 Li Zhao1
Li Zhao1 Quan Chen
Quan Chen Chunyan Li
Chunyan Li James W. Holsinger Jr.
James W. Holsinger Jr. Xiao Ma
Xiao Ma- 1West China School of Public Health, Chengdu, China
- 2University of Kentucky, Lexington, KY, United States
In China, the preventive medicine undergraduate professional training program is the major approach to training public health practitioners. The history of undergraduate education in public health/preventive medicine in China is reviewed utilizing the West China School of Public Health at Sichuan University as an example for analyzing this undergraduate major and its curriculum. Needed reforms in the Chinese undergraduate preventive medicine programs are presented, including review of the traditional preventive medicine course content, revision of its curriculum structure, the need to increase practical experience and to develop variety in teaching and assessment techniques, and systematic planning for curriculum reform. Current efforts at reform of the preventive medicine undergraduate program at Sichuan University’s West China School of Public Health are presented.
The History of Public Health Undergraduate Education in China
Before 1949, a system of specialized public health higher education in China did not exist. In addition to public health education provided by the Peking Union Medical College Dongdan Health Office for interested physicians and nurses, only a few schools, such as Huaxi Union University School of Medicine in Chengdu and Tongji University School of Medicine in Shanghai, had established a department of public health and offered public health programs for medical students. At that time, some scholars who had completed advanced education overseas returned to China when the country decided to carry out public health education and scientific research. Chen Zhiqian (also known as Dr. C. C. Chen), Zhu Zhanggeng, Xu Suen, and others created a health education core at the bachelor’s level at Nanjing Central University Medical School (Weilian, 1988). However, due to the influence of World War II and the conditions related to it, China was unable to establish a public health education system in the first half of the twentieth century.
After 1949, China began to focus on the professional training of public health practitioners. China Medical University and Shenyang Medical College merged and established China’s first independent professional public health department, initiating China’s public health education system. It is important to recognize that in China medical education is a baccalaureate degree.
In August 1950, China’s first national health practice conference established the “Four Health Practice Principles” with “Prevention First” at their core. At that time, there were three medical schools training public health practitioners. Following the conference, China gradually introduced the former Soviet Union’s health and epidemic prevention system, and in 1953, formally established health and epidemic prevention centers in order to improve the health-care system. In 1954, Soviet experts began to train Chinese public health educators. At this time, China was threatened by acute communicable infectious diseases such that the demand for public health practitioners was urgent, as well as the need for training more practitioners for the future. In 1954, the first National Medical Higher Education Conference was held in Beijing. This meeting unified medical specialty higher education, the corresponding academic system, and the development of the curriculum and teaching plans. In 1955, a major change occurred with a nationwide reorientation of the medical schools. Six institutions, Beijing Medical College, Shanghai First Medical College, Harbin Medical College, Wuhan Medical College, Sichuan Medical College (West China Union University) and Shanxi Medical College, established independent departments of public health to provide public health professional higher education and training, forming China’s public health education system.
In 1963, the State Ministry of Education promulgated the College Professional Directory with 10 majors set up under the category of “Health Professional,” including medicine, public health, pediatric medicine, oral medicine, pharmacy, medicinal chemistry, nursing, medical technology, and traditional Chinese medicine and therapy (Ministry of Higher Education of P. R. China, 1963).
China’s public health higher education system was modeled on the former Soviet Union’s system with its major disciplines of epidemiology, biostatistics, environmental health, occupational health, nutrition and food health, school hygiene, health professional, and several others. The development of the new system’s public health courses was based on these disciplines. Although China has been learning from western countries since the 1980s, the public health education system has not changed, and these disciplines are still the required courses in the curriculum of public health higher education in China. In the mid-1980s, the health professional category changed its name to preventive medicine. However, it was changed in name only with the program requirements remaining basically the same. In point of fact, the preventive medicine major was identical to a public health major in other national systems.
