 Damian T. Rieke1,2,3,4*
Damian T. Rieke1,2,3,4* Sebastian Schröder1Philippe Schafhausen5Eric Blanc3,6
Sebastian Schröder1Philippe Schafhausen5Eric Blanc3,6 Erika Zuljan3,6Benjamin von der Emde1Dieter Beule3,6
Erika Zuljan3,6Benjamin von der Emde1Dieter Beule3,6 Ulrich Keller1,4,7Ulrich Keilholz2,4
Ulrich Keller1,4,7Ulrich Keilholz2,4 Konrad Klinghammer1,4
Konrad Klinghammer1,4- 1Department of Hematology, Oncology and Cancer Immunology, Charité – Universitätsmedizin Berlin, Corporate Member of Freie Universität Berlin and Humboldt-Universität zu Berlin, Berlin, Germany
- 2Comprehensive Cancer Center, Charité – Universitätsmedizin Berlin, Corporate Member of Freie Universität Berlin and Humboldt-Universität zu Berlin, Berlin, Germany
- 3Berlin Institute of Health (BIH) at Charité – Universitätsmedizin Berlin, Berlin, Germany
- 4German Cancer Consortium (DKTK) and German Cancer Research Center (DKFZ), Heidelberg, Germany
- 5Department of Oncology, Hematology, and Bone Marrow Transplantation with Section of Pneumology, University Medical Center Hamburg-Eppendorf, Hamburg, Germany
- 6Core Unit Bioinformatics (CUBI), Berlin Institute of Health at Charité – Universitätsmedizin Berlin, Berlin, Germany
- 7Max-Delbrück-Center for Molecular Medicine, Berlin, Germany
Background and purpose: A subgroup of salivary duct carcinoma (SDC) harbor overexpression of the androgen receptor (AR), and co-occurring mutations in the HRAS- and PIK3CA-genes. The impact of genomic complexity on targeted treatment strategies in advanced cancer is unknown.
Materials and methods: We analyzed molecular and clinical data from an institutional molecular tumor board (MTB) to identify AR+, HRAS/PIK3CA co-mutated SDC. Follow-up was performed within the MTB registrational study or retrospective chart review after approval by the local ethics committee. Response was assessed by the investigator. A systematic literature search was performed in MEDLINE to identify additional clinically annotated cases.
Results: 4 patients with AR+ HRAS/PIK3CA co-mutated SDC and clinical follow-up data were identified from the MTB. An additional 9 patients with clinical follow-up were identified from the literature. In addition to AR overexpression and HRAS and PIK3CA-alterations, PD-L1 expression and Tumor Mutational Burden > 10 Mutations per Megabase were identified as additional potentially targetable alterations. Among evaluable patients, androgen deprivation therapy (ADT) was initiated in 7 patients (1 Partial Response (PR), 2 Stable Disease (SD), 3 Progressive Disease (PD), 2 not evaluable), tipifarnib was initiated in 6 patients (1 PR, 4 SD, 1 PD). One patient each was treated with immune checkpoint inhibition (Mixed Response) and combination therapies of tipifarnib and ADT (SD) and alpelisib and ADT (PR).
Conclusion: Available data further support comprehensive molecular profiling of SDC. Combination therapies, PI3K-inhibitors and immune therapy warrant further investigation, ideally in clinical trials. Future research should consider this rare subgroup of SDC.
1 Introduction
Salivary gland cancers (SGC) are a rare group of tumors with an incidence of about 1.3 cases/100,000 individuals in the United States (1). More than 20 distinct malignant subtypes have been described, many of which are defined by recurrent genetic alterations (2).
Salivary duct carcinoma (SDC) is an aggressive high-grade SGC subtype with a dismal prognosis. SDC most commonly arises in the parotid gland and accounts for about 1.8% of major salivary gland tumors in the SEER database (3–5). SDC can arise de-novo or ex pleomorphic adenoma (ex-PA) (4). Due to the aggressive nature of this disease, metastatic spread and a need for systemic therapy is frequent (6).
In addition to chemotherapy, targeted treatment strategies are increasingly used in SDC. SDC harbors recurrent molecular alterations such as HER2 and androgen receptor (AR) amplification and overexpression. Furthermore, FGFR1 amplification, PIK3CA, HRAS and TP53 mutations and PTEN and CDKN2A loss have been described (2, 4, 7, 8). Some of these alterations have been applied as predictive biomarkers for targeted therapy. Previous prospective studies have shown activity of HER2, AR and HRAS-directed therapy in SDC (9–11). Additionally, a prospective basket study showed a benefit of targeted therapy (targeting HER2 amplification, HER2, BRAF and PTCH1 mutation and high tumor mutational burden) in a large group of SGC, including SDC (12). No prospective trials supporting the efficacy of PI3K-inhibitors in PIK3CA-mutant SDC currently exist. A summary of ongoing and published clinical trials relevant for metastatic salivary duct carcinoma is provided in Table 1.
