 Huijie Wang1†
Huijie Wang1† Xu Cao1†Ping Meng2Caihua Zheng2Jinli Liu2Yong Liu1Tianpeng Zhang3Xiaofang Li1Xiaoyang Shi1Xiaoxing Sun1Teng Zhang4Haiying Zuo5Zhichao Wang5Xin Fu6Huan Li6
Xu Cao1†Ping Meng2Caihua Zheng2Jinli Liu2Yong Liu1Tianpeng Zhang3Xiaofang Li1Xiaoyang Shi1Xiaoxing Sun1Teng Zhang4Haiying Zuo5Zhichao Wang5Xin Fu6Huan Li6 Huanwei Zheng2*
Huanwei Zheng2*- 1Department of Endoscopy, Shijiazhuang Traditional Chinese Medicine Hospital, Shijiazhuang, China
- 2Department of Gastroenterology, Shijiazhuang Traditional Chinese Medicine Hospital, Shijiazhuang, China
- 3Department of Anus & Intestine Surgery, Shijiazhuang Traditional Chinese Medicine Hospital, Shijiazhuang, China
- 4Institute of Traditional Chinese Medicine, North China University of Science and Technology, Tangshan, China
- 5Graduate School, Hebei North University, Zhangjiakou, China
- 6Research and Development Department, Wuhan Metware Biotechnology Co., Ltd, Wuhan, China
Objective: The recent World Endoscopy Organization (WEO) guidelines now recognize precursor lesions of colorectal cancer (CRC) as legitimate screening targets. However, an optimal screening method for detecting advanced adenoma (AA), a significant precursor lesion, remains elusive.
Methods: We employed five machine learning methods, using clinical and laboratory data, to develop and validate a diagnostic model for identifying patients with AA (569 AAs vs. 3228 controls with normal colonoscopy). The best-performing model was selected based on sensitivity and specificity assessments. Its performance in recognizing adenoma-carcinoma sequence was evaluated in line with guidelines, and adjustable thresholds were established. For comparison, the Fecal Occult Blood Test (FOBT) was also selected.
Results: The XGBoost model demonstrated superior performance in identifying AA, with a sensitivity of 70.8% and a specificity of 83.4%. It successfully detected 42.7% of non-advanced adenoma (NAA) and 80.1% of CRC. The model-transformed risk assessment scale provided diagnostic performance at different positivity thresholds. Compared to FOBT, the XGBoost model better identified AA and NAA, however, was less effective in CRC.
Conclusion: The XGBoost model, compared to FOBT, offers improved accuracy in identifying AA patients. While it may not meet the recommendations of some organizations, it provides value for individuals who are unable to use FOBT for various reasons.
1 Introduction
Colorectal cancer (CRC) represents a significant threat to residents of China, contributing substantially to the societal burden (1). In China, CRC-related new cases and deaths account for 9.87% and 8.01% of all malignant tumor incidence and mortality, respectively (2). Addressing this public health challenge effectively is of paramount importance (3).
The goal of CRC screening is to reduce mortality and morbidity by identifying treatable CRC cases and precursor lesions, while minimizing health risks and individual burdens (4). In 2023, the CRC Screening Committee of the World Endoscopy Organization (WEO) issued guidelines for evaluating novel non-invasive screening tests for CRC. These guidelines recommend a dual-step screening process, starting with a non-invasive test and, if positive, followed by a colonoscopy. The non-invasive test should be capable of identifying individuals with an increased likelihood of CRC or advanced precursor lesions (5). Advanced adenoma (AA), an important precursor lesion, is currently considered to carry a significantly elevated risk (6). Although the fecal immunochemical test (FIT) is currently the most widely used non-invasive test, its sensitivity for early detection of CRC, especially AA, remains suboptimal (7). As a result, there is an urgent need for more accurate and non-invasive screening strategies that can identify AA, thereby improving survival rates among CRC patients (8).
Recent clinical guidelines from the Asian Pacific Gastroenterology and Digestive Endoscopy highlight the superiority of combining biomarkers over single biomarkers for detecting colorectal neoplasia (8). Machine learning, based on feature combinations, has emerged as a powerful and effective method for predictive analytics. Its successful application in diagnosis, prediction, and treatment selection has received considerable recognition (9). Routine medical laboratory tests are widely used in China and have become an essential part of modern healthcare (10). The results of these tests may contain more information than even the most experienced clinician can discern, making them suitable for analysis through artificial intelligence to uncover subtle interrelationships (11).
Predictive and diagnostic models based on routine clinical and laboratory data have been developed for various cancers (12–15). However, they often exhibit low sensitivity for AAs due to their non-specific symptoms and distinct risk factors compared to those of CRC (16).
The CRC Screening Committee of the WEO outlines a four-phase evaluation process for new tests, starting with Phase I studies involving limited cohorts or case-control studies (5). Based on this premise, we conducted a Phase I exploratory case-control study using clinical and laboratory data. The aim is to construct a machine-learning diagnostic model for identifying AA and to assess its ability to meet the objectives of non-invasive screening tests, as outlined in the WEO guidelines. These objectives include diagnostic performance regarding the adenoma-carcinoma sequence, adjustable thresholds of positivity, and comparison with validated non-invasive screening tests.
2 Materials and methods
2.1 Study design and population
We conducted a retrospective case-control study, comprising a case group with AA (17) and a control group with normal colonoscopies. The objective was to develop (train) and validate (test) a model for diagnosing AA. AA is defined as an adenoma that exhibits any of the following characteristics: size ≥ 1 cm, presence of tubulovillous or villous components, or high-grade dysplasia. The model was constructed based on features obtained as part of routine clinical care, which included demographic characteristics, lifestyle factors, and clinical features (including comorbidities and laboratory indicators). We ensured that data from at least one laboratory test were available within one month before the colonoscopy. In addition, we validated the outcome model in other populations including non-advanced adenoma (NAA) and CRC. NAA refers to an adenoma that does not meet the definition of AA. All subjects were identified using colonoscopy and pathohistological diagnoses obtained from medical records between April 2015 and June 2022. The exclusion criteria were as follows: a history of colorectal surgery, incomplete medical records, substandard bowel preparation, a colonoscopy that did not reach the cecum, and cases that did not meet the standards of data quality control (QC) (Detail for Figure 1). Specifically, the exclusion criteria for CRC did not include substandard bowel preparation and whether the colonoscope reached the cecum.
