 Ana Godoy-Ortíz1,2,3†
Ana Godoy-Ortíz1,2,3† Gonzalo Lendínez-Sánchez2,4*†
Gonzalo Lendínez-Sánchez2,4*† Manuel Zalabardo1,2
Manuel Zalabardo1,2 Javier Pascual1,2,3Ana López-Pascual2,4Alexandra Cantero2,4Nuria Ribelles1,2
Javier Pascual1,2,3Ana López-Pascual2,4Alexandra Cantero2,4Nuria Ribelles1,2 Marcos Iglesias1,2Ester Villar2,4Bella Pajares1,2
Marcos Iglesias1,2Ester Villar2,4Bella Pajares1,2 Tamara Díaz-Redondo2,4Maria Emilia Domínguez-Recio1,2Francisco Carabantes2,4Maria Jose Bermejo1,2Antonio Rueda-Domínguez1,2Emilio Alba1,2,3,5
Tamara Díaz-Redondo2,4Maria Emilia Domínguez-Recio1,2Francisco Carabantes2,4Maria Jose Bermejo1,2Antonio Rueda-Domínguez1,2Emilio Alba1,2,3,5 Alfonso Sánchez-Muñoz1,2,5
Alfonso Sánchez-Muñoz1,2,5- 1Department of Medical Oncology, Virgen de La Victoria University Hospital, Malaga, Spain
- 2The Biomedical Research Institute of Malaga (IBIMA-CIMES-UMA), Malaga, Spain
- 3Centro de Investigacion Biomedica en Red de Cáncer (CIBERONC-CB16/12/00481), Madrid, Spain
- 4Department of Medical Oncology, Hospital Regional Universitario de Malaga, Malaga, Spain
- 5Faculty of Medicine, University of Malaga, Malaga, Spain
Purpose: Evaluate real-world outcomes in three cohorts of patients with early-stage triple-negative breast cancer (TNBC) treated with neoadjuvant chemotherapy (NAC): (1) patients who achieved pathological complete response (pCR); (2) patients without pCR who didn’t receive adjuvant chemotherapy; and (3) patients without pCR who received adjuvant capecitabine.
Methods: Retrospective cross-sectional study from two hospitals in Málaga. Patients with TNBC received standard NAC followed by surgery. Between 2004 and 2015, patients not achieving pCR received no further systemic therapy. From 2015 onward, these patients were treated with adjuvant capecitabine. Kaplan–Meier and log-rank tests were used to compare disease-free survival (DFS) and overall survival (OS).
Results: A total of 312 patients were included in the study. 133 achieved pCR, 84 patients didn’t achieve pCR and didn’t receive adjuvant capecitabine and 95 patients didn’t reach pCR and received adjuvant capecitabine. 89 patients experienced recurrence and 70 patients died. Patients who achieved pCR had a significantly higher DFS (HR 0.21 CI95% 0.12-0.36, p<0.0001) and higher overall survival (HR 0.27 CI95% 0.15-0.49, p<0.0001) compared to those who didn’t. Statistically significant differences in DFS and OS were observed among the three cohorts (DFS: p<0.00001; OS: p=0.00005). However, no statistically significant differences were found between cohorts 2 and 3 in terms of DFS (p=0.94) or OS (p=0.34).
Conclusions: Patients who achieved pCR had better outcomes compared to those who didn’t. Among patients who didn’t achieve pCR, the addition of capecitabine didn’t result in significant improvements in DFS or OS compared to those who didn’t receive adjuvant treatment.
1 Introduction
Triple-negative breast cancer (TNBC) comprises a heterogeneous subgroup of tumors, accounting for approximately 15–20% of all breast cancers. TNBC is clinically defined by the absence of estrogen receptor (ER), progesterone receptor (PR), and human epidermal growth factor receptor 2 (HER2) amplification/overexpression. This breast cancer subtype exhibits a more aggressive natural history and worse disease-specific outcomes compared to other breast cancer subtypes. Standard treatment for early-stage TNBC has traditionally relied on anthracycline and taxane based chemotherapy, with or without platinum salts (1).
Neoadjuvant chemotherapy (NAC) has historically been used to downstage unresectable tumors, improving loco-regional control and increasing the rate of breast-conserving surgery. The neoadjuvant approach provides a valuable in vivo assessment of tumor biological sensitivity and drug efficacy. Patients who achieve pathological complete response (pCR) following NAC (between 30 - 40%), experience a significant improvement in prognosis, with disease-free survival (DFS) and overall survival (OS) comparable to that of patients with less aggressive tumors (2–4),,. However, TNBC patients with residual disease (RD) after chemotherapy face a high risk of relapse and mortality (2, 5), representing a critical unmet clinical need where post-neoadjuvant escalation therapies may still improve survival.
Following the CREATE-X trial, which demonstrated that adjuvant capecitabine improved both DFS and OS, its use as standard systemic therapy in unselected TNBC patients with RD after NAC has become standard therapy (6). The Finnish FinXX study evaluated adjuvant capecitabine in combination with standard adjuvant chemotherapy and, in an exploratory analysis of TNBC patients, reported a statistically significant improvement in recurrence-free survival (RFS, 7). However, the addition of capecitabine, whether concurrently or sequentially after standard adjuvant chemotherapy, has yielded controversial results (8, 9).
In this study, we assessed real-world outcomes in three cohorts of patients with early invasive TNBC treated with NAC based on anthracyclines-cyclophosphamide and/or taxanes, with or without carboplatin:
Cohort 1: Patients who achieved pCR and did not receive adjuvant therapy.
Cohort 2: Patients who did not achieve pCR and did not receive adjuvant chemotherapy or other systemic therapy.
Cohort 3: Patients who did not achieve pCR and received adjuvant chemotherapy with capecitabine.
2 Materials and methods
2.1 Patients and samples
We conducted a retrospective analysis of 312 patients with histologically confirmed invasive TNBC (ER-negative, PR-negative and Her2-negative). All patients received standard NAC. Within 4 to 6 weeks after the last chemotherapy cycle, patients underwent either modified radical mastectomy or conservative surgery with axillary lymph node dissection or sentinel lymph node biopsy according to standard surgical guidelines. Patients treated with breast-conserving surgery received adjuvant radiotherapy after surgery to the whole breast. For patients who underwent mastectomy, radiation therapy was administered to the chest wall and axillary region in patients who had an initial tumor > 5 cm, inflammatory breast cancer or had positive nodes before or after neoadjuvant chemotherapy.
