 Dalton Kambale Munyambalu1
Dalton Kambale Munyambalu1 Idania Hildago2Yves Tibamwenda Bafwa1Charles Abonga Lagoro1
Idania Hildago2Yves Tibamwenda Bafwa1Charles Abonga Lagoro1 Franck Katembo Sikakulya3,4*Bienfait Mumbere Vahwere3Ephraim Dafiewhare1Lazaro Martinez1Fardous Abeya Charles1,5
Franck Katembo Sikakulya3,4*Bienfait Mumbere Vahwere3Ephraim Dafiewhare1Lazaro Martinez1Fardous Abeya Charles1,5- 1Department of Internal Medicine, Kampala International University-Teaching Hospital, Bushenyi, Uganda
- 2Department of Clinical Chemistry Laboratory, Kampala International University-Teaching Hospital, Bushenyi, Uganda
- 3Department of General Surgery, Kampala International University-Teaching Hospital, Bushenyi, Uganda
- 4Faculty of Medicine, Université Catholique du Graben, Butembo, Democratic Republic of Congo
- 5Department of Internal Medicine, Mbarara University of Science and Technology, Mbarara, Uganda
Background: Diabetic peripheral neuropathy (DPN) is the most common complication of diabetes mellitus (DM). Approximately 50% of diabetic patients are estimated to develop DPN, depending on disease duration and diabetic control. Early diagnosis of DPN will avoid complications, including non-traumatic lower limb amputation, which is considered the most debilitating complication, as well as significant psychological, social, and economical problems. There is a paucity of literature on DPN from rural Uganda. This study aimed to deliver the prevalence and grade of DPN among DM patients in rural Uganda.
Methods: A cross-sectional study that recruited 319 known DM patients was conducted in an outpatient clinic and a diabetic clinic at Kampala International University-Teaching Hospital (KIU-TH), Bushenyi, Uganda, between December 2019 and March 2020. Questionnaires were used to obtain clinical and sociodemographic data, a neurological examination was carried out to assess the DPN, and a blood sample was collected from each participant (for random/fasting blood glucose and glycosylated hemoglobin analyses). Data were analyzed using Stata version 15.0.
Results: The sample size was 319 participants. The mean age of study participants was 59.4 ± 14.6 years and there were 197 (61.8%) females. The prevalence of DPN was 65.8% (210/319) (95% CI 60.4% to 70.9%), and 44.8% of participants had mild DPN, 42.4% had moderate DPN, and 12.8% had severe DPN.
Conclusion: The prevalence of DPN at KIU-TH was higher among DM patients and its stage might have a negative impact on the progression of Diabetes Mellitus. Therefore, clinicians should consider neurological examination as a routine during assessment of all DM patients especially in rural areas where resources and facilities are often limited so that complications related to Diabetic mellitus will be prevented.
Introduction
Diabetes mellitus (DM) globally spread and affects people of all ages and races (1). The International Diabetes Federation (IDF) reported, in 2021, that 537 million adults aged 20–79 years are currently living with DM, which represents 10.5% of the world’s population in this age group, with Africa being the part of the world where more than half the people with DM are undiagnosed (2). About 80% of diabetic patients live in low- and middle-income countries and almost 4 million people die of diabetes and its complications, with half of these people below the age of 60 years (1–3). The incidence of diabetic complications is expected to increase, and about 6.7 million adults are estimated to have died as a result of DM or its complications in 2021 (1, 2). DM affects a wide variety of neurological complications, which may involve the peripheral or autonomic nervous system, or both, mostly impairing the quality of life of patients, with impact on morbidity and mortality outcomes (4).
Diabetic peripheral neuropathy (DPN) corresponds to a type of nerve damage that typically affects the feet and legs, and sometimes affects the hands and arms in diabetic patients (5). DPN is the commonest diabetic neuropathy and must be diagnosed after the exclusion of other causes of polyneuropathy. Distal symmetric sensorimotor polyneuropathy is the most common type of DPN (5, 6). However, some patients might be asymptomatic. The condition seems to be irreversible and remains the most common chronic complication of DM (4–6). The real prevalence of DPN is not known and reports vary from 10% to 90% in diabetic patients, depending on the criteria and methods used to define neuropathy, and it has been reported that neurological complications occur equally in both type 1 diabetes mellitus (T1DM) and type 2 diabetes mellitus (T2DM) patients (6). The regional prevalence of DPN is 12.9% in North America and 3.2% generally in Africa (7). Approximately 50% of patients with diabetes are estimated to develop DPN, depending on disease duration and diabetic control (8).
