 Stefano Restaino1
Stefano Restaino1 Federico Paparcura2Cristina Giorgiutti2
Federico Paparcura2Cristina Giorgiutti2 Diletta Trojan3
Diletta Trojan3 Giulia Montagner3Giancarlo Pengo4
Giulia Montagner3Giancarlo Pengo4 Grazia Pividore5Roberta Albanese6Emanuele Rampino6Teresa Dogareschi7Tiziana Bove2,7
Grazia Pividore5Roberta Albanese6Emanuele Rampino6Teresa Dogareschi7Tiziana Bove2,7 Francesca Titone8Marco Trovò8
Francesca Titone8Marco Trovò8 Giorgia Garganese9,10Pier Camillo Parodi6
Giorgia Garganese9,10Pier Camillo Parodi6 Giovanni Scambia10,11
Giovanni Scambia10,11 Lorenza Driul2*Giuseppe Vizzielli2
Lorenza Driul2*Giuseppe Vizzielli2- 1Department of Maternal and Child Health, Obstetrics and Gynecology Clinic, University Hospital of Udine, Udine, Italy
- 2Medical Area Department (Dipartimento di Area Medica, DAME), Università degli Studi di Udine, Udine, Italy
- 3Fondazione Banca dei tessuti di Treviso Onlus, Treviso, Italy
- 4Surgical Video Production & Multimedia Medical – Azienda Sanitaria Universitaria Friuli Centrale, Udine, Italy
- 5Piwimed s.r.l., Udine, Italy
- 6Dipartimento di Scienze Chirurgiche, Clinica di Chirurgia Plastica Ricostruttiva, Università degli Studi di Udine, Udine, Italy
- 7Department of Anesthesia and Intensive Care, University Hospital of Udine, Udine, Italy
- 8Radiation Oncology Department, University Hospital of Udine, Udine, Italy
- 9Gynecology and Breast Care Center, Mater Olbia Hospital, Olbia, Italy
- 10Dipartimento di Scienze della Vita e Sanità Pubblica, Università Cattolica del Sacro Cuore, Roma, Italy
- 11Dipartimento per la salute della Donna e del Bambino e della Salute Pubblica, Fondazione Policlinico Universitario Agostino Gemelli IRCCS, Unità Operativa Complessa Ginecologia Oncologica, Roma, Italy
Background: The application of the amniotic membrane could have a favourable effect on tissue repair and regeneration. We report the first case of implant of an amniotic membrane in a patient affected by myo-cutaneous dehiscence, after a radical surgical treatment for vulvar cancer.
Methods: We describe a case of a 74-years-old patient affected by vulvar cancer. After radiotherapy, the patient underwent to an anterior pelvic exenteration with uretero-ileo-cutaneostomy by Wallace, bilateral pelvic lymphadenectomy, omental biopsies, omental flap, bilateral inguinal lymphadenectomy, resection of ulcerated left inguinal lesion, reconstruction with left gracilis muscle flap and locoregional V-Y advancement flap. The patient developed a myo-cutaneous dehiscence. Two months after the surgery, following an accurate curettage of the wound and negative pressure therapy, a patch of human amniotic membrane was implanted.
Results: The surgical procedure was easy, feasible and did not require long operating room times. No intraoperative or postoperative complications occurred. The results obtained were encouraging with a marked improvement in the surgical wound.
Conclusion: the use of amniotic membranes was safely and easily performed to promote the healing of complicated surgical wounds.
