 Tomasz Bednarczuk1*†
Tomasz Bednarczuk1*† Aleksandra Sugier1*†
Aleksandra Sugier1*† Roberto Attanasio2†
Roberto Attanasio2† Endre V. Nagy3†
Endre V. Nagy3† Roberto Negro4†
Roberto Negro4† Enrico Papini5†
Enrico Papini5† Miloš Žarković6†
Miloš Žarković6† Ersin Akarsu7†
Ersin Akarsu7† Maria Alevizaki8†Göksun Ayvaz9†Biljana Nedeljković Beleslin6†Eszter Berta3†
Maria Alevizaki8†Göksun Ayvaz9†Biljana Nedeljković Beleslin6†Eszter Berta3† Miklos Bodor3†
Miklos Bodor3† Anna M. Borissova10†
Anna M. Borissova10† Mihail Boyanov11,12†Camille Buffet13†Maria-Cristina Burlacu14†Chagit A. Cohen15Jasmina Ćirić6†
Mihail Boyanov11,12†Camille Buffet13†Maria-Cristina Burlacu14†Chagit A. Cohen15Jasmina Ćirić6† Juan J. Díez16,17,18†Harald Dobnig19†Valentin Fadeyev20†Benjamin C. T. Field21†
Juan J. Díez16,17,18†Harald Dobnig19†Valentin Fadeyev20†Benjamin C. T. Field21† Eric Fliers22†Dagmar Führer-Sakel23†Jacob S. Frølich24
Eric Fliers22†Dagmar Führer-Sakel23†Jacob S. Frølich24 Juan C. Galofré25,26†
Juan C. Galofré25,26† Tommi Hakala27†Jan Jiskra28†
Tommi Hakala27†Jan Jiskra28† Peter A. Kopp29†
Peter A. Kopp29† Michael Krebs30†
Michael Krebs30† Michal Kršek28†Martin Kužma31†
Michal Kršek28†Martin Kužma31† Ivica Lazúrová32†Laurence Leenhardt13†
Ivica Lazúrová32†Laurence Leenhardt13† Stephen Ludgate33,34†Vitaliy Luchytskiy35†Anne McGowan33,34†
Stephen Ludgate33,34†Vitaliy Luchytskiy35†Anne McGowan33,34† Miguel Melo36†
Miguel Melo36† Saara Metso27†Carla Moran37,38,39†
Saara Metso27†Carla Moran37,38,39† Tatyana Morgunova20†
Tatyana Morgunova20† Dan A. Niculescu40†
Dan A. Niculescu40† Božidar Perić41†
Božidar Perić41† Tereza Planck42†
Tereza Planck42† Catalina Poiana40†Francisca M. Puga43†
Catalina Poiana40†Francisca M. Puga43† Eyal Robenshtok44†Patrick Rosselet45†
Eyal Robenshtok44†Patrick Rosselet45† Marek Ruchala46†
Marek Ruchala46† Kamilla R. Riis24†
Kamilla R. Riis24† Alla Shepelkevich47†Mykola D. Tronko48†
Alla Shepelkevich47†Mykola D. Tronko48† David Unuane49†Irfan Vardarli50,51†
David Unuane49†Irfan Vardarli50,51† W. Edward Visser52†Andromachi Vryonidou53†
W. Edward Visser52†Andromachi Vryonidou53† Younes Ramazan Younes54†Elena Yurenya55Petros Perros56†
Younes Ramazan Younes54†Elena Yurenya55Petros Perros56† Laszlo Hegedüs24†
Laszlo Hegedüs24†- 1Department of Internal Medicine and Endocrinology, Medical University of Warsaw, Warsaw, Poland
- 2Scientific Committee Associazione Medici Endocrinologi, Udine, Italy
- 3Division of Endocrinology, Department of Medicine, Faculty of Medicine, University of Debrecen, Debrecen, Hungary
- 4Department of Experimental Medicine, University of Salento and Division of Endocrinology V. Fazzi Hospital, Lecce, Italy
- 5Department of Endocrinology and Metabolism, Regina Apostolorum Hospital, Lifenet Health Group, Albano Laziale, Rome, Italy
- 6Faculty of Medicine, University of Belgrade, Belgrade, Serbia
- 7Department of Internal Medicine, Division of Endocrinology, Faculty of Medicine, Gaziantep University, Gaziantep, Türkiye
- 8Endocrine Unit and Diabetes Centre, Department of Clinical Therapeutics, Alexandra Hospital, School of Medicine, National and Kapodistrian University of Athens, Athens, Greece
- 9Department of Endocrinology and Metabolism, Koru Ankara Hospital, Ankara, Türkiye
- 10Clinic of Endocrinology and Metabolism, University Hospital “Sofiamed”, Medical Faculty, Sofia University “Saint Kliment Ohridski”, Sofia, Bulgaria
- 11Clinic of Endocrinology and Metabolism, University Hospital “Alexandrovska”, Sofia, Bulgaria
- 12Department of Internal Medicine, Medical University, Sofia, Bulgaria
- 13Sorbonne Universitè, GRC n 16, GRC Thyroid Tumors, Thyroid Diseases and Endocrine Tumor Department, AP-HP, Hôpital Pitié-Salpêtriére, Paris, France
- 14Department of Endocrinology and Nutrition, Cliniques Universitaires St-Luc, Université Catholique de Louvain, Brussels, Belgium
- 15Rabin Medical Center, Tel-Aviv University, Tel-Aviv, Israel
- 16Department of Endocrinology, Hospital Universitario Puerta de Hierro Majadahonda, Madrid, Spain
- 17Instituto de Investigación Sanitaria Puerta de Hierro Segovia de Arana, Madrid, Spain
- 18Department of Medicine, Universidad Autónoma de Madrid, Madrid, Spain
- 19Thyroid Practice and Specialty Practice for Thyroid Radiofrequency Ablation, Kumberg, Austria
- 20Department of Endocrinology No. 1, N.V. Sklifosovsky Institute of Clinical Medicine, I.M. Sechenov First Moscow State Medical University, Moscow, Russia
- 21Section of Clinical Medicine, Faculty of Health and Medical Sciences, University of Surrey, Guildford, United Kingdom
- 22Department of Endocrinology and Metabolism, Amsterdam UMC, University of Amsterdam, Amsterdam, Netherlands
- 23Department of Endocrinology, Diabetes and Metabolism, University Hospital Essen, University of Amsterdam, Essen, Germany
- 24Department of Endocrinology, Odense University Hospital, Odense, Denmark
- 25Department of Endocrinology, Clínica Universidad de Navarra, Pamplona, Spain
- 26Instituto de Investigación Sanitaria de Navarra, Pamplona, Spain
- 27Department of Surgery, Tampere University Hospital, Tampere, Finland
- 283rd Department of Medicine, 1st Faculty of Medicine, Charles University, General University Hospital, Prague, Czechia
- 29Division of Endocrinology, Diabetology and Metabolism, University of Lausanne, Lausanne, Switzerland
- 30Internal Medicine III, Division of Endocrinology, Medical University of Vienna, Vienna, Austria
- 315th Department of Internal Medicine, Medical Faculty of Comenius University and University Hospital, Bratislava, Slovakia
- 32P. J. Šafárik University Košice, 1st Department of Internal Medicine of the Medical Faculty, Košice, Slovakia
- 33The School of Medicine, Trinity College Dublin, The University of Dublin, Dublin, Ireland
- 34Robert Graves Institute, Tallaght University Hospital, Dublin, Ireland
- 35Department of Reproductive Endocrinology, Institute of Endocrinology and Metabolism named after V.P. Komissarenko, National Academy of Medical Science of Ukraine, Kyiv, Ukraine
- 36Department of Endocrinology, Diabetes and Metabolism Coimbra Local Health Unit, Medical Faculty, University of Coimbra, Coimbra, Portugal
- 37Diabetes and Endocrinology Section, Beacon Hospital, Dublin, Ireland
- 38School of Medicine, University College Dublin, Dublin, Ireland
- 39Endocrine Department, St Vincent’s University Hospital, Dublin, Ireland
- 40Department of Endocrinology, Carol Davila University of Medicine and Pharmacy, Bucharest, Romania
- 41Department of Endocrinology, Diabetes and Metabolic Diseases “Mladen Sekso”, University Hospital Center “Sisters of Mercy”, Zagreb, Croatia
- 42Department of Endocrinology, Skåne University Hospital, Malmö, Sweden
- 43Serviço de Endocrinologia, Diabetes e Metabolismo, ULS São João, Porto, Portugal
- 44Endocrinology Institute, Rabin Medical Center, Gray Faculty of Medicine, Tel Aviv University, Tel-Aviv, Israel
- 45Cabinet Médical 2, Rue Bellefontaine, Lausanne, Switzerland
- 46Department of Endocrinology, Metabolism and Internal Medicine, Poznan University of Medical Sciences, Poznan, Poland
- 47Department of Endocrinology, Belarusian State Medical University, Minsk, Belarus
- 48V. P. Komissarenko Institute of Endocrinology and Metabolism, National Academy of Medical Science of Ukraine, Kyiv, Ukraine
- 49Department of Internal Medicine, Endocrine Unit, UZ Brussel, Vrije Universiteit Brussel, Brussels, Belgium
- 50Department of Medicine I, Klinikum Vest GmbH Knappschaftskrankenhaus Recklinghausen, Academic Hospital, Ruhr-University Bochum, Recklinghausen, Germany
- 515th Medical Department, Division of Endocrinology and Diabetes, Medical Faculty Mannheim, Heidelberg University, Mannheim, Germany
- 52Rotterdam Thyroid Center, Department of Internal Medicine, Erasmus MC, Rotterdam, Netherlands
- 53Department of Endocrinology and Diabetes Centre, Hellenic Red Cross Hospital, Athens, Greece
- 54East Surrey Hospital, Surrey and Sussex Healthcare NHS Trust, Redhill, United Kingdom
- 55Minsk Endocrinology Medical Center, Minsk, Belarus
- 56Translational and Clinical Research Institute, Newcastle University, Newcastle upon Tyne, United Kingdom
Background: Managing patients with fatigue is a clinical challenge. Because fatigue is often reported in hypothyroidism, thyroid hormone (TH) therapy may sometimes be incorrectly considered for biochemically euthyroid individuals. This study aimed to evaluate the prevalence and determinants of this practice in different European countries.
