 Blanka Šebánková
Blanka Šebánková Jaroslav Flegr
Jaroslav Flegr- 1Division of Biology, Faculty of Science, Charles University in Prague, Prague, Czechia
- 2National Institute of Mental Health, Klecany, Czechia
Latent toxoplasmosis is known to be associated with specific changes in animal and human behavior and human personality. Many toxoplasmosis-associated shifts, such as an extroversion-introversion shift or a trust-suspicion shift, go in opposite directions in men and women. The stress coping hypothesis suggests that such behavioral effects of toxoplasmosis are side effects of chronic stress caused by lifelong parasitosis and associated health disorders. Several studies have searched for, and typically found, indices of impaired health in infected subjects. However, subjects were always aware of their toxoplasmosis status, which could influence obtained data and cause false-positive results of the studies. Here we searched for differences in physical and mental health status among 39 Toxoplasma-infected and 40 Toxoplasma-free female university students who completed identical questionnaires (N-70, and anamnestic questionnaire), before and 3 years after they were informed of their toxoplasmosis status. Our results showed that infected women showed indices of poorer health status, not only after, but also before they were informed of their infection. In accordance with previously published data, these indices were more numerous and stronger in Rh-negative than in Rh-positive women. Present results suggest that observed indices of poorer health and symptoms of chronic stress in Toxoplasma-infected subjects are real. Due to its high (30%) prevalence, toxoplasmosis could represent an important factor for public health.
Introduction
The prevalence of toxoplasmosis in the human population varies between 5 to 80% in various countries, depending on temperature, humidity, hygienic standards and kitchen habits (Tenter et al., 2000; Pappas et al., 2009). It is decreasing in many European countries and in Northern America, however, it is mostly increasing in the most populous countries in Eastern Asia, like China. Toxoplasma gondii reproduces sexually in the intestinal cells of its definitive host (any feline species, including domestic cats) and asexually in bodies of intermediate hosts (all warm blooded animals, including humans). In infected immunocompetent humans, a short phase of acute toxoplasmosis, which is accompanied by many nonspecific clinical symptoms including high body temperature, headache, swollen lymphatic nodes and fatigue, spontaneously proceeds into a lifelong latent phase. Latent toxoplasmosis is characterized by the presence of anamnestic IgG anti-Toxoplasma antibodies in serum and slowly dividing bradyzoites in tissue cysts localized mainly in immunoprivileged organs such as the brain, eye, and testes. Latent toxoplasmosis is usually considered harmless for infected immunocompetent subjects. However, many observations—typically anecdotal—suggest that it increases the risk of various disorders, for recent review see (Flegr et al., 2014). Psychiatrists performed systematic studies of the clinical effects of toxoplasmosis. They showed that toxoplasmosis likely strongly increases the risk of schizophrenia, bipolar disorder, obsessive-compulsive disorder, as well as epilepsy and migraines. For reviews (see Flegr, 2015; Sutterland et al., 2015).
Latent toxoplasmosis is also known to be accompanied by many specific changes in behavior and personality of infected animal and human hosts. Toxoplasma is transmitted from an intermediate to a definitive host by predation. Therefore, the behavioral changes observed in infected animals, like that of humans, are usually considered to be a feature of the adaptive manipulation of the parasite, intended to increase the probability of transmission of the dormant stages of Toxoplasma from intermediate to definitive host by trophic route. However, based on the nature of observed changes, especially based on the fact that many Toxoplasma-associated changes are in opposite directions in men and women (Flegr, 2010), it has been suggested that they are just nonspecific side-effects of mild but continuous stress induced by the parasitic disease (Lindová et al., 2010). It is known that men and women behaviorally cope with chronic stress in opposite ways. Stressed women express increased extroversion; they are more likely to seek and provide social support (Stone and Neale, 1984; Rosario et al., 1988; Carver et al., 1989), join with others (Hobfoll et al., 1994), and verbalize toward others or the self (Tamres et al., 2002). In contrast, stressed men express decreased extroversion, and seem to use more individualistic and antisocial (e.g., aggressive, hostile) forms of coping (Carver et al., 1989; Hobfoll et al., 1994).
Several studies have tried to test the stress coping hypothesis by searching for indices of chronic stress in subjects with the latent form of Toxoplasma infection. For example, an ecological study performed in 2014 showed that the prevalence of toxoplasmosis in particular countries largely explains the variability in mortality and morbidity associated with many diseases and disorders (Flegr et al., 2014) between countries. Recently, a large cross-sectional study performed on a nonclinical cohort of 1,500 internet users showed that, after the correction for multiple tests, Toxoplasma-infected subjects, both men and women, scored more poorly in 28 of 29 monitored health-related variables than Toxoplasma-free subjects and reported a significantly higher incidence of 77 (57%), of a list of 134 disorders reported by at least 10 participants of the study; the other 55 disorders showed no differences or only non-significant trends (Flegr and Escudero, 2016). The main problem of the last study was that its participants self-reported their toxoplasmosis status and therefore knew whether or not they were infected. Therefore, it can be speculated that at least some of Toxoplasma-infected participants reported more health problems because of autosuggestion, as they believed that Toxoplasma could (or must) negatively influence their health.
Rh positive and Rh negative subjects express different sensitivity to the effects of latent toxoplasmosis on psychomotor performance (Flegr et al., 2008c, 2012a; Novotná et al., 2008) cognitive performance (Flegr et al., 2012a, 2013), personality profile (Cattell, 1972; Flegr et al., 2010, 2012a, 2013), and mental health (Holub et al., 2011) and also differ in their health status and the incidence of certain disorders (Flegr et al., 2015; Flegr, 2016), but see (Halmin et al., 2017). Many effects of toxoplasmosis are much stronger in Rh negative subjects and some can be detected only in them (Flegr et al., 2009; Kaňková et al., 2010). To detect such Rh dependent effects of toxoplasmosis and to increase the sensitivity of tests by decreasing the total variability of the output variables, it is always necessary to include the confounding variable Rh phenotype into the statistical models.
