 Erica C. Koch Hein1,2*
Erica C. Koch Hein1,2* Francisco Villanueva3Maysa Vilbert4Verónica Araya5Álvaro Abarzúa-Araya2,6Andrea Antúnez-Lay6,7Consuelo Cárdenas2,6Juan Camilo Castro2,6Francisco Dominguez2,8Katherine Droppelmann2,6Nicolás Droppelmann9Héctor Galindo1,2Augusto León2,8Jorge Madrid1,2Ximena Mimica10Montserrat Molgó2,6Sebastián Mondaca1,2Pablo H. Montero2,8Diego Romero7Pablo Uribe2,6Miguel A. Villaseca2,11Eugenio Vinés2,12Celeste Richardson13
Francisco Villanueva3Maysa Vilbert4Verónica Araya5Álvaro Abarzúa-Araya2,6Andrea Antúnez-Lay6,7Consuelo Cárdenas2,6Juan Camilo Castro2,6Francisco Dominguez2,8Katherine Droppelmann2,6Nicolás Droppelmann9Héctor Galindo1,2Augusto León2,8Jorge Madrid1,2Ximena Mimica10Montserrat Molgó2,6Sebastián Mondaca1,2Pablo H. Montero2,8Diego Romero7Pablo Uribe2,6Miguel A. Villaseca2,11Eugenio Vinés2,12Celeste Richardson13 Cristian Navarrete-Dechent2,6,14*
Cristian Navarrete-Dechent2,6,14*- 1Department of Hematology and Oncology, School of Medicine, Pontificia Universidad Católica de Chile, Santiago, Chile
- 2Red de Salud UC CHRISTUS, Santiago, Chile
- 3Department of Dermatology, Faculty of Medicine, Universidad de Chile, Santiago, Chile
- 4Massachusetts General Hospital Cancer Center, Division of Hematology/Oncology, Department of Medicine, Boston, MA, United States
- 5School of Nursing, Pontificia Universidad Católica de Chile, Santiago, Chile
- 6Department of Dermatology, School of Medicine, Pontificia Universidad Católica de Chile, Santiago, Chile
- 7Department of Surgery, Complejo Asistencial Dr. Sótero del Río, Santiago, Chile
- 8Department of Surgical Oncology, School of Medicine, Pontificia Universidad Católica de Chile, Santiago, Chile
- 9Department of Surgery, Clínica Universidad de Los Andes, Santiago, Chile
- 10Fundación Arturo López Pérez, Santiago, Chile
- 11Department of Pathology, School of Medicine, Pontificia Universidad Católica de Chile, Santiago, Chile
- 12Department of Radiation Oncology, School of Medicine, Pontificia Universidad Católica de Chile, Santiago, Chile
- 13Medical Affairs Novartis Chile S.A, Santiago, Chile
- 14Millennium Institute for Intelligent Healthcare Engineering, Santiago, Chile
Background: Melanoma incidence is rising globally, yet epidemiological data from Latin America remain limited. In low- and middle-income countries, such data are essential for shaping evidence-based public health strategies.
Objectives: To describe the demographic, clinical, and pathological characteristics of melanoma in Chile using a multi-institutional registry.
Methods: We conducted a multicenter observational cohort study including patients ≥18 years with histologically confirmed melanoma diagnosed between 2014 and 2022 at one public and one private tertiary center in Santiago. Demographic, clinical, pathological, molecular, and survival data for cutaneous melanoma were analyzed using descriptive and survival statistics.
Results: A total of 1,037 patients were included, of whom 979 (94.4%) had cutaneous melanoma. Among these patients, median age was 55 years and 54.8% were female. Cutaneous melanoma was more often diagnosed at early stages, particularly in the private setting. The most frequent histopathological subtypes were superficial spreading (31.6%), nodular (17.8%), and acral lentiginous melanoma (9.3%). Self-detection was the most common mode of identification (52.8%). Among patients with stage III–IV cutaneous melanoma tested for BRAF, 47.6% were positive. Higher risk of death was associated with advanced stage, nodular or amelanotic subtypes, BRAF-mutant tumors, male sex, and age ≥65 years. Only 34.8% of patients with stage IIB–IV cutaneous melanoma received systemic therapy.
Conclusion: This study offers the most comprehensive characterization of melanoma in Chile to date, underscoring survival disparities by clinical, pathological, and healthcare access factors. Findings highlight the urgent need to expand access to early detection, molecular testing, and systemic therapies.
1 Introduction
Cutaneous melanoma (henceforth, “melanoma” unless otherwise specified) is a skin cancer derived from the skin melanocytes (1). Ultraviolet radiation (UVR) leads to DNA damage and genetic alterations in oncogenes such as BRAF, NRAS, GNAQ, GNA11, c-kit, and subsequent hits in TERT, CDKN2A, and MITF, among others (2). Melanoma cases are increasing, representing about 5% of all new cancers diagnosed in the U.S. (3). Worldwide, in the year 2020, the International Agency for Research on Cancer (IARC) reported 325,000 new cases and 57,000 people died from melanoma (4, 5). In the U.S., the incidence rate of melanoma was 21 per 100,000 new cases, and the death rate was 2.1 per 100,000 people per year between 2016 and 2020, according to the Surveillance, Epidemiology, and End Results (SEER) Program (3). Among the Hispanic people living in the U.S., the rates of new cases and deaths were lower, up to 3.8 and 0.7 per 100,000 people in 2020, respectively (6).
National data on the epidemiological profile of melanoma patients are scarce in Latin American countries (7), with most published data coming from small series or cohort studies (8). Chile does not have a National Registry of Cancer, although there are five-population-based provincial registries (9). None of these operate in the Santiago Metropolitan Region, which constitutes nearly half of the country´s population, and only three of these registries are integrated into the International Association of Cancer Registries (IACR). The incidence of melanoma in Chile varies significantly by the geographic location of its five registries, with an estimated average of 2.4 to 3 cases per 100,000 inhabitants (10).
Chile has a hybrid health system, with public health care FONASA (Fondo Nacional de Salud, or National Health Fund) serving the 70% of the population, mostly patients with lower socioeconomic status (SES) (11). Private health care is provided by ISAPREs (Instituciones de Salud Previsional), and other private health insurance providers. Notably, patients with private insurance are almost always treated at private healthcare institutions, while those covered by the public system primarily receive care at public institutions or choose to access private care by covering additional out-of-pocket costs.
Epidemiological data is especially relevant in low-middle-income countries for planning and implementing evidence- and cost-based public health policies. Also, this information is critical for educating the population and increasing awareness, which may lead to increased adherence to preventive measures and early disease detection. Therefore, aiming to fill-in this information gap and contribute to the growing literature of Latin America, we built a melanoma multicentric register in Chile. In this study, melanoma cases were classified into three major anatomical categories: cutaneous, mucosal, and ocular (including uveal and conjunctival types), following common clinical and epidemiological practice (12). Here, we present the first epidemiological analysis of a large Chilean melanoma registry cohort, describing the demographic, clinical, and pathological characteristics of the cutaneous subtype, as well as survival according to stage at diagnosis, sex, age, histopathological subtype, and BRAF mutation status.
2 Patients and methods
The study was approved by the Research Ethic Boards (REBs) of both institutions: the Pontificia Universidad Católica de Chile REB (ID 190812004), and the Hospital Dr. Sótero del Río REB (approval granted via official letter dated September 12, 2019; no formal ID number was issued, but the letter is available upon request).
2.1 Study design and data collection
In this multi-center observational retrospective and prospective cohort study, we included all patients of the age 18 or older with histopathological diagnosis of melanoma evaluated at the participating centers. Patient data was retrospectively collected at the Red de Salud UC Christus (Tertiary Care Academic private network), and Hospital Dr. Sótero del Río (Tertiary Care Public Center serving to a population of approximately 1,650,000 inhabitants) (13) between January 2014 and November 2019, and prospectively between December 2019 and June 2022. While patients from the public network are generally referred to the Hospital Dr. Sótero del Río based on their residential address, the private centers receive spontaneous consultations, often from patients residing in various districts of Santiago or from other regions of the country. Due to this open referral and access model—particularly in the private sector—this cohort does not represent a geographically defined population, and we therefore did not attempt to estimate melanoma incidence rates in this study.
The electronic biopsy records from the Pathology Department and the skin cancer tumor board documentation from each center were queried by melanoma diagnosis to identify eligible patients. A total of 323 variables were collected from electronic medical records by investigators and a research nurse, including demographic data, clinicopathologic features, treatment history, and follow-up information. The complete list of variables is available as Supplementary Material. Patients were anonymized using a study number. Database quality assessments were performed by an independent investigator comparing entered data with the electronic medical record source. The data cut-off for survival analysis was September 2022.
Our primary objective was to evaluate the demographic, clinical and pathologic characteristics of Chilean patients with cutaneous melanoma. Secondary objectives, also limited to cutaneous melanoma, included: (1) assessment of overall survival (OS) according to stage at diagnosis, based on the 8th edition of the American Joint Committee on Cancer (AJCC) Staging System for cutaneous melanoma (14); (2) assessment of OS according to clinical and molecular variables, including age, sex, histopathological subtype, and BRAF mutation status; (3) exploration of the method of melanoma detection; and (4) description of the use of systemic therapies, including immunotherapy, targeted therapy, and chemotherapy.
Although the WHO Classification of Tumours does not group mucosal melanomas into a single volume, these entities were described across different organ-specific classifications according to their anatomical site, including the Head and Neck Tumours (15), Urinary and Male Genital Tumors (16), Female Genital Tumours (17), and Digestive System Tumours (18). Uveal and conjunctival melanomas are included in the Eye Tumours volume (19), while cutaneous melanomas are covered in the Skin Tumours volume (20). For the purposes of this registry-based analysis, we adopted a unified classification framework to facilitate meaningful comparisons across melanoma subtypes. The histopathologic subtype of cutaneous melanoma was reported according to the Protocol for the Examination of Biopsy Specimens from Patients with Invasive Melanoma of the Skin, Version 1.1.0.0, published by the College of American Pathologists (CAP) (2025) (21).
The method of melanoma detection was classified based on the context in which the primary lesion was identified. Self-detection referred to cases where patients noticed a suspicious lesion themselves and consulted a physician specifically for this concern. Incidental detection occurred during a non-dermatologic medical consultation, in which the lesion was not the main reason for the visit but was noticed and referred for further evaluation. Dermatology screening detection typically took place in the context of preventive care or routine skin checks. Finally, symptom-driven detection referred to cases where the diagnosis followed a consultation prompted by symptoms related to primary or metastatic disease—such as lymphadenopathy, pain, or systemic symptoms—that ultimately led to further work-up and melanoma diagnosis.