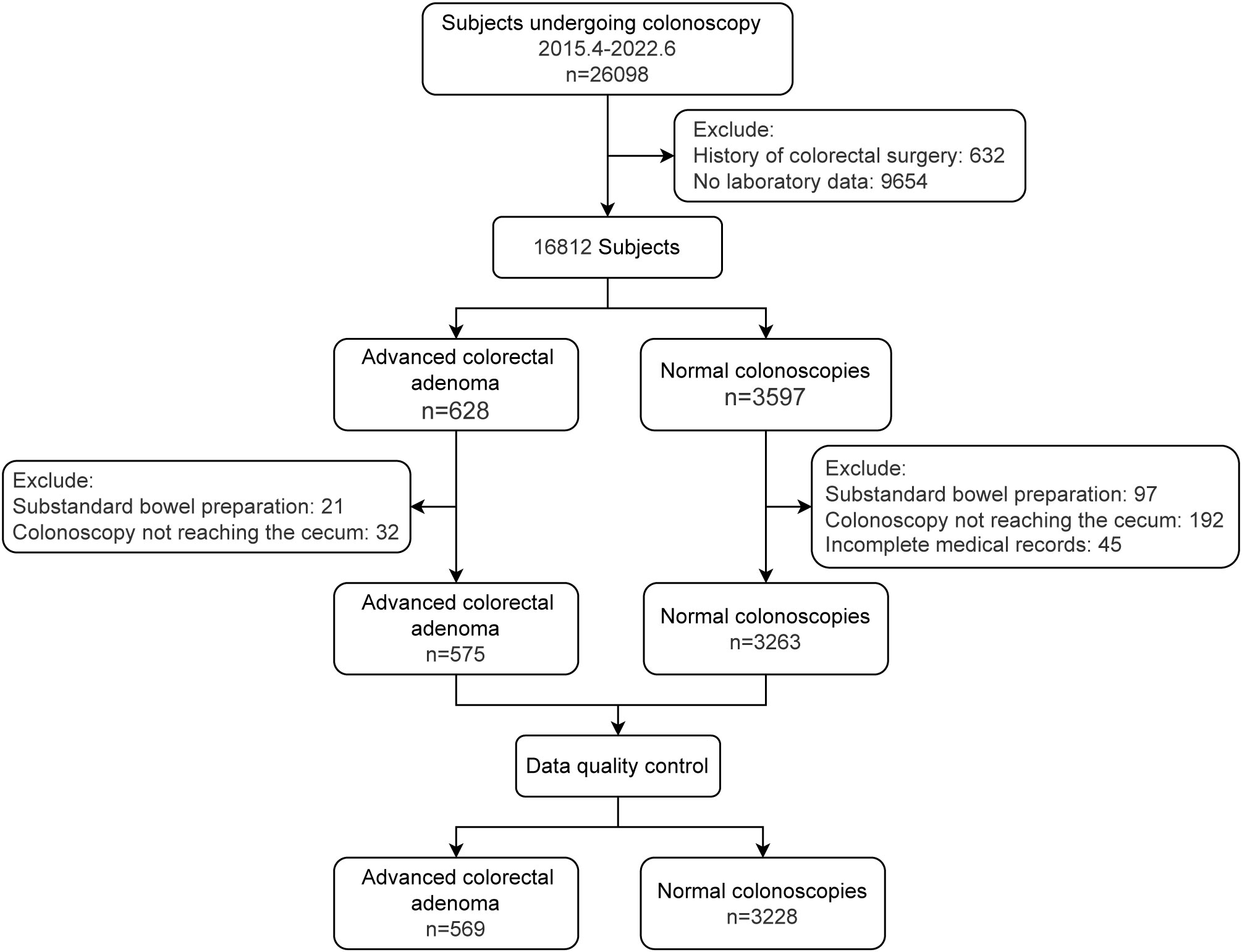
Figure 1 Study population flowchart.
The retrospective study received approval from the Ethics Committee of Shijiazhuang Traditional Chinese Medicine Hospital (NO.20220919029), and the requirements for informed consent were waived due to the retrospective nature of the study.
2.2 Data collection
The present study collected demographic characteristics (age, sex, and marital status), smoking and drinking information (including never, former, and current usage), comorbid conditions, and laboratory test results (routine blood and urine tests, fecal occult blood test [FOBT], biochemistry, tumor markers, and coagulation function). Notably, qualitative FOBT is more prevalent in Chinese hospitals than quantitative FIT. The FOBT method employed in this study was immunocolloid gold (the FOBT was considered positive when the hemoglobin level was greater than or equal to 0.2 μg/ml diluent).
Detailed test methods for laboratory data included in the machine learning analyses were presented in Supplementary Table 1.
2.3 Feature screening
During the data QC process, we retained the features of interest and excluded features with a missing rate exceeding 20% or samples with a missing rate exceeding 50%. For continuous variables with missing values in features retained after QC, we imputed them using k-nearest neighbors (KNN, K = 15). Missing values in categorical variables with a missing rate of less than 20% were imputed using grouped plurality while missing rates of 20% or more were imputed with the new phenotype “MISS”.
Subsequently, we initially screened categorical and continuous variables using the chi-square test and random forest, respectively, to eliminate features with minimal or no impact on grouping. The remaining features’ importance was ranked using the logistic regression (LR), random forest (RF), and least absolute shrinkage and selection operator (LASSO) methods. This step was repeated 10 times to mitigate random bias in data splitting. We took the intersection of the features selected by different models and weighted the importance of each feature, summing them to obtain the importance of weighted features for manual screening.
2.4 Machine learning modeling and validation
We employed five machine learning methods, namely LR, RF, eXtreme Gradient Boosting (XGBoost), KNN, and support vector machine (SVM), for modeling within the caret framework in R. The data were randomly divided into 10 repetitive groupings based on an 8:2 ratio (training group: validation group) to generate 10 sets of training and validation datasets. We modeled the training sets using the aforementioned five methods.
For all methods except LR, we predefined a wide range of parameters and evaluated them using the Grid Searching method using 3 independent 10-fold cross-validations to obtain the most appropriate modeling parameter within the current parameter space, which was then used for model construction.
We predicted scores on the training set data using the models obtained from the five methods. Based on the prediction results of the training set, we plotted receiver operating characteristic (ROC) curves, and the point closest to the top-left corner was selected as the classification threshold (closest.topleft). We applied the model and threshold to the validation set data and calculated the area under the curve (AUC), sensitivity, and specificity to evaluate the model performance and determine the final resultant model.
2.5 Evaluating model performance based on the latest WEO guidelines
We assessed the diagnostic performance of the outcome model in patients with NAA, AA, and CRC in the adenoma-carcinoma sequence using true positive rate (TPR) and false positive rate (FPR). Qualitative FOBT was selected as a validated non-invasive screening test, and we compared the diagnostic performance of the outcome model and the FOBT in patients with FOBT results. We also employed an adjustable positivity threshold to assess disease risk based on an arbitrary risk scale from 0 to 100, calculating the true positives (TP), false negatives (FN), true negatives (TN), false positives (FP), sensitivity (%), specificity (%), positive predictive value (PPV, %), and negative predictive value (NPV, %) (18).