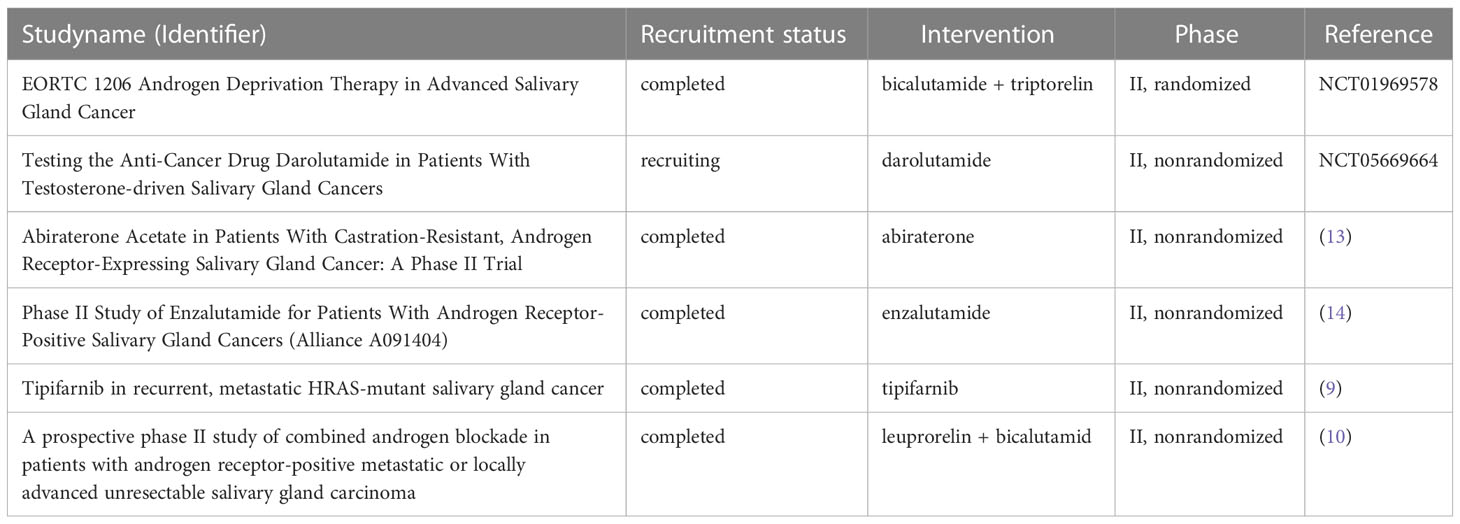
Table 1 Published and ongoing clinical trials relevant for salivary duct carcinoma, as identified from a structured search (MEDLINE clinical trials, search term “salivary gland cancer” on 17th May 2023, clinicaltrials.gov, search term “salivary gland AND metastatic” on 17th May 2023).
These results have led to a recommendation of comprehensive molecular analyses (e.g. next-generation panel or whole-exome sequencing) in patients with advanced SDC. These analyses should be done to assess opportunities for targeted therapy, including HER2- or AR-directed treatment (15, 16). Available data correspond to ESMO Scale of Clinical Actionability (ESCAT) scores of II-B (i.e. investigational therapy, alteration-drug match is associated with antitumor activity but magnitude of benefit is unknown) for AR (>70% positivity by immunohistochemistry, IHC) and HER2 (IHC score 3+ or fluorescence in situ hybridization positivity) in SGC. A participation in clinical trials is strongly recommended (15–17). The use of immune checkpoint inhibition remains investigational (15, 16). However, the FDA-approval of pembrolizumab in tumors with high tumor mutational burden also includes SGC (18).
In SDC, several targetable molecular alterations occur in recurrent patterns. The resulting subgroups of SDC are mainly defined by HER2- and AR-expression. In a retrospective analysis of 63 SDC samples, 34 samples were AR+/HER2- and harbored frequent PIK3CA (50%) and HRAS (41%) mutations (19). In this study, HRAS-mutations were exclusively found in the HER2-/AR+ group and in 93% of cases they co-occurred with a PIK3CA-mutation (19). Additionally, no HRAS mutations were identified in SDC ex pleomorphic adenoma (19). The co-occurrence of three potentially predictive biomarkers complicates selection for targeted treatment decisions in these rare patients. We here present a case series of patients presenting to an institutional molecular tumor board or identified through a systematic search of the literature to assess outcome of AR+, HRAS/PIK3CA SDC patients with targeted treatment.
2 Materials and methods
2.1 Patients
Patients with salivary gland cancer presenting to the molecular tumor board (MTB) of the Charité Comprehensive Cancer Center between 2016 and 2022 were analyzed in a retrospective analysis of the MTB database (20). Original histopathological reports for patients classified as adenocarcinoma NOS, carcinoma NOS, invasive ductal carcinoma or carcinoma ex pleomorphic adenoma were considered. Patients with a final histopathological diagnosis of salivary duct carcinoma and molecular results with AR positivity (any immunohistochemistry, IHC staining) and activating HRAS and PIK3CA-mutations were included in the analysis (Supplementary Figure 1). Next-generation sequencing (NGS) was performed on formalin-fixed, paraffine-embedded tumor tissue for all identified patients, using the SureSelect Custom Library Panel (MH IVD Panel 600+, Agilent Technologies, USA). Library preparation was done using the SureSelectXT Low Input Target Enrichment System (Agilent Technologies, USA). Sequencing was performed on the NextSeq550 system using the NextSeq 500/550 Mid Output Kit v2.5, 300 Cycles (Illumina, USA). Follow-up, including response assessment, progression-free survival (PFS) and overall survival (OS), was performed prospectively within the MTB registrational study or as retrospective chart review. Median follow-up was calculated from the time of diagnosis. No minimum follow-up was required. The analysis was approved by the local ethics committee (Berlin, EA1/305/21).
2.2 Literature search
Systematic literature search (performed by DTR, last updated on 7th November 2022) was performed on MEDLINE using the following terms: “PIK3CA AND HRAS AND SALIVARY” OR “AR AND SALIVARY DUCT CARCINOMA”. Studies and case reports providing individual clinical follow-up data for patients with AR+, HRAS/PIK3CA co-mutated cases were included in the analysis.
