 Ségolène Fleury1,2*
Ségolène Fleury1,2* Paul Tronchon2
Paul Tronchon2 Juliane Rota1Charlotte Meunier1Oliver Mardiros1
Juliane Rota1Charlotte Meunier1Oliver Mardiros1 Virginie Van Wymelbeke-Delannoy1,3
Virginie Van Wymelbeke-Delannoy1,3 Claire Sulmont-Rossé1
Claire Sulmont-Rossé1- 1Centre des Sciences du Goût et de l'Alimentation, AgroSup Dijon, Centre National de la Recherche Scientifique, Institut National de Recherche pour l'Agriculture, l'Alimentation et l'Environnement, Université de Bourgogne Franche-Comté, Dijon, France
- 2Saveurs et Vie, Orly, France
- 3Centre Hospitalier Universitaire Dijon Bourgogne, Unité de Recherche Pôle Personnes Âgées, Dijon, France
Background: Setting up a home-delivered meal service often allows older people suffering from physical and/or cognitive disabilities to stay at home. However, older people who delegate their food activities (food purchasing, cooking…) have been reported to have a worse nutritional status than people who take care of their food activities. In this context, we will conduct a systematic review of all studies related to the nutritional issue in home-delivered meal older recipients.
Methods: In June 2020, we searched 3 databases (Pubmed, Web of Science, EMBASE) to identify studies from all years on older adults at home and receiving home-delivered meal services (population). The following outcomes were considered: nutritional status (Body Mass Index, weight, undernutrition) and nutritional intake. Any nutritional intervention, comparator, and study design were relevant for inclusion.
Results: Forty-eight original studies met the inclusion criteria, most of them being published after the year 2000 (n = 34) and undertaken in the USA (n = 32). The selection includes 30 cross-sectional and 18 longitudinal studies. The main findings of this review are the following: (1) home-delivery meal older recipients are at high risk of undernutrition; (2) providing home-delivery meals may improve the nutritional status and nutrient intake; (3) this improvement is even higher when the home-delivery meal service is improved, for instance by providing dietetic counseling or adding supplementary snacks/meals or enriched food. However, even an improved service does not allow all the older recipients meeting their recommended nutritional allowance.
Conclusion: This review reveals a need to further develop strategies allowing home-delivery meal older recipients to fulfill their nutritional needs. From a methodological point of view, there is a need to describe in more detail the home-delivered services provided to studies' participants to better consider meal frequency and meal content in the results.
Introduction
Home-delivered meal (HDM) services for older adults and/or disabled people were introduced in the United Kingdom during the Second World War, providing meals for people who could no longer prepare food for themselves. Subsequently, this type of service spread first to the United States, Ireland, Australia, and then more generally to the other industrialized countries (1, 2). In the Netherlands, home-delivered meal services seem to be mainly funded by private corporations and not by health insurance or social funds. Conversely, in the United States, home-delivered meal services mainly concern elderly people with financial difficulties and is funded under the Older Americans Act (OAA) (3). Finally, in emerging countries such as Korea and Hong Kong, it is most common to make delivery of fresh products to the elderly (4). In the future, demands to this services that enable seniors to remain residing in their homes can be expected to increase. Indeed, numerous countries in the world are experiencing a tremendous increase of the older population, and notably an increase of the “very old” population, namely people aged 80 or over. The number of 80 and over is expected to increase from 126 million in 2015 to 202 million in 2030 and 426 million in 2050 (5). These “very old” people are also the ones who present the poorest health and accumulate the severest disabilities. Consequently, they are more likely to ask support from care services. More recently, according to home-delivered meal companies, the lockdown due to the Covid-19 epidemic led to an increase in home-delivered meal service demand in major French cities and probably elsewhere in the world.
A couple of authors have pointed out that elderly people who delegate their food activities (food purchasing, cooking…) have a worse nutritional status than people who take care themselves of their food activities. Maitre et al. (6) observed at home that the proportion of elderly people who were at risk of undernutrition was 8% for autonomous persons, 16% for persons receiving non-food-related help, and 46% for persons receiving food-related help. Crichton et al.'s (7) meta-analysis showed that older people receiving homecare services display the highest malnutrition prevalence of all the community-dwelling elderly sample studied.
In this context, the purpose of the present study was to conduct a systematic litterature review of all studies related to the nutritional issue in home-delivered meal older recipients. This review was expected (i) to shed light on the nutritional status of older people who benefit from home-delivery service to better understand their needs and (ii) to evaluate if home-delivered meal service can be a relevant and effective lever to preserve or improve the nutritional status of older people.
Methods
Our systematic literature review followed the approach proposed by Arksey and O'Malley (8) as well as the methodology manual published by the Joanna Briggs Institute (9). This methodology summarizes the evidence available on a topic to convey the breadth and depth of that topic. The protocol was drafted using the Preferred Reporting Items for Systematic Reviews and Meta-analysis Protocols (10). A deposit of the protocol was done on HAL: hal-02901422, version 1.
Research Question
The research question for this review is: “What are the objectives, characteristics and results of existing research conducted on the nutritional issue among older people receiving home-delivered meals (also known as meals-on-wheels)?”
Eligibility Criteria
The PICOS (Population, Intervention, Comparator, Outcome, Study design) eligibility criteria were as follows (11):
Population. Only older adults living at home and receiving home-delivered meal services were eligible. We excluded from the review (1) studies on older people residing at nursing homes or in the hospital and (2) studies that not display specific data and results for home-delivered meal recipients (e.g., studies that display results from a mixed sample including home-delivered meal recipients and recipients of other care services such as home helper or congregate meals).
Intervention. Any nutritional intervention was relevant for inclusion (e.g., studies providing additional food items to regular meals-on-wheels, or studies providing dietary guidance). In addition, studies without an intervention (e.g., observational studies) were eligible for inclusion. Any intervention targeting specific disease rehabilitation was excluded (e.g., intervention targeting patients with hypertension, diabetes, cancer).
Comparators. Any comparator was relevant for inclusion (e.g., studies comparing home-delivered meal recipients with non-recipients, or studies comparing two types of home-delivered meal services). In addition, studies without a comparator were eligible for inclusion.
Outcomes. Two categories of outcomes associated were considered: (1) characterization of the nutritional status (e.g., body mass index—BMI, weight, undernutrition) and (2) characterization of the nutritional intake (e.g., dietary pattern, nutrient intake).
Study Design. All types of study design including observational and interventional design as well as all periods of times and duration of follow-up were eligible.
Others. No restriction on the date of publication was made. Given the 6-month timeline, only publications written in English were considered for inclusion. Conference abstracts, editorials, narrative review, and non-scientific literature (e.g., articles on websites) were excluded.
Information Sources and Search Strategy
After repeated attempts and adjustments, a search strategy combining both thesaurus and free-text terms was developed to retrieve articles of interest in the following databases: PubMed, Web of Science (WOS), and EMBASE (Supplementary File 1). Separate title, abstract, and keyword searches were conducted for older people, home-delivered meal service, and nutritional outcomes on June 2020. The results for the three separate search strings were combined to identify relevant titles. Afterward, references from selected articles and systematic reviews were checked manually for further screening in case they have been not identified during the whole search process. After removing the duplicates, titles, abstracts, and full texts were screened by two independent reviewers against the agreed inclusion and exclusion criteria. For each screening level, a training exercise was conducted prior to the starting of the screening process on a random sample of 50 titles (level one screening), 20 abstracts (level two screening), and 10 full-text (level three screening) to ensure high inter-reviewer reliability. Disagreements between reviewers were resolved by consensus or by consulting a third reviewer. The reasons for exclusion were recorded at the full-text stage.
Charting the Data
A standardized data abstraction form was developed a priori and revised, as needed, after the completion of a training exercise completed on a sample of five articles. All included studies were abstracted by two reviewers, independently, with conflicts resolved by a third reviewer. The data abstraction form included the following items:
- Article identifiers (authors, year of publication)
- Study identifiers (objective, design, country)
- Population (age, gender, sample size, inclusion, and exclusion criteria)
- Intervention (if applicable)
- Comparator (if applicable)
- Outcomes (endpoints, measurement method, main results).
Quality Assessment
All included studies were assessed for quality by two reviewers, independently, with conflicts resolved by a discussion until consensus was reached. The quality of the articles was assessed by using the quality assessment criteria developed by Kmet et al. (12). The criteria were the following:
1. Is the objective of the study sufficiently described?
2. Is the study design evident and appropriate?
3. Is the method of subject selection described and appropriate?
4. If interventional and random allocation was possible, was it described?
5. If interventional and blinding of investigators was possible, was it reported?
6. If interventional and blinding of subjects was possible, was it reported?
7. Are subject characteristics sufficiently described?
8. Are outcome measures well-defined and robust to measurement?
9. Is the sample size appropriate?
10. Are analytic methods described, justified, and appropriate?
11. Is some estimate of variance reported for main results?
12. Are they controlled for confounding?
13. Are the results reported in sufficient detail?
14. Are the conclusions supported by results?
Each question can be answered with “yes,” “partial,” “no,” and “not applicable.” The associated scoring manual of Kmet et al. (12) was used to calculate the quality score as it is described below:
In addition, the description quality of HDM service (meal frequency, type of meals, content of meal) was assessed (but not included in the quality score).