Patients who achieved a pCR did not receive chemotherapy adjuvant therapy or any other systemic therapy. From June 2004 to June 2015, patients who did not achieve pCR also did not receive adjuvant chemotherapy or other systemic treatments. However, since July 2015, patients with residual disease (RD) after NAC were administered adjuvant chemotherapy with oral capecitabine at a dose of 1250 mg/m² twice daily on days 1 to 14 of a 21-day cycle, for six to eight cycles, unless discontinued based on the clinical judgment of the oncologist, the patient’s decision, or any other reason as outlined in Figure 1. Patients who received Olaparib, pembrolizumab, or any adjuvant treatment other than capecitabine were excluded from the analysis. Patients were followed up at our institutions every six months, with annual mammographic screening to assess for breast cancer recurrence or upon presentation of any symptoms or signs suggestive of recurrence.
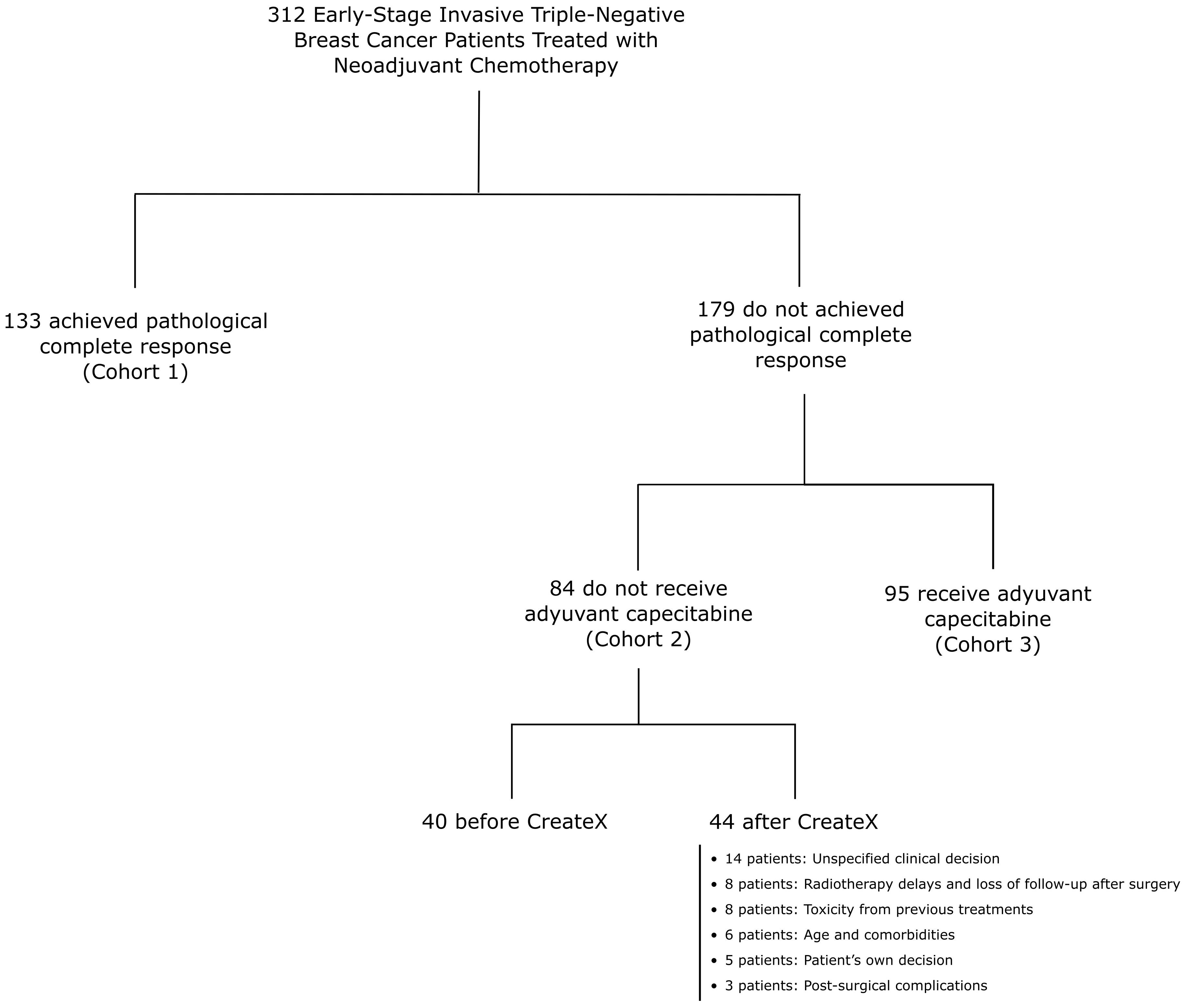
Figure 1. Flowchart of 312 patients with early-stage triple-negative breast cancer stratified by cohorts.
Tumor sample analyses were conducted on biopsy specimens obtained before neoadjuvant treatment. Immunohistochemical staining was performed at our hospital using the following antibodies: estrogen receptor (ER, Clone SP1), progesterone receptor (PR, Clone Y85), and human epidermal growth factor receptor 2 (HER2, HercepTest, DakoCytomation, Glostrup, Denmark).
All patient samples were classified as triple-negative based on immunohistochemistry (IHC), defined as ER-negative, PR-negative, and HER2-negative. ER and PR were considered negative if <1% of tumor cells showed positive staining. HER2 negativity was determined by either IHC scores of 0 or +1, or IHC + 2 with a negative fluorescence in situ hybridization (FISH) result.
Data on Ki-67 expression were collected both as a continuous variable and as a dichotomized variable, using a 50% cutoff. pCR was defined as the absence of invasive tumor cells in both the breast and lymph nodes (10). All patients provided written informed consent to receive treatment, and the study protocols were approved by the corresponding institutional ethics committees.
2.2 Statistical analysis methods
Continuous variables, including mean, median, measures of dispersion, standard deviation, interquartile range, and range, were summarized using measures of central tendency. Categorical variables were presented as frequencies and percentages.
Disease-free survival (DFS) was defined as the time from the date of surgery to either documented disease progression or death from any cause, whichever occurred first. Overall survival (OS) was defined as the time from the date of surgery to death from any cause. Kaplan–Meier curves and log-rank tests were used to compare DFS and OS among cohorts.