2.3 Analysis
Clinical patient characteristics, line and type of treatment, best response, time on treatment, progression-free survival and overall survival were collected, as provided. Best response was assessed by the investigator after a review of CT or MRI radiology reports (complete response, CR; partial response PR; stable disease SD; mixed response, MR; progressive disease, PD). Clinical benefit was defined as CR/PR or SD lasting for at least 6 months. Outcomes with similar treatment strategies (e.g. chemotherapy, androgen deprivation therapy, HER2-directed therapy, HRAS-directed therapy, combination therapy or immune checkpoint inhibition) were summarized. No formal statistical analysis was performed because of insufficient sample size. Cases were consecutively numbered starting with cases retrieved from the internal MTB database and followed by cases identified from the literature.
3 Results
3.1 Patient cohort
Seventeen patients with salivary gland histologies, consistent with SDC, were discussed in the institutional molecular tumor board between 2016 and 2022. After review of final histopathological diagnoses, 4 patients had salivary duct carcinoma with AR expression and HRAS/PIK3CA mutation and were included in the analysis. These patients (3 male, 1 female) were between 48-79 years old at the time of presentation at the MTB. Activating HRAS mutations were identified in the p.Q61 (3 patients) and p.G13 (1 patient) positions. Activating PIK3CA mutations were identified in the p.H1047 (3 patients) and p.E545 (1 patients) positions. Additional molecular findings were low to medium HER2-expression in 3 patients, PD-L1 expression in 2 patients, a tumor mutational burden (TMB) > 10 mutations/Megabase (mut/Mb) and an AR mutation in 1 patient, each. Median follow-up was 14.5 months. Clinical and molecular findings were summarized in Table 2.
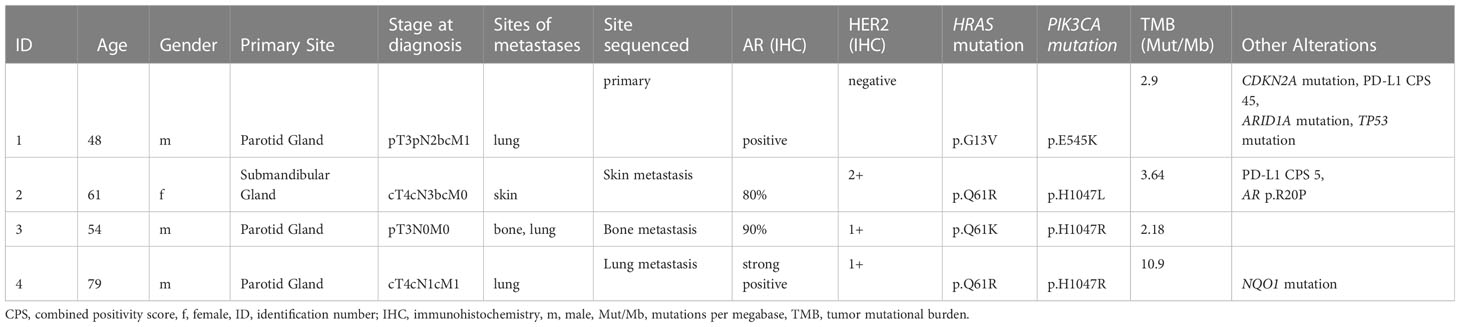
Table 2 Clinical and molecular data for patients identified from the local MTB database.
The medline searches revealed 37 and 89 results, respectively. Of these, 4 studies with individual follow-up data for patients with AR+, PIK3CA/HRAS co-mutated SDC were included after manual review of the identified publications. The publications yielded a total of 9 cases (7 male, 2 female). Age was reported for 5 patients (range 38-65 years). Concurrent molecular alterations were HER2 amplification and overexpression in 1 and TP53 mutations in 2 patients, respectively. Clinical and molecular findings in these patients were summarized in Table 3. A consort diagram of patient identification is provided in Supplementary Figure 1.

Table 3 Clinical and molecular data for patients identified from literature review.Two PIK3CA mutations were identified in patient 12.
Overall, 13 patients (10 male, 3 female; median age in 9 evaluable patients 61 years, range 38-79 years) with AR+, PIK3CA/HRAS co-mutated SDC were identified.
3.2 Treatment
Combined analysis of 13 evaluable patients yielded information on various targeted systemic treatment strategies. Androgen deprivation therapy (ADT) was reported in 7 patients, HRAS-directed treatment in 6 patients, immune checkpoint inhibition in 1 patient and combinations of tipifarnib and ADT and alpelisib and ADT in 1 patient, each. Treatment data, including line of treatment, best response and progression-free survival (PFS) are provided, as available, in Table 4 and Figure 1.
