 Vicente Escudero-Vilaplana1*
Vicente Escudero-Vilaplana1* Antonio Calles2Roberto Collado-Borrell1María Belén Marzal-Alfaro1Carlos Polanco3Carmen Garrido3Jorge Suarez3Aurora Ortiz3
Antonio Calles2Roberto Collado-Borrell1María Belén Marzal-Alfaro1Carlos Polanco3Carmen Garrido3Jorge Suarez3Aurora Ortiz3 Marilena Appierto4
Marilena Appierto4 Marta Comellas4Luis Lizán4,5
Marta Comellas4Luis Lizán4,5- 1Hospital Pharmacy, Hospital General Universitario Gregorio Marañón, Instituto de Investigación Sanitaria Gregorio Marañón, Madrid, Spain
- 2Medical Oncology, Hospital General Universitario Gregorio Marañón, Madrid, Spain
- 3Bristol-Myers Squibb, Madrid, Spain
- 4Outcomes'10, Castellón de la plana, Spain
- 5Medicine Department, Universitat Jaume I, Castellón de la plana, Spain
Purpose: Lung cancer (LC) and its treatment impose a significant burden on patients' life. However, patient-centered outcomes are rarely collected during patient follow-up. Filling this gap, the International Consortium for Health Outcomes Measurement (ICHOM) developed a standard set of variables for newly diagnosed LC patients. In order to facilitate the use of this standard set, the project aims to adapt it to the Spanish setting.
Methods: The variables (instrument and periodicity) to be included in Spanish standard set were selected through consensus during 4 nominal groups (13 oncologists, 14 hospital pharmacists, 4 hospital managers and 3 LC patients), under the supervision of a Scientific Committee (1 oncologist, 3 hospital pharmacists, 2 LC patients advocates).
Results: The variables agreed upon included: (1) case-mix: demographic [age, sex, education and social-family support], clinical [weight loss, smoking status, comorbidities (Charlson index), pulmonary function (FEV-1)], tumor [histology, clinical, and pathological stage (TNM), EGFR, ALK, ROS-1, PD-L1] and treatment factors [intent and completion] and (2) outcomes: degree of health [performance status (ECOG) and quality-of-life (EQ-5D, LCSS)], survival [overall survival and cause of death], quality of death [place of death, end-of-life care and palliative care, death aligned with living will], treatment complications, and others [date of diagnosis and treatment initiation, productivity loss (sick leave)].
Conclusion: The adaptation of ICHOM standard set to the Spanish setting pave the way to standardize the collection of variables in LC.
Introduction
In Spain, 28,645 new cases of lung cancer (LC) are diagnosed each year, representing the leading cause of cancer-related mortality (1). LC shows a heterogeneous histology and genetic profile, with non-small-cell LC (NSCLC) being the most frequent (2). The management of the disease is challenging and the choice of the optimal treatment is based on several factors, including the histology, tumor stage at diagnosis and patient's comorbidities and performance status (3, 4).
Despite the significant advances in LC management over the last decade, the disease still impose a significant psychological, emotional, and financial burden on patients (5–7). Disease symptoms such as fatigue, loss of appetite, shortness of breath, cough and pain have been identified as significant predictors of poor health related quality of life (HRQoL) (8, 9). Of note, systematic weekly collection of LC associated symptoms has been related to higher survival (10–13), better HRQoL and a better allocation of health resources (12).
Despite PROs relevance, their systematic collection using standardized and validated instruments is mostly limited to the clinical research setting. Standardization of health outcomes measurements, both clinical and PROs, in routine clinical practice is key to ensure an effective and efficient healthcare provision. In fact, experience gained from other fields shows that the systematic and standardized collection of outcomes is the sine qua non to improve the quality of any process (14).
The International Consortium for Health Outcomes Measurements (ICHOM) (15) is a non-profit organization that has carried out several initiatives to attain this required standardization. All standard sets developed by ICHOM share hallmark features: (a) outcomes variables are defined according to the pathology; (b) they represent the minimum set of relevant outcomes from both healthcare professional and patient perspective; (c) patients are involved in the standard set development; (d) they include PROs; (e) their methods of measurement and measurement frequency are well-defined to ensure benchmarking.
A standard set of patient-centered outcomes for LC (16) was designed by ICHOM for all patients with newly diagnosed LC, including NSCLC and small cell LC (SCLC), independently of the treatment received (surgery, radiotherapy, chemotherapy, targeted therapy and immunotherapy, palliative care). The set consists of two categories of variable: case-mix and outcomes. The former includes baseline sociodemographic, clinical and tumor-related variables. The latter reflects aspects related to the degree of health (including HRQoL), survival, quality of death, treatment complications as well as others like time from diagnosis to treatment.
The long-term goal of ICHOM initiatives is to develop a series of standard sets of variables to promote the consistency in data collection among different institutions within the same country or different countries. However, when implementing such standard sets, different aspects need to be considered: (1) doctors and patients should be familiarized with the variables included in the set; (2) the technology and instruments needed to measure the selected variables should be available; (3) the target population should be defined according to each country's clinical needs. In this light, the main objective of the present study was to adapt the ICHOM standard set of health outcomes for patients with LC in the Spanish setting.
Materials and Methods
A scientific committee, consisting of an oncologist specialized in LC (AC), three hospital pharmacists (VE-V, BM-A, RC-B.) and two patient advocates (BG, BB), led and coordinated the project.
The project comprised four phases: (1) literature review; (2) first scientific committee meeting; (3) four nominal groups; (4) second scientific committee meeting.
Literature Review
An update of the literature search conducted by ICHOM (16) was carried out in Medline/PubMed. The objective of the literature review was to identify health outcomes (clinical and PROs), the instruments to measure them, as well as, the frequency of measurement to be used during LC patients' follow-up. Clinical trials or systematic reviews in English and/or Spanish published between 01/01/2015 and 31/12/2017 were included in the review. Search terms and strategy are shown in Supplementary Table 1.
First Scientific Committee Meeting
A group discussion was held with the members of the scientific committee to define the variables to be presented and evaluated in the nominal groups. According to this purpose, all variables included in the ICHOM standard set (Table 1) as well as those identified through the updated literature review (Table 2) were screened by the scientific committee.