The aim of the present study was to search for possible indices of poorer physical and mental health status in a group of past and present female university students. These students voluntarily participated in behavioral studies at the Faculty of Science, Charles University, and approximately three years later, also participated in economic game experiments at the University of Economics, Prague. Most participants filled in two identical questionnaires (an anamnestic questionnaire monitoring physical and mental health status, and a standard N-70 questionnaire monitoring seven potentially pathognomonic factors: anxiety, depression, obsession, hysteria, hypochondria, psychosomatic symptoms of vegetative lability, and psychasthenia) before and about three years after they were told whether they are Toxoplasma-infected or not. This experimental setup enables one to discriminate whether the Toxoplasma-infected subjects express the symptoms of impaired health because of the infection or because they know that they are infected and therefore believe that they should express (or report) such symptoms.
Materials and Methods
Participants
Subjects were recruited from a pool of former biology students of the Faculty of Science, Charles University, Prague, who have voluntarily participated in various ethological studies over the past 20 years. All subjects were women who were tested for toxoplasmosis and rhesus (Rh) status between 2002 to 2013. These volunteers often take part in many studies, most of which are not related to Toxoplasma infection. Crucially, toxoplasmosis was not mentioned in the study recruitment invitation, and the experiments were run at the University of Economics—not the usual location for toxoplasmosis-related experiments. Moreover, the experimental games were primarily focused on the examination of the economic behavior of women (Lanchava et al., 2015). Therefore, it is unlikely that subjects suspected that the study was related to toxoplasmosis research. To achieve a balanced design and the highest possible power of the study, we invited all 13 Rh-negative Toxoplasma-infected women in the pool (the rarest combination of the trait within the study), two times higher number (26) of Rh-positive Toxoplasma-infected women, and approximately same numbers of Toxoplasma-free controls, 14 Rh-negative and 26 Rh-positive. Therefore, the frequency of infected subjects and Rh-negative subjects did not correspond to their normal representation in the Czech population. All participants provided written informed consent. Subjects' recruitment and data handling were performed in compliance with the Czech legislation in force, and were approved by the Institutional Review Boards of the Faculty of Science, Charles University (No. 2014/21).
Questionnaires
At the beginning of the present study, the volunteers were asked to complete an anamnestic questionnaire as well as a N-70 questionnaire. Most participants completed these questionnaires at two different time points: before testing for toxoplasmosis, and then about 3 years later at the beginning of the present study. In the anamnestic questionnaire, the participants rated their physical and mental health status by answering a panel of questions such as: “How often do you have allergies [or: non-allergic skin problems; digestive problems; common infectious diseases, such as flu; cardiovascular problems; orthopedic problems; neurological problems; headaches; other chronic or recurring pain; other chronic or recurring health problems; depression; other mental health problems; metabolic problems like diabetes; are you tired after returning from work/school; do you visit medical doctors (not dentists and not for prevention)]?” using a 6-point Likert scale (0: never, 1: maximally once a year, 2: maximally once a month, 3: maximally once a week, 4: several times a week, 5: daily or several times daily). They were also asked how many times they used antibiotics in the past 3 years (5 means 5 or more times), and how many times they spent more than a week in the hospital in the past 5 years. The new version of the questionnaire completed after 3 years also contained the question “At what age do you expect to die?”
The N-70 is originally a Czech questionnaire constructed for the assessment of seven areas of psychiatric symptom clusters - anxiety, depression, obsession, hysteria, hypochondria, psychosomatic symptoms of vegetative lability, and psychasthenia (Vacíř, 1973). The English version of the questionnaire is available at (Flegr et al., 2012b). Subjects are asked to answer 70 questions using a 3-point agreement scale. Scores in each cluster range from 0 to 30. The total N-70 score is the sum for all 70 questions.
Serological Tests
All testing for toxoplasmosis was performed at the National Reference Laboratory for Toxoplasmosis, National Institute of Public Health, Prague. The complement-fixation test (CFT), which determines the overall levels of IgM and IgG antibodies of particular specificity, and Enzyme-Linked Immunosorbent Assays (ELISA) (IgG ELISA: SEVAC, Prague) were used to detect T. gondii infection status of the subjects. ELISA assay cut-point values were established using positive and negative standards according to the manufacturer's instructions. In CFT, the titre of antibodies against T. gondii in sera was measured in dilutions between 1:4 and 1:1024. The subjects with CFT titres between 1:8 and 1:128 were considered T. gondii infected. Only subjects with clearly positive or negative results of CFT and IgG ELISA tests were diagnosed as T. gondii-infected or T. gondii-free, whilst subjects with different results on these tests, or ambiguous results, were retested or excluded from the study.
A standard agglutination method was used for Rh factor examination. A constant amount of anti-D serum (human monoclonal antiD reagent; SeracloneH, Immucor Gamma Inc.) was added to a drop of blood on a white glass plate. Red cells of Rh-positive subjects were agglutinated within 2–5 min.
Data Analysis
Statistica v. 10 was used for the statistical analysis. Differences in age were tested by a t-test. N-70 scores were analyzed using an ANCOVA, with toxoplasmosis, Rh and Rh-toxoplasmosis as factors and age as a confounding variable. Certain scores (obsession and, to a smaller extent, depression) had slightly asymmetric distributions; therefore, we repeated the analyses with nonparametric methods. However, results of the parametric and nonparametric analyses were qualitatively the same. Ordinal and binary data were analyzed by a partial Kendall's correlation test, which is used to measure the strength and significance of the association among binary, ordinal, or continuous data regardless of their distributions and allows for the control of one confounding variable—in this case, age (Siegel and Castellan, 1988). It was not possible to control for both age and Rh, therefore we performed the partial Kendall tests separately for Rh-positive and Rh-negative women. The Excel spreadsheet used to compute the partial Kendall tau and the significance for variables A (diseases) and B (Toxoplasma infection), once C (age) was controlled based on Kendall Taus AB, AC, and BC- is available at: http://web.natur.cuni.cz/flegr/programy.php. The false discovery rate (preset to 0.1) was controlled with the Benjamini-Hochberg procedure (Benjamini and Hochberg, 1995). In contrast to the simple Bonferroni's correction, this procedure also takes into account the distribution of p values of performed multiple tests.