Early diagnosis of DPN will avoid complications, the most debilitating of which is non-traumatic lower limb amputation, resulting in significant psychological and socioeconomic problems for the patient due to depression, societal stigmatization, and job loss due to the loss of a limb (6–8). In Africa there is widespread poverty and inadequate health insurance, which impedes the acquisition of efficient prostheses that would offset some of these problems. Even when overt gangrene has not yet complicated a foot ulcer, treatment of an ulcer drains the financial resources of the patient (9).
Few studies have been carried out in urban Uganda, but less is known in rural areas where patients are coming to seek help for their health in the advanced stages of the disease and with a high risk of complications related to DM (10). Therefore, the purpose of this study was to highlight the prevalence of DPN and its grade among DM patients in a rural southwestern Ugandan health facility.
Methods
Study design
This was a cross-sectional study, conducted from 13 December 2019 to 25 March 2020.
Study site
The study was carried out at Kampala International University Teaching Hospital (KIU-TH) in the Department of Internal Medicine, located in Bushenyi District, in rural southwest Uganda.
Study participants
Participants included all adult known DM patients (aged 18 years and above) who attended the medical outpatient patient department (MOPD), DM clinic, general outpatient department (GOPD), and private outpatient department (POPD) during the duration of the study, and who consented to participate. We excluded any patients with a mental disorder, patients who were unable to withstand an interview, patients who changed their consent, all pregnant women, newly diagnosed DM patients, and very sick DM patients admitted in the medical ward.
Participants were consecutively recruited. The sample size was of 319 patients using Leslie’s formula (1965), as shown in Equation 1:
N = desired sample size for population greater than 10,000.
Z2 = standard normal deviation, assuming a 95% CI Z = 1.96.
P = proportion in the population estimated to have DPN in Uganda (Mulago Hospital, Kampala) = 29.4% according to Kisozi et al. (10).
Data collection
Data were collected using a paper-based investigator-administered questionnaire that was designed in simple English and translated in local language for those who were unable to understand English.
Patients were given information about the study, and then written consent was sought and signed. Demographics (i.e., age, sex, address, marital status, education status), history of chronic illness, such as hypertension, kidney disease, and HIV infection status, and social habits, such as the use of alcohol and volume, smoking cigarette status and number of sticks per day, and adherence to medication were taken.
The body mass index (BMI) was calculated from a ratio of the patients’ weight in kilograms to the square value of the height in meters (kg/m2). Normal BMI was defined as< 24.9 kg/m2, overweight as 25 to 29.9 kg/m2, and obesity as ≥ 30 kg/m2 (WHO, 2000). Blood pressure was measured by using a manual sphygmomanometer, with appropriate cuff sizes for the patient arms being used. High blood pressure was defined as having a systolic blood pressure ≥ l40 mmHg or diastolic pressure ≥ 90 mmHg (European Society of Cardiology/European Society of Hypertension, 2018).
The physical/neurological examination was done. Pressure sensation was assessed using a 10-g monofilament (i.e., the Semmes–Weinstein monofilament test) at four of the ten standard sites of the sole of the feet (plantar base of the big toe, second and fifth toes, and at the heel), avoiding areas with callosity. Vibration sense was elicited using a 128-Hz turning fork at the big toe. Achilles deep tendon reflex was tested by using a standard patellar hammer.
Using a sterile disposable syringe and needle, 4 ml of blood was withdrawn from the anterior cubital fossa of each patient after cleaning the skin with a swab soaked in 70% alcohol. The blood sample was placed in a EDTA (ethylenediaminetetraacetic acid) purple container for random blood sugar (RBS)/fasting blood sugar (FBS) and glycosylated hemoglobin (HbA1c) analyses. Furthermore, RBS/FBS was screened using a Control D glucometer machine made in India (2018) by Haiden Technology with the manufacturer’s glucose sticks. The level of HbA1c was screened using an Ichroma II Machine (2017) and the appropriated reagents for measuring HbA1c. Each study participant received a printed copy of their RBS/FBS and HbA1c results.