The impact of prognostic variables, including menopausal status, < 40 or ≥ 40 years, Ki-67 index ≤ 50% or > 50%, tumour size <5 cm or ≥5 cm, lymph node status previous to surgery, achieving a pCR after NAC and adjuvant capecitabine, was evaluated using Cox proportional hazards regression models.
Survival analysis stratified by germline status mutation in each cohort was estimated using Kaplan-Meier method.
All statistical analyses and figures were generated using SPSS statistical software, version 26 (IBM, Armonk, NY, USA).
Figures were modified using InkScape vector graphics editor software.
3 Results
Data from 312 women with early-stage TNBC treated with NAC between 2004 and 2023 were retrospectively collected. The median age at diagnosis was 48.5 years (range: 26-79) and 177 patients (56.7%) were premenopausal. Axillary lymphs node involvement at diagnosis was observed in 134 patients (42.9%) while 57 patients (18.3%) had a tumour size greater than 5 cm. Ki67 proliferation index was greater than 50% in 203 patients (65.1%). Germline mutation testing was conducted in 205 patients (65.7%), revealing 31 patients with a pathogenic BRCA1 mutation and 8 patients with a pathogenic BRCA2 mutation. However, these patients did not receive adjuvant treatment with Olaparib, as it was not yet approved at that time. Other mutations (detected in 12 patients) were ATM, PALB2, RAD51, CDKN2A, MUTYH and MSH6. The majority of patients (95%) received standard NAC, consisting of anthracyclines, cyclophosphamide, and taxanes, with or without carboplatin. Additional baseline clinical and pathological characteristics, stratified by cohort, are summarized in Table 1.
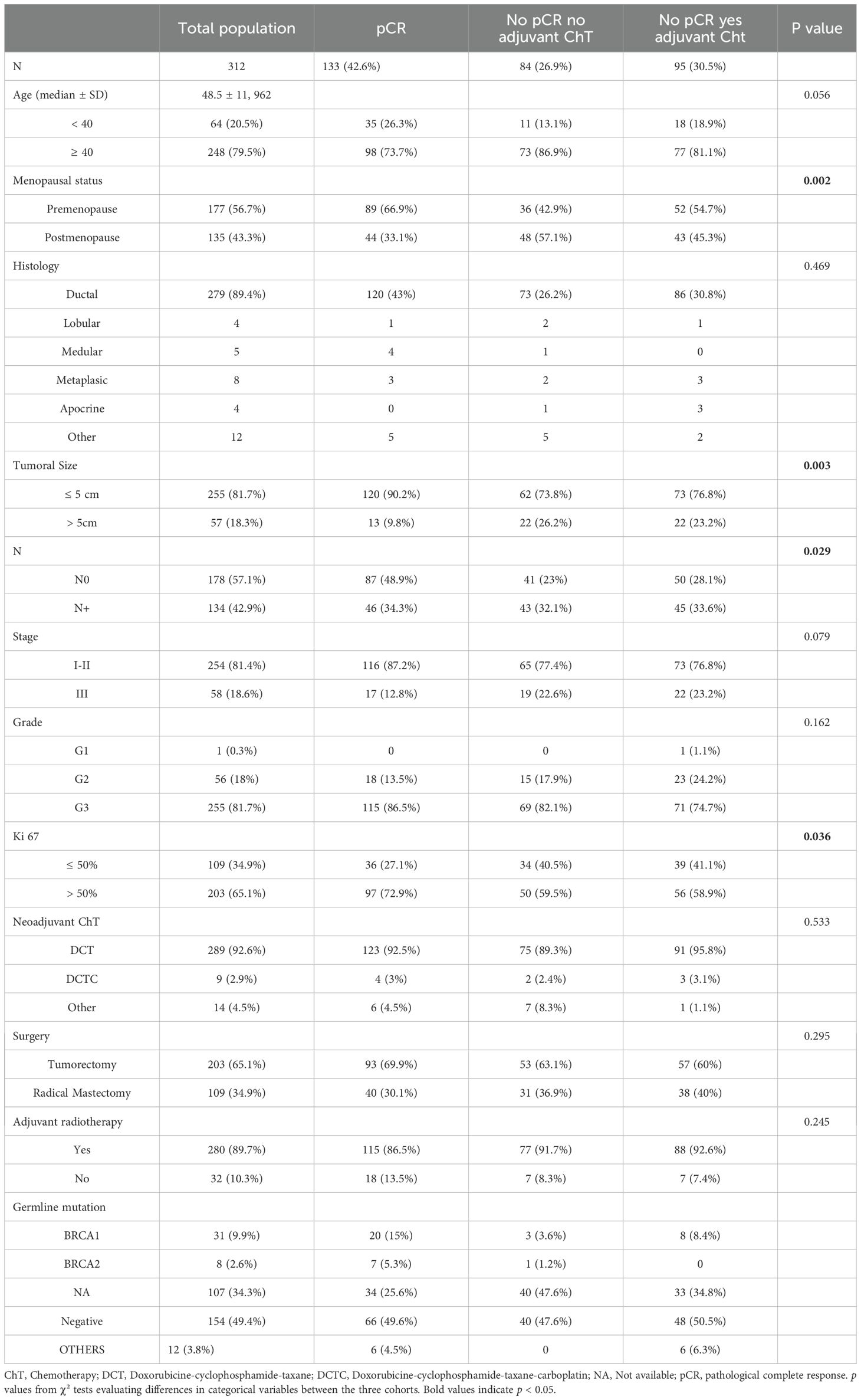
Table 1. Baseline clinical and pathological characteristics of the population.
A pathological complete response was achieved by 133 patients (42.6%) who were categorized as Cohort 1. A total of 179 patients (57.4%) had RD. 84 patients (26.9%) did not receive adjuvant capecitabine and were categorized as Cohort 2. Notably, 44 patients in Cohort 2 did not receive adjuvant capecitabine treatment despite being diagnosed after the publication of the CreateX study results. The reasons for not receiving treatment are detailed in Figure 1. The remaining 95 patients (30.5%) received adjuvant capecitabine and were categorized as Cohort 3.
Median follow-up was of 48 months (range: 3-250; C1 = 59 months, C2 = 58 months; C3 = 39 months). A total of 89 patients (28.5%) experienced disease recurrence. Locoregional recurrence was observed in 24 patients (7.7%), while 63 patients (20.2%) developed distant metastases as their first site of progression. As of the time of this analysis (January 2025), 70 patients (23%) had died, including three patients who passed away without evidence of disease progression (due to sudden death, suicide, and small-cell lung cancer). Death, recurrence, and recurrence type stratified by cohort are summarized in Table 2.