2.2 Statistical analysis
Given that this was a population-based registry, we included all patients, and no formal sample size calculation was performed. Demographic and clinical characteristics of the cohort were analyzed using descriptive statistics. Categorical variables were presented as counts and percentages. Continuous variables were reported as mean ± standard deviation (SD) or median with interquartile range (IQR). Chi-square, Fisher’s exact, and Mann-Whitney U tests were used to assess differences in categorical and continuous variables among subgroups of interest. OS was defined as the time from the diagnosis to death from any cause, with the date obtained from death certificates. OS was censored at the date of last follow-up. Survival curves were estimated using the Kaplan–Meier method, and differences between groups based on pathological stage, sex, age group, BRAF mutation status, and histopathological subtype were assessed using the log-rank test. Histopathologic subtypes that reached median OS were included in the survival analysis (superficial spreading, nodular, acral lentiginous, and amelanotic melanomas). Lentigo maligna melanoma and ‘other’ subtypes were not included in this analysis. The median follow-up was estimated using the reversed Kaplan–Meier method. A Cox proportional hazards model was performed to perform a multivariable regression analysis to assess the association between stage, age, sex, histopathological subtype and BRAF mutation with the risk of mortality. Hazard ratios were adjusted for age and sex. All statistical tests were two-sided, and p value <0.05 was deemed significant. We performed all the statistical analysis in RStudio Version 4.0.2 (R Foundation for Statistical Computing, Vienna, Austria).
3 Results
3.1 Patients
A total of 1,037 patients were identified and included in the study. Demographic patient characteristics are reported in Table 1. The median age of the population was 55 (IQR: 18-97) years. We found a slight female predominance (54.8% vs. 45.2%, respectively). About 7.1% of patients reported a family history of melanoma in first or second-degree relatives.
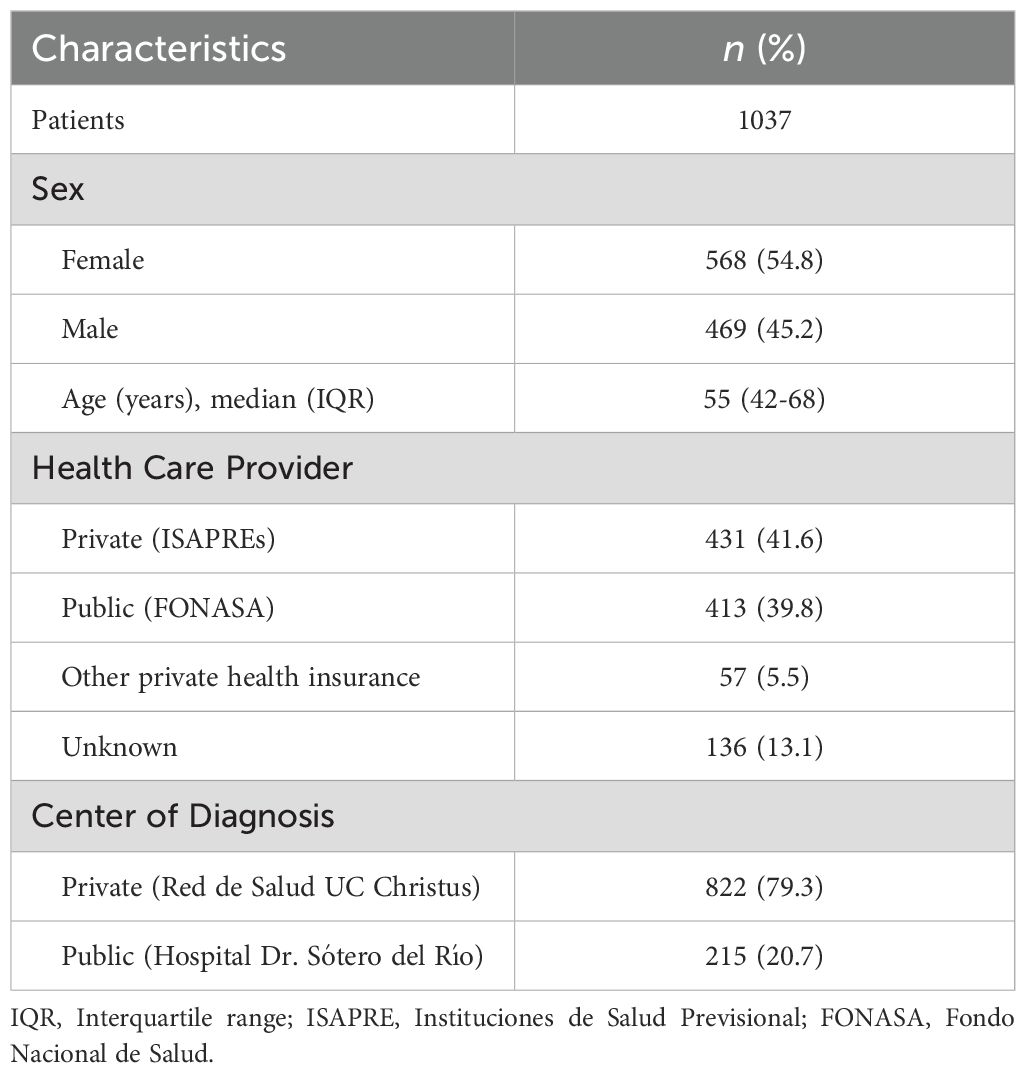
Table 1. Demographic characteristics of 1,037 patients diagnosed with melanoma.
3.2 Clinical and pathologic characteristics
Of the 1,037 patients included in the registry, the majority had cutaneous melanoma (n = 979, 94.4%), followed by mucosal (n = 29, 2.8%), ocular (n = 19, 1.8%), and unknown primary location (n = 10, 1.0%). Table 2 summarizes the clinical and pathological characteristics of patients with cutaneous melanoma.
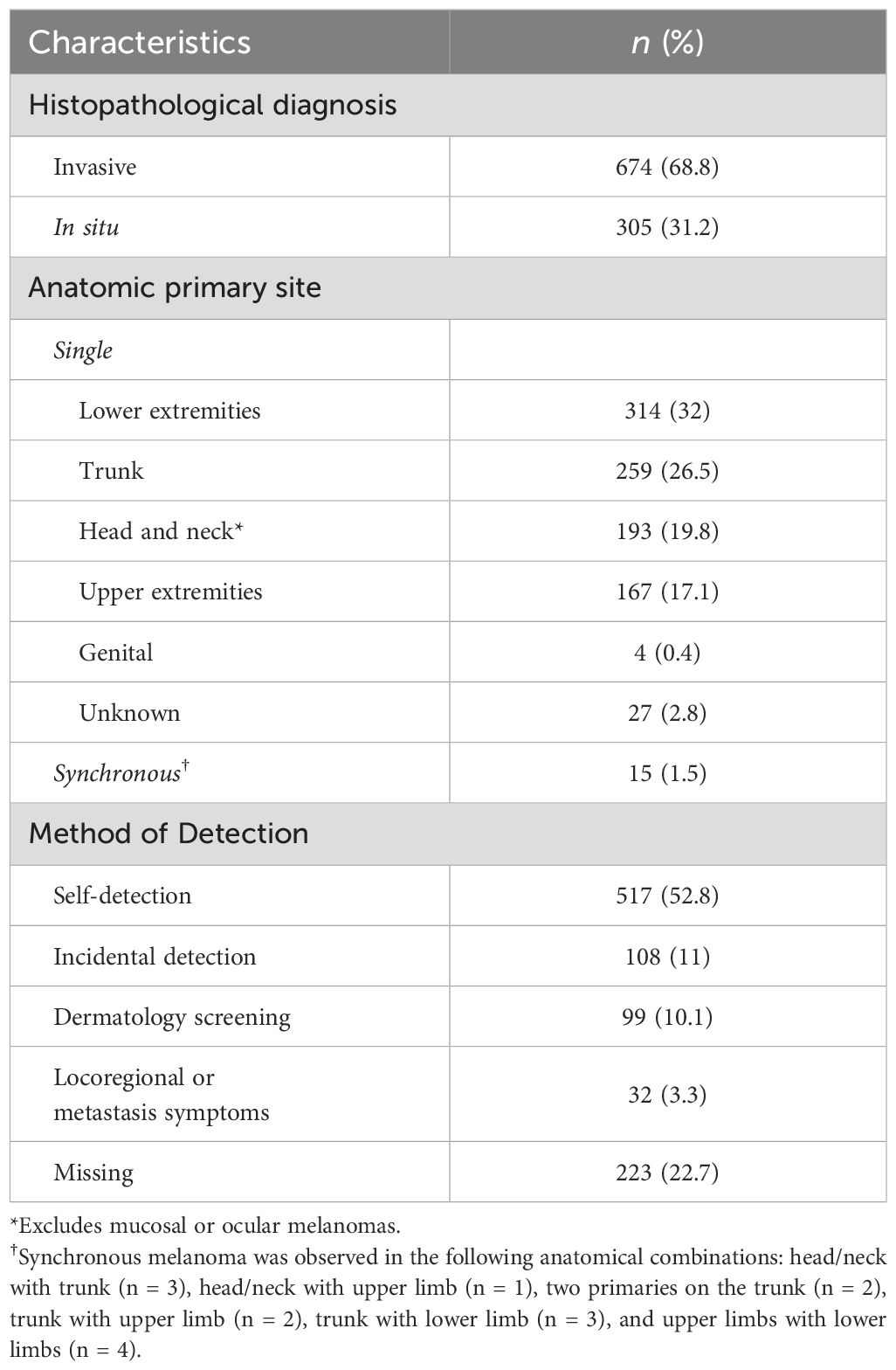
Table 2. Clinical and pathologic features of 979 patients diagnosed with cutaneous melanoma.
Melanoma in situ was diagnosed in 305 (31.2%) patients, and invasive melanoma in 674 (68.8%) patients. Among the female patients, 67.2% presented with invasive cutaneous melanoma, while the corresponding percentage for male patients was 70.9% (p = 0.22). Further stratification by age revealed that for individuals aged 65 and older, 70.9% presented with invasive cutaneous melanoma, similar as for those below 65 years, for whom the percentage was 68% (p = 0.37).
The predominant primary sites for cutaneous melanoma were the lower extremities (32%) and the trunk (26.5%). Among females, the lower extremities were the most common site of origin (38.9%), whereas in males, melanomas most often arose on the trunk (33.8%) (p < 0.001). In all, 52.8% (n=517) of patients had their cutaneous melanoma diagnosed through self-detection and 10.1% (n=99) of patients through formal screening during a dermatologist visit (Table 2). The percentage of cutaneous melanomas diagnosed through dermatology screening varied between private (16.6%) and public healthcare (3.6%) (p < 0.001).
