 Michael Bashir1†
Michael Bashir1† Sayeda Islam2
Sayeda Islam2 Jordan Wrigley3
Jordan Wrigley3 Anita Arias1
Anita Arias1 Roelie M. Wösten-van Asperen4
Roelie M. Wösten-van Asperen4 Kimberly K. Kertis3
Kimberly K. Kertis3 Melissa M. Hudson5
Melissa M. Hudson5 Courtney M. Rowan6
Courtney M. Rowan6 Aimee C. Talleur7Joshua Wolf8,9
Aimee C. Talleur7Joshua Wolf8,9 Benjamin Oelkers1
Benjamin Oelkers1 Melissa R. Hines10*‡
Melissa R. Hines10*‡ Asya Agulnik1,10‡
Asya Agulnik1,10‡- 1Department of Global Pediatric Medicine, St Jude Children’s Research Hospital, Memphis, TN, United States
- 2Washington University in St. Louis School of Medicine, St. Louis, MO, United States
- 3Biomedical Library, St. Jude Children’s Research Hospital, Memphis, TN, United States
- 4Department of Pediatric Intensive Care, University Medical Centre Utrecht, Wilhelmina Children’s Hospital, Utrecht, Netherlands
- 5Division of Cancer Survivorship, Department of Oncology, St Jude Children’s Research Hospital, Memphis, TN, United States
- 6Department of Pediatrics, Division of Critical Care, Riley Hospital for Children, Indiana University School of Medicine, Indianapolis, IN, United States
- 7Department of Bone Marrow Transplantation and Cellular Therapy, St. Jude Children’s Research Hospital, Memphis, TN, United States
- 8Department of Infectious Diseases, St Jude Children’s Research Hospital, Memphis, TN, United States
- 9Department of Pediatrics, University of Tennessee Health Science Center, Memphis, TN, United States
- 10Division of Critical Care, Department of Pediatric Medicine, St Jude Children’s Research Hospital, Memphis, TN, United States
Background: The Pediatric Organ Dysfunction Information Update Mandate (PODIUM) proposed consensus criteria to define organ dysfunction in critically ill children. However, utilization of the PODIUM criteria in pediatric oncology patients and those who have received hematopoietic cell transplantation or cellular therapy (post-HCT/CAR) may inaccurately classify organ dysfunction in these patients due to differences in organ dysfunction etiology, pathophysiology, and risk factors for adverse outcomes. To address this gap, we report a study protocol to systematically review the performance of the PODIUM criteria for pediatric cancer and/or those treated with HCT and determine if adjustments are needed.
Objective: The objectives of this study will be to [1] identify evidence-based criteria for organ dysfunction predicting adverse outcomes among pediatric oncology and post-HCT patients, [2] use these findings to inform adapted consensus criteria (PODIUM-Onc) for organ dysfunction tailored to this high-risk population through a multidisciplinary modified Delphi process, and [3] describe knowledge gaps to guide future research.
Data source and search strategy: We will perform a systematic literature review of studies published since January 1, 2004, using the following databases: MEDLINE (via PubMed), CINAHL (via EBSCO), EMBASE (via Elsevier), and Web of Science (via Clarivate). Search results will be filtered using a pediatric search hedge and further refined to children (0 to 21 years old) during or up to 1 year after treatment for cancer or HCT/CAR for malignancy. Publications without original data (e.g., comments, editorials, letters, notes, conference materials), studies with ≤ 10 patients, and those preceding January 1, 2004, will be excluded.
Study selection: We will include original studies in any language published since January 1, 2004, that meet all eligibility criteria and for which a full text is available.
Data extraction: Data extraction will include information related to study characteristics, hospital characteristics, underlying population characteristics, patient population characteristics, and outcomes.
Data synthesis: We will extract and report data on the study, hospital, and patient characteristics, outcomes, and risk of bias.
Conclusion: By systematically reviewing and analyzing organ-specific factors associated with patient outcomes and synthesizing these findings through a modified Delphi consensus process, we aim to create consensus criteria that will be clinically relevant for pediatric oncology patients and HCT patients. These criteria will provide a foundation to guide clinical care and to support future research in this vulnerable patient population.
Introduction
Multiple organ dysfunction (MOD) remains the leading cause of death in pediatric intensive care units (PICUs) and is a major contributor to both short- and long-term morbidity (1, 2). Children with cancer or those who have undergone hematopoietic cell transplantation (HCT) and/or cellular therapy (CAR) are especially vulnerable, facing an elevated risk of organ dysfunction and significantly higher mortality rates in the PICU (3–6). Mortality among pediatric cancer patients admitted to the PICU is reported to range from 23% to 28%, approximately five-fold higher than the overall PICU mortality of 5% (7, 8). Patients who develop MOD experience even greater risk, with mortality reported between 50% and 66%, depending on the study and timing of organ dysfunction onset (9, 10) The nature of organ dysfunction in pediatric oncology and post-HCT patients is distinct from that of other critically ill children or immunocompromised young adults, driven by unique etiologies, biological mechanisms, and mortality risk factors.
Historically, research on organ dysfunction in critically ill children has been limited by a lack of standardized organ dysfunction definitions. To address this challenge, in 2022 the Pediatric Organ Dysfunction Information Update Mandate (PODIUM) (3) published a consensus-driven set of criteria to standardize organ dysfunction definitions across 11 systems (cardiovascular, gastrointestinal, neurologic, hepatic, coagulation, endothelial, hematologic, respiratory, endocrine, renal, and immune), as well as for multiorgan dysfunction. Developed by an international expert panel informed by systematic literature reviews, these criteria aim to identify children with single or multiple organ dysfunction for research and to serve as entry criteria or outcome measures in clinical trials.
These general PODIUM criteria, however, are likely insufficient to characterize organ dysfunction among children treated for oncologic disorders, including those that receive allogeneic HCT or cellular therapy (5). First, this patient population is underrepresented in the literature reviewed by PODIUM, with only 2.2% (26 of 1,185) of studies including data from these patients (11). Key studies specifically addressing organ dysfunction in children with cancer were also absent (5, 12–15). Second, currently available scoring and severity-of-illness systems developed for the general pediatric population have limited performance in children with cancer (16, 17), and initial findings suggest the PODIUM criteria may face similar limitations (5). Finally, unique pathobiological factors drive organ dysfunction in this patient population (18, 19), stemming from intensive treatment regimens, such as chemotherapy or immunotherapy, HCT-related complications, or the underlying malignancy itself (20–22). For example, sinusoidal obstruction syndrome (SOS) and immune effector cell-associated cytokine release syndrome (CRS) are established forms of endothelial and immune dysfunction with specific severity grading criteria; however, neither is included in PODIUM.
