Writing – review & editing. RD: Writing – review & editing. MS-Y: Conceptualization, Funding acquisition, Project administration, Resources, Writing – review & editing.
Funding
The author(s) declare financial support was received for the research, authorship, and/or publication of this article. This research was funded by Conselho Nacional de Desenvolvimento Científico e Tecnológico (CNPq: 404336/2012-4), Ministério da Ciência e Tecnologia e Inovação, Brazil. The funder was not involved in the study design, collection, analysis, data interpretation, or manuscript writing.
Acknowledgments
We would also like to thank the directors and all the staff from Centro de Saúde Escola Barra Funda “Doutor Alexandre Vranjac” (Irmandade de Misericórdia da Santa Casa de São Paulo) for their support and interest in the development of this study. DNDi is grateful to its donors, public and private, who have provided funding to DNDi since its inception in 2003. A full list of DNDi donors can be found at http://www.dndi.org/donors/donors.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fitd.2024.1331026/full#supplementary-material
References
1. World Health Organization. Chagas disease in Latin America: an epidemiological update based on 2010 estimates. Wkly Epidemiol Rec. (2015) 90(6):33–43.
2. Schmunis G, Yadón Z. Chagas disease: a Latin American health problem becoming a world health problem. Acta Trop. (2010) 115:14–21. doi: 10.1016/j.actatropica.2009.11.003
3. Briceño-León R, Galván J. The social determinants of Chagas disease and the transformation of Latin America. Memorias Do Instituto Oswaldo Cruz. (2007) 102:109–12. doi: 10.1590/s0074-02762007005000095
4. Dias JCP, Cláudio LDG, Lima MM, Albajar-Viñas P, Silva RA, Alves RV, et al. Mudanças no paradigma da conduta clínica e terapêutica da doença de Chagas: avanços e perspectivas na busca da integralidade da saúde. Epidemiol Serv Saúde. (2016) 25:87–90. doi: 10.5123/s1679-49742016000500003
5. Shikanai Yasuda MA, Sátolo CG, Carvalho NB, Atala MM, Ferrufino RQ, Leite RM, et al. Interdisciplinary approach at the primary healthcare level for Bolivian immigrants with Chagas disease in the city of São Paulo. PLoSNegl Trop Dis. (2017) 11:e0005466. doi: 10.1371/journal.pntd.0005466
6. Silva LJ. A evolução da doença de Chagas no estado de São Paulo. Rio de Janeiro, Brasil: Editora Hucitec (1999).
7. Dias JCP, Ramos AN Jr., Gontijo ED, Luquetti A, Shikanai-Yasuda MA, Coura JR, et al. II Consenso Brasileiro em Doença de Chagas, 2015. Epidemiol Serv Saúde. (2016) 25:7–86. doi: 10.5123/s1679-49742016000500002
8. Pan American Health Organization. Guidelines for the diagnosis and treatment of Chagas disease (2019). Washington, DC: PAHO (Accessed 11 December 2022). Available online: Guidelines for the diagnosis and treatment of Chagas disease (who.int).
9. Ending the neglect to attain the Sustainable Development Goals: a road map for neglected tropical diseases 2021–2030 (2020). Geneva: World Health Organization (Accessed 11 December 2022). Available online: Ending the neglect to attain the Sustainable Development Goals: A road map for neglected tropical diseases 2021–2030 (who.int).