The Neuropathy Disability Score (NDS) was used in assessing the grade of DPN for each patient. The NDS system is a tool of neuropathy evaluation score ranging from 0 to 10, which can also be used for assessment of severity of peripheral neuropathy by considering four parameters: vibration sense by using a 128-Hz tuning fork (0 = present, 1 = reduced/absent for each foot), temperature sensation by using a cold tuning fork (0 = present, 1 = reduced/absent for each foot), pin-prick sensation by a monofilament test (0 = present, 1 = reduced/absent for each foot), and ankle reflex/Achilles tendon reflex by using a patellar hammer (0 = normal, 1 = present with reinforcement, 2 = absent per side). Absence of neuropathy (normal) was considered when the score was from 0 up to 2. The grade of DPN disability was graded as follows: mild (scores: 3–5), moderate (scores: 6–8), and severe (scores: 9–10). The NDS is validated and is found to be 65% sensitive and 91% specific for diagnosing diabetic neuropathy (11). We used a 10-g monofilament test, patellar hammer, 128-Hz tuning fork/Hartman C 128 for the assessment of DPN, as described above.
Data analysis
Data were captured in paper forms and entered into Epi Info™ 7.2, Microsoft Excel version 2010 and exported into Stata 15.0 for analysis. Data were processed accordingly and summarized using means for continuous variables or proportions for categorical variables.
For determining the prevalence of DPN at KIU-TH, we summarized data as frequencies and percentages, and 95% CIs were obtained for prevalence as an estimation measure.
Ethics approval and consent to participate
The study was conducted after approval of Kampala International University-Research Ethics Committee (KIU-REC) under reference UG-REC-023/201939.
Written informed consent was obtained. Confidentiality for all the patients involved in the study was assured. People diagnosed with DPN were referred to the appropriate medical personnel.
Results