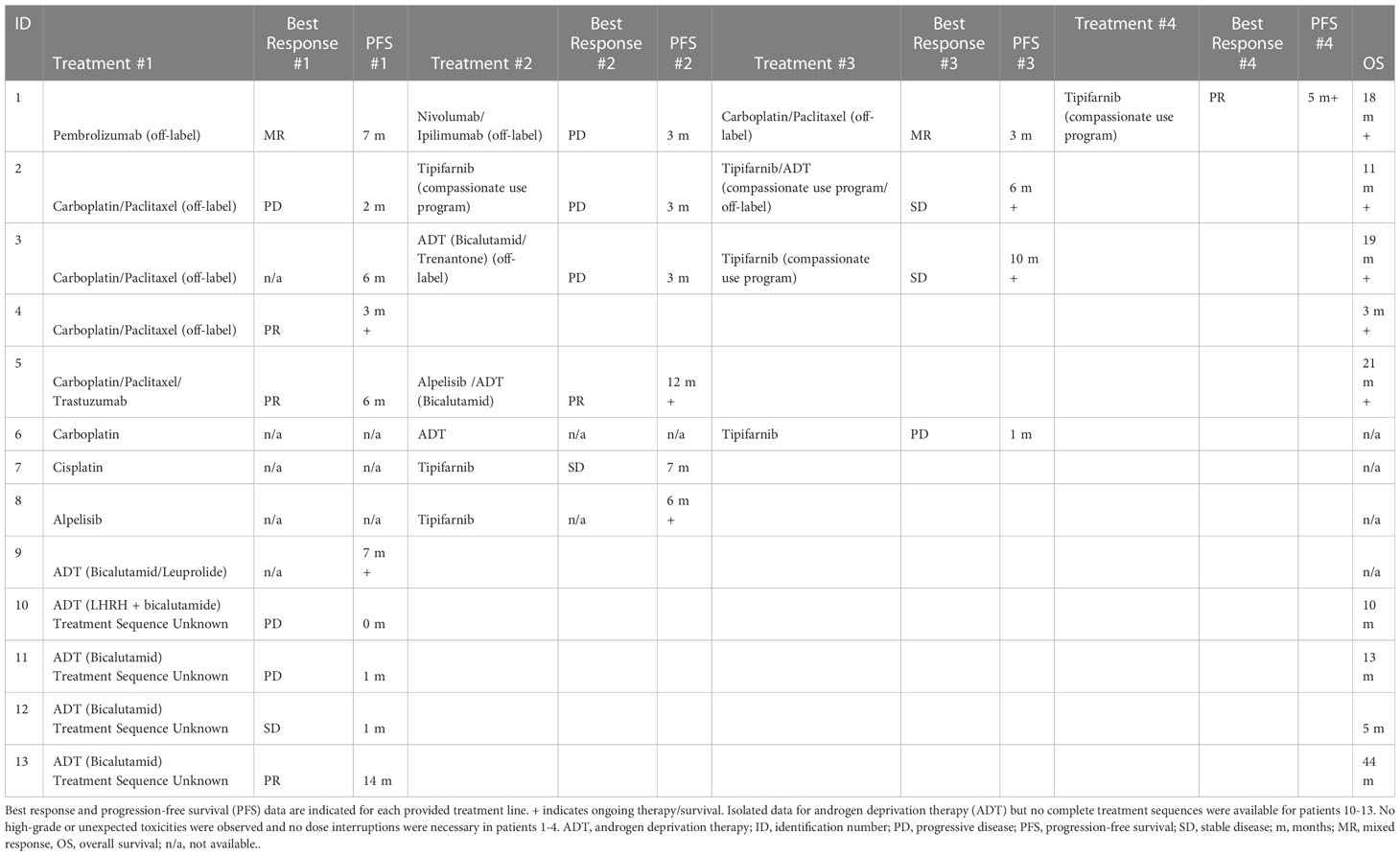
Table 4 Treatment and outcome data for the entire case series.
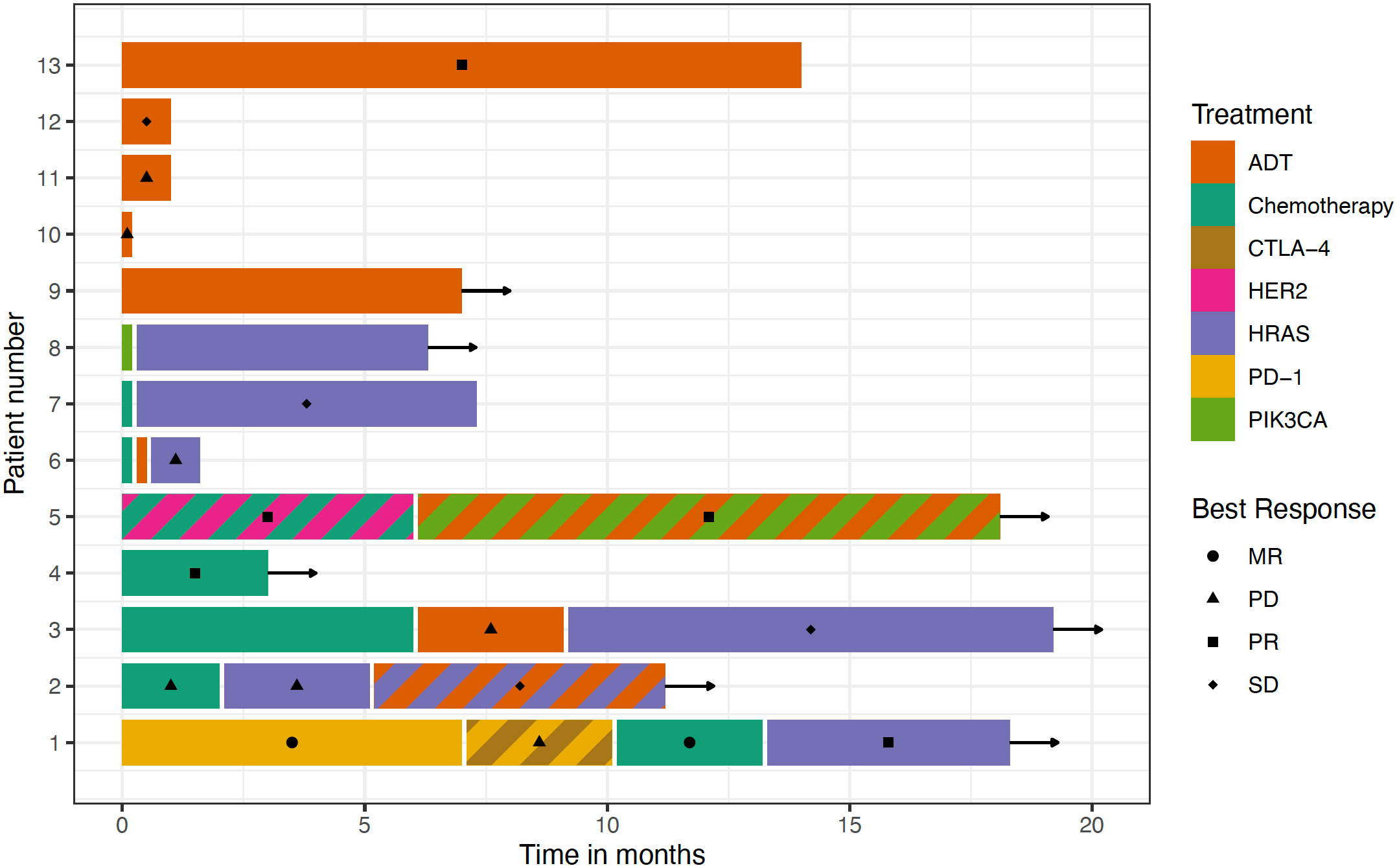
Figure 1 treatment sequences are depicted for the entire case series. No complete treatment sequences were available for patients 10-13. Duration of prior treatment was not provided for patients 6-8 (prior treatment indicated by colored bars). Color indicates the type of treatment; striped colors indicate combination therapy. Best responses are indicated. Arrows indicate ongoing therapy.
3.3 Androgen deprivation therapy
Seven patients were treated with androgen deprivation therapy alone (ADT). Among 6 patients with available data on the specific type of ADT, 3 received bicalutamide and a GnRH-analogue and 3 received bicalutamide alone. Best response was evaluable in 5 patients (1 PR, 1 SD, 3 PD). 6 patients had evaluable PFS (median PFS = 2 months) and 2 of them had PFS > 6 months.
3.4 HRAS-directed therapy
The farnesyltransferase inhibitor tipifarnib as a single agent was administered in 6 patients. Among 5 patients with available data, 1 PR, 2 SD and 2 PD were achieved as best responses. PFS data were available for 6 patients and PFS was more than 6 months in 3 patients.
3.5 Combination therapy
One patient received ADT (bicalutamid/GnRH-Analogue) in combination with tipifarnib after prior progression to tipifarnib after 3 months. This patient achieved stable disease for more than 6 months, which was ongoing at the time of data collection. Another patient achieved a partial response with the PI3K-inhibitor alpelisib in combination with ADT (bicalutamide) for more than 12 months (ongoing at time of publication).
3.6 Other treatment
Chemotherapy use with carboplatin/paclitaxel alone was reported in 4 patients. Among 3 patients with available data, 1 PR, 1 MR and 1 PD were reported. The use of alpelisib as monotherapy was only reported for one patient without information on treatment response. Immune checkpoint inhibition was also reported for one patient with a mixed response for 7 months. Following progression on the single-agent PD-1 inhibitor, this patient was treated with a combination of a PD-1 and a CTLA-4 inhibitor, which was followed by disease progression. One patient with concurrent HER2 amplification received trastuzumab in combination with chemotherapy and achieved a partial response.