Collating, Summarizing, and Reporting the Results
A descriptive summary of the included studies' characteristics was performed. Tables were created to reflect the overall number of studies included, study designs and settings, publication years, the characteristics of the study populations, the outcomes reported, and the countries where the studies were conducted. In line with systematic literature review guidelines, an assessment of the quality of the included studies was performed (9).
Results
General Description of the Systematic Review Article Selection
A total of 10,919 articles were retrieved. After title and abstract screening, 334 records were kept for full-text retrieval and 52 articles were included at full-text review−48 original studies (Figure 1) and four Systematic Literature Reviews (13–16). It should be noted that seven papers including older people with HDM in a broad sample were not included in the synthesis as separated data analyses were not conducted for HDM participants—analyses were done on a broader sample including participants without and with HDM (17–23). Unfortunately, we were not able to find the full text for 12 records despite that we tried to purchase them through the network of university libraries or to contact the authors. Most of these records have old-published years (<1990). The full list of these records can be obtained by contacting the corresponding author of the present paper.
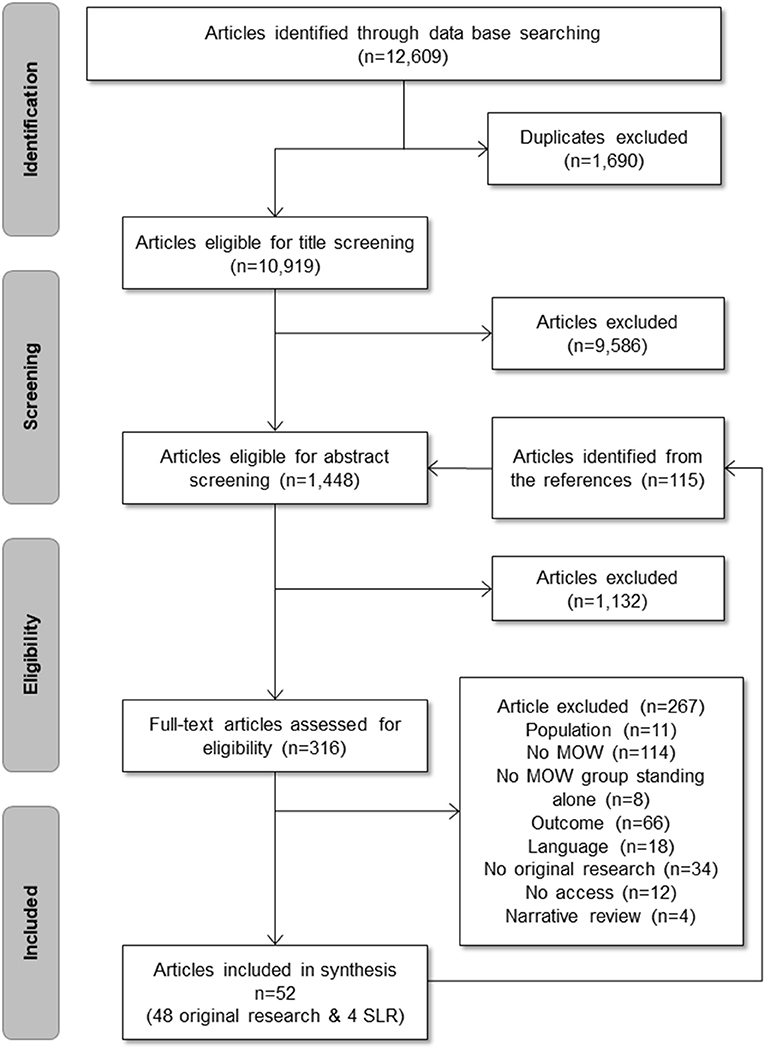
Figure 1. Flowchart.
The articles of this selection were published between years 1985 and 2020, most of them being published after 2000 (n = 34) (Table 1). More than half of these studies were conducted in the USA (n = 32), and two recurrent authors can be identified: Joseph Sharkey and Edward Frongillo. The size of the samples that could be reached varied greatly depending on the studies (ranging from 12 to 4,017 participants). Thirty studies of the selection were cross-sectional, and 18 were longitudinal with follow-up times between 10 days and 2 years (Table 1). In addition, 15 studies implemented a between-subject design while 12 studies implemented a within-subject design; 21 studies were observational (no group nor condition comparison).
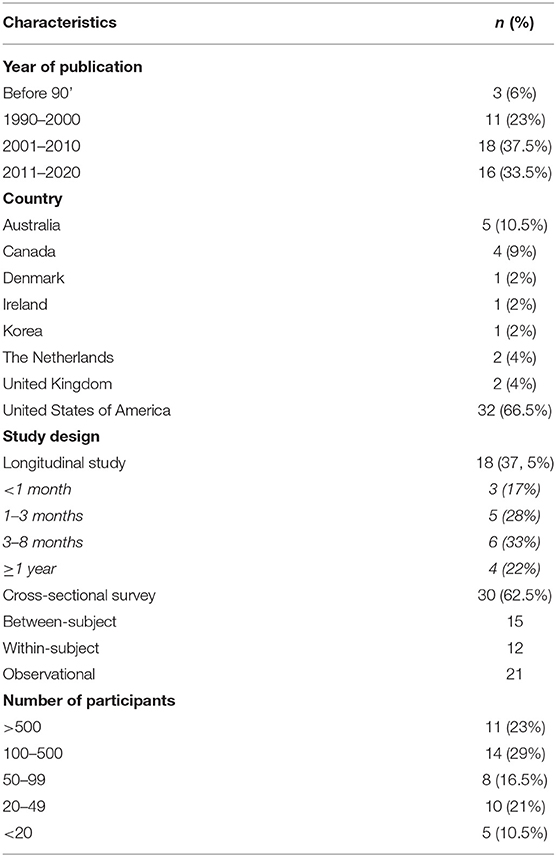
Table 1. Characteristics of the systematic literature review articles.
After conducting this descriptive summary of the collected studies related to the nutritional issue of home-delivered meal recipients, the three following topics were addressed:
- Characterization of the nutritional risk among older home-delivered meal recipients.
- Comparison of home-delivered meal recipients with non-recipients: does receiving home-delivered meal provide a nutritional benefit compared to when home-delivered meal is not received?
- Improvement of home-delivered meal service: which nutritional interventions are effective to improve the nutritional status of home-delivered meal recipients?
Methodological Quality
The methodological quality of the included studies was in general good with an average quality score of 0.81 (standard deviation: 0.13) ranging from 0.54 (24) to 1 (25–27) (Appendix 1). Overall, the control of confounding factors and the characterization of participants were poorly rated in the selected studies. This was because most of the studies did not consider all the factors established as possible confounding variables in studies on older adults: age, gender, diseases, drug intake, functional and cognitive status, socioeconomic status, and dental status. The quality variable related to the outcome was also poorly rated, mainly because several studies measured nutrient intake using only one 24-h recalls and not three (2 weekdays and 1 weekend day) as it is generally recommended (28). Finally, the quality variable that was the most poorly rated was the description quality of HDM service: very few studies provided information about the HDM service provided to the participant (How many meals are delivered per week? Which meals are delivered—breakfast, lunch, dinner? What do they contain—starter, main dish, dairy product, dessert.? How are the meals delivered: frozen, cold, hot?).
Characterization of the Nutritional Risk Among Older Home-Delivered Meal Recipients
Table 2 shows the 22 articles from the systematic literature review, which provide information about the nutritional risk among home-delivered meals recipients.