Introduction
Vulvar cancer is one of most rare gynecological tumors, in fact, it accounts for only 2-5% of the cases (1). Squamous cell carcinoma (SCC) of the vulva, the most common subtype, has traditionally been considered a disease of postmenopausal women, although the average age of incidence has decreased in recent years due to the increase in HPV infections worldwide (1–4). The treatment of vulvar cancer depends mainly on histology and staging (1, 2), other variables influencing the management are age, coexistence of comorbidities and the patient’s performance status. Treatment is predominantly surgical, particularly for SCC, although concomitant chemoradiation is an effective alternative, particularly for advanced tumors and those where pelvic exenteration would be necessary to obtain adequate surgical edges (1–5). The most severe and common postoperative complications of vulvar cancer surgery are lymphedema, lymphocele, and wound dehiscence. In particular, en bloc surgery raised complications and wound dehiscence to 70-90% of cases (6, 7). The use of negative pressure therapy is an option for the conservative management of large wounds dehiscence (8). Human amniotic membrane (HAM) has been reported as a versatile graft in many surgical interventions. The first clinical application of HAM dates back to 1910 (9) and since then several studies reports its efficacy, especially as a biological dressing for chronic wounds (10, 11), but also in gynecological surgery (12, 13). In fact, HAM promotes cell migration and proliferation; it has anti-inflammatory and antimicrobial properties without prompting immunoreaction in the recipient (14–17). We describe the first case of implantation of HAM in a patient affected by vulvar cancer with a myocutaneuos dehiscence.
Case description
We report the case of a 74-year-old female patient with previous bilateral salpingo-oophorectomy and hysterectomy for uterine fibromatosis. She had a clinical history of hypertension and dyslipidaemia and a silent family history. The patient came to our attention due to the development of itching and vulvar oedema associated with leucoxantorrhoea. A gynaecological examination under narcosis with multiple biopsies was performed. Histological examination diagnosed unrelated HPV infiltrating squamous cell carcinoma cT3 N2 MX. Staging MRI and PET-CT were subsequently performed, which confirmed vulvar neoplasia with locoregional infiltration and bilateral lymph node localisation. Imaging also revealed the presence of a lung abdensation, which was biopsied and diagnosed as adenocarcinoma with pulmonary primitivity. The lung tumour underwent radiotherapy treatment, with complete response. On the subsequent PET-CT scan it was no longer described.
For the vulvar neoplasm, the patient underwent radiotherapy treatment for a total of 35 sessions. From 13th July 2021 to 28th September 2021, we performed exclusive radiotherapy treatment of vulvar neoplasm and loco-regional lymph node drainage (total dose 54 Gy in 35 sessions). Three months after radiotherapy treatment, we observed a persistent of the disease confirmed also by PET-CT scan examination. For this reason, the patient was submitted on 27th January 2022 to an anterior pelvic exenteration with uretero-ileo-cutaneostomy packing by Wallace (18), bilateral pelvic lymphadenectomy, omental biopsies, omental flap, bilateral inguinal lymphadenectomy, resection of ulcerated left inguinal lesion, reconstruction with left gracilis muscle flap and locoregional V-Y advancement flap. Two days after surgery, the gracilis muscle flap was distressed with subsequent dehiscence of the surgical wound (Figure 1). For this reason, we decided to apply negative pressure therapy at the dehiscence site. Considering the difficulties in healing on 11th April 2022 we decided to implant amniotic membrane on surgical wound because of its anti-inflammatory and antimicrobial properties (Figures 2A, B). The human amniotic membrane was provided by Treviso Tissue Bank Foundation, a non-profit health organization accredited by the National Transplant Centre. The placenta is collected from donors undergoing caesarean delivery, after their consent for the donation. Donors areselected and screened according to Italian requirement, that includes serological and molecular tests. The placenta is processed in a Good Manufacturing Practice (GMP) compliant facility, shortly after retrieval. The amniotic membrane is carefully detached from the chorion and rinsed with sterile saline solution to remove residual blood. Subsequently, amniotic membrane is immersed in a cocktail of antibiotics validated for tissue decontamination (19, 20). After the removal of blood and spongy residues, amniotic membrane is cut in patches of desired sizes, that are positioned on filters in contact with the stromal side, to keep the orientation. Amniotic membrane is then stored in vapor phase liquid nitrogen, immersed in a cryopreserving solution made up with Base medium (Alchimia Srl, Italy), DMSO (WAK-Chemie, Germany) and human albumin (Kedrion, Italy). On that date, the patient still had a continuous solution between the myocutaneous gracilis flap and the root of the right thigh, about 5-6 cm in longitudinal diameter, which deepened by about 2 cm. There was also a further continuous solution at the level of the root of the left thigh, the myocutaneous flap and the inguinal root, approximately 3 cm in maximum diameter and 1-2 cm deep, which was in continuity with the previous one at the level of the anal margin.