All raw data are available at Figshare 10.6084/m9.figshare.5593960.
Results
The final set contained 14 Rh-negative and 26 Rh-positive Toxoplasma-free women and 13 Rh-negative and 26 Rh-positive Toxoplasma-infected women. Infected women were older than Toxoplasma-free women (24.6 vs. 23.0, t77 = −1.90, p = 0.06). No significant effects of age (p = 0.402, μ2 = 0.01), toxoplasmosis (p = 0.206, μ2 = 0.02), and Rh factor (p = 0.419, μ2 = 0.01) were observed, but a significant effect of toxoplasmosis-Rh factor interaction (p = 0.011, μ2 = 0.08) on total N-70 score was detected with an ANCOVA. The same analysis was performed separately on the seven N-70 traits, and showed significant effects of toxoplasmosis-Rh factor interaction on obsession (p = 0.036, μ2 = 0.06), vegetative lability (p = 0.032, μ2 = 0.06), and psychasthenia (p = 0.008, μ2 = 0.09). The visual inspection of Figure 1 suggests that the Toxoplasma-infected Rh-negative women had much higher N-70 traits, whilst Toxoplama-infected Rh positive subjects had approximately the same or slightly lower N-70 traits than corresponding Toxoplasma-free controls.
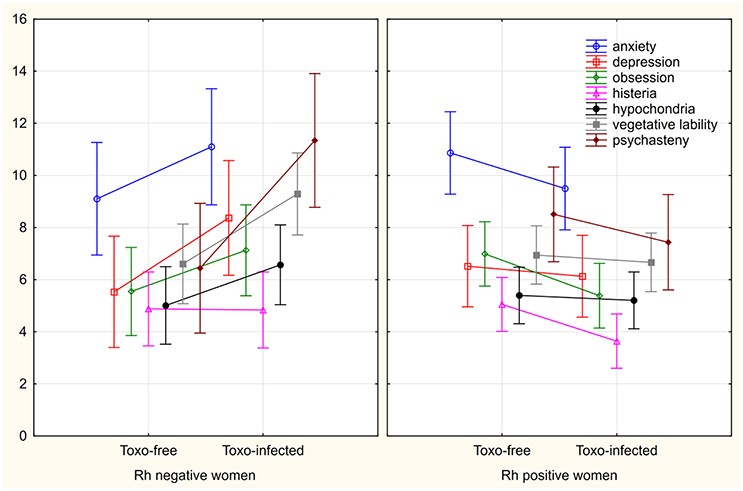
Figure 1. Differences between Toxoplasma-infected and Toxoplasma-free women in seven N-70 factors. The y-axis shows means, spreads 95% C.I.
In the follow up analysis we found that the Toxoplasma-free women answered many questions of the N-70 questionnaire differently than the Toxoplasma-infected women. Partial Kendall analyses, with age as a covariate, were performed on all 79 women, and showed that 13 of 70 observed differences remained significant after the correction for multiple tests. Separate analyses of 27 Rh-negative women and 52 Rh-positive women showed that the number of significant differences between Toxoplasma-infected women and Toxoplasma-free women was 32 of 70 and 12 of 70 in Rh-negative and Rh-positive women, respectively. While in Rh-negative women only 3 of 32 significant associations were negative, i.e., indicated better health status or wellbeing of Toxoplasma-infected women, in Rh-positive subjects, 11 of 12 associations, significant after the correction for multiple tests, were negative (see Table 1).
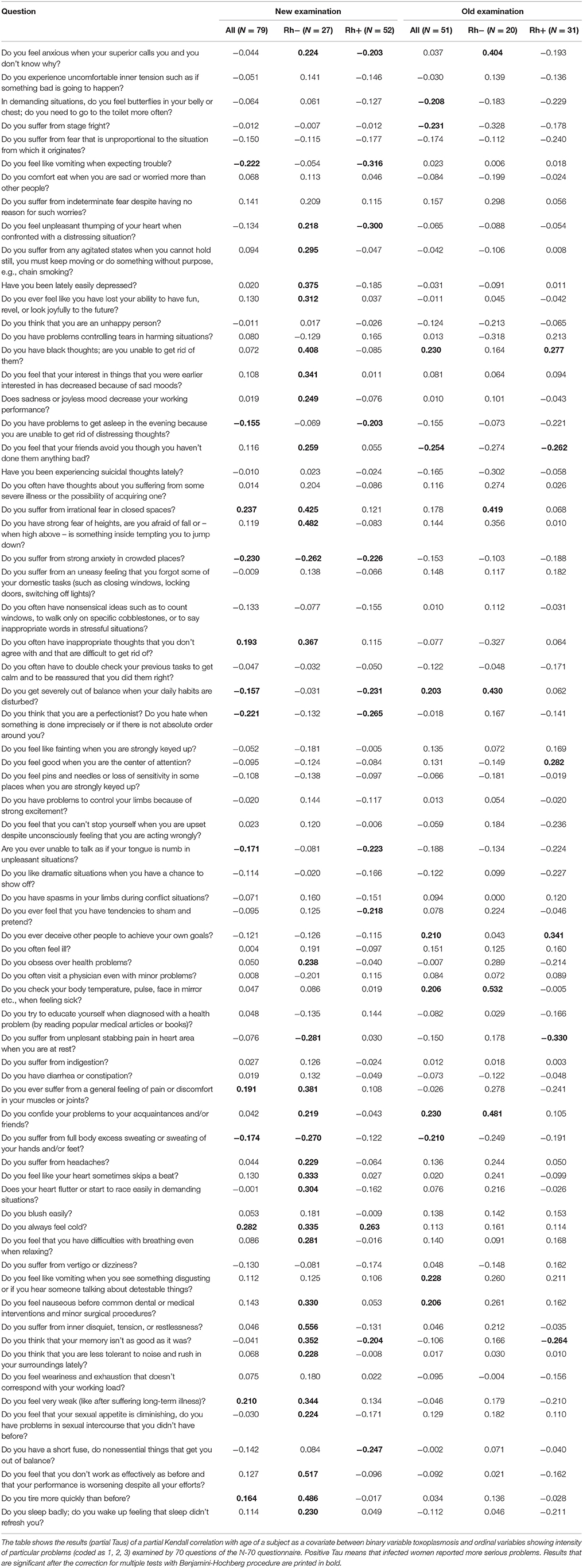
Table 1. Differences between responses of Toxoplasma-infected and Toxoplasma-free women to 70 N-70 questions.
