 Arie Carneiro1,2†
Arie Carneiro1,2† Álan Roger Gomes Barbosa1†
Álan Roger Gomes Barbosa1† Lucas Seiti Takemura1
Lucas Seiti Takemura1 Paulo Priante Kayano1
Paulo Priante Kayano1 Natasha Kouvaleski Saviano Moran2
Natasha Kouvaleski Saviano Moran2 Carolina Ko Chen1Marcelo Langer Wroclawski1,2Gustavo Caserta Lemos1Isabela Werneck da Cunha3Marcos Takeo Obara4Marcos Tobias-Machado2
Carolina Ko Chen1Marcelo Langer Wroclawski1,2Gustavo Caserta Lemos1Isabela Werneck da Cunha3Marcos Takeo Obara4Marcos Tobias-Machado2 Adam G. Sowalsky5
Adam G. Sowalsky5 Bianca Bianco6*
Bianca Bianco6*- 1Department of Urology, Hospital Israelita Albert Einstein, São Paulo, Brazil
- 2Department of Pathology, Hospital Israelita Albert Einstein, São Paulo, Brazil
- 3Department of Pathology, Rede D'OR São Luiz, São Paulo, Brazil
- 4Department of Pathology, Hospital Israelita Albert Einstein, São Paulo, Brazil
- 5Laboratory of Genitourinary Cancer Pathogenesis, Center for Cancer Research, National Cancer Institute, National Institutes of Health, Bethesda, MD, United States
- 6Human Reproduction and Genetics Center, Faculdade de Medicina do ABC, Santo André, Brazil
Background: Prostate cancer (PCa) is a heterogeneous disease that lends itself toward numerous therapeutic options depending on its risk stratification. One of the greatest challenges in PCa urologic practice is to select patients who should be referred for biopsy and, for those patients who are diagnosed with cancer, to differentiate between patients with indolent disease from those with an unfavorable prognosis and, to determine ideal patient management and avoid unnecessary interventions. Accordingly, there is a growing body of literature reporting immunohistochemical studies with the objective of determining a prostate cancer prognosis. Among the most frequent biomarkers studied are Ki-67, p53, PTEN, MYC, and ERG. Based on these findings, we systematically reviewed articles that assessed the role of these main prognostic markers in prostate cancer.
Methods: Consistent with PRISMA guidelines, we performed a systematic literature search throughout the Web of Science and PubMed Medline databases. We considered all types of studies evaluating the role of Ki-67, p53, PTEN, MYC, and ERG immunohistochemical analysis in prostate cancer until July 2017.
Results: We identified 361 articles, 44 of which were summarized in this review. Diagnostically, no single immunohistochemical marker was able to define a tumor as benign or malignant. Prognostically, Ki-67, p53, and MYC were related to the tumor grade given by Gleason score and to the tumor stage (higher levels related to higher tumor grade). Furthermore, Ki-67 was also related to higher PSA levels, shorter disease-free intervals and shorter tumor-specific survival; the latter was also related to p53. The loss of PTEN protein expression showed a higher association with biochemical recurrence and with a worse prognosis, beyond that predicted by the Gleason score and tumor stage. ERG staining also showed a strong association with biochemical recurrence.
Conclusion: There are several studies relating immunohistochemical markers with clinical-laboratorial outcomes in prostate cancer, the most frequent being Ki-67, p53, ERG, PTEN, and MYC. However, none of these markers have been validated by literary consensus to be routinely applied in medical practice.
Introduction
Prostate cancer (PCa), excluding non-melanoma skin tumors, is the most prevalent cancer among men (1–3), with adenocarcinoma being the most frequent histological subtype. Despite the controversy (4), prostate-specific antigen (PSA) serum level (1, 3) screening routinely accompanies digital rectal examination. Diagnostic confirmation is accomplished by prostate biopsy guided by transrectal ultrasonography with or without magnetic resonance imaging (MRI) (5).
The heterogeneity of PCa histology was initially described by Donald Gleason in the 1960s and has improved over the years (6). Incorporating modifications to the Gleason grading system, the methodology used today is according to the International Society of Urological Pathology (ISUP) (7).
As a heterogeneous tumor which in turn allows a variety of therapeutic options, depending on its risk stratification, it is extremely important to identify the factors that determine PCa prognosis, thus defining the best course of clinical management. Significant prospective series show that radical treatment does not benefit low-risk patients according to the D'Amico's classification (8–10). Although the number of patients diagnosed with low-risk tumors and subjected to unnecessary surgery is substantial (11, 12).
Clinicopathological nomograms are commonly used to stratify risk, although with technological development and an increased understanding of tumor biology, immunohistochemical (IHC) and molecular biomarkers are emerging as powerful tools to distinguish tumors with distinct behaviors.
Immunohistochemical analysis consists of using monoclonal or polyclonal antibodies to detect specific antigens in tissue samples, and it is a widely used technique that can be applied in diverse situations, such as cellular differentiation, characterization of a tumor's primary site, detection of metastases, prognostic factors, as a predictor of targeted therapy response and even in the identification of structures, organisms and materials secreted by cells of interest. In prostate cancer, immunohistochemistry has an important role in the diagnostic confirmation of borderline cases due to the presence (or absence) of basal cells, detected by specific antibodies against it combined with racemase expression in luminal epithelial cells. Currently, the identification of biomarkers capable of predicting the course of the disease has been gaining importance (12–14).
Among the most frequent biomarkers studied that are associated with PCa are p53 (tumor protein p53), Ki-67 (marker of proliferation), ERG (ETS-related gene), MYC (proto-oncogene), and PTEN (phosphatase and tensin homolog), which are implicated in the control of cell proliferation and differentiation, angiogenesis, and apoptosis (15–25).
In the main series of active surveillance, approximately 30% of patients are reclassified and subjected to radical therapy. Immunohistochemical markers could be useful for the initial evaluation and for identifying cases with major or minor potential of progression, helping the decision process of whether to start a radical treatment. Another important application would be in patients with a low volume of ISUP 2, for which immunohistochemistry (IHQ) could be useful in selecting candidates for active surveillance.
Based on these findings, we systematically reviewed articles that studied the role of these main IHC prognostic markers in prostate cancer.
Methods
The systematic review was performed in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA) guidelines (26).
Search Strategy
A computerized literature search of PubMed to identify title and abstracts published was performed. The search was performed with and without MESH terms (Ki-67, p53, PTEN, MYC, ERG, immunohistochemistry, and prostate cancer). All references in the selected articles were checked, including hand-typed searches.