Table 2. Recurrence and exitus stratified by cohort.
Patients who achieved a pCR had a significantly higher DFS (HR 0.21 CI95% 0.12-0.36, p<0.0001 and OS (HR 0.27 CI95% 0.15-0.49, p<0.0001) compared with those who did not achieve pCR (Figures 2A, B). Kaplan Meier curves and log-rank test for DFS and OS stratified by cohort are presented in Figures 3A, B. The median DFS and median OS were not reached in any of the three cohorts. Significant differences in DFS and OS were observed among the three cohorts according to the log-rank test (DFS: p < 0.00001; OS: p = 0.00005). However, no statistically significant differences were found between Cohort 2 and Cohort 3 in terms of DFS (p = 0.94) and OS (p = 0.34). The impact of multiple prognostic variables on DFS and OS — including menopausal status, < 40 or ≥ 40 years, Ki-67 index ≤ 50% or > 50%, tumour size <5 cm or ≥5 cm, lymph node status previous to surgery, achieving a pCR after NAC and adjuvant capecitabine — was evaluated using Cox regression analysis. Achieving a pCR was associated with a statistically significant lower risk of event in terms of both DFS (HR 0.25, 95% CI 0.133 – 0.467, p = 0.0001) and OS (HR 0.335, 95% CI 0.173– 0.646, p = 0.001). Additionally, Cox regression analysis revealed a significantly higher risk of events in terms of DFS (HR: 1.841, 95% CI: 1.201–2.821, p = 0.005) and OS (HR: 2.385, 95% CI: 1.445–3.939, p = 0.001) for patients with positive nodal status at diagnosis. Furthermore, patients with tumors >5 cm exhibited a significantly higher risk of events in terms of OS (HR: 1.742, 95% CI: 1.047–2.897, p = 0.033, Supplementary Tables 1, 2).
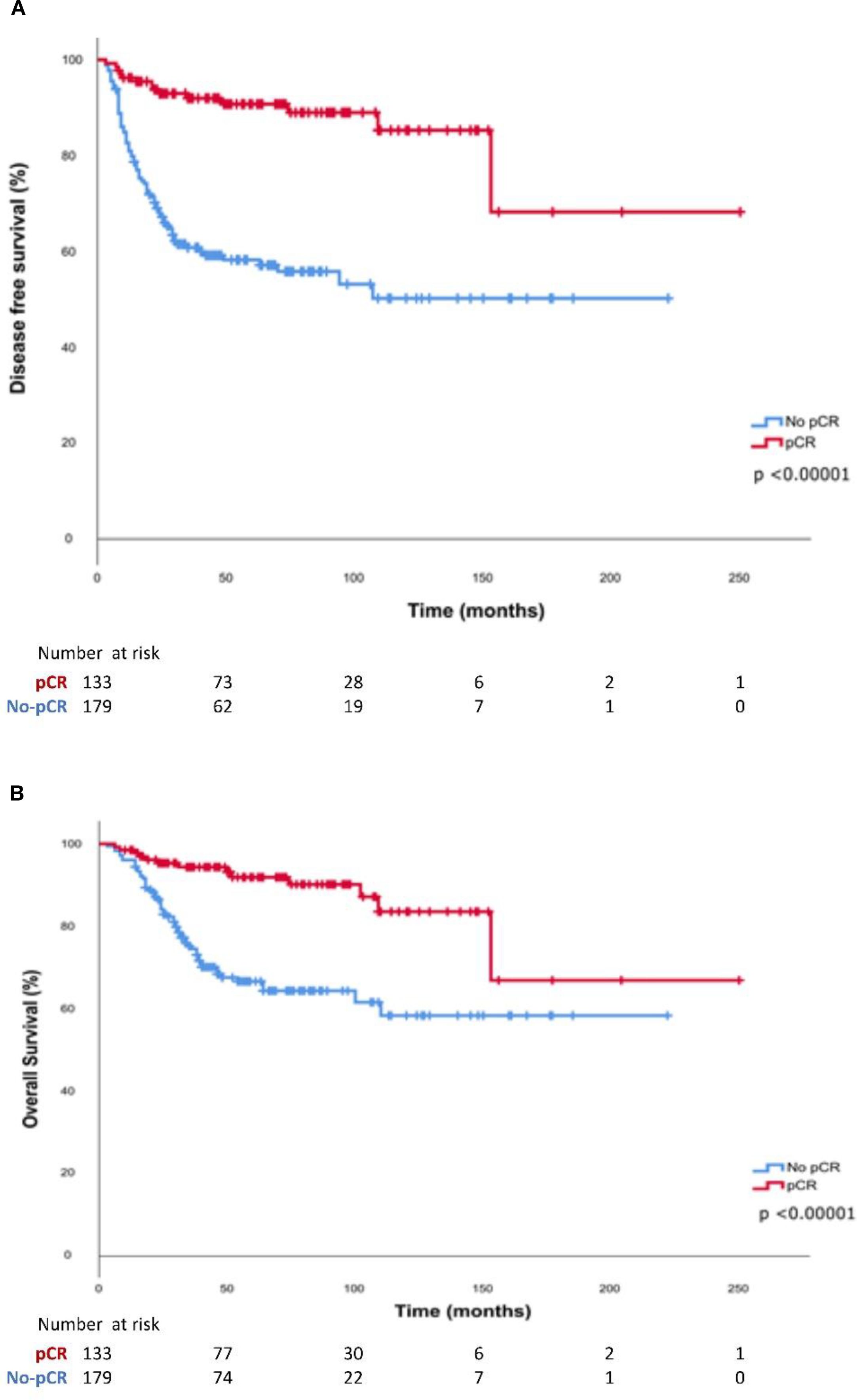
Figure 2. Kaplan-Meier curves of (A) Disease-free survival and (B) Overall survival according to pathological response after neoadjuvant treatment.
