 Diogo Fernandes dos Santos1,2*
Diogo Fernandes dos Santos1,2* Pedro Henrique Sirotheau Corrêa Alves2Fernanda de Oliveira Cirino2
Pedro Henrique Sirotheau Corrêa Alves2Fernanda de Oliveira Cirino2 Leonardo Peixoto Garcia1
Leonardo Peixoto Garcia1 João Paulo Moreira Fernandes1Douglas Eulálio Antunes1
João Paulo Moreira Fernandes1Douglas Eulálio Antunes1 Isabela Maria Bernardes Goulart1,2
Isabela Maria Bernardes Goulart1,2- 1National Reference Center for Sanitary Dermatology and Leprosy, Clinics’ Hospital, School of Medicine, Federal University of Uberlândia (UFU), Uberlândia, MG, Brazil
- 2Postgraduate Program in Health Sciences, School of Medicine, Federal University of Uberlândia (UFU), Uberlândia, MG, Brazil
Background: Leprosy neuritis (LN) is an immune hyperactivity majorly responsible for the deformities and sequelae present in leprosy disease. This observational study aimed to evaluate the use of intravenous methylprednisolone in refractory LN cases in a national reference center of leprosy in Brazil.
Methods: Epidemiological and clinical data were collected, and the following instruments were used on evaluation: visual analog pain scale (VAS), Douler Neuropathic 4 questionnaire (DN4), Screening of Activity Limitation and Safety Awareness (SALSA), and the simplified neurological assessment protocol by the Brazilian Ministry of Health. The initial and final results of pulse therapy were compared.
Results: We included 18 patients. After pulse therapy, there was no difference regarding sensory and motor scores. At the beginning of the treatment, 66.7% (12/18) of patients were using oral prednisone at 35.0 mg (± 12.43). After treatment, 38.9% (7/18) of them maintained oral prednisone at a lower dose (16.4mg ±6.3; p=0.002). Salsa score improved after treatment (p=0.020) and DN4 scores dropped from 6.7 (± 1.7) to 5.2 (± 2.1) (p<0.0001).
Conclusion: Pulse therapy with endovenous methylprednisolone in LN was effective in decreasing pain intensity, preventing worsening of sensory-motor function, and reducing the dose of corticosteroids, reflecting the patient’s improvement of functionality.
Introduction
Leprosy, a chronic infectious disease caused by Mycobacterium leprae (M. leprae), can also be considered an immunological disease, as the host’s immune response to the bacteria largely determines the severity and potential for disability (1, 2). Between 30% and 50% of leprosy patients experience immune hyperactivity, known as leprosy reactions (LR), which can occur before, during, or after multidrug therapy (MDT). These acute episodes are classified into two types: type 1 leprosy reaction (T1LR) and type 2 leprosy reaction (T2LR) (3–5).
T1LR, also known as reverse reaction, primarily affects borderline patients and is characterized by an abrupt increase in cell-mediated immunity against M. leprae. This delayed-type hypersensitivity reaction is associated with a decrease in bacterial load and involves a Th1 cytokine response. Clinically, it presents as an acute exacerbation of existing skin lesions or the appearance of new lesions, often accompanied by peripheral nerve involvement (2–8).
T2LR, or erythema nodosum leprosum (ENL), is a systemic inflammatory process mediated by a Th2 response and related to immune complex deposition. It typically affects borderline and lepromatous patients and is characterized by erythematous, painful subcutaneous nodules, fever, and systemic manifestations such as orchiepididymitis, glomerulonephritis, myositis, arthralgia, iridocyclitis, hepatomegaly, and adenomegaly (2–8).
Leprosy neuritis (LN) is an inflammatory process affecting peripheral nerves and can occur in both T1LR and T2LR. It is defined by the acute onset of new sensory or motor deficits, often accompanied by nerve thickening and neuropathic pain. LN is a major contributor to the deformities and sequelae associated with leprosy, making it a potentially disabling condition (2–9).
The standard treatment for LN involves glucocorticoids, typically prednisone, at 1–1.5 mg/kg/day, with a gradual dose reduction over 12 weeks. However, many patients experience an inadequate response or recurrent episodes of LN, leading to chronic glucocorticoid use and its associated complications, including depression, cataracts, glaucoma, hypertension, edema, congestive heart failure, myocardial infarction, esophagitis, gastritis, peptic ulcer disease, osteoporosis, myopathy, avascular necrosis, diabetes, dyslipidemia, striae, acne, hirsutism, electrolyte disturbances, and Cushing’s syndrome (9).
Therefore, as in other inflammatory neuropathies, intravenous corticosteroids should be considered for severe or refractory LN. While intravenous methylprednisolone has been used to treat LN, its efficacy needs to be systematically evaluated (10–12). This study aimed to evaluate the use of intravenous methylprednisolone in patients with refractory LN at a national leprosy referral center in Brazil.
Materials and methods
Ethics statement
This study has been approved by the Human Research Ethics Committee of the Federal University of Uberlândia (CAAE: 69626123.4.0000.5152). All participants provided written informed consent for a retrospective study.
Patients
This is a retrospective cohort study that evaluated 18 individuals with refractory LN who underwent intravenous methylprednisolone. We considered refractory LN the cases of neuritis that did not respond to standardized clinical treatment within 4 weeks, the typical duration of initial oral corticosteroid therapy, with worsening dermatoneurological evaluation, and the cases of reentrant neuritis (when a new clinical impairment occurs in the attempt to withdraw or reduce the dose of corticosteroids). All patients received oral prednisone at a dose of 1 mg/kg/day for at least 4 weeks during the initial treatment of the reactions, but without effective response. At the time of inclusion in the study, all patients were in the oral prednisone dose reduction phase.
All individuals were over 18 years old and were followed periodically during treatment. Patients who presented LN after the end of MDT were carefully evaluated to rule out criteria for relapse, therapeutic failure, and drug resistance. At the end of MDT treatment, all patients underwent serological evaluation with monitoring of the ELISA index, histopathological evaluation of skin lesions with comparison of the bacilloscopic incidence of the lesions, and molecular evaluation by real-time PCR. All of these laboratory tools are complementary methods for the diagnosis of leprosy.
Intravenous corticosteroids did not interfere with the specific infection treatment. However, we maintained extreme vigilance regarding laboratory monitoring, aiming for early detection of any abnormality that could indicate bacillary proliferation.
Patients with the following criteria were excluded:
- Confirmed metabolic conditions (diabetes mellitus and uremia),
- Malnutrition and vitamin deficiencies (B12 vitamin or folic acid),
- Chronic alcoholism,
- Autoimmune disorders (systemic lupus erythematosus, rheumatoid arthritis, Sjogren’s disease),
- Other infectious diseases (HIV, hepatitis, and Lyme’s disease),
- Inflammatory diseases,
- Pregnancy.
Protocol
All patients received strongyloidiasis prophylaxis with ivermectin before starting the methylprednisolone protocol, following Brazilian Ministry of Health recommendations.
The use of methylprednisolone was carried out in two phases:
Attack: Use of 1 gram of intravenous methylprednisolone per day for five days.
Maintenance: Use 1 gram of intravenous methylprednisolone daily for three days, once a month, for six months.
This pulse therapy regime was chosen based on its reported efficacy in other inflammatory neuropathies and in previous studies regarding leprosy (11).