By 1978, there were 21 higher education institutions offering the public health major in addition to a baccalaureate degree in medicine. By 1986, there were 36 higher education institutions with the number reaching 44 in 1998. During this time, the average number of newly enrolled students for each institution averaged between 40 and 60. For those institutions that established the public health major in the 1950s, the number of newly enrolled students approached 100 per year. Since 1988, the number of universities establishing a major in public health has increased continuously. According to the national Ministry of Education, this number reached to 51 in 2002. A total of 2,541 students graduated with a major in public health in 2002, 3,307 students graduated in 2003, and the newly enrolled numbers for each of those years were 4,189 and 5,103, respectively. By 2004, there were 60 institutions with a major in public health. According to university statistics, this number reached 88 in 2009 and 93 in 2014, having more than doubled in number since 1998. Every year, more than 10,000 students now graduate from these institutions.
After 1978, there were three major changes and revisions to the College Professional Directory. In the 1987 edition, the national Ministry of Education created a new category called “Preventive Medicine” with four majors, preventive medicine, environmental health, sanitary technology, and nutrition and food health, created under this category (Ministry of Education of P. R. China, 1987). This replaced the original category “Health Professional.” In the 1993 edition, maternal and child health was formally introduced into preventive medicine, making a total of five majors under this category (Ministry of Higher Education of P. R. China, 1993). The third revision of the College Professional Directory occurred in 1998 with all majors other than preventive medicine deleted from the directory (State Ministry of Education Higher Education Core, 1998). However, due to the insistence of the West China School of Public Health at Sichuan University, the major in sanitary technology was included in the 2003 edition. Now more than 30 universities offer this major nationwide.
The goal of public health/preventive medicine in China is to train practitioners, who have deep understanding of the knowledge and skills in public health/preventive medicine and who have the capacity to fulfill the required tasks in such public health institutions as the various Centers of Disease Control (CDC) and other health authority agencies. There are four major areas available in the job market for graduates: first, working in a public health professional institution at various levels; i.e., centers of disease control and prevention, occupational disease prevention centers, health-related laboratory agencies, health education centers, community health departments, etc.; second, working at health authority agencies providing health management and service at various levels of government, i.e., environmental protection agencies, food and drug agencies, and customs inspection and quarantine departments; third, working at public health-related companies, i.e., pharmaceutical, insurance and third party laboratory companies; and fourth, performing research and teaching related to work in hospitals or universities.
Undergraduate Public Health/Preventive Medicine Curriculum
The Academic System and Curriculum Structure of Undergraduate Public Health/Preventive Medicine in China
Since the establishment of the public health education system in China, the public health/preventive medicine program began as a 4-year program during the 1950s to the late 1970s, and a 6-year program from 1980 to 1987, and finally it became a 5-year program from 1988 on.
The Chinese public health/preventive medicine undergraduate program is composed of five parts: basic public health courses, basic medical courses, clinical courses, public health/preventive medicine foundations and professional courses, and practice courses (see Table 1). The first four parts are theory-based. Public health/preventive medicine courses are centered on “five major public health components” (environmental health, workplace hygiene, nutrition and food hygiene, child health, radiological), epidemiology, and biostatistics. Practical courses include clinical practice, public health practicum, and capstones. The practical content, respectively, focuses on three areas: clinical skills, public health vocational skills, and scientific research training. As shown in Table 1, the time of the practicum that directly relates to the training of public health vocational skills is relatively short. One of the aims of the capstone project is to train students to understand the basic processes of scientific research and to develop their scientific research ability.
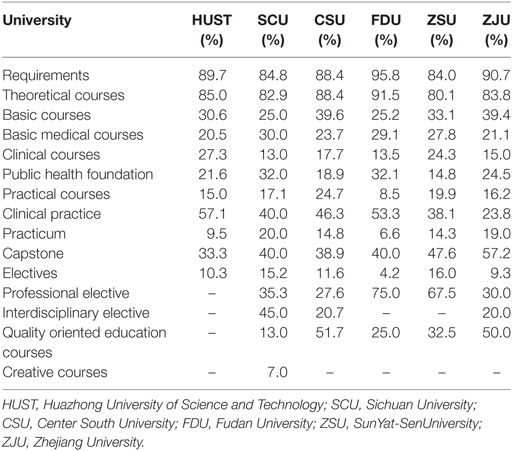
Table 1. The structure of China’s six universities’ public health/preventive medicine undergraduate professional curriculum (credits).