Study Eligibility
The final articles were selected based on the following set of inclusion criteria: (i) examined the association of immunohistochemical expression of Ki-67, p53, PTEN, MYC, and/or ERG with clinical outcome of prostate cancer; (ii) in humans; (iii) non-metastatic prostate cancer; (iv) articles published from 1966 until July 2017. No restriction was made regarding the study type or language. Articles were excluded for any of the following reasons: (i) could not be accessed in its entirety; (ii) were duplicated; (iii) were a review article.
Initially, titles were reviewed to assess whether they met the inclusion criteria. If, after assessing the abstract, there was any doubt regarding whether it met the relevant criteria, it was kept for more thorough, subsequent assessment. The list of potential articles was further shortened by performing detailed evaluations of the methods and results of each remaining paper.
We included patients with localized or locally advanced prostate cancer submitted for or in the process of definitive treatment. None of these patients were submitted to radiotherapy or hormonal therapy before biopsy or prostatectomy.
Data Collection
The following details were recorded for each study: author, year of publication, country where study was performed, study design, number of patients, population/setting, type of material used, main objective of the study (diagnostic and prognostic evaluation) and outcome reported (Gleason Score, PSA level, tumor stage, lymph node stage, tumor diameter, and Gleason upgrading).
Results
The literature search identified a total of 361 studies. Using the above inclusion and exclusion criteria a total of 42 studies were included in the systematic review: 9 concerning Ki-67 and p53; 3 concerning MYC; 15 concerning PTEN, and 17 concerning ERG. (2 studies concerned more than one marker). A schematic of the search is depicted in Figure 1.
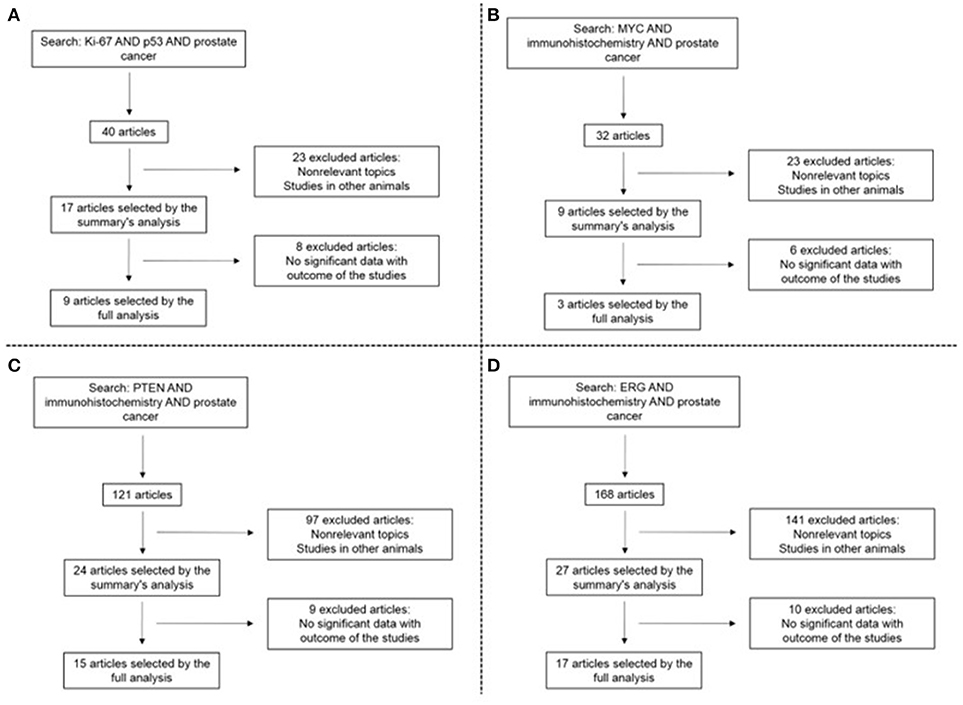
Figure 1. Search results concerning Ki-67 and p53 (A), MYC (B), PTEN (C), and ERG (D).
The attachment archive depicts the characteristics of the studies included in systematic review based on the association of the immunohistochemical expression of Ki-67, p53, PTEN, MYC, and/or ERG with the clinical outcomes of prostate cancer (Supplementary Table 1).
Table 1 lists the main outcomes and studies, according to the studies that analyzed biopsy specimens and prostatectomy specimens.
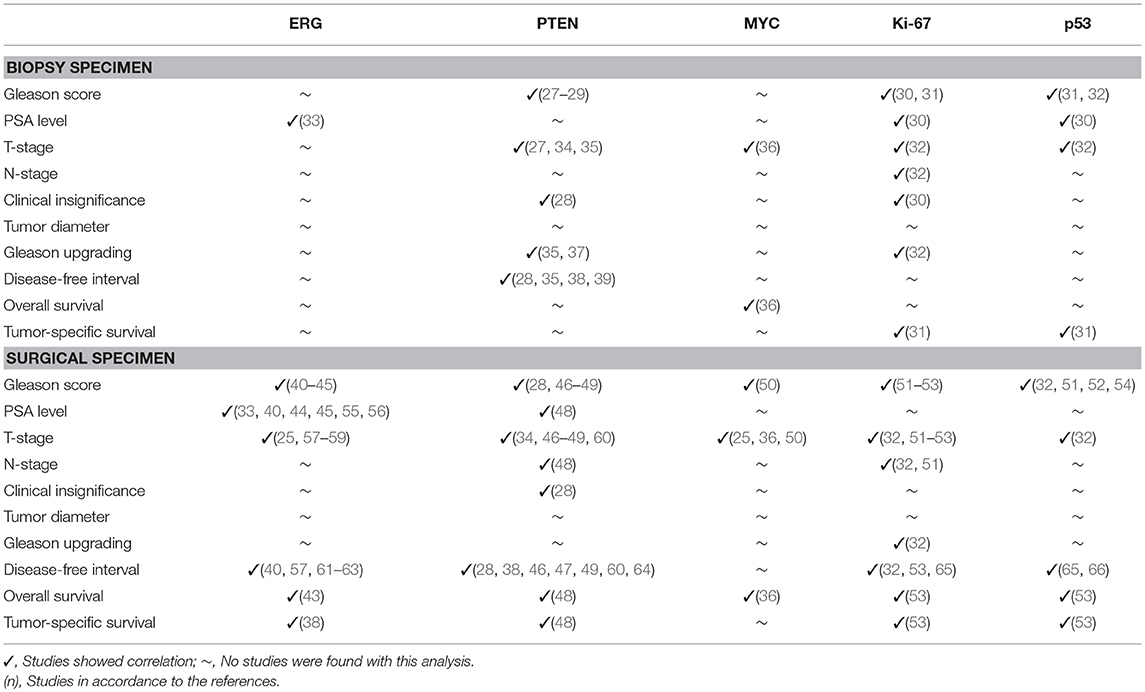
Table 1. Immunohistochemical marker role in predicting outcomes in biopsy and surgical specimen analysis.