Epidemiological, clinical, and neurological assessment
Epidemiological, clinical, and neurological data were collected from patient medical records. All patients underwent standardized sensory and motor neurological evaluations before and after the methylprednisolone protocol, following the Brazilian Ministry of Health guidelines (9).
Sensory function was assessed using a Semmes-Weinstein monofilament set (0.07g, 0.2g, 2g, 4g, 10g, and 300g). The test began with the lightest filament, applied to specific nerve territories. If the patient perceived the stimulus, a score of 5 was assigned for that area. If not, progressively heavier filaments were used until a response was elicited, with scores assigned according to the filament weight that was finally perceived. If no perception was recorded with the 300g filament, a score of 0 was assigned. Seven areas were evaluated in the upper limbs (three each for the ulnar and median nerves, and one for the radial nerve) and ten areas in the lower limbs (nine for the tibial nerve and one for the peroneal nerve). The total possible score was 35 for each upper limb and 50 for each lower limb (9, 13). Figure 1 illustrates the sensory assessment method.
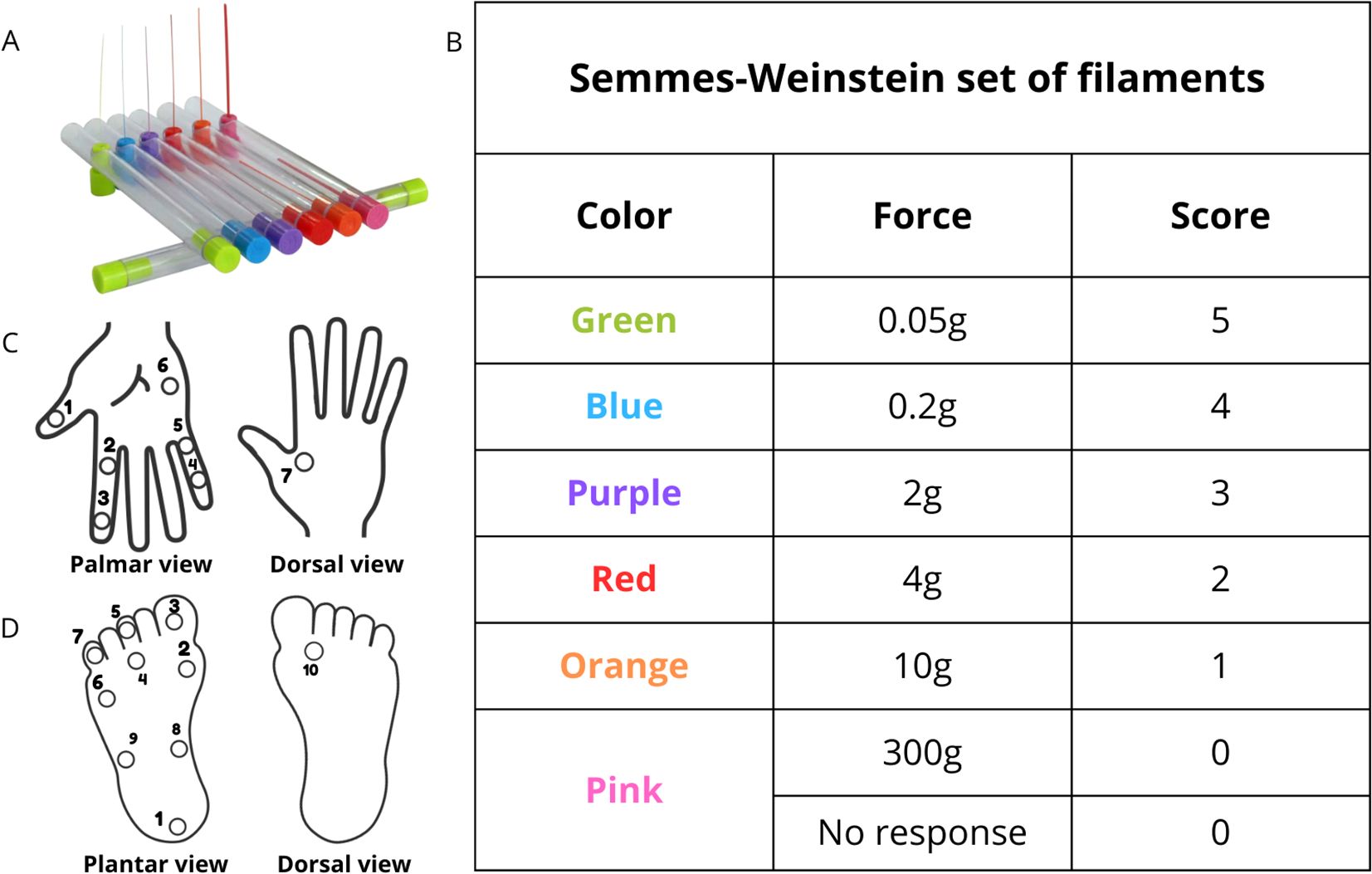
Figure 1. Sensory and motor assessment. (A) Semmes-Weinstein set of filaments used to evaluate sensory function. (B) Each monofilament has a specific force: green 0.05g, blue 0.2g, purple 2g, red 4g, orange 10g and pink 300g, and a correspondent score. (C) In the upper limbs, there are six points of interest for the evaluation in the palmar face and one in the dorsal view of the hand according to the sensory territory of median (1-3), ulnar (4-6) and radial (7) nerves. (D) In the lower limbs, there are nine points in plantar face and one in the dorsal face of the foot according to the sensory territory of tibial (1-9) and common fibular (10) nerves.
Motor strength was assessed using the Medical Research Council (MRC) scale (0-5) for specific muscles innervated by the ulnar, median, radial, and fibular nerves. In the upper limbs, the first dorsal interosseous, abductor digiti minimi, third and fourth lumbricals (ulnar nerve); abductor pollicis brevis, first and second lumbricals (median nerve); and extensor digitorum communis and extensor carpi brevis (radial nerve) were evaluated. In the lower limbs, the tibialis anterior, extensor digitorum longus, and extensor hallucis longus (fibular nerve) were assessed (9). Scores that ranged from 0 to 5 were assigned on each evaluated muscle as the MRC scale, with a maximum score of 10 for median nerve (two assessed muscles), 15 for ulnar nerve (three assessed muscles), 10 for radial nerve (two muscles evaluated) and 15 for common fibular nerve (three assessed muscles). The total possible motor score was 35 for each upper limb and 15 for each lower limb (13). Figure 2 illustrates the motor assessment method.