To address these challenges, we have assembled an international panel of experts in pediatric onco-critical care to identify areas for adjustment of the current PODIUM organ dysfunction criteria for use in pediatric cancer and post-HCT patients, identify evidence-based markers of organ dysfunction that predict adverse outcomes and develop consensus criteria (PODIUM-Onc) tailored to this high-risk population using a multidisciplinary modified Delphi process. These criteria will guide clinical care and inform future research. The planned methodology is described in this protocol paper.
Materials and methods
Systematic review objectives
The objectives of this study are to conduct 12 linked systematic literature reviews to identify specific evidence-based criteria for defining organ dysfunction that predict an increased risk of adverse outcomes among pediatric cancer patients. This study is not a meta-analysis, and does not aim to generate clinical management recommendations. Rather, it seeks to establish a foundational framework upon which future work can validate, refine, and integrate these criteria to better identify children with single or multiple organ dysfunction and to characterize distinct patterns or phenotypes of organ dysfunction associated with poor outcomes.
Protocol and registration
This protocol follows the Preferred Reporting Items for Systematic Review and Meta-Analysis Protocols guidelines (PRISMA) and is registered in the international Prospective Register of Systematic Reviews (PROSPERO 2024 CRD42024608850).
Study team
This proposed work is led by a core team of diverse multidisciplinary experts in pediatric onco-critical care, hematology-oncology, HCT/CAR, and infectious disease, including an MPI team (AAg, MHi), six co-investigators (AAr, MHu, CR, AT, RWA, JWo), four program coordinators/trainees (MB, NBe, SI, BO), a research librarian (JWr), and a data management librarian (KK). This core team is supported by organ-system specific Working Groups comprised of 10–20 experts in the relevant fields (some investigators are included in multiple reviews as per their areas of expertise). The Working Groups were identified to be inclusive of disciplines (oncology, ICU, etc.), professions (nurses, physicians, respiratory therapists, etc.), income level of the country of practice, and to represent all World Health Organization (WHO) regions. Additionally, members of the team are affiliated with multiple professional organizations, including the Pediatric Acute Lung Injury and Sepsis Investigators (PALISI), the European Society of Paediatric and Neonatal Intensive Care (ESPNIC), the Pediatric Acute & Critical Care Medicine Asian Network (PACCMAN), the Sociedad Latinoamericana de Cuidados Intensivos Pediátricos (SLACIP), the Sociedad Latino Americana de Oncología Pediátrica (SLAOP), the Children’s Oncology Group(COG), the Pediatric Transplantation and Cellular Therapy Consortium (PTCTC), and the International Society of Paediatric Oncology (SIOP). This team also includes people with lived experience of cancer, including 2 childhood cancer survivors. These survivors are integral members of our study team and will actively participate in the data synthesis and modified Delphi consensus process alongside clinical experts, contributing as equal partners and co-authors on resulting manuscripts; their involvement in the systematic reviews will be guided by their individual interests and expertise. The modified Delphi panel will be used to reconcile evidence and achieve consensus on the adapted PODIUM-Onc criteria. Table 1 summarizes the combined demographics of the current Core Team [14] and Working Group Members [90]. Figure 1 illustrates the global distribution of PODIUM-Onc collaborators.
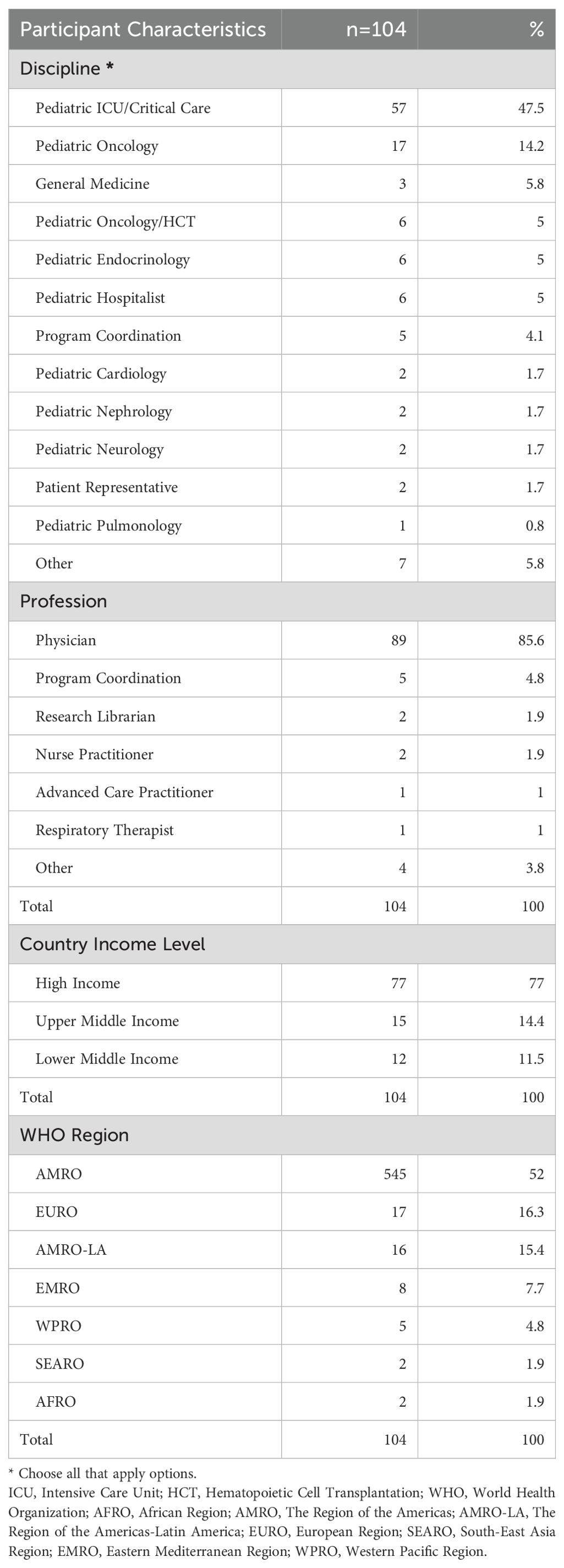
Table 1. Core team and working group demographics.
