 Adriana de Souza Sérgio Ferreira1,2
Adriana de Souza Sérgio Ferreira1,2 Jane Rocha Duarte Cintra1*
Jane Rocha Duarte Cintra1* Vívian Assis Fayer3
Vívian Assis Fayer3 Mário Círio Nogueira3
Mário Círio Nogueira3 Cassimiro Baesso Júnior4
Cassimiro Baesso Júnior4 Maria Teresa Bustamante-Teixeira2,3Alfredo Chaoubah2,3
Maria Teresa Bustamante-Teixeira2,3Alfredo Chaoubah2,3 Arthur Duarte Cintra1,5
Arthur Duarte Cintra1,5 Caroline Montes Simão1,5
Caroline Montes Simão1,5 Maximiliano Ribeiro Guerra3
Maximiliano Ribeiro Guerra3- 1Instituto Oncológico de Juiz de Fora/Hospital 9 de Julho, Departamento de Oncologia Clínica, Juiz de Fora, Brazil
- 2Programa de Pós-Graduação em Saúde da Universidade Federal de Juiz de Fora (UFJF), Faculdade de Medicina, Juiz de Fora, Brazil
- 3Programa de Pós-Graduação em Saúde Coletiva da Universidade Federal de Juiz de Fora (UFJF), Departamento de Saúde Coletiva, Juiz de Fora, Brazil
- 4Hospital Universitário da Universidade Federal de Juiz de Fora (UFJF), Juiz de Fora, Brazil
- 5Faculdade de Ciências Médicas e da Saúde de Juiz de Fora (SUPREMA), Juiz de Fora, Brazil
Background: The incidence of breast cancer is increasing globally; however, survival outcomes vary and are lower in developing countries.
Methods: We analyzed the 5- and 10-year survival rates for breast cancer according to the type of healthcare insurance (public vs. private) in a referral center for cancer care in the Brazilian southeast region. This hospital-based cohort study included 517 women diagnosed with invasive breast cancer between 2003 and 2005. The Kaplan–Meier method was used to estimate the probability of survival, and the Cox proportional hazards regression model was used to assess prognostic factors.
Results: The 5- and 10-year breast cancer survival rates were as follows: private healthcare service survival rate of 80.6% (95% CI 75.0–85.0) and 71.5% (95% CI 65.4–77.1), respectively, and public healthcare service survival rate of 68.5% (95% CI 62.5–73.8) and 58.5% (95% CI 52.1–64.4), respectively. The main factors associated with the worst prognosis were lymph node involvement in both healthcare services and tumor size >2 cm only in public health services. The use of hormone therapy (private) and radiotherapy (public) was associated with the best survival rates.
Conclusions: The survival discrepancies found between health services can be explained mainly by the difference in the stage of the disease at the time of diagnosis, indicating inequalities in access to the early detection of breast cancer.
Background
Among the malignant neoplasms that affect women, breast cancer (BC) is associated with high morbidity and mortality worldwide (1), including in Brazil (2). Although BC incidence remains high in high-income countries, these countries have already experienced a tendency to reduce mortality, while middle- and low-income countries show an increased incidence with still high BC mortality (1). Combining population screening with advances in cancer treatment has been identified as an important factor in reducing mortality and the consequent expansion of the number of survivors in high-income countries (3), which reinforces the understanding that the existing differences in availability and access to early cancer diagnosis and treatment contribute to justifying the disparity observed between regions (3, 4).
The relative 5-year BC survival in Brazil increased from 68.7% between 2000 and 2004 to 75.2% between 2010 and 2014, according to surveillance data produced by the CONCORD-3 study. These percentages are lower than those found in North America and Oceania, which have values close to 90% (5). Meanwhile, the 5-year BC survival in Brazil, estimated through hospital-based studies in recent decades, has ranged from 75% to 87% (6–12), while the 10-year BC survival has ranged from 41% to 78.7% (7, 10, 12–14).
Survival analysis is widely used in oncology, especially in BC assessment, because it provides information on the effectiveness of diagnosis and treatment. Furthermore, when performed using population data, it can contribute to identifying specific characteristics of disease behavior and its prognostic factors (14, 15).
Prognostic factors are fundamental in supporting the adoption of adequate criteria for therapeutic approaches. Staging (6, 16, 17), tumor size, lymph node status (6, 9, 11, 13), and hormone receptor (HR) status (8, 11) are classic BC prognostic factors, for which there is sufficient scientific evidence to support their strong association with survival. Individual characteristics, such as age at diagnosis (18), race (13, 17, 19), and socioeconomic profile (20, 21), and those related to health services, such as therapeutic approaches (11), access, and type of health services (public or private) (22–25), have also been identified as prognostic factors that can influence BC survival.
Since 1988, Brazil has had a public health system, the Sistema Único de Saúde (SUS), which has recognized health as a right and works through a universal system delineated by territories and hierarchical networks at integrated care levels (26). In addition, private health services (individual or corporate plans) serve 24.5% of the Brazilian population, composed mainly of formal workers who are part of corporate health insurance plans (26, 27). In the context of BC, some evaluations indicate that there are differences between public and private health services regarding diagnosis and treatment in Brazil, suggesting that public health service users present with a more advanced stage of BC at diagnosis and, consequently, have a worse prognosis (12, 25, 28).
Considering the relevant role of health services in cancer care, this study aimed to evaluate the 5- and 10-year BC survival rates according to the type of healthcare service (public vs. private) in a reference center in the Zona da Mata Mineira, Minas Gerais State, Brazil.
Method
This hospital-based cohort study included women diagnosed with BC between January 2003 and December 2005 who underwent surgical and/or complementary treatment (chemotherapy, radiotherapy, or hormone therapy).
All women were assisted at a regional oncology referral center located in the city of Juiz de Fora, Minas Gerais, Brazil. In 2019, the municipality presented a population estimate of 568,873 inhabitants (29), which is the hub of healthcare in the southeast macro-region of Minas Gerais State, comprising 94 municipalities, and considered as a reference in the diagnosis and treatment of several medical specialties (30). The oncology reference center where the study was conducted provides care for the public health system (SUS) and the private healthcare system, which is accredited by the High Complexity Assistance Unit in Oncology (UNACON) with radiotherapy, chemotherapy, and cancer surgery services (31).
Data from the institution’s Hospital Cancer Registry were used to recruit information from patients. Data collection was carried out in a standardized form through a review of medical records by a team previously trained and advised by specialists in pathology and oncology. The retrieval of information on the follow-up of women to access vital status (defined as a determination of date of death or date last known alive) was obtained from the consultation of hospital records, the National Mortality Information System, National Registries of the Deceased (32), and the Individual Taxpayer’s Registry (33), in addition to a telephone call made by the institution’s Hospital Cancer Registry and contact with the patients’ mastologist. Among the 563 women identified, 45 patients with carcinoma in situ and one who died less than 30 days after diagnosis were excluded. We analyzed 517 women with invasive cancer, which corresponded to the study population.
The evaluated variables included three dimensions: 1) sociodemographic variables, such as age at diagnosis (<50, 50–60, ≥60 years), skin color (white and non-white), and education level (high/medium, low); 2) tumor aspects: tumor size (≤2 cm, >2 cm), lymph node involvement (present or absent), stage (initial—I, intermediate—II, advanced—III and IV), hormone receptor (positive, negative, not evaluated), and expression of biomarkers such as hormone receptors (HRs) (estrogen and/or progesterone) and human epidermal growth factor receptor-type 2 (HER2) [yes = HR± and Her2+ or HR+ and Her2−; no = HR− and Her2− (triple-negative tumor subtype)]; and 3) characteristics related to health services, such as performing tumor immunohistochemical expression according to the St. Gallen surrogate classification for breast cancer subtypes (34) (done, not done), the average time between diagnosis and first treatment (in days), type of surgery (conservative or radical), and chemotherapy/radiotherapy/hormone therapy use (no, yes). The 5- and 10-year overall BC survival rates were calculated using the time interval between the date of the histopathological report and the date of death or the end of follow-up. Women who remained alive at the end of the follow-up and follow-up losses on the date of the last contact were censored at 60 months (for a 5-year analysis) or 120 months (for a 10-year analysis). All deaths were treated as failures. To assess differences in the distribution of variables, the χ² test was used; when necessary, Fisher’s exact test was used. For the survival estimates and their comparison in relation to the studied variables, the Kaplan–Meier method and the log-rank test were used. The Cox proportional hazards regression model was used to assess prognostic factors by computing the hazard ratio (HR) and the corresponding 95% confidence interval (95% CI). The variable selection for the modeling process was based on clinical relevance and its statistical significance in the univariate analysis, considering the same variables for adjustment at 5 and 10 years in both services (public and private). The variables included in the multiple analyses were removed using the backward elimination process.