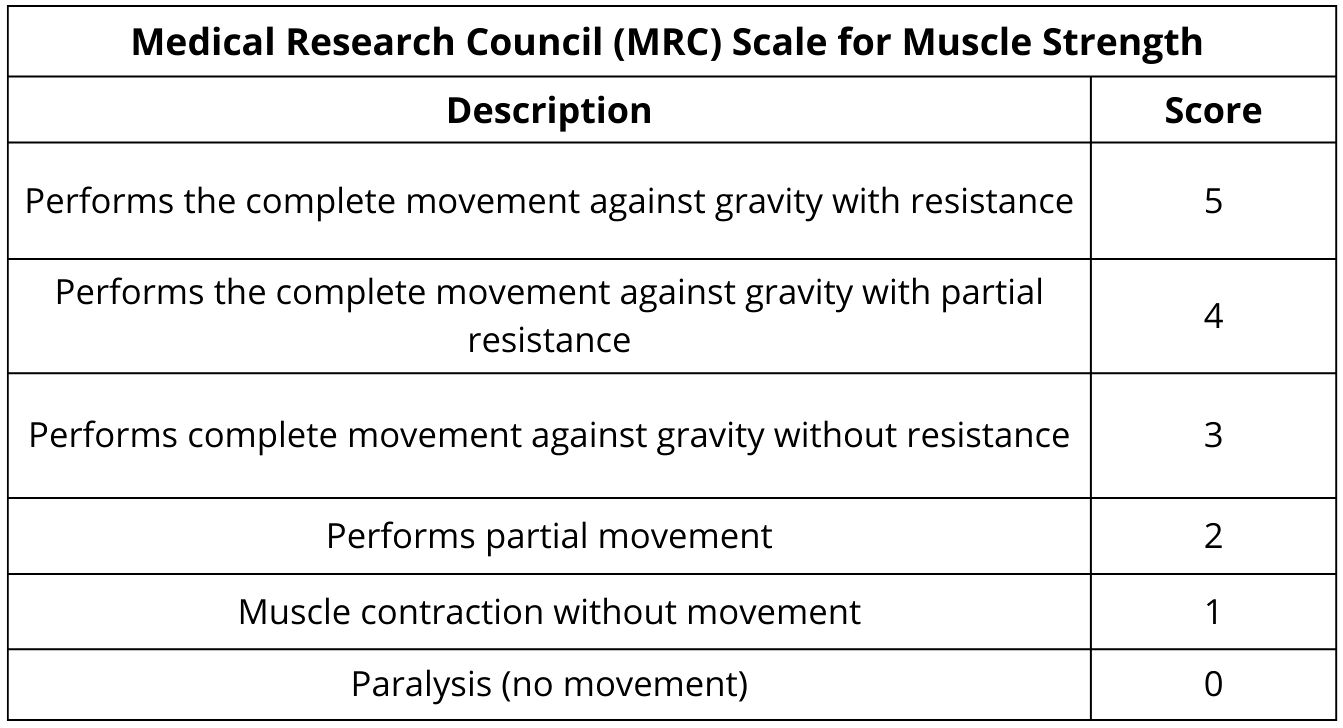
Figure 2. Medical Research Council (MRC) scale for muscle strength used to evaluate upper and lower limbs.
Assessment of pain, degree of physical disability, and functional capacity
Pain intensity was assessed using the Visual Analog Scale (VAS) before and after treatment. Neuropathic pain was assessed using the Douleur Neuropathique en 4 Questions (DN4) questionnaire (14). Functional capacity was assessed using the Screening of Activity Limitation and Safety Awareness (SALSA) questionnaire (15).
The level of functional disability evaluates the neural function integrity and degree of physical disability through voluntary muscle testing and sensory evaluation of the hands and feet. Patients with no neural impairment are classified as disability grade zero (DG0) and disability grade 1 (DG1), which occurs when only sensorial impairment exists. Regarding the degree of disability 2 (DG2), there are visible deficiencies, such as claws (claw of digits), bone resorption, muscle atrophy, contractures, and wounds (9).
Laboratory evaluation
Serum anti-PGL-I IgM levels were measured using ELISA at the beginning and end of the methylprednisolone protocol to monitor bacterial load (16, 17). Results were expressed as an ELISA index, with values above 1.0 considered positive.
Electroneuromyography
Electroneuromyography (ENMG) was performed at baseline to assess the number of affected nerves and the pattern of neural impairment (mononeuropathy or multiple mononeuropathy). In the sensory conduction study, the median, ulnar, radial, sural, and fibular superficial were examined bilaterally. In the motor conduction study, the median, ulnar, common fibular, and tibial bilaterally nerves were examined, supplemented by techniques for focal impairment identification at compression sites often affected in leprosy neuropathy, such as the median nerve at the wrist, ulnar nerve at the elbow, fibular nerve at the fibular head and tibial nerve at the ankle.
Statistical analysis
Continuous data were assessed for normality using the Shapiro-Wilk test. The Wilcoxon Signed-Rank test was used to compare pre- and post-treatment sensory and motor scores. Proportions for laboratory data were compared using the Binomial test. All analyses were performed using SPSS version 22, with a significance level of p < 0.05.
Results
Demographic and clinical characteristics
The sample comprised 18 patients, with a male predominance (88.9%; 16/18). The patients’ median age was 45.8 years (± 16.6). T1LR predominated with 66.7% (12/18), while 33.3% (6/18) were T2LR. Regarding the clinical forms of leprosy, the lepromatous and borderline-borderline forms were predominant. Regarding the operational classification for treatment purposes, all patients were classified as multibacillary (MB). The majority (66.7%, 12/18) presented the LR after the end of treatment. All clinical and epidemiological variables are shown in Table 1.
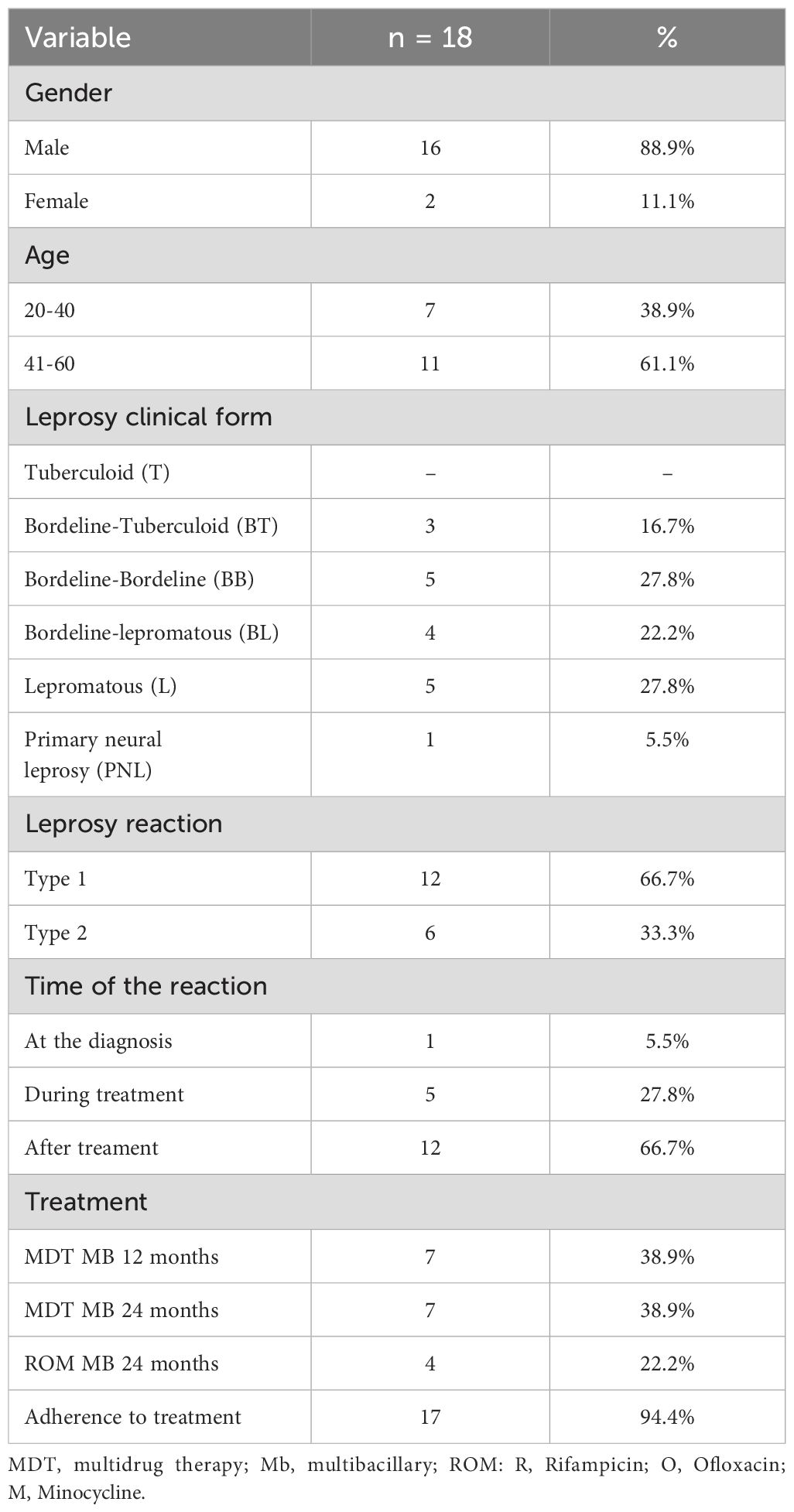
Table 1. Demographic and clinical characteristics of patients with refractory leprosy neuritis.