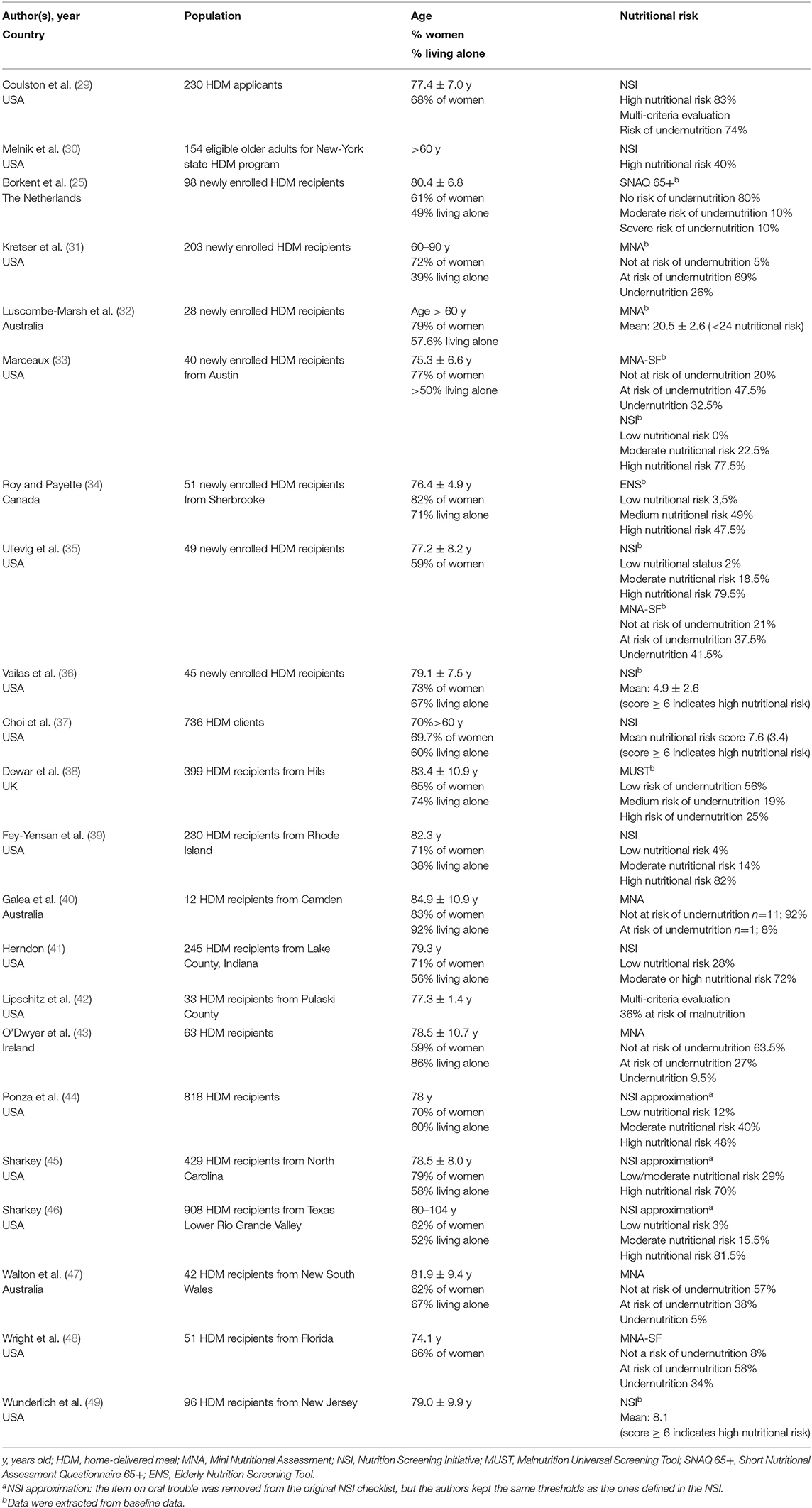
Table 2. Characterization of nutritional risk in HDM applicants and recipients.
Across the 22 studies, eight different screening methods were used. The Nutrition Screening Initiative checklist (NSI) was the most frequently used [n = 12 articles; 24–34, 88]. The NSI has been developed thanks to a collaborative effort between the American Dietetic Association, the American Academy of Family Physicians, and the National Council on the Aging (50, 51). The Mini Nutritional Assessment (MNA) or its short form (MNA-SF) are used in eight articles (31–33, 35, 40, 43, 47, 48). The MNA and MNA-SF are validated tools developed by the International Association of Geriatrics and Gerontology (52). The other tools were the following: the Elderly Nutrition Screening Tool (ENS) (34), the Malnutrition Universal Screening Tool (MUST) (38), and the Short Nutritional Assessment Questionnaire 65+ (SNAQ 65+) (25). Finally, two articles relied on a multi-criterion evaluation to diagnose undernutrition. In Coulston et al. (29), respondents were diagnosed at risk of undernutrition if they met at least one criterion among the following criteria: anthropometric measurements, dietary intakes, and blood sample analysis. In Lipschitz et al. (42), respondents were diagnosed at risk of undernutrition if they met at least one criterion among the following criteria: food intake, ideal body weight, albumin, and Total Iron Binding Capacity.
Nine studies assessed the nutritional status of home-delivered meal applicants or newly enrolled recipients. All these studies but one highlighted the nutritional frailty of this population, with a prevalence for nutritional risk or undernutrition ranging from 79 to 100%. It should be noted that four studies were carried out in the USA, in the context of the Old American Act (OAA) which specifically targets older people with the greatest economic or social need. In the study of Borkent et al. (25) conducted in The Netherlands with the SNAQ 65+ tool, only 20% of newly enrolled HDM were at risk of undernutrition. In parallel, in the study of Sahyoun et al. (53) (n = 566), 39% of the older adults receiving HDM after hospital discharge reported a fair or poor appetite, and in the study of Frongillo et al. (54) (n = 4,019), 17.5% of the older adults eligible of the HDM program reported not eating for 1 day or more. Luscombe-Marsh et al. (32) as well as Vailas et al. (36) reported respectively average MNA (20.5 ± 2.6) and NSI (4.9 ± 2.6) scores revealing a nutritional risk.
Eleven studies assessed the nutritional status of home-delivered meal recipients. Four studies reported that about 40% of their studied sample were at moderate or high nutritional risk [32.5% in O'Dwyer et al. (43); 36% in Lipschitz et al. (42); 43% in Walton et al. (47); 44% in Dewar et al. (38)]. Six studies (all in the USA) reported a high prevalence for nutritional risk or undernutrition, ranging from 70 to 96% (39, 41, 44–46, 48). In addition, Choi et al. (37) and Wunderlich et al. (49) reported respectively average NSI scores (7.6 and 8.1) corresponding to a high nutritional risk. Only one study reported a very low prevalence for undernutrition (8%), but the studied sample only included 12 participants (40).
In a very interesting study, Melnik et al. (30) randomly selected households in the New York state. If the household included at least one person aged 60 years or older, the authors determine his/her eligibility for HDM (e.g., homebound, lack of family support, unable to shop/to prepare their own meals). Overall, eligibility status was determined for more than 4,500 older adults. Finally, a nutritional assessment was performed in a subset of particularly needy HDM eligible adults (n = 146) and in a random subset of non-eligible older adults (n = 408). The results showed that 40% of the HDM eligible group were at high nutritional risk (NSI score) against 15% in the non-eligible group.
Five studies reported data on weight loss or underweight. In two large cohort studies conducted in HDM recipients, one from North Carolina, USA (45), n = 1,026, and a second one from Texas, USA (46), n = 908, respectively 26% and 43% of the respondents reported an unintended weight change of 10 pounds in the last 6 months. Herndon (41) reported that 11% HDM recipient had lost at least 10 pounds (4.5 kg) in the last 6 months. In a study conducted with 244 HDM recipients from New York state, Roe (55) reported that 33 and 11% of the respondents were respectively underweight and overweight. However, O'Dwyer et al. (43) reported that only 3% of HDM recipient were underweight (<18.5 kg/m2).
Ten articles explored food intake in HDM recipients—all these studies were conducted in North America but one in Australia (Table 3). Congruently with the nutritional frailty reported in the studies depicted in Table 2, the studies presented in Table 3 highlight that HDM recipients hardly reached the Recommended Daily Allowance (RDA) for energy and in a lesser extent for protein (24, 26, 42, 44, 56–60). For instance, the large survey of Ponza (44) conducted on 818 older adults enrolled in an HDM program funded by OAA showed that energy and protein intakes were below two-thirds of the RDA for 44 and 14% of the sample, respectively. Borkent et al. (25) showed that only 27% of newly enrolled HDM recipients reached an intake of 1.2 g protein/kg body weight/day—the recommended allowance for this population.
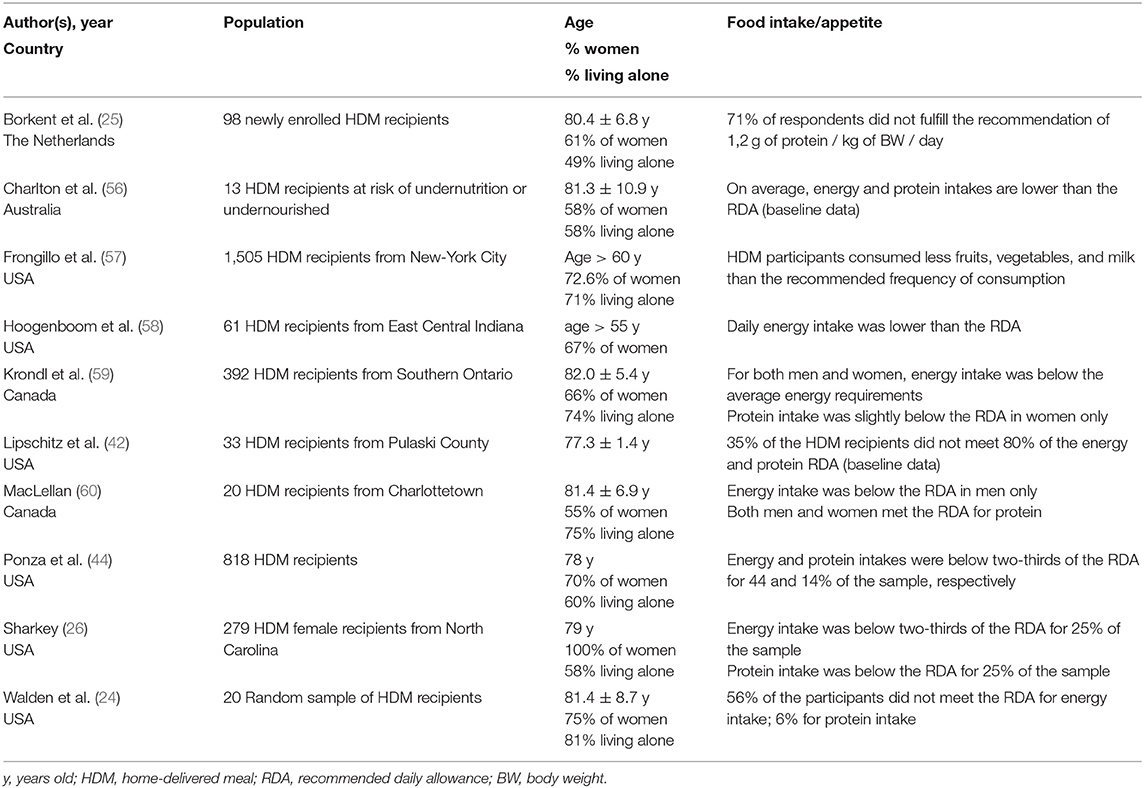
Table 3. Food intake in HDM recipients.
