 Jianyu Wu1†
Jianyu Wu1† Zhi Xiao2†
Zhi Xiao2† Weiming Liang1
Weiming Liang1 Xiaojian Wang1Xinyi Liang1Shan Yin1Yali Yang1Jieru Quan2
Xiaojian Wang1Xinyi Liang1Shan Yin1Yali Yang1Jieru Quan2 Zongyong Li3Chunge Hu1*Ping Wei5*
Zongyong Li3Chunge Hu1*Ping Wei5*- 1The First Affiliated Hospital of Guangxi University of Science and Technology, Guangxi University of Science and Technology, Liuzhou, Guangxi, China
- 2Department of General Surgery, Liuzhou Worker’s Hospital, Liuzhou, Guangxi, China
- 3School of Economics and Management, Guangxi University of Science and Technology, Liuzhou, Guangxi, China
- 4The Second Affiliated Hospital of Guangxi University of Science and Technology, Guangxi University of Science and Technology, Liuzhou, Guangxi, China
- 5Department of General Surgery, Rongshui Miao Autonomous County People's Hospital, Liuzhou, Guangxi, China
Introduction: This meta-analysis was designed to compare the outcomes of transoral endoscopic thyroidectomy vestibular approach (TOETVA) versus endoscopic thyroidectomy via the areola approach (ETAA) for thyroid carcinoma.
Materials and methods: Five databases (PubMed, Embase, Web of Science, Cochrane Library, and Scopus) were systematically searched for studies comparing endoscopic thyroidectomy via TOETVA versus ETAA in patients with thyroid carcinoma. The search was conducted from the databases’ establishment to May 31, 2025. Operative time, intraoperative blood loss, number of central lymph node dissections, postoperative drainage volume, length of hospital stay, postoperative infection, hypoparathyroidism, perioperative recurrent laryngeal nerve injury, complication, hypocalcemia, subcutaneous ecchymosis, cough, trachyphonia, postoperative parathyroid hormone (PTH), postoperative blood calcium, pain score of Visual Analogue Scale (VAS), swallowing discomfort, hematoma, central lymph node dissection time, and satisfaction with cosmetic effects were subjected to meta-analyses.
Results: A total of 15 studies were included in the meta-analysis. The meta-analysis included a group of 1,961 patients diagnosed with thyroid carcinoma. Within this cohort, 777 patients underwent endoscopic thyroidectomy via TOETVA, while 1,184 patients underwent endoscopic thyroidectomy via ETAA. Compared with ETAA, TOETVA yielded lower intraoperative bleeding volume [weighted mean difference (WMD = −1 mL, 95% confidence interval (CI): −3 to 0, p = 0.03], higher number of central lymph node dissections (WMD = 1.4, 95% CI: 0.3 to 2.3, p = 0.02), and higher satisfaction with cosmetic effects of the patients (WMD = 0.93, 95% CI: 0.42 to 1.43, p = 0.0004), but longer operative time (WMD = 17 min, 95% CI: 8 to 26, p = 0.0002). There was no statistically significant difference between the two groups regarding postoperative drainage volume (WMD = −6 mL, 95% CI: −17 to 5, p = 0.31), postoperative infection [odds ratio (OR) = 1.43, 95% CI: 0.47 to 4.43, p = 0.53], perioperative recurrent laryngeal nerve injury (OR = 0.62, 95% CI: 0.30 to 1.28, p = 0.20), hypocalcemia (OR = 0.88, 95% CI: 0.40 to 1.91, p = 0.74), swallowing discomfort (OR = 0.83, 95% CI: 0.24 to 2.95, p = 0.78), hypoparathyroidism (OR = 0.47, 95% CI: 0.18 to 1.18, p = 0.11), and hospitalization time (WMD = 0.03 days, 95% CI: −0.13 to 0.19, p = 0.71).
Conclusions: The findings indicated that both TOETVA and ETAA demonstrated safe and reliable clinical efficacy. TOETVA offers additional benefits concerning satisfaction with cosmetic effects and central lymph node dissection. TOETVA is an optimal option for patients seeking scarless surgical procedures.
Systematic review registration: https://www.crd.york.ac.uk/prospero/, identifier CRD420251021663.
1 Introduction
Thyroid cancer represents the most rapidly increasing malignancy among endocrine tumors across the globe (1). The disease predominantly affects women, with papillary thyroid carcinoma being the most common subtype (2, 3). Due to the generally good prognosis associated with thyroid cancers, early detection and effective surgical intervention are critical components of management (4). Traditional surgical approaches, such as open thyroidectomy, had long been the standard treatment modality (5). Open thyroidectomy (OT), the conventional approach for thyroid neoplasms, is associated with notable drawbacks, including a visible neck scar and postoperative swallowing discomfort. A prominent scar, often a cosmetic concern, particularly for female patients, can impact quality of life (6). Additionally, a meta-analysis comparing endoscopic and open thyroidectomy revealed that OT is associated with significantly higher rates of swallowing discomfort compared to minimally invasive approaches (7). These limitations highlight the need for alternative techniques balancing efficacy and patient satisfaction. However, surgical innovation continues to evolve, offering patients less invasive options aimed at reducing postoperative morbidity and improving cosmetic outcomes (8). Advances in endoscopic thyroidectomy have introduced significant improvements to these traditional methods. Techniques such as endoscopic surgery offer comparable safety and feasibility to open surgery while minimizing the undesirable outcomes associated with larger incisions. Endoscopic approaches reduce postoperative pain, decrease recovery times, and are associated with lower rates of surgical complications, thus enhancing the overall patient experience (9).
In China, the most widely used scarless techniques are transoral endoscopic thyroidectomy vestibular approach (TOETVA) and endoscopic thyroidectomy via the areola approach (ETAA) (10). ETAA involves making incisions in the areola area to access the thyroid gland. This method facilitates excellent visualization and access to the surgical site while potentially preserving vital anatomical structures (11). However, its drawbacks include a higher risk of postoperative complications, such as infection and hematoma formation. Despite these concerns, endoscopic thyroidectomy via the areola approach remains a viable option, particularly for patients with anatomical constraints that limit other approaches (12, 13). Endoscopic thyroidectomy via the areola approach utilizes the natural pigmentation of the areolar tissue to disguise surgical scars. Although not entirely scarless, it presents a viable aesthetic option by making scars less conspicuous (14).