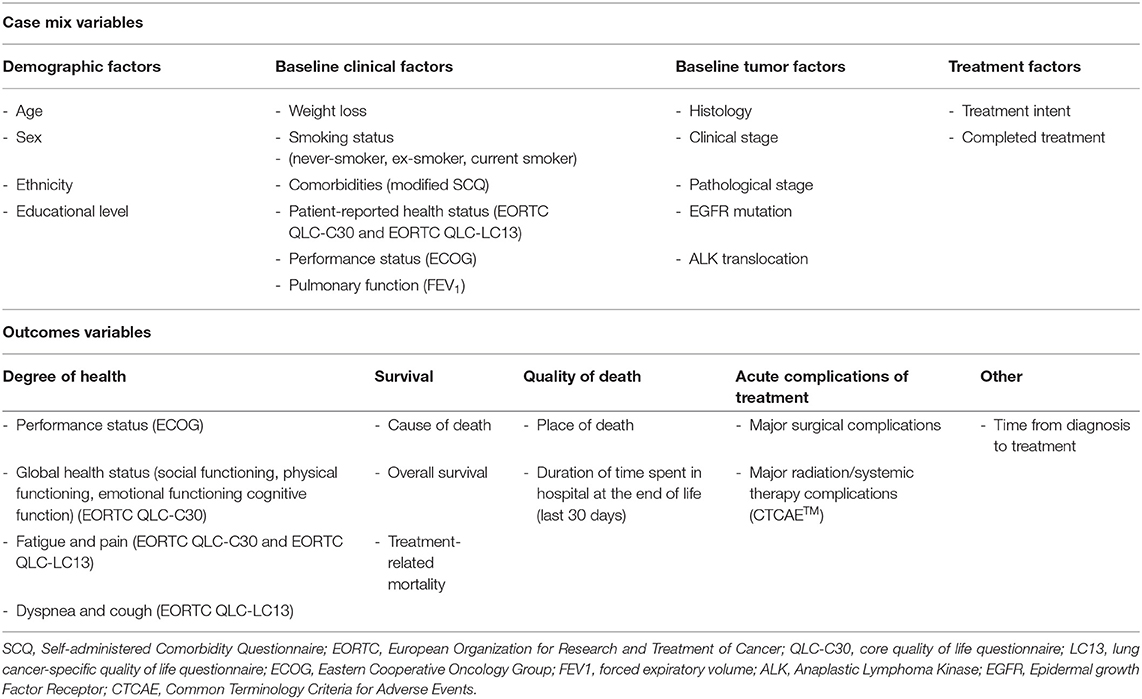
Table 1. ICHOM standard set (16).
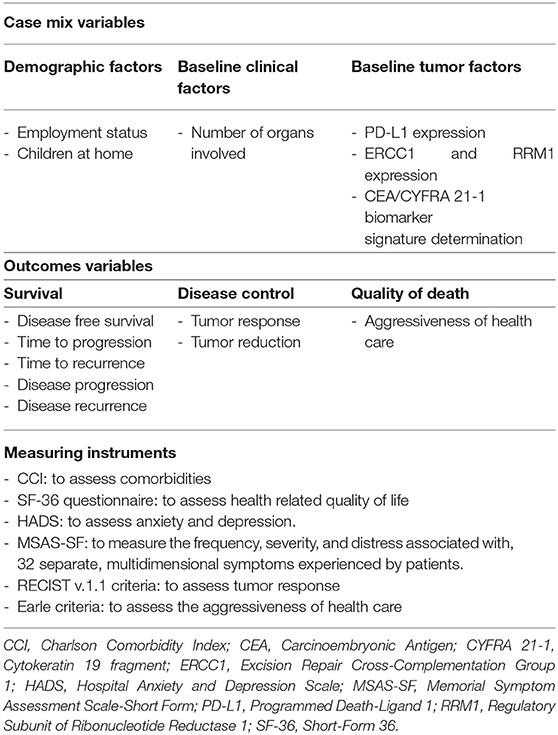
Table 2. Variables and instruments identified in the literature review.
Nominal Group Meetings
The aim of the nominal groups was to reach consensus on the variables to ultimately be included in the standard set of health outcomes for LC in Spain as well as to define the measurement instrument and frequency of measurement to be used.
Nominal group is a qualitative methodology which allows to achieve consensus, while assuring a balanced participation among group members that are given equal opportunity to share their opinion (17). The methodology involves five steps tailored to meet the purpose of the meeting as follows (18): (1) Introduction and explanation: welcoming and explanation of the purpose and procedure of the meeting; (2) Silent generation of ideas: each participant evaluated individually (without consulting or discussing with others) the variables proposed; (3) Sharing ideas: participants shared individually the variables they had selected; (4) Group discussion: participants could seek verbal explanation or further details about any of the variables that other participants had proposed; (5) Voting and ranking: during this phase, participants were asked to prioritize the variables proposed. Variables were included if ≥75% of participants agreed on their inclusion.
In order to be representative at a national level, four nominal groups were conducted, involving experts from different Spanish geographic areas. In each nominal group, participation was limited to a maximum of 12 experts, including oncologists, hospital pharmacists, hospital managers, and patient representatives. Participants of the nominal groups were identified by the scientific committee, in collaboration with patient advocacy groups (Asociación Española de afectados de Cáncer de Pulmón [AEACaP] and Grupo Español de Pacientes con Cáncer [GEPAC]), and the study coordinator. The selection was based on the participant experience in LC management, PRO measurement as well as scientific contributions, availability, and interest in the project.
Second Scientific Committee Meeting
A group discussion was carried out to review the results obtained during the four nominal groups, and to determine the inclusion/exclusion of those variables for which a consensus was not reached during the meetings. Consensus was reached if ≥75% of the members of the scientific committee agreed on the variable inclusion/exclusion. Based on the meeting results, the variables to be included in the standard set of health outcomes for LC were defined.
Results
Literature Review
The database search yielded 260 references, while 8 additional publications were identified by hand-searching. A total of 128 publications were excluded by title and abstract. The full texts of the remaining 140 articles were assessed for eligibility. All of them were included in the qualitative synthesis and reviewed to identify variables, and the respective measuring instruments, that might have not been identified in the review conducted by ICHOM. A flow diagram of the selection process according to the PRISMA Guidelines is depicted in Figure 1.