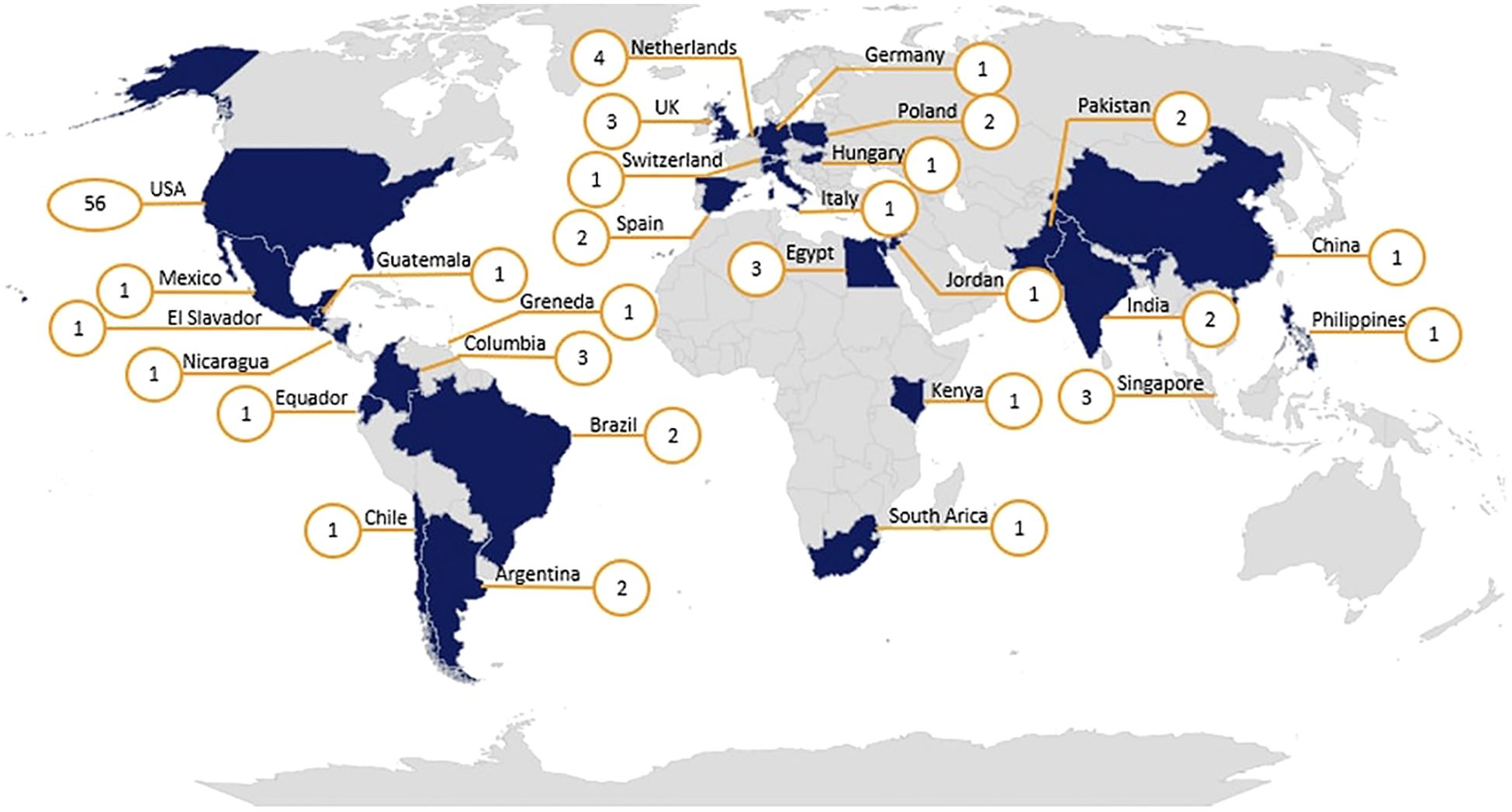
Figure 1. Global distribution of PODIUM-Onc collaborators. Numbers in orange circles represent the number of collaborators in each country.
Population
The population of interest includes children, adolescents, and young adults aged 0–21 years diagnosed with cancer who experience organ dysfunction at any point before, during, or after hematopoietic cell transplantation (HCT), provided the indication for HCT is malignancy, presenting with either single or multiple episodes of acute organ failure within 1 year of completing cancer treatment. “Cancer” is defined as a malignant disease. For studies involving mixed HCT populations (malignant and non-malignant indications), we will include the study if more than 50% of the patients received HCT for malignant conditions. We will only include studies with a sample size of > 10 patients.
We will exclude studies restricted to adult patients (> 21 years old), premature neonates (≤ 36 weeks’ gestation), and mixed populations where data from pediatric cancer patients cannot be extracted separately. We will also exclude studies of non-malignant (benign) tumors and studies including children undergoing HCT where more than 50% are for non-malignant disease to reduce heterogeneity and to maintain focus on defining organ dysfunction within the oncologic context, which differs in its clinical course, risk profile, and therapeutic exposures.
Definition of organ dysfunction and study scope
This study focuses on acute single-organ and multiorgan dysfunction (MOD) in pediatric oncology and post-HCT populations. The organ systems of interest include: respiratory, cardiovascular, neurologic, renal, hepatic, endocrine, endothelial, coagulation, immune, hematologic, and gastroenterology, as well as multiorgan dysfunction, defined as the concurrent dysfunction of two or more organ systems. For the purposes of study inclusion and search consistency, the core panel of experts defined organ toxicity as acute organ dysfunction or failure occurring within 12 months of cancer-directed therapy or hematopoietic cell transplantation (HCT), treated in a hospital setting (PICU, wards, or inpatient), and associated with at least one clinical outcome of interest, such as increased mortality, significant morbidity, prolonged hospitalization, or need for life-sustaining interventions.
Studies focusing solely on chronic organ dysfunction or dysfunction identified in ambulatory settings (e.g., outpatient clinics) are excluded, as we aim to characterize and adapt criteria relevant to acute, hospital-based deterioration in this high-risk population.
Outcome and association
Included studies must report outcomes associated with organ dysfunction or failure, including mortality and morbidity (length of hospital stay, rehospitalization, reoperation, etc.), and analyze how specific organ dysfunction characteristics are statistically associated with these outcomes in the target patient populations. Studies that do not report specified outcomes or evaluate the relationship between organ dysfunction and outcomes are excluded. This focus aligns with our primary aim of identifying evidence-based organ dysfunction criteria linked to adverse outcomes, ensuring that any proposed adaptations to the original PODIUM criteria are rooted in prognostic significance and reflect the clinical trajectory of children with cancer or those undergoing HCT.