Contrastingly, TOETVA provides another alternative for endoscopic thyroidectomy. TOETVA is a scarless endoscopic procedure conducted through the oral vestibule, enabling surgeons to access the thyroid gland without external incisions in the neck (15). This approach offers significant cosmetic advantages, particularly for patients who are concerned about visible scarring (16). TOETVA utilizes natural orifices to achieve truly scarless surgery, placing it at the forefront of cosmetic surgical advancements (17, 18). This method not only achieves the desired cosmetic outcome but also avoids visible scarring altogether, significantly boosting patient satisfaction (19, 20).
Controversy remains regarding the effectiveness and safety of TOETVA in thyroid cancer. Given the growing use of TOETVA, understanding its efficacy and safety profile is critical. A previous meta-analysis comparing TOETVA with conventional OT revealed no significant differences in postoperative outcomes between the two groups (21, 22). Another previous meta-analysis contrasting ETAA with OT demonstrated that ETAA is associated with a prolonged operative duration, increased postoperative drainage volume, and diminished intraoperative bleeding volume; however, no significant differences were observed between the two groups regarding postoperative hospital stay length, lymph node excision count, and surgical complications (21, 22). Furthermore, Tengjiang Long et al. performed a network meta-analysis evaluating various endoscopic surgical techniques, including TOETVA, ETAA, endoscopic gasless transaxillary approach (EGAA), minimally invasive video-assisted approach (MIVAA), and endoscopic bilateral axillo-breast approach (EBABA), in comparison to OT (23). However, there are no meta-analyses comparing TOETVA versus ETAA directly. Our study is the first meta-analysis designed to compare the outcomes of endoscopic thyroidectomy via TOETVA versus ETAA in the treatment of thyroid carcinoma, which would provide clearer insights into the effectiveness and safety of TOETVA versus ETAA for thyroid carcinoma and inform clinical decision-making.
2 Materials and methods
2.1 Search strategy
The present meta-analysis was conducted according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) 2020 guidelines. This study was registered at PROSPERO with registration number PROSPERO(CRD420251021663). Five databases, including PubMed, Embase, Web of Science, Cochrane Library, and Scopus, were systematically searched for literature published up to May 31, 2025, using the following search strategy: “thyroid cancer” AND “transoral endoscopic thyroidectomy vestibular approach” AND “endoscopic thyroidectomy via the areola approach”. Furthermore, a comprehensive manual evaluation of the bibliographies of the identified papers, together with relevant reviews and meta-analyses, was performed to identify any new research that satisfied the inclusion criteria. Supplementary Material 1 presents the search records in detail.
2.2 Inclusion and exclusion criteria
Inclusion criteria were as follows: 1) patients were diagnosed with thyroid cancer, with no age restrictions. 2) Patients in the intervention group underwent endoscopic thyroidectomy via transoral endoscopic thyroidectomy vestibular approach. 3) Patients in the control group underwent endoscopic thyroidectomy via the areola approach. 4) At least one of the following outcomes was reported: surgical time, intraoperative blood loss, number of central lymph node dissections, postoperative drainage volume, length of hospital stay, or satisfaction with cosmetic effects. 5) Study designs were randomized controlled studies, prospective cohort studies, or retrospective cohort studies.
Exclusion criteria were as follows: 1) other types of articles, such as case reports, abstracts, publications, letters, reviews, meta-analyses, editorials, animal studies, and protocols; 2) not relevant; 3) other diseases, such as thyroid nodule or benign thyroid tumor; 4) failed to obtain full text due to inaccessibility of the article; 5) reduplicated cohort of patients; and 6) failed to extract data. There was no language restriction.
2.3 Selection of studies
Selection of studies, including elimination of duplicates, was undertaken using EndNote (Version 20; Clarivate Analytics, Philadelphia, United States). An initial search was undertaken by two reviewers (J.W. and W.L.) who independently deleted duplicate entries, assessed the titles and abstracts for relevance, and classified each study as either included or excluded. Any discrepancies were settled by consensus and arbitrated by a third reviewer (Z.L.).
2.4 Data extraction
Two independent reviewers (J.W. and W.L.) screened the titles and abstracts and subsequently reviewed the full texts. Discrepancies were resolved through consultation with a third reviewer (Z.L.). Data retrieved included the first author’s name, publication year, trial ID, study design, sample size, intervention details, male-to-female ratio, patient age, surgical time, intraoperative blood loss, number of central lymph node dissections, postoperative drainage volume, hospitalization duration, postoperative infection rates, hypoparathyroidism, satisfaction with cosmetic effects, hypocalcemia, swallowing discomfort, and perioperative recurrent laryngeal nerve injury. Hypoparathyroidism was defined as normal parathyroid function confirmed before endoscopic thyroidectomy, followed postoperatively by low parathyroid hormone (PTH) levels in peripheral venous blood tests (24).
2.5 Risk of bias assessment
The risk of bias was assessed by two independent reviewers (J.W. and W.L.). Discrepancies were resolved through consultation with a third reviewer (Z.L.). The Newcastle–Ottawa Scale (NOS) (25) was utilized to assess the quality of cohort studies. The NOS included three domains: 1) selection of the cohort (four items), including representativeness of the case/exposure group (1 point), selection of the non-case/non-exposure group (1 point), definition of exposure (1 point), and no relevant outcome at the start of the study (1 point); 2) comparability (two items), including comparability on most important factors (up to 2 points) and comparability on other risk factors (1 point); and 3) outcome determination (three items), including outcome assessment (1 point), adequacy of follow-up time (1 point), and follow-up completeness (1 point). Studies with scores ≥7 were classified as high quality. Randomized controlled trials (RCTs) were evaluated using the Jadad scale (26), which encompasses three domains: 1) randomization, 2) blinding, and 3) withdrawals and dropouts. A score ranging from 1 to 3 on this scale was classified as indicative of low quality, whereas a score between 4 and 7 signifies high quality.
2.6 Statistical analysis
The selection and duplicate removal of included studies were conducted using EndNote (Version 20; Clarivate Analytics). The statistical analysis was performed using Review Manager 5.3, a software developed by the Cochrane Collaboration in Oxford, UK. The continuous variables were compared using the weighted mean difference (WMD) and a 95% confidence interval (CI). The odds ratio (OR) was used to compare binary variables, along with a 95% CI. The medians and interquartile ranges of continuous data were converted into means and standard deviations. Cochrane’s Q test and the I2 index were used to evaluate the statistical heterogeneity among the included studies. The Mantel–Haenszel methods and the random-effects models were used. A p-value below 0.05 was considered to have statistical significance. Funnel plots were used to evaluate the publication bias.