Regarding invasive cutaneous melanoma (n = 674), the most prevalent histopathologic subtypes were superficial spreading (31.6%), nodular (17.8%), and acral lentiginous (9.3%) (Table 3). There were no statistically significant differences in the distribution of histopathologic subtypes by sex (p = 0.59) or by age group (≥65 vs. <65 years; p = 0.09).
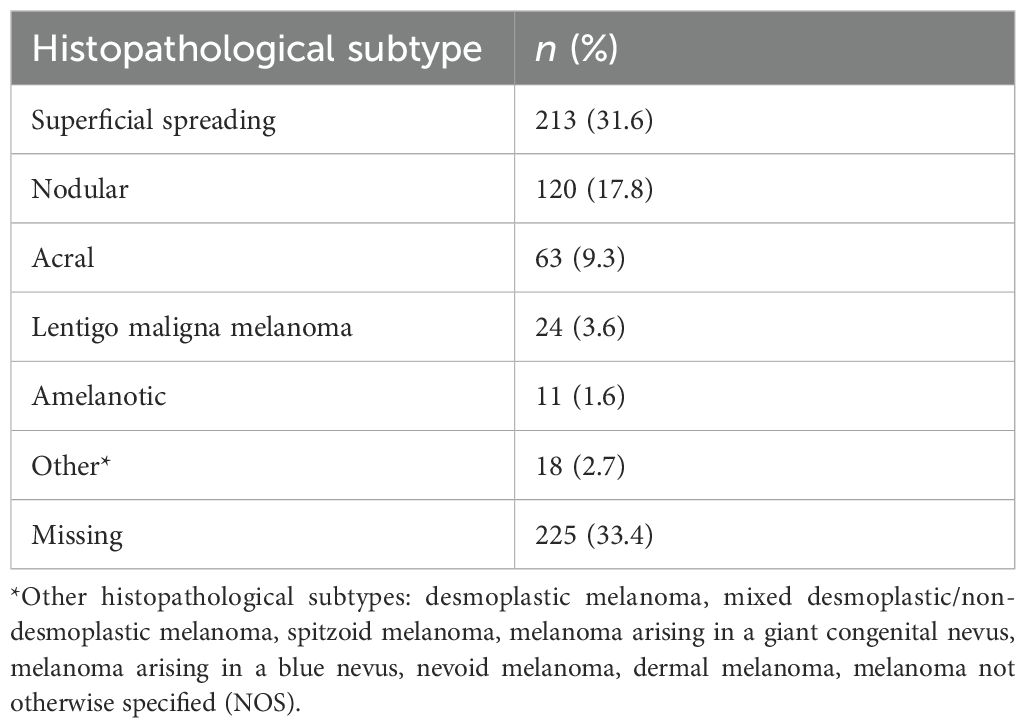
Table 3. Histopathological subtype for 674 invasive cutaneous melanomas according to CAP Protocol v1.1.0.0 (2025) (21).
Among the 29 patients with mucosal melanoma in our cohort, the most frequent primary sites were the gastrointestinal tract (n = 10) and the female genital tract (n = 9). Within the gastrointestinal group, tumors were located in the esophagus (n = 1), stomach (n = 1), anal canal (n = 2), and rectum (n = 5). Head and neck mucosal melanomas accounted for eight cases, including tumors in the nasal cavity and paranasal sinuses (n = 5), oral cavity (n = 2), and nasopharynx (n = 1). One patient had a primary tumor in the urinary tract, specifically the urethra. In two cases, the primary mucosal site of origin could not be determined from the available records and was therefore classified as unknown.
Of the 19 patients with ocular melanoma, 14 were classified as uveal, including 11 choroidal cases and three of unknown uveal subtype. Four patients had conjunctival melanoma. In one case, the specific ocular subtype (uveal or conjunctival) could not be determined and was recorded as unspecified.
3.2.1 Staging details at diagnosis for cutaneous melanoma
Among patients with cutaneous melanoma (N = 979), 62.1% were diagnosed at early stages (pathologic stage 0 or stage I). As shown in Table 4, melanoma was more frequently diagnosed as localized disease (in situ, stage I or II) for patients seen in the private healthcare institution (73.4%) compared with those diagnosed at the public institution (61.9%) (p < 0.001).
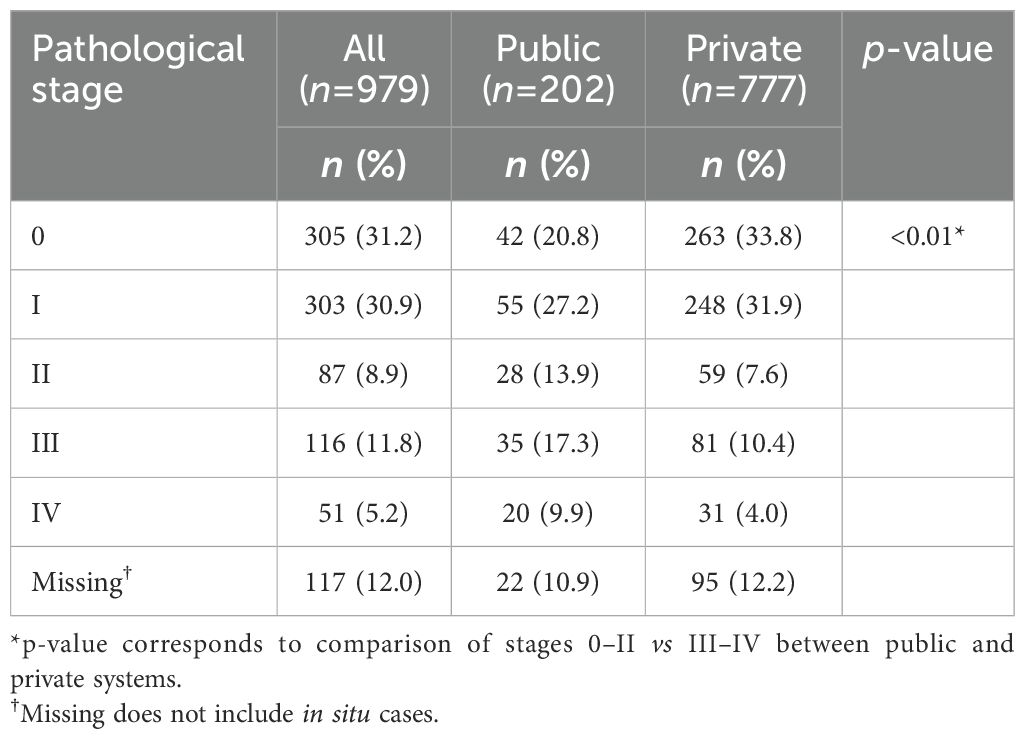
Table 4. Pathological stage of 979 patients with cutaneous melanoma at presentation, according to the AJCC 8th edition (14).
For the patients with cutaneous melanoma, 51 patients (5.2%) presented with distant metastasis at diagnosis. The most frequent sites of distant metastasis were the lung, non-regional lymph nodes and visceral other than lung, in 70.6%, 62.8% and 62.8%, respectively (Table 5).
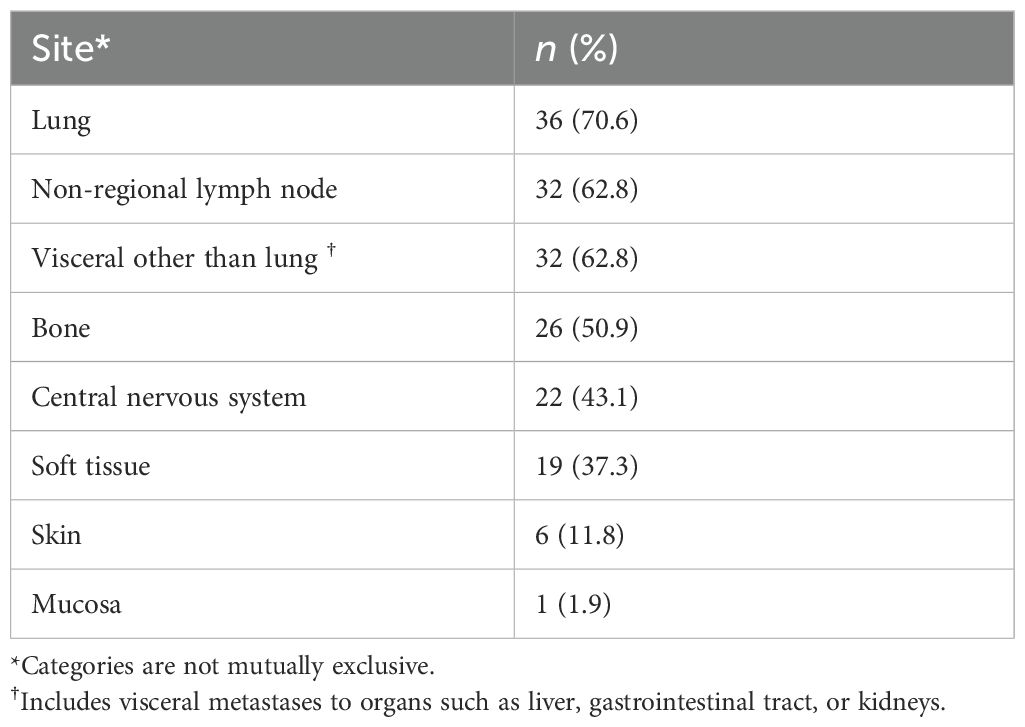
Table 5. Sites of distant metastasis at diagnosis in 51 patients with stage IV cutaneous melanoma.
3.2.2 Molecular analysis in patients with advanced cutaneous melanoma
BRAF mutation analysis was performed in 84 patients with stage III or IV cutaneous melanoma (Table 6). BRAF mutation was detected in 47.6% of the 84 patients with stage III or IV melanoma that underwent this molecular analysis. The demographic and clinical features of these patients harboring BRAF mutation are described in Table 7.