Neurological outcomes
All patients presented a clinical picture compatible with asymmetric multiple mononeuropathy, with clinical evidence of a new deficit and the presence of neural thickening in 88,3% (15/18) of the cases. Electroneuromyography (ENMG) confirmed the clinical diagnosis of asymmetric multiple mononeuropathy in all patients, with an average of 8.2 ± 3.5 sensory nerves and 3.5 ± 2.4 motor nerves affected per patient.
In the clinical assessment of the upper limbs, sensory function was worse on the ulnar territory, with 83,3% (15/18) of patients presenting sensory loss in at least one limb before treatment. In the lower limbs, 94,4% (17/18) of patients presented sensory impairment on tibial territory in at least one limb. After treatment with intravenous methylprednisolone, there was no difference between the sensory scores in all nerves evaluated, confirming the maintenance of the previously observed sensory deficit (Table 2).
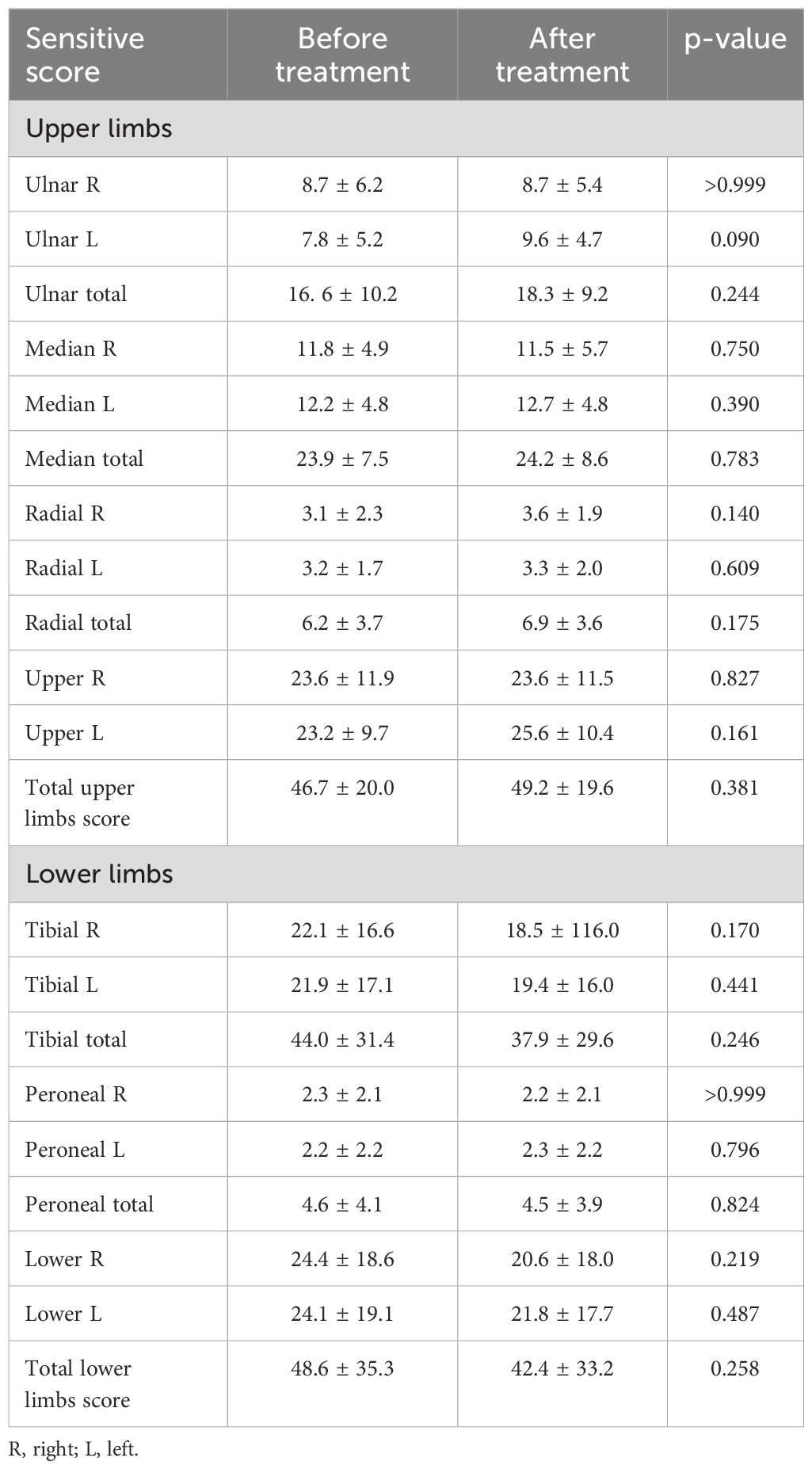
Table 2. Sensory outcomes before and after methylprednisolone treatment.
Regarding motor impairment, the ulnar nerve was also the most common in the upper limbs, with 83,3% (15/18) patients presenting impairment in at least one limb. In lower limbs, 55,5% (10/18) of patients presented motor impairment on the fibular nerve. After treatment with intravenous methylprednisolone, there was no difference between the motor scores in all evaluated nerves, confirming the maintenance of the previously observed motor deficits (Table 3).