Overall, 338 participants arrived at the MOPD, DM clinic, GOPD, and POPD at KIU-TH. Five participants were excluded from the study because three were newly diagnosed as having DM and two were very sick. A total of 333 participants met the inclusion criteria, and among them five declined to consent, and nine declined the examination and the blood sample collection. Finally 319 study participants consented, filled the study questionnaire, were examined, and blood samples taken during the study period and analyzed.
Characteristics of the study participants
In Table 1 below, majority (61.8%) of the participants were females, most (83.7%) of them were married and residing in a rural area (85.3%), with a mean age of 59.4 ± 14.6 years, and were agricultural workers by occupation (77.7%). In addition, most participants were T2DM (95.3%) on oral hypoglycemic agents (63.6%), overweight (55.8%) with a mean BMI of 26.26 ± 3.48 kg/m2, and poor glycemic control (53.9%), with a DM duration of less than 10 years (65.5%), i.e., with a mean duration of 7.33 ± 6.40 years. A few study participants were taking alcohol or had an Audit Score of 1 (10%), with a history of smoking (13.5%) and hypertension (50.2%).
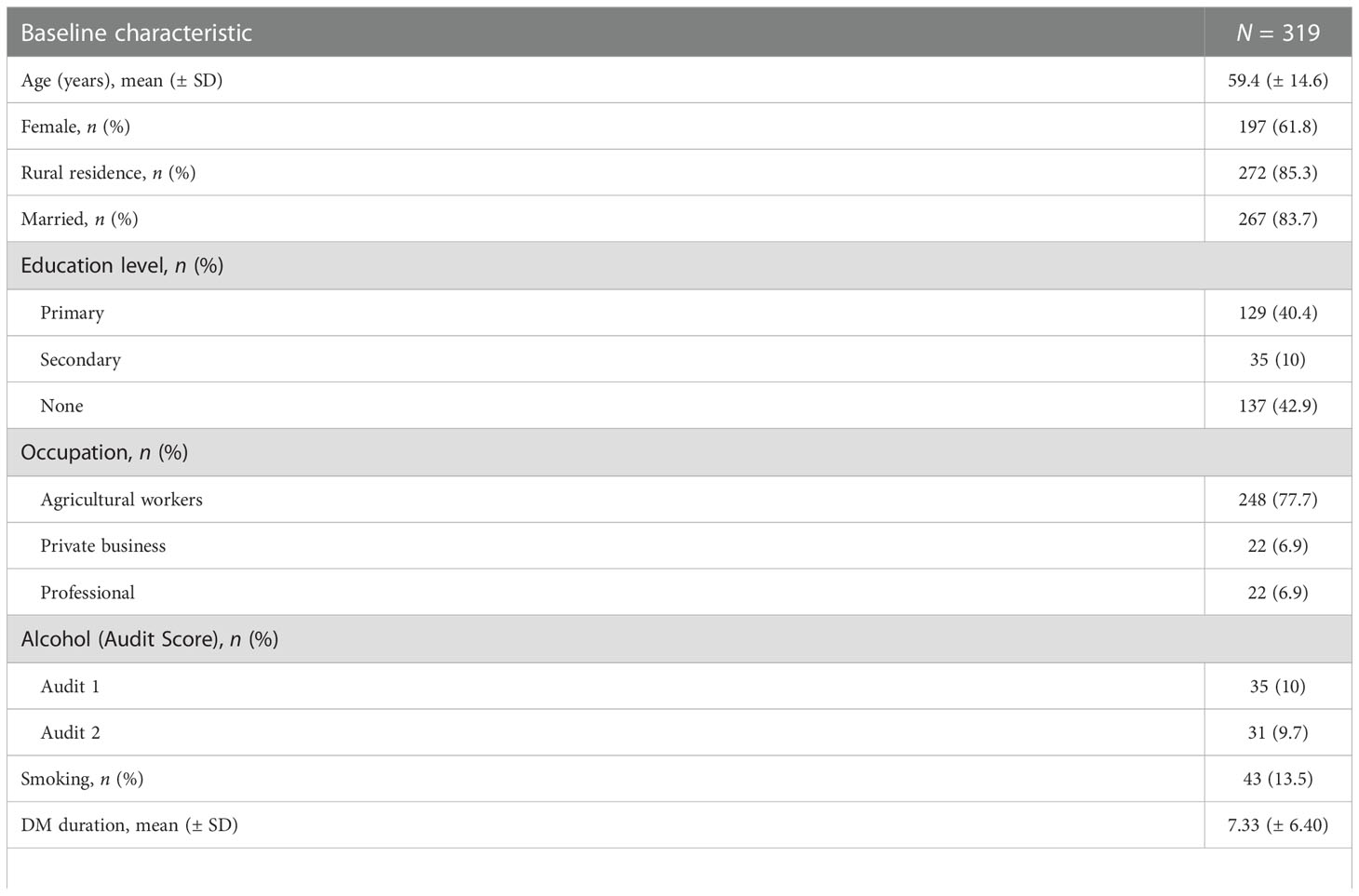
Table 1 Baseline characteristics of the study participants.
Prevalence of DPN
The prevalence of DPN among adult diabetic patients attending Kampala International University-Teaching Hospital was 65.8% (210/319), (95% CI 60.4-70.9) by using the Neuropathy Disability Score (NDS) (Figure 1).
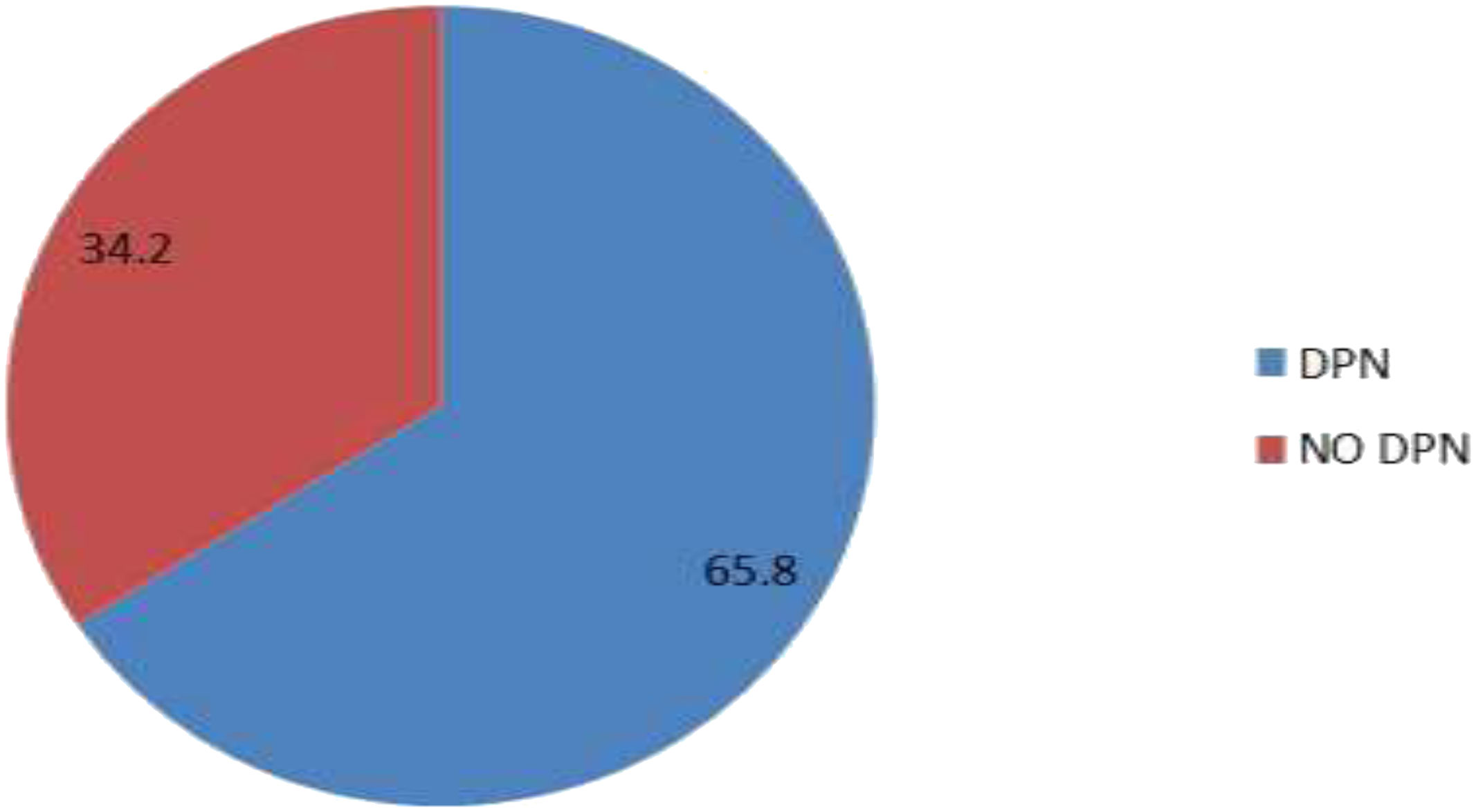
Figure 1 Prevalence of DPN among known DM patients attending KIU-TH.
Grade of DPN among known DM patients attending KIU-TH.
In our study, 210 (65.8%) participants had DPN, 44.8% had mild DPN, 42.4% had moderate DPN, and 12.8% had severe DPN.
Discussion
Characteristics of the study participants
The aim of this study was to determine the prevalence and grade of DPN among known DM patients in a rural setting of Uganda (KIU-TH, Ishaka in the Bushenyi District of southwestern Uganda). In this current study, most of the participants were female, agricultural workers, and from rural residency, with a mean age of 59.4 ± 14.6 years.