Study design and timeframe
We will include original studies published since January 1, 2004, including prospective or retrospective cohort studies, surveillance studies, hospital database publications, cross-sectional studies, data from before-and-after studies, and registry data, regardless of language. The January 2004 cut-off was chosen to align with the methodology of the original PODIUM study and to provide a 20-year timeframe for data collection, which allows for a comprehensive assessment of evolving organ dysfunction definitions over time. While we recognize clinical practices have changed, especially in high-income countries, treatment protocols and diagnostic criteria used in earlier studies may still be relevant in low- and middle-income countries, supporting the global applicability of our adapted criteria.
We will exclude publications limited to abstracts, case reports with ≤ 10 patients, narrative reviews, surveys, study protocols, comments, editorials, letters, notes, conference materials, interventional trials, and any texts where full access to the article is unavailable.
Data sources and search strategy
Our search strategy was collaboratively developed by multidisciplinary co-investigators, an academic librarian, and underwent feasibility testing. We employed a mix of controlled vocabulary terms, such as PubMed Medical Subject Headings (MeSH), and keywords derived from the original 2017 and updated 2020 PODIUM searches. Terms and search strings were curated based on team discussions, alignment with our research objectives, and recent updates to controlled vocabularies and database search algorithms. This strategy encompasses concepts for oncology, HCT/CAR, pediatric patients, multiorgan dysfunction, association analysis, and outcomes, resulting in a highly comprehensive and targeted modular search. To ensure capturing publications focused on the pediatric population, we limited results based on a comprehensive set of subject headings and keywords for “children” and “youth”, because there is no consistent or replicable way to limit search results based on years of age in literature databases. Specific years of age were applied to studies in the screening process. Organ toxicity will be captured using terms and concepts that refer to acute dysfunction, failure, or injury in specific organ systems. We will include search terms for both general and organ-specific toxicities (e.g., hepatotoxicity, nephrotoxicity, neurotoxicity, cardiotoxicity), as well as broader terms such as organ dysfunction, organ failure, and multiorgan dysfunction syndrome (MODS). Importantly, we will not rely solely on the term “toxicity” as it is often underused or inconsistently applied in clinical literature. Instead, we will use a combination of Controlled vocabulary (e.g., MeSH terms like Organ Dysfunction Scores, Organ Failure, Treatment-Related Adverse Events). Keywords referring to both clinical syndromes (e.g., acute kidney injury, sinusoidal obstruction syndrome, cytokine release syndrome) and pathophysiological terms indicating toxicity or damage. To ensure comprehensive inclusion, these terms will be paired with population filters (pediatrics, oncology, HCT) and outcome-related terms (e.g., mortality, prognosis, ICU admission). (The full description of the search terms is found in Supplementary 1).
The search results will be translated across databases and compiled into a Data Set (Reference Manager). In the Reference Manager, we will perform full-text searches for each organ system, enabling us to capture precise and comprehensive data from both abstracts and full-text articles. Each organ-specific search subset will then be uploaded individually into Covidence (23), a web-based platform designed to streamline systematic reviews, allowing us to assess overlaps and relationships between the different organ systems. This strategy will be applied to 11 organ-specific reviews (respiratory, cardiovascular, neurology, renal, hepatic, endocrine, endothelial, coagulation, immune, hematology, and gastroenterology) and one multisystem organ dysfunction review of scoring systems used to predict outcomes in children with cancer.
Study selection and screening process
Titles retrieved from the search will be uploaded to Covidence for systematic review processes, including screening, full-text uploads, and conflict resolution. Citations will be assessed for eligibility based on title, abstract, and full text.
For each systematic review, a diverse group of experts in pediatric oncology, critical care, HCT, infectious disease, and relevant subspecialties were invited to join organ-specific Working Groups. To ensure consistency and accuracy, Working Group members will participate in a training session covering how to use Covidence software, study inclusion and exclusion criteria, and will complete a training set of 10 sample publications (titles and abstracts) before commencing abstract screening. The training set, prepared by the co-investigators, will intentionally include 3–5 true positives. Members of each Working Group will independently screen the training set and discuss their decisions during a group meeting to achieve alignment.
For the main screening phase, per Cochrane recommendations in Covidence (24), each title and abstract will be independently reviewed by two Working Group members using predefined eligibility criteria. Titles rejected by both reviewers will be excluded, while those accepted by both will proceed to full-text screening. In cases of disagreement, a third reviewer will resolve the conflict. Each full-text article will be reviewed by two members of the Working Group to assess eligibility for inclusion in the final set for data extraction. Any conflicts during screening or assessment will be resolved by a third member of the Support Group using Covidence’s conflict resolution feature. For full texts with exclusion criteria, a reason for exclusion will be recorded (e.g., wrong study year; wrong study design (review, case series ≤ 10 patients); Wrong patient population (adults, not cancer patients); not acute organ dysfunction; no outcomes data; full text not found; duplicate publication). Figure 2 provides a sample full-text screening guide for respiratory failure, and each organ-specific review will have a similar adapted guide.