10. Ramos AN Jr., Carvalho DM. Os diferentes significados da certificação conferida ao Brasil como estando livre da doença de Chagas. Cad Saúde Pública. (2001) 17:1403–12. doi: 10.1590/S0102-311X2001000600011
11. Dias JCP. Globalização, iniquidade e doença de Chagas. Cad Saúde Pública. (2007) 23:S13–22. doi: 10.1590/S0102-311X2007001300003
12. Briceño-León R. Chagas disease and globalization of the Amazon. Cad Saúde Pública. (2007) 23:S33–40. doi: 10.1590/S0102-311X2007001300005
13. Briceño-León R. La enfermedad de Chagas en las Américas: una perspectiva de ecosalud. Cad Saúde Pública. (2009) 25:S71–82. doi: 10.1590/S0102-311X2009001300007
14. Silva RA, Wanderley DMV, Forsyth F, Leite RM, Luna EJ, Carneiro N Jr., et al. Awareness of Chagas disease and socioeconomic characteristics of Bolivian immigrants living in Sao Paulo, Brazil. Rev Inst Med Trop São Paulo. (2020) 62:e39. doi: 10.1590/S1678-9946202062039
15. Forsyth C, Meymandi S, Moss I, Cone J, Cohen R, Batista C. Proposed multidimensional framework for understanding Chagas disease healthcare barriers in the United States. PloS Negl Trop Dis. (2019) 13:e0007447. doi: 10.1371/journal.pntd.0007447
16. De Maio F, Llovet I, Dinardi G. Chagas disease in non-endemic countries: “sick immigrant” phobia or a public health concern? Crit Public Health. (2014) 24:372–80. doi: 10.1080/09581596.2013.836589
17. Requena-Méndez A, Albajar-Viñas P, Angheben A, Chiodini P, Gascón J, Muñoz J. Health policies to control Chagas disease transmission in European countries. PloS Negl Trop Dis. (2014) 8:e3245. doi: 10.1371/journal.pntd.0003245
18. Getaz L, Da Silva-Santos L, Wolff H, Vitoria M, Serre-Delcor N, Lozano-Becerra JC, et al. Persistent infectious and tropical diseases in immigrant correctional populations. Rev Esp Sanid Penit. (2016) 18:57–66. doi: 10.4321/S1575-06202016000200004
19. Sargent C, Larchanché S. Transnational migration and global health: the production and management of risk, illness and access to care. Annu Rev Anthropol Palo Alto. (2011) 40:345–61. doi: 10.1146/annurev-anthro-081309-145811
20. Azogue E. Women and congenital Chagas’ Disease in Santa Cruz, Bolivia: epidemiological and sociocultural aspects. Soc Sci Med. (1993) 37:503–11. doi: 10.1016/0277-9536(93)90285-C
21. Forsyth CJ. Controlled but not cured: structural processes and explanatory models of Chagas disease in tropical Bolivia. Soc Sci Med. (2015) 145:7–16. doi: 10.1016/j.socscimed.2015.09.022
22. Martínez-Parra AG, Pinilla-Alfonso MY, Abadía-Barrero CE. Sociocultural dynamics that influence Chagas disease health care in Colombia. Soc Sci Med. (2018) 215:142–50. doi: 10.1016/j.socscimed.2018.09.012
23. Wimmer A, Schiller NG. Methodological nationalism and beyond: nation-state building, migration and the social sciences. Glob Netw. (2002) 2:301–34. doi: 10.1111/1471-0374.00043
24. Goldberg A. Abordaje antropológico comparativo en torno a la incidencia del Chagas y la tuberculosis en immigrantes Bolivianos residents en Barcelona y Buenos Aires, respectivamente. eä (2010). Available at: http://issuu.com/eajournal/docs/incidencia-chagas-tuberculosis-inmigrantes (Accessed 27 April 2018).
25. Auger S. Comentario sobre el criterio de visibilidad e invisibilidad en la enfermedad de Chagas-Mazza. Salud colectiva. (2012) 8:29–31. doi: 10.1590/S1851-82652012000300006
26. Sanmartino M, Saavedra AA, Prat JG, Barba MCP, Albajar-Viñas P. Que no tengan miedo de nosotros: el Chagas según los propios protagonistas. Interface (Botucatu). (2015) 19:1063–75. doi: 10.1590/1807-57622014.1170
28. Quaranta I. Costruzione e negoziazione sociale di una sindrome. Un’indagine antropologica sul contenzioso intorno alla Chronic fatigue syndrome (CFS) nel Regno Unito. AM Vol. 4. Rivista Della Società Italiana Di Antropologia Medica (1999) p. 7–8; 129-172. Available at: http://www.amantropologiamedica.unipg.it/index.php/am/article/view/65.
29. Poole D ed. Unruly order: Violence, Power, And Cultural Identity In The High Provinces Of Southern Peru. San Francisco: Westview Press (1994).
30. Luna EJA, Furucho CR, Silva RA, Wanderley DM, Carvalho NB, Satolo CG, et al. Prevalence of Trypanosoma cruzi infection among Bolivian immigrants in the city of São Paulo, Brazil. Mem Inst Oswaldo Cruz. (2017) 112:70–4. doi: 10.1590/0074-02760160384
31. Good BJ. Medicine, Rationality and Experience: An Anthropological Perspective. Cambridge: Cambridge University Press (1994).