All analyses were performed using the Stata software package (version 16.0, StataCorp, TX, USA), and the research was approved by the Research Ethics Committee of the Federal University of Juiz de Fora (reference no. 2.038.397). The level of statistical significance was set at 5%. The quality of adjustment was assessed based on the likelihood ratio and overall measure of adjustment quality.
Results
Of the 517 women evaluated, 248 (48.1%) were assisted in private healthcare and 269 (51.9%) in public healthcare. Table 1 shows the distribution of women according to the study variables stratified by the type of health service assistance (private or public).
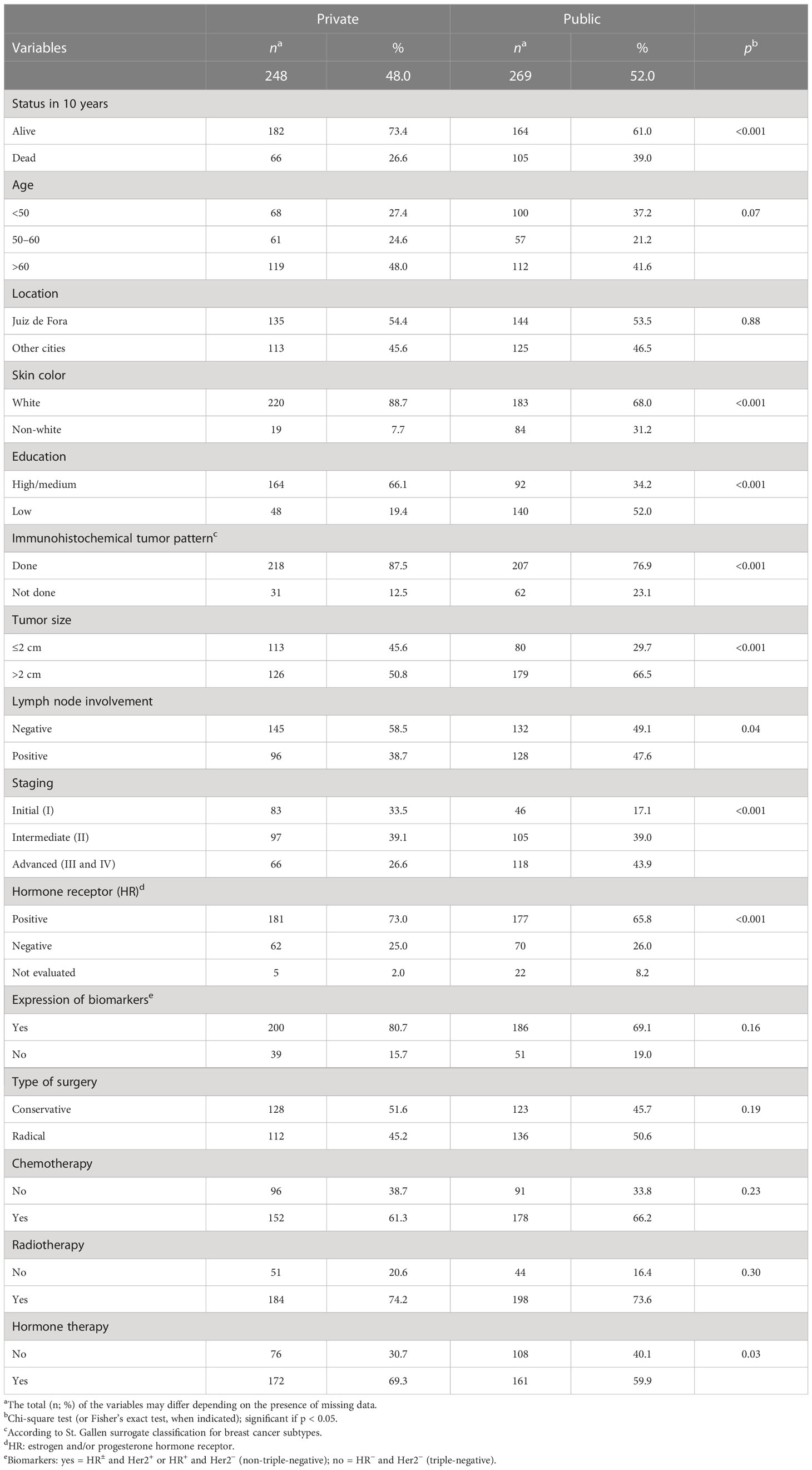
Table 1 Distribution of study variables according to the type of healthcare services for the hospital-based cohort.
The most frequent characteristics found in both services were as follows: age group over 60 years, white skin color, residence in the municipality of the regional oncology referral center (Juiz de Fora), underwent tumor immunohistochemical expression, first treatment within 15 days of diagnosis, intermediate stage (II), tumor size >2 cm, positive hormone receptors, identified biomarker expression, and had undergone chemotherapy, radiotherapy, and hormone therapy (Table 1).
Among the women assisted in public healthcare, in the 10-year follow-up, higher percentages of death (39%, p < 0.001), low schooling level (63%, p < 0.001), non-white skin color (31.5%, p < 0.001), tumor size >2 cm (69.1%, p < 0.001), lymph node involvement (49.2%, p < 0.05), and advanced stage (III and IV) (37.3%, p < 0.001) were observed, compared with those assisted by private healthcare.
Considering the characteristics related to healthcare services, having not performed immunohistochemical tumor expression (23.1%, p < 0.001) and the use of hormone therapy (40.1%, p = 0.04) were more frequent in the public healthcare service than in the private healthcare service. No significant differences were identified in relation to the type of surgery and chemotherapy or radiation therapy according to the type of health service. The average time between diagnosis and first treatment was 11.78 days (95% CI 1.76–21.80) in the private healthcare service and 18.6 days (95% CI 10.34–26.87) in the public healthcare service.
Regarding the biological aspects of the tumor, significant differences were observed between public and private health services concerning positive hormone receptors (73.1% vs. 65.8%, p = 0.005), whereas no significant difference was observed in the absence of any qualified tumor biomarkers (triple-negative tumor subtype) (21.5% vs. 16.3%, p = 0.16).
The overall 5-year BC survival rates were 80.6% (95% CI 75.0–85.0) in the private health service and 68.5% in the public health service (95% CI 62.5–73.8), respectively, while the 10-year BC survival rates were 71.5% (95% CI 65.4–77.1) and 58.5% (95% CI 52.1–64.4), respectively.
Table 2 shows the 5- and 10-year BC survival rates according to the type of healthcare for the study variables. Unadjusted survival function estimates that indicated better survival (p < 0.05), at 5 and 10 years, were observed among white women with tumors <2 cm, initial (I) and intermediate (II) stages, positive hormone receptors, and who underwent conservative surgical treatments and hormone therapy. The survival percentages of these characteristics in private health services were greater than those in public health services.