2.6 Statistical analysis
To compare the differences among groups, we adopted the Wilcoxon test, t-test, or chi-square test, depending on the type and distribution of the data. We performed ROC curve analysis using the pROC package in R, and the Delong method was used to calculate the confidence intervals. The bootstrap method was applied to calculate the 95% confidence intervals for sensitivity and specificity. The Hanley-McNeil test was used to analyze the statistical significance of the difference in AUC between the outcome model and FOBT (19).
3 Results
3.1 Study participants
We initially included a total of 575 AAs and 3263 controls. After QC, 569 AAs and 3228 controls were eligible for machine learning modeling and validation. The demographic and clinical characteristics of the study participants are shown in Table 1. Supplementary Table 2 provides more descriptive information on features.

Table 1 Demographic and clinical characteristics of the study participants.
3.2 Feature screening
We collected 167 features, and after data QC and feature screening, 60 features were retained for machine learning modeling (see Supplementary Table 3 for details). In ROC analyses using separate variable to differentiate between the AA and control groups (Figure 2, Table 2), none of these indicators demonstrated strong discriminatory power (AUC<0.8), with age exhibiting the highest discriminatory power (AUC=0.77).
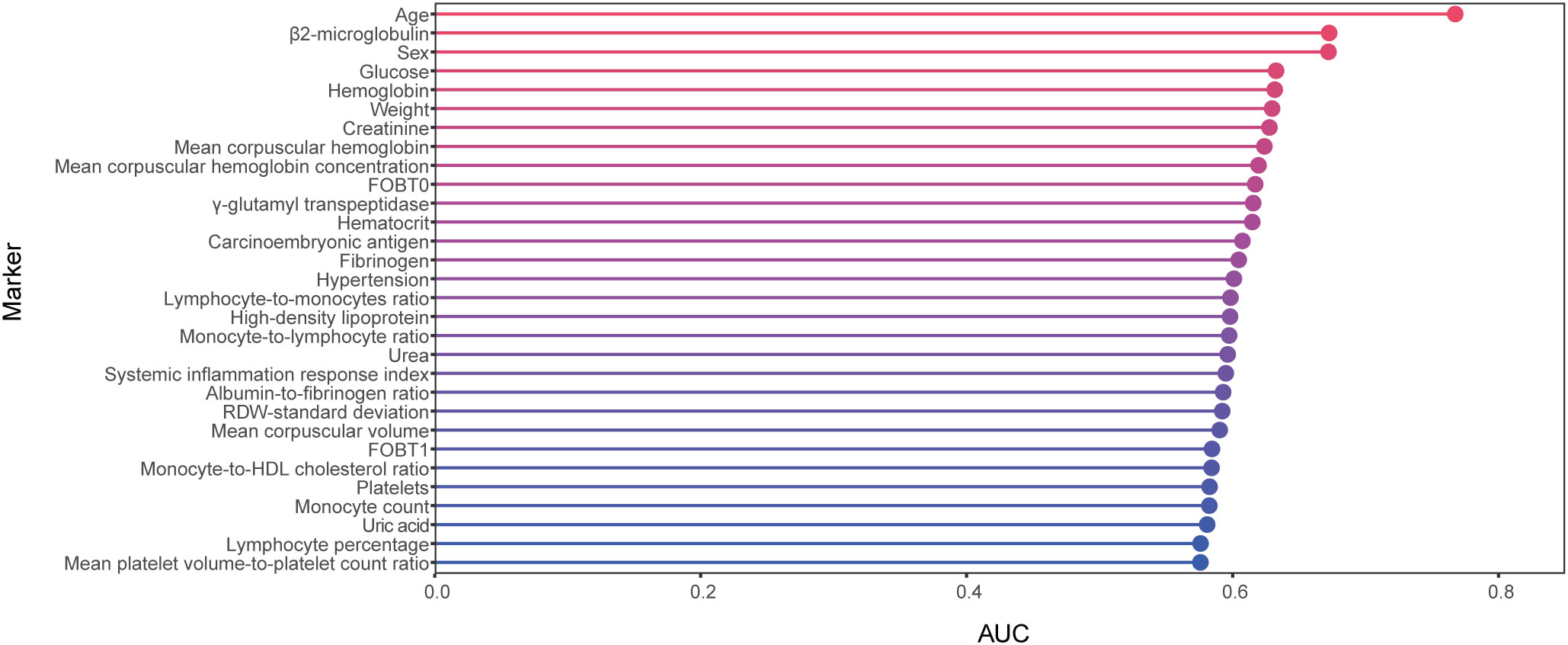
Figure 2 Cleveland dot plots show AUCs for Top 30 parameters identifying AAs and controls. AA, advanced adenoma.
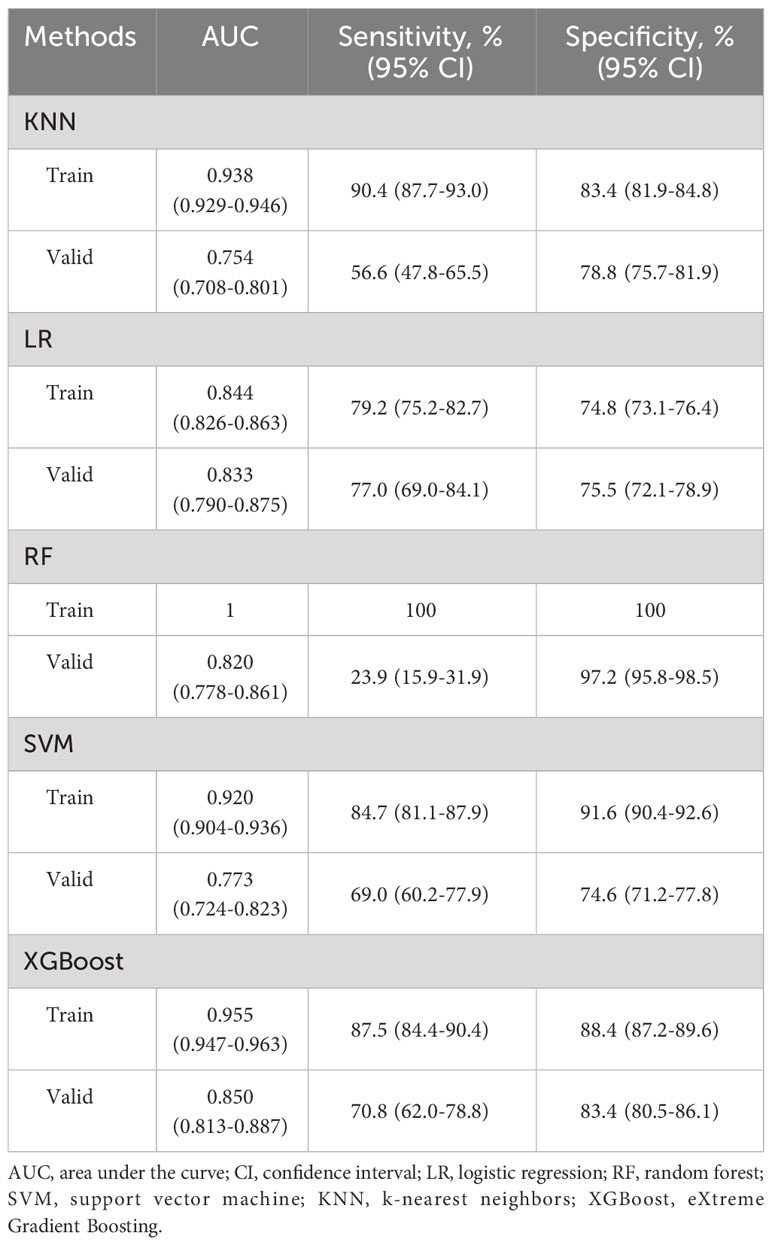
Table 2 Diagnostic performance of various models in training and validation sets.