The existence of a statistical association between two factors does not mean a causal relation between these factors. However, the existence of a causal relation can be supported when one or more Bradford-Hill criteria of causality are fulfilled. To search for such support, we tested the biological gradient of the effect of toxoplasmosis. This was achieved by studying the correlation between the concentration of anti-Toxoplasma antibodies and N-70 factors in a subset of Toxoplasma-infected women. Figure 2 and Table 2 show that the CFT titre of antibodies in Toxoplasma-infected women correlate with the total N-70 score, as well as with all seven N-70 factors in Rh factor-negative women but not in Rh factor-positive women. Existence of this correlation (satisfaction of the criterion 5 - the biological gradient) supports, but of course does not prove, the existence of the causal relation between the Toxoplasma infection and neuroticism.
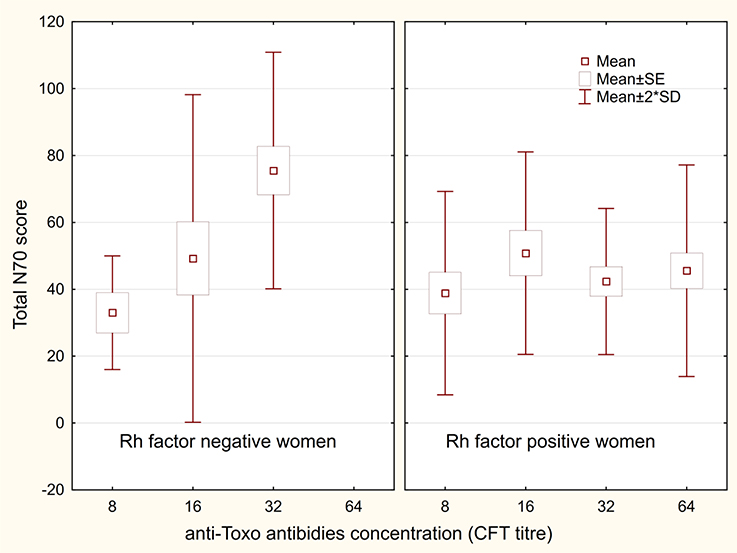
Figure 2. Correlation between N-70 score and anti-Toxoplasma antibodies concentration. The boxes indicate the mean ±standard error, and spreads indicate the mean ±2 × standard deviation.
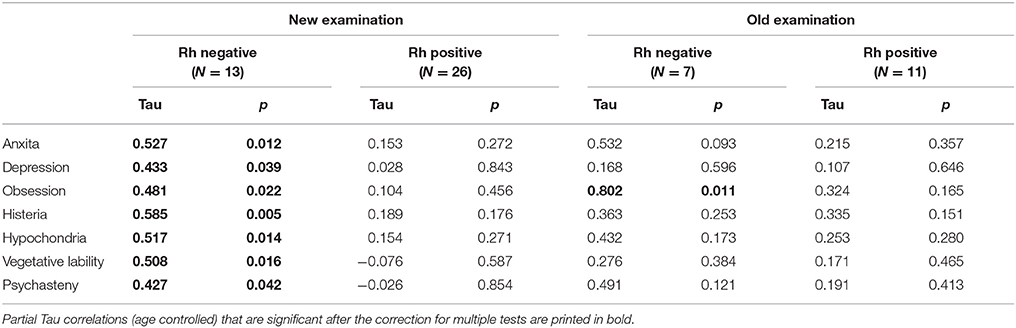
Table 2. Correlation between concentration of anti-Toxoplasma antibodies and N-70 factors.
Twenty (20) Rh-negative women (7 Toxoplasma-infected) and 31 Rh-positive women (11 Toxoplasma-infected) also completed the questionnaire 3 years earlier, before they knew whether or not they were infected. We repeated all analyses with this smaller data set. No effects of toxoplasmosis or toxoplasmosis-Rh factor interaction were significant after the correction for multiple tests, possibly due to the low number (7) of Toxoplasma-infected, Rh negative women, the results not shown. However, the follow up analyses once again showed that many of the seventy N-70 questions were answered differently by the Toxoplasma-infected and Toxoplasma-free women (11 in the whole set, 5 in the subset of 20 Rh-negative women and 6 in the subset of 31 Rh positive women; Benjamini-Hochberg correction for multiple tests, see Table 1). Figure 3 shows that N-70 pathognomonic factors mostly decreased or stayed constant between the first and the second examination in Rh-positive Toxoplasma-infected and Toxoplasma-free women and in Rh-negative Toxoplasma-free women, but three factors (anxiety, depression, and psychasthenia) increased in Rh-negative Toxoplasma-infected women. The repeat measure ANCOVA with N-70 factors, measured before testing for toxoplasmosis and about 3 years later, showed that the time-toxoplasmosis-Rh interaction had a significant effect only on depression (p = 0.027, μ2 = 0.10).