32. Umezawa EF, Nascimento NS, Kesper NJR, Coura JR, Borges-Pereira J, Junqueira AC, et al. Immunoblot assay using excreted-secreted antigen of Trypanosoma cruzi in serodiagnosis of congenital, acute, and chronic Chagas disease. J Clin Microbiol. (1996) 34:2143–7. doi: 10.1590/S1413-81232008000900025
33. Ballester-Gil LM, Stotz EN, Hasslocher-Moreno AM, Azavedo BA, Araújo-Jorge TC. O saber do paciente chagásico sobre a sua doença: construção compartilhada de um instrumento para a pesquisa e teste de sua aplicabilidade. Ciênc saúde coletiva. (2008) 13:2199–214. doi: 10.1590/S1413-81232008000900025
34. Gomes R, Mendonça EA, Pontes ML. As representações sociais e a experiência da doença. Cad Saúde Pública. (2002) 18:1207–14. doi: 10.1590/S0102-311X2002000500013
35. Baeninger R. organizator. Imigração Boliviana no Brasil. Campinas: Núcleo de Estudos de População-Nepo/Unicamp, Fapesp, CNPq, Unfpa (2012).
36. Silveira C, Carneiro N Jr., Ribeiro MCSA, Barata RCB. Living conditions and access to health services by Bolivian immigrants in the city of São Paulo, Brazil. Cad Saúde Pública. (2013) 29:2017–27. doi: 10.1590/0102-311X00113212
37. Goldberg A, Silveira C. Desigualdad social, condiciones de acceso a la salud pública y procesos de atención en inmigrantes Bolivianos de Buenos Aires y São Paulo: una indagación comparativa. Saude Soc. (2013) 22:283–97. doi: 10.1590/S0104-12902013000200003
38. Carneiro N Jr., Silveira C, Silva LMB, Yasuda MAS. Migração Boliviana e doença de Chagas: limites na atuação do Sistema Único de Saúde brasileiro (SUS). Interface (Botucatu). (2018) 22:87–96. doi: 10.1590/1807-57622016.0338
39. Aith FMA, Forsyth C, Shikanai-Yasuda MA. Chagas disease and healthcare rights in the Bolivian immigrant community of São Paulo, Brazil. Trop Med Infect Dis. (2020) 5:62. doi: 10.3390/tropicalmed5020062
40. Villela MM, Pimenta DN, Lamounier PA, Dias JCP. Avaliação de conhecimentos e práticas que adultos e crianças têm acerca da doença de Chagas e seus vetores em região endêmica de Minas Gerais, Brasil. Cad Saúde Pública. (2009) 25:1701–10. doi: 10.1590/S0102-311X2009000800006
41. Magnani C, Dias JCP, Gontijo ED. Como as ações de saúde pensam o homem e como o homem as repensa: uma análise antropológica do controle da doença de Chagas. Cad Saúde Pública. (2009) 25:1947–56. doi: 10.1590/S0102-311X2009000900009
42. Ríos-Osorio LA, Crespo-González JJ, Zapata-Tamayo MA. Etnometodología para la comprensión y el manejo de la Enfermedad de Chagas en las poblaciones indígenas Wiwa asentadas en la vertiente suroriental de la Sierra Nevada de Santa Marta. Saude Soc. (2012) 21:446–57. doi: 10.1590/S0104-12902012000200017
43. Cucunubá ZM, Manne-Goehler JM, Díaz D, Nouvellet P, Bernal O, Marchiol A, et al. How universal is coverage and access to diagnosis and treatment for Chagas disease in Colombia? A health systems analysis. Soc Sci Med (1982). (2017) 175:187–98. doi: 10.1016/j.socscimed.2017.01.002
44. Linardelli MF, Anzorena C. Cuidar, gestionar, esperar. Estrategias de mujeres migrantes ante contextos restrictivos de acceso a la atención sanitaria. Jangwa Pana. (2021) 20:206–24. doi: 10.21676/16574923.4177
45. Magnani C, Oliveira BG, Gontijo ED. Representações, mitos e comportamentos do paciente submetido ao implante de marcapasso na doença de Chagas. Cad Saúde Pública. (2007) 23:1624–32. doi: 10.1590/S0102-311X2007000700013
46. Sanmartino M. “Tener Chagas” en contexto urbano: concepciones de varones residentes en la región de la Plata (Argentina). Rev Biomed. (2009) 20:216–27. doi: 10.32776/revbiomed.v20i3.138