Diagnosis
The vast majority of prostate cancer diagnoses are based on morphological assessment. IHC is complimentary in case of doubt, but its interpretation should always be evaluated in conjunction with histomorphology. None of the IHQ markers used with a diagnostic purpose (p63, high molecular weight keratins, racemase and ERG) are specific and/or sensitive enough to classify a case as benign or malignant.
Prognosis
Ki-67
Ki-67 is a protein expressed in the nucleus of proliferating cells during mitosis interphase. It is expressed during late G1, S, G2, and M phases, but not during G0 phase (15). The Ki-67 protein is a cellular proliferation marker (16, 17) and it is widely used given its high reproducibility (15).
Of the selected articles, the analyzed materials in studies were from: prostatectomy specimens (5 studies) (32, 51–53, 65), biopsy specimens (3 studies) (30–32), and transurethral resections (TUR) (2 studies) (52, 53).
Chevrier et al. (51) quantitatively and positively correlated Ki-67 expression based on the H-score and tumor grade given by the Gleason score: H-score 2, 21, and 52 for Gleason score (3 + 3 = 6, 3 + 4 = 7, and 4 + 4 = 8), respectively (p = 0.0002). Other studies also showed significant statistical correlation between Ki-67 and the Gleason score (30, 31, 52, 53), of which 2 were biopsy specimens (30, 31) and the others were prostatectomy and/or TUR specimens (52, 53).
Ki-67 protein overexpression was also shown to be related to T stage and lymph node invasion (32, 51). Its higher expression was more related to stage T3 than to T2 (p = 0.0001), and found more in N1 (p = 0.0389) the latter also shown in Zellweger et al. (32). Zellweger et al. (32) showed that Ki-67 >10% (high) was associated with adverse pT stage (p = 0.036), specifically to seminal vesicle invasion (pT3b) with OR = 12 (2.5–57.0, 95% CI), p = 0.002.
Elevated Ki-67 showed an association with PSA serum levels for PSA ≤ 2.5 ng/ml compared with PSA between 10 and 20 ng/ml (p < 0.05) (30). In turn, low levels of Ki-67 were related to clinically insignificant tumors [determined by the Epstein criteria (67) and by PRIAS (68)], at p = 0.05 and 0.005, respectively (30).
In a study comparing biopsy and prostatectomy specimens, an elevated Ki-67 (>10%) in the biopsy was related to a higher Gleason score in the prostatectomy specimen (p = 0.001) (32). In the same study, an association between Ki-67 and the disease/biochemical recurrence-free interval was found, as also shown by Inoue et al. (65).
In general, an association between elevated Ki-67 and a higher percentage of tumor cell involvement on biopsy (p = 0.037), as well as shorter tumor-specific survival (p = 0.0007), can be found in the literature (31).
p53
Tumor protein 53 (p53) regulates the control of cell cycle progression and cell proliferation, as well as the intrinsic mitochondrial apoptosis pathway (16, 18). p53 acts as a transcription factor, controlling genes to prevent cell proliferation after DNA damage (19). When mutations in the TP53 gene occur, cells that contain damaged DNA are not repaired nor are cells destroyed, resulting in the inability to stop the cell cycle or to initiate apoptosis, thus allowing the emergence of malignant cells (20). Mutations in TP53 occur in more than 50% of malignancies, including high grade prostate cancers (21).
Of the selected articles, the analyzed materials in the studies were: specimens from prostatectomies (7 studies) (32, 51–54, 65, 66), biopsies (3 studies) (30–31), and TUR (2 studies) (52, 53).
Regarding p53 as an immunohistochemical marker, the relationship between its expression and tumor grade (Gleason score) was reported in various studies (32, 51, 52, 54). Chevrier et al. (51) showed this relationship in a quantitative manner using the H-score system, comparing histologic groups as follows: Gleason 3 + 3 had an H-score of 3, Gleason 3 + 4 had an H-score of 65 and Gleason 5 + 4 H-score = 195 (p = 0.0430) (51).
Zellweger et al. (32) demonstrated the relationship between p53 positivity (>20% of highly reactive nuclei) and seminal vesicle invasion (p = 0.001) (32). Nagao et al. showed a relationship between p53 and the PSA level (comparing PSA ≤ 2.5 ng/ml and PSA between 10 and 20 ng/ml) (p < 0.05) (30).
An association between p53 and biochemical recurrence free survival was shown in two studies, Inoue et al. (65) and Osman et al. (66) (p = 0.0097 and p < 0.01, respectively) (65, 66). In survival studies, p53 overexpression predicted shorter tumor-specific survival (p < 0.05) (53) and overall survival (p = 0.024) (31).
ERG
ERG (ETS-related gene) expresses an essential protein for the maintenance of vascular integrity. It is associated with cellular structure maintenance, and its loss leads to higher endothelial permeability. It is also associated with haematopoiesis, maintenance of platelets in peripheral blood and pre-cartilage formation (in mesoderm cells). Typically, it is not present in normal prostatic tissue. The protein is overexpressed in prostate cancer when the androgen-induced TMPRSS2 (transmembrane serine protease 2) gene fuses to the ERG gene (22).
Of the selected articles, the analyzed materials in the studies were specimens from prostatectomies (17 studies) (25, 33, 38, 40–45, 55–59, 61–63), TUR (3 studies) (33, 38, 59), biopsies (2 studies) (38, 33).