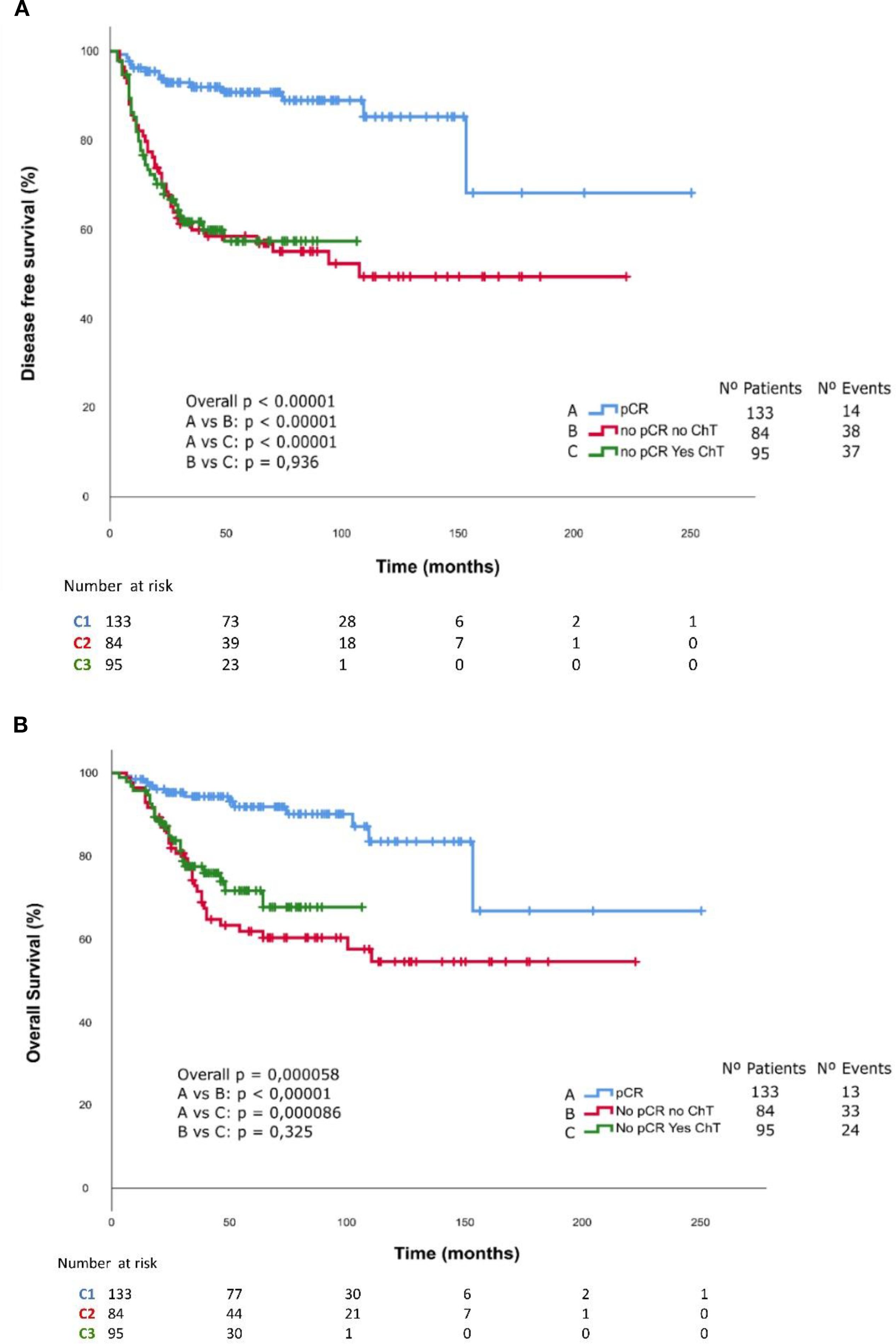
Figure 3. Kaplan-Meier curves of (A) Disease-free survival and (B) Overall survival stratified by cohort.
We conducted an exploratory analysis of DFS and OS stratified by germline mutation status within each cohort. Patients with undetermined germline status were excluded from this analysis. Among the 205 patients with available germline data, those carrying pathogenic mutations (n = 51) achieved significantly better outcomes in both DFS and OS compared with non-mutated patients (n = 154), with a DFS HR of 0.43 (95% CI = 0.20–0.96, p = 0.039) and an OS HR of 0.31 (95% CI = 0.11–0.88, p = 0.027).
Six subgroups were subsequently defined according to the three main cohorts (1, 2, and 3) and germline mutation status (positive or negative). Patients in Cohort 1, who achieved a pCR, demonstrated the most favourable survival outcomes. Notably, none of the patients within this cohort who carried a germline mutation experienced disease recurrence or death during follow-up.
In contrast, patients in Cohorts 2 and 3 who did not achieve pCR showed poorer survival outcomes, irrespective of their germline mutation status or receipt of adjuvant capecitabine. Kaplan–Meier survival curves for DFS and OS according to germline status are presented in Figures 4A, B.