Figure 1 Myo-cutaneous dehiscence.
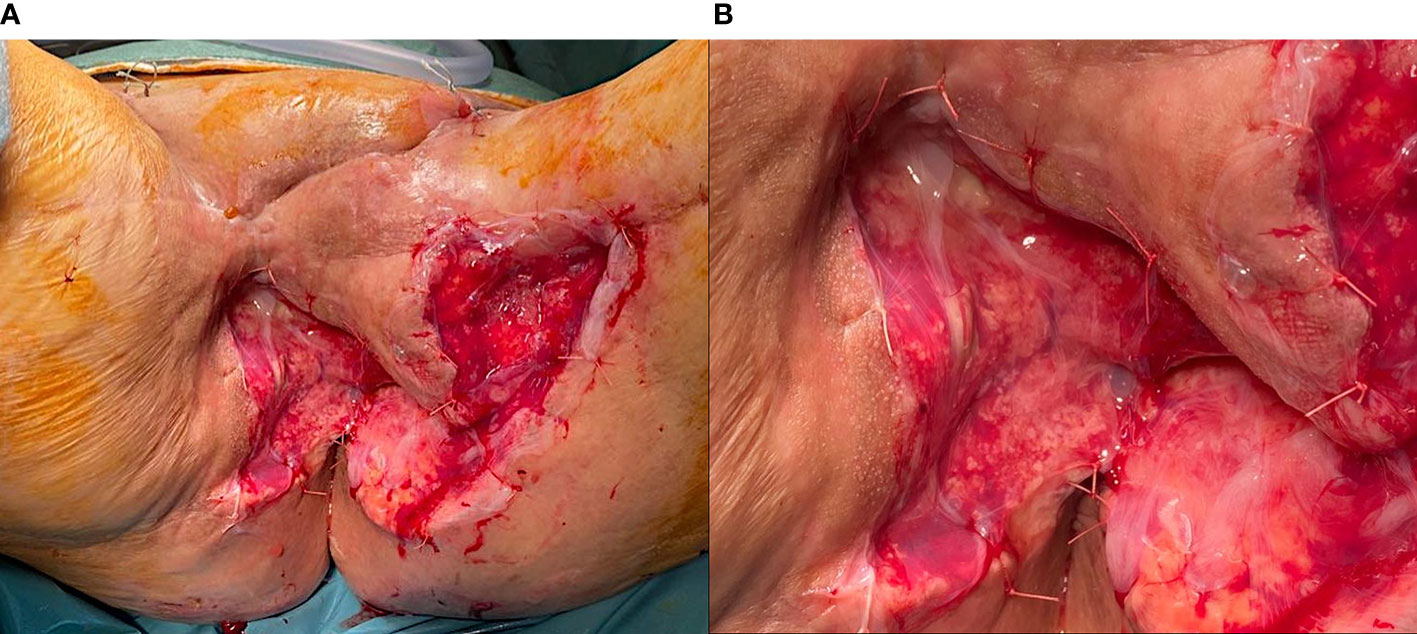
Figure 2 (A) Human amniotic membrane application. (B) Human amniotic membrane detail.