3 Results
3.1 Search results
The process of literature selection and inclusion is presented in Figure 1. Our initial search identified a total of 1,492 studies. After excluding duplicates, 1,037 studies remained. Full-text screening excluded 270 articles of other types, 132 articles of other diseases, and 610 unrelated articles. Ultimately, 15 studies (10, 24, 27–39) were included in this meta-analysis.

Figure 1. Flowchart of literature search strategies.
3.2 Patient characteristics and quality assessment
This study included a total of 15 articles, comprising two RCTs and 13 cohort studies. Among them, 777 patients underwent endoscopic thyroidectomy via TOETVA, while 1,184 patients underwent endoscopic thyroidectomy via ETAA. All included studies were conducted within China. Details of author, year, study period, study design, sample, gender, age, diameter of tumor and tumor distribution were summarized in Table 1. The quality of RCTs was assessed using the modified Jadad scale, and both RCTs were rated as high quality (Table 2). The quality of cohort studies was assessed using the NOS, and both studies were rated as high quality (Table 3).

Table 1. Basic characteristics of included trials.

Table 2. Quality assessment of RCTs.

Table 3. Quality assessment according to the Newcastle–Ottawa scale.
3.3 Outcomes
Table 4 summarizes the results of meta-analyses for all clinical outcomes.

Table 4. Results of the meta-analysis.
3.3.1 Operative time (min)
The data were provided in 11 (10, 27–31, 33–35, 37, 38) out of the 15 articles included. The operative time in the ETAA group was significantly shorter than that in the TOETVA group (WMD = 17 min, 95% CI: 8 to 26, p = 0.0002, I2 = 94%) (Figure 2). Sensitivity analysis showed that the outcomes were stable (Supplementary Figure S1). In addition, we used a funnel plot to evaluate the publication bias. The results did not reveal any significant evidence of publication bias (Supplementary Figure S2).

Figure 2. Forest plot of the meta-analysis for operative time.
3.3.2 Intraoperative bleeding volume (mL)
The data were provided in 10 (27–31, 33–35, 37, 38) out of the 15 articles included. The intraoperative bleeding volume in the TOETVA group was significantly lower than that in the ETAA group (WMD = −1.46 mL, 95% CI: −2.79 to −0.13, p = 0.03, I2 = 30%) (Figure 3). Sensitivity analysis showed that the outcomes were stable (Supplementary Figure S3). In addition, we used a funnel plot to evaluate the publication bias. The results did not reveal any significant evidence of publication bias (Supplementary Figure S4).

Figure 3. Forest plot of the meta-analysis for intraoperative bleeding volume.
3.3.3 Number of central lymph node dissections
The data were provided in 10 (10, 24, 28, 30, 32–35, 38, 39) out of the 15 articles included. The number of central lymph node dissections in the ETAA group was significantly lower than that in the TOETVA group (WMD = 1.38, 95% CI: 0.25 to 2.50, p = 0.02, I2 = 93%) (Figure 4). Sensitivity analysis showed that the outcomes were stable (Supplementary Figure S5). In addition, we used a funnel plot to evaluate the publication bias. The results did not reveal any significant evidence of publication bias (Supplementary Figure S6).

Figure 4. Forest plot of the meta-analysis for number of central lymph node dissections.
3.3.4 Postoperative drainage volume (mL)
The data were provided in nine (10, 28, 29, 31, 33–35, 38, 39) out of the 15 articles included. There was no significant difference in postoperative drainage volume between the two groups (WMD = −6 mL, 95% CI: −17 to 5, p = 0.31, I2 = 93%) (Figure 5). Sensitivity analysis showed that the outcomes were stable (Supplementary Figure S7). In addition, we used a funnel plot to evaluate the publication bias. The results did not reveal any significant evidence of publication bias (Supplementary Figure S8).
![A forest plot comparing the mean differences between TOETVA and ETAA across several studies. Each row represents a study with columns for mean, standard deviation, total, and weight. The plot shows individual study results as squares with confidence intervals and an overall effect size as a diamond, favoring TOETVA on the left and ETAA on the right. The overall mean difference is -5.89 with a confidence interval of [-17.27, 5.49].](https://www.frontiersin.org/files/Articles/1606389/fonc-15-1606389-HTML/image_m/fonc-15-1606389-g005.jpg)
Figure 5. Forest plot of the meta-analysis for postoperative drainage volume.
3.3.5 Hospitalization time (days)
The data were provided in 10 (10, 27–31, 33–35, 38) out of the 15 articles included. There was no significant difference in hospitalization time between the two groups (WMD = 0.03 days, 95% CI: −0.13 to 0.19, p = 0.71, I2 = 76%) (Figure 6). Sensitivity analysis showed that the outcomes were stable (Supplementary Figure S9). In addition, we used a funnel plot to evaluate the publication bias. The results did not reveal any significant evidence of publication bias (Supplementary Figure S10).

Figure 6. Forest plot of the meta-analysis for hospitalization time.
3.3.6 Postoperative infection
The data were provided in eight (24, 27–29, 31, 33, 35, 37) out of the 15 articles included. There was no significant difference in postoperative infection between the two groups (OR = 1.43, 95% CI: 0.47 to 4.34, p = 0.53, I2 = 0%) (Figure 7). Sensitivity analysis showed that the outcomes were stable (Supplementary Figure S11). In addition, we used a funnel plot to evaluate the publication bias. The results did not reveal any significant evidence of publication bias (Supplementary Figure S12).

Figure 7. Forest plot of the meta-analysis for postoperative infection.
3.3.7 Hypoparathyroidism
The data were provided in nine (10, 24, 27, 29, 32–34, 37, 38) out of the 15 articles included. There was no significant difference in hypoparathyroidism between the two groups (OR = 0.47, 95% CI: 0.18 to 1.18, p = 0.11, I2 = 67%) (Figure 8). Sensitivity analysis showed that the outcomes were stable (Supplementary Figure S13). In addition, we used a funnel plot to evaluate the publication bias. The results did not reveal any significant evidence of publication bias (Supplementary Figure S14).

Figure 8. Forest plot of the meta-analysis for parathyroid gland injury.
3.3.8 Perioperative recurrent laryngeal nerve injury
The data were provided in nine (24, 27, 29, 31, 32, 34, 35, 37, 38) out of the 15 articles included. There was no significant difference in perioperative recurrent laryngeal nerve injury between the two groups (OR = 0.62, 95% CI: 0.30 to 1.28, p = 0.20, I2 = 0%) (Figure 9). Sensitivity analysis showed that the outcomes were stable (Supplementary Figure S15). In addition, we used a funnel plot to evaluate the publication bias. The results did not reveal any significant evidence of publication bias (Supplementary Figure S16).