Methods: We analyzed aggregate data from the THESIS (Treatment of Hypothyroidism in Europe by Specialists: an International Survey) online survey. We analyzed responses from 5,695 members of 28 national endocrine/thyroid societies’ specialists to the statement: “Thyroid hormones may be indicated in biochemically euthyroid patients with unexplained fatigue”.
Results: Overall, 7.5% (426/5695) of respondents indicated that TH therapy might be considered for euthyroid patients with unexplained fatigue. The proportion of positive responses varied widely across different countries (between 1.1% in Switzerland and 29.3% in Serbia; p=2 ×10-16) and regions (between 4.7% in Western Europe and 8.7% in Western Asia or 8.8% in Eastern Europe; p=0.004). TH were more frequently prescribed for unexplained fatigue by male respondents (Odds Ratio, OR 1.45, 95% CI 1.18-1.78) and physicians practicing in private practice (OR 1.27, 95% CI 1.02-1.58), and less frequently by endocrinologists (OR 0.62, 95% CI 0.46-0.83).
Conclusion: A small, yet not negligible percentage of European thyroid-focused physicians consider using TH for euthyroid patients with unexplained fatigue, with significant variations based on geographic, demographic, and practice-related factors. Using levothyroxine and/or liothyronine in such cases lacks evidence and may partially contribute to the concerning overuse of TH therapy.
1 Introduction
Fatigue is among the most frequently reported symptoms of overt hypothyroidism, potentially causing significant impairment in daily activities and severely impacting patients’ quality of life (QoL) (1–4). Fatigue is reported across all age groups in hypothyroid patients, with a prevalence reaching 95% in individuals under 50 years old and its severity correlates with the decrease in serum thyroxine (T4) levels (5, 6). Although thyroid hormones play a pivotal role in maintaining neuronal integrity and function in the adult brain, the pathophysiology underlying hypothyroidism-related fatigue remains largely unknown (7, 8). It is speculated that: (i) fatigue results from a substantial decrease in the basal metabolic rate; (ii) TH exert a modulatory effect on the brain’s serotonergic system, (iii) general autoimmune/inflammatory mechanisms may contribute to fatigue, and (iv) fatigue may be associated with various comorbidities, including mental disorders, which are more prevalent among hypothyroid patients (9–16).
The association between fatigue and subclinical hypothyroidism remains controversial. Although fatigue is a predominant symptom in subclinical hypothyroidism, its prevalence does not differ significantly from euthyroid individuals and is strongly associated with concomitant diseases (17). Furthermore, several randomized controlled trials indicate that levothyroxine (LT4) treatment for subclinical hypothyroidism in adults does not improve general QoL or alleviate thyroid-related symptoms, including fatigue (18). Therefore, the treatment of subclinical hypothyroidism with TH warrants careful consideration, especially in those individuals with mild elevations of thyroid-stimulating hormone (TSH).
A recent and concerning trend is the lowering of the TSH threshold for initiating thyroid hormone therapy, with as many as 20-30% of patients started on LT4 despite having normal TSH levels (19). One reason behind the tendency to treat euthyroid individuals is the mistaken belief that symptoms commonly linked to hypothyroidism are more dependable for diagnosis than thyroid function tests (20–24). Therefore, exploring the influence of patient-reported fatigue on physicians’ decisions to prescribe TH may be important in understanding the escalating overuse of LT4. The aim of this survey was to explore the impact of patient-reported unexplained fatigue on thyroid specialists’ decisions regarding the prescription of TH.
2 Materials and methods
2.1 Design
The study is a part of an aggregate data analysis from all national THESIS surveys (Treatment of Hypothyroidism in Europe by Specialists: an International Survey). The THESIS study design and survey details have been previously described in detail (25–29). The project was supervised by a Steering Committee (LH, EVN, EP, PP, RA, RN). Briefly, 26 European countries, each with a population over 4 million, a national endocrine or thyroid professional society, and a national medical journal, participated in the project. Additionally, two Western Asian countries, Turkey and Israel, were included. Participating countries were grouped by geographic region according to the United Nations Statistics Division definition (https://data.un.org/en/index.html): Western Europe (Austria, Belgium, France, Germany, Netherlands, Switzerland), Northern Europe (Denmark, Finland, Ireland, Sweden, United Kingdom), Southern Europe (Croatia, Greece, Italy, Portugal, Serbia, Spain), Eastern Europe (Belarus, Bulgaria, Czech Republic, Hungary, Poland, Romania, Russia, Slovakia, Ukraine), and Western Asia (Israel, Turkey).
The survey targeted practicing specialists, who were members of their respective national endocrine/thyroid societies and managed patients with hypothyroidism. Participants anonymously answered 8 questions regarding their demographics and 23 questions or statements concerning the use of TH in diverse clinical scenarios. The relevant statement regarding fatigue was: “Thyroid hormones may be indicated in biochemically euthyroid patients with unexplained fatigue”. Respondents were asked to select either “yes” or “no.” To further characterize respondents endorsing TH use in euthyroid patients with unexplained fatigue, an additional survey question was re-analyzed regarding potential causes of persistent symptoms in LT4-treated hypothyroid patients achieving normal serum TSH. Respondents expressed their opinion (strongly disagree/disagree/neutral/agree/strongly agree) about potential causes: (i) inability of levothyroxine to restore normal physiology, (ii) psychosocial factors, (iii) comorbidities, (iv) chronic fatigue syndrome, (v) unrealistic patient expectations, (vi) underlying inflammation due to autoimmunity, (vii) burden of chronic disease, and (viii) burden of medication adherence.
2.2 Statistics
Data analysis was performed using ‘R’ software. Survey results were not weighted. Categorical (qualitative) variables were presented as frequencies and percentages, while quantitative variables were presented as mean and standard deviation or median and range. Associations between categorical variables were evaluated using Pearson’s chi-square test. Cramer’s V test was used to determine effect size, independent of sample size and p-value. Cramer’s V (ϕc) values were interpreted according to Rea and Parker: <0.1 (negligible), 0.1-0.2 (weak), 0.2-0.4 (moderate), 0.4-0.6 (relatively strong) and >0.6 (strong association). Multivariate analysis was conducted using logistic regression. Statistical significance was set at p <0.05.
3 Results
3.1 Baseline characteristics of respondents
Respondent characteristics have been previously described in detail (29). Briefly, survey invitations were distributed to 17,232 members of national thyroid or endocrine societies, with 5695 (33.0%) physicians completing the survey. The majority of respondents were specialists in endocrinology (5132/5695, 90.1%), aged over 40 years (4038/5695, 70.9%), with over 10 years of clinical practice (4487/5693, 78.8%). Most respondents managed more than 100 hypothyroid patients per year (3526/5677, 62.1%), whereas only 2.8% (158/5677) infrequently treated such patients (less than 10 patients per year). Females comprised 65% (3700/5695) of physicians (Table 1).