3.7 Toxicity
No major (common terminology criteria of adverse events, CTCAE grade 4 or higher) or unexpected toxicities were observed in the 4 patients identified from the MTB database and no dose reductions were required. In published data, a dose reduction because of toxicity was required in six patients (46%) receiving tipifarnib (4 because of cytopenia, 2 because of reversible renal failures), hypoglycemia requiring dose reduction was reported for alpelisib (9, 21). Toxicity data were not reported in the literature for patients receiving antiandrogen therapy in this cohort (22, 23). Available data from combined ADT in SGC reported no CTCAE grade 4/5 events and discontinuation of part of the combined ADT due to adverse events in 2 out of 36 patients (10).
4 Discussion
This is, to the best of our knowledge, the largest clinical case series of AR+, PIK3CA/HRAS co-mutated salivary duct carcinoma. The co-occurrence of these alterations has been described in previous analyses of this disease but was not associated with prognosis (19). The co-occurrence of these alterations poses a challenge for personalized therapy strategies. It is currently unclear, if response to targeted therapy is different in this subgroup. Despite the low number of patients, the heterogeneity of administered treatments in the cohort and the lack of data on mechanisms of secondary resistances, these results still hold important information because of the rarity of this disease. It should be noted that at least 2/13 patients in the cohort did not receive upfront palliative systemic therapy with ADT or chemotherapy (15, 16). This is likely caused by the lack of guidelines at the time of treatment initiation and a lack of data for the specific situation in AR+, HRAS/PIK3CA co-mutated tumors. Yet, despite available data and guidelines, current treatment strategies are not satisfactory and there is a lack of prospective clinical trials. The administration of experimental therapies, including immune checkpoint inhibition, will therefore likely remain a reality in these tumors, thus making sharing of real-world data essential.