It may be noted in Table 1 that there is a significantly larger number of theoretical courses than practice-based courses among the public health/preventive medicine required courses. Fewer courses are designed to develop students’ professional skills. Among the elective courses, the proportion of practice-based elective courses is relatively large and the proportion of cross-disciplinary elective courses is relatively small. Due to the nature of the public health courses, they can be divided into two categories: public health basic courses and public health specialized courses. Basic courses can be divided into methodological and natural science courses; specialized courses can be divided into traditional courses and sociology courses.
Table 2 demonstrates that the public health programs in China are composed of traditional health science (39.0%), methodology (26.5%), and social science (16.2%) courses. Meanwhile, Sichuan University and Fudan University offer an introduction to public health courses in the early years of the student’s undergraduate education.
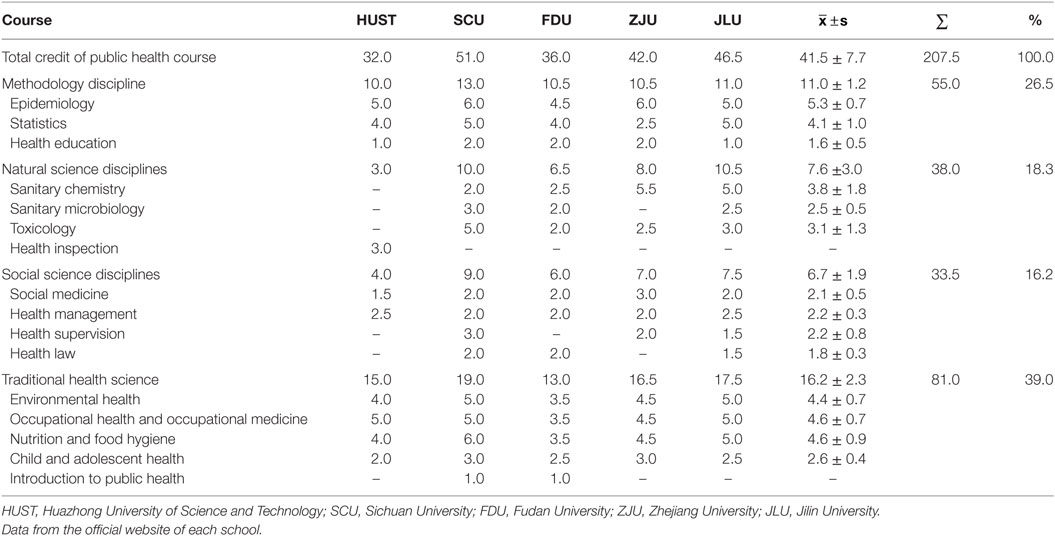
Table 2. Public health course credit for preventive medicine undergraduates in five Chinese universities.
The Chinese Undergraduate Preventive Medicine Programs: Needed Reforms
Curriculum and Traditional Course Content Review
China’s public health/preventive medicine educational program has a long history, and the current curriculum model has become dated (Chengsong, 2014). Since the establishment of hygiene studies in the 1950s, the “three-stage” (Wang et al., 2012) (basic–clinical–prevention) teaching style has been utilized, and the curriculum model has been unchanged. Basic science and clinical medicine courses have comprised a significant percentage of the program’s coursework. The specialized courses are still composed of the “five major public health components,” including epidemiology and biostatistics, providing core public health/preventive medicine content (Yuan et al., 2012). The result has been that students have obtained a solid foundation in the biomedical aspects of the program.