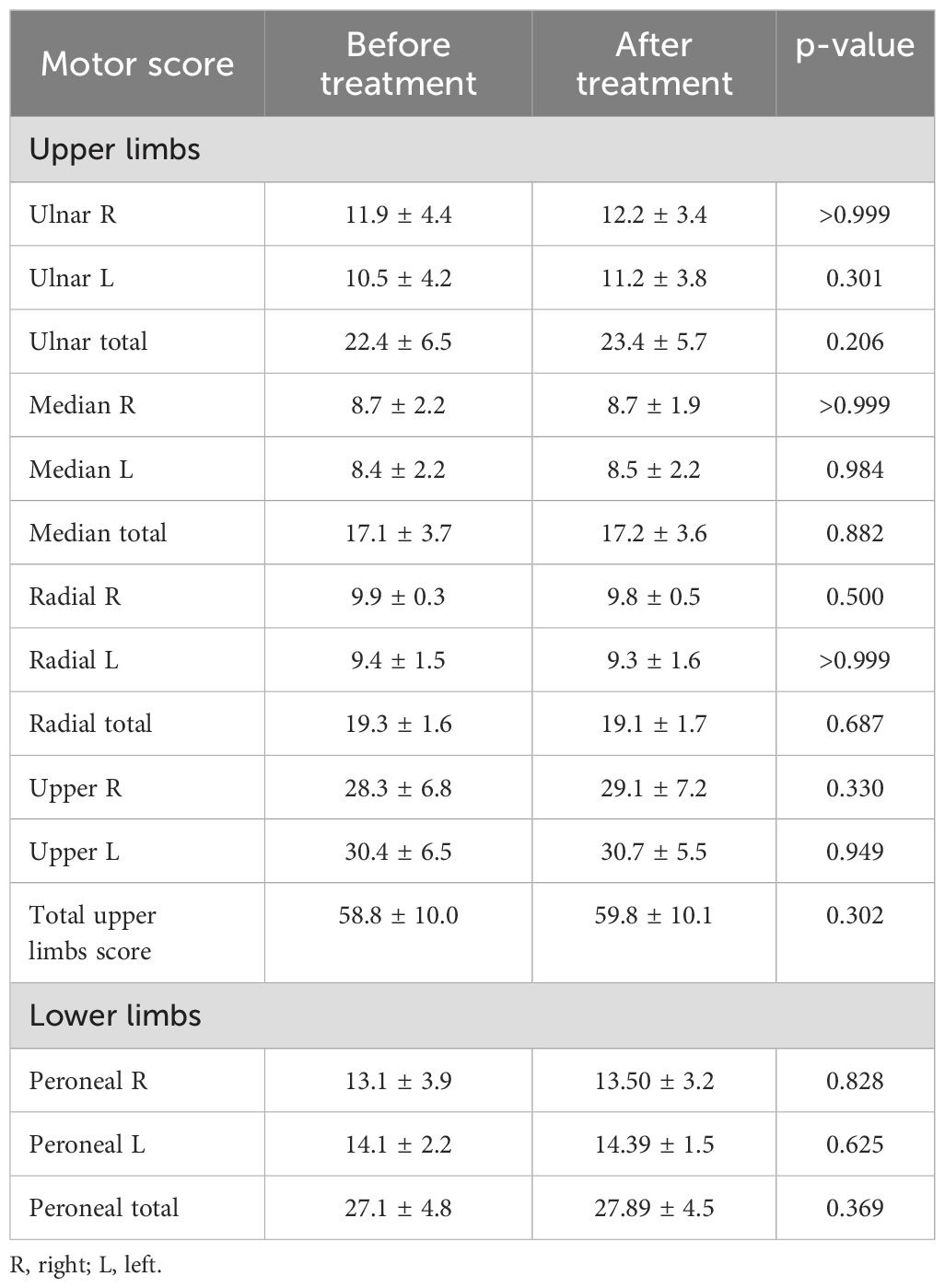
Table 3. Motor outcomes before and after methylprednisolone treatment.
Electroneuromyographic findings indicate a significant number of affected nerves in all patients, corroborating the presence of permanent sequelae and less chance of recovery in our sample, composed by severe and refractory cases. Thus, the stability of sensory-motor function can be viewed as a favorable result since many patients worsen their neurological deficit late in leprosy (18–20). Electroneuromyographic evaluation was also important for recognizing motor impairment and, consequently, the greater severity of reaction episodes, corroborating the need for more effective approaches.
Some electroneuromyographic abnormalities, such as the presence of conduction block and temporal dispersion, accompanied by phlogistic signs on palpation of the peripheral nerve, may suggest the presence of a pseudoabscess (18). However, it should be confirmed by some imaging method, such as peripheral nerve ultrasonography.
Laboratory findings
Anti-PGLI IgM ELISA serology was positive in 13/18 (72.2%) patients at baseline, with a mean index of 1.9 ± 2.2. At the end of the methylprednisolone treatment, 10/18 (55.6%) patients were positive (p = 0.3921), with a mean index of 1.2 ± 0.8 (p = 0.2465). There was no statistically significant change in anti-PGLI IgM levels.
Although this drop in the ELISA index was not significant, it is important to reinforce that there was no increase in this index, which could suggest a relapse or therapeutic failure. This result confirms that there was no bacillary proliferation during pulse therapy.
Pain and functional assessment outcomes
The mean SALSA score improved significantly from 55.8 ± 17.9 at baseline to 47.7 ± 16.2 at the end of treatment (p = 0.020).
All patients had neuropathic pain at baseline, as assessed by the DN4 questionnaire. At the end of treatment, 13/18 (72.2%) patients still had neuropathic pain (p = 0.016). The mean DN4 score decreased significantly from 6.7 ± 1.7 to 5.2 ± 2.1 (p < 0.0001).
The mean VAS pain score decreased significantly from 7.8 ± 3.1 at baseline to 4.3 ± 2.7 at the end of treatment (p = 0.0019).
These findings show an improvement in the functionality of the participants. However, a significant proportion of patients presented neuropathic pain during the follow-up period, reinforcing the need to optimize pain treatment in these patients, also differentiating the presence of chronic pain and new LR episodes (21, 22).
Disability grade
At baseline, 10/18 (55.6%) patients were classified as DG2 and 8/18 (44.4%) as DG1. At the end of treatment, 12/18 (66.7%) patients were DG2. Although not significant (p = 0.494), this result demonstrates the worsening of disability in 2 patients (11.1% of cases). One of these patients presented the BB clinical form and the other BL and both were treated with the MDT-MB regimen.
Prednisone dosage
At baseline, 12/18 (66.7%) patients received oral prednisone for over three months, with a mean dose of 35.0 ± 12.43 mg. After methylprednisolone treatment, the mean oral prednisone dose was significantly reduced to 16.4 ± 6.3 mg (p = 0.002), with 7/18 (38.9%) patients continuing oral prednisone.
This drop in corticosteroid dosage, considerably due to the clinical response, also contributes to a better quality of life in these patients, considering the numerous adverse effects of the chronic use of corticosteroids. The recommended dose is 1 mg/kg/day, and all patients received this dose at the initial stage of treatment for the leprosy reaction. Pulse therapy was indicated during prednisone withdrawal, a time when many patients recur or present new symptoms. Therefore, the dose at the time pulse therapy was initiated was lower. If pulse therapy had not been instituted, all these patients would have used a higher oral corticosteroid dose.
Discussion
Our data show an improvement in quality of life, based on the reduction in corticosteroid dosage, pain intensity, neuropathic pain and SALSA score (Figure 3). The presence of deformities and neural sequelae already at the beginning of intravenous treatment reinforces not only the late indication for this conduct but also the difficulty of referring these patients to centers that perform it.