HER2 overexpression or amplification is a well-defined therapeutic target in SDC (11). HER2 positivity has been found to be mutually exclusive with the AR+, HRAS/PIK3CA co-mutated subgroup (19). In this cohort, concurrent HER2 expression or amplification was reported in 6 patients with mostly low to moderate staining intensity. One patient was reported to harbor a concurrent HER2 amplification and received trastuzumab in combination with chemotherapy, achieving a partial response. These results suggest, that HER2-positivity is not entirely mutually exclusive with the here described subgroup and HER2-directed treatment might be an additional option in some of the patients. In addition to HER2-directed antibodies, efficacy of HER2-directed antibody drug conjugates was shown in salivary gland cancer (24).
In the group of patients treated with ADT, a clinical benefit was observed in about a third of the evaluable patients, which is less than the clinical benefit rate of about 75% in previously reported results (10). However, clinical benefit was found in some patients, thus providing evidence of activity and the low number of patients does not allow further conclusions. Furthermore, previous work did not show an impact of oncogenic drivers, including HRAS and PIK3CA mutations, on the efficacy of ADT but studies on larger cohorts are warranted (10). Therefore, these data do not provide evidence against the use of ADT in the AR+, HRAS/PIK3CA co-mutated subgroup. Importantly, no data currently exist for the use of abiraterone in castration-resistant AR+, HRAS/PIK3CA co-mutated SDC. Abiraterone is active as a second line ADT in AR+ salivary gland cancer and might represent an additional treatment strategy for the here reported subgroup (13). Additional data on limited activity with enzalutamide were reported previously (14). In this phase 2 trial, tumor regressions were also noted among patients with prior ADT (14).
In patients receiving HRAS-directed therapy, 1 objective response and clinically meaningful disease stabilizations in about half of the patients was reported. These results are similar to previously reported results in SGC (9). In the same trial, co-occuring PIK3CA-alterations or the type of HRAS mutation (more common Q61 or less common G13) did also not seem to impact treatment efficacy (9). Again, these data further support the investigation of tipifarnib in the here reported disease subgroup.
Two patients received combination therapy after prior progression of disease. One patient achieved disease stabilization with tipifarnib and ADT after prior progression with tipifarnib monotherapy. In this patient, tipifarnib treatment was continued because of low toxicity and improvement in local symptoms. However, disease stabilization might be mediated by ADT alone. Another patient achieved a partial response with the PI3K-inhibitor alpelisib and ADT. The impact of the individual drugs in this combination therapy can also not be assessed. Further investigation of combination therapies is warranted.
A single agent PI3K-inhibitor was only used in 1 patient and no response data were available. The published results from the NCI-MATCH subprotocol Z1F of Copanlisib in PIK3CA-mutated cancer did show activity of the drug in several cancer types, but no SDC were enrolled (25). Additional research is needed to establish the activity of single-agent PI3K-inhibitors in SDC.
The activity of immune checkpoint inhibition also remains to be determined. One patient in the reported cohort achieved a mixed response with single-agent PD-1 blockade for 7 months, followed by disease progression. The same patient then experienced disease progression with combined PD-1 and CTLA-4 inhibition. Immune checkpoint inhibition was administered in this patient because of high PD-L1 expression and the co-occurrence of driver alterations, potentially complicating single-agent targeted treatment. These results suggest, that immune checkpoint inhibitors might be an additional treatment option in some patients. An analysis of 109 patients with advanced SGC in the Keynote-158 study showed an overall response rate of 4.6% in the overall population and 10.7% (n=3/28) in the PD-L1 positive population (26). Only 3 patients in this trial were found to be TMB-high, among which 1 had an objective reponse (26). PD-L1 expression or a high TMB > 10 mut/Mb was reported in 2 patients in the here reported cohort, accordingly.
For untargeted therapies, best data currently exist for carboplatin/paclitaxel use, which is also supported by previous analyses and yields clinically meaningful benefit (27).
In summary, the here provided data show multiple targeted treatment strategies for patients with AR+, HRAS/PIK3CA co-mutated SDC. Best available evidence, expected toxicities and patient factors need to be considered for a choice of treatment in this rare subgroup. These results support comprehensive molecular profiling of SDC. Additional molecular analyses might help with further establishing active signaling pathways for treatment stratification. Further research is required to establish optimal treatment combinations and sequences, which is a challenge in this rare disease.
Data availability statement
The original contributions presented in the study are included in the article/Supplementary Material. Further inquiries can be directed to the corresponding author.
Ethics statement
The studies involving human participants were reviewed and approved by Charité - Universitätsmedizin Berlin. Written informed consent for participation was not required for this study in accordance with the national legislation and the institutional requirements.
Author contributions
DR, SS, PS and KK provided patient data, DR performed a systematic review of the literature, DR, EZ, BE, DB, EB, UK (8th Author), UK (9th Author) and KK analyzed data. DR, UK (9th Author) and KK wrote the manuscript. All authors contributed to the article and approved the submitted version.
Funding
DR is a participant in the Berlin Institute of Health – Charité Clinical Scientist Program funded by the Charité – Universitätsmedizin Berlin and the Berlin Institute of Health. We acknowledge financial support from the Open Access Publication Fund of Charité – Universitätsmedizin Berlin and the German Research Foundation (DFG).