3.3 Modelling and validation using different models
We successfully built five models using different machine learning methods (KNN, XGBoost, LR, RF, and SVM). We calculated the AUC, sensitivity, and specificity for both the training and validation sets to characterize the diagnostic performance of these models (Figure 3A, Table 2). Overall, the XGBoost model showed the most promising diagnostic performance for identifying patients with AA while maintaining a validation set specificity of at least 0.8. The XGBoost model demonstrated good diagnostic performance in both the training and validation sets, with a sensitivity of 87.5% (95% CI, 84.4−90.4%) (AA=456, Control=2583) and a specificity of 88.4% (95% CI, 87.2−89.6%) in the training set. And the validation set performance resulted in 70.8% (95% CI, 62.0−78.8%) sensitivity and 83.4% (95% CI, 80.5−86.1%) specificity (AA=113, Control=645). Conversely, the RF model, which performed well in the training set, exhibited 97.2% specificity but only 23.9% sensitivity in the validation set, suggesting potential overfitting. The combined diagnostic performance of KNN, LR, and SVM in the validation set did not match that of XGBoost. Thus, based on these results, we concluded that the XGBoost method provided the best performance on the dataset and selected it as the final model.
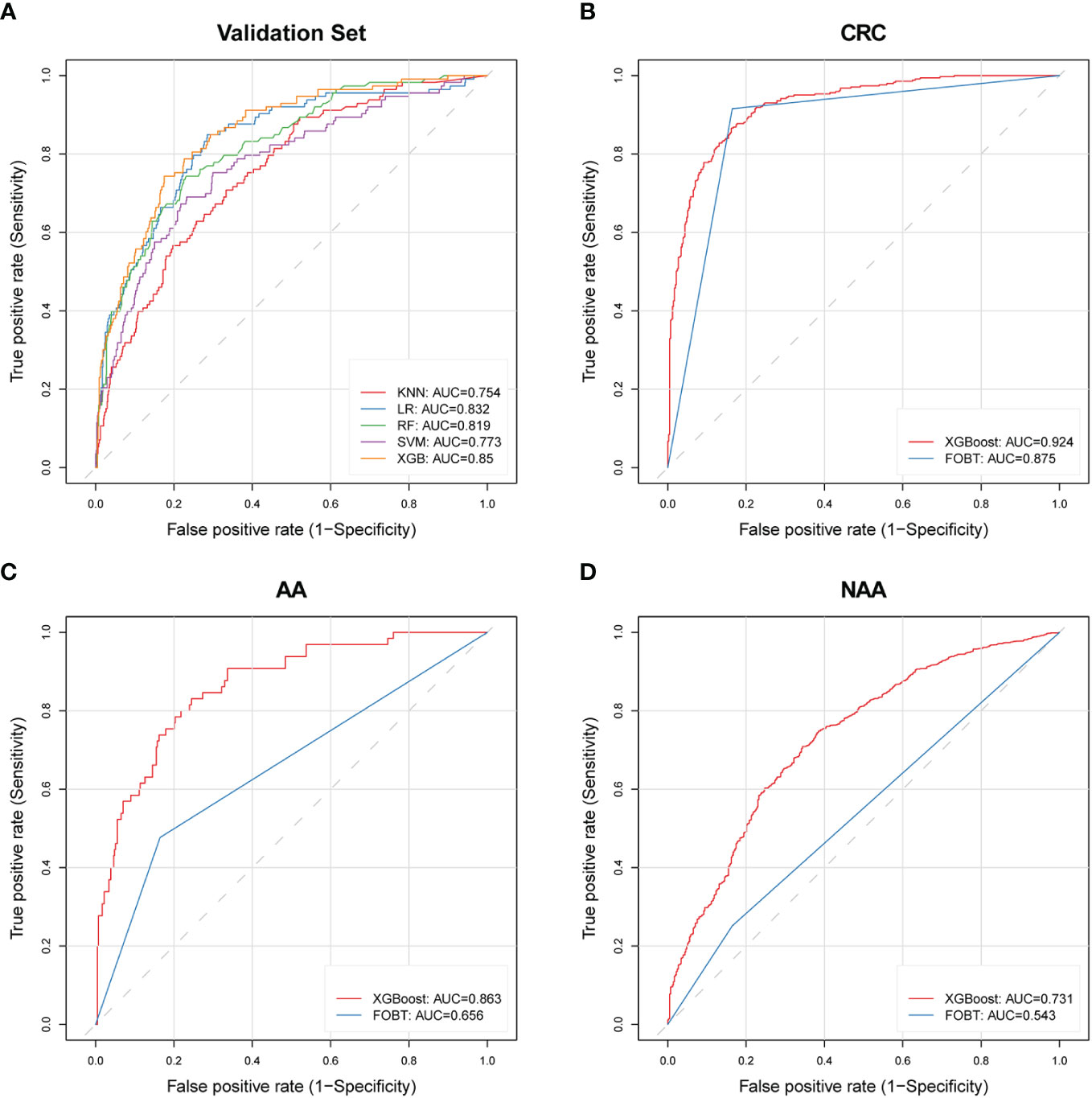
Figure 3 ROC curves of machine learning models and FOBT in different validation cohorts. (A) Five constructed machine learning models in the validation set; (B) XGBoost model and FOBT in the CRC validation set with FOBT results; (C) XGBoost model and FOBT in the AA validation set with FOBT results; (D) XGBoost model and FOBT in the NAA validation set that includes FOBT results. AA, advanced adenoma; NAA, non-advanced adenoma; CRC, colorectal cancer; ROC, receiver operating characteristic; XGBoost, eXtreme Gradient Boosting; FOBT, fecal occult blood test; LR, logistic regression; RF, random forest; SVM, support vector machine; KNN, k-nearest neighbors; AUC, area under the curve.