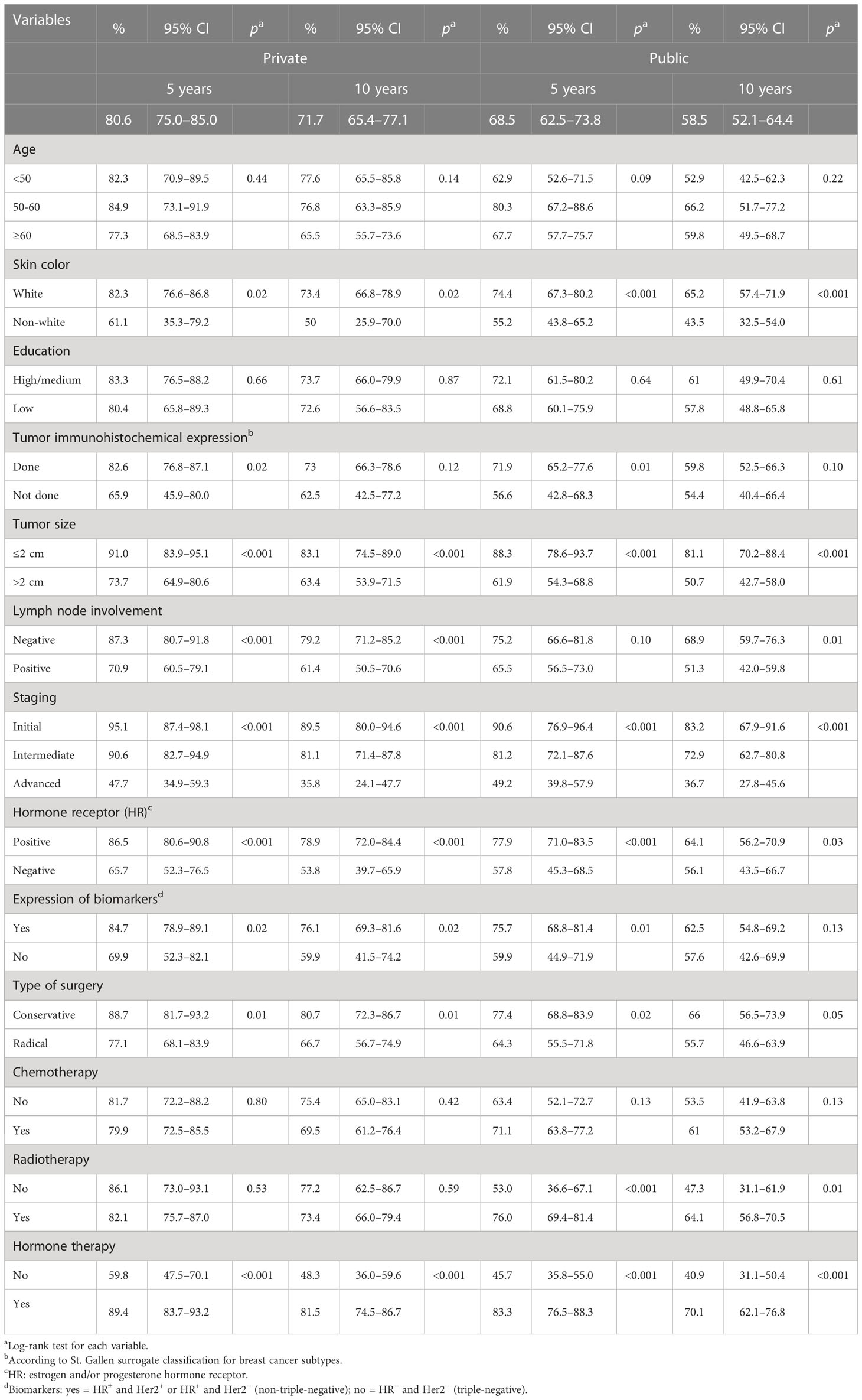
Table 2 Distribution of the 5- and 10-year breast cancer survival rates, according to the type of healthcare services and study variables, for the hospital-based cohort.
In the first 5 years of follow-up, the absence of an immunohistochemical profile was associated with lower survival among women from both health service types (Table 2). In this condition, the overall 5-year BC survival was 65.9% (95% CI 45.9–80.0, p < 0.05) in private health services and 56.6% (95% CI 42.8–68.3, p < 0.05) in public health services, in which 23.1% had not performed the immunohistochemical profile, a percentage significantly higher than that found in the private health service (12.5%, Table 1).
In the public health service, better 5- and 10-year survival rates were found among women who received radiotherapy (76% and 64%, respectively). Such a difference was not observed in women who were assisted in private health services.
In private health services, the prognostic factors independently associated with the risk of death, at 5 and 10 years, were the stage at diagnosis and the use of hormone therapy. While advanced staging (III and IV) was associated with an increased risk of death (5 years: HR = 11.4; 95% CI 3.75–34.9; 10 years: HR = 7.87; 95% CI 3.40–18.2), the use of hormone therapy had a protective effect (5 years: HR = 0.34; 95% CI 0.17–0.67; 10 years: HR = 0.38; 95% CI 0.21–0.66). In addition, non-white skin color was associated with a higher 10-year risk of death (HR = 1.14; 95% CI 1.01–4.96), with a trend toward a higher 5-year risk (HR = 2.23; 95% CI 0.88–5.67).
Having undergone radical surgery and the absence of hormone receptors and HER2 were associated with a higher risk of death only in the univariate analysis.
Regarding the public health service, an almost five-fold increased risk of death was observed at 5 and 10 years among women with advanced staging (HR = 4.66) compared with the initial staging. A significantly higher risk of death was also found among non-white women, when compared with white women, in 5 years (HR = 1.98; 95% CI 1.19–3.28) and 10 years (HR = 1.91; 95% CI 1.23–2.97). Hormone therapy and radiotherapy maintained the protective effect throughout the entire evaluation period, indicating that women treated with these treatments survived longer than those who were not treated with these therapeutic modalities (hormone therapy—5 years: HR = 0.28; 10 years: HR = 0.44; radiotherapy—5 years: HR = 0.47; 10 years: HR = 0.52). In addition, the use of chemotherapy reduced the risk of death by 50% at 10 years (HR = 0.51; 95% CI 0.29–0.89).
Table 3 shows the adjusted association measures of the Cox models for the 5- and 10-year BC survival rates according to the type of health services used. The 5- and 10-year overall BC survival curves for significant variables in the univariate analysis (log-rank test) according to the type of health service are illustrated in Figures 1, 2, respectively.