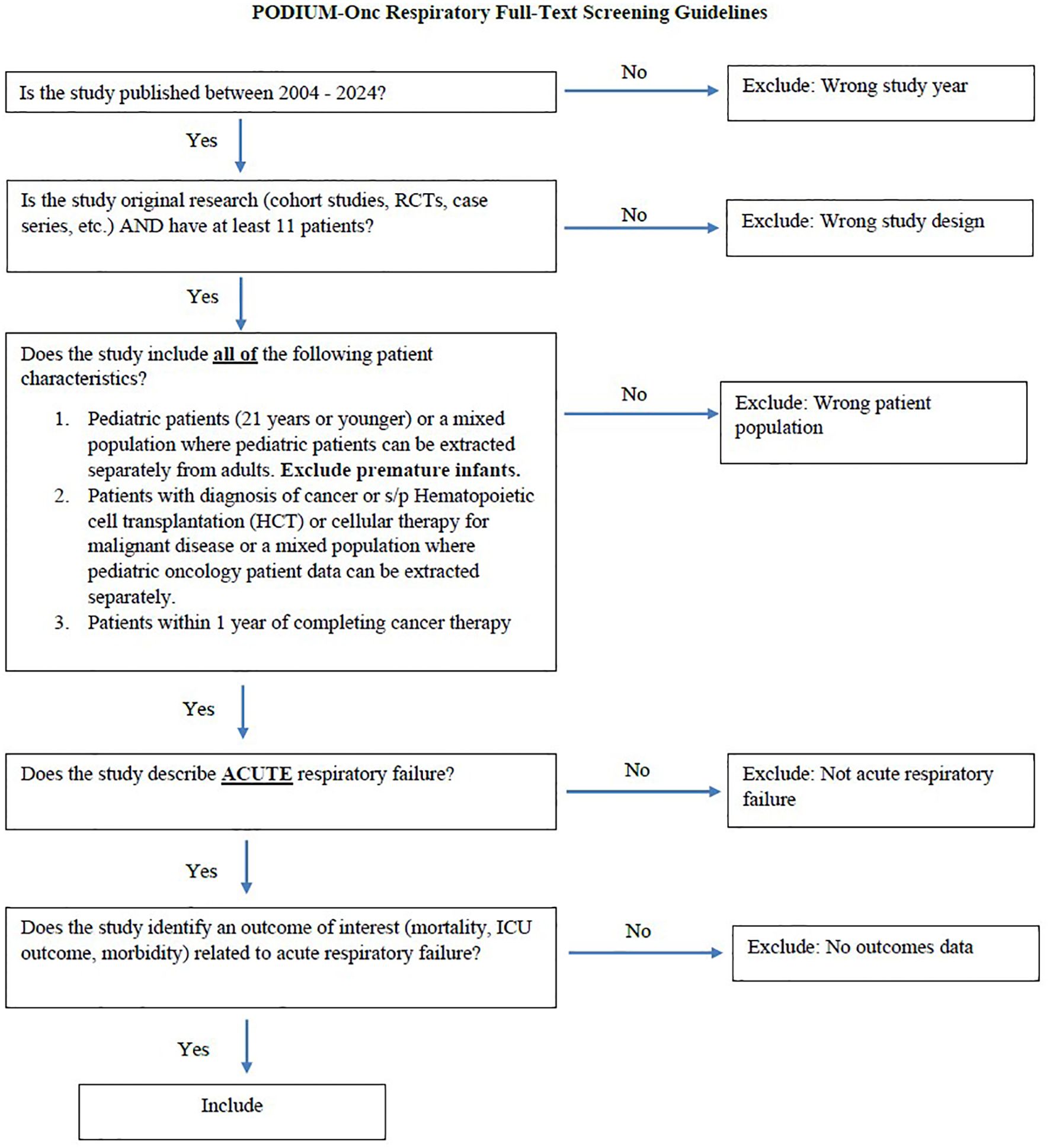
Figure 2. Full-text screening guide for Respiratory Failure; each-specific review will have a similar adapted guide.
Citations identified during title and abstract screening will be excluded if the full text cannot be retrieved after the following steps: searching journal subscriptions at two or more academic institutions, conducting a general web-based search using Google, submitting Interlibrary Loan requests to at least two academic institutions, and directly emailing the corresponding author or editor for the article. Publications with data from more than one country (e.g., global prevalence studies) will be included if they meet the inclusion criteria. For studies published in languages other than English, a bilingual member of the study team will assist in determining inclusion or exclusion.
Data management and extraction
Data management in a large project is crucial. The expected volume of more than 100,000 articles to process presents practical management issues. Multiple organ systems may be addressed in one article, which increases the complexity of retrieving and sorting articles before dissemination to each team. A data management plan (Supplementary 2) was developed to establish viable details of document collection, organization, and short-term storage. Constructing the plan will help the team define procedures like file naming conventions, metadata variables, and assigning responsibilities at each stage of the process, thus addressing legal issues of sponsorship requirements and copyright.
Data from all eligible full-text articles will be extracted by one Working Group member and independently verified by a second member, and entered into REDCap, a secure web-based application designed for electronic data capture (25). During the screening phase, data extraction conflicts will be resolved by a third Working Group member. Data extraction will include information related to study characteristics (i.e., title, authors, year of publication, date of enrollment, language, journal, study design, sample size, inclusion/exclusion criteria, data source), hospital setting (general PICU, oncology PICU, oncology wards, emergency room and operating room), specific definitions of organ failure, outcomes (mortality, functional outcomes/residual morbidity, organ-specific outcomes, outcomes related to MODS, other patient-centered outcomes), and mitigating factors (factors or diagnoses leading that affect outcomes in the setting of organ failure). The data extraction form will be adapted from the original PODIUM study. Studies published in languages other than English will have data extracted by a bilingual member of the study team.
Risk of bias in individual studies
The Quality in Prognosis Studies (QUIPS) (26) tool for prognostic factors studies will be used to assess risk of bias in the included studies. The following domains will be evaluated: study participation, study attrition, prognostic factor measurement, outcome measurement, potential confounding factors, and appropriateness of statistical analysis and reporting. Each of the 6 domains will be rated as having low, moderate, or high risk of bias. Two team members will independently assess the risk of bias, and any conflicts will be resolved by discussion or by a third member of the Working Group if consensus cannot be reached. The full QUIPS 6-domain questionnaire is provided in Supplementary 3.
Data synthesis and analysis
Data will be analyzed for each systematic review (11 organ-specific reviews and 1 MODS search) to synthesize information on risk factors and definitions of organ dysfunction associated with poor outcomes. Data synthesis will include [1] quantitative analysis of the number of participants/episodes and strength of the relationship between given risk factor/organ dysfunction definition and outcome, and [2] narrative synthesis to identify mitigating factors impacting outcomes with organ dysfunction in children with cancer. Given the anticipated heterogeneity in study design and analytic techniques, a formal meta-analysis is not planned, and formal subgroup analysis will not be possible. However, where the literature allows, we will explore differences across patient populations, countries, study settings, study languages, study designs, types of data collection (prospective vs. retrospective), data sources (chart review, prospective data collection, electronic medical record [EMR] query, or registry), participating sites (single-center vs. multicenter), age categories (neonates: 0–30 days; infants: 31 days to <1 year; children: 1 to <12 years; adolescents: 12 to <18 years; young adults: 18 to 21 years), reason for HCT (malignant, mixed malignant and non-malignant), and type of HCT or cellular therapy (autologous HCT, allogeneic HCT, or CAR-T). These subgroup considerations have been incorporated into our Case Report Form (CRF) (Supplementary 3).