Figure 9. Forest plot of the meta-analysis for perioperative recurrent laryngeal nerve injury.
3.3.9 Satisfaction with cosmetic effects
The data were provided in six (28–30, 35, 37, 39) out of the 15 studies included. The satisfaction with cosmetic effects of the patients in the TOETVA group was higher than that in the ETAA group (WMD = 0.93, 95% CI: 0.42 to 1.43, p = 0.0004, I2 = 92%) (Figure 10). Sensitivity analysis showed that the outcomes were stable (Supplementary Figure S17). In addition, we used a funnel plot to evaluate the publication bias. The results did not reveal any significant evidence of publication bias (Supplementary Figure S18).
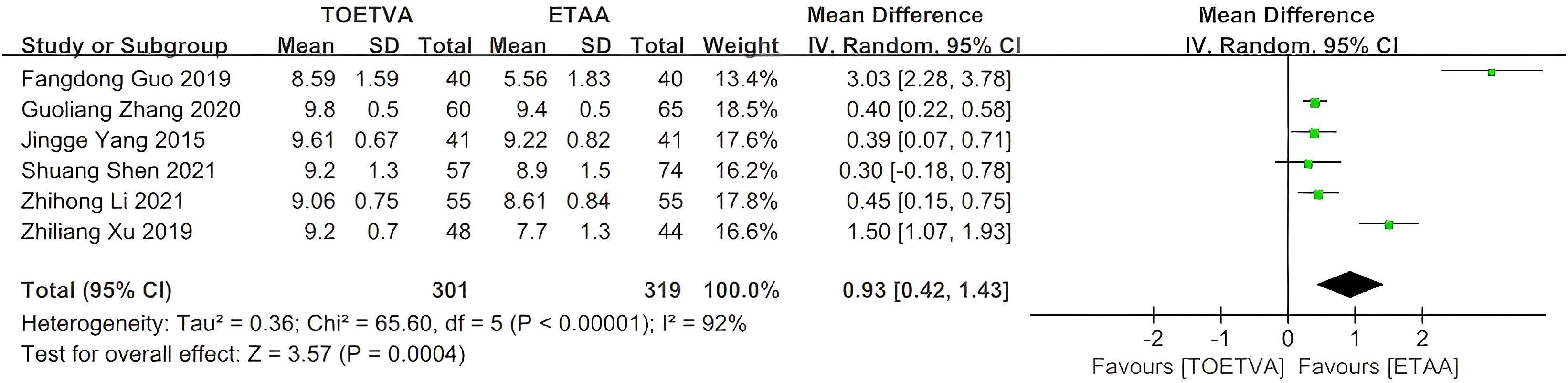
Figure 10. Forest plot of the meta-analysis for the overall satisfaction of the patients.
3.3.10 Hypocalcemia
The data were provided in two (31, 35) out of the 15 articles included. There was no significant difference in hypocalcemia between the two groups (OR = 0.88, 95% CI: 0.40 to 1.91, p = 0.74, I2 = 0%) (Figure 11). Sensitivity analysis showed that the outcomes were stable (Supplementary Figure S19). In addition, we used a funnel plot to evaluate the publication bias. The results did not reveal any significant evidence of publication bias (Supplementary Figure S20).
![Forest plot comparing TOETVA and ETAA. Two studies are listed: Nian Li 2023 and Zhiliang Xu 2019, with events and totals for each. Weights are 68.2% and 31.8% respectively. Odds ratios are 0.77 [0.30, 1.97] and 1.16 [0.29, 4.64]. Total odds ratio is 0.88 [0.40, 1.91]. Heterogeneity indicators and overall effect are noted.](https://www.frontiersin.org/files/Articles/1606389/fonc-15-1606389-HTML/image_m/fonc-15-1606389-g011.jpg)
Figure 11. Forest plot of the meta-analysis for hypocalcemia.
3.3.11 Swallowing discomfort
The data were provided in two (29, 35) out of the 15 articles included. There was no significant difference in swallowing discomfort between the two groups (OR = 0.83, 95% CI: 0.24 to 2.95, p = 0.78, I2 = 0%) (Supplementary Figure S21). Sensitivity analysis showed that the outcomes were stable (Supplementary Figure S22). In addition, we used a funnel plot to evaluate the publication bias. The results did not reveal any significant evidence of publication bias (Supplementary Figure S23).
4 Discussion
4.1 General interpretation of the results in the context of other evidence
This meta-analysis compared the outcomes of endoscopic thyroidectomy via TOETVA versus ETAA in the treatment of thyroid carcinoma. The findings revealed that TOETVA was associated with significantly less intraoperative bleeding, more central lymph node dissections, and higher satisfaction with cosmetic effects, but longer operative time. There was no statistically significant difference between the groups regarding postoperative drainage volume, hospitalization time, postoperative infection, hypoparathyroidism, swallowing discomfort, hypocalcemia, and perioperative recurrent laryngeal nerve injury.
This meta-analysis demonstrated that TOETVA was associated with significantly reduced intraoperative blood loss compared to ETAA. This difference may have been attributed to the direct, minimally invasive access provided by TOETVA, which allowed for precise dissection around the thyroid gland while minimizing trauma to surrounding tissues. In contrast, ETAA required broader dissection fields, potentially increasing the likelihood of encountering and damaging blood vessels (38, 40, 41). Nevertheless, given that the discrepancy was at approximately 1 mL, it is probable that there was no clinically relevant difference between the two procedures. This may fall within the surgeon’s margin of error in estimating intraoperative blood loss. The number of central lymph node dissections in the TOETVA group was significantly greater than in the ETAA group, likely due to enhanced visibility and accessibility to the central neck compartment, facilitating more comprehensive lymph node removal (42). Operative time was significantly shorter in the ETAA group than in the TOETVA group, possibly reflecting the added technical complexity and meticulous nature of the transoral endoscopic approach (43). Conversely, no statistically significant difference was observed in postoperative drainage volume between the two approaches, suggesting comparable fluid accumulation despite differing surgical techniques. This could have resulted from similar dissection extents in both methods, leading to equivalent lymphatic and venous disruptions. In Asian countries such as China, Thailand (44), Japan (45), and Korea (46), surgeons typically keep drains post-thyroidectomy, with the primary criterion for drain removal being a daily drainage volume of 20 mL or less. Previous meta-analyses have indicated that both TOETVA (21, 22) and ETAA (21, 22) were associated with significantly increased postoperative drainage volume compared with open thyroidectomy. The placing of surgical drains has several advantages: 1) the drain facilitates the evacuation of blood (hemorrhage) and serous fluid from the surgical bed, reducing the risk of postoperative hematoma or seroma, which could compress vital structures (e.g., trachea and recurrent laryngeal nerve). 2) By removing accumulated fluid, the drain minimizes the potential medium for bacterial growth, thus lowering the chance of surgical site infection. 3) The drain allows clinicians to assess the volume and character of the effluent (e.g., bloody and chylous), which may indicate hemorrhage or lymphatic fistulas (e.g., thoracic duct injury during central neck dissection). 4) By eliminating dead space, the drain helps the thyroid bed and surrounding tissues adhere properly, improving wound healing.