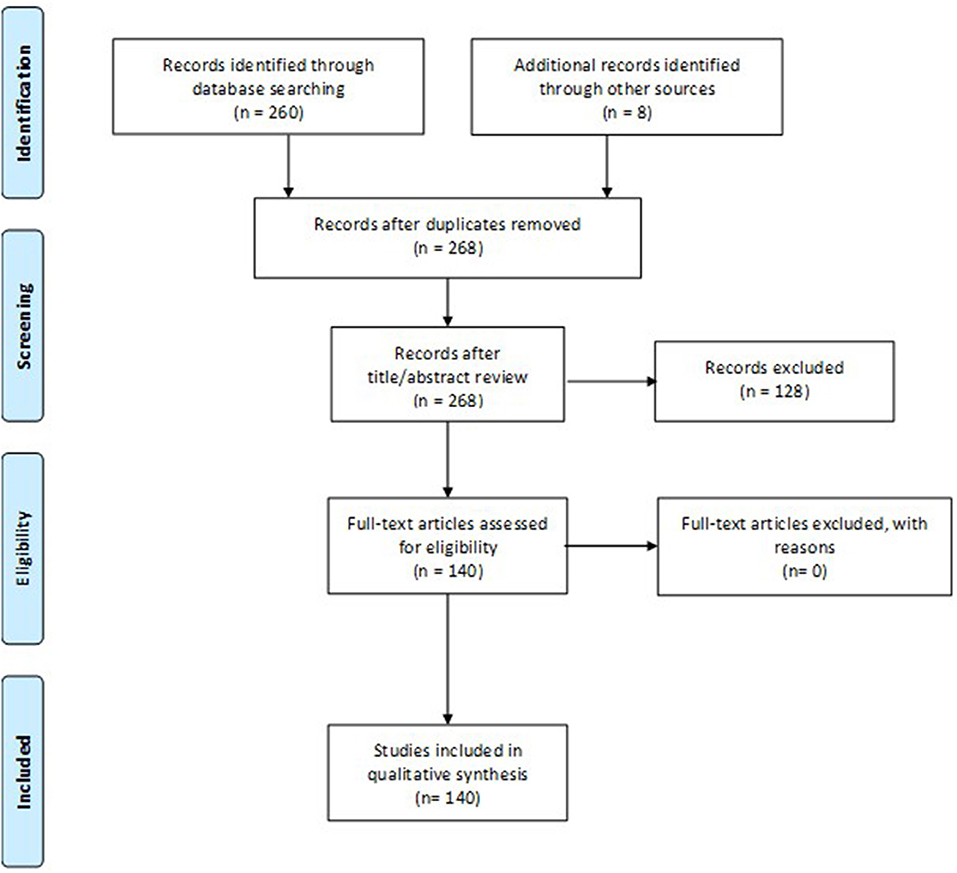
Figure 1. PRISMA Flow diagram.
Following publication screening, a total of 14 variables (6 case-mix and 8 outcomes variables) and 6 measuring instruments, that had not been included in the ICHOM catalog, were identified (Table 2).
First Scientific Committee Meeting
Through the review of the variables included in the ICHOM standard set (Table 1) as well as those identified through the updated literature review (Table 2), a total of 17 case-mix and 25 outcomes variables were selected by the scientific committee to be presented and evaluated during the nominal groups. Selected variables, together with their measuring instruments are presented in Supplementary Tables 2, 3. During the meeting, the scope of the standard set was also defined. In line with the ICHOM standard set for LC, the target population of the standard set defined within the present project framework was set to include all patients with newly diagnosed LC, regardless of the disease stage, type or therapeutic options.
Nominal Group Meetings
Overall, 13 oncologists, 14 hospital pharmacists, 4 hospital managers and 3 LC patients participated in the nominal group meetings. Thirty-five case-mix variables and 45 outcomes variables were proposed during the meetings. Nevertheless, consensus was only achieved for 13 case-mix (n=2 demographic factors, n = 3 baseline clinical factors, n = 7 baseline tumor factors and n = 1 treatment factors) and six outcomes variables across the four nominal groups (Supplementary Tables 2, 3).
Second Scientific Committee Meeting
Based on the results achieved during the nominal group meetings, the scientific committee identified the variables to be included in the standardized set of health outcomes for LC. The variables finally included in the standard set are presented below.
Case-Mix Variables (Table 3)
Case-mix variables include those that allow patient characterization. Assessment of these variables should be carried out in the first visit after diagnosis, prior to treatment initiation.