To address discrepancies in the evidence base, as was done in the original PODIUM study, this narrative synthesis will inform a modified Delphi process during the consensus-building phase. This process will reconcile divergent findings and inform the development of the adapted PODIUM-Onc criteria. The Delphi process will be conducted in accordance with the Conducting and REporting DElphi Studies (CREDES) guidelines to ensure methodological rigor, transparency, and robust stakeholder engagement (27).
Anticipated results
Through these linked systematic reviews, we expect to identify characteristics of organ dysfunction associated with clinically important outcomes among children with cancer. Findings from these reviews will inform a planned expert modified consensus process to systematically adapt the existing PODIUM criteria for use in these unique and high-risk patients. Ultimately, this work will be used to standardize the identification and characterization of organ dysfunction in children with cancer in clinical care and research. This work will also establish a methodology for how to adapt PODIUM criteria for other populations. We anticipate that for some organ systems, this review will identify limited data on dysfunction criteria; this will serve to highlight critical gaps in the current literature and guide recommendations for future research efforts.
Discussion
Children with cancer are a unique patient population requiring unified, systematic, and tailored definitions for single and multiorgan dysfunction to allow for research and informed clinical care. The proposed study will address this need by synthesizing data needed to inform adaptation of the PODIUM organ failure criteria to accurately identify and further study organ dysfunction in this vulnerable patient population. Globally, approximately 43% of childhood cancer cases were undiagnosed, with substantial regional variation, ranging from 3% in high-income countries (HICs) to 57% in low- and middle-income countries (LMICs), highlighting both inequities in access to care and limitations in available data. The adapted PODIUM-Onc criteria aim to provide a framework applicable across settings to support equitable advances in pediatric oncology critical care, reduce disparities in outcome measurement, and improve survival worldwide (28).
Study strengths
This proposed study has several notable strengths. Our work leverages the methodology used to develop the original PODIUM criteria. The search strategy, data extraction, and bias assessment tools all build off the original study and are adapted to account for the unique pathophysiology, etiology, and outcomes of organ failure among children with cancer. Our study leadership team and Working Groups intentionally include investigators who contributed to the development of the original criteria.
In designing this study, we have also addressed some of the limitations of the original study. Our search strategy specifically focuses on terms unique to our target population, which were iteratively designed by our expert team. We will develop a comprehensive Data Set (Reference Manager), enabling full-text searches for organ failure terms—a necessary step given that much of the organ failure literature in children with cancer discusses MODS, rather than single-organ failure, and therefore would not be captured in a traditional search strategy. This review is planned as a one-time systematic review; however, the methodology has been designed to allow for straightforward updating in the future as new evidence becomes available. Furthermore, we will evaluate the applicability of the adapted PODIUM-Onc criteria to ensure that the resulting framework has a real-world impact and can meaningfully improve care for children with cancer.
Our diverse Working Group team intentionally includes investigators from a variety of specialties, disciplines, countries, and practice settings to provide comprehensive expertise on organ failure in this patient population. Importantly, the group also includes survivors of pediatric cancer, whose lived experiences bring valuable perspectives to the interpretation of findings and the development of organ dysfunction criteria relevant to this community.
We aim to comprehensively assess the global literature on organ dysfunction in pediatric cancer. To achieve this goal, we have not included any language filters in this search. Our global collaborative Working Group team includes investigators fluent in English, Spanish, Portuguese, German, Polish, Chinese, French, Turkish, Arabic, Russian, Italian, Dutch, Korean, and Urdu, among others. If a study is identified in a language not spoken by our primary study team, we will leverage the St. Jude Global Critical Care Program network of over 1300 clinicians from 80 countries to aid in screening and, if needed, data extraction. Through this approach, we are confident in our ability to rigorously evaluate all studies published on these topics in the current literature, regardless of language (29).
Additionally, we recognize this proposed work requires a large investigative team. As described, we have already assembled 104 collaborators (14 Core Team and 90 Working Group Members). More investigators will be invited as needed to ensure a comprehensive expert team to rigorously perform all systematic reviews.
Potential challenges and proposed solutions
While the field of pediatric onco-critical care has experienced significant growth over the past decade, the proposed approach may encounter some limitations. First, there may be limited literature available for certain organ systems in children with cancer and post-HCT, as well as in LMIC settings, which will likely be underrepresented in the review (30). This underrepresentation could limit the generalizability of our findings to global populations. In such cases, we will report available data and describe needed areas of future work.
Second, children receiving HCT for malignancy often undergo more intensive conditioning regimens, have prior exposure to chemotherapy or radiation, and face unique oncologic complications influencing both the risk and trajectory of organ dysfunction. While many organ toxicities following HCT can occur across both malignant and non-malignant indications, we have intentionally limited our population to children with malignancy, including those who received HCT or cellular therapy for cancer indications. This decision was made to reduce heterogeneity and ensure the clinical relevance of adapted criteria specifically for children with cancer. We recognize the overlap in toxicities between malignant and non-malignant HCT populations and acknowledge that the resulting definitions may not fully apply to children undergoing HCT for non-malignant diseases. Nevertheless, we hope the criteria developed through this work will serve as a foundation to inform future efforts to adapt organ dysfunction criteria tailored to the non-malignant HCT population.
Third, a formal meta-analysis is not planned due to the anticipated heterogeneity across eligible studies. This heterogeneity includes variation in study design (retrospective vs prospective, single- vs multicenter, registry-based vs institutional), differences in the definitions of organ dysfunction, inconsistent reporting of outcomes (mortality, ICU admission, length of stay, quality of life, etc.), variability in underlying patient populations (different malignancies, prior therapies, transplant timing, and comorbidities), and additional heterogeneity anticipated between studies conducted in low- and middle-income versus high-income countries due to differences in healthcare infrastructure, diagnostic practices, supportive care resources, and treatment protocols. Additionally, the evolving definitions of organ dysfunction and the changes in treatment practices over time might add to the complexity. Pooling such heterogeneous data would not yield valid or interpretable summary estimates. Instead, we will conduct a structured narrative synthesis to transparently summarize the range of definitions and risk factors reported, describe associations with outcomes, and highlight areas of convergence and divergence across studies.
Finally, there is a risk of publication bias, as studies with significant or positive findings are more likely to be published than those with negative or inconclusive results.