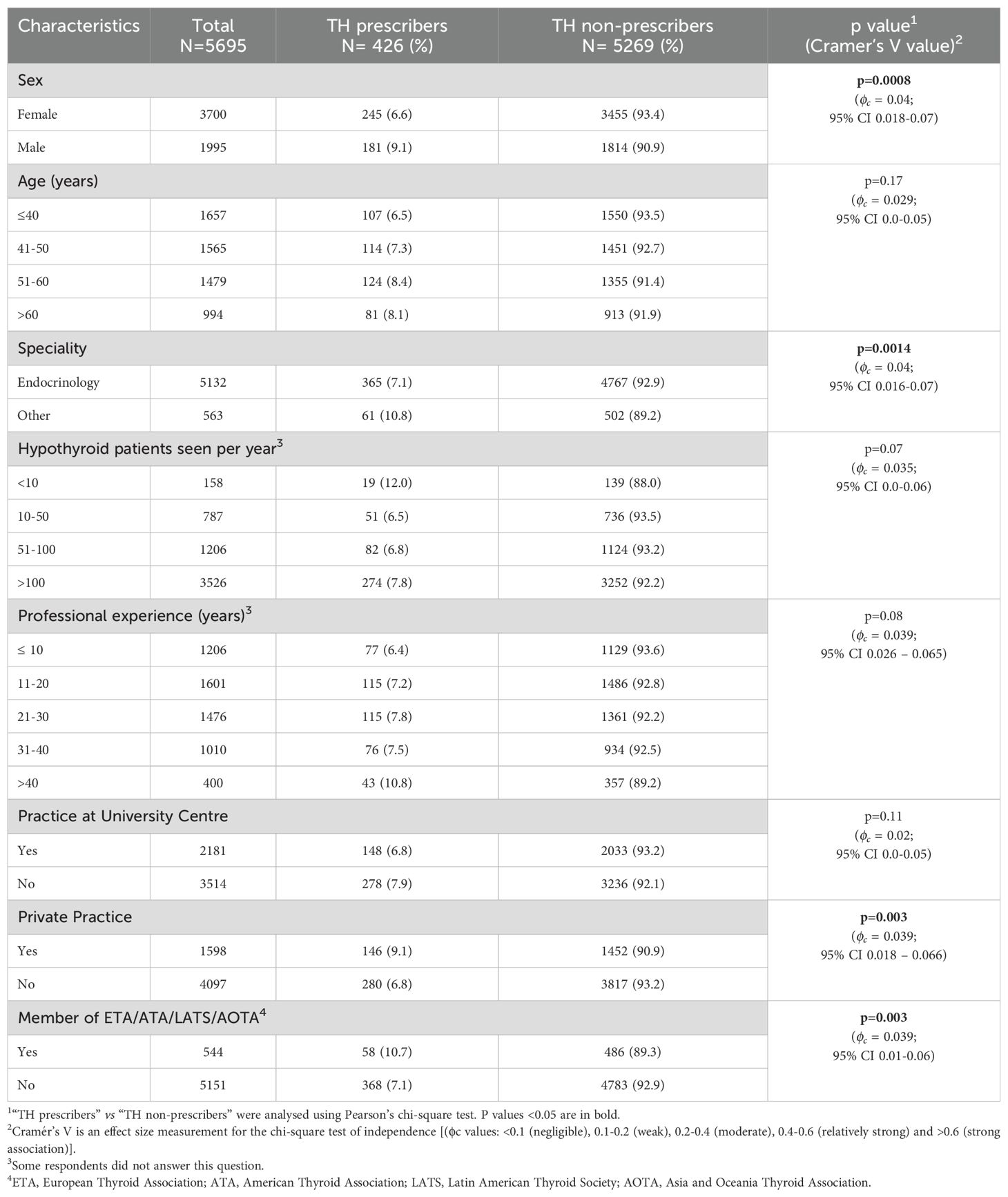
Table 1. Characteristics of respondents.
3.2 Univariate analysis: characteristics of respondents who considered the use of TH in unexplained fatigue
Of all respondents, 7.5% (426/5695) indicated that TH use may be considered in biochemically euthyroid patients with unexplained fatigue. The likelihood of prescribing TH for unexplained fatigue was significantly higher among respondents who were: (i) male compared to female (9.1% vs. 6.6%, p=0.0008, Cramer’s V 0.04, 95% CI: 0.018-0.07), (ii) non-endocrinologists compared to endocrinologists (10.8% vs. 7.1%, p=0.001, Cramer’s V 0.04, 95% CI: 0.016-0.07), (iii) members of international thyroid associations compared to non-members (10.7% vs. 7.1%, p=0.003, Cramer’s V 0.04, 95% CI: 0.016-0.06) and (iv) specialists working in private practice compared to specialists in public or academic service (9.1% vs. 6.8%, p=0.003, Cramer’s V 0.04, 95% CI: 0.019- 0.07). Respondents who infrequently managed hypothyroid patients showed a trend towards affirmative responses, although this difference did not reach statistical significance (Table 1).
The proportion of physicians considering the use of TH in unexplained fatigue varied significantly among geographic regions and countries (p=0.004, Cramer V 0.05, 95% CI: 0.02-0.07, and p=2×10-16, Cramer V 0.16, 95% CI: 0.12–0.18, respectively). The lowest percentage of affirmative responses were observed in Western Europe (44/938, 4.7%), while the highest percentages were in Western Asia (27/312, 8.7%) and Eastern Europe (147/1679, 8.8%) (Table 2). Fewer than 5% of respondents in Switzerland (1.1%), France (2.8%), Spain (4.1%), Portugal (4.6%), Russia (4.6%), and Italy (4.7%) indicated that TH might be appropriate for unexplained fatigue. Conversely, over 10% of respondents in Ukraine (10.3%), Germany (11.2%), Finland (11.4%), Poland (12.0%), Greece (12.7%), and Serbia (29.3%) considered TH for this indication (Table 2, Figure 1).
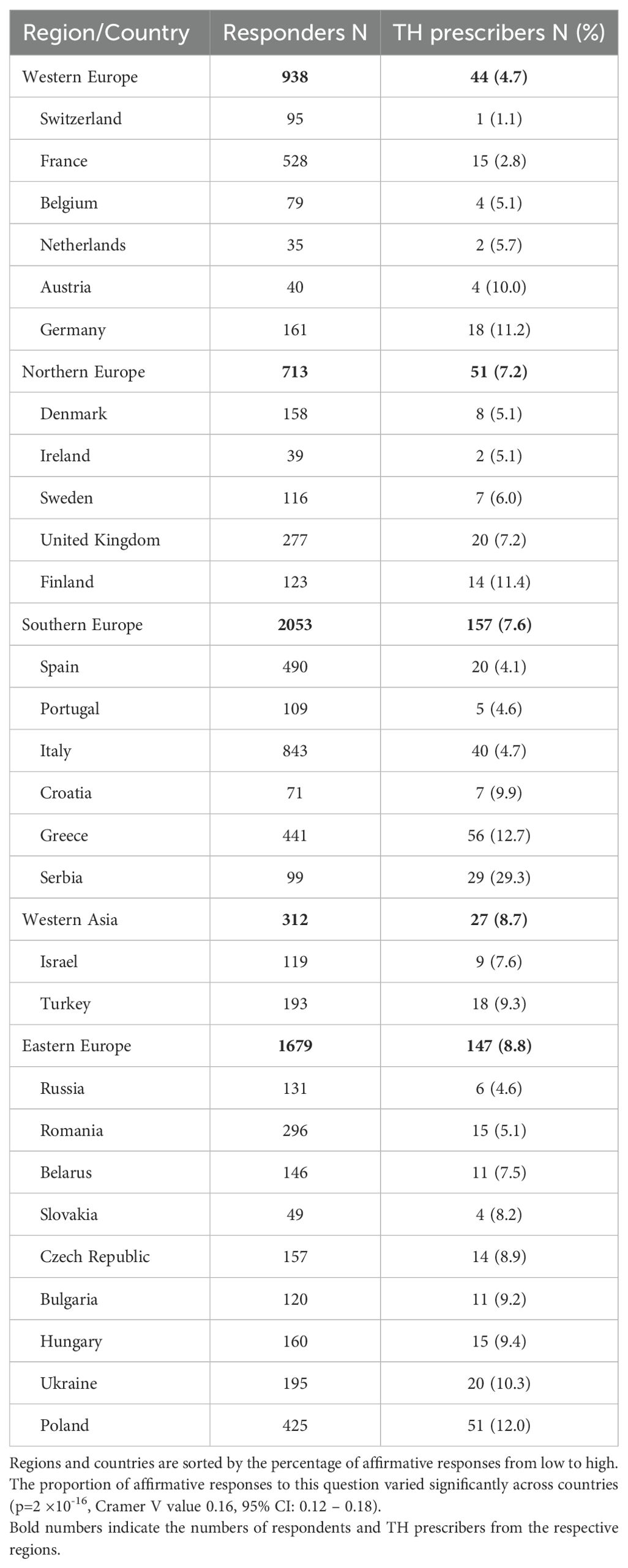
Table 2. Number of responders who considered the use of thyroid hormones (TH) in euthyroid patients with unexplained fatigue by region and country.