Different modalities were used among studies that evaluated satisfaction with cosmetic effects. In six studies (28–30, 35, 37, 39), the cosmetic satisfaction data were collected as follows: the score was measured after surgery using a visual analog scale. A Vernier caliper, 0–10 cm in length, is marked with 10 divisions, and the two ends of the caliper represent “0” and “10”. Within the 10 divisions, 0 points means that the aesthetic effect is very poor and the patient is dissatisfied; 10 points means that the patient is very satisfied. The pooled results revealed that TOETVA was linked with significantly higher satisfaction with cosmetic effects compared with ETAA. Another two included studies assessed satisfaction with cosmetic outcomes using other modalities; however, their data were removed from this meta-analysis due to variations in measurement units. Yingying Liu et al. (34) evaluated cosmetic outcomes using a scoring system (1, extreme; 2, fair; 3, normal; 4, not at all), while Cunchuan Wang et al. (27) evaluated cosmetic outcomes using another scoring system (0, no satisfaction; 1, mild satisfaction; 2, moderate satisfaction; and 3, pronounced satisfaction). Despite employing various methods, both studies indicated that TOETVA was associated with markedly greater satisfaction with cosmetic outcomes in comparison to ETAA. There were several reasons why patients in the TOETVA group were significantly more satisfied than those in the ETAA group. First, although both TOETVA and ETAA underscore the trend toward more aesthetically appealing thyroid surgery, TOETVA utilizes natural orifices to accomplish a genuinely scarless procedure, effectively avoiding the exposure of thyroid cancer history. Second, reduced postoperative pain and traction feeling led to increased patient satisfaction in the TOETVA group (30). In addition, the TOETVA technique significantly enhanced patients’ self-confidence post-surgery, facilitated speedy recovery, and improved their quality of life. Patients who undergo the TOETVA surgery exhibit enhanced cosmetic pleasure, improved social functioning, and reduced mental health issues, facilitating a swift return to normalcy in life and work. Consequently, patient satisfaction is elevated, and patients will experience a superior quality of life (37). Furthermore, Guoliang Zhang et al. (29) reported that the cosmetic satisfaction score of the TOETVA group was significantly superior to that of the ETAA group at the 1-month postoperative follow-up; however, at the 3-month mark, the scores of both groups were comparable, with no statistically significant difference, suggesting that outcomes may vary according to the healing process. Unfortunately, most of the literature did not provide results for long-term satisfaction with cosmetic effects, which makes it impossible for us to further analyze long-term cosmetic effects.
The findings indicated that TOETVA and ETAA demonstrated no statistically significant difference in postoperative hospitalization duration. This similarity may have stemmed from both approaches adhering to minimally invasive principles, which reduced tissue trauma and enabled early ambulation. Furthermore, no significant difference in hypoparathyroidism, swallowing discomfort, or hypocalcemia was observed between TOETVA and ETAA, likely due to enhanced visualization and nerve monitoring that assisted in preserving parathyroid function during both procedures. The anatomical proximity and improved visual access may also have contributed to reduced surgical trauma to these glands (47, 48). Regarding hematoma, two included studies reported the following: Shen et al. (37) reported one case in the TOETVA group and one case in the ETAA group; Li et al. (31) reported no hematoma occurrence in both groups. Hematoma complications appear to be few in both surgical approaches; however, a meta-analysis on hematoma could not be performed due to the absence of pertinent data in the other included literature. Lastly, no significant differences were found between TOETVA and ETAA regarding recurrent laryngeal nerve (RLN) injury or postoperative infection rates, indicating that both approaches maintained comparable safety profiles for these critical postoperative outcomes (49, 50).
4.2 Limitations of the evidence included in the review
First, the majority of the included studies was retrospective in nature and had small sample sizes, with a relatively limited number of randomized controlled trials. This limited the overall quality and robustness of the results. Second, among the included studies, only one study reported the recurrence of cancer (34), and all other included studies did not report long-term oncologic outcomes, such as mortality, recurrence, or distant metastasis rates. This prevented the analysis of long-term tumor prognosis outcomes. Third, the complication profiles are significantly different for patients who underwent total thyroidectomy compared to thyroid lobectomy, especially when it comes to postoperative hypoparathyroidism, hypocalcemia, hematoma, and swallowing discomfort. However, the included studies did not disaggregate outcome data for patients categorized by type of surgery, which prevented further subgroup analysis to explore the impact of surgical type. In addition, heterogeneity in baseline characteristics across studies may have introduced selection bias.
4.3 Limitations of the review processes used
First, the literature search strategy, although comprehensive across PubMed, Embase, Web of Science, Cochrane Library, and Scopus, may have failed to capture all relevant studies due to database-specific indexing variations or unpublished data, which introduced potential selection bias. Additionally, statistical heterogeneity was extreme for several pooled outcomes, which may be caused by different basic characteristics of included trials, such as tumor distribution, type of surgery, and TNM stage. However, we failed to perform subgroup or meta-regression analyses to explore its sources due to the absence of precise outcome data for patients categorized by tumor distribution, type of surgery, and TNM stage. These limitations in data availability compromised the ability to assess heterogeneity thoroughly and may have influenced pooled effect estimates. Furthermore, another limitation of this study was that TOETVA and ETAA were not compared with open surgery. A previous systematic review and meta-analysis (51) demonstrated that endoscopic thyroidectomy does not surpass open surgery regarding operation and drainage duration, volume of drainage fluid, length of hospital stay, or transient recurrent laryngeal nerve palsy, yet it is comparable to open surgery concerning retrieved lymph nodes and permanent complications. A network meta-analysis is advised to determine whether TOETVA and ETAA demonstrate comparable safety and efficacy to traditional open thyroidectomy. Furthermore, all included studies were conducted in China, which limited the generalizability of the findings to global populations.