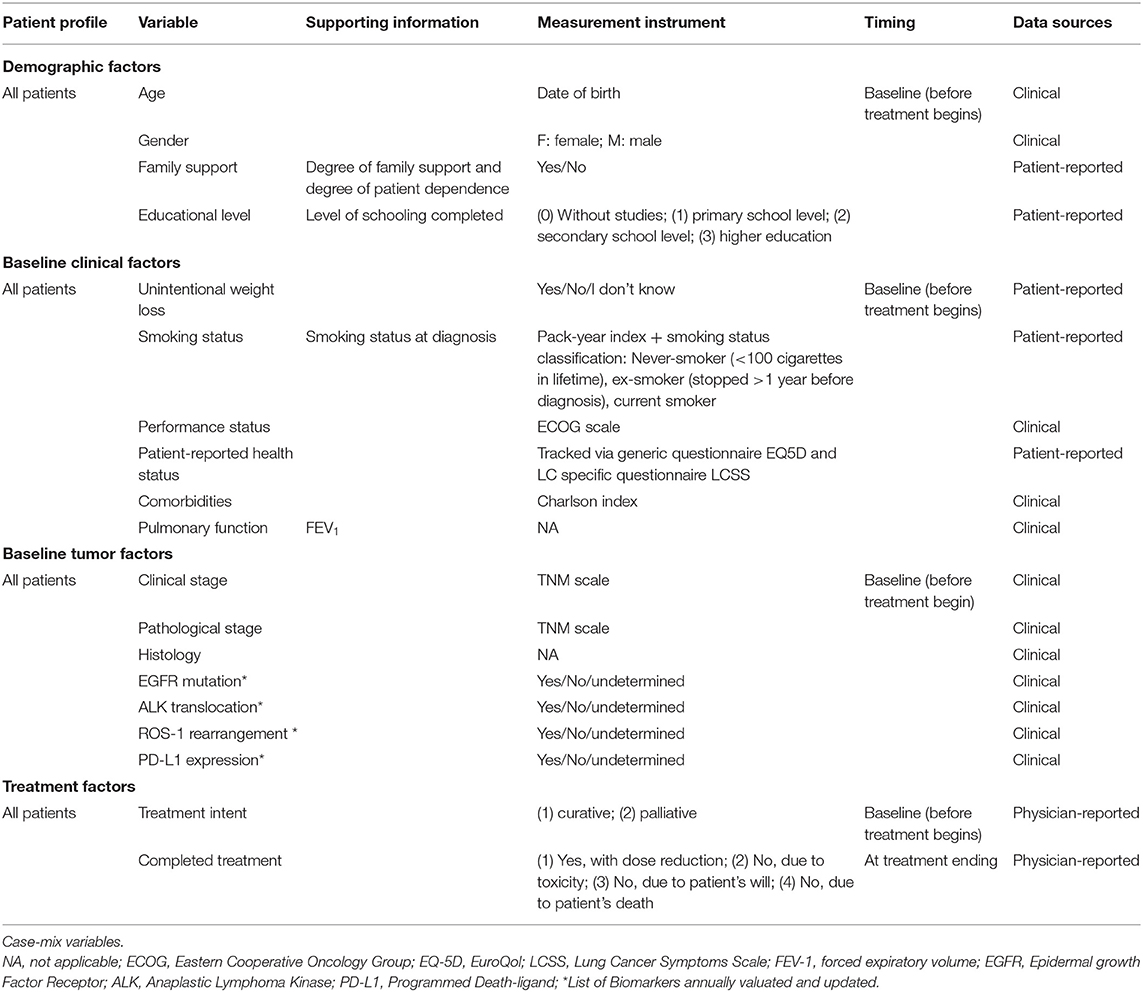
Table 3. Spanish standard set of patient-centered outcomes in LC.
In addition to the sociodemographic variables included in the original ICHOM standard set (age and gender), it was agreed to collect the family support, as it may reflect the patient's family environment, as well as, the degree of patient dependence. Even though consensus was not reached among the nominal groups about whether to include educational level as a case mix variable, the scientific committee considered appropriate to include it as a surrogate measurement of socioeconomic status. This decision was motivated by previous studies showing a relationship between educational level and patient prognosis (19, 20). Conversely, despite ICHOM recommendation, collection of ethnicity data was considered not relevant to the Spanish setting, and was, therefore, excluded from the set.
Aligned with the ICHOM recommendations, it was agreed to gather data regarding the following baseline clinical factors: unintentional weight loss, smoking status, comorbidities, performance status and patient's HRQoL. In addition, due to its prognostic value, assessment of pulmonary function, through the measurement of forced expiratory volume (FEV-1), was also included in the set.
Consensus was reached on the use of Charlson Comorbidity Index (21) to collect the comorbidities. Experts discouraged the use of the questionnaire suggested by ICHOM, the Modified Self-administered Comorbidity Questionnaire (22) for two main reasons. First, a Spanish translation and validation of the questionnaire is not currently available. Second, experts considered that self-reporting of comorbidities may lead to underestimating of the comorbidities perceived by patients as irrelevant or unknown.
To assess patients' performance status, experts agreed on the use of the Eastern Cooperative Oncology Group (ECOG) scale. This scale describes a patient's level of functioning in terms of self-care, carrying out daily activities, and physical ability (23).
The ICHOM proposed instruments to measure patient-reported health status [EORTC-QLQ-C30 (24) and the LC specific version QLQ-LC13 (25)] were not deemed appropriate in the Spanish setting, as they are burdensome to complete and their use is limited in routine clinical practice. Instead, consensus was reached to use the generic questionnaire EuroQol EQ-5D (26, 27), that is currently widely used in the Spanish setting, and the LC specific questionnaire Lung Cancer Symptom Scale (LCSS) (28), for which a Spanish validated version is already available. The combined use of both questionnaires allows to gather information about patient perspective on their physical and emotional functioning, fatigue, vitality, pain, cough, breathing difficulty, hemoptysis, and loss of appetite.
The clinical and pathological stage, defined by the TNM staging scale, tumor histology and basis of diagnosis (clinical, histological, or cytological), were identified as key variables to be recorded as a case-mix variable.
Consensus was reached on including LC predictive biomarkers such as EGFR gene mutational status, ALK gene translocation, ROS-1 rearrangement and PD-L1 expression. Due to the continuous advances on the molecular mechanisms of LC, it was agreed to annually evaluate and update the list of biomarkers to be included in the standard set.
Regarding patient treatment, it was agreed to collect data on treatment intention (curative vs. palliative) and whether treatment was completed (with or without dose reduction) or non-completed (due to toxicity, patient's decision or patient's death).
Outcomes (Table 4)
Survival
LC is associated with high mortality rates (1). Thus, overall survival was considered a key variable to be included in the standard set for patient's follow up. Moreover, participants agreed on gathering information regarding the cause of death, indicating whether it was tumor or treatment related. Conversely, following ICHOM recommendations, progression-free survival (PFS) was excluded from the standard set. Although PFS is commonly assessed in most clinical trials as a measure of disease control, it was considered potentially unreliable due to ascertainment bias and, ultimately, less important than overall survival.