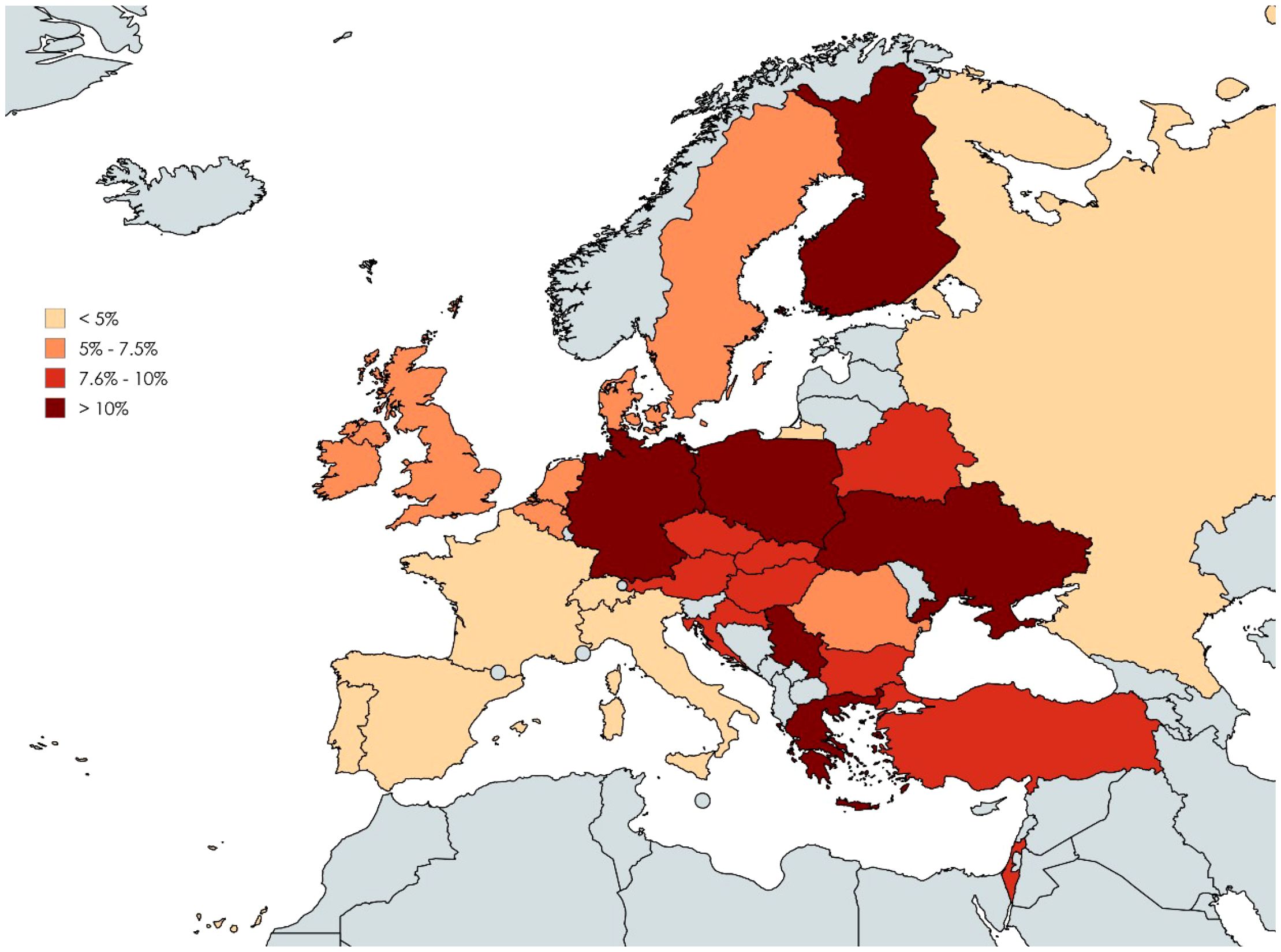
Figure 1. Proportion of respondents considering thyroid hormone (TH) use in biochemically euthyroid patients with unexplained fatigue by country. Color-coding corresponds to percentages of affirmative responses: <5%, 5% - 7.5%, 7.6% - 10% and >10%. Created with MapChart.
3.3 Multivariate analysis: characteristics of respondents who considered the use of TH in unexplained fatigue
Multivariate analysis confirmed positive associations between male gender (p=0.0004, OR: 1.45, 95% CI: 1.18-1.78), practicing in private clinics (p=0.03, OR: 1.27, CI: 1.02-1.58), and practicing outside Western Europe (p=0.006) with more frequent consideration of TH for unexplained fatigue in euthyroid patients. Endocrinologists were less inclined to prescribe TH for this indication than non-endocrinologists (p=0.001, OR: 0.62, 95% CI: 0.46-0.83) (Table 3).
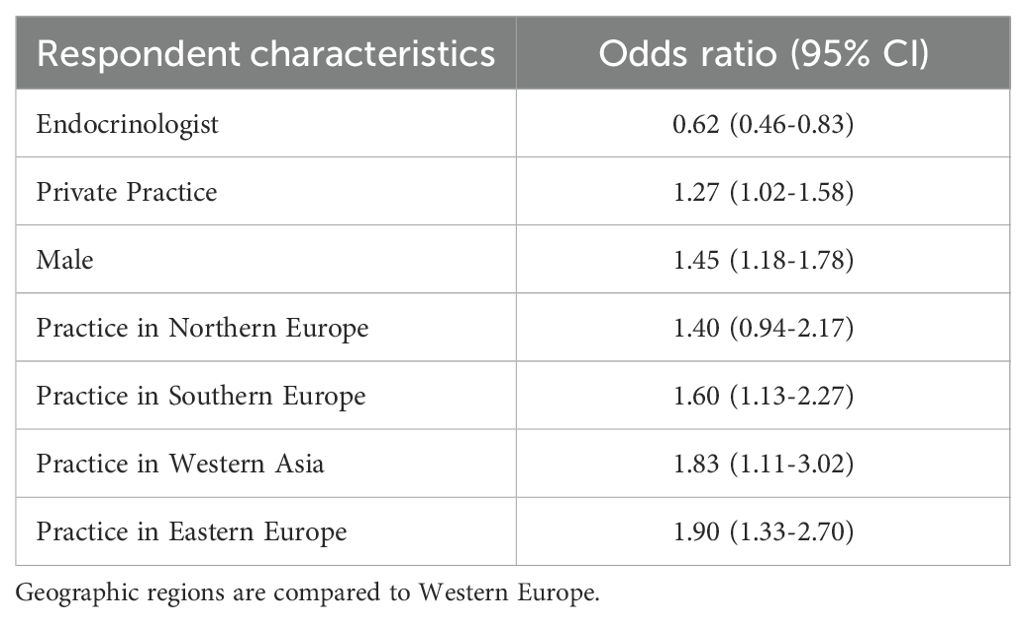
Table 3. Propensity to prescribe TH in biochemically euthyroid patients with unexplained fatigue (multivariate analysis).
3.4 Association between respondents’ view on TH indication for unexplained fatigue and their opinion on potential causes of persistent symptoms
Participants attributing persistent symptoms to the inability of LT4 to restore normal physiology or underlying autoimmune inflammation were significantly more likely to consider TH for euthyroid patients with unexplained fatigue (p<0.001; Cramer’s V 0.072, 95% CI: 0.045–0.103 and Cramer’s V 0.102, 95% CI: 0.074–0.133, respectively). Respondents attributing persistent symptoms to psychosocial factors were less likely to suggest TH therapy for unexplained fatigue (p<0.001, Cramer’s V 0.067, 95% CI: 0.04–0.098) (Figure 2; Supplementary Table S1).