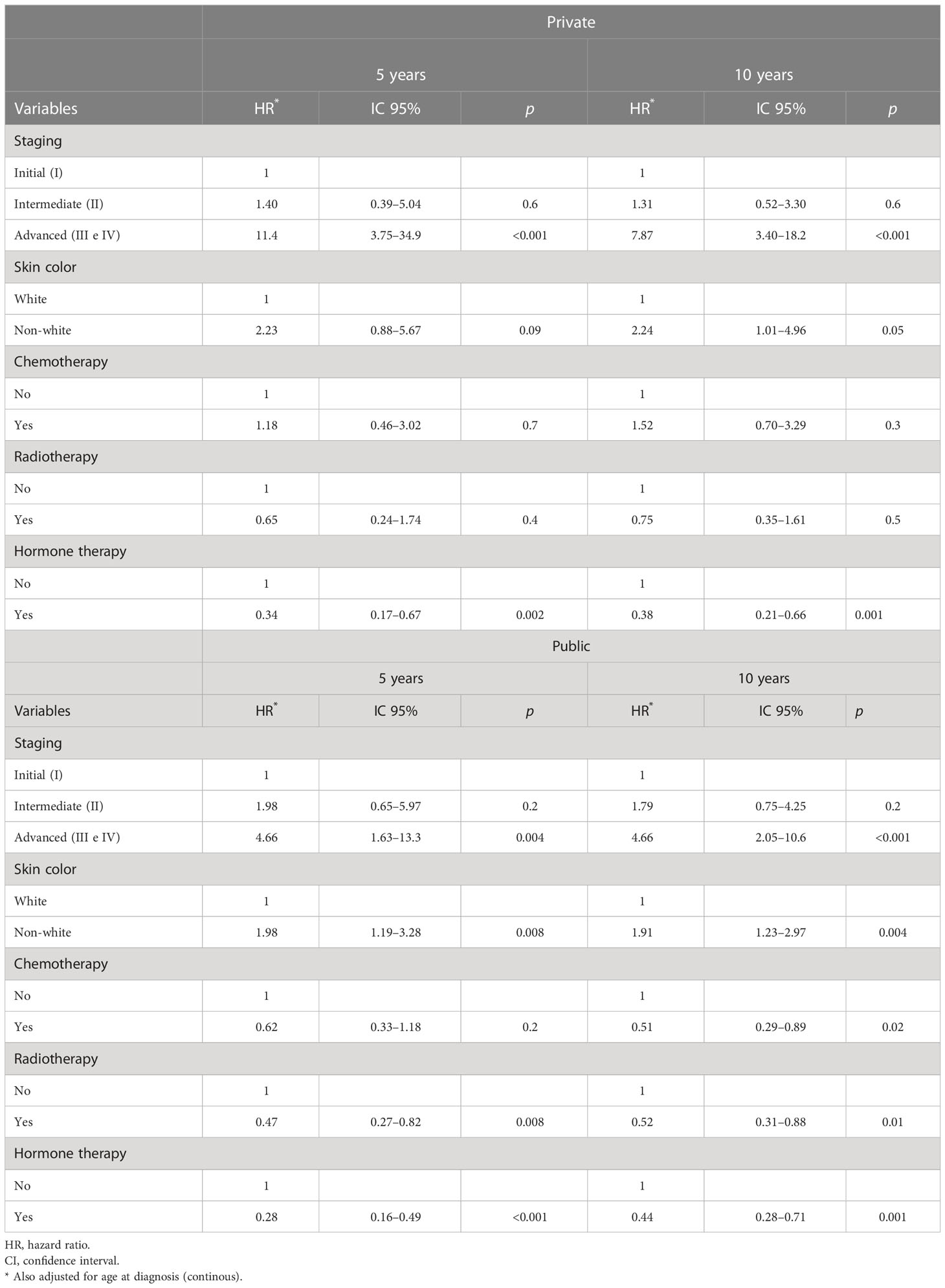
Table 3 Adjusted measures of association of the Cox models for 5 and 10-year breast cancer survival rates, according to type of health care service.
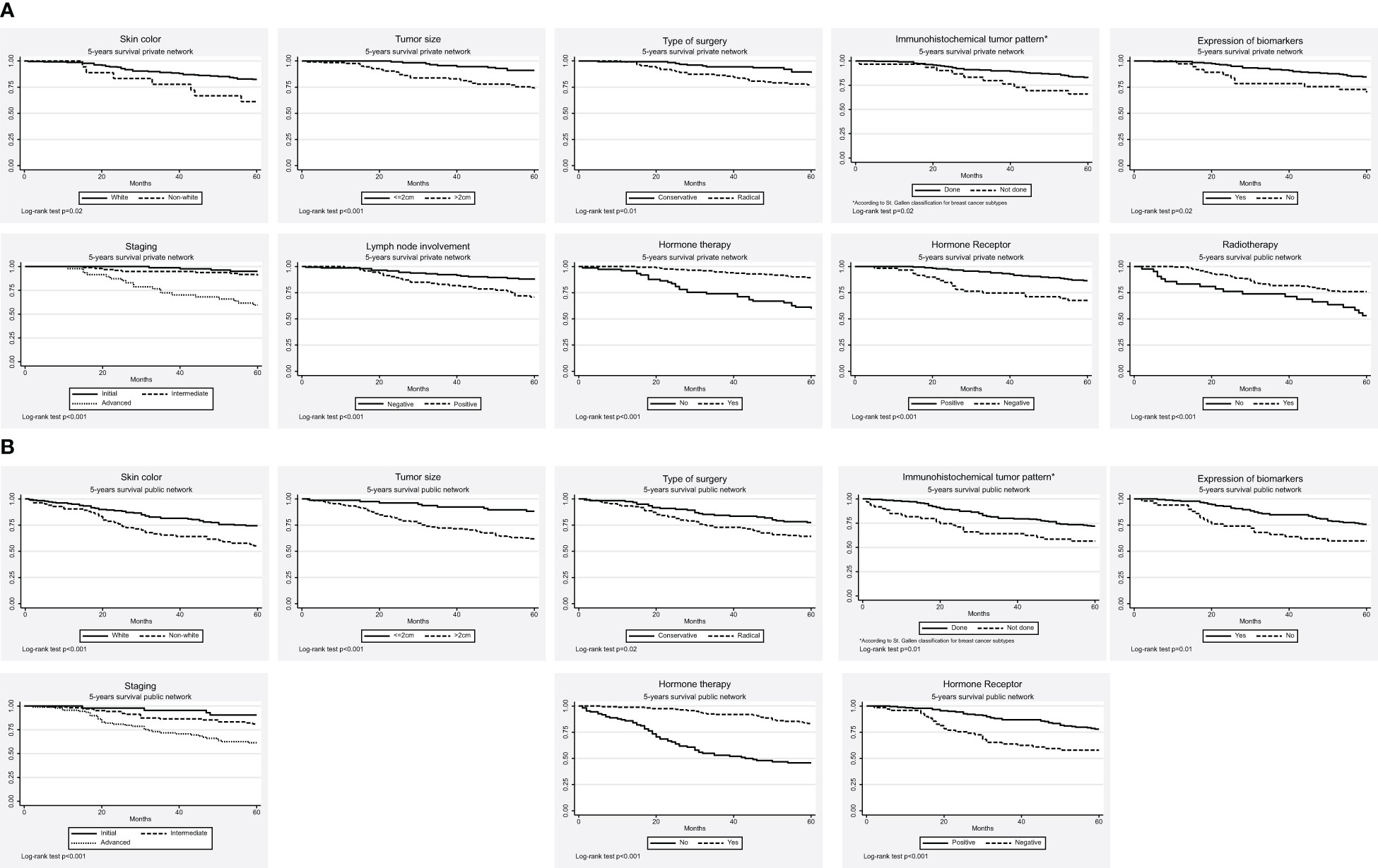
Figure 1 The 5-year breast cancer survival curves, according to the type of healthcare services. (A) Private (B) Public.
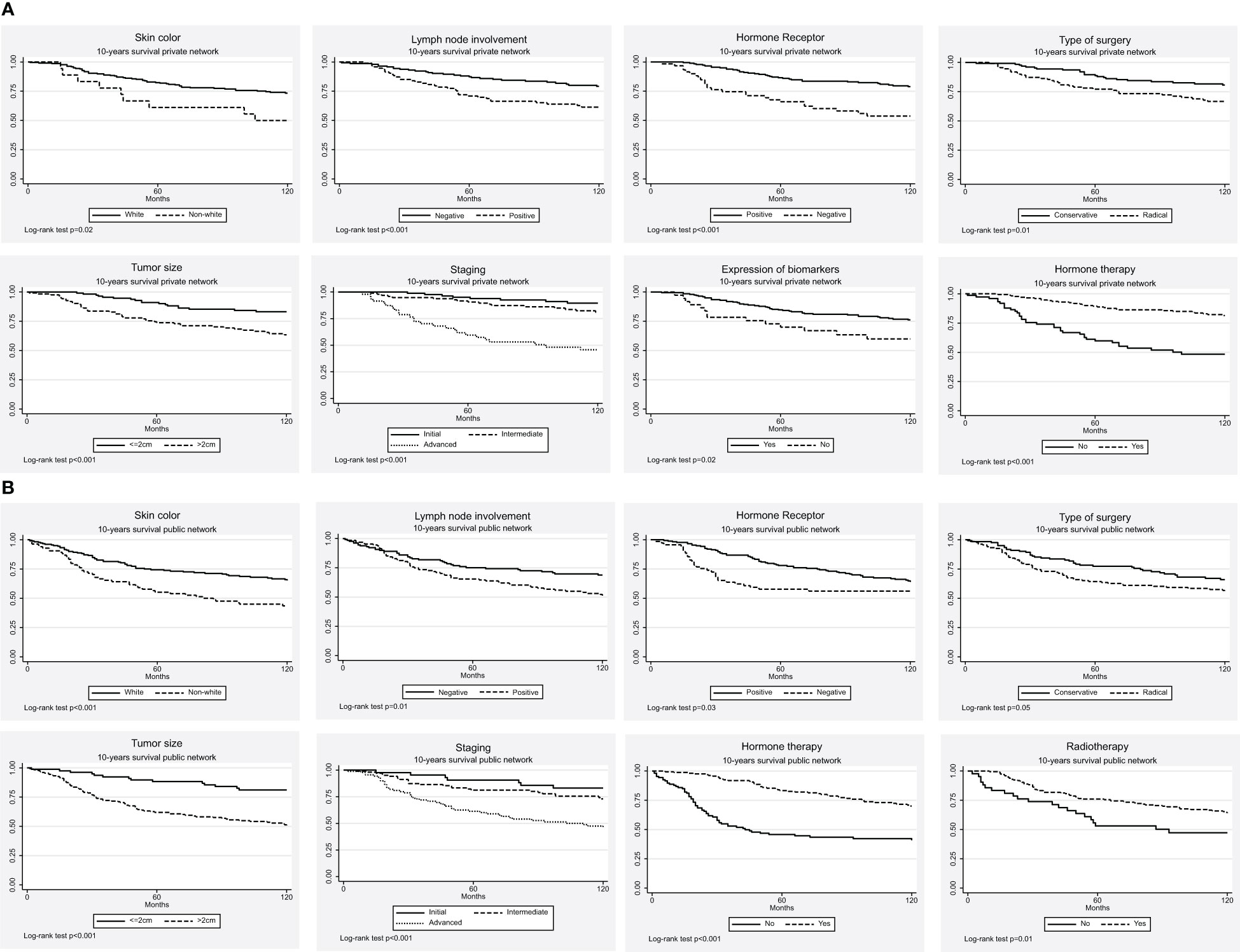
Figure 2 The 10-year breast cancer survival curves, according to the type of healthcare services. (A) Private (B) Public.