Conflict of interest
DR has received consultant and/or advisory board and/or speaker fees from Roche, Bayer, Bristol-Myers Squibb and Lilly. PS has received honoraria personal from BMS, MSD, Incyte, SOBI, AOP, Novartis, Alexion, AstraZeneca, BPM, and ROCHE and travel support from BMS, SOBI, AOP, and Novartis. UK 8th Author reports a consulting role for Roche, Janssen-Cilag, Takeda, BMS, Gilead, Hexal, Pfizer, Astra-Zeneca, Pentixapharm and honoraria from Gilead, Amgen, Novartis, BMS, Roche, Takeda, MSD, as well as research funding from Celgene, Takeda, BMS, Roche, Astra-Zeneca, Novartis, MSD, Janssen-Cilag, Pfizer. Other support was declared from Roche, BMS, Gilead, Takeda, Janssen-Cilag and Celgene. UK 9th Author has received advisory board/speaker bureau, trial support, research collaboration or research support from Amgen, AstraZeneca, BMS, Boehringer Ingelheim, Glycotope, Innate, Lilly, Medimmune, MerckSerono, MSD/Merck, Novartis, Pfizer, Roche/Genentech and Sirtex. KK: Advisory Boards, travel grants and speaker’s fees: MSD, BMS, Merck, Novartis, Bayer.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fonc.2023.1107134/full#supplementary-material
Supplementary Figure 1 | Consort diagram showing the identification of patients for the final cohort. MTB, molecular tumor board; HNC, head and neck cancer; SGC, salivary gland cancer; SDC, salivary duct carcinoma.
References
1. Helen Lin H, Limesand KH, Ann DK. Current state of knowledge on salivary gland cancers. Crit Rev Oncog (2018) 23:139–51. doi: 10.1615/CRITREVONCOG.2018027598
2. Skálová A, Hyrcza MD, Leivo I. Update from the 5th edition of the world health organization classification of head and neck tumors: salivary glands. Head Neck Pathol (2022) 16:40–53. doi: 10.1007/S12105-022-01420-1
3. Kleinsasser O, Klein HJ, Hübner G. [Salivary duct carcinoma. a group of salivary gland tumors analogous to mammary duct carcinoma]. Arch Klin Exp Ohren Nasen Kehlkopfheilkd (1968) 192:100–5. doi: 10.1007/BF00301495
4. Schmitt NC, Kang H, Sharma A. Salivary duct carcinoma: an aggressive salivary gland malignancy with opportunities for targeted therapy. Oral Oncol (2017) 74:40–8. doi: 10.1016/J.ORALONCOLOGY.2017.09.008
5. Jayaprakash V, Merzianu M, Warren GW, Arshad H, Hicks WL, Rigual NR, et al. Survival rates and prognostic factors for infiltrating salivary duct carcinoma: analysis of 228 cases from the surveillance, epidemiology, and end results database. Head Neck (2014) 36:694–701. doi: 10.1002/HED.23350
6. Mifsud M, Sharma S, Leon M, Padhya T, Otto K, Caudell J. Salivary duct carcinoma of the parotid: outcomes with a contemporary multidisciplinary treatment approach. Otolaryngol Head Neck Surg (2016) 154:1041–6. doi: 10.1177/0194599816636812
7. Ross JS, Gay LM, Wang K, Vergilio JA, Suh J, Ramkissoon S, et al. Comprehensive genomic profiles of metastatic and relapsed salivary gland carcinomas are associated with tumor type and reveal new routes to targeted therapies. Ann Oncol (2017) 28:2539–46. doi: 10.1093/ANNONC/MDX399
8. Dalin MG, Desrichard A, Katabi N, Makarov V, Walsh LA, Lee KW, et al. Comprehensive molecular characterization of salivary duct carcinoma reveals actionable targets and similarity to apocrine breast cancer. Clin Cancer Res (2016) 22:4623–33. doi: 10.1158/1078-0432.CCR-16-0637
9. Hanna GJ, Guenette JP, Chau NG, Sayehli CM, Wilhelm C, Metcalf R, et al. Tipifarnib in recurrent, metastatic HRAS-mutant salivary gland cancer. Cancer (2020) 126:3972–81. doi: 10.1002/CNCR.33036
10. Fushimi C, Tada Y, Takahashi H, Nagao T, Ojiri H, Masubuchi T, et al. A prospective phase II study of combined androgen blockade in patients with androgen receptor-positive metastatic or locally advanced unresectable salivary gland carcinoma. Ann Oncol (2018) 29:979–84. doi: 10.1093/ANNONC/MDX771
11. Takahashi H, Tada Y, Saotome T, Akazawa K, Ojiri H, Fushimi C, et al. Phase II trial of trastuzumab and docetaxel in patients with human epidermal growth factor receptor 2-positive salivary duct carcinoma. J Clin Oncol (2019) 37:125–34. doi: 10.1200/JCO.18.00545
12. Kurzrock R, Bowles DW, Kang H, Meric-Bernstam F, Hainsworth J, Spigel DR, et al. Targeted therapy for advanced salivary gland carcinoma based on molecular profiling: results from MyPathway, a phase IIa multiple basket study. Ann Oncol (2020) 31:412–21. doi: 10.1016/J.ANNONC.2019.11.018
13. Locati LD, Cavalieri S, Bergamini C, Resteghini C, Colombo E, Calareso G, et al. Abiraterone acetate in patients with castration-resistant, androgen receptor-expressing salivary gland cancer: a phase II trial. J Clin Oncol (2021) 39:4061–8. doi: 10.1200/JCO.21.00468