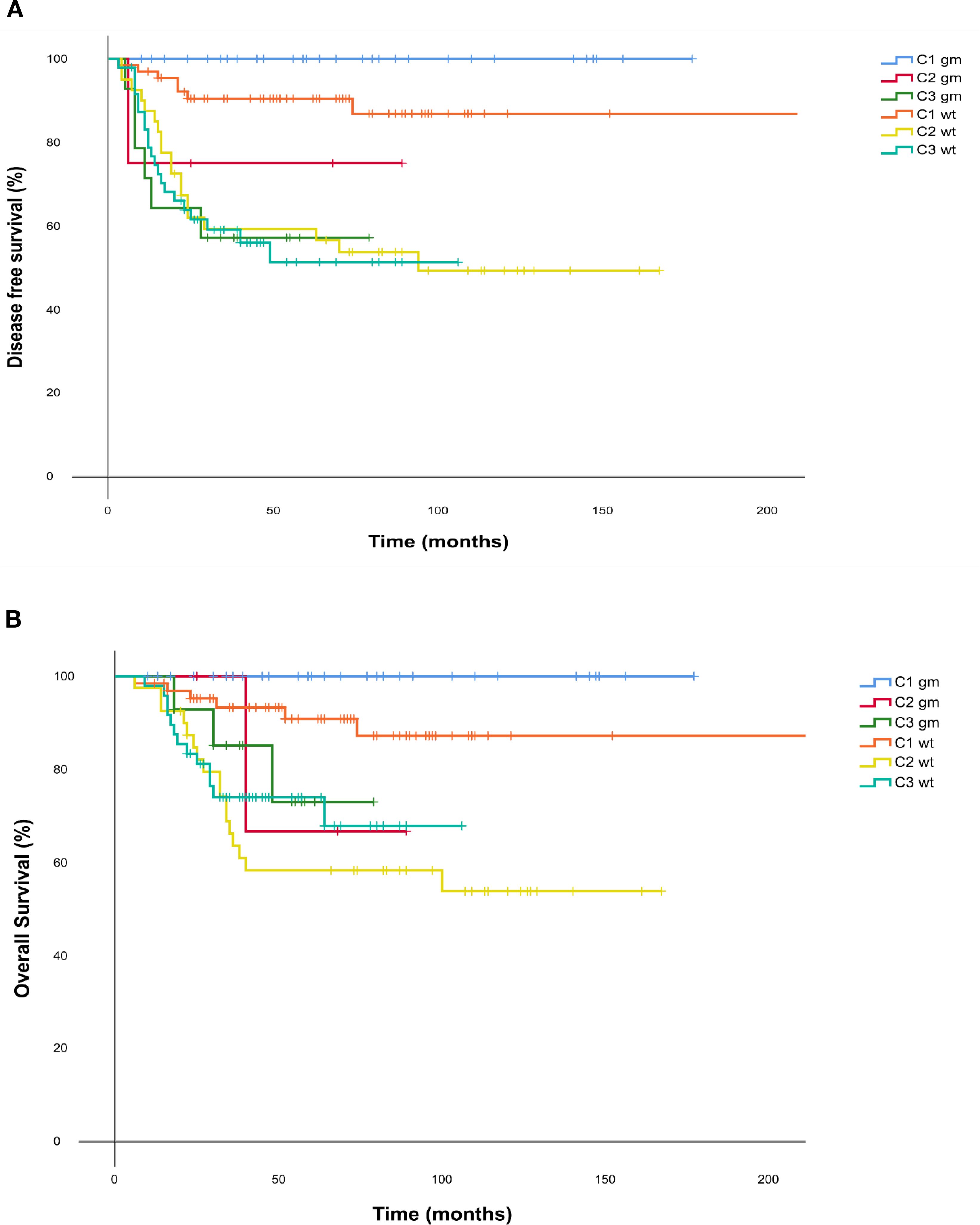
Figure 4. (A) Disease free survival and (B) Overall Survival Kaplan Meier curves for each cohort according to their mutational status. C1 = Cohort 1: pCR; C2 = Cohort 2: no pCR no adjuvant capecitabine; C3 = Cohort 3: no pCR yes adjuvant capecitabine. DFS, disease free survival; gm, germline mutated; OS, Overall survival; wt = wild type.
4 Discussion
In this retrospective study, we compared the outcome measured as DFS and OS of three cohorts of early TNBC patients treated with NAC: cohort 1 (patients who achieved a pCR); cohort 2 (not pCR and did not receive adjuvant chemotherapy); and cohort 3 (not pCR and adjuvant capecitabine). Our results demonstrated that patients who achieved a pCR (42.6%) had superior DFS and OS. However, Cohort 3 did not show an improved outcome compared to Cohort 2, suggesting the hypothesis that treatment with capecitabine in the absence of pCR after NAC may not provide a significant survival benefit in all patients with early TNBC.
The objective of precision medicine in TNBC implies that breast cancer treatment should be tailored based on the inherent risk of recurrence and individual sensitivity to different chemotherapies or alternative therapeutic approaches, such as targeted therapies or immunotherapy. First, it is essential to identify TNBC patients who require treatment beyond standard NAC. Two approaches may help in determining patients at the highest risk of recurrence and, therefore, in need of additional therapy. On an individual level, achieving a pCR is associated with improved survival (2, 5), whereas patients with residual disease (RD) face a higher risk of recurrence and mortality. Another strategy involves the use of highly sensitive diagnostic tests to detect and quantify minimal residual disease (MRD), such as circulating tumor cells (CTCs) or circulating tumor DNA (ctDNA), through blood-based “liquid biopsy” assays. The presence of these biomarkers during treatment has been linked to a less favorable prognosis in both early and advanced breast cancer (11, 12), although they do not yet have established predictive value.
Second, multiple clinical trials have explored the addition of novel treatment options to standard chemotherapy to improve patient outcomes. In this context, the phase III CREATE-X trial (6) aimed to identify a cohort of high-risk patients. The study included 910 women who had received standard NAC regimens and had RD after surgery. Patients were randomized to either no further therapy or six to eight cycles of sequential capecitabine. Capecitabine therapy improved 5-year DFS (70% vs. 56%) and OS (78.8% vs. 70.3%) in the subgroup of 286 women with TNBC. Based on these results, the use of adjuvant capecitabine in unselected TNBC patients with RD after NAC was established as the standard of care.
However, in the adjuvant setting, the addition of capecitabine—either concurrently, sequentially after standard chemotherapy, or as a metronomic regimen—has yielded controversial results in reducing the risk of recurrence. Furthermore, it substantially increases treatment toxicity without consistently improving OS (8, 13–16), or provides benefits only in certain subgroups of TNBC patients. For instance, in the phase III CIBOMA trial, only the non-basal TNBC subgroup (27% of patients, as expected) derived benefit from capecitabine, as observed in a retrospective and prespecified analysis (8). More recently, FOXC1, a transcriptional driver of cell plasticity and metastasis, was identified as a single biomarker assessed via standardized immunohistochemistry. This marker demonstrated the ability to identify basal-like breast cancer, further corroborating the lack of benefit of adjuvant capecitabine in basal TNBC subtyping according to PAM50 and IHC (17).
The phase III FinXX trial randomized patients to receive docetaxel with or without the addition of capecitabine, followed by epirubicin/cyclophosphamide. In the general population DFS and OS did not differ significantly between the groups after 10 years of follow up. Only in an exploratory subgroup analysis, a significant improvement in DFS and OS was observed in the TNBC subgroup, which comprised 202 patients (13% of the total population, 18). Furthermore, CREATE-X study included a preselected population with worse prognosis and a relative resistance to standard chemotherapy, conducted in an exclusively Asian population. This homogeneity may partially explain differences in capecitabine tolerance and efficacy (19). In contrast, studies based on real-world data and clinical experiences involving predominantly Caucasian populations, such as our study, provide valuable insights. In routine clinical practice, treatment strategies may differ from those applied in randomized controlled trials, making real-world studies a useful tool to assess the generalizability of trial results to broader, non-trial patient populations (20).