Conclusion
By systematically reviewing and analyzing organ-specific factors associated with patient outcomes, we aim to create consensus criteria that are clinically relevant for pediatric oncology patients and HCT patients to support future research in this vulnerable patient population.
Author contributions
MB: Data curation, Project administration, Writing – original draft, Writing – review & editing. SI: Data curation, Project administration, Visualization, Writing – review & editing. JWr: Data curation, Methodology, Software, Writing – review & editing. AAr: Funding acquisition, Writing – review & editing. RA: Funding acquisition, Writing – review & editing. KK: Data curation, Methodology, Software, Writing – review & editing. MMH: Funding acquisition, Writing – review & editing. CR: Funding acquisition, Writing – review & editing. AT: Funding acquisition, Writing – review & editing. JWo: Funding acquisition, Writing – review & editing. BO: Visualization, Project administration, Writing – review & editing. MRH: Conceptualization, Funding acquisition, Methodology, Supervision, Writing – original draft, Writing – review & editing. AAg: Conceptualization, Funding acquisition, Methodology, Supervision, Writing – original draft, Writing – review & editing.
Funding
The author(s) declare financial support was received for the research and/or publication of this article. Research effort to create this publication was supported by Developmental Funds from the St. Jude Comprehensive Childhood Cancer Center (5P30CA021765).
Conflict of interest
JWr maintains a full-time position with the Future of Privacy Forum, a Washington, DC-based, member-driven data privacy policy organization that includes members across the life sciences sector. JWr's research in meta-analytics and health sciences is conducted independently and is unaffiliated with her role at the Future of Privacy Forum. JWo has received in-kind support for investigator-initiated research from Scynexis Inc. and Karius Inc. (concluded). He has served as a co-investigator on a grant for investigator-initiated research funded by Pfizer Inc. (concluded). He is a paid author for UpToDate (ongoing) and receives funding from the National Institutes of Health for investigator-initiated research (ongoing). CR receives support from the NHLBI, grant K23HL150244.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The author(s) declared that they were an editorial board member of Frontiers, at the time of submission. This had no impact on the peer review process and the final decision.
Generative AI statement
The author(s) declare that no Generative AI was used in the creation of this manuscript.
Any alternative text (alt text) provided alongside figures in this article has been generated by Frontiers with the support of artificial intelligence and reasonable efforts have been made to ensure accuracy, including review by the authors wherever possible. If you identify any issues, please contact us.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fonc.2025.1591263/full#supplementary-material
References
1. Leclerc F, Leteurtre S, Duhamel A, Grandbastien B, Proulx F, Martinot A, et al. Cumulative influence of organ dysfunctions and septic state on mortality of critically ill children. Am J Respir Crit Care Med. (2005) 171:348–53. doi: 10.1164/rccm.200405-630OC
2. Typpo K, Watson RS, Bennett TD, Farris RW, Spaeder MC, and Petersen NJ. Outcomes of day 1 multiple organ dysfunction syndrome in the PICU. Pediatr Crit Care Med. (2019) 20:914–22. doi: 10.1097/PCC.0000000000002044
3. Bembea MM, Agus M, Akcan-Arikan A, Alexander P, Basu R, Bennett TD, et al. Pediatric organ dysfunction information update mandate (PODIUM) contemporary organ dysfunction criteria: executive summary. Pediatrics. (2022) 149:S1–S12. doi: 10.1542/peds.2021-052888B
4. Zinter MS, DuBois SG, Spicer A, Matthay K, and Sapru A. Pediatric cancer type predicts infection rate, need for critical care intervention, and mortality in the pediatric intensive care unit. Intensive Care Med. (2014) 40:1536–44. doi: 10.1007/s00134-014-3389-2
5. Soeteman M, Fiocco MF, Nijman J, Bollen CW, Marcelis MM, Kilsdonk E, et al. Prognostic factors for multi-organ dysfunction in pediatric oncology patients admitted to the pediatric intensive care unit. Front Oncol. (2023) 13:1192806. doi: 10.3389/fonc.2023.1192806
6. Caballero-Bellón M, Alonso-Saladrigues A, Bobillo-Perez S, Faura A, Arqués L, Rivera C, et al. Risk factors and outcome of chimeric antigen receptor T-cell patients admitted to pediatric intensive care unit: CART-PICU study. Front Immunol. (2023) 14:1219289. doi: 10.3389/fimmu.2023.1219289
7. Heneghan JA and Pollack MM. Morbidity: changing the outcome paradigm for pediatric critical care. Pediatr Clinics. (2017) 64:1147–65. doi: 10.1016/j.pcl.2017.06.011
8. Owens C, Mannion D, O’Marcaigh A, Waldron M, Butler K, and O’Meara A. Indications for admission, treatment and improved outcome of paediatric haematology/oncology patients admitted to a tertiary paediatric ICU. Ir J Med Sci. (2011) 180:85–9. doi: 10.1007/s11845-010-0634-8
9. Pechlaner A, Kropshofer G, Crazzolara R, Hetzer B, Pechlaner R, and Cortina G. Mortality of hemato-oncologic patients admitted to a pediatric intensive care unit: a single-center experience. Front Pediatrics. (2022) 10:795158. doi: 10.3389/fped.2022.795158
10. Sivan Y, Schwartz P, Schonfeld T, Cohen I, and Newth C. Outcome of oncology patients in the pediatric intensive care unit. Intensive Care Med. (1991) 17:11–5. doi: 10.1007/BF01708402
11. Wösten-van Asperen RM, Hines MR, Schlapbach LJ, and Agulnik A. Tailoring organ dysfunction criteria for critically ill children with cancer. Lancet Child Adolesc Health. (2025) 9(4):217–9. doi: 10.1016/S2352-4642(24)00305-5
12. Flerlage T, Fan K, Qin Y, Agulnik A, Arias AV, Cheng C, et al. Mortality risk factors in pediatric onco-critical care patients and machine learning derived early onco-critical care phenotypes in a retrospective cohort. Crit Care Explorations. (2023) 5:e0976. doi: 10.1097/CCE.0000000000000976