Surgical procedure
Under general anaesthesia, the patient was placed in the lithotomy position. We removed the negative pressure therapy. Following an accurate curettage of the vulvar scar with a curette to remove the granulation tissue, the tract was prepared for the implant of the HAM. The cryopreserved HAM resting on a filter was thawed in the operating room by immersion in a bath of saline solution at 40°C, without removing the packaging. It was subsequently washed twice in saline solution at 25°C; finally, one side of the square HAM was transfixed with a resorbable suture (2-0 Vicryl™, Ethicon Endo-Surgery, Inc., Cincinnati, OH, USA). Attention was paid to place the epithelial side of the HAM outward, to face the dehiscence wound (Figures 2A, B). The temporal timeline of the clinical case is showed in Figure 3.
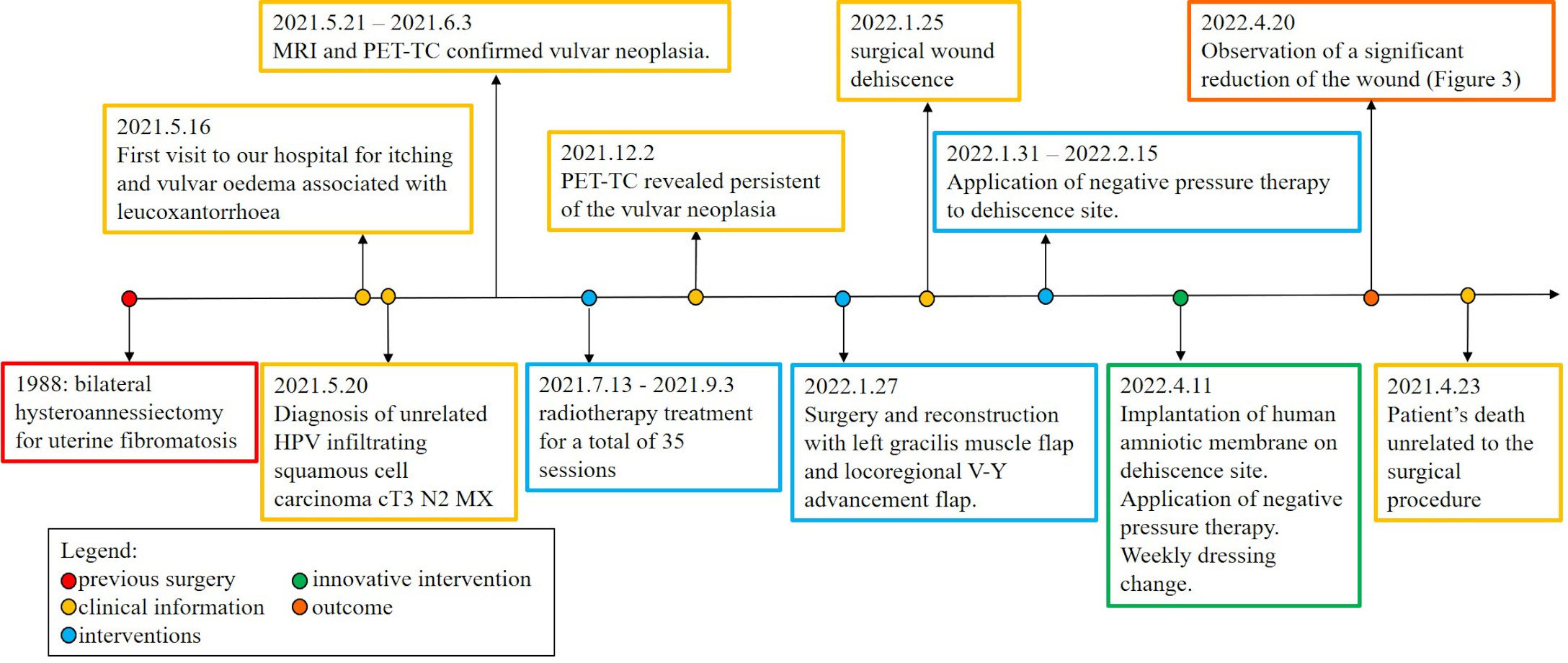
Figure 3 Timeline of the clinical case.