Preclinical models have supported the use of platinum agents in the basal TNBC subtype (21, 22). Addition of platinum agents to anthracycline and taxane consistently increased the pCR rates in clinical trials (23–25). Consequently, most oncologists have incorporated platinum agents into NAC regimens. However, these neoadjuvant trials were not powered to evaluate DFS or OS benefits. The results of the phase III EA1131 trial, which included patients with clinical stage II or III TNBC (basal vs. non-basal) and ≥1 cm residual disease in the breast post-NAC, demonstrated that adjuvant platinum agents did not improve outcomes and were associated with greater toxicity compared to capecitabine (26). Given that chemotherapy-based treatment may have reached the limit of its efficacy, novel therapeutic approaches are being explored for specific TNBC subgroups, particularly those with PD-L1-positive tumors or germline pathogenic BRCA mutations. However, only a fraction of these patients responds to immune checkpoint inhibitors (ICIs) or poly (ADP-ribose) polymerase (PARP) inhibitors, and even among responders, resistance and relapse frequently occur. The phase III Keynote-522 study demonstrated that the addition of pembrolizumab to NAC resulted in a statistically significant improvement in pCR rates, event-free survival, and OS (27). Another example is the phase III OlympiA trial, which included patients with HER2-negative early breast cancer with high-risk clinicopathological features and germline BRCA1 or BRCA2 pathogenic mutations who had received local treatment and neoadjuvant or adjuvant chemotherapy. The study compared one year of olaparib versus placebo, with most participants (81%) having TNBC. Patients who received olaparib had significantly improved distant DFS and OS, particularly among those who did not achieve a pCR. Notably, post-neoadjuvant capecitabine was not permitted in this trial, leaving the relative efficacy of olaparib compared to capecitabine in this setting unknown (28–30).
Subgroup analyses of the CREATE-X or GEICAM studies did not include germline BRCA mutation status, leaving the effect of adjuvant capecitabine in this population largely undefined. A correlative analysis of the GEICAM study, showed a decreased benefit from capecitabine in patients with basal-like tumors, which comprise the majority (~90%) of germline BRCA mutated breast cancer (6, 8, 31). Moreover, both a prespecified correlative analysis of the GEICAM/CIBOMA trial and findings from the EA1131 study suggest that patients with non-basal early-stage TNBC are more likely to derive benefit from adjuvant capecitabine (15, 26).
In our exploratory analysis, which grouped various germline mutations—predominantly BRCA1/2—we observed a trend toward improved outcomes among mutation carriers who achieved a pathological complete response (pCR), compared to non-carriers who also achieved a pCR.
Conversely, patients who failed to achieve a pCR exhibited poorer survival outcomes, regardless of germline mutation status or receipt of adjuvant capecitabine.
These findings should be interpreted with caution given the limited sample size, which may have restricted the ability to detect significant differences between subgroups. An increased sample size is necessary to determine whether our results are consistent with previously published findings in this setting.
Finally, our study has several limitations. As a retrospective study, establishing causal relationships is challenging due to the potential presence of unmeasured confounding factors. The lack of randomization may introduce biases that compromise the validity of the results, which are difficult to mitigate or correct. One potential limitation of our study is the temporal difference among the cohorts C1-C2 vs C3. This temporal gap may reflect improvements in diagnostic tools, surgical techniques and systemic treatments, which could have influenced patient outcomes. However, we attempted to minimize this potential bias by including clinicopathological and treatment-related variables in the multivariate model to adjust for possible confounders.
We believe that our findings provide relevant insights into the potential utility—or lack thereof—of adjuvant capecitabine in TNBC patients with residual disease (RD) after NAC in real-world settings. This is supported by the significant number of patients analyzed, the comparable clinico-pathological characteristics, and the similar NAC regimens used in Cohorts 2 and 3, along with an adequate follow-up period.
The visual differences observed in the Kaplan-Meier curves between Cohorts 2 and 3 in terms of OS may be attributed to differences in follow-up duration, as Cohort 3 had a shorter follow-up period than Cohort 2. With extended follow-up, the OS curve may more closely resemble the DFS curve, which are nearly overlapping.
In conclusion, adjuvant capecitabine may not provide a survival benefit for all TNBC patients with RD after NAC. A deeper understanding of distinct biological subtypes and molecular characteristics within RD will enable more personalized treatment decisions, optimizing therapeutic strategies for each patient subgroup while minimizing unnecessary toxicities.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statement
Ethical approval was not required for the studies involving humans because this retrospective study was conducted using previously collected and anonymized data; therefore, in accordance with current regulations, ethical committee approval was not required. The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
Author contributions
AG-O: Conceptualization, Data curation, Investigation, Methodology, Project administration, Supervision, Validation, Visualization, Writing – original draft, Writing – review & editing. GL-S: Conceptualization, Data curation, Formal Analysis, Investigation, Methodology, Resources, Software, Supervision, Validation, Visualization, Writing – original draft, Writing – review & editing. MZ: Conceptualization, Data curation, Investigation, Methodology, Supervision, Validation, Writing – original draft, Writing – review & editing. JP: Conceptualization, Data curation, Formal Analysis, Investigation, Methodology, Project administration, Supervision, Validation, Writing – original draft, Writing – review & editing. AL-P: Data curation, Methodology, Supervision, Validation, Writing – review & editing. AC: Conceptualization, Data curation, Methodology, Validation, Writing – review & editing. NR: Data curation, Methodology, Project administration, Supervision, Writing – review & editing. MI: Data curation, Investigation, Validation, Writing – review & editing. EV: Data curation, Validation, Writing – review & editing. BP: Data curation, Validation, Writing – review & editing. TD-R: Data curation, Investigation, Methodology, Supervision, Writing – review & editing. MD-R: Data curation, Validation, Writing – review & editing. FC: Data curation, Methodology, Supervision, Writing – review & editing. MB: Data curation, Supervision, Writing – review & editing. AR-D: Data curation, Methodology, Supervision, Writing – review & editing. EA: Data curation, Investigation, Methodology, Supervision, Validation, Writing – review & editing. AS-M: Conceptualization, Data curation, Formal Analysis, Investigation, Methodology, Project administration, Supervision, Validation, Visualization, Writing – original draft, Writing – review & editing.
Funding
The author(s) declare that no financial support was received for the research, and/or publication of this article.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Generative AI statement
The author(s) declare that no Generative AI was used in the creation of this manuscript.