Garoushi et al. in a meta-analysis study conducted in the USA, the UK, France, Belgium, and South Africa (2018), and Morkid et al. in Bangladesh (2010), found that advanced age was significant with the occurrence of DPN (12). DPN develops progressively over months to years, and by the time the aging process is taking place there is a decrease in peripheral nerves function, mostly in lower extremities, with physical disabilities, gait disturbance, and falls.
Prevalence of DPN
The overall prevalence of peripheral neuropathy among adult diabetic patients attending KIU-TH was 65.8% (95% CI 60.4% to 70.9%).
This study’s result is similar to the global prevalence of DPN (1). This could be explained by the fact that the global prevalence considers all the population by using a standard score (NDS) for assessing DPN. In a study carried out in India, the prevalence of DPN is lower than of this study (13). This disparity is due to the age of the participants, in which the previous study enrolled patients from age 30 years and above and they considered all the neurological complications in diabetic patients.
The prevalence of DPN in our study is similar to a study carried out in Morocco (14). The reason for the similarity could be because of the, almost, same social conditions as African countries and because methods used for the assessment of DPN were the same. This current study found a lower prevalence than a study carried out in Nigeria by Salawu et al. (15), because our study included all types of diabetes, whereas the other study considered only patients with T2DM.
The prevalence of DPN in this study was higher than those in studies carried out in Cameroon and Kampala (4, 10). In our study, the prevalence is higher probably because of the sample size, and the tools and criteria used for diagnosing DPN. In addition, the above study that was carried out in Kampala was conducted among newly diagnosed DM patients only.