3.4 Evaluating the diagnostic performance of models based on the latest WEO guidelines
3.4.1 Diagnostic performance in the adenoma-carcinoma sequence
We validated the diagnostic performance of the XGBoost model in the validation set for AA (n=113), NAA (n=3047), and CRC (n=488) (Table 3). In these three groups, the FPR was 16.6% and the TPR was 70.8% (AA), 42.7% (NAA), and 80.1% (CRC), respectively.
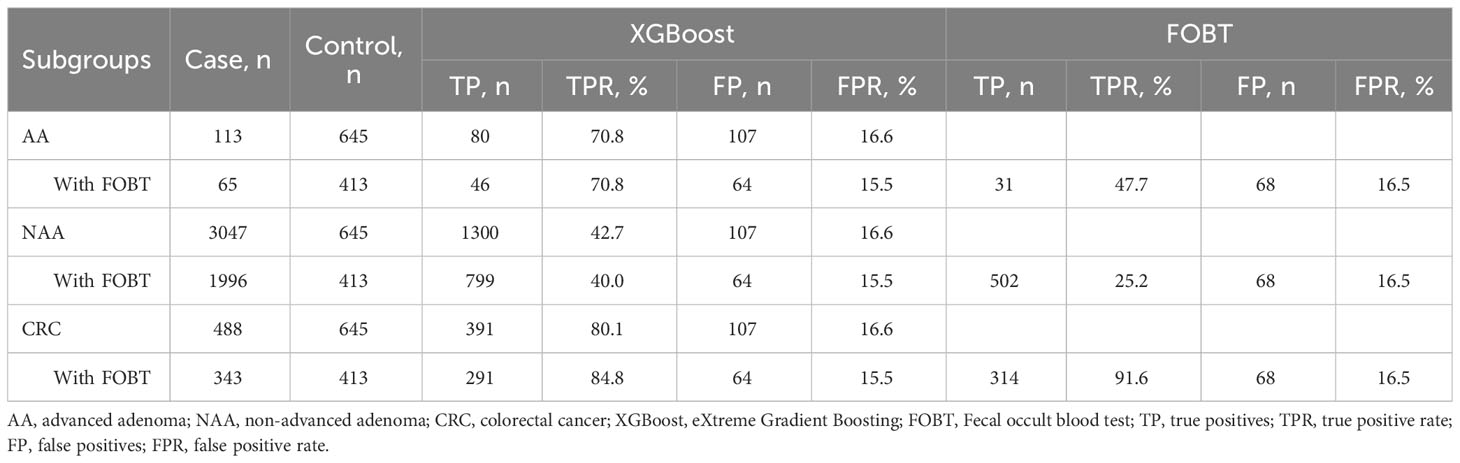
Table 3 Diagnostic performance of the XGBoost model and FOBT in the validation set of advanced adenoma, non-advanced adenoma, and colorectal cancer.
3.4.2 Comparison of diagnostic performance of XGBoost model and FOBT
In this study, we screened three subsets with FOBT results: CRC (n=343), NAA (n=1996), and AA (n=65). This was done to compare the diagnostic performance of the XGBoost model with that of the FOBT, as shown in Table 4. The FPR of the XGBoost model (15.5%) was superior to that of the FOBT (16.5%). The TPR of the XGBoost model for NAA and AA was 40.03% and 70.8%, respectively, which were better than FOBT (25.2% and 47.7%). However, in CRC, the TPR of the XGBoost model (84.8%) was lower than that of FOBT (91.6%). The ROC curves of the XGBoost model and FOBT for these three subsets are depicted in Figures 3B–D, respectively. Moreover, we analyzed the difference in AUC between the XGBoost model and FOBT. As shown in Table 4, we found that in all three validation sets, the AUC of the XGBoost model was significantly higher than that of FOBT (all P<0.05). This indicates that from the perspective of AUC, the XGBoost model outperforms FOBT.

Table 4 Comparison of AUC between XGBoost and FOBT in different validation sets.
3.4.3 Adjustable positivity thresholds for the XGBoost model
We transformed the calculation results of the XGBoost model into risk scores with a score range of 0 to 100, allowing visualization of sensitivity, specificity, and other indicators at different thresholds (Table 5). For example, choosing a score of 10 as the positive threshold resulted in a sensitivity of 87.6% and specificity of 64.34%, while a score of 20 yielded a sensitivity of 74.3% and specificity of 82.5.