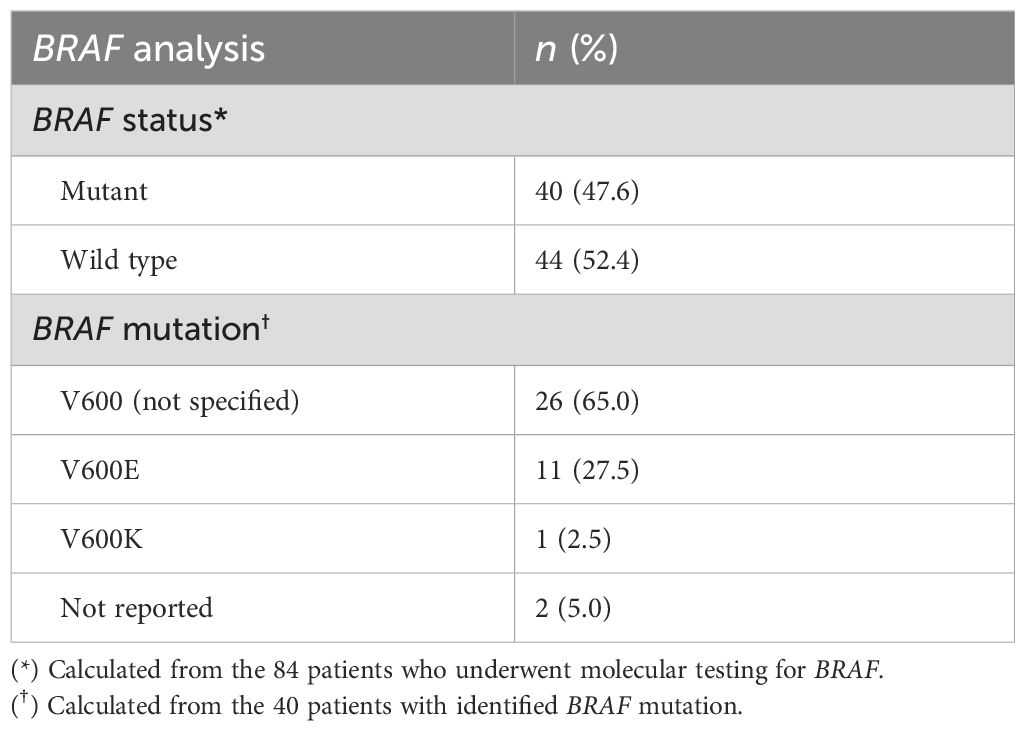
Table 6. BRAF analysis in 84 patients with stage III or IV cutaneous melanoma.
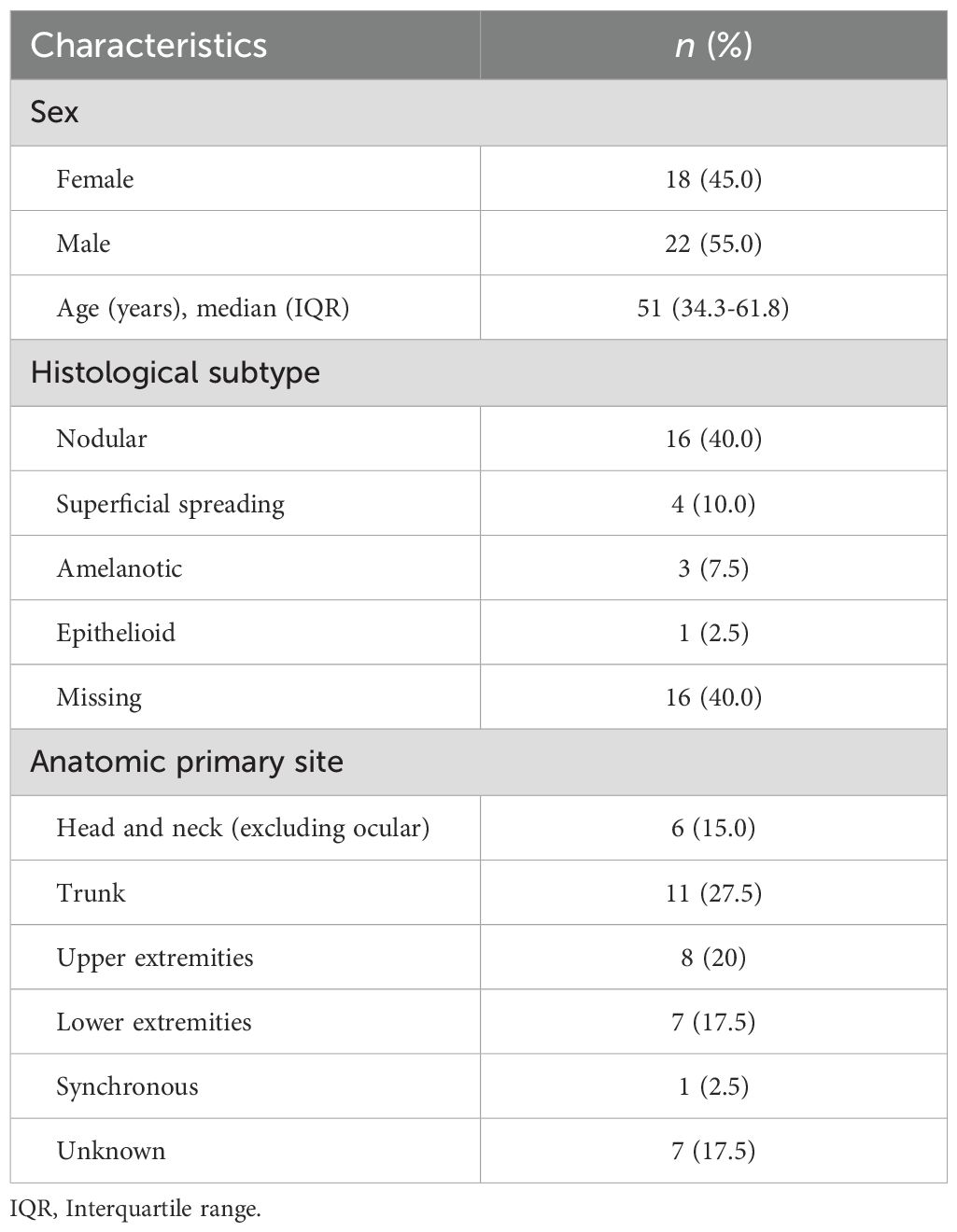
Table 7. Demographic and clinical features of 40 patients with stage III or IV cutaneous melanoma harboring BRAF mutation.
NRAS mutation analysis was tested in 25 patients with advanced melanoma; seven of them were positive for Q61X mutation. Only four patients with advanced melanoma were tested for KIT mutations, with one of them resulting positive for mutation E554K.
3.3 Treatment modalities used for invasive cutaneous melanoma
A total of 86.1% of the 674 patients underwent surgery with curative intent. Radiation therapy (RT) was administered to 65 patients (9.7% of the cohort); among them, 29 (44.6%) received RT as adjuvant treatment, 28 (43.1%) as palliative treatment, and eight (12.3%) as definitive therapy. Of the 221 patients with invasive cutaneous melanoma stage IIB or higher, only 77 (34.8%) received systemic therapy (Table 8).

Table 8. Systemic therapy in 77 patients with stage IIb or higher cutaneous melanoma.
Among these, 61% initiated treatment in the adjuvant setting. Most of them (97.9%) received immunotherapy, while one patient (2.1%) received targeted therapy. The majority of these adjuvant-treated patients (n = 41, 89%) had stage III disease. The remainder included one patient (2.2%) with completely resected stage IV disease, two patients (4.4%) with stage IIB, and one patient (2.2%) with stage IIC; staging data were missing for one patient. Of the 77 patients who received systemic therapy, 39% were treated for unresectable or metastatic disease. Among them, 80% received immunotherapy, 13.3% received targeted therapy, and 6.7% received chemotherapy. The one patient with missing immunotherapy details in the palliative setting was treated at another institution covered by their health insurance; while clinical notes confirmed immunotherapy was administered, they did not specify whether it was anti–PD-1 monotherapy or combined with anti–CTLA-4.
3.4 Survival for invasive cutaneous melanoma
Kaplan–Meier analysis revealed significant differences in overall survival (OS) according to pathological stage, sex, age group, and histopathological subtype, but not by BRAF mutation status (Figure 1). The median follow-up for the cohort was 31 months.
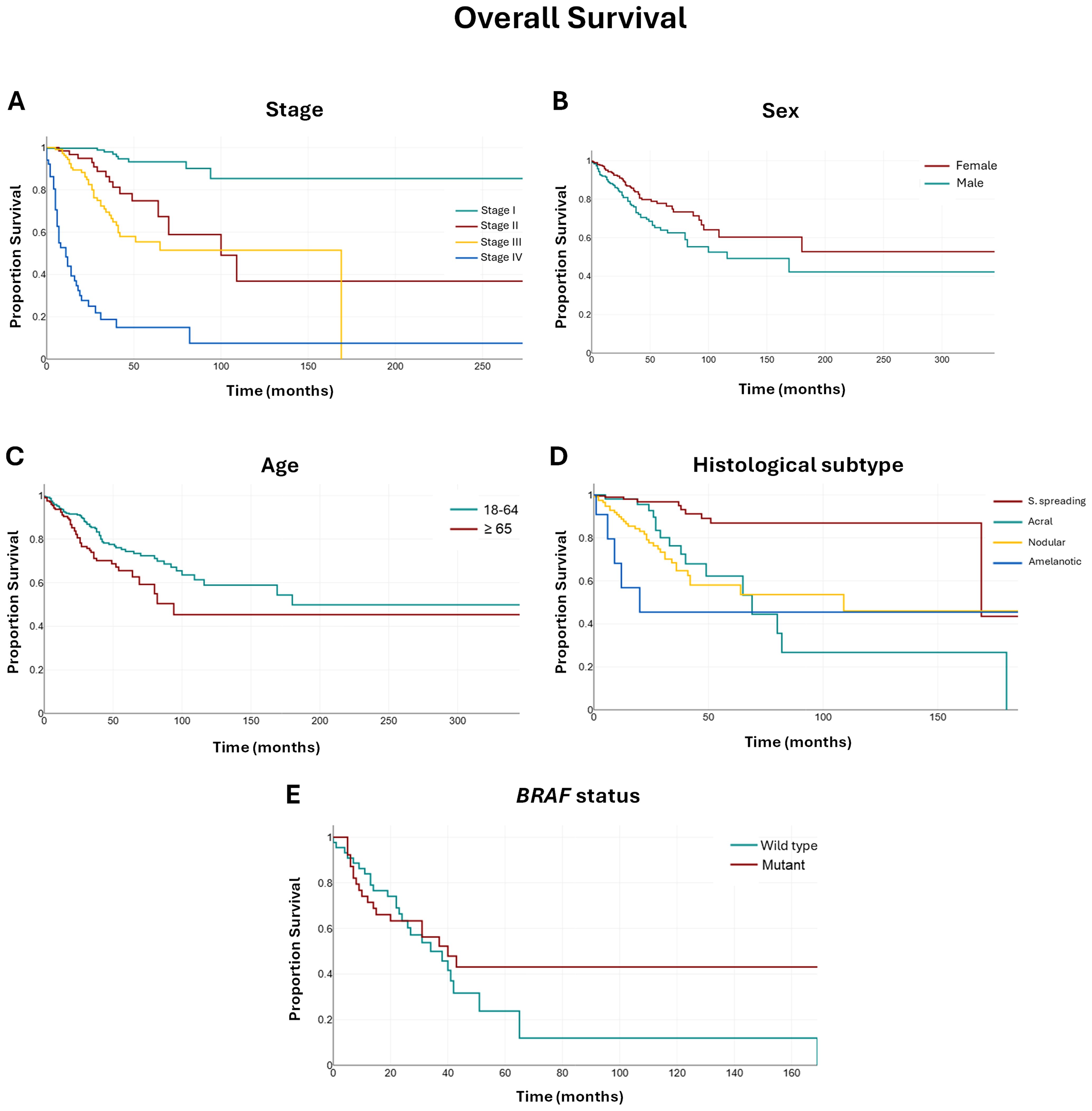
Figure 1. Kaplan–Meier survival curves (A–E) according to pathological stage, sex, age group, histopathological subtype, and BRAF mutation status in patients with invasive cutaneous melanoma. Abbreviations: S. spreading: superficial spreading melanoma. Note: Lentigo maligna melanoma and other subtypes were not included in this analysis.