Discussion
The overall 5- and 10-year BC survival rates were higher in the private healthcare service than in the public healthcare service. The advanced stage at diagnosis was the main factor independently associated with the worst prognosis in both health services. Therapeutic approaches to hormone therapy (in both health services), radiotherapy, and chemotherapy (in the public health service) were associated with better prognosis, whereas non-white race/skin color was associated with worse prognosis in both health services.
According to the international literature, these findings reinforce the differences in access to diagnosis and treatment in more vulnerable populations, such as those found in the Concord study, which was conducted on five continents and showed marked differences in 5-year BC survival between high-income countries (USA and Australia: ~90%) and low-income countries (South Africa: ~40%) (5). Other studies carried out in North American populations also reinforce that advanced stage at diagnosis, low socioeconomic status, and non-white race are associated with lower BC survival and are important determinants for identifying health disparities in this population (35–37).
Brazilian hospital-based studies, which mostly only evaluated women who were assisted in public health services, showed a 5-year BC survival equal to or greater than 75% (6–12), while the 10-year BC survival assessments pointed out a greater range of values, ranging between 41% and 78.7% (7, 10, 12–14). The 5-year BC survival rate found in these studies was higher than that obtained in the present study for women assisted in public health services (68.5%), which was not observed in private health services. To interpret these differences in survival, the higher percentage of characteristics suggestive of better BC prognosis in women who participated in some of these studies, such as earlier stages and positive estrogen and progesterone receptors, must be taken into account (7, 11). In line with the findings of the present study, a study that evaluated health inequities in BC survival in Brazil also observed a worse survival rate in women treated at the public health service compared with those treated at private health services, which was related to advanced staging at BC diagnosis in the public health service (25).
The 10-year overall survival of BC found in the public health service (58.5%) was higher than that observed in a study carried out at the SUS reference center for BC treatment in Joinville, State of Santa Catarina, in the southern region of Brazil (41%) (14). However, it was lower than the 10-year survival found in a university teaching hospital in Belo Horizonte, Minas Gerais (64.5%) (12). Again, these findings may be due to the difference in the distribution of BC stages between regions, since advanced stages were more frequent in Santa Catarina than in Minas Gerais, which concentrated higher percentages of early stages and well-differentiated tumors, characteristics associated with the best survival (12, 14, 23).
Most of the differences found in BC survival according to the type of health service are explained mainly by the difference in the disease stage when women arrived at the health service, indicating inequalities in access to the early detection of BC (12, 23). When the National Cancer Control Policy in Brazil was instituted (38) in 2005, and with its subsequent insertion in the strategic action plan for coping with chronic non-communicable diseases (39), an expansion of access to mammography was observed for the age group of 50 to 69. Another important breakthrough observed was the approval of legal regulations in Brazil, which established a 30-day deadline for diagnostic confirmation and a 60-day deadline to begin treatment (40). In the present study, we observed a high percentage of women who started treatment within 30 days (over 80%) in both types of health services, indicating that access to treatment after BC diagnostic confirmation occurs in a timely manner in both services. However, obstacles in the structure and limited investments in the public cancer care network continue to harm access to early BC diagnosis, recommendations, and timely treatment. These are probably the greatest challenges to enabling a cancer control policy in Brazil that guarantees equity in access to information, tracking, diagnosis, and therapeutic approaches.
The presence of lymph node involvement and tumor size >2 cm are classic prognostic factors associated with a worse prognosis and, consequently, lower survival (6, 7, 9, 13, 14, 18). Lymph node involvement was associated with a higher risk of death in both types of healthcare services, while larger tumor size was associated with a higher risk of death only in the public health service. Women who received treatment in private health service exhibited BC at earlier stages when compared with those treated at the public health service, a finding that corroborates the results of other national studies (12, 23). Such findings suggest greater difficulty in accessing diagnostic confirmation methods and mammographic screening within the Brazilian public health service (41–43), as well as lower percentages of adherence to mammographic screening (43, 44).
The risk of death among non-white women who used the public health service was significantly higher in 5 and 10 years, which can be explained by the higher percentage of advanced stages among women being treated in the public health service. Interestingly, non-white skin color was also associated with the highest risk of death in 10 years among women treated in private health services, showing racial inequalities related to BC control, even in the private network. National and international studies that have investigated BC survival have used skin color as an indirect way of measuring ‘women’s socioeconomic conditions (13, 19, 25, 45–47). Such differences should consider the difficulty in accurately defining skin color due to the intense miscegenation of the Brazilian population and the fact that, in this study, we obtained this information from the individual perceptions of health service professionals. In Brazil, Cabral et al., in their evaluation of Brazilian women with more vulnerable social profiles, such as black skin color and low education, showed long intervals between diagnosis and treatment, regardless of the stage of the disease (48). Our results corroborate those obtained in a study carried out in the southern region of the Mississippi Delta in the United States, which showed high rates of advanced stages in black women in the region, regardless of tumor subtype (20). Racial disparities were also found among African-American women when compared with European-American women, indicating that race/skin color is an important prognostic factor for BC survival. Even when tumor factors are controlled, women of African descent have a higher risk of death from BC, which suggests some secondary effects related to ethnic factors. At diagnosis, these women also have more advanced and aggressive tumors, with a disproportionate chance of survival, most likely due to inadequate access to healthcare as well as socioeconomic disadvantages (35). It is important to highlight that although tumor staging is one of the mediating factors of racial disparities in BC survival identified in several studies, it does not explain all inequalities in prognosis. Other important factors already identified are differences in treatment, the prevalence of comorbidities, and in more recent studies, the interactions between genetic and environmental factors that are mediated by epigenetic modifications (35–37). Another important aspect to emphasize is that racial disparities in BC survival are detected even in models that are also adjusted for socioeconomic variables, indicating that the race/skin color variable is not only a proxy for socioeconomic status, although the latter also plays a role in racial disparities in healthcare (19, 35–37).