Necessary Public Health Curriculum Structure Revisions
China’s public health education curriculum structure and content has failed to meet the requirements of modern public health. Updating of curriculum has been slow and has failed to reflect modern trends in public health/preventive medicine practitioner development. It lacks core courses in the humanities and non-scientific areas (Wang et al., 2001). The public health/preventive medicine program has been considered outdated (Cheng et al., 2007) with inadequate education in emergency response capabilities, on-site ethical practice, scientific research, and other significant areas of public health/preventive medicine knowledge.
Increase Practicum Time and Choice of Venues
Among the three categories of practice courses, the public health-related practicum makes up the smallest proportion of the curriculum, leading directly to a paucity of knowledge of public health practice for students (He, 2013). Usually, the public health practicum focuses on the different CDC levels in China, health authority agencies, and the customs inspection and quarantine departments.
Increase Variety in Teaching Techniques
Currently, the course format is based on a lecture approach (Zhang et al., 2005) with few courses offering laboratory experience or field practice. Even though students acquire a solid foundation of theoretical knowledge, the curriculum is inadequate to develop practice capacity (Jin et al., 2010). There is too great an emphasis on theoretical knowledge with little to connect it to real-world practice with a failure to expend energy on creative and practice skills (Cheng et al., 2007).
Innovate and Develop Curriculum Assessment
In terms of curriculum assessment, the public health/preventive medicine program’s major assessment process is based on testing the students’ degree of mastery of knowledge. The main purpose of the examinations is to examine the student’s base of theoretical knowledge. At present, China has not developed a unified and authoritative public health/preventive medicine program assessment and evaluation mechanism. The assessment of a school’s public health/preventive medicine curriculum is to a certain extent reflected in the Ministry of Education’s organized undergraduate teaching level assessment and the selection of quality courses at all levels. At the same time, there is a lack of nationwide authority for public health/preventive medicine education certification and standardization. In order to improve the processes of public health/preventive medicine education, program assessment mechanisms need to be strengthened and improved.
Systematic Planning for Curriculum Reform
Due to the initiation of the national school reform effort in 2000, the majority of China’s public health colleges were merged into comprehensive universities. Utilizing the comprehensive universities’ advantages has not occurred to any significant degree nor has it been studied in practice. Although some current research has focused on the reform of public health/preventive medicine education, no research has approached reform from a holistic point-of-view. As an example of the difficulty in reforming the curriculum, cross-linking, cross-penetration, and integration between courses within the program has not occurred (He, 2013).
Improve Variation between Universities
The objectives of the public health/preventive medicine programs among the different schools are similar. No clear difference is apparent between the various universities’ public health/preventive medicine programs regardless of the level of the university or its style. The institutions having the objective of educating public health/preventive medicine practitioners should utilize their respective regional advantages and develop their own characteristic courses based on the societal needs of the population served.
Curriculum Reform Development and Practice at Sichuan University’s West China School of Public Health
Due to the profound changes in China’s economic and social life as well as the process of globalization, some infectious diseases have been revived, new infectious diseases have emerged, chronic diseases have become increasingly prominent, and public health crises/emergencies have been occurring more frequently. The practice of public health and public health education has been facing unprecedented challenges. Accordingly, public health education reform is required to fulfill the historic mission of improving the health of the public and to meet its socioeconomic requirements. Sichuan University’s West China School of Public Health is one example of a university that is revising its public health/preventive medicine curriculum.
The Basis for Curriculum Reform
The reform of the West China School of Public Health preventive medicine undergraduate major was based on the “Public Health Education Basic Requirements (PHEBR)” (Chinese Preventive Medicine Association of Public Health Education Branch and the Public Health Dean/Department Director Contact Conference, 2006) Based on global experience, the PHEBR includes public health practice guidelines centered on professional knowledge and core competency. The PHEBR is composed of a total of 37 competency items divided into six areas: (1) professionalism, i.e., consciously establish, strengthen, and maintain the values of the public health practitioner; (2) medical foundation, i.e., learning the appropriate way to utilize basic medical knowledge; (3) population health, i.e., thinking through the needs of the population served and building a profound understanding of socio-ecological health model; (4) health management and social mobilization, i.e., understanding modern management concepts, knowledge and skills, and being aware of the appropriate use of health-related resources; (5) information management, i.e., correctly collect and utilize various types of health-related information and apply it in practice; (6) scientific research, i.e., being able to critically assess existing knowledge, technology, and information, and apply it in professional activities and research.