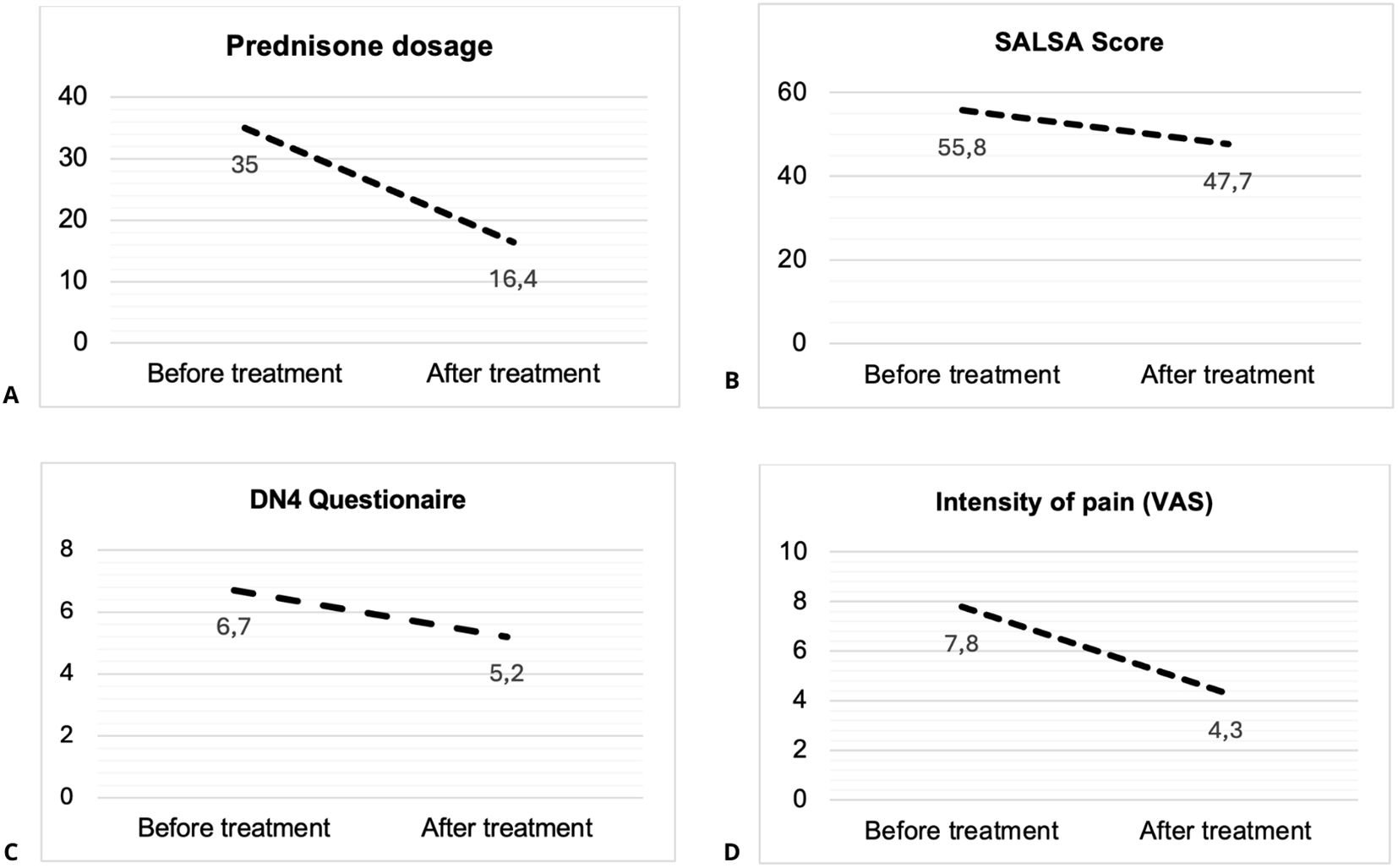
Figure 3. Changes in (A) Prednisone Dosage, (B) SALSA Score, (C) DN4 Score, and (D) VAS Score, Before and After Methylprednisolone Treatment. SALSA, Screening of Activity Limitation and Safety Awareness; DN4, Douler Neuropathic 4 questionnaire; VAS, Visual analog scale.
One of the limitations of the study is that pulse therapy is still indicated only for severe cases of leprosy reaction, and it consists in a small sample of patients with a retrospective design. The main merit of this study is to raise the discussion about the possibilities that can be used in the most effective treatment with fewer adverse effects in leprosy neuritis.
Ideally, all severe cases should be routinely followed up with an electroneuromyographic and/or ultrasound evaluation, and this is another limitation of our study. However, we recognize that this approach is not available in endemic countries. Therefore, our study reinforces that detailed clinical evaluation is sufficient to identify more severe cases, which may benefit from pulse therapy.
A significant proportion of leprosy patients presented irreversible neural damage during sickness, which occurs mainly during the reactional episodes (18, 19). In our study, all of the patients who underwent the use of intravenous methylprednisolone presented a lack of response to oral treatment of reaction episodes, often accompanied by a high incidence of adverse effects related to chronic use of corticosteroids.
It is important to emphasize that in some cases, even after intravenous methylprednisolone, the patient can still present new reaction episodes, reinforcing the need for strict clinical monitoring. Furthermore, a considerable proportion of the patients included in this study underwent the procedure many months after the end of MDT.
Few studies have systematically described the use of intravenous methylprednisolone in LN, also confirming the absence of a significant clinical improvement regarding sensory-motor function. However, the severity of the symptoms and the late indication justify these data, reinforcing the need to review the protocols that guide conduct in this severe and disabling condition (11, 12).
Lugão et al. describe a dosage similar to that proposed in this study and demonstrate effectiveness in reducing the dose of oral prednisone. However, there was no objective evaluation regarding the control of neuropathic pain and improvement in quality of life. In addition, there was no proposal for monitoring relapse and treatment failure, which may be related to a higher prevalence of leprosy reactions (11). Walker et al. conducted a study using methylprednisolone just for three days at the start of a 16-week corticosteroid treatment regime of prednisolone in patients with T1LR. They did not demonstrate a significant difference in improvement in individuals in the methylprednisolone group. This result was probably due to the limited use of the medication, which did not promote a lower incidence of adverse events, since most patients continued to need to continue taking oral prednisone during the study (12).
Although few studies have proposed using other immunosuppressive medications, such as azathioprine, cyclosporine, and methotrexate, in the treatment of LR (23–27), the lack of systematized studies reinforces the negligence in proposing new strategies in the treatment of leprosy, favoring an improved quality of life in individuals who, in addition to deformities and social stigma, are susceptible to the adverse effects of prolonged treatment of the disease itself. Thus, future studies should consider the use of immunosuppression to spare the use of oral corticosteroids in leprosy neuritis, as is already done in other inflammatory neuropathies.
The use of corticosteroid-sparing immunosuppressants should be encouraged in treating LR, using effective doses and for a prolonged period, considering the chronicity and recurrence of this condition. There is no absolute contraindication to the use of these medications. However, it is essential to emphasize that leprosy is a complex disease and that antimicrobial treatment is prolonged. Therefore, patients should undergo careful laboratory and clinical evaluation, preventing relapse and/or treatment failure, as well as clinical complications such as anemia, leukopenia, and opportunistic infections.