The recommendation for hormone therapy was relatively high in both groups (positive hormone receptor status >65% for both health services), which may explain the better survival for women who received this therapeutic modality in both types of health services. However, a higher percentage of unevaluated hormone receptors was found in the public health service than in the private health service (8.2% public vs. 2.0% private; p = 0.005), which points to disparities in access to diagnostic and therapeutic methods between health services. Hormone therapy was also associated with a better prognosis in a study carried out on Brazilian women by Mendonça et al. (6), De Moraes et al. (7), and Guerra et al. (25).
We verified worse survival for tumors with no expression of any biomarker (triple-negative tumor subtype), corroborating the worst prognosis of this specific tumor subtype and reinforcing the need for a deeper understanding of molecular characteristics to provide more effective treatments. Similar results have been reported by Gonçalves et al. (49) comparing triple-negative and non-triple-negative tumors. In the present study, the distribution of this tumor subtype was similar between both healthcare services, which strengthens the impression that from a biological point of view, the populations under comparison were similar. In the multivariate analysis, we observed that other tumor factors independently influenced survival, such as tumor size in the public health service and lymph node involvement in both health services—factors that are related to the more advanced stage of the disease. These findings were similar to those observed by Fayaz et al. (50) in a 10-year survival study of patients with triple-negative tumors, where staging and lymphovascular invasion were the most relevant prognostic factors for the lowest survival.
Regarding the local therapeutic approach, radiotherapy was associated with better BC survival in 5 and 10 years only at public health services, which is in line with the findings of a study carried out in the western Brazilian Amazon region (11). The distribution of radiotherapy offered in the oncology care network and the displacements needed to arrive at the treatment site can partially explain the difficulties related to accessing this treatment in Brazil (51). Radiotherapy requires complex equipment infrastructure, physical facilities, and highly trained human resources so that it is offered in an appropriate way to the population, conditions that, together, limit its distribution and offer in the SUS network (51). In a study conducted in New Mexico, USA, a two-fold risk of death was identified in women who did not receive radiotherapy compared with those who used the therapies indicated by the National Comprehensive Cancer Network (NCCN) guidelines (52). The use of radiotherapy after conservative surgery reduces the rate of locoregional recurrence and the risk of death from BC, according to a meta-analysis conducted in 2011 by the Early Breast Cancer Trialists’ Collaborative Group (EBCTCG), which included more than 10,000 women with pathologically negative or positive lymph nodes (53). Other studies reinforce the beneficial effect of radiotherapy after mastectomy and adjuvant chemotherapy, even among high-risk cases with lymph node involvement, large tumors, compromised surgical margins, or even in the presence of a combination of risk factors, such as age ≤50 years, triple-negative tumor, high tumor grade, and lymphovascular invasion (54, 55).
For women treated in the public health service, the protective effect of chemotherapy on long-term BC survival (10 years) was also identified. It should be noted that current chemotherapy is more effective, with a reduction in BC mortality with the use of more active regimens, especially in patients with more advanced stages of the disease, when compared with the absence (non-recommendation) of chemotherapy (56).
Although the study has limitations inherent to the use of secondary data, hospital-based cancer registries (HCRs) are recognized as important centers for collecting information on the quality of cancer care. In Brazil, accredited oncology services are required to keep HCRs active and updated, transferring information regarding the care and treatment of cancer patients to the National Cancer Institute (INCA), which uses these data to compare the quality of care provided by oncology services and promote public health policies (57). In the healthcare services where our study was conducted, the HCR has been consolidated and has been in operation since 2000. In addition, a hospital cohort allows greater access to patient follow-up, which contributes to minimizing losses of follow-up that usually occur in cohort studies; a hospital-based cohort allows the adoption of different strategies to retrieve follow-up information, contributing to minimizing the impact of these losses as well as making it possible to recover some selected socioeconomic information through telephone contact, as was carried out for all cases in this study. Although the mean follow-up time was longer in the private network than in the public network, both for the 5-year survival analysis (private: 53.6 months; 95% CI = 51.8–55.3; public: 47.8 months; 95% CI = 45.5–50.0) and 10-year survival analysis (private: 92.4 months; 95% CI = 87.7–97.1; public: 80.5 months; 95% CI = 75.2–85.8), more deaths were identified in the public network than in the private network, and loss to follow-up was not significantly different between health services. As a result of the strategies adopted to retrieve the information, we identified very few losses over 60 months (private: 4.0%; public: 7.4%) and 120 months (private: 18.3%; public: 15.2%).
Furthermore, even in the face of difficulties in evaluating therapeutic recommendations due to the scarcity of available information, the main predictive factors that could influence the use of these therapies were considered during the analysis. On the other hand, the results emphasized the importance of the information produced by health services, which makes it possible to identify the challenges faced, particularly in the public health service responsible for the cancer care of the majority of the Brazilian population (42), as well as makes it possible to produce relevant content to support BC control practices and improve service quality.
Conclusions
There was a greater BC survival rate in the private healthcare service at 5 and 10 years compared with the public health service, with a worse prognosis related to the advanced stages of the disease and non-white skin color. Hormone treatment contributed to the reduction of the risk of death in both services, pointing to the sustained protective effect in the private network over 10 years, most likely as a result of better guidance of the recommended treatment.
The results of this study strongly emphasize the influence of social inequality on the prognosis of breast cancer in Brazil, highlighting the need, mainly on the part of the public authorities, to reinforce strategies for BC prevention aimed at health education and communication, disease and risk factor surveillance, and early detection, in addition to guaranteeing access to the recommended treatment for all identified cases, especially in the public healthcare network.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statement
This retrospective cohort study was approved by the appropriate ethics committee (Research Ethics Committee of the Universidade Federal de Juiz de Fora, Minas Gerais, Brazil, under reference No. 2.038.397, CAAE: 04575712.4.0000.5147), which allowed dispensing with informed consent for this research, according to national regulations (Res. CNS 196/96). The data were collected from the records of the oncology reference center, and the confidentiality of the participants was protected. We emphasize that all participants are fully anonymous, the database does not contain direct or indirect identifiers, and publication of such data does not compromise anonymity or confidentiality and does not breach local data protection laws.
Author contributions
AF, VF, JC and MG conceived the study. JC, ADC, VF, CS, CJ and MG were responsible for the data collection, analysis, and interpretation. AF, VF, MN, AC, MB-T and MG designed the analysis and wrote the manuscript. All authors (AF, MG, MB-T, VF, JC, MN, ADC, CS, AC, and CJ) commented on the initial drafts of the manuscript, critically reviewed the manuscript, and read and approved the final version.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Sung H, Ferlay J, Siegel RL, Laversanne M, Soerjomataram I, Jemal A, et al. Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin (2021) 71(3):209–49. doi: 10.3322/caac.21660
2. Brazil I. The context of breast cancer in Brazil: synthesis of data from information systems. Rio de Janeiro: INCA (2019). Available at: https://www.inca.gov.br/sites/ufu.sti.inca.local/files//media/document//a_situacao_ca_mama_brasil_2019.pdf.