Interestingly, Foglerlevitt et al. (61) measured the rate of consumption of delivered meals by HDM recipients and observed that meal utilization of the delivered meals was 81% for energy and 83% for protein. Furthermore, Galea et al. (40) observed that home-delivered meals met the nutritional recommended guidelines in terms of energy and protein, but only if all the three components of the meal were ordered (soup, main dish, dessert).
Comparison of Nutritional Outcomes Between Recipients and Non-recipients of Home-Delivered Meal Service
Eighteen studies compared the nutritional outcomes (food and/or nutrient intakes, body weight, or nutritional status) between a situation where the older participants are receiving home-delivered meals and a situation where participants are not receiving home-delivered meals (Table 4). These studies include one randomized control trial (62), eight parallel-group design studies (3, 4, 32, 34, 63–66), and two cross-sectional studies (67, 68), all of these studies comparing a HDM group vs. a non-HDM group. Four pre–post studies (33, 35, 48, 69) included newly enrolled HDM recipients to be followed up over 2 or 3 months after implementing a home-delivery meal service. Finally, three within-subject design studies (24, 47, 70) compared food intake between 1 day with HDM and 1 day without HDM.
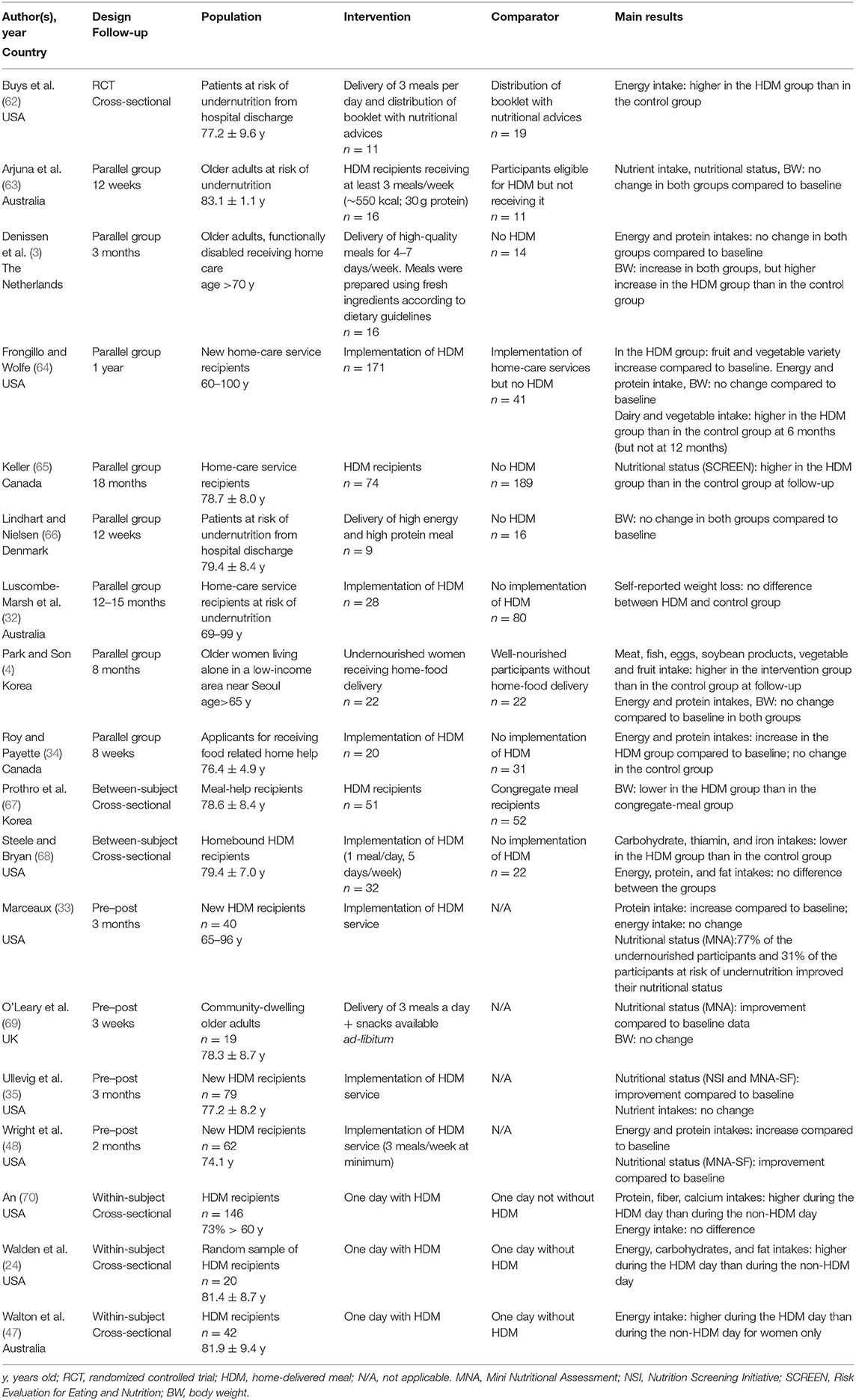
Table 4. Comparison of nutritional outcomes between recipients and non-recipients of home-delivered meal service.
Six articles reported an improvement of energy intake with HDM (24, 34, 47, 48, 62, 64) while six observed no difference between a HDM vs. non-HDM situation (3, 33, 35, 63, 68, 70). Six articles reported an improvement of protein intake with HDM (33, 34, 48, 64, 70), and 1 observed no differences between a HDM vs. non-HDM situation (47). In parallel, Frongillo and Wolfe (64) and Park and Son (4) reported higher meat consumption in HDM recipients than in non-HDM participants. Interestingly, the three within-subject articles showed higher energy and/or protein intakes when participants received a home-delivered meal than when they cooked their own meal (24, 47, 70).
None of the studies observed an improvement of body weight with HDM (4, 32, 64, 66, 67, 69) except for Denissen et al.'s (3). The latter observed a higher body weight increase in participants who have received high-quality HDM for 3 months (nutritious and appealing meals prepared with fresh ingredients) compared to participants who did not receive HDM meanwhile. Interestingly, Prothro and Rosenbloom (67) observed lower body weight in HDM recipients compared to older adults taking part in congregate meals.
Finally, all the studies that have looked at the nutritional status observed a decrease of the nutritional risk with HDM (33, 35, 48, 65, 69). For instance, Marceaux (33) observed in newly enrolled HDM recipients that 31% of the participants at risk of undernutrition and 77% of the undernourished participants improved their nutritional status after receiving HDM for 3 months.
Impact of an Improved Home-Delivered Meal Service on Nutritional Outcomes Compared to a Regular Service
Nine studies assessed the impact of an “improved” HDM service on nutritional outcomes compared to a regular service (Table 5). Improvement consisted in providing energy and/or protein enriched meals and/or snacks [six studies: 21, 44, 45, 49, 56, 64], in providing additional meals and/or snack (e.g., breakfast) to the regular offer (31, 71), or in providing dietetic counseling (49).