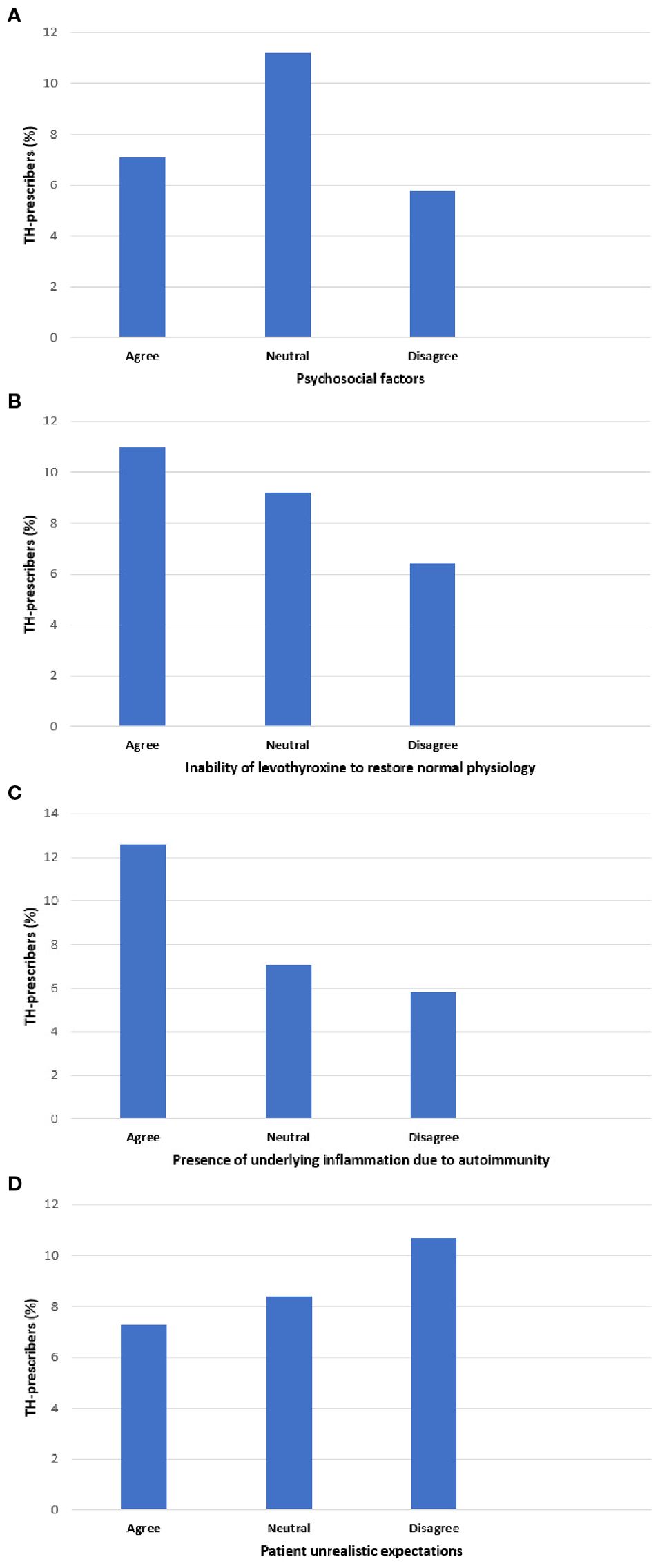
Figure 2. Association between respondent willingness to prescribe thyroid hormones (TH) for euthyroid patients with fatigue, and respondent perceptions about causes of persistent symptoms in hypothyroid patients treated with levothyroxine who have achieved serum TSH levels within the reference range. The horizontal axis shows respondent perceptions for possible causes (A–D) of persistent symptoms in hypothyroid patients treated with LT4 who achieve a normal TSH. For each cause (A–D), responses were grouped into three categories: “agree”, “neutral” or disagree. The vertical axis shows the percentage of respondents identified as TH-prescribers for unexplained fatigue. Pearson’s chi-square test: p<0.001.
4 Discussion
To our knowledge, this is the first survey investigating TH use for fatigue of unknown etiology in euthyroid patients. Respondents were predominantly experienced, thyroid-focused physicians from nearly all European countries. A key finding is that a small, yet not negligible percentage of respondents (7.5%) would consider prescribing TH for biochemically euthyroid patients with unexplained fatigue. Considering the high prevalence of fatigue in the general population, such inappropriate use of LT4 therapy may be one of the factors contributing to the escalating overuse of TH in euthyroid individuals (19).
Fatigue is a complex symptom that is reported by healthy individuals and patients with both acute and chronic diseases (30). An estimated 5% to 10% of primary care consultations pertain to fatigue and its highly non-specific nature presents a diagnostic and therapeutic challenge. A systematic review of 26 studies examining the causes of fatigue identified depression as the most frequent diagnosis (18.5%), while underlying somatic diseases (e.g., anemia, diabetes, hypothyroidism, malignancies) accounted for only 4.3% of cases. Myalgic encephalomyelitis/chronic fatigue syndrome was diagnosed in less than 2% of patients (31). Ultimately, an underlying etiology cannot be identified in approximately one-third of cases with fatigue, a situation referred to as medically not yet explained symptoms (MNYES). The management of these patients is a clinical challenge and may lead to inappropriate TH therapy (32–34).
Although the vast majority of respondents follow evidence-based recommendations, it is noteworthy that this survey found that approximately 1 out of 13 European thyroid specialists would consider prescribing TH to biochemically euthyroid patients with unexplained fatigue. Consistent with prior THESIS reports, this management approach exhibits significant variations across geographic regions and countries. Generally, TH use for fatigue was lowest in Western Europe, particularly Switzerland and France (less than 1 out of 30 respondents). Conversely, more than 1 out of 10 respondents in Ukraine, Germany, Finland, Poland, Greece, and Serbia may consider prescribing TH for unexplained fatigue (35–40). In comparison to most European countries, the use of TH in this setting was considered less frequently by specialists in Australia (3%, 2 out of 80), Latin America (2.5%, 2 out of 81), Canada (2.9%, 2 out of 68) and in Japan (2.9%, 6 out of 207) (41–44). The reasons for this discrepancy are at present unknown. It can be speculated that variations in clinical practices across countries or regions may arise from differences in guideline availability, healthcare systems structures, resource allocation and accessibility, patient advocacy, misinformation, training and education standards, as well as cultural influences (23).
Furthermore, the practice of considering TH therapy for fatigue was associated with physician gender (male), specialty (non-endocrinologist), and work setting (private practice). Since the questionnaire did not investigate the rationale for treating these patients, definitive explanations for the observed variations across respondent characteristics cannot be established (26–28, 45, 46). The differences in TH use observed between endocrinologists and non-endocrinologists may reflect greater awareness of the limitations and possible side effects of TH treatment. Further exploration of THESIS data yielded an interesting observation. Respondents’ views on potential causes of persistent symptoms in LT4 treated hypothyroid patients despite normal serum TSH have been previously described in detail (25). Briefly, respondents considered psychosocial factors the primary cause of persistent symptoms. Conversely, underlying inflammation due to autoimmunity and the inability of LT4 to restore normal physiology were considered the least important factors. Respondents attributing persistent symptoms to inability of LT4 to restore normal physiology or underlying autoimmune inflammation were significantly more likely to recommend TH for euthyroid patients with unexplained fatigue. These physicians might wrongly perceive symptoms commonly associated with hypothyroidism as more reliable diagnostic indicators than thyroid function tests. Attributing unexplained fatigue to “clinical hypothyroidism in biochemically euthyroid individuals” may lead to thinking traps and fallacies, including: misdiagnosis, false association, somatic fixation, premature attribution to chronic illness and ultimately in offering an ineffective treatment (47). A randomized double-blind placebo-controlled crossover trial of LT4 in euthyroid patients with symptoms of hypothyroidism demonstrated that TH are no more effective than placebo in improving psychological and physical well-being in such patients (48). Clinicians should instead consider MNYES and adopt a ‘two-track approach” to patient management by giving equal attention to both physical and psychosocial aspects, and, if needed, consulting other health professionals (21, 49, 50).
Several important limitations of this survey warrant discussion. The survey explored TH use for unexplained fatigue via a single statement, lacking any clinical context (e.g., fatigue duration, comorbidities, longitudinal TSH concentrations and anti-thyroid antibody levels). It remains speculative whether TH prescription for fatigue is more common in patients with increasing, “high-normal” TSH levels over time, or very high thyroid peroxidase antibodies levels (51). Although many associations in this study are highly significant, the low Cramer V-values (most often below 0.1) implies that other important drivers for considering TH for euthyroid patients with unexplained fatigue remain to be identified. The strength of this study lie in its large cohort of respondents who regularly manage hypothyroid patients across a wide range of settings (academic centers, public hospitals/clinics, and private practice) and represents nearly all eligible European countries with national endocrine or thyroid societies. Thus, this provides a novel insight into the (mis)use of LT4 and clinical practice in managing fatigue across Europe.
In conclusion, the use of TH in patients with unexplained fatigue may be one of the factors contributing to the escalating overuse of TH. If fatigue relief is the goal of TH treatment in euthyroid subjects, then this approach is likely to result in therapeutic failure, a delay in reaching an appropriate diagnosis and potential harm of overtreatment (including increased risk of cardiovascular morbidity and osteoporosis) (21, 52–54). The results of this study should prompt national endocrine and thyroid associations in countries where TH is frequently recommended for fatigue to validate these findings, explore the underlying drivers, and provide education on the appropriate use of LT4 therapy.
Data availability statement
The datasets presented in this article are not readily available because Data is the property of the THESIS sub-committee. Requests to access the datasets should be directed to TB, dG9tYXN6LmJlZG5hcmN6dWtAd3VtLmVkdS5wbA==.
Ethics statement
Ethical approval was not required for the study involving humans in accordance with the local legislation and institutional requirements. Written informed consent to participate in this study was not required from the participants or the participants’ legal guardians/next of kin in accordance with the national legislation and the institutional requirements.