In the analysis of reviewed articles, there was a consistency between the relationship of ERG protein expression and the biochemical recurrence of PCa (38, 40, 57, 61–63). Hagen et al. showed that 13 of 28 patients (46.4%) who had surgical specimens with high ERG levels developed recurrence compared to only 3 (12%) of 25 patients who had tumors with low ERG levels (p = 0.006) (57). Font-Tello et al. also showed this association, with PSA progression observed in 3 of 25 (12%) ERG-negative patients compared to 13 of 38 (34.2%) ERG-positive patients (p = 0.04) (61). Kim et al. presented a relative risk for biochemical recurrence in ERG-positive patients of 8.964 (p = 0.002) (40).
An association between ERG-positive immunohistochemistry and Gleason score was frequently reported (41–45). Suh et al. (41) showed that ERG protein expression was more frequently detected in the subgroup with a lower primary Gleason grade (less than or equal to 7) than in the subgroup with a higher Gleason grade (p = 0.011) (41). Kron et al. (42) obtained similar results, with ERG positivity found more frequently in Gleason score 6 and 7 tumors, whereas a Gleason score of 8 to 10 displayed a lower positive frequency (p < 0.01) (42).
For PSA levels, ERG-positive cases were associated with lower preoperative PSA compared to ERG-negative cases (33, 40, 44, 45, 55, 56). Brooks et al. (45) showed a mean PSA of 7.9 ng/ml in patients with positive ERG expression and a mean PSA of 9.3 ng/ml in ERG-negative patients (p = 0.0003) (45). Kim et al. compared a group of patients with PSA serum levels lower than 10 ng/ml to a group of patients with PSA higher or equal to 10 ng/ml and showed that the relative risk for positive ERG protein expression was 4.3 favorable for the group with lower PSA levels (p = 0.039) (40).
For the presence of adverse pathologic features, Udager et al. (25) showed that ERG-positive tumors were associated with extraprostatic extension (p = 0.02). They also showed that these tumors were associated with elevated pathological stage greater than or equal to pT3 (p = 0.035) (25). This correlation was also reported by other groups (58, 59, 61).
Finally, several reports indicated that ERG-positive patients were enriched for PCa diagnosis at a younger age (44, 45, 55, 59). Schaefer et al. showed a mean age of 60 years for ERG-positive tumors in contrast to 63 years for ERG-negative tumors (p < 0.0001)(44). Similarly, Brooks et al. showed a mean age of 60.5 vs. 62.5; p < 0.0001, with the ERG-positive expression group having a younger age (45).
PTEN
PTEN (phosphatase and tensin homolog) is a tumor suppressor gene. It is a lipid phosphatase and a negative regulator of the PI3K/AKT/mTOR pathway, which controls cellular processes such as survival, proliferation, metabolim, migration and cellular architecture. The PTEN protein is frequently absent in some cases of prostate cancer, indicating a loss of function (23).
Of the selected articles, the analyzed materials in the studies were: specimens from prostatectomies (10 studies) (27, 28, 34, 38, 46–49, 60, 64), biopsies (6 studies) (28, 29, 35, 37–39), and TUR (3 studies) (34, 38, 69).
One of the most consistent correlations found in the literature was between the loss of PTEN and a higher recurrence rate or shorter disease-free interval, with the finding that PTEN is considered a biochemical recurrence predictor (28, 34, 38, 39, 46, 47, 60, 64). Murphy et al. showed that among Gleason score 7 or higher tumors, those with PTEN loss had a recurrence rate of 80% compared to 55% in those with intact PTEN (28).
In addition, a correlation between loss of PTEN staining and a worse disease prognosis was frequently observed. Studies revealed a higher risk of death among patients with prostate cancer and loss of PTEN staining compared to patients with proficient and/or partially reduced PTEN protein staining (48, 49, 69). Lahdensuo et al. presented a hazard ratio for risk of death by prostate cancer of 2.156 (95% CI 1.169–3.976, p = 0.014) in a univariate analysis that compared those with a total loss of PTEN to those with partial or no loss of PTEN (48).
Lotan et al. reported a relationship between the loss of PTEN protein and Gleason upgrading from biopsy to prostatectomy. They found that 18.3% (13/71) of tumors that had Gleason upgrading presented PTEN protein loss compared to 7% (7/103) of those without Gleason upgrading (p = 0.02) (37). Guedes et al. also showed this correlation (35).
PTEN loss was associated with extraprostatic extension in numerous studies (35, 46, 47), notably seminal vesicle invasion (46, 47, 60). It also showed an association with a higher Gleason score (27, 29, 46–49). Genomically, homozygous loss of PTEN was present in only 4% of patients with Gleason score 6 compared to 18% of those with a Gleason score of 8 to 10 (p < 0.0001) (47).
MYC
MYC is a nuclear transcription factor related to regulation of the cell cycle progression, metabolism, ribosome biogenesis, protein synthesis, mitochondrial functions and stem cell self-renewal. Its protein is frequently overexpressed in prostate cancer and can have a role in tumor initiation and/or progression (24, 25).
Of the selected articles, the analyzed materials in the studies were specimens from prostatectomy (3 studies) (25, 36, 50) and biopsies (2 studies) (25, 36).
In our literature review, we found correlations between MYC and the Gleason score. Prowatke et al. (50) showed that a decrease of MYC protein expression was related to an increase in Gleason score. MYC expression was 74, 54, and 28% in tumors with Gleason score 6, 7 and 8–9, respectively (p = 0.001) (50).
A correlation between a reduction of MYC protein expression and an increase of T-stage was also demonstrated, with 73% in pT2 and 36% in pT3–4, (p = 0.001) (50). These findings were also reported by Zeng et al. (36) (p < 0.001). Udager et al. demonstrated that MYC overexpression was related to the presence of extraprostatic extension (p = 0.004) in a multivariate analysis with HR = 5.780 (95% CI 2.125 to 15.722) (p < 0.001) (25).
Discussion
Prostate cancer screening is constantly questioned because large studies failed to demonstrate any survival benefit (70–72) and because the overdiagnosis caused by the detection of indolent tumors leads to overtreatment and a worsened quality of life because of the treatment (73).
Although active surveillance should remain the preferred option in managing very low-risk and the majority of low-risk prostate cancers (74), it is constantly under-used in clinical practice worldwide. According to the US National Cancer Data Base, in 2013, less than 20% of men with low-risk prostate cancer were managed conservatively (75).
Active surveillance presents a cancer-specific survival similar to active treatment in very low and low-risk PCa patients. However, the disease progression-free survival rate is significantly higher in active surveillance patients, compared to men treated with radical prostatectomy or radiation therapy (9). Therefore, it is of foremost importance to determine whether there are any other factors that could improve the selection of patients that can be safely managed without definitive treatment.