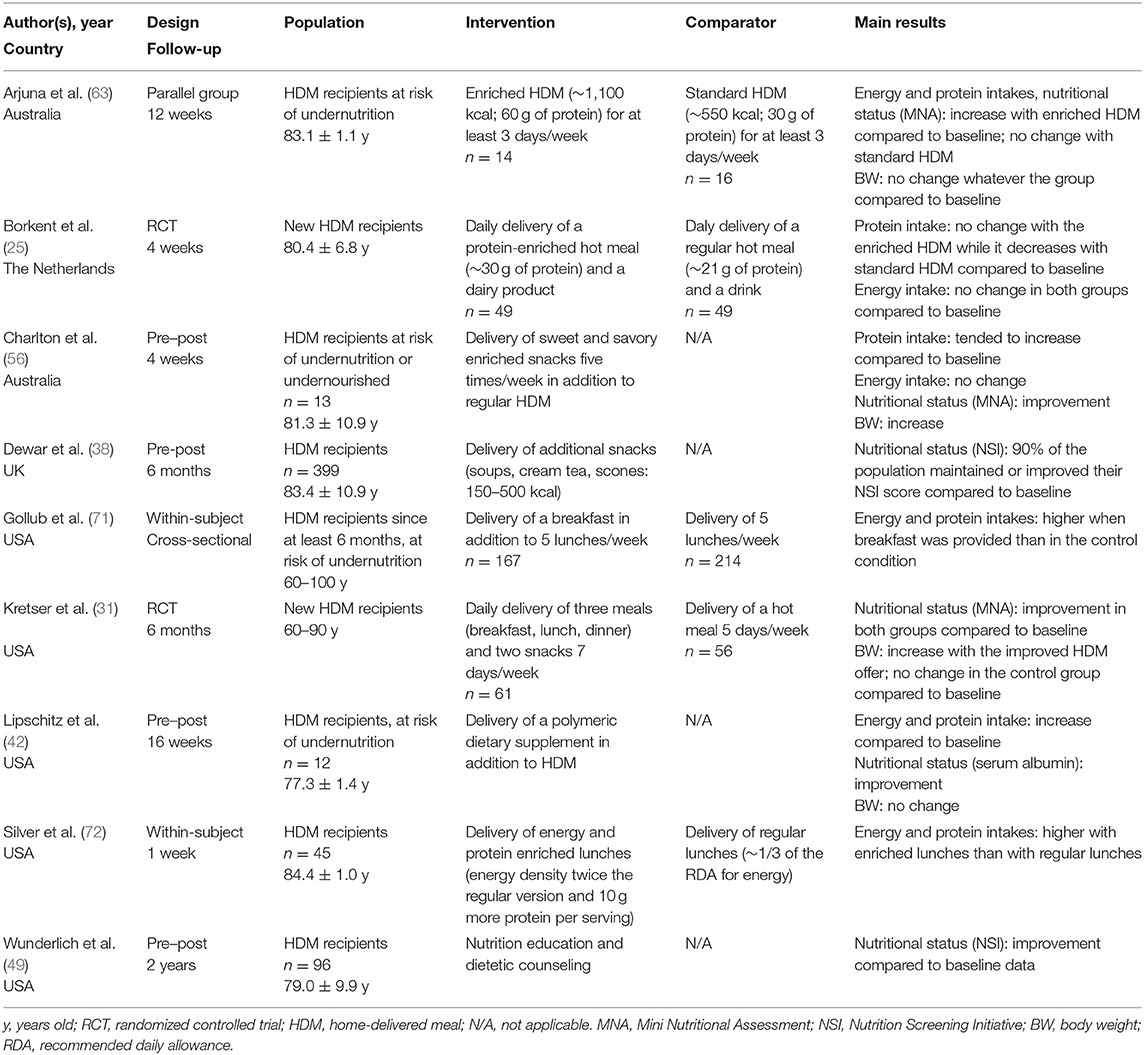
Table 5. Impact of an improved HDM service on nutritional outcome compared to a regular service.
Providing enriched home-delivered meals led to a stabilization (25) or an increase of energy and/or protein intake as well as to an improvement of the nutritional status (38, 42, 56, 63). For instance, in Arjuna et al. (63), HDM recipients at risk of undernutrition in the improved condition were delivered with meals containing twice as much energy and protein as the regular version. After 12 weeks, results showed an increase of energy and protein intakes as well as a decrease of the nutritional risk (MNA) with the enriched HDM offer while no change was observed with the regular HDM offer. Borkent et al. (25) observed that protein intake remained stable when newly enrolled HDM recipients were provided with enriched hot meals while it decreased with the provision of a regular hot meal. However, provided enriched meals do not guarantee that people will meet the recommended nutritional allowance. In Borkent et al. (25), about two-thirds of the enriched HDM group did not reach the threshold of 1.2 g protein/kg of body weight/day (they were about 90% in the regular HDM group). A similar result was observed for energy intake in Charlton et al. (56).
Providing three meals and two snacks seven days per week led to an increase of body weight compared to HDM recipients who received a hot meal 5 days per week (31). Providing breakfasts in addition to lunches led to an increase of energy and protein intake compared to HDM recipients who received only lunches (71). Finally, providing dietetic counseling led to an improvement of the nutritional status (NSI) in HDM recipients after 2 years of follow-up (49).
Discussion
Literature inquiry led to the identification of four systematic literature reviews close to the scope of the present review. The systematic review of Campbell et al. (13) targeted all studies related to home-delivered meals and included 80 articles. This literature review did not focus on older adults (the review included studies on people aged 45+ years). Included articles were sorted according to their experimental design, each design including various outcomes (e.g., satisfaction, food insecurity, nutritional outcomes, health outcomes, care expenditures). Campbell et al. (13) provided few conclusions about the nutritional issue in home-delivered meal recipients. Rather, they provided a detailed overview of the different types of studies that have been conducted on home-delivered meal services and recipients. Two systematic literature reviews addressed a topic close to our second question (comparison of home-delivered meal recipients with non-recipients). However, the one of Zhu and An (16) was restricted to studies conducted in the USA, in relationship with the Older Americans Act. This review concluded that the US home-delivered meal programs improve diet and increase nutrient intakes among recipients. The recent review of Walton et al. (15) assessed the impact of receiving meal services on nutritional intake compared to when no meal services are received in older adults living at home. In this review, meal services were not only restricted to home-delivered meals but also included congregate meals. The results highlighted a positive impact of home-delivered meals on energy and protein intake in older adults. However, this review did not explore the impact of meal services on the nutritional status and the undernutrition risk among the older population. Finally, the systematic literature review of IJmker-Hemink et al. (14) explored the effectiveness of various interventions to improve nutrition and satisfaction outcomes in adults receiving home-delivered meals. This review led to the identification of 12 studies assessing the impact of an improved home-delivered meal service on nutritional outcomes (14 assessed satisfaction outcomes). However, in their review, the authors did not separate the studies assessing the impact of providing HDM service vs. no HDM service (as we did on Table 4) from assessing the impact of an improved HDM service (e.g., with dietetic counseling, enriched meal) vs. providing a standard HDM service (as we did on Table 5).
The present review aimed at compiling all the studies related to the nutritional issue in home-delivered meal older recipients. Whether older people are newly enrolled in an HDM service or are already beneficiary of an HDM service, the prevalence of the nutritional risk is high or even very high. Over the 19 studies included in our review, 15 studies displayed a prevalence higher than 35%—higher than 70% in 10 studies. In parallel, nine studies highlighted that HDM recipients hardly reached the Recommended Daily Allowance for energy and to a lesser extent for protein. In fact, this service is rarely a comfort service, but it generally counterweights the difficulties encountered by older people in feeding themselves (73). Several authors reported that older beneficiaries of HDM service have less social contact and are less mobile compared to the general population (1, 53, 74, 75). In numerous countries (and in particular in the USA where the majority of the studies were conducted), the HDM service often targets older people with a low socioeconomic status, with high levels of food insecurity (76, 77). All these factors—loneliness, functional disabilities, poor financial resources—are known to be risk factors for undernutrition (37, 78–80).
Results of the present literature review highlight that providing older people with HDM service improves their nutritional status, leading to a decrease in the undernutrition prevalence. Most of the studies also show that providing home-delivered meals leads to a higher energy intake (seven studies over 12) and protein intake (five studies over six). None reported a decline in dietary intake. These results are in line with previous literature reviews' findings. Zhu and An (16) concluded that the US home-delivered meal programs improve diet and increase nutrient intakes among recipients. Similarly, Walton et al. (15) highlighted a positive impact of home-delivered meals on energy and protein intake in older adults. In addition, several studies showed that improving the HDM service by providing dietetic counseling to the beneficiaries, or providing additional snacks/meals, or providing calorie and/or protein enriched dishes improved the nutritional status and/or dietary intakes compared to a regular HDM service (31, 38, 42, 49, 56, 63, 71). However, providing an improved home-delivered meal service was not always enough to allow all the older recipients meeting the recommended nutritional allowance (25, 56). For instance, in Borkent et al. (25), about two-thirds of the enriched home-delivered meal group did not reach the threshold of 1.2 g protein/kg of body weight/day (81). This raises the importance of further developing new enrichment solutions to fill this gap.
It should also be noted that all these studies aimed at improving the nutritional content of home-delivered meals. However, further research should also consider improving the sensory quality of the home-delivered foods. In line with the studies carried out by Sulmont-Rossé et al. (82), it would be interesting to optimize the sensory quality of the meals by recruiting the tasting panel among HDM recipients. Improving meals according to older people's feedback led to an increase of food intake in nursing home (83). In addition, improvements could also target the quality of the service such as providing choice and providing social support during the meal. In addition, it can be hypothesized that the combination of several levers is necessary to have significant improvements in food intake rather than implementing only one lever in the fields. In fact, such multidimensional interventions were implemented in nursing homes and proved to be efficient (83–87). For instance, Kremer et al. (86) combined improvement at the product level (e.g., attractive visual presentation), at the people level (e.g., promoting choice to give the older residents more control), and at the situation level (e.g., promoting an attractive social environment) to improve the meals in nursing homes. Such improvements led to an increase in food intake (and meal enjoyment) compared to a regular nursing home setting.