4.4 Implications of the results for practice, policy, and future research
The findings indicated that both TOETVA and ETAA in thyroid surgery demonstrated safe and reliable clinical efficacy. TOETVA offers additional benefits in terms of satisfaction with cosmetic effects, intraoperative bleeding, and lymph node dissection in the central area. TOETVA should be a preferred option for patients seeking scar-free surgery. Standardized guidelines were deemed necessary to refine patient selection algorithms and optimize training programs for TOETVA, given its technical complexity and steep learning curve.
It is advised to conduct more multi-center RCTs with a large sample and longer follow-up in the future to confirm our conclusion. Long-term oncologic surveillance should be an important indicator. The incorporation of patient-reported outcomes, such as quality of life and cosmetic satisfaction, was emphasized to enhance clinical relevance.
In conclusion, the present meta-analysis evaluated the outcomes of endoscopic thyroidectomy via TOETVA versus ETAA for thyroid carcinoma. The results showed that both TOETVA and ETAA exhibited safe and dependable clinical effectiveness. TOETVA provided extra advantages regarding satisfaction with cosmetic effects, intraoperative bleeding, and lymph node dissection in the central region. TOETVA is an ideal choice for patients seeking scarless surgery.
Data availability statement
The datasets presented in this study can be found in online repositories. The names of the repository/repositories and accession number(s) can be found in the article/Supplementary Material.
Author contributions
JW: Conceptualization, Data curation, Project administration, Writing – original draft, Formal analysis. ZX: Conceptualization, Data curation, Formal analysis, Funding acquisition, Writing – review & editing. WL: Writing – original draft, Formal analysis, Conceptualization, Project administration, Data curation. XW: Writing – original draft, Investigation, Methodology. XL: Methodology, Investigation, Writing – original draft. SY: Software, Writing – original draft, Supervision. YY: Supervision, Writing – original draft, Software. JQ: Writing – review & editing, Visualization, Validation. ZL: Writing – review & editing, Funding acquisition, Visualization, Resources. CH: Funding acquisition, Resources, Writing – review & editing. PW: Funding acquisition, Resources, Writing – review & editing.
Funding
The author(s) declare financial support was received for the research and/or publication of this article. The authors disclose the receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Key Laboratory Construction Project of Guangxi Health Commission (ZPZH2020007) and the Scientific Research Foundation of Guangxi Health Commission (Z-B20230966).
Acknowledgments
Everyone who contributed significantly to this study has been listed.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Generative AI statement
The author(s) declare that no Generative AI was used in the creation of this manuscript.
Any alternative text (alt text) provided alongside figures in this article has been generated by Frontiers with the support of artificial intelligence and reasonable efforts have been made to ensure accuracy, including review by the authors wherever possible. If you identify any issues, please contact us.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fonc.2025.1606389/full#supplementary-material
References
1. Seib CD and Sosa JA. Evolving understanding of the epidemiology of thyroid cancer. Endocrinol Metab Clin North Am. (2019) 48:23–35. doi: 10.1016/j.ecl.2018.10.002
2. Lam D, Davies L, and Sawka AM. Women and thyroid cancer incidence: overdiagnosis versus biological risk. Curr Opin Endocrinol Diabetes Obes. (2022) 29:492–6. doi: 10.1097/med.0000000000000756
3. Kitahara CM and Sosa JA. The changing incidence of thyroid cancer. Nat Rev Endocrinol. (2016) 12:646–53. doi: 10.1038/nrendo.2016.110
4. Frasca F, Piticchio T, Le Moli R, Tumino D, Cannavò S, Ruggeri RM, et al. Early detection of suspicious lymph nodes in differentiated thyroid cancer. Expert Rev Endocrinol Metab. (2022) 17:447–54. doi: 10.1080/17446651.2022.2112176
5. Nguyen HX, Nguyen HX, Nguyen TTP, and Van Le Q. Transoral endoscopic thyroidectomy by vestibular approach in viet nam: surgical outcomes and long-term follow-up. Surg Endosc. (2022) 36:4248–54. doi: 10.1007/s00464-021-08759-6
6. Chen ZX, Song YM, Chen JB, Zhang XB, Pang FS, Lin ZH, et al. Safety and feasibility of the transoral endoscopic thyroidectomy vestibular approach with neuroprotection techniques for papillary thyroid carcinoma. BMC Surg. (2022) 22:270. doi: 10.1186/s12893-022-01707-8
7. Gupta K and Kataria K. Comparison of different approaches of endoscopic thyroidectomy and open thyroidectomy: A meta-analysis. Indian J Surg. (2024) 86:206–19. doi: 10.1007/s12262-023-04002-9
8. Patel KN, Yip L, Lubitz CC, Grubbs EG, Miller BS, Shen W, et al. The american association of endocrine surgeons guidelines for the definitive surgical management of thyroid disease in adults. Ann Surg. (2020) 271:e21–93. doi: 10.1097/sla.0000000000003580
9. Duncan TD, Rashid Q, Speights F, and Ejeh I. Transaxillary endoscopic thyroidectomy: an alternative to traditional open thyroidectomy. J Natl Med Assoc. (2009) 101:783–7. doi: 10.1016/s0027-9684(15)31006-3
10. Sun H, Zheng H, Wang X, Zeng Q, Wang P, and Wang Y. Comparison of transoral endoscopic thyroidectomy vestibular approach, total endoscopic thyroidectomy via areola approach, and conventional open thyroidectomy: A retrospective analysis of safety, trauma, and feasibility of central neck dissection in the treatment of papillary thyroid carcinoma. Surg Endosc. (2020) 34:268–74. doi: 10.1007/s00464-019-06762-6
11. Lin P, Liang F, Han P, Cai Q, Chen R, Lin X, et al. Gasless endoscopic thyroidectomy via the anterior chest approach: the experience with 1500 cases. Surg Endosc. (2023) 37:7867–75. doi: 10.1007/s00464-023-10401-6
12. Huang XM, Sun W, Hong Y, Cai Q, Liang FY, and Han P. Minimally invasive endoscopic thyroidectomy via an anterior chest approach for early papillary thyroid cancer. Zhonghua Er Bi Yan Hou Tou Jing Wai Ke Za Zhi. (2012) 47:571–4.