For this, several IHC markers, are readouts for tumor behavior and were used to better define the prognosis and course of management for men with prostate cancer. However, there remains no literary consensus about which markers are more reliable for those purposes. In this manuscript, we emphasized what we believe to be the most promising markers, p53, Ki-67, MYC, ERG and PTEN, analyzed in both the biopsy and post-prostatectomy setting.
In the diagnostic scenario, in this systematic review, no immunohistochemical marker was found to be significant for diagnosing or defining a tumor as benign or malignant.
By contrast, for determining prognosis, immunohistochemical markers stand out in several studies, some presenting with consistent results. Ki-67, p53, and MYC were consistently related to the tumor grade given by Gleason score and to the tumor stage (higher levels related to higher tumor grade). Ki-67 was also related to higher PSA levels, shorter disease-free interval and shorter tumor-specific survival. Additionally, data showed a relationship between p53 and shorter tumor-specific survival. The loss of PTEN protein expression was related to biochemical recurrence and a worse prognosis, beyond Gleason score and tumor stage. One of the most consistent findings was the association between ERG staining and biochemical recurrence.
Considering all these findings in this systematic review, we propose that immunohistochemical markers are in the process of becoming consistent prognostics tools in clinical practice. As a scientific approach, the relationship between these markers and certain outcomes in prostate cancer is increasingly shown. However, gaining statistical significance and strength in clinical practice remains necessary.
Although cost-effective analyses are missing, a wider utilization of IHC markers in daily routine practice could facilitate decision-making by the clinician and even encourage the patient to follow the most appropriate path for disease management.
Conclusion
In summary, there are several studies relating immunohistochemical markers with clinical-laboratory outcomes in prostate cancer, the most frequent being Ki-67, p53, ERG, PTEN, and MYC. However, none of these markers have been validated and, consequently, they cannot be applied in medical practice.
Positive staining for Ki-67, p53 and MYC were related to higher tumor grade and stage. Ki-67 was also related to PSA levels, disease-free interval and tumor-specific survival (the latter also being related to p53). For PTEN, its loss showed a higher association with biochemical recurrence and a worse prognosis, as well as Gleason score and tumor stage. Finally, ERG showed a strong association with biochemical recurrence.
If applied in specific situations, the use of these markers could guide the process of therapeutic decision making.
Author Contributions
AC, ÁB MW and BB drafted the manuscript and worked on the conception, design and interpretation of data. ÁB and LT selected articles, screened titles and abstracts, assessed study quality and extracted data. AC, ÁB, LT, PK, NM, CC, MW, IC, BB, GL, AS, MO and MT-M were involved in the interpretation and discussion of the results and critically revised the systematic review for important intellectual content. All authors approved the final version of the systematic review.
Conflict of Interest Statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Supplementary Material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fonc.2018.00377/full#supplementary-material
Abbreviations
PCa, Prostate cancer; PSA, Prostate-specific antigen; ISUP, International Society of Urological Pathology; IHC, Immunohistochemical; ERG, ETS-related gene; PTEN, Phosphatase and tensin homolog; TUR, Transurethral resection; MRI, Magnetic resonance imaging; EAU, European Association of Urology; AUA, American Urological Association.
References
1. Smith T, Coburn M. Sabiston Textbook of Surgery: The Biological Basis of Modern Surgical Practice. 20 th Edn. Elsevier (2017).
2. Narayan VM, Konety BR, Warlick C. Novel biomarkers for prostate cancer: an evidence-based review for use in clinical practice. Int J Urol. (2017) 24:352–60. doi: 10.1111/iju.13326
3. Sharma S, Zapatero-Rodriguez J, O'Kennedy R. Prostate cancer diagnostics: clinical challenges and the ongoing need for disruptive and effective diagnostic tools. Biotechnol Adv. (2017) 35:135–49. doi: 10.1016/j.biotechadv.2016.11.009
4. Moyer VA, Force USPST. Screening for prostate cancer: U.S. preventive services task force recommendation statement. Ann Intern Med. (2012) 157:120–34. doi: 10.7326/0003-4819-157-2-201207170-00459
5. Garisto JD, Klotz L. Active surveillance for prostate cancer: how to do it right. Oncology (2017) 31:333–40, 45.
6. Gleason DF, Mellinger GT. Prediction of prognosis for prostatic adenocarcinoma by combined histological grading and clinical staging. J Urol. (1974) 111:58–64. doi: 10.1016/S0022-5347(17)59889-4
7. Gordetsky J, Epstein J. Grading of prostatic adenocarcinoma: current state and prognostic implications. Diagn Pathol. (2016) 11:25. doi: 10.1186/s13000-016-0478-2
8. Wilt TJ, Brawer MK, Jones KM, Barry MJ, Aronson WJ, Fox S, et al. Radical prostatectomy versus observation for localized prostate cancer. N Engl J Med. (2012) 367:203–13. doi: 10.1056/NEJMoa1113162
9. Hamdy FC, Donovan JL, Lane JA, Mason M, Metcalfe C, Holding P, et al. 10-Year outcomes after monitoring, surgery, or radiotherapy for localized prostate cancer. N Engl J Med. (2016) 375:1415–24. doi: 10.1056/NEJMoa1606220
10. Holmberg L, Bill-Axelson A, Steineck G, Garmo H, Palmgren J, Johansson E, et al. Results from the scandinavian prostate cancer group trial number 4: a randomized controlled trial of radical prostatectomy versus watchful waiting. J Natl Cancer Inst Monogr. (2012) 2012:230–3. doi: 10.1093/jncimonographs/lgs025
11. Van der Kwast TH. Prognostic prostate tissue biomarkers of potential clinical use. Virchows Archiv (2014) 464:293–300. doi: 10.1007/s00428-014-1540-7
12. Jakobsen NA, Hamdy FC, Bryant RJ. Novel biomarkers for the detection of prostate cancer. J Clin. Urol. (2016) 9(Suppl. 2):3–10. doi: 10.1177/2051415816656121
13. McGrath S, Christidis D, Perera M, Hong SK, Manning T, Vela I, et al. Prostate cancer biomarkers: are we hitting the mark? Prostate Int. (2016) 4:130–5. doi: 10.1016/j.prnil.2016.07.002
14. Sharma P, Zargar-Shoshtari K, Pow-Sang JM. Biomarkers for prostate cancer: present challenges and future opportunities. Future Sci OA (2016) 2:FSO72. doi: 10.4155/fso.15.72
15. Sulik M. Expression of Ki-67 as a proliferation marker in prostate cancer. Polish Ann Med. (2011) 18:8. doi: 10.1016/S1230-8013(11)70019-4
16. Missaoui N, Abdelkarim SB, Mokni M, Hmissa S. Prognostic factors of prostate cancer in Tunisian men: immunohistochemical study. Asian Pac J Cancer Prev. (2016) 17:2655.