Author contributions
TB: Methodology, Formal analysis, Writing – review & editing, Writing – original draft. ASu: Formal analysis, Writing – review & editing, Writing – original draft. RA: Writing – review & editing, Formal analysis, Methodology, Supervision. EN: Writing – review & editing, Supervision, Methodology, Conceptualization, Formal analysis. RN: Methodology, Supervision, Writing – review & editing, Formal analysis. EP: Formal analysis, Writing – review & editing, Conceptualization, Methodology, Supervision. MŽ: Writing – review & editing, Formal analysis, Methodology, Supervision. EA: Writing – review & editing. MA: Writing – review & editing. GA: Writing – review & editing. BN: Writing – review & editing. EB: Writing – review & editing. MkB: Writing – review & editing. AB: Writing – review & editing. MhB: Writing – review & editing. CB: Writing – review & editing. M-CB: Writing – review & editing. CC: Writing – review & editing. JĆ: Writing – review & editing. JD: Writing – review & editing. HD: Writing – review & editing. VF: Writing – review & editing. BF: Writing – review & editing. EF: Writing – review & editing. DF-S: Writing – review & editing. JF: Writing – review & editing. JG: Writing – review & editing. TH: Writing – review & editing. JJ: Writing – review & editing. PK: Writing – review & editing. MKr: Writing – review & editing. MKš: Writing – review & editing. MKu: Writing – review & editing. IL: Writing – review & editing. LL: Writing – review & editing. SL: Writing – review & editing. VL: Writing – review & editing. AM: Writing – review & editing. MM: Writing – review & editing. SM: Writing – review & editing. CM: Writing – review & editing. TM: Writing – review & editing. DN: Writing – review & editing. BP: Writing – review & editing. TP: Writing – review & editing. CP: Writing – review & editing. FP: Writing – review & editing. ER: Writing – review & editing. PR: Writing – review & editing. MR: Writing – review & editing. KR: Writing – review & editing. ASh: Writing – review & editing. MT: Writing – review & editing. DU: Writing – review & editing. IV: Writing – review & editing. WV: Writing – review & editing. AV: Writing – review & editing. YY: Writing – review & editing. EY: Writing – review & editing. PP: Formal analysis, Methodology, Writing – review & editing, Supervision, Conceptualization. LH: Writing – review & editing, Supervision, Formal analysis, Methodology, Conceptualization.
Funding
The author(s) declare that no financial support was received for the research, and/or publication of this article.
Acknowledgments
We gratefully thank the leadership of the 28 countries’ Endocrine Societies, as well as all the members generously answering the questionnaire.
Conflict of interest
LH, PP, EP, EN received consultancy fees from IBSA Biochimique SA. Author IV was employed by the company Klinikum Vest GmbH Knappschaftskrankenhaus Recklinghausen.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be perceived as a potential conflict of interest.
The author(s) declared that they were an editorial board member of Frontiers, at the time of submission. This had no impact on the peer review process and the final decision.
Generative AI statement
The author(s) declare that no Generative AI was used in the creation of this manuscript.
Any alternative text (alt text) provided alongside figures in this article has been generated by Frontiers with the support of artificial intelligence and reasonable efforts have been made to ensure accuracy, including review by the authors wherever possible. If you identify any issues, please contact us.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fendo.2025.1713814/full#supplementary-material
Supplementary Table 1 | Association between respondents’ view that thyroid hormones may be indicated in biochemically euthyroid subjects with unexplained fatigue (TH prescribers) and potential causes of persistent symptoms in LT4-treated patients with hypothyroidism who achieve normal serum TSH. 1 Not all respondents answered the question concerning the cause of persistence of hypothyroid symptoms despite normal serum TSH. 2 “TH prescribers” vs “TH non-prescribers” were analysed using Pearson’s chi-square test. P values <0.05 are in bold. Cramér’s V is an effect size measurement for the chi-square test of independence. 3 The causes of persistent symptoms are ranked from most to least important. 4 Answers agree/strongly agree and disagree/strongly disagree were analyzed together.
References
1. Hegedüs L, Bianco AC, Jonklaas J, Pearce SH, Weetman AP, and Perros P. Primary hypothyroidism and quality of life. Nat Rev Endocrinol. (2022) 18:230–42. doi: 10.1038/s41574-021-00625-8
2. Taylor PN, Medici MM, Hubalewska-Dydejczyk A, and Boelaert K. Hypothyroidism. Lancet. (2024) 404:1347–64. doi: 10.1016/S0140-6736(24)01614-3
3. Grixti L, Fisher H, Priestley J, McMullan C, Woollven A, Perros P, et al. Prevalence and severity of fatigue in treated hypothyroidism: results of a UK survey. Eur Thyroid J. (2025) 14:e250044. doi: 10.1530/ETJ-25-0044
4. Chaker L, Razvi S, Bensenor IM, Azizi F, Pearce EN, and Peeters RP. Hypothyroidism. Nat Rev Dis Primer. (2022) 8. doi: 10.1038/s41572-022-00357-7
5. Carlé A, Pedersen IB, Knudsen N, Perrild H, Ovesen L, Andersen S, et al. Hypothyroid symptoms fail to predict thyroid insufficiency in old people: A population-based case-control study. Am J Med. (2016) 129:1082–92. doi: 10.1016/j.amjmed.2016.06.013
6. Larsen CB, Winther KH, Cramon PK, Rasmussen ÅK, Feldt-Rasmussen U, Groenvold M, et al. Severity of hypothyroidism is inversely associated with impaired quality of life in patients referred to an endocrine clinic. Thyroid Res. (2023) 16:37. doi: 10.1186/s13044-023-00178-0
7. de Souza JS. Thyroid hormone biosynthesis and its role in brain development and maintenance. Adv Protein Chem Struct Biol. (2024) 142:329–65. doi: 10.1016/bs.apcsb.2023.12.024
8. Sinkó R, Salas-Lucia F, Mohácsik P, Halmos E, Wittmann G, Egri P, et al. Variable transduction of thyroid hormone signaling in structures of the mouse brain. Proc Natl Acad Sci U.S.A. (2025) 122:e2415970122. doi: 10.1073/pnas.2415970122
9. Bauer M, Heinz A, and Whybrow PC. Thyroid hormones, serotonin and mood: of synergy and significance in the adult brain. Mol Psychiatry. (2002) 7:140–56. doi: 10.1038/sj.mp.4000963
10. Louwerens M, Appelhof BC, Verloop H, Medici M, Peeters RP, Visser TJ, et al. Fatigue and fatigue-related symptoms in patients treated for different causes of hypothyroidism. Eur J Endocrinol. (2012) 167:809–15. doi: 10.1530/EJE-12-0501
11. Martin JV and Sarkar PK. Nongenomic roles of thyroid hormones and their derivatives in adult brain: are these compounds putative neurotransmitters? Front Endocrinol. (2023) 14:1210540. doi: 10.3389/fendo.2023.1210540
12. Raij T and Raij K. Association between fatigue, peripheral serotonin, and L-carnitine in hypothyroidism and in chronic fatigue syndrome. Front Endocrinol. (2024) 15:1358404. doi: 10.3389/fendo.2024.1358404
13. Finsterer J and Mahjoub SZ. Fatigue in healthy and diseased individuals. Am J Hosp Palliat Med. (2014) 31:562–75. doi: 10.1177/1049909113494748
14. Brenta G and Gottwald-Hostalek U. Comorbidities of hypothyroidism. Curr Med Res Opin. (2025) 41:421–9. doi: 10.1080/03007995.2025.2476075
15. Thvilum M, Brandt F, Almind D, Christensen K, Brix TH, and Hegedüs L. Increased psychiatric morbidity before and after the diagnosis of hypothyroidism: A nationwide register study. Thyroid. (2014) 24:802–8. doi: 10.1089/thy.2013.0555
16. Thvilum M, Brandt F, Almind D, Christensen K, Brix TH, and Hegedüs L. Type and Extent of Somatic Morbidity before and after the Diagnosis of Hypothyroidism. A Nationwide Register Study. PloS One. (2013) 8:e75789. doi: 10.1371/journal.pone.0075789
17. Carlé A, Karmisholt JS, Knudsen N, Perrild H, Thuesen BH, Ovesen L, et al. Does subclinical hypothyroidism add any symptoms? Evidence from a danish population-based study. Am J Med. (2021) 134:1115–1126.e1. doi: 10.1016/j.amjmed.2021.03.009
18. Feller M, Snel M, Moutzouri E, Bauer DC, De Montmollin M, Aujesky D, et al. Association of thyroid hormone therapy with quality of life and thyroid-related symptoms in patients with subclinical hypothyroidism: A systematic review and meta-analysis. JAMA. (2018) 320:1349. doi: 10.1001/jama.2018.13770
19. Brito JP, Ross JS, El Kawkgi OM, Maraka S, Deng Y, Shah ND, et al. Levothyroxine use in the United States, 2008-2018. JAMA Intern Med. (2021) 181:1402. doi: 10.1001/jamainternmed.2021.2686
20. Dzurec LC. Experiences of fatigue and depression before and after low-dose 1-thyroxine supplementation in essentially euthyroid individuals. Res Nurs Health. (1997) 20:389–98. doi: 10.1002/(sici)1098-240x(199710)20:5%3C389::aid-nur3%3E3.0.co;2-k
21. Hegedüs L, Nagy EV, Papini E, and Perros P. Limiting the use and misuse of liothyronine in hypothyroidism. Nat Rev Endocrinol. (2025) 21:3–4. doi: 10.1038/s41574-024-01055-y
22. Weetman AP. Thyroxine treatment in biochemically euthyroid but clinically hypothyroid individuals. Clin Endocrinol (Oxf). (2002) 57:25–7. doi: 10.1046/j.1365-2265.2002.01561.x
23. Perros P, Poots A, Nagy EV, Papini E, Hay H, Abad-Madroñero J, et al. Knowledge gaps about the diagnosis and treatment of hypothyroidism: an international patient survey. Front Endocrinol. (2025) 16:1663497. doi: 10.3389/fendo.2025.1663497