Patients with stage I disease had the longest OS, with the median not reached during the observation period. In contrast, median OS declined with advancing stage: 100 months for stage II (95% CI: 64–109), 69 months for stage III (95% CI: 41–65), and 11 months for stage IV (95% CI: 6–16).
When stratified by sex, females had a longer median OS compared with males (median not reached vs. 116 months; 95% CI: 80–169). Similarly, patients aged 18–64 years showed a significantly longer median OS of 180 months (95% CI: 116–180) compared with 94 months (95% CI: 69–94) in those aged ≥65 years.
Regarding histopathological subtypes, patients with superficial spreading melanoma had the longest median OS at 169 months (95% CI: 169–169), followed by nodular melanoma (109 months; 95% CI: 42–109), acral lentiginous melanoma (69 months; 95% CI: 49–82), and amelanotic melanoma (20 months; 95% CI: 9–20).
The presence of a BRAF mutation was not associated with a statistically significant difference in OS: median OS was 40 months (95% CI: 20–43) for patients with BRAF-mutant tumors versus 34 months (95% CI: 24–41) for those with BRAF wild-type tumors.
In the multivariable Cox regression model, pathological stage remained the strongest predictor of all-cause mortality. Compared with patients with stage I disease, the adjusted hazard of death increased significantly in those with stage II, stage III, and was highest in stage IV (Table 9).
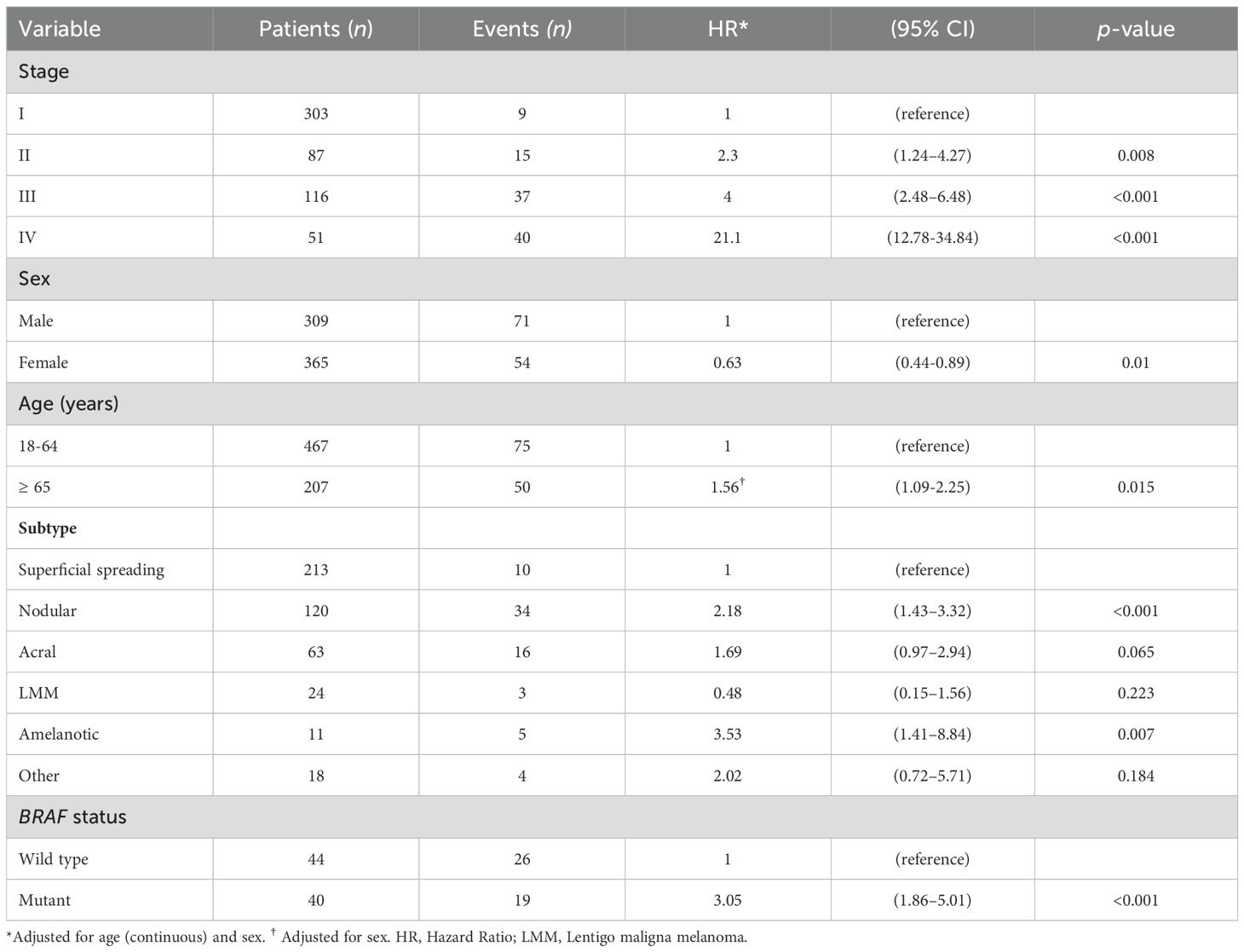
Table 9. Adjusted hazard ratios for all-cause mortality in patients with invasive cutaneous melanoma.
Female sex was independently associated with a lower risk of death compared to male sex, whereas age ≥65 years was linked to increased mortality. Regarding histopathological subtype, nodular melanoma conferred a significantly higher adjusted mortality risk relative to superficial spreading melanoma, and amelanotic melanoma was also associated with increased risk. No statistically significant differences were observed for acral lentiginous melanoma, lentigo maligna melanoma, or other melanoma subtypes (Table 9). Finally, the presence of a BRAF mutation was associated with a higher adjusted risk of death compared to wild-type cases (Table 9).
4 Discussion
In this large cohort of 1,037 melanoma patients from two tertiary care centers in Chile, we provide a comprehensive characterization of the clinical and pathological features of melanoma in a real-world Latin American setting. We identified several key findings: (1) most patients with cutaneous melanoma were diagnosed at an early stage, particularly in the private healthcare setting; (2) self-detection was the most common method of lesion identification; (3) superficial spreading melanoma was the most frequent histopathological subtype, followed by nodular and acral lentiginous melanoma; (4) overall survival and risk of death differed significantly across subgroups, with statistically worse outcomes among patients with advanced stage at diagnosis, nodular or amelanotic melanoma, older age, and male sex. Additionally, the presence of BRAF mutations was associated with an increased risk of mortality; and (5) a limited proportion of patients with advanced disease received systemic therapy.
The mean age at diagnosis around the sixth decade of life is similar to worldwide data (22), other registries from Latin America (23–26), and prior studies from Chile (27, 28). The female predominance observed in our cohort aligns with findings from other retrospective Chilean studies of patients with cutaneous malignant melanoma, where the proportion of female patients ranged from 60.6% to 64.9% (27–30). Similarly, two Brazilian studies reported that 56.3% to 58.8% of cutaneous melanoma cases occurred in women (31, 32). This pattern is also reflected in a Colombian population-based registry (60%) (26) and a Mexican study (58.5%) (25), whereas male predominance was reported in Argentinian, North American, and global datasets (5, 24, 33–35). In Europe, the incidence of cutaneous melanoma is also generally higher among women (36). These differences might be associated with biological, ethnic, occupational, and cultural elements that vary between female and male patients in distinct countries and cultures.
The distribution of primary tumor site in our cohort showed a statistically significant difference by sex, with melanomas more frequently located on the lower extremities in women and on the trunk in men (p<0.001). This anatomical distribution has been consistently reported in previous studies and is thought to reflect differences in patterns of sun exposure, clothing, and behavioral factors (22, 23, 37–42).
It is noteworthy that a substantial portion of cases, specifically 51.5%, of the diagnosed melanoma cases stemmed from patients’ self-awareness. This underscores the pivotal role of individual vigilance in early detection and emphasizes the critical need for widespread public education initiatives at different population levels (e.g. primary education, involvement of laypersons such as hairdressers and podiatrists, etc.). Similar results have been obtained in prior studies in which melanoma self-detection was the primary method of melanoma diagnosis, with 47%-57% of patients detecting their own melanoma (43–45). By enhancing the knowledge and awareness of melanoma signs and encouraging proactive self-examinations, we can potentially contribute to early detection, timely intervention, and improved outcomes. This emphasizes the significance of educational campaigns aimed at empowering the population to take an active role in their skin health. The markedly lower proportion of cutaneous melanomas diagnosed through dermatology screening in the public sector (3.6%) compared to the private sector (16.6%) (p < 0.001) highlights disparities in access to preventive care, consistent with previous studies reporting that individuals with higher socioeconomic status are more likely to seek dermatologist evaluations and present with earlier-stage disease (45–47). Additionally, 10.7% of melanoma cases were incidentally identified during medical visits originally scheduled for reasons unrelated to skin concerns. Although with a more controversial role, population-based screening by dermatologists, general physicians, or advanced medical providers might also have a critical role in the early detection of melanoma and potential reduction in mortality in selected patients (48, 49).