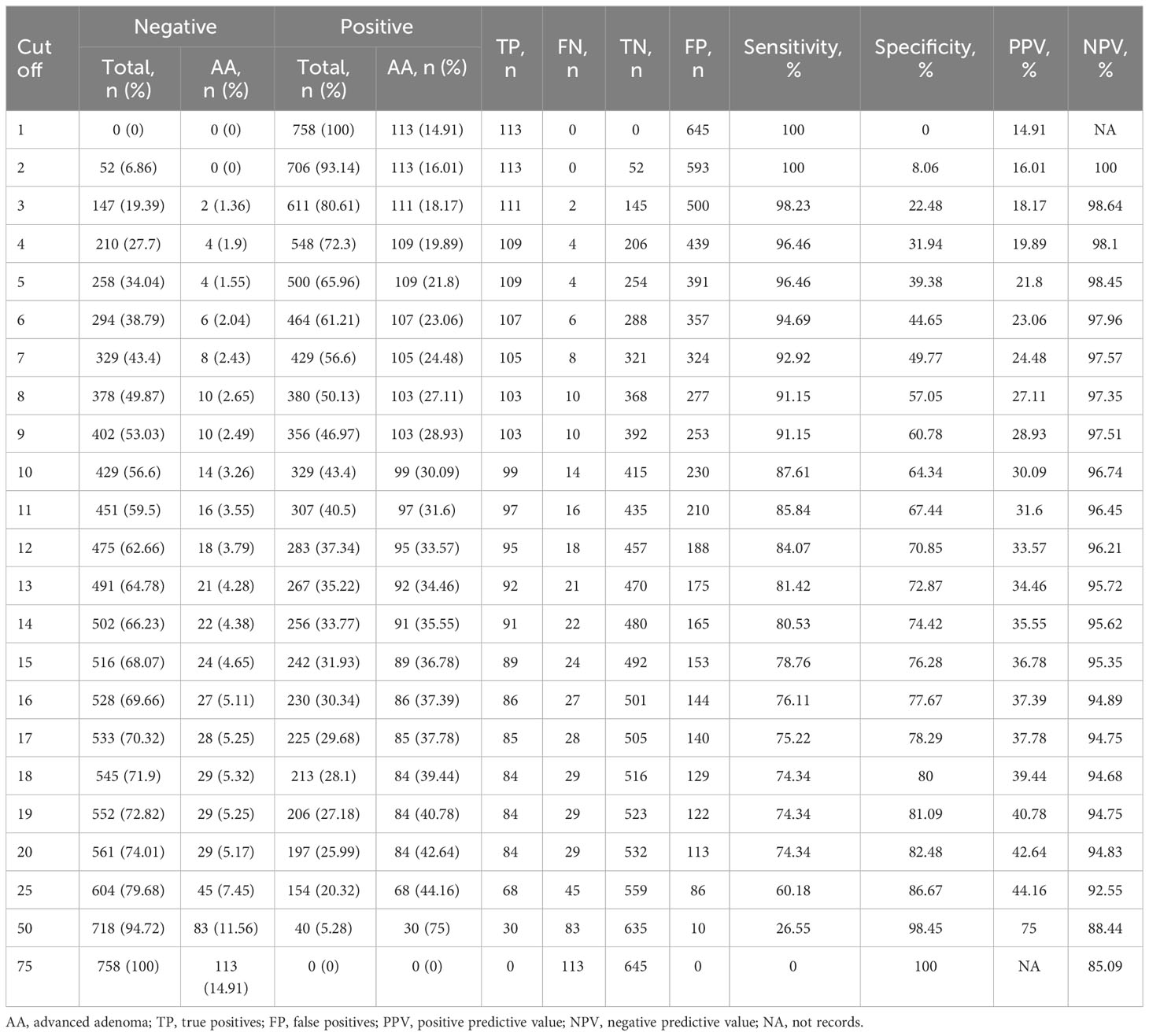
Table 5 Relative risk scores for predicting a diagnosis of AA within the next 30 days at different thresholds in the test set.
4 Discussion
The recent guidelines from the WEO for endoscopic CRC screening have incorporated principles such as treating screening as a multistep process, recognizing precursor lesions for CRC as legitimate targets, using FIT as a current comparator, and providing the ability to adjust thresholds for new test positivity. In light of this, we conducted a phase I exploratory study using 60 clinical and laboratory data points to develop and validate an XGBoost model for identifying patients with AA. The model exhibited a sensitivity of 70.8% and specificity of 83.4% in the validation set, successfully detecting NAA with a sensitivity of 42.7% and CRC with a sensitivity of 80.1%. The risk assessment scale, transformed by the XGBoost model, showcased varying levels of disease risk at different positivity thresholds, and notably, the XGBoost model outperformed FOBT in identifying more patients with AA.
Detecting and endoscopically resecting colorectal precancerous lesions, such as AA, has been recognized as an effective method for preventing the occurrence of CRC and reducing CRC-induced mortality (20). Ensuring the identification of AA is a crucial objective in CRC screening programs (21). Despite colonoscopy being the most frequently recommended and performed screening method, its adoption remains low among the Chinese population, with some individuals preferring less invasive alternatives such as FOBT or FIT (22). Additionally, a significant number of subjects show a preference for blood-based screening tests over stool-based tests (23), which poses challenges to the widespread implementation of stool tests. Developing AA identification tools based on easily accessible data without imposing additional burdens on patients or healthcare providers increases the likelihood of enabling patients to benefit from screening. Pan et al. (24) constructed a diagnostic model based on serum N-glycan levels with machine learning involving a population comprising cases of AA and CRC. In this model, the sensitivity and specificity for diagnosing AA were reported as 58% and 85%, respectively. However, it’s important to note that, like many existing CRC diagnostic models, Pan et al. did not create a dedicated model exclusively for AA (25–28). This approach could explain the poor performance of the model in identifying AA. Xiang et al. (20) developed a serum metabolite-based diagnostic model for AA (255 AAs and 178 controls) with a sensitivity of 44.7% and a specificity of 88.9%. The study highlighted that the sensitivity of all current AA diagnostic models remains below 45% at a similar level of specificity. While our model achieves a sensitivity above 50% for detecting AA at this level of specificity, it does not meet the requirements set by certain agencies, such as the United States Preventive Services Task Force, which mandates an acceptable sensitivity of at least 70% for CRC and a specificity of at least 90% for both cancer and advanced precursor lesion (29).
In China, certain large-scale CRC screening programs and hospitals typically employ the qualitative immunogold method for FOBT (30–32). However, there remain individuals who either cannot or choose not to provide stool samples. Importantly, the diagnostic model utilized in this study does not necessarily rely on FOBT results; it is designed to apply to subjects without FOBT. In the current exploratory study of the adenoma-carcinoma sequence, the XGBoost model demonstrated superiority over FOBT in diagnosing NAA and AA but was found to be less effective than FOBT in diagnosing CRC. The simplicity and rapidity of the FOBT, and notably high sensitivity for CRC screening render it irreplaceable in the context of the adenoma-carcinoma sequence. Additionally, the XGBoost model offers potential benefits to patients who do not undergo FOBT for various reasons.
The test positivity threshold plays a crucial role in determining various important parameters. Specifically, it influences the test positivity rate, which subsequently impacts the workload of colonoscopy, the quantity of CRC or AA that warrant detection through colonoscopy (a potentially cost-effective alternative measure), the detection rate of the target lesion, and the positive predictive value (33). Non-invasive screening tests with adjustable positivity thresholds or algorithms enable the selection of test accuracy parameters, including diagnostic sensitivity and specificity, as well as test positivity rates that optimally align with the intended goals of the screening program (5). We present test accuracy parameters at different positivity thresholds in the risk assessment table. The capacity to modify detection thresholds can effectively manage the expenses related to colonoscopy, workforce availability, treatment costs, and the public expectations that are integral to equity-focused programs (5). By offering diverse risk stratification data, it can enhance physicians’ clinical decision-making process for individual patients.