13. Huang XM, Sun W, Zeng L, Liu X, Lu X, Xu YD, et al. Gasless endoscopic thyroidectomy via an anterior chest approach–a review of 219 cases with benign tumor. World J Surg. (2011) 35:1281–6. doi: 10.1007/s00268-011-1087-6
14. Qu R, Li J, Yang J, Sun P, Gong J, and Wang C. Treatment of differentiated thyroid cancer: can endoscopic thyroidectomy via a chest-breast approach achieve similar therapeutic effects as open surgery? Surg Endosc. (2018) 32:4749–56. doi: 10.1007/s00464-018-6221-1
15. Anuwong A. Transoral endoscopic thyroidectomy vestibular approach: A series of the first 60 human cases. World J Surg. (2016) 40:491–7. doi: 10.1007/s00268-015-3320-1
16. Rege SA, Janesh M, Surpam S, Shivane V, Arora A, and Singh A. Transoral endoscopic thyroidectomy using vestibular approach: A single center experience. J Postgrad Med. (2019) 65:81–6. doi: 10.4103/jpgm.JPGM_117_18
17. Divarci E, Ulman H, Ozok G, Ozen S, Ozdemir M, and Makay O. Transoral endoscopic thyroidectomy vestibular approach (Toetva): A novel surgical technique for scarless thyroidectomy in pediatric surgery. J Pediatr Surg. (2022) 57:1149–57. doi: 10.1016/j.jpedsurg.2022.01.038
18. Kose OC, Turk Y, Ozdemir M, Makay O, and Icoz G. Patient eligibility for transoral endoscopic thyroidectomy vestibular approach in an endemic region. Sisli Etfal Hastan T&305;p Bul. (2021) 55:304–9. doi: 10.14744/semb.2021.87160
19. Wu YJ, Chi SY, Chan YC, Chou FF, Wee SY, and Wu KT. Scarless completion thyroidectomy after initial transoral approach for differentiated thyroid cancer: how and when to start? Surg Laparosc Endosc Percutan Tech. (2021) 31:554–7. doi: 10.1097/sle.0000000000000933
20. Russell JO, Clark J, Noureldine SI, Anuwong A, Al Khadem MG, Yub Kim H, et al. Transoral thyroidectomy and parathyroidectomy - a north american series of robotic and endoscopic transoral approaches to the central neck. Oral Oncol. (2017) 71:75–80. doi: 10.1016/j.oraloncology.2017.06.001
21. Wang Y, Zhou S, Liu X, Rui S, Li Z, Zhu J, et al. Transoral endoscopic thyroidectomy vestibular approach vs conventional open thyroidectomy: meta-analysis. Head Neck. (2021) 43:345–53. doi: 10.1002/hed.26486
22. Yuan Y, Sun C, Yin T, Shao C, Pan B, Lu D, et al. Comparison of endoscopic thyroidectomy by complete areola approach and conventional open surgery in the treatment of differentiated thyroid carcinoma: A retrospective study and meta-analysis. Front Surg. (2022) 9:1000011. doi: 10.3389/fsurg.2022.1000011
23. Long T, Li J, Yuan Y, Yang Z, Xu P, Pan B, et al. Comparison of endoscopic surgical approaches for total thyroidectomy: A systematic review and bayesian network meta-analysis. Gland Surg. (2025) 14:1–12. doi: 10.21037/gs-24-424
24. Xu W, Teng C, Ding G, and Zhao N. Oncologic safety and surgical outcomes of the different surgical approaches of endoscopic thyroidectomy for papillary thyroid carcinoma. Surg Today. (2023) 53:554–61. doi: 10.1007/s00595-022-02630-4
25. Stang A. Critical evaluation of the newcastle-ottawa scale for the assessment of the quality of nonrandomized studies in meta-analyses. Eur J Epidemiol. (2010) 25:603–5. doi: 10.1007/s10654-010-9491-z
26. Jadad AR, Moore RA, Carroll D, Jenkinson C, Reynolds DJ, Gavaghan DJ, et al. Assessing the quality of reports of randomized clinical trials: is blinding necessary? Control Clin Trials. (1996) 17:1–12. doi: 10.1016/0197-2456(95)00134-4
27. Wang C, Zhai H, Liu W, Li J, Yang J, Hu Y, et al. Thyroidectomy: A novel endoscopic oral vestibular approach. Surgery. (2014) 155:33–8. doi: 10.1016/j.surg.2013.06.010
28. Guo F, Wang W, Zhu X, Xiang C, Wang P, and Wang Y. Comparative study between endoscopic thyroid surgery via the oral vestibular approach and the areola approach. J Laparoendosc Adv Surg Tech A. (2020) 30:170–4. doi: 10.1089/lap.2019.0562
29. Zhang G, Li B, Zhang G, Lin Y, Chen Y, and Gao J. Pros and cons of transoral endoscopic thyroidectomy via vestibular approach: A comparative study. Surg Laparosc Endosc Percutan Tech. (2020) 31:331–6. doi: 10.1097/sle.0000000000000875
30. Yang J, Wang C, Li J, Yang W, Cao G, Wong HM, et al. Complete endoscopic thyroidectomy via oral vestibular approach versus areola approach for treatment of thyroid diseases. J Laparoendosc Adv Surg Tech A. (2015) 25:470–6. doi: 10.1089/lap.2015.0026
31. Li N, Shen H, Zhang J, Dong B, Wang Y, and Li T. A new transoral vestibulum single incision endoscopic-assisted thyroidectomy with gasless. Laryngoscope. (2024) 134:2976–84. doi: 10.1002/lary.31197
32. Xu W, Teng C, Ding G, and Zhao N. Hypoparathyroidism risk after total endoscopic thyroidectomy for papillary thyroid cancer: A comparison of the transoral vestibular and breast approaches. Cancer Manag Res. (2022) 14:2485–92. doi: 10.2147/cmar.S380024
33. Zhang WD, Dai L, Wang YC, Xie YY, Guo JY, Li JJ, et al. Transoral endoscopic thyroidectomy vestibular approach versus endoscopic thyroidectomy via areola approach for patients with unilateral papillary thyroid carcinoma: A retrospective study. Surg Laparosc Endosc Percutan Tech. (2021) 31:550–3. doi: 10.1097/sle.0000000000000932
34. Liu Y, Lin F, Yan W, Lin E, Kuang P, Hong X, et al. Comparison of endoscopic thyroidectomy via the oral vestibule approach and the areola approach for papillary thyroid carcinoma. BMC Surg. (2024) 24:127. doi: 10.1186/s12893-024-02413-3