Finally, based on the data found in this study, we propose an earlier indication for intravenous methylprednisolone, aiming at an early reduction in oral corticosteroid therapy and mitigating systemic adverse effects related to the chronic use of corticosteroids. Furthermore, it is essential to reinforce the need for adequate control of neuropathic pain and, as it is a chronic infection, one of the necessary precautions in the immunosuppression of these patients is adequate control of the bacillary load and vigilance in the early recognition of cases of therapeutic failure and relapse (Figure 4).
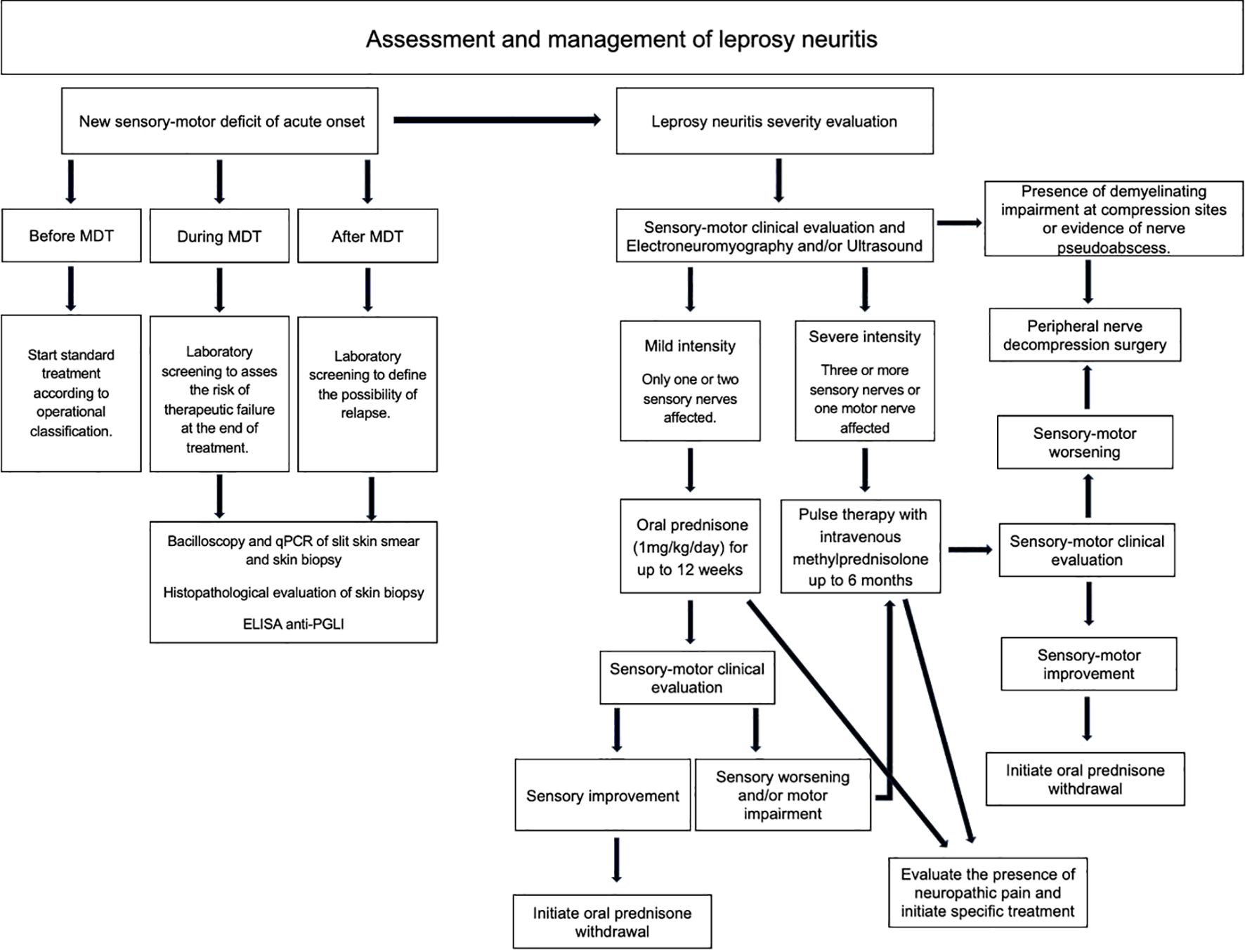
Figure 4. Algorithm proposed for the treatment of leprosy neuritis using pulse therapy with intravenous methylprednisolone. MDT, multidrug therapy; qPCR, quantitative polymerase chain reaction; ELISA, enzyme-linked immunoassay; Anti-PGLI, anti- phenolic glycolipid 1.
Data availability statement
The original contributions presented in the study are included in the article/supplementary material. Further inquiries can be directed to the corresponding author.
Ethics statement
The studies involving humans were approved by Human Research Ethics Committee of the Federal University of Uberlândia. The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study. Written informed consent was obtained from the individual(s) for the publication of any potentially identifiable images or data included in this article.
Author contributions
DS: Writing – original draft, Writing – review & editing. PC: Writing – original draft, Writing – review & editing. FC: Writing – original draft, Writing – review & editing. LG: Writing – original draft, Writing – review & editing. JF: Writing – original draft, Writing – review & editing. DA: Writing – original draft, Writing – review & editing. IG: Writing – original draft, Writing – review & editing.
Funding
The author(s) declare that financial support was received for the research and/or publication of this article. This work was supported by the Brazilian National Council for Scientific and Technological Development (CNPq) through The Cientific Iniciation Program (PIC) from the Brazilian Company of Hospital Services (EBSERH) at the Clinical Hospital of the Federal University of Uberlandia/EBSERH under grant number CNPq 116623/2023-3.
Acknowledgments
The authors thanks all the staff of the National Reference Centre in Leprosy of the Federal University of Uberlandia (CREDESH) for fundamental support to this research and for the care provided to the leprosy patients. We are also thankful to all the individuals that agreed to participate in this study.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Generative AI statement
The author(s) declare that no Generative AI was used in the creation of this manuscript.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Ebenezer GJ, Scollard DM. Treatment and evaluation advances in leprosy neuropathy. Neurotherapeutics. (2021) 18:2337–50. doi: 10.1007/s13311-021-01153-z
2. Dewi DAR, Djatmiko CBP, Rachmawati I, Arkania N, Wiliantari NM, Nadhira F. Immunopathogenesis of type 1 and type 2 leprosy reaction: an update review. Cureus. (2023) 15:e49155. doi: 10.7759/cureus.49155
3. White C, Franco-Paredes C. Leprosy in the 21st century. Clin Microbiol Rev. (2015) 28:80–94. doi: 10.1128/CMR.00079-13
4. Froes LARJ, Sotto MN, Trindade MAB. Leprosy: clinical and immunopathological characteristics. Bras Dermatol. (2022) 97:338–47. doi: 10.1016/j.abd.2021.08.006
5. Antunes DE, Santos DF, Lima MIS, Caixeta LP, Correa MBC, Moraes ECDS, et al. Clinical, epidemiological, and laboratory prognostic factors in patients with leprosy reactions: A 10-year retrospective cohort study. Front Med. (2022) 9:841030. doi: 10.3389/fmed.2022.841030
6. Maymone MBC, Venkatesh S, Laughter M, Abdat R, Hugh J, Dacso MM, et al. Leprosy: Treatment and management of complications. J Am Acad Dermatol. (2020) 83:17–30. doi: 10.1016/j.jaad.2019.10.138
7. Sugawara-Mikami M, Tanigawa K, Kawashima A, Kiriya M, Nakamura Y, Fujiwara Y, et al. Pathogenicity and virulence of Mycobacterium leprae. Virulence. (2022) 13:1985–2011. doi: 10.1080/21505594.2022.2141987
8. Goulart LR, Goulart IM. Leprosy pathogenetic background: a review and lessons from other mycobacterial diseases. Arch Dermatol Res. (2009) 301:123–37. doi: 10.1007/s00403-008-0917-3
9. Brasil, Ministério da Saúde, Secretaria de Vigilância em Saúde, Departamento de Vigilâncias das Doenças Transmissíveis. Diretrizes para vigilância, atenção e eliminação da Hanseníase como problema de saúde pública: manual técnico-operacional. Brasília (DF: Ministério da Saúde (2016). p. 58.