Training Objectives: Excellence for the People
Modern public health practice and public health education have increasingly highlighted the need for broad human engagement, extensive social participation, diverse cultural understanding, strict ethical principles and legal norms, human and environmental understanding, international vision and global cooperation, and cross-integration between management and information technology. Preventive medicine professional education objectives should be based on current reality and engaging the future. In addition, due to the specific aspects of public health, there is a need for preventive medicine undergraduate students to develop a caring attitude toward their fellow humans and society in general. They should also keep in mind the need for a spirit of constantly seeking quality improvement. Considering the history and characteristics of the West China School of Public Health, training objectives for the preventive medicine undergraduate program includes developing a profound humanistic background, a rigorous scientific spirit, a strong sense of innovation, and a broad international viewpoint.
Adjust the Curriculum Structure
The preventive medicine undergraduate curriculum at the West China School of Public Health includes two phases. The first phase includes two stages: (1) general education and professional basic science education and (2) personalized education. The course credits for the general education stage account for 20.95% of the total credits applied toward graduation. The professional basic science course credits account for 29.76% and personalized education course credits account for 49.29% of the total credits in this phase. The second phase of the curriculum consists of two parts: (1) public health theoretical courses and (2) field practicum. The practicum includes a traditional clinical practice practicum, a graduation capstone project, experimental courses, and innovative educational activities. In addition, there are three different types of theoretical public health elective courses offered, including courses in academic research, practical application of knowledge, and innovative exploration.
The Reformed Curriculum and Teaching Techniques
The reformed curriculum has the following characteristics: based on the basic requirements and needs of public health in China, the undergraduate public health/preventive medicine program curriculum has been integrated and reformed. In the new program, some courses in the original curriculum, such as maternal and child health and children and juvenile health were combined and integrated to form a new “Maternal, Child and Youth Health” course. The environmental health and occupational health courses were combined to form the “Environmental and Occupational Health” course.
New courses were created and added to the curriculum based on the development of new disciplines, including such courses as “Introduction to Public Health” and “Evidence-based Public Health Practice.” Education in the humanities, management, and research practice were strengthened. The “three-phases” curriculum format was changed into five components in the new curriculum program, including: “personality and literary,” “expression and understanding,” “development basis,” “profession and service,” and “research and inquiry.”
Implementation of a public health case and health project teaching method occurred in order to improve the student’s ability to self-learn. The traditional classroom teaching methods including the use of a lecture style of teaching has significant shortcomings; however, for the foreseeable future, it will remain the major teaching methodology for public health teaching, especially as the basic learning theory. Classroom teaching is irreplaceable for the time being. In the reform of traditional classroom teaching methods, several new teaching methods are advocated: (1) research teaching methods; (2) the gradual development of the public health case teaching methodology; (3) a public health project teaching method (PH-PTM); and (4) other research teaching methods. The public health case teaching method has the following characteristics: (1) clearly enunciated teaching relevance; (2) concise cases with informative content; (3) appropriate questions and instruction; and (4) knowledge content involved in the case that students can easily obtain through a variety of means. The PH-PTM can be divided into five stages: (1) clarifying project tasks; (2) making plans; (3) implementing plans; (4) evaluating results; and (5) applying outcomes.
The quality management of practitioner training was strengthened, including changing assessment methodologies by mobilizing “teaching” and “learning” processes. In the process of evaluating student performance, the entire learning process became the focus of assessment: (1) using multiple testing methods such as presentations and case analyses instead of a single closed book examination; (2) changing the one-time final examination to several quizzes to encourage student learning throughout the semester; (3) developing additional non-standard examination questions to encourage creative thinking; (4) emphasizing teaching assessment and evaluation, especially student feedback; and (5) introducing a peer evaluation process in course teaching. Peers are required to communicate with lecturers after class and discuss certain topics, such as teaching content, teaching methods, and classroom management, in order to improve the teaching ability of faculty members.