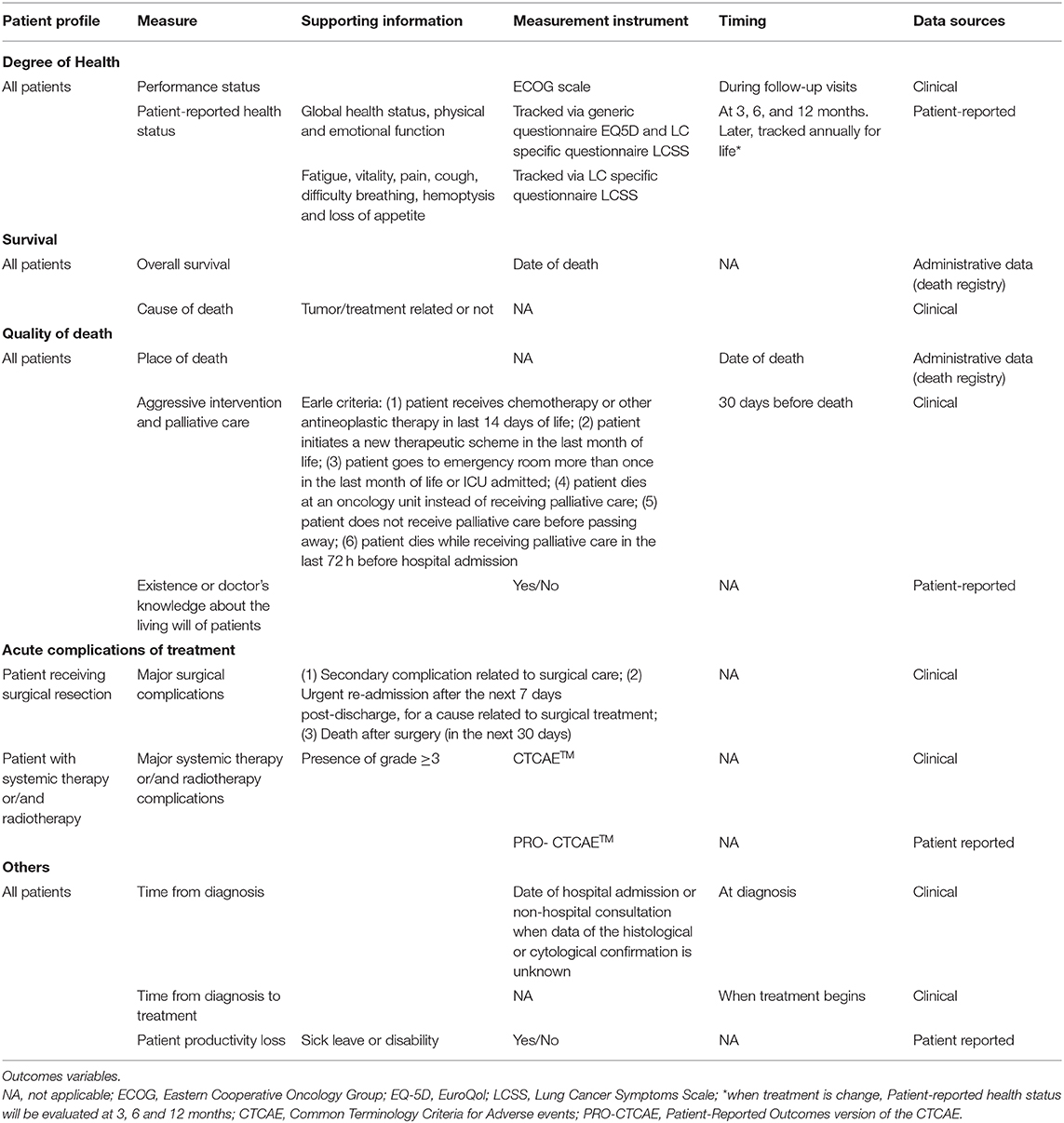
Table 4. Spanish standard set of patient-centered outcomes in LC.
Complications of treatment
In line with ICHOM classification, treatment complications were divided to surgery-related or associated with systemic therapy and/or radiotherapy. Participants agreed on monitoring surgery-related complications using the Observatorio de Resultados del Servicio Madrileño de Salud (Outcomes Observatory of Madrid Healthcare Services) classification. This classification includes the reporting of whether the patient: (1) suffers a secondary complication related to surgical care, (2) requires an urgent re-admission for a cause related to surgical treatment in the first 7 days following discharge, or (3) dies in the first 30 days after surgery (29).
In regard to the complications of systemic therapy and/or radiotherapy, participants emphasized the importance of both patient self-reporting and clinician reporting of adverse events. Therefore, a consensus was reached to collect all grade 3 or higher adverse events using both the Common Terminology Criteria for Adverse Events (CTCAE) and Patient-Reported Outcomes version of the CTCAE (PRO-CTCAE). Although the use of such instruments might be time-consuming, participants agreed that a standardized collection of treatment toxicities is necessary to avoid the risk of overlooking important complications, and to ensure their inclusion in the medical record.
Degree of health
HRQoL and performance status are frequently impaired in LC patients (5, 8). Therefore, and in line with ICHOM recommendations, it was agreed to collect both variables at baseline and during patients' follow up. As previously indicated, ECOG scale (23) was selected to assess patients' performance status, while the EQ-5D (26, 27) and LCSS questionnaire (28) were chosen for the assessment of patients' HRQoL.
Quality of death (end of life care)
Ensuring an adequate quality of end-of-life care as well as the respect of patients' wills has become a key healthcare objective (30). Therefore, besides capturing place of death, participants stressed the importance of assessing the alignment between the care received at the end of life and patients' living will. For this purpose, it was agreed to register whether patients had a living will, received aggressive care, and had access to palliative care in the last 30 days of life, using Earle Criteria adapted for individual patient use (Table 4). Earle Criteria evaluate quality of end of life care by assessing: (a) administration of new anticancer therapies or continuation of ongoing treatments very near death, (b) number of emergency room visits, inpatient hospital admissions or intensive care unit days near the end of life and (c) inadequate access to palliative care and/or enrollment in hospice (31).
Others
Experts agreed to report both the date of diagnosis and the time interval from diagnosis to treatment. Patient's and/or caregiver's working life might be substantially influenced by both the disease and treatment, causing potential situations of absenteeism, presentism, or sick leave. In this light, experts agreed to report patient's and/or caregiver's productivity loss, by collecting sick leave or occupational disability for both patients and caregivers.
Discussion
In clinical practice, measurement of outcomes that matter to LC patients, aside from survival, remains limited. However, to promote patient-centered care, the collection of outcomes based on the patient's priorities is crucial. Experience from the implementation of ICHOM standard sets in clinical practice, in diseases such as hip and knee osteoarthritis (32), cleft lip and palate (33), coronary artery disease (34) or Parkinson's Disease (35), has shown a positive impact on all phases of the care process. Likewise, a one-year pilot study conducted in Netherlands demonstrated that the ICHOM standard set can be implemented during routine lung cancer treatment without significantly disturbing the routine workflow (36, 37). The authors concluded that the collection of PROs is not too time-consuming, however it requires ad hoc tools and dedicated staff (36, 37).