17. Kim SH, Park WS, Park BR, Joo J, Joung JY, Seo HK, et al. PSCA, Cox-2, and Ki-67 are independent, predictive markers of biochemical recurrence in clinically localized prostate cancer: a retrospective study. Asian J Androl. (2017) 19:458–62. doi: 10.4103/1008-682X.180798
18. Kudahetti S, Fisher G, Ambroisine L, Foster C, Reuter V, Eastham J, et al. p53 immunochemistry is an independent prognostic marker for outcome in conservatively treated prostate cancer. BJU Int. (2009) 104:20–4. doi: 10.1111/j.1464-410X.2009.08407.x
20. Klumb CE, Júnior GBC. Avaliação dos métodos de detecção das alterações do gene e proteína p53 nas neoplasia linfóides. Rev Bras Hematol Hemoter. (2002) 24:111–25. doi: 10.1590/S1516-84842002000200008
21. Kumari R, Sen N, Das S. Tumour suppressor p53: understanding the molecular mechanisms inherent to cancer. Curr. Sci. (2014) 107:786–94.
22. Adamo P, Ladomery M. The oncogen ERG: a key factor in prostate cancer. Oncogene (2015) 35:403–14. doi: 10.1038/onc.2015.109
23. Ferraldeschi R, Nava Rodrigues D, Riisnaes R, Miranda S, Figueiredo I, Rescigno P, Ravi P, et al. PTEN protein loss and clinical outcome from castration-resistant prostate cancer treated with abiraterone acetate. Eur Urol. (2015) 67:795–802. doi: 10.1016/j.eururo.2014.10.027
24. Gurel B, Iwata T, Koh CM, Jenkins RB, Lan F, Van Dang C, et al. Nuclear MYC protein overexpression is an early alteration in human prostate carcinogenesis. Mod Pathol. (2008) 21:1156–67. doi: 10.1038/modpathol.2008.111
25. Udager AM, DeMarzo AM, Shi Y, Hicks JL, Cao X, Siddiqui J, et al. Concurrent nuclear ERG and MYC protein overexpression defines a subset of locally advanced prostate cancer: potential opportunities for synergistic targeted therapeutics. Prostate (2016) 76:845–53. doi: 10.1002/pros.23175
26. Moher D, Liberati A, Tetzlaff J, Altman D, Group TP. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. PLoS Med. (2009) 6:e1000097. doi: 10.1371/journal.pmed.1000097
27. Lotan TL, Gurel B, Sutcliffe S, Esopi D, Liu W, Xu J, et al. PTEN protein loss by immunostaining: analytic validation and prognostic indicator for a high risk surgical cohort of prostate cancer patients. Clin Cancer Res. (2011) 17:6563–73. doi: 10.1158/1078-0432.CCR-11-1244
28. Murphy SJ, Karnes RJ, Kosari F, Castellar BE, Kipp BR, Johnson SH, et al. Integrated analysis of the genomic instability of PTEN in clinically insignificant and significant prostate cancer. Modern Pathol. (2016) 29:143–56. doi: 10.1038/modpathol.2015.136
29. Shah RB, Bentley J, Jeffery Z, DeMarzo AM. Heterogeneity of PTEN and ERG expression in prostate cancer on core needle biopsies: implications for cancer risk stratification and biomarker sampling. Hum Pathol. (2015) 46:698–706. doi: 10.1016/j.humpath.2015.01.008
30. Nagao K, Yamamoto Y, Hara T, Komatsu H, Inoue R, Matsuda K, et al. Ki67 and BUBR1 may discriminate clinically insignificant prostate cancer in the PSA range <4 ng/ml. Jpn J Clin Oncol. (2011) 41:555–64. doi: 10.1093/jjco/hyq233
31. Bubendorf L, Tapia C, Gasser TC, Casella R, Grunder B, Moch H, et al. Ki67 labeling index in core needle biopsies independently predicts tumor-specific survival in prostate cancer. Hum Pathol. (1998) 29:949–54. doi: 10.1016/S0046-8177(98)90199-X
32. Zellweger T, Gunther S, Zlobec I, Savic S, Sauter G, Moch H, et al. Tumour growth fraction measured by immunohistochemical staining of Ki67 is an independent prognostic factor in preoperative prostate biopsies with small-volume or low-grade prostate cancer. Int J Cancer (2009) 124:2116–23. doi: 10.1002/ijc.24174
33. Aldaoud N, Abdo N, Al Bashir S, Alqudah M, Marji N, Alzou'bi H, et al. Prostate cancer in Jordanian-Arab population: ERG status and relationship with clinicopathologic characteristics. Virchows Arch. (2017). 471:753–9. doi: 10.1007/s00428-017-2160-9
34. Jiang FN, He HC, Zhang YQ, Yang DL, Huang JH, Zhu YX, et al. An integrative proteomics and interaction network-based classifier for prostate cancer diagnosis. PLoS ONE (2013) 8:e63941. doi: 10.1371/journal.pone.0063941
35. Guedes LB, Tosoian JJ, Hicks J, Ross AE, Lotan TL. PTEN loss in gleason score 3 + 4 = 7 prostate biopsies is associated with nonorgan confined disease at radical prostatectomy. J Urol. (2017) 197:1054–9. doi: 10.1016/j.juro.2016.09.084
36. Zeng W, Sun H, Meng F, Liu Z, Xiong J, Zhou S, et al. Nuclear C-MYC expression level is associated with disease progression and potentially predictive of two year overall survival in prostate cancer. Int J Clin Exp Pathol. (2015) 8:1878–88.