This study has several limitations. Firstly, the study population originates from a single center, warranting further validation in diverse countries or regions to achieve widespread applicability. Secondly, it’s noteworthy that a significant portion of the AA cases were recruited from clinical settings with relatively high prevalence rates, which might limit the full representativeness of our results in the general population. Lastly, certain non-routine laboratory indicators included in this study, such as tumor markers and coagulation function, may contribute to an increase in the cost for the patient.
In conclusion, we adhered to WEO guidelines, constructing the XGBoost model of the AA patients using clinical and laboratory data in a phase I exploratory study. We established adjustable positivity thresholds to accommodate diverse screening program objectives. This model significantly outperforms FOBT in identifying patients with NAA and AA in the adenoma-carcinoma sequence; however, it cannot replace FOBT for CRC patients. Despite the XGBoost model’s substantially improved accuracy in AA identification compared to existing screening methods (e.g., FOBT), it has not yet met the recommendations of certain organizations. Nevertheless, it holds the potential to provide valuable benefits for individuals who are unable to undergo the FOBT test due to various reasons.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statement
The studies involving humans were approved by Medical Ethics Committee of Shijiazhuang Traditional Chinese Medicine Hospital. The studies were conducted in accordance with the local legislation and institutional requirements. The ethics committee/institutional review board waived the requirement of written informed consent for participation from the participants or the participants’ legal guardians/next of kin because the requirements for informed consent were waived due to the retrospective nature.
Author contributions
HW: Conceptualization, Investigation, Writing – original draft, Writing – review & editing. XC: Conceptualization, Project administration, Writing – original draft. PM: Data curation, Investigation, Writing – original draft. CZ: Data curation, Investigation, Writing – original draft. JL: Data curation, Investigation, Writing – original draft. TPZ: Data curation, Investigation, Writing – original draft. YL: Data curation, Investigation, Writing – original draft. XL: Data curation, Investigation, Writing – original draft. XYS: Data curation, Investigation, Writing – original draft. XXS: Data curation, Investigation, Writing – original draft. TZ: Data curation, Investigation, Writing – original draft. HYZ: Data curation, Investigation, Writing – original draft. ZW: Data curation, Investigation, Writing – original draft. XF: Formal analysis, Methodology, Writing – review & editing. HL: Formal analysis, Methodology, Writing – review & editing. HWZ: Conceptualization, Funding acquisition, Writing – review & editing, Supervision.
Funding
The author(s) declare financial support was received for the research, authorship, and/or publication of this article. This work was supported by the Hebei Administration of Traditional Chinese Medicine (grant number 2023145), the Hebei Provincial Health Commission (Grant Number 20171005), and the National Famous Old Traditional Chinese Medicine Experts Inheritance Studio Construction Program of National Administration of TCM (grant number: [2022] No. 75).
Conflict of interest
XF and HL were employed by Wuhan Metware Biotechnology Co., Ltd.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fonc.2024.1325514/full#supplementary-material
References
1. Maomao C, He L, Dianqin S, Siyi H, Xinxin Y, Fan Y, et al. Current cancer burden in China: Epidemiology, etiology, and prevention. Cancer Biol Med (2022) 19:1121–38. doi: 10.20892/j.issn.2095-3941.2022.0231
2. Dong C, Ding Y, Weng S, Li G, Huang Y, Hu H, et al. Update in version 2021 of csco guidelines for colorectal cancer from version 2020. Chin J Cancer Res (2021) 33:302–7. doi: 10.21147/j.issn.1000-9604.2021.03.02
3. Rabeneck L, Chiu H-M, Senore C. International perspective on the burden of colorectal cancer and public health effects. Gastroenterology (2020) 158:447–52. doi: 10.1053/j.gastro.2019.10.007
4. Rex DK, Boland CR, Dominitz JA, Giardiello FM, Johnson DA, Kaltenbach T, et al. Colorectal cancer screening: Recommendations for physicians and patients from the u.S. Multi-society task force on colorectal cancer. Gastroenterology (2017) 153:307–23. doi: 10.1053/j.gastro.2017.05.013
5. Robert SB, Carlo S, Graeme PY, James A, Robert B, Sally B, et al. An efficient strategy for evaluating new non-invasive screening tests for colorectal cancer: The guiding principles. Gut (2023) 72:1904–18. doi: 10.1136/gutjnl-2023-329701
6. Bosch LJW, Melotte V, Mongera S, Daenen KLJ, Coupé VMH, van Turenhout ST, et al. Multitarget stool DNA test performance in an average-risk colorectal cancer screening population. Am J Gastroenterol (2019) 114:1909–18. doi: 10.14309/ajg.0000000000000445
7. Jin P, You P, Fang J, Kang Q, Gu F, Cai Y, et al. Comparison of performance of two stool DNA tests and a fecal immunochemical test in detecting colorectal neoplasm: A multicenter diagnostic study. Cancer Epidemiol Biomarkers Prev (2022) 31:654–61. doi: 10.1158/1055-9965.EPI-21-0991
8. Francis KLC, Martin CSW, Andrew TC, James EE, Han-Mo C, Govind KM, et al. Joint asian pacific association of gastroenterology (apage)–asian pacific society of digestive endoscopy (apsde) clinical practice guidelines on the use of non-invasive biomarkers for diagnosis of colorectal neoplasia. Gut (2023) 72:1240. doi: 10.1136/gutjnl-2023-329429
9. Saberi-Karimian M, Khorasanchi Z, Ghazizadeh H, Tayefi M, Saffar S, Ferns GA, et al. Potential value and impact of data mining and machine learning in clinical diagnostics. Crit Rev Clin Lab Sci (2021) 58:275–96. doi: 10.1080/10408363.2020.1857681
10. Li X, Lu J, Hu S, Cheng KK, De Maeseneer J, Meng Q, et al. The primary health-care system in China. Lancet (2017) 390:2584–94. doi: 10.1016/S0140-6736(17)33109-4
11. Ngiam KY, Khor IW. Big data and machine learning algorithms for health-care delivery. Lancet Oncol (2019) 20:e262–73. doi: 10.1016/S1470-2045(19)30149-4