Patient information collated via PRO measures (PROMs) allows clinicians to explore the perspective of the patients on different aspects of the disease, during the follow-up.
This, in turn, promote a better involvement of the patient in disease management (32–35). Moreover, PROMs use provides the opportunity for patients to engage in their consultation in advance, increasing self-awareness of their health and helping them to tailor the consultation to their needs (32–35). Of note, healthcare professionals also perceive the use of these standard sets as a valuable tool that facilitates benchmarking. Indeed, clinicians can learn from the outcomes data they gather and, at the same time, share their knowledge and learn from the experience of other healthcare professionals in different settings (32–35).
Adaptation of the ICHOM standard set for LC to the Spanish setting are essential steps in order to allow its implementation in routine clinical practice since it allows to identify those variables and its instruments, proposed by ICHOM that (1) are routinely collected in Spanish clinical practice and/or Spanish clinicians and patients are familiarized with; (2) the technology needed to measure them is available in the Spanish setting; and (3) the instruments to collect them are available and validated in Spanish language.
In this regard, several of the PROMs proposed by ICHOM have either not yet been validated or have had limited use in the Spanish context, thus hindering their use in daily practice. Thus, although divergence from the original standard set developed by ICHOM might partly complicate international benchmarking of LC patients' outcomes, selecting the most suitable PROMs to our setting is essential to ensure their use.
This standard set reflects the opinion of a group of 35 experts on the management of LC and 5 patient representatives. Since one of the main purposes of the standard set is to reflect outcomes that matter to patients, their broad participation in the project is one of its main strengths. Patient representatives have been actively involved in the decision-making process as members of the scientific committee or participants in the nominal groups. Although no major differences are expected, it is important to highlight that different groups of experts and patients could have agreed on different recommendations. In order to minimize this potential bias, and ensure national representativeness, participants from four broad geographic areas were involved in the project.
It must be acknowledged that the update of the literature review, on which the present standard set is based, covers studies published until 31/12/2017. Thus, some relevant variables (e.g., the determination of recently identified LC related biomarkers) may have not been considered when elaborating the standard set. To minimize this limitation, and due to the continuing advances in both the knowledge and treatment of this disease, we recommend to periodically update the list of biomarkers to evaluate during patient follow-up. In addition, we also suggest that the present standard set be periodically updated.
Of note, the present adaptation of the ICHOM standard set for LC represents a starting point, and several barriers need to be addressed on the road to its successful implementation in the Spanish setting. Namely, the time required for the collection of the variables proposed, the lack of digital tools allowing a systematic and automatic PROMs compilation, together with a limited education and information of patients and clinicians about PROMs, have been identified as the main barriers to the implementation of the present standard set (38). Newer platforms for data collection, based on information and communication technologies, may reduce both patient and clinician burden, as well as, data processing time, thus facilitating the use or PROMS in clinical practice (39). Other barriers to be tackled to ensure widespread use of this standard set are inherent to the structure of the Spanish national healthcare system (SNHS). Indeed, one of the main characteristics of the SNHS is its heterogeneity: healthcare processes, organizational models as well as information systems differ widely both among and within regions. This heterogeneity has been also observed in the context of LC, with a recent study showing remarkable differences among Spanish regions in the provision of care for LC patients (40). Overall, these data indicate the need to promote harmonization of the best practice in LC management and treatment to guarantee the success of this initiative.
Besides addressing the aforementioned barriers, a further step to test the feasibility and promote the integration of the defined standard set into the Spanish healthcare model may involve the conduction of a pilot implementation study. Indeed, due to the heterogeneity of SNHS, a pilot study is key to determine the feasibility and viability of introducing the standard set in routine clinical practice. The results of the pilot study may provide insights into the main resource requirements and organizational challenges to be tackled during the implementation.
Although data from Standard Set implementation is limited, previous experiences suggest that several requirements are needed to ensure its implementation in a particular setting: (1) appropriate staff to support the implementation of PROMs tools, facilitate ongoing data collection, and maximize the completeness of data collection and, (2) adequate technology to support for database/platform development. Moreover, during the implementation process the knowledge of existing workflows for patient assessment and review, and the patient's journey in the hospital system is crucial.
Conclusion
The present adaptation of ICHOM standard set may facilitate its implementation in Spanish clinical practice, paving the way to standardize the collection of variables in LC, and promoting the incorporation of patients' perspective in LC management. In turn, the information provided through the systematic compilation of this set of variables may allow both clinicians and health policy makers to define strategies aimed at achieving high-quality and patient-centered care.
Data Availability Statement
All datasets generated for this study are included in the article/Supplementary Material.
Ethics Statement
Ethical review and approval was not required for the study on human participants in accordance with the local legislation and institutional requirements.
Author Contributions
VE-V, AC, MB, RC-B, CP, CG, JS, AO, and LL contributed to the conceptualization and design of the study. MA contributed to the conceptualization and design of the study, data curation, and data analysis. MC contributed to the conceptualization and design of the study, data curation, data analysis, and wrote the first draft of the manuscript. All authors contributed to manuscript revision, read, and approved the submitted version.
Funding
The project was funded by Bristol-Myers Squibb.
Conflict of Interest
VE-V has received support to continuing education/advisory fees from Amgen, Astellas, AstraZeneca, Boehringer-Ingelheim, Bristol-Myers Squibb, Ipsen Pharma, Janssen, and Merck Sharp & Dohme. AC has received honorary/consulting fees from AstraZeneca, Boehringer-Ingelheim, Pfizer, Roche/Genentech, Eli Lilly and Company, Novartis, Merck Sharp & Dohme, and Bristol-Myers Squibb. MB has received support to continuing education/advisory fees from Abbvie and Roche. RC-B has received support to continuing education/advisory fees: Boehringer-Ingelheim, Janssen and Merck Sharp & Dohme, Hoffmann-La Roche and Pfizer. CP, CG, JS, and AO are employees of Bristol-Myers Squibb. MA, MC, and LL work for an independent research entity that received funding from Bristol-Myers Squibb to coordinate and conduct the study.