37. Lotan TL, Carvalho FL, Peskoe SB, Hicks JL, Good J, Fedor H, et al. PTEN loss is associated with upgrading of prostate cancer from biopsy to radical prostatectomy. Mod Pathol. (2015) 28:128–37. doi: 10.1038/modpathol.2014.85
38. Leinonen KA, Saramaki OR, Furusato B, Kimura T, Takahashi H, Egawa S, et al. Loss of PTEN is associated with aggressive behavior in ERG-positive prostate cancer. Cancer Epidemiol Biomarkers Prev. (2013) 22:2333–44. doi: 10.1158/1055-9965.EPI-13-0333-T
39. Fontugne J, Lee D, Cantaloni C, Barbieri CE, Caffo O, Hanspeter E, et al. Recurrent prostate cancer genomic alterations predict response to brachytherapy treatment. Cancer Epidemiol Biomarkers Prevent. (2014) 23:594–600. doi: 10.1158/1055-9965.EPI-13-1180
40. Kim SH, Joung JY, Lee GK, Hong EK, Kang KM, Yu A, et al. Overexpression of ERG and wild-type PTEN are associated with favorable clinical prognosis and low biochemical recurrence in prostate cancer. PLoS ONE (2015) 10:e0122498. doi: 10.1371/journal.pone.0122498
41. Suh JH, Park JW, Lee C, Moon KC. ERG immunohistochemistry and clinicopathologic characteristics in Korean prostate adenocarcinoma patients. Korean J Pathol. (2012) 46:423–8. doi: 10.4132/KoreanJPathol.2012.46.5.423
42. Kron K, Liu L, Trudel D, Pethe V, Trachtenberg J, Fleshner N, et al. Correlation of ERG expression and DNA methylation biomarkers with adverse clinicopathologic features of prostate cancer. Clin Cancer Res. (2012) 18:2896–904. doi: 10.1158/1078-0432.CCR-11-2901
43. Szász AM, Majoros A, Rosen P, Srivastava S, Dobi A, Szendroi A, et al. Prognostic potential of ERG (ETS-related gene) expression in prostatic adenocarcinoma. Int Urol Nephrol. (2013) 45:727–33. doi: 10.1007/s11255-013-0406-2
44. Schaefer G, Mosquera JM, Ramoner R, Park K, Romanel A, Steiner E, et al. Distinct ERG rearrangement prevalence in prostate cancer: higher frequency in young age and in low PSA prostate cancer. Prostate Cancer Prostatic Dis. (2013) 16:132–8. doi: 10.1038/pcan.2013.4
45. Brooks JD, Wei W, Hawley S, Auman H, Newcomb L, Boyer H, et al. Evaluation of ERG and SPINK1 by immunohistochemical staining and clinicopathological outcomes in a multi-institutional radical prostatectomy cohort of 1067 patients. PLoS ONE (2015) 10:e0132343. doi: 10.1371/journal.pone.0132343
46. Silva MP, Barros-Silva JD, Ersvær E, Kildal W, Hveem TS, Pradhan M, et al. Cancer prognosis defined by the combined analysis of 8q, PTEN and ERG. Transl Oncol. (2016) 9:575–82. doi: 10.1016/j.tranon.2016.08.005
47. Lotan TL, Wei W, Morais CL, Hawley ST, Fazli L, Hurtado-Coll A, et al. PTEN loss as determined by clinical-grade immunohistochemistry assay is associated with worse recurrence-free survival in prostate cancer. Eur Urol Focus (2016) 2:180–8. doi: 10.1016/j.euf.2015.07.005
48. Lahdensuo K, Erickson A, Saarinen I, Seikkula H, Lundin J, Lundin M, et al. Loss of PTEN expression in ERG-negative prostate cancer predicts secondary therapies and leads to shorter disease-specific survival time after radical prostatectomy. Modern Pathol. (2016) 29:1565–74. doi: 10.1038/modpathol.2016.154
49. Ahearn TU, Pettersson A, Ebot EM, Gerke T, Graff RE, Morais CL, et al. A prospective investigation of PTEN loss and ERG expression in lethal prostatecancer. J Natl Cancer Inst. (2016) 108:1–9. doi: 10.1093/jnci/djv346
50. Prowatke I, Devens F, Benner A, Gröne EF, Mertens D, Gröne HJ, et al. Expression analysis of imbalanced genes in prostate carcinoma using tissue microarrays. Br J Cancer (2007) 96:82–8. doi: 10.1038/sj.bjc.6603490
51. Chevrier M, Bobbala D, Villalobos-Hernandez A, Khan MG, Ramanathan S, Saucier C, et al. Expression of SOCS1 and the downstream targets of its putative tumor suppressor functions in prostate cancer. BMC Cancer (2017) 17:157. doi: 10.1186/s12885-017-3141-8
52. Zellweger T, Ninck C, Bloch M, Mirlacher M, Koivisto PA, Helin HJ, et al. Expression patterns of potential therapeutic targets in prostate cancer. Int J Cancer (2005) 113:619–28. doi: 10.1002/ijc.20615
53. Zellweger T, Ninck C, Mirlacher M, Annefeld M, Glass AG, Gasser TC, et al. Tissue microarray analysis reveals prognostic significance of syndecan-1 expression in prostate cancer. Prostate (2003) 55:20–9. doi: 10.1002/pros.10209
54. Bubendorf L, Sauter G, Moch H, Jordan P, Blochlinger A, Gasser TC, et al. Prognostic significance of Bcl-2 in clinically localized prostate cancer. Am J Pathol. (1996) 148:1557–65.
55. Xu B, Chevarie-Davis M, Chevalier S, Scarlata E, Zeizafoun N, Dragomir A, et al. The prognostic role of ERG immunopositivity in prostatic acinar adenocarcinoma: a study including 454 cases and review of the literature. Hum Pathol. (2014) 45:488–97. doi: 10.1016/j.humpath.2013.10.012
56. Hoogland AM, Jenster G, van Weerden WM, Trapman J, van der Kwast T, Roobol MJ, et al. ERG immunohistochemistry is not predictive for PSA recurrence, local recurrence or overall survival after radical prostatectomy for prostate cancer. Mod Pathol. (2012) 25:471–9. doi: 10.1038/modpathol.2011.176
57. Hagen RM, Adamo P, Karamat S, Oxley J, Aning JJ, Gillatt D, et al. Quantitative analysis of ERG expression and its splice isoforms in formalin-fixed, paraffin-embedded prostate cancer samples: association with seminal vesicle invasion and biochemical recurrence. Am J Clin Pathol. (2014) 142:533–40. doi: 10.1309/AJCPH88QHXARISUP
58. Weinmann S, Van Den Eeden SK, Haque R, Chen C, Richert-Boe K, Schwartzman J, et al. Immunohistochemical expression of ERG in the molecular epidemiology of fatal prostate cancer study. Prostate (2013) 73:1371–7. doi: 10.1002/pros.22684
59. Graff RE, Meisner A, Ahearn TU, Fiorentino M, Loda M, Giovannucci EL, et al. Pre-diagnostic circulating sex hormone levels and risk of prostate cancer by ERG tumour protein expression. Br J Cancer (2016) 114:939–44. doi: 10.1038/bjc.2016.61
60. Halvorsen OJ, Haukaas SA, Akslen LA. Combined loss of PTEN and p27 expression is associated with tumor cell proliferation by Ki-67 and increased risk of recurrent disease in localized prostate cancer. Clin Cancer Res. (2003) 9:1474–9.