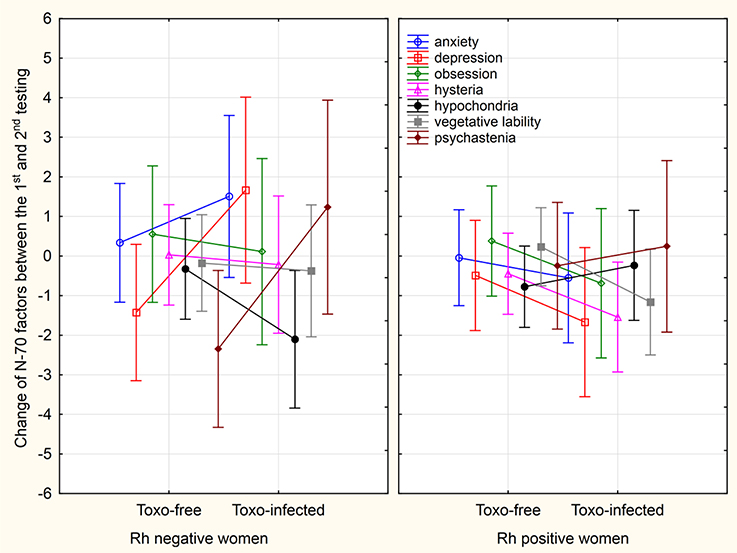
Figure 3. Changes in N-70 factors between the first and second testing. The spreads show 95% C.I.
In the anamnestic questionnaire, the subjects rated their health status before testing for toxoplasmosis, and during N-70 testing 3 years later. Table 3 shows that infected Rh-negative as well as the Rh-positive Toxoplasma-infected women express several indices of impaired physical and mental health before, as well as after, obtaining the information about their toxoplasmosis status. For example, they estimated their probable age of survival to be lower than Toxoplasma-free women, reported more frequent hospitalizations in the past 5 years, and to have more serious or more frequent neurological problems.
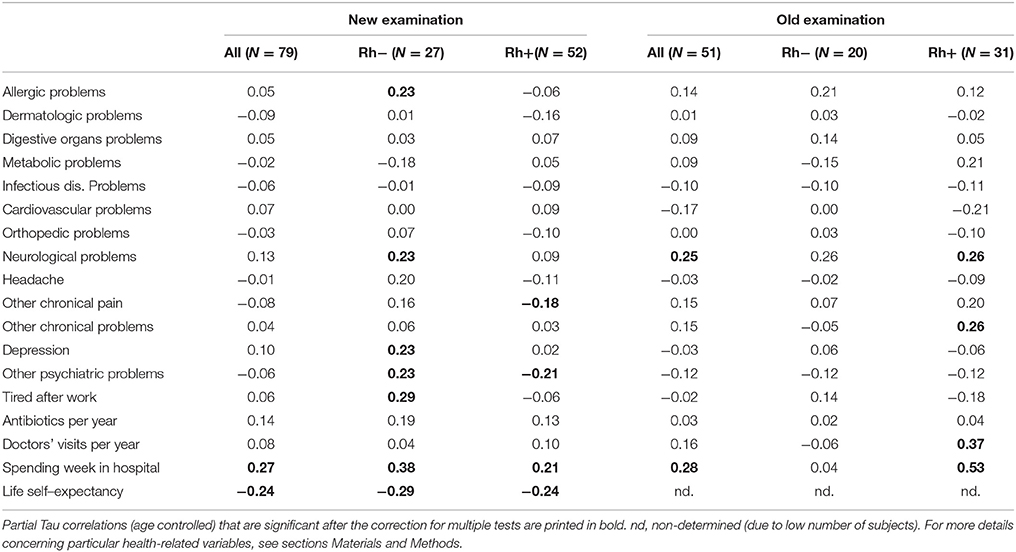
Table 3. Differences in health related variables between Toxoplasma-infected and Toxoplasma-free women.
Discussion
The present study showed that Toxoplasma-infected women with Rh-negative phenotype expressed higher levels of certain potentially pathognomonic factors measured with the N-70 questionnaire, especially obsessiveness, vegetative lability, and psychasthenia. In the infected subjects, the level of these factors correlated positively with the concentration of anti-Toxoplasma antibodies in Rh-negative women but not in more numerous Rh-positive women. Both Rh-negative and Rh-positive women reported more serious and more frequent physical and mental health-related problems. Differences between Toxoplasma-infected and Toxoplasma-free subjects in potentially pathognomonic factors and health-related variables were also observed in a subset of women who completed the N-70 and anamnestic questionnaires 3 years before the present study, i.e., during a time when they were not aware whether they were infected or not.
Poorer health status of Toxoplasma-infected subjects was observed in many case-controlled studies—for a review see (Flegr et al., 2014). A recent study performed on a large nonclinical cohort of 1,486 volunteers showed that Toxoplasma-infected subjects scored more poorly in 28 of 29 health-related variables, including number of stays in the hospital, number of doctors visits, frequency of being tired, and seriousness or frequency of allergic, neurological and mental health problems. In contrast to previous studies, here we demonstrated the existence of toxoplasmosis-related effects before the subjects were informed of whether they are Toxoplasma-infected or not. This means that the observed effects could not be the result of autosuggestion based on the subjects' belief that toxoplasmosis has a negative effect on their health. The only factor that significantly increased in Rh-negative, Toxoplasma-infected women was depression, i.e., the factor that was not significantly higher in Toxoplasma-infected than in Toxoplasma-free Rh-negative women during the second N-70 testing. Our conclusion—that impaired physical and mental health status, not autosuggestion, was responsible for higher N-70 factors—was also supported by the fact that Toxoplasma-infected women had the same level of hypochondria as the Toxoplasma-free women. The negative effects of toxoplasmosis on human health were also demonstrated in a recent ecological study (Flegr et al., 2014). The prevalence of toxoplasmosis in 88 countries correlated positively with specific disease burden for 23 of 128 studied disorders. The effects of toxoplasmosis on public health was relatively large. For example, the differences in prevalence of toxoplasmosis explained 23% of variability in total disease burden between European countries (Flegr et al., 2014).
At the same time, the present results concerning factors in women measured with the N-70 questionnaire contrasted with results of a similar study performed on male soldiers who went through the entrance examinations for (well-paid) participation in international military missions. The authors of the study suggested that the Toxoplasma-infected subjects were objectively motivated to mask their negative and accentuate their positive characteristics. It is, however, also possible that toxoplasmosis had an opposite effect on these pathognomonic factors in men and women as it has been already demonstrated for many personality factors and behavioral patterns (Lindová et al., 2006, 2010; Flegr et al., 2011).