Acknowledgments
The authors would like to thank to all participants in the nominals groups and to the following Spanish Scientific Societies for endorsing the Project: Sociedad Española de Oncología Médica (SEOM), Grupo Español de Cáncer de Pulmón (GECP), Fundación para la Excelencia y la Calidad de la Oncología (ECO), Asociación para la Investigación del Cáncer de Pulmón en Mujeres (ICAPEM) and Sociedad Española de Farmacia Hospitalaria (SEFH)], and to Spanish patients' advocacy groups [Asociación Española de Afectados de Cáncer de Pulmón (AEACaP) and Grupo Español de Pacientes con Cáncer (GEPAC)].
Supplementary Material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fonc.2020.01645/full#supplementary-material
References
1. Sociedad Española de Oncología Médica. Las cifras del cáncer en España 2018. Sociedad Española de Oncología Médica (2018).
2. Escuín JS. Lung cancer in Spain. Current epidemiology, survival, and treatment. Arch Bronconeumol. (2009) 45:341–8. doi: 10.1016/S1579-2129(09)72435-8
3. Lemjabbar-Alaoui H, Hassan OU, Yang Y, Buchanan P. Lung cancer: biology and treatment options. Biochim Biophys Acta. (2015) 1856:189–210. doi: 10.1016/j.bbcan.2015.08.002
4. Majem M, Juan O, Insa A, Reguart N, Trigo JM, Carcereny E, et al. SEOM clinical guidelines for the treatment of non-small cell lung cancer (2018). Clin Transl Oncol. (2019) 21:3–17. doi: 10.1007/s12094-018-1978-1
5. Gralla RJ, Hollen PJ, Msaouel P, Davis BV, Petersen J. An evidence-based determination of issues affecting quality of life and patient-reported outcomes in lung cancer: results of a survey of 660 patients. J Thorac Oncol. (2014) 9:1243–8. doi: 10.1097/JTO.0000000000000244
6. Walker MS, Houts AC, Miller PJE, Schwartzberg LS, Stepanski EJ, Pohl GM, et al. Analysis of the psychological impact of cancer-related symptoms on patients with non-small cell lung cancer. Psychooncology. (2017) 26:755–62. doi: 10.1002/pon.4071
7. Migliorino MR, Santo A, Romano G, Cortinovis D, Galetta D, Alabiso O, et al. Economic burden of patients affected by non-small cell lung cancer (NSCLC): the LIFE study. J Cancer Res Clin Oncol. (2017) 143:783–91. doi: 10.1007/s00432-016-2326-x
8. Iyer S, Taylor-Stokes G, Roughley A. Symptom burden and quality of life in advanced non-small cell lung cancer patients in France and Germany. Lung Cancer. (2013) 81:288–93. doi: 10.1016/j.lungcan.2013.03.008
9. Iyer S, Roughley A, Rider A, Taylor-stokes G. The symptom burden of non-small cell lung cancer in the USA : a real-world cross-sectional study. Support Care Cancer. (2014) 22:181–7. doi: 10.1007/s00520-013-1959-4
10. Denis F, Basch E, Septans A-L, Bennouna J, Urban T, Dueck AC, et al. Two-year survival comparing web-based symptom monitoring vs routine surveillance following treatment for lung cancer. JAMA. (2019) 321:306–7. doi: 10.1001/jama.2018.18085
11. Denis F, Lethrosne C, Pourel N, Molinier O, Pointreau Y, Domont J, et al. Randomized trial comparing a web-mediated follow-up with routine surveillance in lung cancer patients. J Natl Cancer Inst. (2017) 109:1–8. doi: 10.1093/jnci/djx029
12. Basch E, Deal AM, Kris MG, Scher HI, Hudis CA, Sabbatini P, et al. Symptom monitoring with patient-reported outcomes during routine cancer treatment: a randomized controlled trial. J Clin Oncol. (2016) 34:557–65. doi: 10.1200/JCO.2015.63.0830
13. Basch E, Deal AM, Dueck AC, Scher HI, Kris MG, Hudis C, Schrag D. Overall survival results of a trial assessing patient-reported outcomes for symptom monitoring during routine cancer treatment. JAMA. (2017) 318:197–8. doi: 10.1001/jama.2017.7156
14. Porter M, Larsson S, Lee T. Standardizing patient outcomes measurement Michael. N Engl Med. (2016) 374:504–6. doi: 10.1056/NEJMp1511701
15. International Consortium for Health Outcomes Measurement (ICHOM) (2019). Available online at: https://www.ichom.org/standard-sets/ (accessed July 18, 2019).
16. Mak KS, Van Bommel ACM, Stowell C, Abrahm JL, Baker M, Baldotto CS, et al. Defining a standard set of patient-centred outcomes for lung cancer. Eur Respir J. (2016) 48:852–60. doi: 10.1183/13993003.02049-2015
17. Gallagher M, Hares T, Spencer J, Bradshaw C, Webb I. The nominal group technique: a research tool for general practice? Fam Pract. (1993) 10:76–81. doi: 10.1093/fampra/10.1.76
18. Potter M, Gordon S, Hamer P. The Nominal Group Technique: a useful consensus methodology in physiotherapy research. New Zeal J Physiother. (2004) 32:126–30.