61. Font-Tello A, Juanpere N, de Muga S, Lorenzo M, Lorente JA, Fumado L, et al. Association of ERG and TMPRSS2-ERG with grade, stage, and prognosis of prostate cancer is dependent on their expression levels. Prostate (2015) 75:1216–26. doi: 10.1002/pros.23004
62. Taris M, Irani J, Blanchet P, Multigner L, Cathelineau X, Fromont G. ERG expression in prostate cancer: the prognostic paradox. Prostate (2014) 74:1481–7. doi: 10.1002/pros.22863
63. Nishijima J, Hara T, Ikemoto K, Oga A, Kobayashi K, Kawai Y, et al. Clinical significance of ERG rearrangement subtype and its association with increased p53 expression in Japanese and German prostate cancer. Neoplasma (2015) 62:278–87. doi: 10.4149/neo_2015_033
64. Tosoian JJ, Almutairi F, Morais CL, Glavaris S, Hicks J, Sundi D, et al. Prevalence and prognostic significance of PTEN Loss in african-american and european-american men undergoing radical prostatectomy. Eur Urol. (2017) 71:697–700. doi: 10.1016/j.eururo.2016.07.026
65. Inoue T, Segawa T, Shiraishi T, Yoshida T, Toda Y, Yamada T, et al. Androgen receptor, Ki67, and p53 expression in radical prostatectomy specimens predict treatment failure in Japanese population. Urology (2005) 66:332–7. doi: 10.1016/j.urology.2005.02.028
66. Osman I, Drobnjak M, Fazzari M, Ferrara J, Scher HI, Cordon-Cardo C. Inactivation of the p53 pathway in prostate cancer: impact on tumor progression. Clin Cancer Res. (1999) 5:2082–8.
67. Epstein JI, Chan DW, Sokoll LJ, Walsh PC, Cox JL, Rittenhouse H, et al. Nonpalpable stage T1c prostate cancer: prediction of insignificant disease using free/total prostate specific antigen levels and needle biopsy findings. J Urol. (1998) 160(6 Pt 2):2407–11. doi: 10.1097/00005392-199812020-00008
68. Bokhorst LP, Valdagni R, Rannikko A, Kakehi Y, Pickles T, Bangma CH, et al. A decade of active surveillance in the PRIAS study: an update and evaluation of the criteria used to recommend a switch to active treatment. Eur Urol. (2016) 70:954–60. doi: 10.1016/j.eururo.2016.06.007
69. Cuzick J, Yang ZH, Fisher G, Tikishvili E, Stone S, Lanchbury JS, et al. Prognostic value of PTEN loss in men with conservatively managed localised prostate cancer. Br J Cancer (2013) 108:2582–9. doi: 10.1038/bjc.2013.248
70. Schröder FH, Hugosson J, Roobol MJ, Tammela TL, Ciatto S, Nelen V, et al. Screening and prostate-cancer mortality in a randomized European study. N Engl J Med. (2009) 360:1320–8. doi: 10.1056/NEJMoa0810084
71. Andriole GL, Crawford ED, Grubb RL, Buys SS, Chia D, Church TR, et al. Mortality results from a randomized prostate-cancer screening trial. N Engl J Med. (2009) 360:1310–9. doi: 10.1056/NEJMoa0810696
72. Martin RM, Donovan JL, Turner EL, Metcalfe C, Young GJ, Walsh EI, et al. Effect of a low-intensity PSA-based screening intervention on prostate cancer mortality: the CAP randomized clinical trial. JAMA (2018) 319:883–95. doi: 10.1001/jama.2018.0154
73. Chen RC, Basak R, Meyer AM, Kuo TM, Carpenter WR, Agans RP, et al. Association between choice of radical prostatectomy, external beam radiotherapy, brachytherapy, or active surveillance and patient-reported quality of life among men with localized prostate cancer. JAMA (2017) 317:1141–50. doi: 10.1001/jama.2017.1652
74. Sanda MG, Cadeddu JA, Kirkby E, Chen RC, Crispino T, Fontanarosa J, et al. Clinically localized prostate cancer: AUA/ASTRO/SUO guideline. Part I: risk stratification, shared decision making, and care options. J Urol. (2018) 199:683–90. doi: 10.1016/j.juro.2017.11.095
Keywords: immunohistochemistry, prostate cancer, biomarkers, ERG, MYC, Ki-67, p53, PTEN
Citation: Carneiro A, Barbosa ÁRG, Takemura LS, Kayano PP, Moran NKS, Chen CK, Wroclawski ML, Lemos GC, Cunha IWd, Obara MT, Tobias-Machado M, Sowalsky AG and Bianco B (2018) The Role of Immunohistochemical Analysis as a Tool for the Diagnosis, Prognostic Evaluation and Treatment of Prostate Cancer: A Systematic Review of the Literature. Front. Oncol. 8:377. doi: 10.3389/fonc.2018.00377
Received: 20 June 2018; Accepted: 23 August 2018;
Published: 18 September 2018.
Edited by:
Giuseppe Di Lorenzo, Azienda Ospedaliera Universitaria Federico II, ItalyReviewed by:
Antonio Rozzi, INI, Istituto Neurotraumatologico Italiano, ItalyEthel Pereira, Massachusetts General Hospital, Harvard Medical School, United States
Chakrabhavi Dhananjaya Mohan, University of Mysore, India
Copyright © 2018 Carneiro, Barbosa, Takemura, Kayano, Moran, Chen, Wroclawski, Lemos, Cunha, Obara, Tobias-Machado, Sowalsky and Bianco. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Bianca Bianco, YmlhbmNhLmJpYW5jb0BmbWFiYy5icg==
† These authors share first authorship