Limitations and Strengths of the Present SLR
The main strength of this work is that it is a solid literature search, with a complete overview of nutritional issues in home-delivery meal older recipients. A limitation of this review is that we were not able to find the full text for 12 records, mainly because of old published years (<1990) and despite the fact that several channels were used to find them (research on the web, order from university libraries, contact of the authors… none of these articles were available online). From a methodological point of view, an important limitation highlighted by the quality evaluation is the lack of information provided by the authors on the home-delivered meal service. Most of the studies did not indicate which meals are delivered to their participants (e.g., breakfast, lunch, dinner), how often in a week they are delivered, their content (e.g., starter, main dish, dessert; nutrient content), or their presentation (e.g., portion or batch, frozen or cold or hot). However, these factors may impact the outcome variables (nutritional status, food intake) measured in the studies and possibly explain divergences observed between the results of different studies. For instance, Galea et al. (40) highlighted that home-delivered meals meet the recommended guidelines in terms of protein and energy intake, but only if the three components of the meal are ordered (main dish, soup, dessert).
Another limitation to compare the studies is the large variety of tools used to assess the nutritional risk, as it was already highlighted by the systematic review on undernutrition diagnosis tools (88). In the present review, eight different screening tools can be listed from the included studies. The most used is the Nutritional Screening Initiative (NSI) checklist, but it is only used in the US studies. Interestingly, this tool was developed in the USA based on consensus between health and social care professionals (89). Initially, this tool aimed at raising caregivers' awareness about the importance of the nutritional risk among the aged population. However, this tool is also used to screen for older adults at risk of undernutrition (50), as it is the case in the studies included in our review.
In parallel, it should be noted that most of the studies were carried out in the USA (32 over 48) which prevents the generalization of the present conclusions to other countries. Finally, it is interesting to note that very few changes in body weight were observed in longitudinal or cohort studies. Among the review selection, only one article reported a higher weight of the home-delivered meal participants in comparison to participants without home-delivered meal (3) and only two articles showed that an improved home-delivered meals service led to an increase of body weight over the time (31, 56). In eight studies, no changes in the body weight were observed, even in the long follow-up [e.g., 12 weeks in Arjuna et al. (63); 16 weeks in Lipschitz et al. (42)]. This questions the relevance of weight change as an outcome variable in such study and/or the way this outcome variable is measured [for instance, in Arjuna et al. (63), participants were weighted while they wore “light clothing,” which may have induced variability].
Conclusion
The main findings of this review can be summarized in the following points: (1) home-delivery meal older recipients are at high risk of undernutrition; (2) providing home-delivery meals may improve the nutritional status and nutrient intake; (3) this improvement is even higher when the home-delivery meal service is improved, for instance by providing dietetic counseling and adding supplementary snacks/meals or calorie- and/or protein-enriched food. However, even an improved service does not allow all the older recipients meeting their recommended nutritional allowance. The implication of these results for the structures providing home-delivered meals services is to develop innovative strategies to allow their recipients fulfilling their nutritional needs. These strategies should probably take into account both sensory issues (e.g., improving the appealing and palatability of meals), nutritional issues (e.g., providing enriched food), and the psycho-social issue (e.g., providing choice to give the older recipients more control). Finally, the implication of this review for the research is to carry out more randomized control trials and to provide a more precise description of the home-delivered service provided to the recipients to better take into account the meal frequency and content in the results.
Data Availability Statement
The original contributions presented in the study are included in the article/Supplementary Material, further inquiries can be directed to the corresponding author/s.
Author Contributions
SF: conceptualization, research, resource provision, data collection, writing original version, and visualization. PT: review and correction. JR, CM, and OM: research and data collection. VV: conceptualization, validation, review, and correction. CS-R: conceptualization, validation, review and correction, and visualization. All authors contributed to the article and approved the submitted version.
Funding
This study is part of the Ph.D. work of SF, funded by a CIFRE contract between the company Saveurs et Vie and the French Association Nationale Recherche Technologie (ANRT N°1576).
Conflict of Interest
SF and PT were employed by company Saveurs et Vie.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Supplementary Material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fnut.2021.629580/full#supplementary-material
References
2. Kaplan J, Williams C. Social components of Meals on Wheels Service. Gerontologist. (1961) 1:51–5. doi: 10.1093/geront/1.1.51
3. Denissen KFM, Janssen LMJ, Eussen SJPM, van Dongen MCJM, Wijckmans NEG, van Deurse NDM, et al. Delivery of nutritious meals to elderly receiving home care: feasibility and effectiveness. J Nutr Health Aging. (2017) 21:370–80. doi: 10.1007/s12603-016-0790-2
4. Park JK, Son SM. Nutrient intakes and serum lipid profiles are improved in elderly Korean women with home food delivery. Nutr Res. (2007) 27:78–85. doi: 10.1016/j.nutres.2006.12.007
5. United Nations Department of Economic and Social Affairs Population Division. World Population Prospects Highlights, 2019 Revision. (2019).
6. Maitre I, Van Wymelbeke V, Amand M, Vigneau E, Issanchou S, Sulmont-Rossé C. Food pickiness in the elderly: relationship with dependency and malnutrition. Food Qual Preference. (2014) 32:145–51. doi: 10.1016/j.foodqual.2013.04.003
7. Crichton M, Craven D, Mackay H, Marx W, de van der Schueren M, Marshall S. A systematic review, meta-analysis and meta-regression of the prevalence of protein-energy malnutrition: associations with geographical region and sex. Age Ageing. (2018) 48:38–48. doi: 10.1093/ageing/afy144
8. Arksey H, O'Malley L. Scoping studies: towards a methodological framework. Int J Soc Res Methodol. (2005) 8:19–32. doi: 10.1080/1364557032000119616
9. Peters MDJ, Godfrey CM, Khalil H, McInerney P, Parker D, Soares CB. Guidance for conducting systematic scoping reviews. Int J Evid Based Healthcare. (2015) 13:141–6. doi: 10.1097/XEB.0000000000000050
10. Shamseer L, Moher D, Clarke M, Ghersi D, Liberati A, Petticrew M, et al. Preferred reporting items for systematic review and meta-analysis protocols (PRISMA-P) 2015: elaboration and explanation. BMJ. (2015) 349:g7647. doi: 10.1136/bmj.g7647
11. Stone PW. Popping the (PICO) question in research and evidence-based practice. Appl Nursing Res. (2002) 15:197–8. doi: 10.1053/apnr.2002.34181
12. Kmet LM, Lee RC, Cook LS, Alberta Heritage Foundation for Medical Research University of Calgary Faculty of Medicine. Standard quality assessment criteria for evaluating primary research papers from a variety of fields. Alberta Heritage Foundation for Medical Research. (2004).