Both the present and previous studies show a much stronger effect of toxoplasmosis on Rh-negative than Rh-positive subjects. In the present study, we observed significantly higher N-70 factors in Toxoplasma-infected Rh-negative women and slightly (not significantly) lower N-70 factors (i.e., better physical and mental health) in Toxoplasma-infected Rh-positive women. Detailed analyses of the N-70 questionnaire responses of Toxoplasma-infected and Toxoplasma-free Rh-positive women showed that 11 of 12 significant differences indicated better physical or mental health of infected subjects. Such paradoxical (positive) effects of Toxoplasma infection have been previously reported to exist. The case control study performed on 500 blood donors showed that Toxoplasma-infected Rh-positive heterozygotes showed better psychomotor performance—namely, shorter reaction times—than Toxoplasma-free Rh-positive heterozygotes. At the same time, psychomotor performance of infected Rh-positive homozygotes and especially of infected Rh-negative homozygotes was much poorer than that of corresponding controls (Novotná et al., 2008). It has been shown that toxoplasmosis has various effects on human physiology and some of these effects, such as increase of testosterone (Flegr et al., 2008a,b) or partial immunosuppression (Flegr and StříŽ, 2011), could have a positive impact on human performance and health in certain situations. It must be remembered that our population of Rh-positive women represents a mixture of homozygotes and heterozygotes. At the same time, current data suggests that protective effects of Rh factor positivity are fully expressed only in the Rh-positive heterozygotes (Novotná et al., 2008; Flegr, 2016). Therefore, future studies should be performed on DNA genotyped populations. The difference between Rh-positive homozygotes and heterozygotes, namely permanent protection against the prolongation of reaction times in heterozygotes and only temporary protection in homozygytes (Novotná et al., 2008), suggests that not only the RhD molecule, but also a product of another gene in a strong genetic linkage with the RHD gene, might be responsible for the observed toxoplasmosis-related effects of Rh phenotype (Flegel, 2006). For testing such hypothesis, Rh genotype instead of Rh phenotype needs to be monitored in the participants of future studies.
It should be reminded that nearly all inhabitants of many African countries are Toxoplasma-infected and that latent toxoplasmosis was probably the natural status of humans in most parts of world for most of the evolutionary history of our species. Also, the large incidence of Rh-negativity (about 17%) in Europe is rather atypical and it has been suggested that it is related to the low prevalence of toxoplasmosis on this continent before the advent of a domestic cat (Flegr et al., 2008c). It is therefore possible that not only the Rh-negative, Toxoplasma-infected subjects, but partly also the Rh-positive, Toxoplasma-free subjects could have certain health-related problems.
A combination of results of observational studies performed on humans, and especially experimental studies performed on animals, suggests (but of course does not prove) that toxoplasmosis is the cause rather than the effect of impaired physical and mental health of infected hosts. The present study showed that the level of N-70 pathognomonic factors correlated with the level of anti-Toxoplasma antibodies measured with CFT. This test measured the concentration of specific IgM and of certain subclasses of IgG antibodies reacting with various Toxoplasma antigens. It has been shown that the intensity of the CFT signal decreases with time from the infection and could be therefore used as a proxy of the duration of latent toxoplasmosis. The intensity of many toxoplasmosis-associated changes, such as personality factor changes (Flegr et al., 2000) or the impairment of reaction times (Havlíček et al., 2001), are negatively correlated with the concentration of anti-Toxoplasma antibodies measured with CFT. It has been shown that CFT titres are probably a better proxy for the duration of the infection than the concentration of IgG measured with enzyme-linked immunosorbent assay (Kodym et al., 2007) but worse than—now rarely used—indirect immunofluorescence assay (Kaňková et al., 2007). The existence of a negative correlation is mostly considered to be indirect evidence for models suggesting that given toxoplasmosis-associated changes represent slow cumulative effects of latent infection. In contrast, a positive correlation between the concentration of antibodies and the changes suggests that the observed effects represent transient vanishing effects of acute toxoplasmosis. Such positive correlations were observed, for example, for the probability of traffic accidents (Flegr et al., 2009) and predisposition to gestational diabetes mellitus (Kaňková et al., 2015), and now additionally for N-70 factors.
Limitations
The main limitation of the present study is that its participants were tested for toxoplasmosis several years before the current study. Toxoplasmosis is a life-long infection and, therefore, women with positive results of the serological test stay infected for their entire lives. However, at least some originally Toxoplasma-free women could have acquired the infection in the years that passed between the diagnosis and the start of the present study. Monte Carlo model-based analysis showed that the presence of such false negative subjects in the study population could easily result in Type 2 error, i.e., failure to detect existing effects of toxoplasmosis, but could not result in false positive results of a study—in the detection of non-existing effects (Flegr and Horáček, 2017). For technical reasons (too low number of Toxoplasma-infected, Rh-negative men in the Czech population and therefore also in our file), we had to perform the study only on women. The recent study performed on the population of our volunteers showed that prevalence of toxoplasmosis is higher in women (30.1%) than in men (20.1%) (Flegr, 2017). However, most of the behavioral and health-related effects of toxoplasmosis are stronger in men than in women. Therefore, it would be necessary to repeat the study on a male population in the future.
Conclusions
Our results support the notion that many behavioral effects of toxoplasmosis represent side-effects of mild but long-term impaired health status rather than a product of adaptive parasitic manipulation aimed to increase the chances for the transmission of Toxoplasma from intermediate to definitive hosts. The results also suggest that toxoplasmosis likely has a serious impact on subjectively perceived physical and mental health. Toxoplasmosis affects about one third of the human population worldwide and therefore its global impact on public health may be important. No method of treatment of latent toxoplasmosis and no vaccine that could protect humans against the infection are currently available. The results that slowly accumulated over the past 15 years strongly suggest that such methods and vaccines should be intensively searched for.