10. Rao PS, Sugamaran DS, Richard J, Smith WC. Multi-centre, double blind, randomized trial of three steroid regimens in the treatment of type-1 reactions in leprosy. Lepr Rev. (2006) 77:25–33. doi: 10.47276/lr.77.1.25
11. Lugão HB, Savarese LG, Silva SRML, Nogueira-Barbosa MH, Foss NT, Frade MAC. Methylprednisolone pulse therapy for leprosy neuritis: A retrospective study with sensory testing and peripheral nerve ultrasonography correlation. Indian J Dermatol Venereol Leprol. (2021) 88:114–16. doi: 10.25259/IJDVL_1280_20
12. Walker SL, Nicholls PG, Dhakal S, Hawksworth RA, Macdonald M, Mahat K, et al. A phase two randomised controlled double blind trial of high dose intravenous methylprednisolone and oral prednisolone versus intravenous normal saline and oral prednisolone in individuals with leprosy type 1 reactions and/or nerve function impairment. PloS Negl Trop Dis. (2011) 5:e1041. doi: 10.1371/journal.pntd.0001041
13. Tiago LMP, Barbosa MFF, Santos DFD, Faria AD, Gonçalves MA, Costa AV, et al. Late follow-up of peripheral neural decompression in leprosy: functional and clinical outcomes. Arq Neuropsiquiatr. (2021) 79:716–23. doi: 10.1590/0004-282X-ANP-2020-0032
14. Santos JG, Brito JO, de Andrade DC, Kaziyama VM, Ferreira KA, Souza I, et al. Translation to portuguese and validation of the Douleur Neuropathique 4 questionnaire. J Pain. (2010) 11:484–90. doi: 10.1016/j.jpain.2009.09.014
15. Salsa Collaborative Study Group. The development of a short questionnaire for screening of activity limitation and safety awareness (SALSA) in clients affected by leprosy or diabetes. Disabil Rehabil. (2007) 29:689–700. doi: 10.1080/09638280600926587
16. Lobato J, Costa MP, Reis Ede M, Gonçalves MA. Comparison of three immunological tests for leprosy diagnosis and detection of subclinical infection. Lepr Rev. (2011) 82:389–401. doi: 10.47276/lr.82.4.389
17. dos Santos DF, Mendonça MR, Antunes DE, Sabino EFP, Pereira RC, Goulart LR, et al. Molecular, immunological and neurophysiological evaluations for early diagnosis of neural impairment in seropositive leprosy household contacts. PloS Negl Trop Dis. (2018) 12:e0006494. doi: 10.1371/journal.pntd.0006494
18. Dos Santos DF, Borges IS, Garcia LP, Antunes DE, Luppi AM, Goulart IMB. Description of electroneuromiographic and laboratorial findings in leprosy neuropathy, according to its clinical forms: the confirmation of a spectral disease. Front Med. (2024) 10:1304131. doi: 10.3389/fmed.2023.1304131
19. Tomaselli PJ, Dos Santos DF, Dos Santos ACJ, Antunes DE, Marques VD, Foss NT, et al. Primary neural leprosy: clinical, neurophysiological and pathological presentation and progression. Brain. (2022) 145:1499–506. doi: 10.1093/brain/awab396
20. Santos DFD, Mendonça MR, Antunes DE, Sabino EFP, Pereira RC, Goulart LR, et al. Revisiting primary neural leprosy: clinical, serological, molecular, and neurophysiological aspects. PloS Negl Trop Dis. (2017) 11:e0006086. doi: 10.1371/journal.pntd.0006086
21. Santos VS, Santana JC, Castro FD, Oliveira LS, Santana JC, Feitosa VL, et al. Pain and quality of life in leprosy patients in an endemic area of Northeast Brazil: a cross-sectional study. Infect Dis Poverty. (2016) 5:18. doi: 10.1186/s40249-016-0113-1
22. Pitta IJR, Hacker MA, Vital RT, Andrade LR, Spitz CN, Sales AM, et al. Leprosy reactions and neuropathic pain in pure neural leprosy in a reference center in Rio de Janeiro - Brazil. Front Med. (2022) 9:865485. doi: 10.3389/fmed.2022.865485
23. Marlowe SN, Hawksworth RA, Butlin CR, Nicholls PG, Lockwood DN. Clinical outcomes in a randomized controlled study com-paring azathioprine and prednisolone versus prednisolone alone in the treatment of severe leprosy type 1 reactions in Nepal. Trans R Soc Trop Med Hyg. (2004) 98:602–9. doi: 10.1016/j.trstmh.2003.12.013
24. Lockwood DN, Darlong J, Govindharaj P, Kurian R, Sundarrao P, John AS. AZALEP a randomized controlled trial of azathioprine to treat leprosy nerve damage and Type 1 reactions in India: main findings. PloS Negl Trop Dis. (2017) 11:e0005348. doi: 10.1371/journal.pntd.0005348
25. Durães SM, Salles SdeA, Leite VR, Gazzeta MO. Azathioprine as a steroid sparing agent in leprosy type 2 reactions: report of nine cases. Lepr Rev. (2011) 82:304–9. doi: 10.47276/lr.82.3.304
26. Perez-Molina JA, Arce-Garcia O, Chamorro-Tojeiro S, Norman F, Monge-Maillo B, Comeche B, et al. Use of methotrexate for leprosy reactions. Experience of a referral center and systematic review of the literature. Travel Med Infect Dis. (2020) 37:101670. doi: 10.1016/j.tmaid.2020.101670
Keywords: leprosy, peripheral neuropathy, leprosy reaction, leprosy neuritis, methylprednisolone, neuropathic pain
Citation: Santos DF, Alves PHSC, Cirino FO, Garcia LP, Fernandes JPM, Antunes DE and Goulart IMB (2025) Evaluation of pulse therapy with intravenous methylprednisolone on leprosy neuritis in a Brazilian referral center. Front. Trop. Dis. 6:1560079. doi: 10.3389/fitd.2025.1560079
Received: 13 January 2025; Accepted: 24 March 2025;
Published: 14 April 2025.
Edited by:
Angélica Gobbo, Federal University of Pará, BrazilReviewed by:
Leticia Gomes De Pontes, Departamento de Bioquímica e Imunologia da Universidade de Minas Gerais, BrazilGlauber Voltan, Instituto Humanizare, Brazil
Copyright © 2025 Santos, Alves, Cirino, Garcia, Fernandes, Antunes and Goulart. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Diogo Fernandes dos Santos, ZGlvZ29mc2FuQGdtYWlsLmNvbQ==