The higher prevalence of invasive melanoma compared to in situ cases may be attributed to the fact that patients with more advanced disease, requiring a multidisciplinary treatment approach, are often referred to our tertiary centers. Therefore, this might not reflect the true proportion of melanoma in situ vs. invasive cases in our country.
Similar to findings in Caucasian populations, we noted a predominance of the superficial spreading melanoma subtype, with nodular melanoma following as the second most frequent subtype (50). Interestingly, acral was the third most common histopathogical subtype. Higher proportion of acral subtype has been reported in other series among Hispanic White and Latino population (25, 51–53). A recent Mexican study including 1219 patients reported that 44% of their cases were acral melanoma (25). Furthermore, a strong relationship between the frequency of acral melanoma subtype and the percentage of people with mixed Spanish and Amerindian ancestry was described in a Peruvian cohort (54). Unfortunately, 34.2% of patients (N=230) in our cohort had no histopathological subtype information, often due to prior excisional biopsies performed externally, with pathology reports lacking subtype data.
As in other countries, significant differences in population and disease characteristics are observed in Chile regarding public and private healthcare systems, reflecting underlying socioeconomic disparities (7, 24, 46, 55–57). In our cohort, patients diagnosed in the public institution had significantly more advanced disease, with 26.7% presenting with stage III or IV melanoma compared to 14.4% in the private institution (p < 0.001). This is consistent with findings from one of the largest Chilean retrospective cohorts, which reported higher rates of invasive melanoma and Breslow thickness >1 mm among patients treated in the public setting (27). Moreover, the proportion of patients presenting with metastatic disease in the public setting (9.9%) in our cohort exceeded that reported in the U.S. SEER database (4%) (3, 58). Socioeconomic disparities have been consistently associated with later-stage melanoma diagnosis. Lower education levels are linked to decreased awareness and fewer skin examinations (59–62), and low SES remains an independent predictor of advanced disease even after adjusting for education (63). Limited access to dermatologic care in low-SES populations further contributes to diagnostic delays (64). In Chile, where the public healthcare system primarily serves lower-SES groups, these factors likely explain the higher burden of advanced and metastatic melanoma observed in that setting.
Consistent with international melanoma guidelines, the primary therapeutic approach in our cohort was surgery. A minority of patients underwent adjuvant systemic therapy. A relevant finding of our series was that nearly half of patients diagnosed with advanced cutaneous melanoma (stages III and IV) did not undergo BRAF testing. BRAF testing is considered the standard practice for determining the optimal systemic therapy approach in both adjuvant and metastatic scenarios, as outlined in established international guidelines (65, 66). Systemic therapy with immune checkpoint inhibitors or combined BRAF/MEK-targeted therapy is recommended by international guidelines for patients with resected stage IIB to IV melanoma, as well as for those with unresectable or metastatic disease (65, 66). However, in our cohort, only a minority of patients received these treatments. Among the 221 patients with stage IIB or higher melanoma, only 34.8% received systemic therapy—either as adjuvant treatment or as first-line therapy for advanced, unresectable, or metastatic disease. This highlights a significant gap between guideline-based standards of care and real-world clinical practice in our setting, likely driven by limited drug availability, delayed regulatory approvals, and coverage restrictions in the public healthcare system. In Chile, anti-PD-1 immune checkpoint inhibitors have only been available and reimbursed in the public healthcare institutions since 2019 for patients with melanoma in the adjuvant or metastatic setting. Other recommended therapies, such as anti-CTLA-4 antibodies (e.g., ipilimumab) and BRAF/MEK inhibitors, remain unavailable through the public health system.
In our cohort, BRAF mutations were identified in 47.6% of patients with stage III or IV cutaneous melanoma who underwent molecular testing, a frequency consistent with global estimates ranging from 40% to 60% (67–70). As in previous reports, the most frequent mutation detected was in codon V600 (68). However, due to test limitations, 65% of cases were reported only as “V600” without specifying the exact variant; among those with detailed results, V600E was the most common (27.5%), followed by V600K (2.5%), consistent with international data where V600E accounts for the majority of BRAF-mutated melanomas (68, 71). Patients harboring BRAF mutations were younger (median age 51 years), predominantly male, and most frequently were diagnosed with nodular melanoma subtype—a pattern that aligns with previous cohorts where nodular melanoma is commonly associated with BRAF mutations (68, 71). The trunk was the most frequent anatomical site in our series (27.5%), consistent with previous reports in BRAF-mutant melanoma where this location predominates over the extremities and head and neck (68, 71, 72). Notably, the presence of a BRAF mutation was not associated with a statistically significant difference in unadjusted overall survival. However, in multivariable analysis, BRAF mutation conferred a significantly increased risk of death (HR: 3.05; 95% CI: 1.86–5.01), echoing findings from historical pre-targeted therapy cohorts with median survival was eight to ten months (73). For instance, Long et al. reported a median OS of 11.1 months in untreated BRAF-mutant metastatic melanoma, compared with 46.1 months in BRAF wild-type patients (68). In our cohort, only four patients received BRAF/MEK inhibitors in the palliative setting, reinforcing the continued limitations in access to precision oncology. While our sample size was limited, this is, to our knowledge, the first Chilean study to report on BRAF mutation prevalence and clinical correlations in melanoma. As highlighted by Salman et al. in a recent regional review, molecular epidemiologic data on melanoma remain scarce in Latin America, with only a handful of small series from Argentina, Mexico, and Brazil reporting similar mutation frequencies (74). Our findings contribute to filling this knowledge gap and emphasize the need to expand access to molecular diagnostics and targeted therapies, particularly in public healthcare systems across the region.
4.1 Limitations
Limitations include the observational nature of the study, and the relatively short follow-up period. We did not centrally review all biopsies performed outside our institution, contributing to variability in pathology interpretation across different pathologists and to missing data. It is well known that interobserver concordance rates among pathologists are low for melanocytic lesions, including invasive melanomas (75).
As with many retrospective registry-based studies, some clinical variables were missing due to incomplete or inconsistent documentation in medical records. For example, skin characteristics such as Fitzpatrick skin type and the presence of multiple or atypical moles were not reported for most patients due to missing data.
In addition, insurance status was unknown in 136 patients, as this information is not automatically recorded in the electronic health records of the participating centers and relies on manual physician input. In 27 cases, the primary tumor location was undocumented, often because biopsies or diagnostic workups were performed at external institutions and original reports were unavailable. Data on the method of melanoma detection were missing in 223 cases, reflecting inconsistencies in the recording of clinical history. Furthermore, 225 patients had unknown histopathologic subtypes, typically due to inaccessible or insufficient pathology reports from external institutions. These limitations underscore the challenges of retrospective data collection in large multicenter cohorts.
5 Conclusions
This study provides an overview of melanoma at presentation and offers insights into its initial management across two markedly different healthcare settings in Chile. By establishing and maintaining a dedicated registry, we aim to generate essential data that can inform evidence-based policymaking and support a more strategic, targeted approach to addressing the evolving cancer landscape in the country.
This registry is envisioned to be an ongoing resource that can enhance our understanding, inform public health initiatives, and support advancements in melanoma care.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statement
The studies involving humans were approved by Pontificia Universidad Catolica de Chile and Hospital Dr. Sótero del Río. The studies were conducted in accordance with the local legislation and institutional requirements. Written informed consent for participation was not required from the participants or the participants’ legal guardians/next of kin in accordance with the national legislation and institutional requirements.
Author contributions
EK: Conceptualization, Data curation, Formal analysis, Funding acquisition, Investigation, Methodology, Project administration, Resources, Software, Supervision, Validation, Visualization, Writing – review & editing, Writing – original draft. FV: Formal analysis, Investigation, Methodology, Software, Writing – review & editing. MV: Investigation, Methodology, Software, Supervision, Writing – review & editing. VA: Investigation, Methodology, Software, Supervision, Writing – review & editing. ÁA-A: Conceptualization, Data curation, Investigation, Methodology, Software, Supervision, Validation, Writing – original draft, Writing – review & editing. AA-L: Data curation, Investigation, Methodology, Supervision, Validation, Writing – review & editing. CC: Data curation, Formal analysis, Investigation, Supervision, Writing – review & editing. JC: Formal analysis, Investigation, Methodology, Supervision, Writing – review & editing. FD: Conceptualization, Data curation, Investigation, Methodology, Supervision, Writing – review & editing. KD: Conceptualization, Data curation, Formal analysis, Funding acquisition, Investigation, Methodology, Project administration, Resources, Software, Supervision, Validation, Visualization, Writing – review & editing. ND: Data curation, Writing – original draft. HG: Conceptualization, Data curation, Formal analysis, Funding acquisition, Investigation, Methodology, Project administration, Supervision, Writing – original draft, Writing – review & editing. AL: Data curation, Formal analysis, Investigation, Methodology, Supervision, Writing – review & editing. JM: Formal analysis, Funding acquisition, Methodology, Project administration, Supervision, Writing – review & editing. XM: Investigation, Methodology, Supervision, Writing – review & editing. MM: Conceptualization, Data curation, Investigation, Methodology, Supervision, Writing – review & editing. SM: Data curation, Funding acquisition, Investigation, Methodology, Software, Supervision, Validation, Writing – review & editing. PM: Data curation, Investigation, Methodology, Supervision, Writing – review & editing. DR: Investigation, Methodology, Supervision, Writing – review & editing. PU: Conceptualization, Data curation, Formal analysis, Investigation, Methodology, Project administration, Software, Writing – review & editing. MAV: Data curation, Investigation, Methodology, Software, Supervision, Validation, Writing – review & editing. EV: Conceptualization, Data curation, Investigation, Methodology, Project administration, Writing – review & editing. CR: Writing – original draft, Funding acquisition. CN-D: Conceptualization, Data curation, Formal analysis, Funding acquisition, Investigation, Methodology, Project administration, Resources, Software, Supervision, Validation, Visualization, Writing – original draft, Writing – review & editing.
Funding
The author(s) declare financial support was received for the research and/or publication of this article. An International Grant was provided by Medical Affairs Novartis Chile SA in 2021 through the Institution Pontificia Universidad Católica de Chile.
Conflict of interest
Author CR was employed by Medical Affairs Novartis Chile SA. Author EK declares the following conflicts of interest: Honoraria: Bristol-Myers Squibb Chile; Speakers Bureau: MSD Oncology, Pfizer. Author CN-D declares the following conflicts of interest: Speakers Bureau, MSD Oncology.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The authors declare that this study received funding from Medical Affairs Novartis Chile SA. The funder was not involved in the study design, collection, analysis, interpretation of data, the writing of this article or the decision to submit it for publication.
Generative AI statement
The author(s) declare that no Generative AI was used in the creation of this manuscript.