24. Laryea EA. Subclinical hypothyroidism. To treat or not to treat. Can Fam Physician Med Fam Can. (1993) 39:1997–8.
25. Attanasio R, Žarković M, Papini E, Nagy EV, Negro R, Perros P, et al. Patients’ persistent symptoms, clinician demographics and geo-economic factors are associated with choice of therapy for hypothyroidism by European thyroid specialists: The “THESIS”* collaboration (*Treatment of Hypothyroidism in Europe by Specialists, an International Survey). Thyroid. (2024) 34(4):429–441. doi: 10.1089/thy.2023.0580
26. Galofré JC, Díez JJ, Attanasio R, Nagy EV, Negro R, Papini E, et al. Treatment of obesity with thyroid hormones in europe. Data from the THESIS* Collaboration. J Endocrinol Invest. (2024) 48:201–12. doi: 10.1007/s40618-024-02409-z
27. Negro R, Žarković M, Attanasio R, Hegedüs L, Nagy EV, Papini E, et al. Use of levothyroxine for euthyroid, thyroid antibody positive women with infertility: Analyses of aggregate data from a survey of European thyroid specialists (Treatment of Hypothyroidism in Europe by Specialists: An International Survey). Clin Endocrinol (Oxf). (2024) 101:180–90. doi: 10.1111/cen.15099
28. Papini E, Attanasio R, Žarković M, Nagy EV, Negro R, Perros P, et al. Thyroid hormones for euthyroid patients with simple goiter growing over time: a survey of European thyroid specialists. Endocrine. (2024) 87:262–72. doi: 10.1007/s12020-024-04002-z
29. Žarković M, Attanasio R, Nagy EV, Negro R, Papini E, Perros P, et al. Characteristics of specialists treating hypothyroid patients: the “THESIS” collaborative. Front Endocrinol. (2023) 14:1225202. doi: 10.3389/fendo.2023.1225202
30. Dukes JC, Chakan M, Mills A, and Marcaurd M. Approach to fatigue. Med Clin North Am. (2021) 105:137–48. doi: 10.1016/j.mcna.2020.09.007
31. Stadje R, Dornieden K, Baum E, Becker A, Biroga T, Bösner S, et al. The differential diagnosis of tiredness: a systematic review. BMC Fam Pract. (2016) 17:147. doi: 10.1186/s12875-016-0545-5
32. Hegedüs L, van der Feltz-Cornelis CM, Papini E, Nagy EV, Weetman AP, and Perros P. Medically not yet explained symptoms in hypothyroidism. Nat Rev Endocrinol. (2024) 20:685–93. doi: 10.1038/s41574-024-01022-7
33. Perros P, van der Feltz-Cornelis C, Papini E, Nagy EV, Weetman AP, and Hegedüs L. The enigma of persistent symptoms in hypothyroid patients treated with levothyroxine: A narrative review. Clin Endocrinol (Oxf). (2023) 98:461–8. doi: 10.1111/cen.14473
34. Van Der Feltz-Cornelis CM, Sweetman J, Edwards M, Gall N, Gilligan J, Hayle S, et al. Identifying the top research priorities in medically not yet explained symptoms (MNYES): a James Lind Alliance priority setting partnership. BMJ Open. (2022) 12:e061263. doi: 10.1136/bmjopen-2022-061263
35. Bednarczuk T, Attanasio R, Hegedüs L, Nagy EV, Negro R, Papini E, et al. Use of thyroid hormones in hypothyroid and euthyroid patients: a THESIS* questionnaire survey of Polish physicians. *THESIS: Treatment of hypothyroidism in Europe by specialists: an international survey. Endokrynol Pol. (2021) 72:357–65. doi: 10.5603/EP.a2021.0048
36. Metso S, Hakala T, Attanasio R, Nagy E, Negro R, Papini E, et al. Use of thyroid hormones in the treatment of hypothyroidism: Thesis questionnaire survey for Finnish specialists. Finnish Med J. (2021) 48:2885–9.
37. Buffet C, Belin L, Attanasio R, Negro R, Hegedüs L, Nagy EV, et al. Real-life practice of thyroid hormone use in hypothyroid and euthyroid patients: A detailed view from the THESIS questionnaire survey in France. Ann Endocrinol. (2022) 83:27–34. doi: 10.1016/j.ando.2021.11.002
38. Paschou SA, Alevizaki M, Attanasio R, Hegedüs L, Nagy EV, Papini E, et al. Use of thyroid hormones in hypothyroid and euthyroid patients: a 2020 THESIS questionnaire survey of members of the Hellenic Endocrine Society. Hormones. (2022) 21:103–11. doi: 10.1007/s42000-021-00335-w
39. Nedeljkovic-Beleslin B, Attanasio R, Hegedüs L, Nagy E, Negro R, Papini E, et al. Use of thyroid hormones in hypothyroid and euthyroid patients: A THESIS questionnaire survey of Serbian physicians. Srp Arh Celok Lek. (2022) 150:667–74. doi: 10.2298/SARH211221110N
40. Vardarli I, Brandenburg T, Hegedüs L, Attanasio R, EndreV N, Papini E, et al. A questionnaire survey of german thyroidologists on the use of thyroid hormones in hypothyroid and euthyroid patients: the THESIS (Treatment of hypothyroidism in europe by specialists: an international survey) collaborative. Exp Clin Endocrinol Diabetes. (2022) 130:577–86. doi: 10.1055/a-1832-0644
41. Cassemiro JF, Ilera V, Batalles S, Reyes A, Nagy EV, Papini E, et al. Use of thyroid hormones in hypothyroid and euthyroid patients: a 2022 THESIS questionnaire survey of members of the Latin American Thyroid Society (LATS). Thyroid Res. (2023) 16:40. doi: 10.1186/s13044-023-00182-4
42. Lafontaine N, Brown SJ, Perros P, Papini E, Nagy EV, Attanasio R, et al. Use of thyroid hormones in hypothyroid and euthyroid patients: A survey of members of the Endocrine Society of Australia. Clin Endocrinol (Oxf). (2024) 100:477–85. doi: 10.1111/cen.15049
43. Liu A, Morrison D, Hegedüs L, Nagy EV, Papini E, Perros P, et al. Canadian endocrinologists′ Perspectives on treatment with thyroid hormone substitutions in euthyroid and hypothyroid patients: A 2023 THESIS questionnaire survey. Clin Endocrinol (Oxf). (2025) 103(5):739–748. doi: 10.1111/cen.70009
44. Nagayama Y, Tajiri J, Murakami T, Watanabe N, Sato S, Shindo H, et al. A questionnaire survey of thyroid specialists in Japan on the use of thyroid hormones in hypothyroid and euthyroid patients. Endocr J. (2025) 72(8):911–923. doi: 10.1507/endocrj.ej25-0106
45. Galofré JC, Díez JJ, Attanasio R, Nagy EV, Bednarczuk T, Papini E, et al. Thyroid hormone treatment for hypercholesterolemia in euthyroid patients: results from a european survey of thyroid specialists. Clin Endocrinol (Oxf). (2025) 103(5):749–756. doi: 10.1111/cen.70014
46. Ludgate S, McGowan A, Moran C, Attanasio R, Žarković M, Nagy EV, et al. The use of thyroid hormones in the treatment of euthyroid patients with treatment-resistant depression. Data from a survey of 5695 European national endocrine professional organization members. Front Endocrinol. (2025) 16:1665720. doi: 10.3389/fendo.2025.1665720
47. Maisel P, Baum E, and Donner-Banzhoff N. Fatigue as the chief complaint. Dtsch Ärztebl Int. (2021) 118(33-34):556–576. doi: 10.3238/arztebl.m2021.0192