Results
No intraoperative or postoperative complications occurred. Stool softeners and analgesics were prescribed as needed. We continued to use negative pressure therapy at the wound site, changing the dressing weekly. Within 10 days of the amniotic membranes being placed, the wounds had significantly reduced (Figure 4). On 23rd April 2022 the patient died for other circumstances unrelated to the surgical procedure. However, the results obtained were encouraging with a marked improvement in the surgical wound.

Figure 4 Effect of human amniotic membrane after two weeks.
Discussion
The implantation of amniotic membranes on surgical wounds appears to be safe; moreover, the psychological impact of the treatment on our patient was acceptable, with an improvement also in terms of pain and thus quality of life. HAM has already been used in several sites of the gastrointestinal tract, such as the duodenum, colon and rectovaginal fistula (21, 22). The use of HAM is also a widespread clinical practice in other fields of medicine such as eye surgery and the treatment of an increasing number of ocular surface diseases (23).
To our knowledge, this is the first case of using HAM to promote healing of a surgical wound in a patient with gynecological oncology. The benefits of amniotic membrane placement in difficult-to-heal surgical wounds could be related to its anti-inflammatory and antimicrobial properties and low immunogenicity (14–17). In fact, no immunosuppression therapy was administered to the patients and no immune reaction was triggered by the HAM, analogously to other published clinical application of this graft (24–27).
Due to sudden death, it was not possible to evaluate the long-term outcome of this procedure, but the results obtained seemed encouraging, considering the progression of healing achieved in the first two weeks after application of the amniotic membrane.
-.1This is an isolated case of the application of HAM, with a follow-up that is too limited to establish their real effectiveness.
Within the limits of this case report, a promising suggestion has been made regarding the use of HAM for gynecological surgery.
Conclusion
Taking into account the high risk of dehiscence in vulvar cancer patients undergoing radical surgery, the use of HAMs could be a weapon to be considered. Case series providing longer follow-up should be encouraged, in order to provide useful data for increased use of this technique. In particular, future clinical studies could aim at comparing the efficacy of HAM versus traditional techniques.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statement
Ethical review and approval was not required for the study on human participants in accordance with the local legislation and institutional requirements. The patients/participants provided their written informed consent to participate in this study. Written informed consent was obtained from the individual(s) for the publication of any potentially identifiable images or data included in this article.
Author contributions
SR: Conceptualization and original draft preparation; FP: data curation and methodology; CG: data curation; GM and DT were involved in the drafting and revision of the manuscript. GP: software; GP: visualization; RA: supervision; ER: supervision; TD: methodology; TB: supervision; GG: validation; PP: validation; GS: validation; LD: validation; GV: Conceptualization and supervision. All authors contributed to the article and approved the submitted version.
Acknowledgments
We thank Dr Morandini Marzia, Dr Barbui Elisa, Dr Spampinato Angelina, all nursing personnel and operating room staff of the Obstetrics and Gynecology Unit.