Summary
In 2015, the Fifth Plenary Session of the 18th Central Committee Conference of China raised the concern of “Healthy China” to a national strategic level. In August 2016, the National Conference on Health developed the themes of putting the people’s health at the center of health policy development by concentrating on prevention as the driving force of health policy, utilizing both Chinese traditional and western-style medicine, considering health issues in the development of all public policies, and involving the public in the development of the new policies. The Health China 2030 Plan pointed out that the core of the healthy China strategy is a new policy based on good health and health practices. Talented public health practitioners are the key human health resource required to implement the “Healthy China” strategy and achieve the “prevention first” policy. The undergraduate education of public health/preventive medicine students is a key element in developing talented public health practitioners. By reviewing the history of public health/preventive medicine practitioner education in China, analyzing the current situation and difficulties in the public health/preventive medicine curriculum, and reviewing the practice and experience of curriculum reform in public health colleges, the requirements of a new era in the education of public health/preventive medicine practitioners in China has been presented.
Author Contributions
LZ drafted the paper under the supervision of XM. RW, JX, and CL provided data input and research assistance. QC and JH were responsible for translation and finial editing of the manuscript.
Conflict of Interest Statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
References
Cheng, G., Li, W., and Zhu, C. (2007). Discussion public health professional training. J. Res. Med. Educ. 6, 298–299.
He, Y. (2013). A preliminary study on graduation practice in preventive medicine. J. Educ. Forum 14, 213–214.
Jin, Y., Huang, S., and Zhao, H. (2010). Discussion of preventive medicine undergraduate education reform from the social demand perspective. J. China Off Campus Educ. 4, 32.
Department of Higher Education, Ministry of Education of P. R. China. (1998). Directory of Undergraduate Education and Introduction. Beijing: Higher Education Press, 12.
Wang, S., Xiao, H., Somg, L., Xu, J., and Wang, X. (2001). Reform and practice in public health professional education. Jiangsu J. Prev. Med. 12, 77–79.
Wang, S., Zhang, W., and Du, Y. (2012). Evaluation of the undergraduate preventive medicine major and association analysis. Chin J. Med. Educ. 32, 44–46.
Ministry of Higher Education of P. R. China. (1963). No. 3411 Education Office File (63). Ministry of Education. China.
Ministry of Education of P. R. China. (1987). College Professional Directory. Higher Education Section Two No. 015 File (87).
Ministry of Higher Education of P. R. China. (1993). College Professional Directory (New Ed.). Higher Education Section Two No. 13 File.
Chinese Preventive Medicine Association of Public Health Education Branch and the Public Health Dean/Department Director Contact Conference. (2006). Public Health Education Basic Requirements. Vol. 7, 1–4.
Yuan, L., Wang, J., Xiao, D., and Lei, Y. (2012). Research on the settings of preventive medicine major and the mechanism of public health professional training in China. J. China Higher Med. Educ. 10, 44–45.
Keywords: preventive medicine, undergraduate public health education, professional public health training, public health education, preventive medicine education
Citation: Zhao L, Wang R, Xin J, Chen Q, Li C, Holsinger JW Jr. and Ma X (2017) Analysis of the Preventive Medicine Undergraduate Curriculum in China: The West China School of Public Heath Experience: A Case Study. Front. Educ. 2:28. doi: 10.3389/feduc.2017.00028
Received: 31 March 2017; Accepted: 09 June 2017;
Published: 10 July 2017
Edited by:
John R. Finnegan, University of Minnesota, United StatesReviewed by:
Donna Jeanne Petersen, University of South Florida, United StatesPradeep Nair, Central University of Himachal Pradesh, India
Copyright: © 2017 Zhao, Wang, Xin, Chen, Li, Holsinger and Ma. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) or licensor are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: James W. Holsinger Jr., andoQGVtYWlsLnVreS5lZHU=