12. Gould MK, Huang BZ, Tammemagi MC, Kinar Y, Shiff R. Machine learning for early lung cancer identification using routine clinical and laboratory data. Am J Respir Crit Care Med (2021) 204:445–53. doi: 10.1164/rccm.202007-2791OC
13. Li H, Lin J, Xiao Y, Zheng W, Zhao L, Yang X, et al. Colorectal cancer detected by machine learning models using conventional laboratory test data. Technol Cancer Res Treat (2021) 20:15330338211058352. doi: 10.1177/15330338211058352
14. Yan W, Shi H, He T, Chen J, Wang C, Liao A, et al. Employment of artificial intelligence based on routine laboratory results for the early diagnosis of multiple myeloma. Front Oncol (2021) 11:608191. doi: 10.3389/fonc.2021.608191
15. Tsai IJ, Shen W-C, Lee C-L, Wang H-D, Lin C-Y. Machine learning in prediction of bladder cancer on clinical laboratory data. Diagnostics (2022) 12:203. doi: 10.3390/diagnostics12010203
16. Stegeman I, de Wijkerslooth TR, Stoop EM, van Leerdam ME, Dekker E, van Ballegooijen M, et al. Colorectal cancer risk factors in the detection of advanced adenoma and colorectal cancer. Cancer Epidemiol (2013) 37:278–83. doi: 10.1016/j.canep.2013.02.004
17. Baron JA, Cole BF, Sandler RS, Haile RW, Ahnen D, Bresalier R, et al. A randomized trial of aspirin to prevent colorectal adenomas. N Engl J Med (2003) 348:891–9. doi: 10.1056/NEJMoa021735
18. Soerensen PD, Christensen H, Laursen SGW, Hardahl C, Brandslund I, Madsen JS. Using artificial intelligence in a primary care setting to identify patients at risk for cancer: A risk prediction model based on routine laboratory tests. Clin Chem Lab Med (2022) 60:2005–16. doi: 10.1515/cclm-2021-1015
19. Hanley JA, McNeil BJ. A method of comparing the areas under receiver operating characteristic curves derived from the same cases. Radiology (1983) 148:839–43. doi: 10.1148/radiology.148.3.6878708
20. Xiang J, Li L, Guo X, Li X, Lin K, Yang L, et al. Abstract 3346: Evaluation of a serum-based test integrating tumor tissue and gut microbiome derived metabolites for diagnosis of advanced colorectal adenoma. Cancer Res (2023) 83:3346. doi: 10.1158/1538-7445.AM2023-3346
21. Lidgard GP, Domanico MJ, Bruinsma JJ, Light J, Gagrat ZD, Oldham–Haltom RL, et al. Clinical performance of an automated stool DNA assay for detection of colorectal neoplasia. Clin Gastroenterol Hepatol (2013) 11:1313–8. doi: 10.1016/j.cgh.2013.04.023
22. Hongda C, Ni L, Jiansong R, Xiaoshuang F, Zhangyan L, Luopei W, et al. Participation and yield of a population-based colorectal cancer screening programme in China. Gut (2019) 68:1450. doi: 10.1136/gutjnl-2018-317124
23. Osborne JM, Flight I, Wilson CJ, Chen G, Ratcliffe J, Young GP. The impact of sample type and procedural attributes on relative acceptability of different colorectal cancer screening regimens. Patient Prefer Adher (2018) 12:1825–36. doi: 10.2147/ppa.S172143
24. Pan Y, Zhang L, Zhang R, Han J, Qin W, Gu Y, et al. Screening and diagnosis of colorectal cancer and advanced adenoma by bionic glycome method and machine learning. Am J Cancer Res (2021) 11:3002–20.
25. de Meij TG, Larbi IB, van der Schee MP, Lentferink YE, Paff T, Terhaar sive Droste JS, et al. Electronic nose can discriminate colorectal carcinoma and advanced adenomas by fecal volatile biomarker analysis: Proof of principle study. Int J Cancer (2014) 134:1132–8. doi: 10.1002/ijc.28446
26. van Keulen KE, Jansen ME, Schrauwen RWM, Kolkman JJ, Siersema PD. Volatile organic compounds in breath can serve as a non-invasive diagnostic biomarker for the detection of advanced adenomas and colorectal cancer. Aliment Pharmacol Ther (2020) 51:334–46. doi: 10.1111/apt.15622
27. Telleria O, Alboniga OE, Clos-Garcia M, Nafría-Jimenez B, Cubiella J, Bujanda L, et al. A comprehensive metabolomics analysis of fecal samples from advanced adenoma and colorectal cancer patients. Metabolites (2022) 12:550. doi: 10.3390/metabo12060550
28. Xu J, Zheng Z, Yang L, Li R, Ma X, Zhang J, et al. A novel promising diagnosis model for colorectal advanced adenoma and carcinoma based on the progressive gut microbiota gene biomarkers. Cell Biosci (2022) 12:208. doi: 10.1186/s13578-022-00940-1
29. Force, U. P. S. T. Screening for colorectal cancer: Us preventive services task force recommendation statement. JAMA (2016) 315:2564–75. doi: 10.1001/jama.2016.5989%JJAMA
30. Huang Y, Li Q, Ge W, Cai S, Zhang S, Zheng S. Predictive power of quantitative and qualitative fecal immunochemical tests for hemoglobin in population screening for colorectal neoplasm. Eur J Cancer Prev (2014) 23:27–34. doi: 10.1097/CEJ.0b013e328364f229
31. Huang Y, Cai S, Li Q, Song Y, Yuan Y, Zhang S, et al. Six years of colorectal cancer mortality surveillance in the screening population for a risk stratified screening program. Cancer Epidemiol (2021) 73:101937. doi: 10.1016/j.canep.2021.101937
32. Zhang M, Zhao L, Zhang Y, Jing H, Wei L, Li Z, et al. Colorectal cancer screening with high risk-factor questionnaire and fecal immunochemical tests among 5, 947, 986 asymptomatic population: A population-based study. Front Oncol (2022) 12:893183. doi: 10.3389/fonc.2022.893183
Keywords: advanced colorectal adenoma, machine learning, non-invasive test, risk assessment, adjustable thresholds
Citation: Wang H, Cao X, Meng P, Zheng C, Liu J, Liu Y, Zhang T, Li X, Shi X, Sun X, Zhang T, Zuo H, Wang Z, Fu X, Li H and Zheng H (2024) Machine learning-based identification of colorectal advanced adenoma using clinical and laboratory data: a phase I exploratory study in accordance with updated World Endoscopy Organization guidelines for noninvasive colorectal cancer screening tests. Front. Oncol. 14:1325514. doi: 10.3389/fonc.2024.1325514
Received: 21 October 2023; Accepted: 05 February 2024;
Published: 23 February 2024.
Edited by:
Vera Rebmann, University of Duisburg-Essen, GermanyReviewed by:
Akira Umemura, Iwate Medical University, JapanYuhan Zhang, Chinese Academy of Medical Sciences and Peking Union Medical College, China
Copyright © 2024 Wang, Cao, Meng, Zheng, Liu, Liu, Zhang, Li, Shi, Sun, Zhang, Zuo, Wang, Fu, Li and Zheng. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Huanwei Zheng, MTMzMjMxMTkzMTdAMTYzLmNvbQ==
†These authors have contributed equally to this work and share first authorship