Any alternative text (alt text) provided alongside figures in this article has been generated by Frontiers with the support of artificial intelligence and reasonable efforts have been made to ensure accuracy, including review by the authors wherever possible. If you identify any issues, please contact us.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fonc.2025.1604442/full#supplementary-material
References
1. Shain AH, Yeh I, Kovalyshyn I, Sriharan A, Talevich E, Gagnon A, et al. The genetic evolution of melanoma from precursor lesions. New Engl J Med. (2015) 373:1926–36. doi: 10.1056/nejmoa1502583
2. Langselius O, Rumgay H, de Vries E, Whiteman DC, Jemal A, Parkin DM, et al. Global burden of cutaneous melanoma incidence attributable to ultraviolet radiation in 2022. Int J Cancer. (2025) 157(6):1110-9. doi: 10.1002/ijc.35463
3. National Cancer Institute. Bethesda, M. Surveillance, epidemiology, and end results (SEER) program. In: Cancer stat facts: melanoma of the skin. Available online at: www.seer.cancer.gov.
4. Ferlay J, Colombet M, Soerjomataram I, Parkin DM, Piñeros M, Znaor A, et al. Cancer statistics for the year 2020: An overview. Int J Cancer. (2021) 149:778–89. doi: 10.1002/ijc.33588
5. Arnold M, Singh D, Laversanne M, Vignat J, Vaccarella S, Meheus F, et al. Global burden of cutaneous melanoma in 2020 and projections to 2040. JAMA Dermatol. (2022) 158:495. doi: 10.1001/jamadermatol.2022.0160
6. U.S. Department of Health and Human Services and C.f.D.C.a.P.a.N.C.I. U.S. Cancer Statistics Working Group. U.S. Cancer Statistics Data Visualizations Tool, based on 2022 submission data (1999-2020). Atlanta (GA): U.S. Department of Health and Human Services.
7. Sabatini-Ugarte N, Molgó M, and Vial G. Melanoma en Chile ¿Cuál es nuestra realidad? Rev Médica Clínica Las Condes. (2018) 29:468–76. doi: 10.1016/j.rmclc.2018.06.006
8. Schmerling RA, Loria D, Cinat G, Ramos WE, Cardona AF, Sánchez JL, et al. Cutaneous melanoma in Latin America: the need for more data. Rev Panamericana Salud Pública. (2011) 30:431–8. doi: 10.1590/s1020-49892011001100005
9. Cid C, Herrera C, Rodríguez R, Bastías G, and Jiménez J. Assessing the economic impact of cancer in Chile: a direct and indirect cost measurement based on 2009 registries. Medwave. (2016) 16:e6509. doi: 10.5867/medwave.2016.07.6509
10. Chile M. Primer informe de registros pobla- cionales de cancer de Chile. In: Quinquenio 2003-2007. p. 1–178.
11. Becerril-Montekio V, Reyes J, and Manuel A. The health system of Chile. Salud pública México. (2011) 53 Suppl 2:s132–143. Available online at: https://www.scielosp.org/pdf/spm/v53s2/09.pdf.
12. Keraliya AR, Krajewski KM, Braschi-Amirfarzan M, Tirumani SH, Shinagare AB, Jagannathan JP, et al. Extracutaneous melanomas: a primer for the radiologist. Insights Imaging. (2015) 6:707–17. doi: 10.1007/s13244-015-0427-8
13. Gattini C. Servicio de salud metropolitano sur oriente. In: Perfil institucional. OCHISAP (2015) Santiago, Chile.
14. Amin MB, Edge SB, Greene FL, Byrd DR, Brookland RK, Washington MK, et al. AJCC cancer staging manual Vol. 1024. Chicago (IL): Springer (2017).
15. Board, W.C.o.T.E. Head and neck tumours. 5th edition ed Vol. 9. . Lyon: International Agency for Research on Cancer (2024).
16. Board, W.C.o.T.E. Urinary and male genital tumours. 5th edition ed Vol. 8. . Lyon: International Agency for Research on Cancer (2022).
17. Board, W.C.o.T.E. Female genital tumours. 5th edition ed Vol. 4. . Lyon: International Agency for Research on Cancer (2020).
18. Board, W.C.o.T.E. Digestive system tumours. 5th edition ed Vol. 1. . Lyon: International Agency for Research on Cancer (2019).
19. Board, W.C.o.T.E. Eye tumours (Eye and orbit). 5th edition ed Vol. 13. . Lyon: International Agency for Research on Cancer (2023).
20. Board, W.C.o.T.E. Skin tumours. 5th edition ed Vol. 11. . Lyon: International Agency for Research on Cancer (2022).
21. College of American. P. Protocol for the examination of biopsy specimens from patients with invasive melanoma of the skin, version 1.1.0.0. Northfield, IL: College of American Pathologists (2025).
22. Erdei E and Torres SM. A new understanding in the epidemiology of melanoma. Expert Rev Anticancer Ther. (2010) 10:1811–23. doi: 10.1586/era.10.170
23. Vazquez Vde L, Silva TB, Vieira Mde A, de Oliveira AT, Lisboa MV, de Andrade DA, et al. Melanoma characteristics in Brazil: demographics, treatment, and survival analysis. BMC Res Notes. (2015) 8:4. doi: 10.1186/s13104-015-0972-8
24. Loria D, Abriata G, Santoro F, and Latorre C. Cutaneous melanoma in Argentina: an analysis of its characteristics and regional differences. ecancermedicalscience. (2020) 14:1017. doi: 10.3332/ecancer.2020.1017
25. Lino-Silva LS, Domínguez-Rodríguez JA, Aguilar-Romero JM, Martínez-Said H, Salcedo-Hernández RA, García-Pérez L, et al. Melanoma in Mexico: clinicopathologic features in a population with predominance of acral lentiginous subtype. Ann Surg Oncol. (2016) 23:4189–94. doi: 10.1245/s10434-016-5394-x
26. Oliveros H, Stavoli JU, Proaños NJ, Amador JR, and Reyes LF. Incidence and survival of patients with melanoma in Colombia. Cancer Epidemiol. (2025) 96:102784. doi: 10.1016/j.canep.2025.102784
27. Martínez G, Bobadilla F, Kinzel F, Fernández J, Sazunic I, Delgado MM, et al. Cutaneous Malignant melanoma in Chile: differences in tumor thickness and overall survival between patients from public and private health care centers. Dermatol Pract Conceptual. (2023):e2023273. doi: 10.5826/dpc.1304a273
28. Zemelman VB, Valenzuela CY, Sazunic I, and Araya I. Malignant melanoma in Chile: different site distribution between private and state patients. Biol Res. (2014) 47:1–5. doi: 10.1186/0717-6287-47-34
29. Bobadilla F, Sazunic I, Vega N, Fernández J, and Muñoz C. Análisis descriptivo de 561 biopsias con diagnóstico de melanoma entre los años 2006 y 2012 en un laboratorio de dermatopatología de la región metropolitana. Rev Chil Dermatol. (2014) 30:275–8. Available online at: https://www.scielosp.org/pdf/spm/v53s2/09.pdf.
30. Schwartz AR, Muñoz CO, Fantóbal AR, and Zemelman VD. Análisis de la correlación clínico-histopatológica de tumores cutáneos Malignos/Analysis of clinical and histopathological correlation in Malignant skin tumours. Rev Chil. Dermatol. (2006) 22:160–5. Available online at: https://www.sochiderm.org/web/revista/25_1/publication.pdf
31. Wainstein AJA, Duprat Neto JP, Enokihara MY, Brechtbühl ER, Riccardi F, Landman G, et al. Demographic, clinical, and pathologic features of patients with cutaneous melanoma: final analysis of the Brazilian melanoma group database. JCO Global Oncol. (2020), 575–82. doi: 10.1200/jgo.20.00005
32. Ferrari Júnior NM, Muller H, Ribeiro M, Maia M, and Sanches Júnior JA. Cutaneous melanoma: descriptive epidemiological study. Sao Paulo Med J. (2008) 126:41–7. doi: 10.1590/s1516-31802008000100008
33. Siegel RL, Miller KD, Wagle NS, and Jemal A. Cancer statistics, 2023. CA: A Cancer J Clin. (2023) 73:17–48. doi: 10.3322/caac.21763
34. Siegel RL, Miller KD, and Jemal A. Cancer statistics, 2016. . CA Cancer J Clin. (2016) 66:7–30. doi: 10.3322/caac.21332
35. Smith AJ, Lambert PC, and Rutherford MJ. Understanding the impact of sex and stage differences on melanoma cancer patient survival: a SEER-based study. Br J Cancer. (2021) 124:671–7. doi: 10.1038/s41416-020-01144-5
36. Arnold M, Holterhues C, Hollestein LM, Coebergh JW, Nijsten T, Pukkala E, et al. Trends in incidence and predictions of cutaneous melanoma across Europe up to 2015. . J Eur Acad Dermatol Venereol. (2014) 28:1170–8. doi: 10.1111/jdv.12236
37. Gillgren P, Brattström G, Frisell J, Persson JO, Ringborg U, and Hansson J. Effect of primary site on prognosis in patients with cutaneous Malignant melanoma. A study using a new model to analyse anatomical locations. Melanoma Res. (2005) 15:125–32. doi: 10.1097/00008390-200504000-00007
38. Chevalier V, Barbe C, Le Clainche A, Arnoult G, Bernard P, Hibon E, et al. Comparison of anatomical locations of cutaneous melanoma in men and women: a population-based study in France. Br J Dermatol. (2014) 171:595–601. doi: 10.1111/bjd.13052
39. Gordon D, Gillgren P, Eloranta S, Olsson H, Gordon M, Hansson J, et al. Time trends in incidence of cutaneous melanoma by detailed anatomical location and patterns of ultraviolet radiation exposure: a retrospective population-based study. . Melanoma Res. (2015) 25:348–56. doi: 10.1097/cmr.0000000000000170
40. Stanienda-Sokół K, Salwowska N, Sławińska M, Wicherska-Pawłowska K, Lorenc A, Wcisło-Dziadecka D, et al. Primary locations of Malignant melanoma lesions depending on patients’ Gender and age. Asian Pac J Cancer Prev. (2017) 18:3081–6. doi: 10.22034/apjcp.2017.18.11.3081
41. Clark LN, Shin DB, Troxel AB, Khan S, Sober AJ, and Ming ME. Association between the anatomic distribution of melanoma and sex. J Am Acad Dermatol. (2007) 56:768–73. doi: 10.1016/j.jaad.2006.12.028