Conflict of interest
Author GPi was employed by Piwimed s.r.l.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Rogers LJ, Cuello MA. Cancer of the vulva. Int J Gynaecol Obstet (2018) 143 Suppl 2:4–13. doi: 10.1002/ijgo.12609
2. Kang YJ, Smith M, Barlow E, Coffey K, Hacker N, Canfell K. Vulvar cancer in high-income countries: Increasing burden of disease. Int J Cancer (2017) 141:2174–86. doi: 10.1002/ijc.30900
3. Hacker NF, Eifel PJ, van der Velden J. Cancer of the vulva. Int J Gynecol Obstet (2015) 131(Suppl 2):S76–83. doi: 10.1016/j.ijgo.2015.06.002
4. Koh WJ, Greer BE, Abu-Rustum NR, Campos SM, Cho KR, Chon HS, et al. Vulvar cancer, version 1.2017, NCCN clinical practice guidelines in oncology. J Natl Compr Canc Netw (2017) 15(1):92–12. doi: 10.6004/jnccn.2017.0008
5. Rao YJ, Chin RI, Hui C, Mutch DG, Powell MA, Schwarz JK, et al. Improved survival with definitive chemoradiation compared to definitive radiation alone in squamous cell carcinoma of the vulva: A review of the national cancer database. Gynecol Oncol (2017) 146(3):572–9. doi: 10.1016/j.ygyno.2017.06.022
6. Rahm C, Adok C, Dahm-Kähler P, Bohlin KS. Complications and risk factors in vulvar cancer surgery - a population-based study. Eur J Surg Oncol (2022) 48(6):1400–6. doi: 10.1016/j.ejso.2022.02.006
7. Gitas G, Proppe L, Baum S, Kruggel M, Rody A, Tsolakidis D, et al. A risk factor analysis of complications after surgery for vulvar cancer. Arch Gynecol Obstet (2021) 304(2):511–9. doi: 10.1007/s00404-020-05949-w
8. Norman G, Shi C, Goh EL, Murphy EM, Reid A, Chiverton L, et al. Negative pressure wound therapy for surgical wounds healing by primary closure. Cochrane Database Syst Rev (2022) 4(4):CD009261. doi: 10.1002/14651858.CD009261.pub7
9. Davis JW. Skin transplantation with a review of 550 cases at the johns Hopkins hospital. Johns Hopkins Med J (1910) 15:307. doi: 10.1097/00000658-190909000-00022
10. Valiente MR, Nicolás FJ, García-Hernández AM, Fuente Mora C, Blanquer M, Alcaraz PJ, et al. Cryopreserved amniotic membrane in the treatment of diabetic foot ulcers: A case series. J Wound Care (2018) 27(12):806–15. doi: 10.12968/jowc.2018.27.12.806
11. Mermet I, Pottier N, Sainthillier JM, Malugani C, Cairey-Remonnay S, Maddens S, et al. Use of amniotic membrane transplantation in the treatment of venous leg ulcers. Wound Repair Regener (2007) 15(4):459–64. doi: 10.1111/j.1524-475X.2007.00252.x
12. Bleggi-Torres LF, Werner B, Piazza MJ. Ultrastructural study of the neovagina following the utilization of human amniotic membrane for treatment of congenital absence of the vagina. Braz J Med Biol Res (1997) 30(7):861–4. doi: 10.1590/S0100-879X1997000700007
13. Fotopoulou C, Sehouli J, Gehrmann N, Schoenborn I, Lichtenegger W. Functional and anatomic results of amnion vaginoplasty in young women with Mayer-Rokitansky-Küster-Hauser syndrome. Fertil Steril (2010) 94(1):317–23. doi: 10.1016/j.fertnstert.2009.01.154
14. Wassmer CH, Berishvili E. Immunomodulatory properties of amniotic membrane derivatives and their potential in regenerative medicine. Curr Diabetes Rep (2020) 20(8):31. doi: 10.1007/s11892-020-01316-w
15. Hao Y, Ma DH, Hwang DG, Kim WS, Zhang F. Identification of antiangiogenic and antiinflammatory proteins in human amniotic membrane. Cornea (2000) 19(3):348–52. doi: 10.1097/00003226-200005000-00018
16. Adinolfi M, Akle CA, McColl I, Fensom AH, Tansley L, Connolly P, et al. Expression of HLA antigens, beta 2-microglobulin and enzymes by human amniotic epithelial cells. Nature (1982) 295(5847):325–7. doi: 10.1038/295325a0