35. Xu Z, Song J, Wang Y, Tan L, Sun S, and Meng Y. A comparison of transoral vestibular and bilateral areolar endoscopic thyroidectomy approaches for unilateral papillary thyroid microcarcinomas. Wideochir Inne Tech Maloinwazyjne. (2019) 14:501–8. doi: 10.5114/wiitm.2019.84759
36. Li MC, Zhang QS, Li D, Chen G, Chen Z, and Lyu J. the effect of operative approach selection on the protection of parathyroid function in thyroid cancer. Zhonghua Er Bi Yan Hou Tou Jing Wai Ke Za Zhi. (2020) 55:921–5. doi: 10.3760/cma.j.cn115330-20200519-00422
37. Shen S, Hu X, Qu R, Guo Y, Luo L, and Chen X. Comparing quality of life between patients undergoing trans-areola endoscopic thyroid surgery and trans-oral endoscopic thyroid surgery. BMC Surg. (2021) 21:277. doi: 10.1186/s12893-021-01267-3
38. Liu ZD, Li YJ, Yu X, Xiang C, Wang P, and Wang Y. a comparative study on the efficacy of transoral vestibular approach, via bilateral areola approach endoscopic and open thyroidectomy on stage T1b papillary thyroid carcinoma. Zhonghua Er Bi Yan Hou Tou Jing Wai Ke Za Zhi. (2020) 55:905–12. doi: 10.3760/cma.j.cn115330-20200520-00430
39. Zhihong L, Yihong T, and Weixin L. Comparative study on the curative effect and safety of endoscopic micro-papillary carcinoma thyroid surgery through oral vestibule and chest-breast approaches. Chin J Anat Clinics. (2021) 26:209–13. doi: 10.3760/cma.j.cn101202-20200721-00231
40. Anuwong A, Sasanakietkul T, Jitpratoom P, Ketwong K, Kim HY, Dionigi G, et al. Transoral endoscopic thyroidectomy vestibular approach (Toetva): indications, techniques and results. Surg Endosc. (2018) 32:456–65. doi: 10.1007/s00464-017-5705-8
41. Fu X, Ma Y, Hou Y, Liu Y, and Zheng L. Comparison of endoscopic bilateral areolar and robotic-assisted bilateral axillo-breast approach thyroidectomy in differentiated thyroid carcinoma: A propensity-matched retrospective cohort study. BMC Surg. (2023) 23:338. doi: 10.1186/s12893-023-02250-w
42. Liao HJ, Dong C, Kong FJ, Zhang ZP, Huang P, and Chang S. The cusum analysis of the learning curve for endoscopic thyroidectomy by the breast approach. Surg Innov. (2014) 21:221–8. doi: 10.1177/1553350613500722
43. Chai YJ, Chung JK, Anuwong A, Dionigi G, Kim HY, Hwang KT, et al. Transoral endoscopic thyroidectomy for papillary thyroid microcarcinoma: initial experience of a single surgeon. Ann Surg Treat Res. (2017) 93:70–5. doi: 10.4174/astr.2017.93.2.70
44. Anuwong A, Ketwong K, Jitpratoom P, Sasanakietkul T, and Duh QY. Safety and outcomes of the transoral endoscopic thyroidectomy vestibular approach. JAMA Surg. (2018) 153:21–7. doi: 10.1001/jamasurg.2017.3366
45. Nakajo A, Arima H, Hirata M, Mizoguchi T, Kijima Y, Mori S, et al. Trans-oral video-assisted neck surgery (Tovans). A new transoral technique of endoscopic thyroidectomy with gasless premandible approach. Surg Endosc. (2013) 27:1105–10. doi: 10.1007/s00464-012-2588-6
46. Kim HY, Chai YJ, Dionigi G, Anuwong A, and Richmon JD. Transoral robotic thyroidectomy: lessons learned from an initial consecutive series of 24 patients. Surg Endosc. (2018) 32:688–94. doi: 10.1007/s00464-017-5724-5
47. Park D, Cho H, Lee E, Oh MY, Kim K, Chai YJ, et al. Feasibility and safety of transoral robotic parathyroidectomy: initial experience with a new approach for parathyroid surgery. Asian J Surg. (2024) 47:4300–6. doi: 10.1016/j.asjsur.2024.07.162
48. Wu Z, Fang JG, Chen X, Hou LZ, Zhong Q, Ma HZ, et al. Protection of nerve function during transoral endoscopic thyroidectomy by vestibular approach. Zhonghua Er Bi Yan Hou Tou Jing Wai Ke Za Zhi. (2020) 55:893–8. doi: 10.3760/cma.j.cn115330-20200526-00447
49. Zhao Q, Wang W, Yu X, and Wang Y. Application of transoral endoscopic parathyroidectomy via vestibular approach, endoscopic parathyroidectomy via areola approach for parathyroid adenoma. Eur Arch Otorhinolaryngol. (2021) 278:1559–65. doi: 10.1007/s00405-020-06231-0
50. Yan X, Zhu C, Wu W, Geng X, Ding Y, and Li Y. Transoral endoscopic thyroidectomy vestibular approach for papillary thyroid microcarcinoma: an analysis of clinical outcomes. Am J Transl Res. (2022) 14:7907–15.
Keywords: thyroid carcinoma, endoscopic, thyroidectomy, transoral endoscopic thyroidectomy vestibular approach, endoscopic thyroidectomy via areola approach, cosmetic, satisfaction, meta-analysis
Citation: Wu J, Xiao Z, Liang W, Wang X, Liang X, Yin S, Yang Y, Quan J, Li Z, Hu C and Wei P (2025) Outcomes of transoral endoscopic thyroidectomy vestibular approach versus endoscopic thyroidectomy via areola approach in the treatment of thyroid carcinoma: a meta-analysis. Front. Oncol. 15:1606389. doi: 10.3389/fonc.2025.1606389
Received: 05 April 2025; Accepted: 06 August 2025;
Published: 09 September 2025.
Edited by:
Erivelto Martinho Volpi, Hospital Alemão Oswaldo Cruz, BrazilReviewed by:
Rafael De Cicco, Doctor Arnaldo Cancer Institute, BrazilHui Zheng, MedStar Georgetown University Hospital, United States
Hayato Nakanishi, Mayo Clinic, United States
Copyright © 2025 Wu, Xiao, Liang, Wang, Liang, Yin, Yang, Quan, Li, Hu and Wei. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Chunge Hu, Y2h1bmdlaHUyMDI1QDE2My5jb20=; Ping Wei, cGluZ3dlaTIwMjUxQDE2My5jb20=
†These authors have contributed equally to this work and share first authorship