13. Rowan CM, McArthur J, Hsing DD, Gertz SJ, Smith LS, Loomis A, et al. Acute respiratory failure in pediatric hematopoietic cell transplantation: a multicenter study. Crit Care Med. (2018) 46:e967–e74. doi: 10.1097/CCM.0000000000003277
14. Lindell RB, Fitzgerald JC, Rowan CM, Flori HR, Di Nardo M, Napolitano N, et al. The use and duration of preintubation respiratory support is associated with increased mortality in immunocompromised children with acute respiratory failure. Crit Care Med. (2022) 50:1127–37. doi: 10.1097/CCM.0000000000005535
15. Rowan CM, Fitzgerald JC, Agulnik A, Zinter MS, Sharron MP, Slaven JE, et al. Risk factors for noninvasive ventilation failure in children post-hematopoietic cell transplant. Front Oncol. (2021) 11:653607. doi: 10.3389/fonc.2021.653607
16. Rubnitz Z, Sun Y, Agulnik A, Merritt P, Allison K, Ferrolino J, et al. Prediction of attributable mortality in pediatric patients with cancer admitted to the intensive care unit for suspected infection: A comprehensive evaluation of risk scores. Cancer Med. (2023) 12:21287–92. doi: 10.1002/cam4.6709
17. Schober S, Huber S, Braun N, Döring M, Lang P, Hofbeck M, et al. Prognostic factors and predictive scores for 6-months mortality of hematopoietic stem cell transplantation recipients admitted to the pediatric intensive care unit. Front Oncol. (2023) 13:1161573. doi: 10.3389/fonc.2023.1161573
18. Nguyen J, Thompson JM, Balcarcel DR, Alder MN, McKeone DJ, Halstead ES, et al. Immunocompromised children with acute respiratory distress syndrome possess a distinct circulating inflammatory profile. Crit Care Explorations. (2023) 5:e0844. doi: 10.1097/CCE.0000000000000844
19. Gaugler M, Swinger N, Rahrig AL, Skiles J, and Rowan CM. Multiple organ dysfunction and critically ill children with acute myeloid leukemia: Single-center retrospective cohort study. Pediatr Crit Care Med. (2023) 24:e170–e8. doi: 10.1097/PCC.0000000000003153
20. Vythoulkas D, Tsirigotis P, Griniezaki M, Konstantellos I, and Lazana I. Endothelial dysfunction syndromes after allogeneic stem cell transplantation. Cancers (Basel). (2023) 15:680. doi: 10.3390/cancers15030680
21. Ragoonanan D, Khazal SJ, Abdel-Azim H, McCall D, Cuglievan B, Tambaro FP, et al. Diagnosis, grading and management of toxicities from immunotherapies in children, adolescents and young adults with cancer. Nat Rev Clin Oncol. (2021) 18:435–53. doi: 10.1038/s41571-021-00474-4
22. Lee DW, Santomasso BD, Locke FL, Ghobadi A, Turtle CJ, Brudno JN, et al. ASTCT consensus grading for cytokine release syndrome and neurologic toxicity associated with immune effector cells. Biol Blood Marrow Transplant. (2019) 25:625–38. doi: 10.1016/j.bbmt.2018.12.758
23. Covidence. (2019). Melbourne, Australia: Covidence. Available online at: https://www.covidence.org/ (Accessed September 26, 2025).
24. Cochrane. Covidence: The Cochrane Collaboration. London, United Kingdom: Cochrane Training (2025). Available online at: https://training.cochrane.org/resource/tsc-induction-mentoring-training-guide/7-archie-and-revman/86-covidence (Accessed September 26, 2025).
25. Harris PA, Taylor R, Thielke R, Payne J, Gonzalez N, and Conde JG. Research electronic data capture (REDCap)—a metadata-driven methodology and workflow process for providing translational research informatics support. J BioMed Inform. (2009) 42:377–81. doi: 10.1016/j.jbi.2008.08.010
26. Hayden JA, van der Windt DA, Cartwright JL, Côté P, and Bombardier C. Assessing bias in studies of prognostic factors. Ann Intern Med. (2013) 158:280–6. doi: 10.7326/0003-4819-158-4-201302190-00009
27. Jünger S, Payne SA, Brine J, Radbruch L, and Brearley SG. Guidance on Conducting and REporting DElphi Studies (CREDES) in palliative care: Recommendations based on a methodological systematic review. Palliat Med. (2017) 31:684–706. doi: 10.1177/0269216317690685
28. Ward ZJ, Yeh JM, Bhakta N, Frazier AL, and Atun R. Estimating the total incidence of global childhood cancer: a simulation-based analysis. Lancet Oncol. (2019) 20:483–93. doi: 10.1016/S1470-2045(18)30909-4
29. Hospital SJCsR. The Global Critical Care Program strives to strengthen care for critically ill children with cancer everywhere (2025). Available online at: https://global.stjude.org/en-us/programs/transversal-programs/critical-care.html (Accessed September 26, 2025).
30. Gabela A, Wösten-van Asperen RM, Arias AV, Acuna C, Al Zebin Z, Lopez-Baron E, et al. The burden of pediatric critical illness among pediatric oncology patients in low-and middle-income countries: A systematic review and meta-analysis. Crit Rev Oncol Hematol. (2024) 203:104467. doi: 10.1016/j.critrevonc.2024.104467
Keywords: multiorgan dysfunction, pediatric oncology, hematopoietic (stem cell) transplant (HSCT), critical care, PICU (pediatric intensive care unit), systematic reviews, protocol paper
Citation: Bashir M, Islam S, Wrigley J, Arias A, Wösten-van Asperen RM, Kertis KK, Hudson MM, Rowan CM, Talleur AC, Wolf J, Oelkers B, Hines MR and Agulnik A (2025) Developing organ dysfunction diagnostic criteria for children with cancer and post-hematopoietic cell transplantation: protocol of systematic review. Front. Oncol. 15:1591263. doi: 10.3389/fonc.2025.1591263
Received: 10 March 2025; Accepted: 29 September 2025;
Published: 15 October 2025.
Edited by:
Jaume Mora, Sant Joan de Déu Hospital, SpainReviewed by:
Matteo Di Nardo, Bambino Gesù Children’s Hospital (IRCCS), ItalyIolanda Jordan, Sant Joan de Déu Hospital, Spain
Alberto Olaya Vargas, National Institute of Pediatrics, Mexico
Copyright © 2025 Bashir, Islam, Wrigley, Arias, Wösten-van Asperen, Kertis, Hudson, Rowan, Talleur, Wolf, Oelkers, Hines and Agulnik. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Melissa R. Hines, bWVsaXNzYS5oaW5lc0BzdGp1ZGUub3Jn
†Present address: Michael Bashir, Department of Internal Medicine, Mississippi Baptist Medical Center, Jackson, MS, United States
‡These authors have contributed equally to this work