3. Goss PE, Lee BL, Badovinac-Crnjevic T, Strasser-Weippl K, Chavarri-Guerra Y, Louis JS, et al. Planning cancer control in Latin America and the Caribbean. Lancet Oncol (2013) 14(5):391–436. doi: 10.1016/S1470-2045(13)70048-2
4. Unger-Saldaña K, Miranda A, Zarco-Espinosa G, Mainero-Ratchelous F, Bargalló-Rocha E, Miguel Lázaro-León J. Health system delay and its effect on clinical stage of breast cancer: multicenter study. Cancer. (2015) 121(13):2198–206. doi: 10.1002/cncr.29331
5. Allemani C, Matsuda T, Di Carlo V, Harewood R, Matz M, Nikšić M, et al. Global surveillance of trends in cancer survival 2000-14 (CONCORD-3): analysis of individual records for 37513025 patients diagnosed with one of 18 cancers from 322 population-based registries in 71 countries. Lancet. (2018) 391(10125):1023–75. doi: 10.1016/S0140-6736(17)33326-3
6. Mendonça GAS, Silva AM, Caula WM. Tumor characteristics and five-year survival in breast cancer patients at the national cancer institute, Rio de Janeiro, Brazil. Cad Saude Publica. (2004) 20(5):1232–9. doi: 10.1590/S0102-311X2004000500017
7. De Moraes AB, Zanini RR, Turchiello MS, Riboldi J, De Medeiros LR. Survival study of breast cancer patients treated at the hospital of the federal university in Santa maria, Rio grande do sul, Brazil. Cad Saude Publica. (2006) 22(10):2219–28. doi: 10.1590/S0102-311X2006001000028
8. Schneider IJC, d’Orsi E. Five-year survival and prognostic factors in women with breast cancer in Santa catarina state, Brazil. Cad Saude Publica. (2009) 25(6):1285–96. doi: 10.1590/S0102-311X2009000600011
9. Guerra MR, Mendonça GAS, Bustamante-Teixeira MT, Cintra JRD, Carvalho LM, Magalhães LMPV. Five-year survival and prognostic factors in a cohort of breast cancer patients treated in juiz de fora, minas gerais state, Brazil. Cad Saude Publica. (2009) 25(11):2455–66. doi: 10.1590/S0102-311X2009001100015
10. Ayala ALM. Survival of women with breast cancer, of a city in the south of Brazil. Rev Bras enferm. (2012) 65(4):566–70. doi: 10.1590/S0034-71672012000400003
11. Fujimoto RHP, Koifman RJ, Silva IF. Survival rates of breast cancer and predictive factors: a hospital-based study from western Amazon area in Brazil. Ciênc. saúde coletiva; (2019) 24(1):261–73. doi: 10.1590/1413-81232018241.35422016
12. Balabram D, Turra CM, Gobbi H. Survival of patients with operable breast cancer (Stages I-III) at a Brazilian public hospital-a closer look into cause-specific mortality. BMC Cancer. (2013) 13(434). doi: 10.1186/1471-2407-13-434
13. Fayer VA, Guerra MR, Cintra JRD, Bustamante-Teixeira MT. Ten-year survival and prognostic factors for breast cancer in the southeast region of Brazil. Rev Bras Epidemiol. (2016) 19(4):766–78. doi: 10.1590/1980-5497201600040007
14. Ayala ALM, Anjos JC, Cassol GA, Höfelmann DA. Survival rate of 10 years among women with breast cancer: a historic cohort from 2000-2014. Cien Saude Colet. (2019) 24(4):1537–50. doi: 10.1590/1413-81232018244.16722017
15. Bustamante-Teixeira MT, Faerstein E, Latorre MR. Survival analysis techniques. Cad Saude Publica. (2002) 18(3):579–94. doi: 10.1590/S0102-311X2002000300003
16. Sant M, Allemani C, Capocaccia R, Hakulinen T, Aareleid T, Coebergh JW, et al. Stage at diagnosis is a key explanation of differences in breast cancer survival across Europe. Int J Cancer. (2003) 106(3):416–22. doi: 10.1002/ijc.11226
17. Siegel RL, Miller KD, Jemal A. Cancer statistics, 2019. CA Cancer J Clin (2019) 69(1):7–34. doi: 10.3322/caac.21551
18. Soerjomataram I, Louwman MW, Ribot JG, Roukema JA, Coebergh JW. An overview of prognostic factors for long-term survivors of breast cancer. Breast Cancer Res Treat (2008) 107:309–30. doi: 10.1007/s10549-007-9556-1
19. Nogueira MC, Guerra MR, Cintra JRD, Corrêa CSL, Fayer VA, Bustamante-Teixeira MT. Racial disparity in 10-year breast cancer survival: a mediation analysis using potential responses approach. Cad Saude Publica. (2018) 34(9):e00211717. doi: 10.1590/0102-311x00211717
20. Zahnd WE, Sherman RL, Klonoff-Cohen H, Mclafferty SL, Farner S, Rosenblatt KA. Breast cancer staging by subtype in the lower Mississippi delta region states. Cancer Epidemiol. (2019) 63(2019):101624. doi: 10.1016/j.canep.2019.101624
21. Boscoe FP, Henry KA, Sherman RL, Johnson CJ. The relationship between cancer incidence, stage and poverty in the united states. Int J Cancer. (2016) 139(3):607–12. doi: 10.1002/ijc.30087
22. Arnold M, Rutherford MJ, Bardot A, Ferlay J, Andersson TML, Myklebust TA, et al. Progress in cancer survival, mortality, and incidence in seven high-income countries 1995-2014 (ICBP SURVMARK-2): a population-based study. Lancet Oncol (2019) 20(11):1493–505. doi: 10.1016/S1470-2045(19)30456-5
23. Brito C, Portela MC, Vasconcellos MTL. Survival of breast cancer women in the state of Rio de Janeiro, southeastern Brazil. Rev Saude Publica (2009) 43(3):481–9. doi: 10.1590/S0034-89102009000300012
24. Edwards BK, Noone A-M, Mariotto AB, Simard EP, Boscoe FP, Henley SJ, et al. Annual report to the nation on the status of cancer, 1975-2010, featuring prevalence of comorbidity and impact on survival among persons with lung, colorectal, breast, or prostate cancer. Cancer. (2014) 120(9):1290–314. doi: 10.1002/cncr.28509
25. Guerra MR, Azevedo e silva G, Nogueira MC, Leite ICG, de Oliveira RdeVC, Cintra JRD, et al. Breast cancer survival and health iniquities. Cad Saude Publica. (2015) 31(8):1673–84. doi: 10.1590/0102-311X00145214
26. Giovanella L, Mendoza-Ruiz A, Pilar ACA, Rosa MC, Martins GB, Santos IS, et al. Universal health system and universal health coverage: assumptions and strategies. Ciênc saúde coletiva. (2018) 23(6):1763–76. doi: 10.1590/1413-81232018236.05562018
27. Supplementary National Agency of Health. Information notebook in the health insurance: beneficiaries, providers and plans (2019). Rio de Janeiro: ANS. Available at: http://www.ans.gov.br/images/stories/Materiais_para_pesquisa/Perfil_setor/Dados_e_indicadores_do_setor/total-cad-info-jun-2019.pdf (Accessed 15 Jan 2020).
28. Liedke PE, Finkelstein DM, Szymonifka J, Barrios CH, Chavarri-Guerra Y, Bines J, et al. Outcomes of breast cancer in Brazil related to health care coverage: a retrospective cohort study. Cancer Epidemiol Biomarkers Prev (2014) 23(1):126–33. doi: 10.1158/1055-9965.EPI-13-0693
29. Brazil MS. Resident population - minas gerais (2020). Available at: http://tabnet.datasus.gov.br/cgi/tabcgi.exe?ibge/cnv/poptmg.def (Accessed 2 Apr 2020).
30. Malachias I, Leles FAG, Pinto MAS. Minas gerais health regionalization master plan. Belo Horizonte: Secretaria de Estado de Saúde de Minas Gerais (2010). Available at: https://www.saude.mg.gov.br/images/noticias_e_eventos/000_2016/Livro%20Plano%20Diretor%20de%20Regionalizao%20-%20PDR-SUS-MG.pdf.
31. Brazil MS. Ministerial ordinance no 140, 27 Feb 2014. redefines the criteria and parameters of health facilities qualified in specialized care in oncology (2014). Available at: http://bvsms.saude.gov.br/bvs/saudelegis/sas/2014/prt0140_27_02_2014.html (Accessed 19 May 2020).
32. Brazil CNF. National registry of deceased (2017). Available at: https://www.falecidosnobrasil.org.br/ (Accessed 2 Sep 2017).
33. Brazil RF. Situação cadastral do cadastro de pessoas físicas (2017). Available at: https://servicos.receita.fazenda.gov.br/Servicos/CPF/ConsultaSituacao/ConsultaPublica.asp (Accessed 22 Oct 2017).