14. Ho AL, Foster NR, Zoroufy AJ, Campbell JD, Worden F, Price K, et al. Phase II study of enzalutamide for patients with androgen receptor-positive salivary gland cancers (Alliance A091404). J Clin Oncol (2022) 40:4240–9. doi: 10.1200/JCO.22.00229
15. van Herpen C, Vander Poorten V, Skalova A, Terhaard C, Maroldi R, van Engen A, et al. Salivary gland cancer: ESMO-European reference network on rare adult solid cancers (EURACAN) clinical practice guideline for diagnosis, treatment and follow-up. ESMO Open (2022) 7:100602. doi: 10.1016/J.ESMOOP.2022.100602/ATTACHMENT/06B11B84-E961-43A3-BB8F-BD5E325E30EE/MMC1.PDF
16. Geiger JL, Ismaila N, Beadle B, Caudell JJ, Chau N, Deschler D, et al. Management of salivary gland malignancy: ASCO guideline. J Clin Oncol (2021) 39(17):1909–41. doi: 10.1200/JCO.21.00449
17. Mateo J, Chakravarty D, Dienstmann R, Jezdic S, Gonzalez-Perez A, Lopez-Bigas N, et al. A framework to rank genomic alterations as targets for cancer precision medicine: the ESMO scale for clinical actionability of molecular targets (ESCAT). Ann Oncol (2018) 29:1895–902. doi: 10.1093/ANNONC/MDY263
18. Marcus L, Fashoyin-Aje LA, Donoghue M, Yuan M, Rodriguez L, Gallagher PS, et al. FDA Approval summary: pembrolizumab for the treatment of tumor mutational burden-high solid tumors. Clin Cancer Res (2021) 27:4685–9. doi: 10.1158/1078-0432.CCR-21-0327
19. Mueller SA, Gauthier MEA, Blackburn J, Grady JP, Kraitsek S, Hajdu E, et al. Molecular patterns in salivary duct carcinoma identify prognostic subgroups. Mod Pathol (2020) 33:1896–909. doi: 10.1038/S41379-020-0576-2
20. Lamping M, Benary M, Leyvraz S, Messerschmidt C, Blanc E, Kessler T, et al. Support of a molecular tumour board by an evidence-based decision management system for precision oncology. Eur J Cancer (2020) 127:41–51. doi: 10.1016/j.ejca.2019.12.017
21. Sheth H, Kumar P, Shreenivas A, Sambath J, Pragya R, Madre C, et al. Excellent response with alpelisib and bicalutamide for advanced salivary duct carcinoma with PIK3CA mutation and high androgen receptor expression-a case report. JCO Precis Oncol (2021) 5:744–50. doi: 10.1200/PO.20.00436
22. You Y, Wang P, Wan X, Xu L, Gong Y, Zhang W. Androgen deprivation therapy for patients with androgen-Receptor-Positive metastatic salivary duct carcinoma: a case report and review of the literature. Onco Targets Ther (2021) 14:3481–6. doi: 10.2147/OTT.S304900
23. van Boxtel W, Verhaegh GW, van Engen-van Grunsven IA, van Strijp D, Kroeze LI, Ligtenberg MJ, et al. Prediction of clinical benefit from androgen deprivation therapy in salivary duct carcinoma patients. Int J Cancer (2020) 146:3196–206. doi: 10.1002/IJC.32795
24. Li BT, Shen R, Offin M, Buonocore DJ, Myers ML, Venkatesh A, et al. Ado-trastuzumab emtansine in patients with HER2 amplified salivary gland cancers (SGCs): results from a phase II basket trial. J Clin Oncol (2019) 37:6001–1. doi: 10.1200/JCO.2019.37.15_SUPPL.6001
25. Damodaran S, Zhao F, Deming DA, Mitchell EP, Wright JJ, Gray RJ, et al. Phase II study of copanlisib in patients with tumors with PIK3CA mutations: results from the NCI-MATCH ECOG-ACRIN trial (EAY131) subprotocol Z1F. J Clin Oncol (2022) 40:1552–61. doi: 10.1200/JCO.21.01648
26. Even C, Delord JP, Price KA, Nakagawa K, Oh DY, Burge M, et al. Evaluation of pembrolizumab monotherapy in patients with previously treated advanced salivary gland carcinoma in the phase 2 KEYNOTE-158 study. Eur J Cancer (2022) 171:259–68. doi: 10.1016/J.EJCA.2022.05.007
Keywords: salivary gland cancer, salivary duct carcinoma, targeted therapy, precision oncology, molecular tumor board, head and neck cancer
Citation: Rieke DT, Schröder S, Schafhausen P, Blanc E, Zuljan E, von der Emde B, Beule D, Keller U, Keilholz U and Klinghammer K (2023) Targeted treatment in a case series of AR+, HRAS/PIK3CA co-mutated salivary duct carcinoma. Front. Oncol. 13:1107134. doi: 10.3389/fonc.2023.1107134
Received: 24 November 2022; Accepted: 26 May 2023;
Published: 20 June 2023.
Edited by:
Stefano Cavalieri, National Cancer Institute Foundation (IRCCS), ItalyReviewed by:
Elena Colombo, Fondazione Istituto Nazionale dei Tumori, ItalyLuigi Lorini, Humanitas Research Hospital, Italy
Copyright © 2023 Rieke, Schröder, Schafhausen, Blanc, Zuljan, von der Emde, Beule, Keller, Keilholz and Klinghammer. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Damian T. Rieke, ZGFtaWFuLnJpZWtlQGNoYXJpdGUuZGU=