19. Brusselaers N, Mattsson F, Lindblad M, Lagergren J. Association between education level and prognosis after esophageal cancer surgery: a Swedish population-based cohort study. PLoS ONE. (2015) 10:e0121928. doi: 10.1371/journal.pone.0121928
20. Cavalli-Björkman N, Lambe M, Eaker S, Sandin F, Glimelius B. Differences according to educational level in the management and survival of colorectal cancer in Sweden. Eur J Cancer. (2011) 47:1398–406. doi: 10.1016/j.ejca.2010.12.013
21. Charlson ME, Pompei P, Ales KL, MacKenzie R. A new method of classifying prognostic comorbidity in longitudinal studies: development and validation. J Chron Dis. (1987) 40:373–83. doi: 10.1016/0021-9681(87)90171-8
22. Sangha O, Stucki G, Liang MH, Fossel AH, Katz JN. The self-administered comorbidity questionnaire: a new method to assess comorbidity for clinical and health services research. Arthritis Rheum. (2003) 49:156–63. doi: 10.1002/art.10993
23. Oken MM, Creech R, Tormey DC, Horton J, Davis TE, McFadden ET, et al. Toxicity and response criteria of the Eastern Cooperative Oncology Group. Am J Clin Oncol. (1982) 5:649–55. doi: 10.1097/00000421-198212000-00014
24. Fayers P, Bottomley A. Quality of life research within the EORTC—the EORTC QLQ-C30. Eur J Cancer. (2002) 38:125–33. doi: 10.1016/S0959-8049(01)00448-8
25. Bergman B, Aaronson NK, Ahmedzai S, Kaasa S, The E Sullivan M EORTC J. The EORTC QLQ-LC13: a modular supplement to the Quality of Life Questionnaire (QLQ-C30) for use in lung cancer clinical trials. Gr Qual Life Eur. (1994) 13:635–42. doi: 10.1016/0959-8049(94)90535-5
26. Tsang HHL, Cheung JPY, Wong CKH, Cheung PWH, Lau CS, Chung HY. Psychometric validation of the EuroQoL 5-dimension (EQ-5D) questionnaire in patients with spondyloarthritis. Arthritis Res Ther. (2019) 21:41. doi: 10.1186/s13075-019-1826-x
27. Badia X, Roset M, Montserrat S, Herdman M, Segura A. The Spanish version of EuroQol: a description and its applications. European Quality of Life scale. Med Clin. (1999) 112 (Suppl.):79–85.
28. Hollen PJ, Gralla RJ, Kris MG, Potanovich LM. Quality of Life Assessment in individuals with lung cancer : Testing the Lung Cancer Symptom Scale (LCSS). Eur J Cancer. (1993) 29A:S51–8. doi: 10.1016/S0959-8049(05)80262-X
29. Servicio_Madrileño_de_Salud. Observatorio de Resultados del Servicio Madrileño de Salud Informe de Atención Primaria. Servicio_Madrileño_de_Salud (2013).
30. Rodríguez-Prat A, Monforte-Royo C, Porta-Sales J, Escribano X, Balaguer A. Patient perspectives of dignity, autonomy and control at the end of life: systematic review and meta-ethnography. PLoS ONE. (2016) 11:e0151435. doi: 10.1371/journal.pone.0151435
31. Earle CC, Park ER, Lai B, Weeks JC, Ayanian JZ, Block S. Identifying potential indicators of the quality of end-of-life cancer care from administrative data. J Clin Oncol. (2003) 21:1133–8. doi: 10.1200/JCO.2003.03.059
32. Ackerman IN, Cavka B, Lippa J, Bucknill A. The feasibility of implementing the ICHOM Standard Set for Hip and Knee Osteoarthritis: a mixed-methods evaluation in public and private hospital settings. J Patient-Reported Outcomes. (2018) 2:32. doi: 10.1186/s41687-018-0062-5
33. Arora J, Haj M. Implementing ICHOM's Standard Sets of Outcomes: Cleft Lip and Palate at Erasmus University Medical Centre in the Netherlands. London: International Consortium for Health Outcomes Measurement (ICHOM) (2016). Available online at: www.ichom.org
34. Arora J, Tavella R. Implementing ICHOM's Standard Sets of Outcomes: Coronary Artery Disease in the Coronary Angiogram Database of South Australia (CADOSA). London: International Consortium for Health Outcomes Measurement (ICHOM) (2017). Available online at: www.ichom.org
35. Arora J, Lewis S, Cahill A. Implementing ICHOM's Standard Sets of Outcomes: Parkinson's Disease at Aneurin Bevan University Health Board in South Wales, UK. London: International Consortium for Health Outcomes Measurement (ICHOM) (2017). Available online at: www.ichom.org
36. van Meerbeeck J, De Backer L, Hiddinga B, Janssens A. Pilot Trial of the ICHOM Lung Cancer Standard Set. European Respiratory Society, PA4234.
37. Van Meerbeeck J, De Backer L, Janssens A, Hiddinga B, Vanhoutte G. P1.04-028 Collection of ICHOM-Defined Patient-Reported Outcome Measures (PROMs) during Routine Lung Cancer Treatment: A Pilot Study. J Thorac Oncol. (2017) 12:S612. doi: 10.1016/j.jtho.2016.11.784
38. Alonso-Caballero J, Ferrer-Fores M. Monografías de Política y Gestión. Resultados reportados por los pacientes (PROs). Madrid (2017).
39. Wildevuur SE, Wl Simonse L. Information and communication technology–enabled person-centered care for the “Big Five” chronic conditions: scoping review. J Med Internet ResJ Med Internet Res. (2015) 17:e77. doi: 10.2196/jmir.3687
40. Rodríguez-Barranco M, Salamanca-Fernández E, Fajardo ML, Bayo E, Chang-Chan YL, Expósito J, et al. Patient, tumor, and healthcare factors associated with regional variability in lung cancer survival: a Spanish high-resolution population-based study. Clin Transl Oncol. (2019) 21:621–9. doi: 10.1007/s12094-018-1962-9
Keywords: lung cancer, patient-centered care, outcome measurement, patient-reported outcomes, patient centricity, quality of life, standard set, ICHOM
Citation: Escudero-Vilaplana V, Calles A, Collado-Borrell R, Belén Marzal-Alfaro M, Polanco C, Garrido C, Suarez J, Ortiz A, Appierto M, Comellas M and Lizán L (2020) Standardizing Health Outcomes for Lung Cancer. Adaptation of the International Consortium for Health Outcomes Measurement Set to the Spanish Setting. Front. Oncol. 10:1645. doi: 10.3389/fonc.2020.01645
Received: 04 March 2020; Accepted: 27 July 2020;
Published: 02 September 2020.
Edited by:
Stephen V. Liu, Georgetown University Medical Center, United StatesReviewed by:
Sushma Jonna, MedStar Georgetown University Hospital, United StatesManuel Cobo Dols, Junta de Andalucía, Spain
Copyright © 2020 Escudero-Vilaplana, Calles, Collado-Borrell, Belén Marzal-Alfaro, Polanco, Garrido, Suarez, Ortiz, Appierto, Comellas and Lizán. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Vicente Escudero-Vilaplana, dmljZW50ZS5lc2N1ZGVyb0BzYWx1ZC5tYWRyaWQub3Jn