17. Akle CA, Adinolfi M, Welsh KI, Leibowitz S, McColl I. Immunogenicity of human amniotic epithelial cells after transplantation into volunteers. Lancet (1981) 2(8254):1003–5. doi: 10.1016/S0140-6736(81)91212-5
18. Wallace DM. Ureteric diversion using a conduit: a simplified technique. Br J Urol (1966) 38(5):522–7. doi: 10.1111/j.1464-410X.1966.tb09747.x
19. Montagner G, Trojan D, Cogliati E, Manea F, Vantini A, Paolin A. Stability analysis of the antibiotic cocktail used by treviso tissue bank foundation for tissues decontamination. Cell Tissue Banking (2018) 19(4):721–6. doi: 10.1007/s10561-018-9725-y
20. Serafini A, Riello E, Trojan D, Cogliati E, Palù G, Manganelli R, et al. Evaluation of new antibiotic cocktails against contaminating bacteria found in allograft tissues. Cell Tissue Banking (2016) 17(4):619–28. doi: 10.1007/s10561-016-9581-6
21. Niknejad H, Peirovi H, Jorjani M, Ahmadiani A, Ghanavi J, Seifalian AM. Properties of the amniotic membrane for potential use in tissue engineering. Eur Cell Mater (2008) 15:88–99. doi: 10.22203/eCM.v015a07
22. Hosseini SV, Haghpanah Aski M, Al-Hurry AMAH, Hassan A-RK, Khazraei H, Zabangirfard Z, et al. Simultaneous application of human amniotic membrane and tachosil® in the repair of recto-vaginal fistula in an animal model. Comp Clin Path (2017) 26:405–9. doi: 10.1007/s00580-016-2391-1
23. Paolin A, Cogliati E, Trojan D, Griffoni C, Grassetto A, Elbadawy HM, et al. Amniotic membranes in ophthalmology: long term data on transplantation outcomes. Cell Tissue Bank (2016) 17(1):51–8. doi: 10.1007/s10561-015-9520-y
24. Frigerio I, Bannone E, Trojan D, Montagner G, Bergamaschi G, Butturini G. Implantation of amniotic membrane over pancreatic anastomosis after pancreaticoduodenectomy: report of the first case. J Surg Case Rep (2019) 2019(5):rjz097. doi: 10.1093/jscr/rjz097
25. Ragazzo M, Val M, Montagner G, Trojan D, Fusetti S, Guarda Nardini L. Human amniotic membrane: an improvement in the treatment of medication-related osteonecrosis of the jaw (MRONJ)? a case-control study. Cell Tissue Bank (2022) 23(1):129–41. doi: 10.1007/s10561-021-09922-y
26. Grossi U, Romano M, Rossi S, Gallo G, Picciariello A, Felice C, et al. Anal fistula human amniotic membrane endosealing (F-HAME): A proof of concept study. Front Surg (2022) 9:869923. doi: 10.3389/fsurg.2022.869923
Keywords: amniotic membrane, case report, allograft, vulvar cancer, dehiscence
Citation: Restaino S, Paparcura F, Giorgiutti C, Trojan D, Montagner G, Pengo G, Pividore G, Albanese R, Rampino E, Dogareschi T, Bove T, Titone F, Trovò M, Garganese G, Parodi PC, Scambia G, Driul L and Vizzielli G (2022) Human amniotic membrane for myocutaneous dehiscence after a radical surgical treatment of vulvar cancer: A case report. Front. Oncol. 12:1009884. doi: 10.3389/fonc.2022.1009884
Received: 02 August 2022; Accepted: 31 August 2022;
Published: 23 September 2022.
Edited by:
Federico Ferrari, University of Brescia, ItalyReviewed by:
Vito Andrea Capozzi, University Hospital of Parma, ItalyFrancesco Marasciulo, Civil Hospital of Brescia, Italy
Copyright © 2022 Restaino, Paparcura, Giorgiutti, Trojan, Montagner, Pengo, Pividore, Albanese, Rampino, Dogareschi, Bove, Titone, Trovò, Garganese, Parodi, Scambia, Driul and Vizzielli. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Lorenza Driul, bG9yZW56YS5kcml1bEB1bml1ZC5pdA==