13. Campbell AD, Godfryd A, Buys DR, Locher JL. Does participation in home-delivered meals programs improve outcomes for older adults? J Nutr Gerontol Geriatr. (2015) 34:124–67. doi: 10.1080/21551197.2015.1038463
14. IJmker-Hemink VE, Dijxhoorn DN, Briseno Ozumbilla CM, Wanten GJ, van den Berg MG. Effective elements of home-delivered meal services to improve energy and protein intake: a systematic review. Nutrition. (2020) 69:110537. doi: 10.1016/j.nut.2019.06.018
15. Walton K, Rosario VA, Pettingill H, Cassimatis E, Charlton K. The impact of home-delivered meal services on the nutritional intake of community living older adults: a systematic literature review. J Human Nutr Dietet. (2020) 33:38–47. doi: 10.1111/jhn.12690
16. Zhu H, An R. Impact of home-delivered meal programs on diet and nutrition among older adults: a review. Nutr Health. (2013) 22:89–103. doi: 10.1177/0260106014537146
17. Lindegaard Pedersen J, Pedersen PU, Damsgaard EM. Nutritional follow-up after discharge prevents readmission to hospital—a randomized clinical trial. J Nutr Health Aging. (2017) 21:75–82. doi: 10.1007/s12603-016-0745-7
18. Millen B, Ohls J, Ponza M, McCool A. The elderly nutrition program: an effective national framework for preventive nutrition interventions. J Am Dietetic Assoc. (2002) 102:6. doi: 10.1016/S0002-8223(02)90055-6
19. Payette H, Coulombe C, Boutier V, Gray-Donald K. Nutrition risk factors for institutionalization in a free-living functionally dependent elderly population. J Clin Epidemiol. (2000) 53:579–87. doi: 10.1016/S0895-4356(99)00186-9
20. Soini H, Routasalo P, Lauri S. Nutrition in patients receiving home care in Finland—tackling the multifactorial problem. J Gerontol Nursing. (2006) 32:12–7. doi: 10.3928/00989134-20060401-04
21. Tsuji T, Yamamoto K, Yamasaki K, Hayashi F, Momoki C, Yasui Y, et al. Lower dietary variety is a relevant factor for malnutrition in older Japanese home-care recipients: a cross-sectional study. BMC Geriatr. (2019) 19:197. doi: 10.1186/s12877-019-1206-z
22. Vieira ER, Vaccaro JA, Zarini GG, Huffman FG. Health indicators of US older adults who received or did not receive meals funded by the Older Americans Act. J Aging Res. (2017) 2017:1–8. doi: 10.1155/2017/2160819
23. Kim K, Frongillo EA. Participation in food assistance programs modifies the relation of food insecurity with weight and depression in elders. J Nutr. (2007) 137:1005–10. doi: 10.1093/jn/137.4.1005
24. Walden O, Hayes PA, Lee DY, Montgomery DH. The provision of weekend home delivered meals by state and a pilot study indicating the need for weekend home delivered meals. J Nutr Elderly. (1989) 8:31–43. doi: 10.1300/J052v08n01_04
25. Borkent JW, Beelen J, Linschooten JO, Roodenburg AJC, de van der Schueren MAE. The ConsuMEER study: a randomised trial towards the effectiveness of protein-rich ready-made meals and protein-rich dairy products in increasing protein intake of community-dwelling older adults after switching from self-prepared meals towards ready-made meals. J Nutr Sci. (2019) 8:e30. doi: 10.1017/jns.2019.27
26. Sharkey JR, Giuliani C, Haines PS, Branch LG, Busby-Whitehead J, Zohoori N. Summary measure of dietary musculoskeletal nutrient (calcium, vitamin D, magnesium, and phosphorus) intakes is associated with lower-extremity physical performance in homebound elderly men and women. Am J Clin Nutr. (2003) 77:847–56. doi: 10.1093/ajcn/77.4.847
27. Sharkey JR. Nutrition Risk Screening: the Interrelationship of food insecurity, food intake, and unintentional weight change among homebound elders. J Nutr Elderly. (2004) 24:19–34. doi: 10.1300/J052v24n01_02
28. Sun Y, Roth DL, Ritchie CS, Burgio KL, Locher JL. Reliability and predictive validity of energy intake measures from the 24-hour dietary recalls of homebound older adults. J Am Dietet Assoc. (2010) 110:773–8. doi: 10.1016/j.jada.2010.02.003
29. Coulston AM, Craig L, Voss AC. Meals-on-wheels applicants are a population at risk for poor nutritional status. J Am Dietetic Assoc. (1996) 96:570–3. doi: 10.1016/S0002-8223(96)00157-5
30. Melnik TA, Blizniak P, Lannon PB, Porter MF, Wales KR. Home delivered meals program in New York State: population-based estimates of eligibility, program targeting, and nutritional risk. J Nutr Elderly. (1999) 18:33–44. doi: 10.1300/J052v18n03_03
31. Kretser AJ, Voss T, Kerr WW, Cavadini C, Friedmann J. Effects of two models of nutritional intervention on homebound older adults at nutritional risk. J Am Dietet Assoc. (2003) 103:329–36. doi: 10.1053/jada.2003.50052
32. Luscombe-Marsh N, Chapman I, Visvanathan R. Hospital admissions in poorly nourished, compared with well-nourished, older south Australians receiving “Meals on Wheels”: findings from a pilot study: nutrition and “Meals on Wheels.” Austral J Ageing. (2014) 33:164–9. doi: 10.1111/ajag.12009
33. Marceaux S. The Impact of Participation in Meals on Wheels and More (MOWAM) in Austin, TX, on dietary intake and health status. Austin, TX: Texas State University-San Marcos. (2012).
34. Roy M-A, Payette H. Meals-on-wheels improves energy and nutrient intake in a frail free-living elderly population. J Nutr Health Aging. (2006) 10:554–60.
35. Ullevig SL, Sosa ET, Crixell S, Uc E, Greenwald B, Marceaux S, et al. Impact of home-delivered meals on nutrition status and nutrient intake among older adults in central Texas. J Nutr Health Aging. (2018) 22:861–8. doi: 10.1007/s12603-018-1038-0
36. Vailas L, Nitzke S, Becker M, Gast J. Risk indicators for malnutrition are associated inversely with quality of life for participants in meal programs for older adults. J Am Dietet Assoc. (1998) 98:123. doi: 10.1016/S0002-8223(98)00123-0
37. Choi NG, Teeters M, Perez L, Farar B, Thompson D. Severity and correlates of depressive symptoms among recipients of Meals on Wheels: age, gender, and racial/ethnic difference. Aging Mental Health. (2010) 14:145–54. doi: 10.1080/13607860903421078
38. Dewar M, Dickinson A, Smeeton N. Tracking and treating malnutrition: a retrospective observational study of the nutritional status of vulnerable people accessing a meals-on-wheels (MOW) service. Primary Health Care Res Dev. (2020) 21:e19. doi: 10.1017/S1463423620000195
39. Fey-yensan N, English C, Ash S, Wallace C, Museler H. Food safety risk identified in a population of elderly home-delivered meal participants. J Am Dietetic Assoc. (2001) 101:259. doi: 10.1016/S0002-8223(01)00259-0
40. Galea SA, Walton K, Charlton K, Mcmahon A. What's on the tray? Nutritional intake of meals on wheels clients. Nutr Dietet. (2013) 70:79–80. doi: 10.1111/1747-0080.12028
41. Herndon AS. Using the Nutrition Screening Initiative to Survey the nutritional status of clients participating in a home delivered meals program. J Nutr Elderly. (1995) 14:15–29. doi: 10.1300/J052v14n04_02
42. Lipschitz D, Mitchell C, Steele R, Milton K. Nutritional-evaluation and supplementation of elderly subjects participating in a meals-on-wheels program. J Parenteral Enteral Nutr. (1985) 9:343–7. doi: 10.1177/0148607185009003343
43. O'Dwyer C, Corish CA, Timonen V. Nutritional status of Irish older people in receipt of meals-on-wheels and the nutritional content of meals provided. J Human Nutr Dietet. (2009) 22:521–7. doi: 10.1111/j.1365-277X.2009.00992.x
44. Ponza M. Serving Elders at Risk The Older Americans Act Nutrition Programs: National Evaluation of The Elderly Nutrition Program 1993–1995. Washington, DC: U.S. Department of Health and Human Services - Office of the Assistant Secretary for Aging (1996). p. 331.
45. Sharkey JR. Responding to the challenges of recruiting and retaining homebound older men and women in a study of nutrition and function: a university-community collaborative strategy. J Nutr Elderly. (2002) 22:15–35. doi: 10.1300/J052v22n02_02
46. Sharkey J. Variations in nutritional risk among Mexican American and non-Mexican American homebound elders who receive home-delivered meals. J Nutr Elderly. (2004) 23:1–19. doi: 10.1300/J052v23n04_01
47. Walton K, Charlton KE, Manning F, McMahon AT, Galea S, Evans K. The nutritional status and energy and protein intakes of MOW clients and the need for further targeted strategies to enhance intakes. Appetite. (2015) 95:528–32. doi: 10.1016/j.appet.2015.08.007
48. Wright L, Vance L, Sudduth C, Epps JB. The impact of a home-delivered meal program on nutritional risk, dietary intake, food security, loneliness, and social well-being. J Nutr Gerontol Geriatr. (2015) 34:218–27. doi: 10.1080/21551197.2015.1022681
49. Wunderlich S, Bai Y, Piemonte J. Nutrition risk factors among home delivered and congregate Fmeal participants: need for enhancement of nutrition education and counseling among home delivered meal participants. J Nutr Health Aging. (2011) 15:768–73. doi: 10.1007/s12603-011-0090-9
50. Dwyer J. Strategies to Detect and Prevent Malnutrition in the Elderly: The Nutrition Screening Initiative. Nutrition Today (USA). (1994). Available online at: https://agris.fao.org/agris-search/search.do?recordID=US9611527 (accessed October 2020).
51. Posner BM, Jette AM, Smith KW, Miller DR. Nutrition and health risks in the elderly: the nutrition screening initiative. Am J Public Health. (1993) 83:972–8. doi: 10.2105/AJPH.83.7.972
52. Vellas B, Villars H, Abellan G, Soto ME, Rolland Y, Guigoz Y, et al. Overview of the MNA® - Its history and challenges. J Nutr. (2006) 10:11.