Author Contributions
JF designed the study and performed the analyses. BŠ collected and preprocessed the data. Both authors contributed to and have approved the final manuscript.
Funding
The work was supported by project UNCE 025 (Charles University in Prague) and the Czech Science Foundation (Grant No. P407/16/20958).
Conflict of Interest Statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Acknowledgments
We would like to thank Charlie Lotterman and Lucy Burns for their help with the final version of the paper.
References
Benjamini, Y., and Hochberg, Y. (1995). Controlling the false discovery rate: a practical and powerful approach to multiple testing. J. R. Stat. Soc. B. Met. 57, 289–300.
Carver, C. S., Scheier, M. F., and Weintraub, J. K. (1989). Assessing coping strategies - a theoretically based approach. J. Pers. Soc. Psychol. 56, 267–283. doi: 10.1037/0022-3514.56.2.267
Flegel, W. A. (2006). Molecular genetics of RH and its clinical application. Transfus. Clin. Biol. 13, 4–12. doi: 10.1016/j.tracli.2006.02.011
Flegr, J. (2010). Influence of latent toxoplasmosis on the phenotype of intermediate hosts. Folia Parasitol. 57, 81–87. doi: 10.14411/fp.2010.010
Flegr, J. (2015). Neurological and neuropsychiatric consequences of chronic Toxoplasma infection. Parasitology 2, 163–172. doi: 10.1007/s40588-015-0024-0
Flegr, J. (2016). Heterozygote advantage probably maintains Rhesus factor blood group polymorphism: ecological regression study. PLoS ONE 11:e0147955. doi: 10.1371/journal.pone.0147955
Flegr, J. (2017). Predictors of Toxoplasma gondii infection in Czech and Slovak populations: the possible role of cat-related injuries and risky sexual behavior in the parasite transmission. Epidemiol. Infect. 145, 1351–1362. doi: 10.1017/S095026881700019X
Flegr, J., and Escudero, D. Q. (2016). Impaired health status and increased incidence of diseases in Toxoplasma-seropositive subjects – an explorative cross-sectional study. Parasitology 143, 1974–1989. doi: 10.1017/S0031182016001785
Flegr, J., Geryk, J., Volny, J., Klose, J., and Cernochova, D. (2012a). Rhesus factor modulation of effects of smoking and age on psychomotor performance, intelligence, personality profile, and health in Czech soldiers. PLoS ONE 7:e49478. doi: 10.1371/journal.pone.0049478
Flegr, J., Hampl, R., Černochová, D., Preiss, M., Bičíkova, M., Sieger, L., et al. (2012b). The relation of cortisol and sex hormone levels to results of psychological, performance, IQ and memory tests in military men and women. Neuro Endocrinol. Lett. 33, 224–235. doi: 10.6084/m9.figshare.5593984
Flegr, J., Hoffmann, R., and Dammann, M. (2015). Worse health status and higher incidence of health disorders in Rhesus negative subjects. PLoS ONE 10:e0141362. doi: 10.1371/journal.pone.0141362
Flegr, J., and Horáček, J. (2017). Toxoplasma-infected subjects report an Obsessive-Compulsive Disorder diagnosis more often and score higher in Obsessive-Compulsive Inventory. Eur. Psychiatry 40, 82–87. doi: 10.1016/j.eurpsy.2016.09.001
Flegr, J., and StříŽ, I. (2011). Potential immunomodulatory effects of latent toxoplasmosis in humans. BMC Infect. Dis. 11:274. doi: 10.1186/1471-2334-11-274
Flegr, J., Klose, J., Novotná, M., Berenreitterová, M., and Havlíček, J. (2009). Increased incidence of traffic accidents in Toxoplasma-infected military drivers and protective effect RhD molecule revealed by a large-scale prospective cohort study. BMC Infect. Dis. 9:72. doi: 10.1186/1471-2334-9-72
Flegr, J., Kodym, P., and Tolarová, V. (2000). Correlation of duration of latent Toxoplasma gondii infection with personality changes in women. Biol. Psychol. 53, 57–68. doi: 10.1016/S0301-0511(00)00034-X
Flegr, J., Lenochová, P., Hodný, Z., and Vondrová, M. (2011). Fatal attraction phenomenon in humans: cat odour attractiveness increased for Toxoplasma-infected men while decreased for infected women. PLoS Negl. Trop. Dis. 5:e1389. doi: 10.1371/journal.pntd.0001389
Flegr, J., Lindová, J., and Kodym, P. (2008a). Sex-dependent toxoplasmosis-associated differences in testosterone concentration in humans. Parasitology 135, 427–431. doi: 10.1017/S0031182007004064
Flegr, J., Lindová, J., Pivoňková, V., and Havlíček, J. (2008b). Brief communication:latent toxoplasmosis and salivary testosterone concentration-important confounding factors in second to fourth digit ratio studies. Am. J. Phys. Anthropol. 137, 479–484. doi: 10.1002/ajpa.20888
Flegr, J., Novotná, M., Fialová, A., Kolbeková, P., and Gašová, Z. (2010). The influence of RhD phenotype on toxoplasmosis- and age-associated changes in personality profile of blood donors. Folia Parasitol. 57, 143–150. doi: 10.14411/fp.2010.018
Flegr, J., Novotná, M., Lindová, J., and Havlíček, J. (2008c). Neurophysiological effect of the Rh factor. Protective role of the RhD molecule against Toxoplasma-induced impairment of reaction times in women. Neuro Endocrinol. Lett. 29, 475–481. doi: 10.6084/m9.figshare.5593993
Flegr, J., Prandota, J., Sovickova, M., and Israili, Z. H. (2014). Toxoplasmosis - a global threat. Correlation of latent toxoplasmosis with specific disease burden in a set of 88 countries. PLoS ONE 9:e90203. doi: 10.1371/journal.pone.0090203