47. Valdez-Tah A. Making sense of Chagas Disease among Mexican Immigrants in California. Med Anthropol. (2021) 40:511–24. doi: 10.1080/01459740.2021.1894560
48. Ventura-Garcia L, Muela-Ribera J, Martínez-Hernaez A. Chagas, risk and health seeking among Bolivian women in Catalonia. Med Anthropol. (2021) 40:541–56. doi: 10.1080/01459740.2020.1718125
49. Uchôa E, Firmo JOA, Dias EC, Pereira MSN, Gontijo ED. Signos, significados e ações associados à doença de Chagas. Cad Saúde Pública. (2002) 18:71–9. doi: 10.1590/S0102-311X2002000100008
50. Romay-Barja M, Iglesias-Rus L, Boquete T, Benito A, Blasco-Hernández T. Key Chagas disease missing knowledge among at-risk population in Spain affecting diagnosis and treatment. Infect Dis Poverty. (2021) 10:55. doi: 10.1186/s40249-021-00841-4
51. Castaldo M, Cavani A, Segneri M-C, Costanza G, Mirisola C, Marrone R. Anthropological study on Chagas Disease: Sociocultural construction of illness and embodiment of health barriers in Bolivian migrants in Rome, Italy. PloS One. (2020) 15:e0240831. doi: 10.1371/journal.pone.0240831
52. Forsyth CJ, Hernandez S, Flores CA, Roman MF, Nieto JM, Marquez G, et al. “It’s like a phantom disease”: patient perspectives on access to treatment for Chagas disease in the United States. Am J Trop Med Hyg. (2018) 98:735–41. doi: 10.4269/ajtmh.17-0691
53. Creswell JW, Creswell JD. Research design: qualitative, quantitative, and mixed methods approaches. Fifth edition. Los Angeles: SAGE (2018).
54. Ventura-Garcia L, Roura M, Pell C, Posada E, Gascón J, Aldasoro E, et al. Socio-cultural aspects of Chagas disease: a systematic review of qualitative research. PloS Negl Trop Dis. (2013) 7:e2410. doi: 10.1371/journal.pntd.0002410
55. Sanmartino M, Amieva C, Medone P. Representaciones sociales sobre la problemática de Chagas en un servicio de salud comunitaria del Gran La Plata, Buenos Aires, Argentina. Glob Health Promot. (2018) 25:102–10. doi: 10.1177/1757975916677189
56. Sanmartino M, Forsyth CJ, Avaria A, Velarde-Rodriguez M, Gómez i Prat J, Albajar-Viñas P. The multidimensional comprehension of Chagas disease. Contributions, approaches, challenges and opportunities from and beyond the Information, Education and Communication field. Mem Inst Oswaldo Cruz. (2021) 116:e200460. doi: 10.1590/0074-02760200460
Keywords: human migration, Bolivians, Chagas disease, social representations, neglected tropical diseases
Citation: Silveira C, Forsyth C, Junior NC, Goldberg A, da Silva LMB, da Silva RA and Shikanai-Yasuda MA (2024) Representations of Chagas disease among Bolivian immigrants in the city of São Paulo. Front. Trop. Dis 5:1331026. doi: 10.3389/fitd.2024.1331026
Received: 03 November 2023; Accepted: 26 March 2024;
Published: 22 April 2024.
Edited by:
Maya Semrau, Brighton and Sussex Medical School, United KingdomReviewed by:
Fernando Val, Fundação de Medicina Tropical Doutor Heitor Vieira Dourado (FMT-HVD), BrazilAlba Valdez Tah, National School of Higher Studies Unit Mérida, Mexico
Copyright © 2024 Silveira, Forsyth, Junior, Goldberg, da Silva, da Silva and Shikanai-Yasuda. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Cássio Silveira, Y2Fzc2lvc2lsdmVpcmFzY0BnbWFpbC5jb20=
†ORCID: Cássio Silveira, orcid.org/0000-0001-7165-1730
Colin Forsyth, orcid.org/0000-0003-1481-8367
Nivaldo Carneiro Junior, orcid.org/0000-0003-1358-9160
Alejandro Goldberg, orcid.org/0000-0002-0514-394
Lia Maria Britto da Silva, orcid.org/000-0002-8622-6574
Rubens Antonio da Silva, orcid.org/0000-0003-1636-0652
Maria Aparecida Shikanai-Yasuda, orcid.org/0000-0003-3864-041X