53. Sahyoun NR, Anyanwu UO, Sharkey JR, Netterville L. Recently hospital-discharged older adults are vulnerable and may be underserved by the Older Americans Act nutrition program. J Nutr Elderly. (2010) 29:227–40. doi: 10.1080/01639361003772608
54. Frongillo EA, Rauschenbach BS, Roe DA, Williamson DF. Characteristics related to elderly persons' not eating for 1 or more days: implications for meal programs. Am J Public Health. (1992) 82:600–2. doi: 10.2105/AJPH.82.4.600
55. Roe DA. In-home nutritional assessment of inner-city elderly. Am Inst Nutr.(1990) 120(Suppl.11):1538–43. doi: 10.1093/jn/120.suppl_11.1538
56. Charlton KE, Walton K, Moon L, Smith K, Mcmahon AT, Ralph F, et al. “It could probably help someone else but not me”: a feasibility study of a snack programme offered to meals on wheels clients. J Nutr Health Aging. (2013) 17:364–9. doi: 10.1007/s12603-013-0035-6
57. Frongillo Edward A, Cantor MH, MacMillan T, Issacman TD, Sherrow R, Henry M, et al. Who are the recipients of meals-on-wheels in New York City? A profile of based on a representative sample of Meals-on-Wheels recipients, part II. Care Manag J. (2010) 11:129–39. doi: 10.1891/1521-0987.11.2.129
58. Hoogenboom MS, Spangler AA, Crose R. Functional status and nutrient intake from the council on aging meal and total daily intake of congregate, adult day care and homebound program participants. J Nutr Elderly. (1998) 17:1–18. doi: 10.1300/J052v17n03_01
59. Krondl M, Lau D, Coleman P, Stocker G. Tailoring of nutritional support for older adults in the community. J Nutr Elderly. (2003) 23:17–32. doi: 10.1300/J052v23n02_02
60. Maclellan DL. Contribution of home-delivered meals to the dietary intake of the elderly. J Nutr Elderly. (1997) 16:17–32. doi: 10.1300/J052v16n03_02
61. Foglerlevitt E, Lau D, Csima A, Krondl M, Coleman P. Utilization of home-delivered meals by recipients 75 years of age or older. J Am Dietet Assoc. (1995) 95:552–7. doi: 10.1016/S0002-8223(95)00150-6
62. Buys DR, Campbell AD, Godfryd A, Flood K, Kitchin E, Kilgore ML, et al. Meals enhancing nutrition after discharge: findings from a pilot randomized controlled trial. J Acad Nutr Dietet. (2017) 117:599–608. doi: 10.1016/j.jand.2016.11.005
63. Arjuna T, Miller M, Soenen S, Chapman I, Visvanathan R, Luscombe-Marsh ND. Serve size and estimated energy and protein contents of meals prepared by ‘Meals on Wheels' south Australia Inc.: findings from a Meal Audit Study. Foods. (2018) 7:26. doi: 10.3390/foods7020026
64. Frongillo EA, Wolfe WS. Impact of Participation in home-delivered meals on nutrient intake, dietary patterns, and food insecurity of older persons in New York State. J Nutr Elderly. (2010) 29:293–310. doi: 10.1080/01639366.2010.499094
65. Keller HH. Meal programs improve nutritional risk: a longitudinal analysis of community-living seniors. J Am Dietet Assoc. (2006) 106:1042–8. doi: 10.1016/j.jada.2006.04.023
66. Lindhardt T, Nielsen MH. Older patients' use of technology for a post-discharge nutritional intervention – a mixed-methods feasibility study. Int J Med Inform. (2017) 97:312–21. doi: 10.1016/j.ijmedinf.2016.10.017
67. Prothro JW, Rosenbloom CA. Body measurements of black and white elderly persons with emphasis on body composition. Gerontology. (1995) 41:22–38. doi: 10.1159/000213659
68. Steele MF, Bryan JD. Dietary intake of homebound elderly recipients and nonrecipients of home-delivered meals. J Nutr Elderly. (1986) 5:23–34. doi: 10.1300/J052v05n02_04
69. O'Leary MF, Barreto M, Bowtell JL. Evaluating the effect of a home-delivered meals service on the physical and psychological well-being of a UK population of older adults – a pilot and feasibility study. J Nutr Gerontol Geriatr. (2020) 39:1–15. doi: 10.1080/21551197.2019.1684417
70. An R. Association of home-delivered meals on daily energy and nutrient intakes: findings from the national health and nutrition examination surveys. J Nutr Gerontol Geriatr. (2015) 34:263–72. doi: 10.1080/21551197.2015.1031604
71. Gollub EA, Weddle DO. Improvements in nutritional intake and quality of life among frail homebound older adults receiving home-delivered breakfast and lunch. J Am Dietet Assoc. (2004) 104:1227–35. doi: 10.1016/j.jada.2004.05.204
72. Silver HJ, Dietrich MS, Castellanos VH. Increased energy density of the home-delivered lunch meal improves 24-hour nutrient intakes in older adults. J Am Dietet Assoc. (2008) 108:2084–9. doi: 10.1016/j.jada.2008.09.005
73. Fleury S, Sulmont-Rossé C, Tronchon P, Wymelbeke VV, Roux S. Le portage de repas à domicile: processus d'installation et d'appropriation de ce service par les personnes âgées en perte d'autonomie. Nutr Clin Métabol. (in press). doi: 10.1016/j.nupar.2020.10.004
74. Chumbler N, Beverly C, Beck C. Determinants of in-home health and support service utilization for rural older adults. Res Sociol Health Care. (1998) 27:15–205.
75. De Graaf C, Van Staveren W, Sneeuw K, Stam N. The elderly and food services: consumers' perspective of a meals-on-wheels service. In: Somogyi JC and Koskinen EH, editors, Forum of Nutrition, Vol. 45. (1990). p. 133–42. doi: 10.1159/000418684
76. DiMaria-Ghalili RA, Laverty N, Baron K, Nasser JA. Benchmarking a home-delivered meal program's annual satisfaction survey: a metropolitan area neighborhood nutrition alliance (MANNA) initiative in Philadelphia. J Nutr Gerontol Geriatr. (2015) 34:189–206. doi: 10.1080/21551197.2015.1035824
77. Lee L-C, Tsai AC, Wang J-Y. Need-based nutritional intervention is effective in improving handgrip strength and Barthel Index scores of older people living in a nursing home: a randomized controlled trial. Int J Nurs Stud. (2015) 52:904–12. doi: 10.1016/j.ijnurstu.2015.01.008
78. Krassie J, Smart C, Roberts DCK. A Review of the nutritional needs of Meals on Wheels consumers and factors associated with the provision of an effective Meals on Wheels service—an Australian perspective. Eur J Clin Nutr. (2000) 54:275–80. doi: 10.1038/sj.ejcn.1600790
79. Locher JL, Robinson CO, Roth DL, Ritchie CS, Burgio KL. The effect of the presence of others on caloric intake in homebound older adults. J Gerontol Ser A Biol Sci Med Sci. (2005) 60:1475–8. doi: 10.1093/gerona/60.11.1475
80. van der Pols-Vijlbrief R, Wijnhoven HAH, Visser M. Perspectives on the causes of undernutrition of community-dwelling older adults: a qualitative study. J Nutr Health Aging. (2017) 21:1200–9. doi: 10.1007/s12603-017-0872-9
81. Deutz NEP, Bauer JM, Barazzoni R, Biolo G, Boirie Y, Bosy-Westphal A, et al. Protein intake and exercise for optimal muscle function with aging: recommendations from the ESPEN Expert Group. Clin Nutr. (2014) 33:929–36. doi: 10.1016/j.clnu.2014.04.007
82. Sulmont-Rossé C, Maître I, Feyen V, Vandenberghe-Descamps M, Labouré H, Feron G, et al. Quels aliments pour maintenir la prise alimentaire chez les personnes âgées et prévenir la dénutrition?? Innov Agron. (2018) 65:99–111. doi: 10.15454/1.5408041258793853E12
83. Van Wymelbeke V, Sulmont-Rossé C, Feyen V, Issanchou S, Manckoundia P, Maître I. Optimizing sensory quality and variety: an effective strategy for increasing meal enjoyment and food intake in older nursing home residents. Appetite. (2020) 153:104749. doi: 10.1016/j.appet.2020.104749
84. Desai J, Winter A, Young KWH, Greenwood CE. Changes in type of foodservice and dining room environment preferentially benefit institutionalized seniors with low body mass indexes. J Am Dietet Assoc. (2007) 107:808–14. doi: 10.1016/j.jada.2007.02.018
85. Elmståhl S, Blabolil V, Fex G, Küller R, Steen B. Hospital nutrition in geriatric long-term care medicine. Comprehensive Gerontol. (1987) 1:29–33. doi: 10.1093/ageing/16.1.73
86. Kremer S, Derks J, Nijenhuis-De Vries M, Boer EPJ, Gorselink M. Effect of a holistic meal and ambiance concept on main meal enjoyment and food intake of dutch nursing home residents: a pilot study. J Aging Res Clin Practice. (2012) 1:237–44.
87. Nijs KAND, de Graaf C, Kok FJ, van Staveren WA. Effect of family style mealtimes on quality of life, physical performance, and body weight of nursing home residents: cluster randomised controlled trial. BMJ. (2006) 332:1180–4. doi: 10.1136/bmj.38825.401181.7C
88. van Bokhorst–de van der Schueren MAE, Guaitoli PR, Jansma EP, de Vet HCW. A systematic review of malnutrition screening tools for the nursing home setting. J Am Med Directors Assoc. (2014) 15:171–84. doi: 10.1016/j.jamda.2013.10.006
Keywords: aged, older adults, meals-on-wheels, malnutrition, food intake, body weight
Citation: Fleury S, Tronchon P, Rota J, Meunier C, Mardiros O, Van Wymelbeke-Delannoy V and Sulmont-Rossé C (2021) The Nutritional Issue of Older People Receiving Home-Delivered Meals: A Systematic Review. Front. Nutr. 8:629580. doi: 10.3389/fnut.2021.629580
Received: 15 November 2020; Accepted: 29 January 2021;
Published: 04 March 2021.
Edited by:
Kazim Sahin, Firat University, TurkeyReviewed by:
Meghit Boumediene Khaled, University of Sidi-Bel-Abbès, AlgeriaGülden Pekcan, Hasan Kalyoncu University, Turkey
Copyright © 2021 Fleury, Tronchon, Rota, Meunier, Mardiros, Van Wymelbeke-Delannoy and Sulmont-Rossé. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Ségolène Fleury, segolene.fleury@inrae.fr