42. de Vries E, Sierra M, Piñeros M, Loria D, and Forman D. The burden of cutaneous melanoma and status of preventive measures in Central and South America. Cancer Epidemiol. (2016) 44:S100–9. doi: 10.1016/j.canep.2016.02.005
43. Brady MS, Oliveria SA, Christos PJ, Berwick M, Coit DG, Katz J, et al. Patterns of detection in patients with cutaneous melanoma. Cancer. (2000) 89:342–7. doi: 10.1002/1097-0142(20000715)89:2<342::aid-cncr19>3.0.co;2-p
44. Watts CG, McLoughlin K, Goumas C, van Kemenade CH, Aitken JF, Soyer HP, et al. Association between melanoma detected during routine skin checks and mortality. . JAMA Dermatol. (2021) 157:1425–36. doi: 10.1001/jamadermatol.2021.3884
45. Melia J, Harland C, Moss S, Eiser JR, and Pendry L. Feasibility of targeted early detection for melanoma: a population-based screening study. Br J Cancer. (2000) 82:1605–9. doi: 10.1054/bjoc.2000.1183
46. Wich LG, Ma MW, Price LS, Sidash S, Berman RS, Pavlick AC, et al. Impact of socioeconomic status and sociodemographic factors on melanoma presentation among ethnic minorities. J Community Health. (2011) 36:461–8. doi: 10.1007/s10900-010-9328-4
47. Idorn LW and Wulf HC. Socioeconomic status and cutaneous Malignant melanoma in Northern Europe. Br J Dermatol. (2014) 170:787–93. doi: 10.1111/bjd.12800
48. Baltus H, Hübner J, Garbe C, Hagenström K, Rohr M, Hischke S, et al. Evaluation of skin cancer screening in Germany - a Microsimulation. . J Dtsch Dermatol Ges. (2025) 23:19–27. doi: 10.1111/ddg.15539
49. Mangione CM, Barry MJ, Nicholson WK, Chelmow D, Coker TR, Davis EM, et al. Screening for skin cancer: US preventive services task force recommendation statement. . JAMA. (2023) 329:1290–5. doi: 10.1001/jama.2023.4342
50. Druskovich C, Kelley J, Aubrey J, Palladino L, and Wright GP. A review of melanoma subtypes: genetic and treatment considerations. J Surg Oncol. (2025) 131:356–64. doi: 10.1002/jso.27953
51. Holman DM, King JB, White A, Singh SD, and Lichtenfeld JL. Acral lentiginous melanoma incidence by sex, race, ethnicity, and stage in the United States, 2010-2019. Prev Med. (2023) 175:107692. doi: 10.1016/j.ypmed.2023.107692
52. Huang K, Fan J, and Misra S. Acral lentiginous melanoma: incidence and survival in the United States, 2006-2015, an analysis of the SEER registry. J Surg Res. (2020) 251:329–39. doi: 10.1016/j.jss.2020.02.010
53. Avilés-Izquierdo JA, Longo-Imedio MI, and Lázaro-Ochaita P. Acral cutaneous melanoma in a Spanish Caucasian population. Melanoma Res. (2010). doi: 10.1097/CMR.0b013e3282f1d2b6
54. Carrera C and Puig-Butille JA. Clinical, epidemiological, and molecular heterogeneity in acral melanoma. J Invest Dermatol. (2018) 138:254–5. doi: 10.1016/j.jid.2017.09.027
55. Mandalà M, Imberti GL, Piazzalunga D, Belfiglio M, Lucisano G, Labianca R, et al. Association of socioeconomic status with Breslow thickness and disease-free and overall survival in stage I-II primary cutaneous melanoma. Mayo Clin Proc. (2011) 86:113–9. doi: 10.4065/mcp.2010.0671
56. MacKie RM and Hole DJ. Incidence and thickness of primary tumours and survival of patients with cutaneous Malignant melanoma in relation to socioeconomic status. BMJ: Br Med J. (1996) 312:1125–8. doi: 10.1136/bmj.312.7039.1125
57. Baumert J, Plewig G, Volkenandt M, and Schmid-Wendtner MH. Factors associated with a high tumour thickness in patients with melanoma. Br J Dermatol. (2007) 156:938–44. doi: 10.1111/j.1365-2133.2007.07805.x
58. Saginala K, Barsouk A, Aluru JS, Rawla P, and Barsouk A. Epidemiology of melanoma. Med Sci. (2021) 9:63. doi: 10.3390/medsci9040063
59. Strömberg U, Peterson S, Holmberg E, Holmén A, Persson B, Sandberg C, et al. Cutaneous Malignant melanoma show geographic and socioeconomic disparities in stage at diagnosis and excess mortality. Acta Oncol. (2016) 55:993–1000. doi: 10.3109/0284186x.2016.1144934
60. Eriksson H, Lyth J, Månsson-Brahme E, Frohm-Nilsson M, Ingvar C, Lindholm C, et al. Low level of education is associated with later stage at diagnosis and reduced survival in cutaneous Malignant melanoma: a nationwide population-based study in Sweden. Eur J Cancer. (2013) 49:2705–16. doi: 10.1016/j.ejca.2013.03.013
61. Youl PH, Baade PD, Parekh S, English D, Elwood M, and Aitken JF. Association between melanoma thickness, clinical skin examination and socioeconomic status: results of a large population-based study. Int J Cancer. (2011) 128:2158–65. doi: 10.1002/ijc.25540
62. Grange F, Barbe C, Aubin F, Lipsker D, Granel-Brocard F, Velten M, et al. Clinical and sociodemographic characteristics associated with thick melanomas. A population-based, case-case study in France. Arch Dermatol. (2012) 148:1370–6. doi: 10.1001/archdermatol.2012.2937
63. Salvaggio C, Han SW, Martires K, Robinson E, Madankumar R, Gumaste P, et al. Impact of socioeconomic status and ethnicity on melanoma presentation and recurrence in caucasian patients. Oncology. (2016) 90:79–87. doi: 10.1159/000441524
64. Jiang AJ, Rambhatla PV, and Eide MJ. Socioeconomic and lifestyle factors and melanoma: a systematic review. Br J Dermatol. (2015) 172:885–915. doi: 10.1111/bjd.13500
65. NCCN clinical practice guidelines in oncology (NCCN guidelines®) for guideline melanoma: cutaneous V.2.2024. Available online at: https://www.nccn.org/professionals/physician_gls/pdf/cutaneous_melanoma.pdf.
66. Michielin O, Van Akkooi ACJ, Ascierto PA, Dummer R, and Keilholz U. Cutaneous melanoma: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann Oncol. (2019) 30:1884–901. doi: 10.1093/annonc/mdz411
67. Vanni I, Tanda ET, Spagnolo F, Andreotti V, Bruno W, and Ghiorzo P. The current state of molecular testing in the BRAF-mutated melanoma landscape. Front Mol Biosci. (2020), 7-2020. doi: 10.3389/fmolb.2020.00113
68. Long GV, Menzies AM, Nagrial AM, Haydu LE, Hamilton AL, Mann GJ, et al. Prognostic and clinicopathologic associations of oncogenic BRAF in metastatic melanoma. J Clin Oncol. (2011) 29:1239–46. doi: 10.1200/jco.2010.32.4327
69. Davies H, Bignell GR, Cox C, Stephens P, Edkins S, Clegg S, et al. Mutations of the BRAF gene in human cancer. Nature. (2002) 417:949–54. doi: 10.1038/nature00766
70. Roa P, Bremer NV, Foglizzo V, and Cocco E. Mutations in the serine/threonine kinase BRAF: oncogenic drivers in solid tumors. Cancers. (2024) 16:1215. doi: 10.3390/cancers16061215
71. Menzies AM, Haydu LE, Visintin L, Carlino MS, Howle JR, Thompson JF, et al. Distinguishing clinicopathologic features of patients with V600E and V600K BRAF-mutant metastatic melanoma. Clin Cancer Res. (2012) 18:3242–9. doi: 10.1158/1078-0432.Ccr-12-0052
72. Bauer J, Büttner P, Murali R, Okamoto I, Kolaitis NA, Landi MT, et al. BRAF mutations in cutaneous melanoma are independently associated with age, anatomic site of the primary tumor, and the degree of solar elastosis at the primary tumor site. Pigment Cell Melanoma Res. (2011) 24:345–51. doi: 10.1111/j.1755-148x.2011.00837.x
73. Korn EL, Liu PY, Lee SJ, Chapman JA, Niedzwiecki D, Suman VJ, et al. Meta-analysis of phase II cooperative group trials in metastatic stage IV melanoma to determine progression-free and overall survival benchmarks for future phase II trials. J Clin Oncol. (2008) 26:527–34. doi: 10.1200/jco.2007.12.7837
74. Salman P, De Melo AC, Rico-Restrepo M, Rodriguez J, Russi A, Schmerling RA, et al. Addressing the unmet needs of patients with BRAF-mutated melanoma in Latin America: Expert perspective. . Front Oncol. (2023) 13:1032300. doi: 10.3389/fonc.2023.1032300
Keywords: melanoma, skin cancer, immunotherapy, diagnosis, survival, Latin America
Citation: Koch Hein EC, Villanueva F, Vilbert M, Araya V, Abarzúa-Araya Á, Antúnez-Lay A, Cárdenas C, Castro JC, Dominguez F, Droppelmann K, Droppelmann N, Galindo H, León A, Madrid J, Mimica X, Molgó M, Mondaca S, Montero PH, Romero D, Uribe P, Villaseca MA, Vinés E, Richardson C and Navarrete-Dechent C (2025) Melanoma in Chile: demographics and clinico-pathological features. Front. Oncol. 15:1604442. doi: 10.3389/fonc.2025.1604442
Received: 01 April 2025; Accepted: 31 July 2025;
Published: 09 September 2025.
Edited by:
Eric X. Wei, Stanford University, United StatesReviewed by:
Jessica Maldonado-Mendoza, Metropolitan Autonomous University, MexicoJulian A. Gajón, National Autonomous University of Mexico, Mexico
Gianfranco Manneschi, Istituto per lo Studio, la Prevenzione e la Rete Oncologica - ISPRO, Italy
Copyright © 2025 Koch Hein, Villanueva, Vilbert, Araya, Abarzúa-Araya, Antúnez-Lay, Cárdenas, Castro, Dominguez, Droppelmann, Droppelmann, Galindo, León, Madrid, Mimica, Molgó, Mondaca, Montero, Romero, Uribe, Villaseca, Vinés, Richardson and Navarrete-Dechent. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Erica C. Koch Hein, ZWtvY2hAdWMuY2w=; Cristian Navarrete-Dechent, Y3RuYXZhcnJAZ21haWwuY29t