Grade of DPN
In our study, 210 (65.8%) participants had DPN, 44.8% (94/210) had mild DPN, 42.4% (89/210) had moderate DPN, and 12.8% (27/210) had severe DPN.
The study of Kazemi et al. in Iran (16) found that most of their participants had mild DPN and a few of them developed severe DPN, which corresponds to our findings as well, whereby the method used for the assessment of DPN were similar (NDS), with the same study design by considering a large number of DM patients. However, in Kampala, Kisozi et al. (10) got a larger number of patients with moderate DPN. The discrepancy could have been explained by the fact that in our study we used different tools for assessing DPN in the context of a rural setting and few of our participants had foot ulcers as a predictor of advanced DPN.
Vogt et al., in their study carried out in Tanzania (17), detected that severe DPN represented almost one-quarter of patients, which is different from our findings, because from their research, they compared only assessment tools for DPN without considering patient findings based on symptoms and signs. The NDS is an important tool for assessing DPN and constitutes a good predictor for risk of ulceration. Knowing DPN patients based on this score might help us to prevent patients from foot ulceration, diabetic foot, and other related complications that have a poor prognosis (18).
Strengths and limitations
This is the first study concerning DPN in the southwest of Uganda and the sample size used was large to make a clear conclusion about our findings. Furthermore, the study did not use other diagnostic specific tests of DPN, such us corneal confocal microscopy and electrophysiological studies (e.g., nerve conduction studies, electromyography).
Conclusion
The prevalence of DPN among known diabetic patients attending KIU-TH was higher, classified respectively in mild, moderate, and severe DPN, according to the number among DM patients. This might have a negative impact as DM is progressing. Therefore, for better prevention of other chronic complications, clinicians should consider neurological examination as routine during regular assessment of all DM patients, especially in rural areas where resources and facilities are often limited.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statement
The studies involving human participants were reviewed and approved by Kampala International University-Research Ethics Committee. The patients/participants provided their written informed consent to participate in this study.
Author contributions
DM conceived, designed the study, participated in the data collection, analysis, and drafted the manuscript. FA and YB analyzed the data and performed statistical tests. IH prepared and analyzed the collected blood samples. FS, BM, LM, ED, and CL assisted in the study conception/design and critically reviewed the manuscript. All authors approved the manuscript for publication.
Acknowledgments
We thank the research assistants who helped in recruitment of participants and collecting blood samples, the research participants and all DM patients who consented to participate in the study, the administration of KIU-TH and Clinical Chemistry Lab/KIU-TH.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Abbreviations
BMI, body mass index; DM, diabetes mellitus; DPN, diabetic peripheral neuropathy; FBS, fasting blood sugar; GOPD, general outpatient department; HbA1c, glycosylated hemoglobin; IDF, International Diabetes Federation; KIU-TH, Kampala International University-Teaching Hospital; MOPD, medical outpatient patient department; NDS, Neuropathy Disability Score; POPD, private outpatient department; RBS, random blood sugar; T1DM, type 1 diabetes mellitus; T2DM, type 2 diabetes mellitus.
References
1. Ede O, Eyichukwu GO, Madu KA, Ogbonnaya IS, Okoro KA, Basil-Nwachuku C, et al. Evaluation of peripheral neuropathy in diabetic adults with and without foot ulcers in an African population. J Biosci Med (2018) 6(12):71–8. doi: 10.4236/jbm.2018.612007
2. International Diabetes Federation. IDF diabetes atlas. 10th edn. (Brussels, Belgium: IDF) (2021). Available at: https://www.diabetesatlas.org.