48. Pollock MA, Sturrock A, Marshall K, Davidson KM, Kelly CJG, McMahon AD, et al. Thyroxine treatment in patients with symptoms of hypothyroidism but thyroid function tests within the reference range: randomised double blind placebo controlled crossover trial. BMJ. (2001) 323:891–5. doi: 10.1136/bmj.323.7318.891
49. Burton C, Mooney C, Sutton L, White D, Dawson J, Neilson AR, et al. Effectiveness of a symptom-clinic intervention delivered by general practitioners with an extended role for people with multiple and persistent physical symptoms in England: the Multiple Symptoms Study 3 pragmatic, multicentre, parallel-group, individually randomised controlled trial. Lancet. (2024) 403:2619–29. doi: 10.1016/S0140-6736(24)00700-1
50. Perros P, Nagy EV, Papini E, Abad-Madroñero J, Lakwijk P, Poots AJ, et al. Hypothyroidism and type D personality: results from E-MPATHY, a cross-sectional international online patient survey. J Clin Endocrinol Metab. (2024) 110:e97–e108. doi: 10.1210/clinem/dgae140
51. Guldvog I, Reitsma LC, Johnsen L, Lauzike A, Gibbs C, Carlsen E, et al. Thyroidectomy versus medical management for euthyroid patients with hashimoto disease and persisting symptoms: A randomized trial. Ann Intern Med. (2019) 170:453–64. doi: 10.7326/M18-0284
52. Abrahamsen B, Jørgensen HL, Laulund AS, Nybo M, Bauer DC, Brix TH, et al. The excess risk of major osteoporotic fractures in hypothyroidism is driven by cumulative hyperthyroid as opposed to hypothyroid time: an observational register-based time-resolved cohort analysis. J Bone Miner Res. (2015) 30:898–905. doi: 10.1002/jbmr.2416
53. Centanni M, Duntas L, Feldt-Rasmussen U, Koehrle J, Peeters RP, Razvi S, et al. ETA guidelines for the use of levothyroxine sodium preparations in monotherapy to optimize the treatment of hypothyroidism. Eur Thyroid J. (2025) 14(4):e250123. doi: 10.1530/etj-25-0123
Keywords: euthyroidism, fatigue, levothyroxine, thyroid hormone, survey
Citation: Bednarczuk T, Sugier A, Attanasio R, Nagy EV, Negro R, Papini E, Žarković M, Akarsu E, Alevizaki M, Ayvaz G, Nedeljković Beleslin B, Berta E, Bodor M, Borissova AM, Boyanov M, Buffet C, Burlacu M-C, Cohen CA, Ćirić J, Díez JJ, Dobnig H, Fadeyev V, Field BCT, Fliers E, Führer-Sakel D, Frølich JS, Galofré JC, Hakala T, Jiskra J, Kopp PA, Krebs M, Kršek M, Kužma M, Lazúrová I, Leenhardt L, Ludgate S, Luchytskiy V, McGowan A, Melo M, Metso S, Moran C, Morgunova T, Niculescu DA, Perić B, Planck T, Poiana C, Puga FM, Robenshtok E, Rosselet P, Ruchala M, Riis KR, Shepelkevich A, Tronko MD, Unuane D, Vardarli I, Visser WE, Vryonidou A, Younes YR, Yurenya E, Perros P and Hegedüs L (2025) Use of thyroid hormones in euthyroid patients with unexplained fatigue: analyses of aggregate data from European national surveys of professional endocrine society members. Front. Endocrinol. 16:1713814. doi: 10.3389/fendo.2025.1713814
Received: 26 September 2025; Accepted: 20 October 2025;
Published: 05 November 2025.
Edited by:
Francesco S. Celi, UCONN Health, United StatesReviewed by:
Giorgio Napolitano, University of Studies G. d’Annunzio Chieti and Pescara, ItalyAnupam Kotwal, University of Nebraska Medical Center, United States
Copyright © 2025 Bednarczuk, Sugier, Attanasio, Nagy, Negro, Papini, Žarković, Akarsu, Alevizaki, Ayvaz, Nedeljković Beleslin, Berta, Bodor, Borissova, Boyanov, Buffet, Burlacu, Cohen, Ćirić, Díez, Dobnig, Fadeyev, Field, Fliers, Führer-Sakel, Frølich, Galofré, Hakala, Jiskra, Kopp, Krebs, Kršek, Kužma, Lazúrová, Leenhardt, Ludgate, Luchytskiy, McGowan, Melo, Metso, Moran, Morgunova, Niculescu, Perić, Planck, Poiana, Puga, Robenshtok, Rosselet, Ruchala, Riis, Shepelkevich, Tronko, Unuane, Vardarli, Visser, Vryonidou, Younes, Yurenya, Perros and Hegedüs. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Tomasz Bednarczuk, dG9tYXN6LmJlZG5hcmN6dWtAd3VtLmVkdS5wbA==; Aleksandra Sugier, YWxla3NhbmRyYS5zdWdpZXJAdWNrd3VtLnBs
†ORCID: Tomasz Bednarczuk, orcid.org/0000-0002-5752-8709
Aleksandra Sugier, orcid.org/0009-0002-1317-1522
Roberto Attanasio, orcid.org/0000-0002-1417-287X
Endre V. Nagy, orcid.org/0000-0002-9286-6471
Roberto Negro, orcid.org/0000-0001-9282-4530
Enrico Papini, orcid.org/0000-0003-4790-2733
Miloš Žarković, orcid.org/0000-0001-9977-5970
Ersin Akarsu, orcid.org/0000-0003-2786-6616
Maria Alevizaki, orcid.org/0000-0003-3726-5793
Göksun Ayvaz, orcid.org/0000-0002-1213-6832
Biljana Nedeljković Beleslin, orcid.org/0000-0002-1687-9297
Eszter Berta, orcid.org/0000-0003-0439-9867
Miklos Bodor, orcid.org/0000-0002-0789-5156
Anna M. Borissova, orcid.org/0000-0003-0553-408X
Mihail Boyanov, orcid.org/0000-0002-5695-2831
Camille Buffet, orcid.org/0000-0003-1389-4157
Maria-Cristina Burlacu, orcid.org/0000-0002-8437-3933
Jasmina Ćirić, orcid.org/0000-0001-6960-9699
Juan J. Díez, orcid.org/0000-0002-2017-0694
Harald Dobnig, orcid.org/0000-0001-7574-9292
Valentin Fadeyev, orcid.org/0000-0002-3026-6315
Benjamin C. T. Field, orcid.org/0000-0002-1883-1588
Eric Fliers, orcid.org/0000-0001-8048-9050
Dagmar Führer-Sakel, orcid.org/0000-0003-0357-4192
Juan C. Galofré, orcid.org/0000-0003-0227-3566
Tommi Hakala, orcid.org/0000-0002-9373-4462
Jan Jiskra, orcid.org/0000-0003-0920-4854
Peter A. Kopp, orcid.org/0000-0001-5980-0529
Michael Krebs, orcid.org/0000-0002-9265-7274
Michal Kršek, orcid.org/0000-0002-5941-3489
Martin Kužma, orcid.org/0000-0002-1294-1217
Ivica Lazúrová, orcid.org/0000-0002-3163-1097
Laurence Leenhardt, orcid.org/0000-0003-4131-6813
Stephen Ludgate, orcid.org/0000-0002-9597-9471
Vitaliy Luchytskiy, orcid.org/0000-0002-3515-3264
Anne McGowan, orcid.org/0000-0003-4222-622X
Miguel Melo, orcid.org/0000-0002-8365-1380
Saara Metso, orcid.org/0000-0001-8197-7603
Carla Moran, orcid.org/0000-0002-7318-7166
Tatyana Morgunova, orcid.org/0000-0003-1500-1586
Dan A. Niculescu, orcid.org/0000-0002-6439-3523
Božidar Perić, orcid.org/0000-0001-9998-4895
Tereza Planck, orcid.org/0000-0003-1398-5067
Catalina Poiana, orcid.org/0000-0002-5795-3318
Francisca M. Puga, orcid.org/0000-0002-9510-419X
Eyal Robenshtok, orcid.org/0000-0002-6268-4212
Patrick Rosselet, orcid.org/0009-0004-3793-8163
Marek Ruchala, orcid.org/0000-0002-6296-7220
Kamilla R. Riis, orcid.org/0000-0003-2679-7153
Alla Shepelkevich, orcid.org/0000-0002-8213-2968
Mykola D. Tronko, orcid.org/0000-0001-7421-0981
David Unuane, orcid.org/0000-0002-8488-1735
Irfan Vardarli, orcid.org/0009-0009-2554-0971
W. Edward Visser, orcid.org/0000-0002-5248-863X
Andromachi Vryonidou, orcid.org/0000-0002-0544-5952
Younes Ramazan Younes, orcid.org/0000-0003-0929-1003
Petros Perros, orcid.org/0000-0001-7320-5574
Laszlo Hegedüs, orcid.org/0000-0002-9691-7619