34. Vasconcelos I, Hussainzada A, Berger S, Fietze E, Linke J, Siedentopf F, et al. The st. gallen surrogate classification for breast cancer subtypes successfully predicts tumor presenting features, nodal involvement, recurrence patterns and disease free survival. Breast. (2016) 29:181–5. doi: 10.1016/j.breast.2016.07.016
35. Joshi S, Garlapati C, Aneja R. Epigenetic determinants of racial disparity in breast cancer: looking beyond genetic alterations. Cancers (Basel). (2022) 14(8):1903. doi: 10.3390/cancers14081903
36. Ellis L, Canchola AJ, Spiegel D, Ladabaum U, Haile R, Gomez SL. Racial and ethnic disparities in cancer survival: the contribution of tumor, sociodemographic, institutional, and neighborhood characteristics. J Clin Oncol (2018) 36:25–33. doi: 10.1200/JCO.2017.74.2049
37. Jemal A, Robbins AS, Lin CC, Flanders WD, DeSantis CE, Ward EM, et al. Factors that contributed to black-white disparities in survival among nonelderly women with breast cancer between 2004 and 2013. J Clin Oncol (2018) 36:14–24. doi: 10.1200/JCO.2017.73.7932
38. Brazil MS. Ministerial ordinance n°2.439/GM, 8 Dec 2005. establishing the national oncological care policy: promotion, prevention, diagnosis, rehabilitation and palliative care, to be implemented in all federal units, observing skills Vol. Seção 1. . Brasil: Diário Oficial da República Federativa do Brasil (2005). p. 80.
39. Brazil MS. Strategic action plan for chronic non-communicable diseases (NCDs) in Brazil -2011 to 2022 (2011). Available at: http://bvsms.saude.gov.br/bvs/publicacoes/plano_acoes_enfrent_dcnt_2011.pdf (Accessed 07 May 2020).
40. Brazil C. Decree n°13.896, 30 Oct 2019. establishing that the examinations related to the diagnosis of malignant neoplasia be carried out within a maximum period of thirty days and to start the treatment the period of sixty days . Available at: http://www.planalto.gov.br/ccivil_03/_ato2019-2022/2019/lei/l13896.htm (Accessed 31 May 2020).
41. Azevedo e Silva G, Bustamante-Teixeira MT, Aquino EML, Tomazelli JG, Dos-Santos-Silva I. Access to early breast cancer diagnosis in the Brazilian unified national health system: an analysis of data from the health information system. Cad Saude Publica. (2014) 30(7):1537–50. doi: 10.1590/0102-311X00156513
42. Rezende MCR, Koch HA, Figueiredo JA, Thuler LCS. Factors leading to delay in obtaining definitive diagnosis of suspicious lesions for breast cancer in a dedicated health unit in Rio de Janeiro. Rev Bras Ginecol Obs. (2009) 31(2):75–81. doi: 10.1590/S0100-72032009000200005
43. Oliveira EXG, Pinheiro RS, Melo ECP, Carvalho MS. Socioeconomic and geographic constraints to access mammography in Brazil, 2003-2008. Cienc e Saude Coletiva (2011) 16(9):3649–64. doi: 10.1590/S1413-81232011001000002
44. Marchi AA, Gurgel MSC. Adherence to the opportunistic mammography screening in public and private health systems. Rev Bras Ginecol Obs. (2010) 32(4):191–7. doi: 10.1590/S0100-72032010000400007
45. Travassos C, Williams DR. The concept and measurement of race and their relationship to public health: a review focused on Brazil and the united states. Cad Saúde Pública. (2004) 20(3):660–78. doi: 10.1590/S0102-311X2004000300003
46. Qin Yu X. Socioeconomic disparities in breast cancer survival: relation to stage at diagnosis, treatment and race. BMC Cancer. (2009) 9(364). doi: 10.1186/1471-2407-9-364
47. Akinyemiju T, Sakhuja S, Vin-Raviv N. Racial and socio-economic disparities in breast cancer hospitalization outcomes by insurance status. Cancer Epidemiol. (2016) 43:63–9. doi: 10.1016/j.canep.2016.06.011
48. Cabral ALLV, Giatti L, Casale C, Cherchiglia ML. Social vulnerability and breast cancer: differentials in the interval between diagnosis and treatment of women with different sociodemographic profiles. Cien Saude Colet. (2019) 24(2):613–22. doi: 10.1590/1413-81232018242.31672016
49. Gonçalves H, Guerra MR, Cintra JRD, Fayer VA, Brum IV, Bustamante-Teixeira MT. Survival study of triple-negative and non–Triple-Negative breast cancer in a Brazilian cohort. Clin Med Insights Oncol (2018) 12:1179554918790563. doi: 10.1177/1179554918790563
50. Fayaz S, Demian GA, El-Sherify M, Eissa H, Aziz M, Abuzallouf S. Triple negative breast cancer: 10-year survival update of the applied treatment strategy in Kuwait. Gulf J Oncol (2019) 1(29):53–9. doi: https://pubmed.ncbi.nlm.nih.gov/30957764/
51. Oliveira EXG, Melo ECP, Pinheiro RS, Noronha CP, Carvalho MS. Access to cancer care: mapping hospital admissions and high-complexity outpatient care flows. Case Breast Cancer (2011) 27(2):317–26. doi: 10.1590/S0102-311X2011000200013. Cad Saude Publica.
52. Hill DA, Friend S, Lomo L, Wiggins C, Barry M, Prissbutz E, et al. Breast cancer survival, survival disparities, and guideline-based treatment. Breast Cancer Res Treat (2018) 170(2):405–14. doi: 10.1007/s10549-018-4761-7
53. Breast Cancer Trialists E, Group C. Effect of radiotherapy after breast-conserving surgery on 10-year recurrence and 15-year breast cancer death: meta-analysis of individual patient data for 10,801 women in 17 randomised trials. Lancet (2011) 378(9804):1707–16. doi: 10.1016/S0140-6736(11)61629-2
54. Recht A, Comen EA, Fine RE, Fleming GF, Hardenbergh PH, Ho AY, et al. Postmastectomy radiotherapy: an American society of clinical oncology, American society for radiation oncology, and society of surgical oncology focused guideline update. Ann Surg Oncol (2017) 24(1):38–51. doi: 10.1245/s10434-016-5558-8
55. Overgaard M, Hansen PS, Overgaard J, Rose C, Andersson M, Bach F, et al. Postoperative radiotherapy in high-risk premenopausal women with breast cancer who receive adjuvant chemotherapy. N Engl J Med (1997) 337(14):949–55. doi: 10.1056/NEJM199710023371401
56. Peto R, Davies C, Godwin J, Gray R, Pan HC, Clarke M, et al. Comparisons between diff erent polychemotherapy regimens for early breast cancer: meta-analyses of long-term outcome among 100 000 women in 123 randomised trials. Lancet. (2012) 379(9814):432–44. doi: 10.1016/S0140-6736(11)61625-5
57. Brasil - Ministério da Saúde. Instituto nacional do câncer, in: Registros de câncer (2021). Rio de Janeiro: INCA. Available at: https://www.inca.gov.br/numeros-de-cancer/registros-de-cancer (Accessed 18 julho 2022).
Keywords: survival analysis, cohort study, breast neoplasm, prognosis, neoplasm staging
Citation: Ferreira AdSS, Cintra JRD, Fayer VA, Nogueira MC, Júnior CB, Bustamante-Teixeira MT, Chaoubah A, Cintra AD, Simão CM and Guerra MR (2023) Breast cancer survival and the health system in Brazil: an analysis of public and private healthcare. Front. Oncol. 13:927748. doi: 10.3389/fonc.2023.927748
Received: 24 April 2022; Accepted: 01 May 2023;
Published: 25 May 2023.
Edited by:
Ariella Hanker, University of Texas Southwestern Medical Center, United StatesReviewed by:
Caroline Aquino Moreira-Nunes, Federal University of Ceara, BrazilRegis Resende Paulinelli, Universidade Federal de Goiás, Brazil
Copyright © 2023 Ferreira, Cintra, Fayer, Nogueira, Júnior, Bustamante-Teixeira, Chaoubah, Cintra, Simão and Guerra. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Jane Rocha Duarte Cintra, amFuZXJkY0B0ZXJyYS5jb20uYnI=