Flegr, J., Preiss, M., and Klose, J. (2013). Toxoplasmosis-associated difference in intelligence and personality in men depends on their Rhesus blood group but not ABO blood group. PLoS ONE 8:e61272. doi: 10.1371/journal.pone.0061272
Halmin, M., Rostgaard, K., Lee, B. K., Wikman, A., Norda, R., Nielsen, K. R., et al. (2017). Length of storage of red blood cells and patient survival after blood transfusion a binational cohort study. Ann. Intern. Med. 166, 248–256. doi: 10.7326/M16-1415
Havlíček, J., Gašová, Z., Smith, A. P., Zvára, K., and Flegr, J. (2001). Decrease of psychomotor performance in subjects with latent ‘asymptomatic’ toxoplasmosis. Parasitology 122, 515–520. doi: 10.1017/S0031182001007624
Hobfoll, S. E., Dunahoo, C. L., Ben-Porath, Y., and Monnier, J. (1994). Gender and coping: the dual-axis model of coping. Am. J. Comm. Psych. 22, 49–82. doi: 10.1007/BF02506817
Holub, D., Bankovská, M., Dragomirecká, E., Rodriguez, M., Preiss, M., Novák, T., et al. (2011). Possible protective function of Rh factor in schizophrenia. Psychiatrie 15, 37–42. doi: 10.6084/m9.figshare.5593999
Kaňková, Š., Flegr, J., and Calda, P. (2015). An elevated blood glucose level and increased incidence of gestational diabetes mellitus in pregnant women with latent toxoplasmosis. Folia Parasitol. 62, 1–6. doi: 10.14411/fp.2015.056
Kaňková, Š., Šulc, J., and Flegr, J. (2010). Increased pregnancy weight gain in women with latent toxoplasmosis and RhD-positivity protection against this effect. Parasitology 137, 1773–1779. doi: 10.1017/S0031182010000661
Kaňková, Š., Šulc, J., Nouzová, K., Fajfrlik, K., Frynta, D., and Flegr, J. (2007). Women infected with parasite Toxoplasma have more sons. Naturwissenschaften 94, 122–127. doi: 10.1007/s00114-006-0166-2
Kodym, P., Machala, L., Roháčová, H., Širocká, B., and Malý, M. (2007). Evaluation of a commercial IgE ELISA in comparison with IgA and IgM ELISAs, IgG avidity assay and complement fixation for the diagnosis of acute toxoplasmosis. Clin. Microbiol. Infec. 13, 40–47. doi: 10.1111/j.1469-0691.2006.01564.x
Lanchava, L., Carlson, K., Sebankova, B., Flegr, J., and Nave, G. (2015). No evidence of sssociation between Toxoplasma gondii infection and financial risk taking in females. PLoS ONE 10:e0136716. doi: 10.1371/journal.pone.0136716
Lindová, J., Kuběna, A. A., Šturcová, A., Křivohlavá, R., Novotná, M., Rubešová, A., et al. (2010). Pattern of money allocation in experimental games supports the stress hypothesis of gender differences in Toxoplasma gondii-induced behavioural changes. Folia Parasitol. 57, 136–142. doi: 10.14411/fp.2010.017
Lindová, J., Novotná, M., Havlíček, J., Jozífková, E., Skallová, A., Kolbeková, P., et al. (2006). Gender differences in behavioural changes induced by latent toxoplasmosis. Int. J. Parasitol. 36, 1485–1492. doi: 10.1016/j.ijpara.2006.07.008
Novotná, M., Havlíček, J., Smith, A. P., Kolbeková, P., Skallová, A., Klose, J., et al. (2008). Toxoplasma and reaction time: role of toxoplasmosis in the origin, preservation and geographical distribution of Rh blood group polymorphism. Parasitology 135, 1253–1261. doi: 10.1017/S003118200800485X
Pappas, G., Roussos, N., and Falagas, M. E. (2009). Toxoplasmosis snapshots: global status of Toxoplasma gondii seroprevalence and implications for pregnancy and congenital toxoplasmosis. Int. J. Parasitol. 39, 1385–1394. doi: 10.1016/j.ijpara.2009.04.003
Rosario, M., Shinn, M., Mørch, H., and Huckabee, C. B. (1988). Gender differences in coping and social supports: testing socialization and role constraint theories. J. Community Psychol. 16, 55–69. doi: 10.1002/1520-6629(198801)16:1<55::AID-JCOP2290160108>3.0.CO;2-U
Siegel, S., and Castellan, N. J. (1988). Nonparametric Statistics for the Behavioral Sciences. New York, NY: McGraw-Hill.
Stone, A. A., and Neale, J. M. (1984). New measure of daily coping: development and preliminary results. J. Pers. Soc. Psychol. 46, 892–906. doi: 10.1037/0022-3514.46.4.892
Sutterland, A. L., Fond, G., Kuin, A., Koeter, M. W., Lutter, R., Van Gool, T., et al. (2015). Beyond the association. Toxoplasma gondii in schizophrenia, bipolar disorder, and addiction: systematic review and meta-analysis. Acta Psychiatr. Scand. 132, 161–179. doi: 10.1111/acps.12423
Tamres, L. K., Janicki, D., and Helgeson, V. S. (2002). Sex differences in coping behavior: a meta-analytic review and an examination of relative coping. Pers. Soc. Psych. Rev. 6, 2–30. doi: 10.1207/S15327957PSPR0601_1
Keywords: longitudinal study, neuroticism, mental health, latent toxoplasmosis, public health, rhesus factor
Citation: Šebánková B and Flegr J (2017) Physical and Mental Health Status in Toxoplasma-Infected Women before and 3 Years after They Learn about Their Infection: Manipulation or Side-Effects of Impaired Health? Front. Ecol. Evol. 5:144. doi: 10.3389/fevo.2017.00144
Received: 25 May 2017; Accepted: 07 November 2017;
Published: 21 November 2017.
Edited by:
David Hughes, Pennsylvania State University, United StatesReviewed by:
Peter L. Hurd, University of Alberta, CanadaIvar Folstad, University of Tromsø, Norway
Copyright © 2017 Šebánková and Flegr. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) or licensor are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Jaroslav Flegr, ZmxlZ3JAY2VzbmV0LmN6