3. Iyagba A, Onwuchekwa A. Diabetic cachectic neuropathy: An uncommon neurological complication of diabetes. SAMJ: South Afr Med J (2016) 106(12):1190–1. doi: 10.7196/SAMJ.2016.v106.v106.i12.11198
4. Kuate-Tegueu C, Temfack E, Ngankou S, Doumbe J, Djientcheu VP, Kengne AP. Prevalence and determinants of diabetic polyneuropathy in a sub-Saharan African referral hospital. J Neurological Sci (2015) 355(1-2):108–12. doi: 10.1016/j.jns.2015.05.035
6. Vinik AI, Erbas T, Casellini CM. Diabetic cardiac autonomic neuropathy, inflammation and cardiovascular disease. J Diabetes Invest (2013) 4(1):4–18. doi: 10.1111/jdi.12042
7. Tesfaye S, Boulton AJ, Dickenson AH. Mechanisms and management of diabetic painful distal symmetrical polyneuropathy. Diabetes Care (2013) 36(9):2456–65. doi: 10.2337/dc12-1964
8. Singh R, Kishore L, Kaur N. Diabetic peripheral neuropathy: current perspective and future directions. Pharmacol Res (2014) 80:21–35. doi: 10.1016/j.phrs.2013.12.005
9. Ogbera AO, Fasanmade O, Ohwovoriole AE, Adediran O. An assessment of the disease burden of foot ulcers in patients with diabetes mellitus attending a teaching hospital in Lagos, Nigeria. Int J Lower Extremity Wounds (2006) 5:244–9. doi: 10.1177/1534734606294538
10. Kisozi T, Mutebi E, Kisekka M, Lhatoo S, Sajatovic M, Kaddumukasa M, et al. Prevalence, severity and factors associated with peripheral neuropathy among newly diagnosed diabetic patients attending mulago hospital: a cross-sectional study. Afr Health Sci (2017) 17(2):463–73. doi: 10.4314/ahs.v17i2.21
11. Dyck PJ, Bushek W, Spring EM, Karnes JL, Litchy WJ, O'Brien PC. Vibratory and cooling detection thresholds compared with other tests in diagnosing and staging diabetic neuropathy. Diabetes Care (1987) 10(4):432–40. doi: 10.2337/diacare.10.4.432
12. Garoushi S, Johnson MI, Tashani OA. Point prevalence of painful diabetic neuropathy in the middle East and north Africa region: A systematic review with meta-analysis. Libyan J Med Sci (2018) 2(3):85. doi: 10.4103/LJMS.LJMS-36-18
13. Battula P, Afreen S, Meena E, Reddy S, Sujatha G. Prevalence of sensory peripheral neuropathy in diabetic patients at diabetes care center;a cross sectional study,4066-4071. Int J Res Med Sci (2017) 5(9):4066–71. doi: 10.18203/2320-6012.ijrms20173984
14. Chahbi Z, Hicham B, Bouchra L, Mohamed Z, Sanae E, Lahoussaine A, et al. The prevalence of painful diabetic neuropathy in 300 Moroccan diabetics. Pan Afr Med J (2018) 31(1). doi: 10.11604/pamj.2018.31.158.14687
15. Salawu F, Shadrach L, Adenie T, Martins O, Bukbuk D, et al. "Diabetic peripheral neuropathy and its risk factors in a Nigerian population with type 2 diabetes mellitus. Afr J Diabetes Med (2018) 26(1). doi: 10.4103/liuj.liuj-62-18
16. Kazemi M, Abbas M, Javad K, Mahjub H, Javad F. Diabetic peripheral neuropathy class prediction by multicategory support vector machine model: A cross-sectional study. Epidemiol. Health (2016) 38. doi: 10.4178/epih.e2016011
17. Vogt EC, Øksnes M, Suleiman F, Juma BA, Thordarson HB, Ommedal O, et al. Assessment of diabetic polyneuropathy in Zanzibar: Comparison between traditional methods and an automated point-of-care nerve conduction device. J Clin Trans Endocrinology (2017) 10:9–14. doi: 10.1016/j.jcte.2017.09.001
Keywords: diabetic peripheral neuropathy, prevalence and grade, Kampala, Uganda, diabetes mellitus
Citation: Munyambalu DK, Hildago I, Bafwa YT, Lagoro CA, Sikakulya FK, Vahwere BM, Dafiewhare E, Martinez L and Charles FA (2023) Prevalence and grade of diabetic peripheral neuropathy among known diabetic patients in rural Uganda. Front. Clin. Diabetes Healthc. 3:1001872. doi: 10.3389/fcdhc.2022.1001872
Received: 24 July 2022; Accepted: 30 November 2022;
Published: 11 January 2023.
Edited by:
Raffaele Ivan Cincione, University of Foggia, ItalyReviewed by:
Alfredo Caturano, University of Campania Luigi Vanvitelli, ItalyLixin Guo, Beijing Hospital, Peking University, China
Copyright © 2023 Munyambalu, Hildago, Bafwa, Lagoro, Sikakulya, Vahwere, Dafiewhare, Martinez and Charles. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Franck Katembo Sikakulya, ZnJhbmNrc2lrYWt1bHlhQGdtYWlsLmNvbQ==