Any alternative text (alt text) provided alongside figures in this article has been generated by Frontiers with the support of artificial intelligence and reasonable efforts have been made to ensure accuracy, including review by the authors wherever possible. If you identify any issues, please contact us.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fonc.2025.1648272/full#supplementary-material
References
1. Geyer CE, Sikov WM, Huober J, Rugo HS, Wolmark N, O'Shaughnessy J, et al. Long-term efficacy and safety of addition of carboplatin with or without veliparib to standard neoadjuvant chemotherapy in triple-negative breast cancer: 4-year follow-up data from BrighTNess, a randomized phase III trial. Ann Oncol. (2022) 33:384–94. doi: 10.1016/j.annonc.2022.01.009
2. Cortazar P, Zhang L, Untch M, Mehta K, Costantino JP, Wolmark N, et al. Pathological complete response and long-term clinical benefit in breast cancer: the CTNeoBC pooled analysis. Lancet. (2014) 384:164–72. doi: 10.1016/S0140-6736(13)62422-8
3. Carey LA, Dees EC, Sawyer L, Gatti L, Moore DT, Collichio F, et al. The triple negative paradox: primary tumor chemosensitivity of breast cancer subtypes. Clin Cancer Res. (2007) 13:2329–34. doi: 10.1158/1078-0432.CCR-06-1109
4. Liedtke C, Mazouni C, Hess KR, André F, Tordai A, Mejia JA, et al. Response to neoadjuvant therapy and long-term survival in patients with triple-negative breast cancer. J Clin Oncol. (2008) 26:1275–81. doi: 10.1200/JCO.2007.14.4147
5. Symmans WF, Wei C, Gould R, Yu X, Zhang Y, Liu M, et al. Long-term prognostic risk after neoadjuvant chemotherapy associated with residual cancer burden and breast cancer subtype. J Clin Oncol. (2017) 35:1049–60. doi: 10.1200/JCO.2015.63.1010
6. Masuda N, Lee SJ, Ohtani S, Im YH, Lee ES, Yokota I, et al. Adjuvant capecitabine for breast cancer after preoperative chemotherapy. N Engl J Med. (2017) 376:2147–59. doi: 10.1056/NEJMoa1612645
7. Joensuu H, Kellokumpu-Lehtinen PL, Huovinen R, Jukkola-Vuorinen A, Tanner M, Kokko R, et al. Adjuvant capecitabine in combination with docetaxel, epirubicin, and cyclophosphamide for early breast cancer: the randomized clinical finXX trial. JAMA Oncol. (2017) 3:793. doi: 10.1001/jamaoncol.2016.6120
8. Lluch A, Barrios CH, Torrecillas L, Ruiz-Borrego M, Bines J, Segalla J, et al. Phase III trial of adjuvant capecitabine after standard neo-/adjuvant chemotherapy in patients with early triple-negative breast cancer (GEICAM/2003-11_CIBOMA/2004-01). J Clin Oncol. (2020) 38:203–13. doi: 10.1200/JCO.19.00904
9. Von Minckwitz G, Rezai M, Loibl S, Fasching PA, Huober J, Tesch H, et al. Capecitabine in addition to anthracycline- and taxane-based neoadjuvant treatment in patients with primary breast cancer: phase III GeparQuattro study. J Clin Oncol. (2010) 28:2015–23. doi: 10.1200/JCO.2009.23.8303
10. Fisher B, Bryant J, Wolmark N, Mamounas E, Brown A, Fisher ER, et al. Effect of preoperative chemotherapy on the outcome of women with operable breast cancer. J Clin Oncol. (1998) 16:2672–85. doi: 10.1200/JCO.1998.16.8.2672
11. Radovich M, Jiang G, Hancock BA, Chitambar C, Nanda R, Falkson C, et al. Association of circulating tumor DNA and circulating tumor cells after neoadjuvant chemotherapy with disease recurrence in patients with triple-negative breast cancer: preplanned secondary analysis of the BRE12–158 randomized clinical trial. JAMA Oncol. (2020) 6:1410–5. doi: 10.1001/jamaoncol.2020.2295
12. Magbanua MJM, Swigart LB, Wu HT, Hirst GL, Yau C, Wolf DM, et al. Circulating tumor DNA in neoadjuvant-treated breast cancer reflects response and survival. Ann Oncol. (2021) 32:229–39. doi: 10.1016/j.annonc.2020.11.007
13. Li J, Yu K, Pang D, Wang C, Jiang J, Yang S, et al. Adjuvant capecitabine with docetaxel and cyclophosphamide plus epirubicin for triple-negative breast cancer (CBCSG010): an open-label, randomized, multicenter, phase III trial. J Clin Oncol. (2020) 38:1774–84. doi: 10.1200/JCO.19.02474
14. Wang X, Wang SS, Huang H, Cai L, Zhao L, Peng RJ, et al. Effect of capecitabine maintenance therapy using lower dosage and higher frequency vs observation on disease-free survival among patients with early-stage triple-negative breast cancer who had received standard treatment: the SYSUCC-001 randomized clinical trial. JAMA. (2020) 325:1. doi: 10.1001/jama.2020.23370
15. Asleh K, Lluch A, Goytain A, Barrios C, Wang XQ, Torrecillas L, et al. Triple-negative PAM50 non-basal breast cancer subtype predicts benefit from extended adjuvant capecitabine. Clin Cancer Res. (2023) 29:389–400. doi: 10.1158/1078-0432.CCR-22-2191
16. O’Shaughnessy J, Koeppen H, Xiao Y, Lackner MR, Paul D, Stokoe C, et al. Patients with slowly proliferative early breast cancer have low five-year recurrence rates in a phase III adjuvant trial of capecitabine. Clin Cancer Res. (2015) 21:4305–11. doi: 10.1158/1078-0432.CCR-15-0636
17. Rojo Todo FG, Taylor CR, Barrios CH, Torrecillas L, Ruiz-Borrego M, Bines J, et al. Non-basal subtype defined by FOXC1 expression as an independent predictor of capecitabine efficacy in the triple negative breast cancer GEICAM/2003-11_CIBOMA/2004–01 trial. J Clin Oncol. (2024) 42:516–6. doi: 10.1200/JCO.2024.42.16_suppl.516
18. Joensuu H, Kellokumpu-Lehtinen PL, Huovinen R, Jukkola-Vuorinen A, Tanner M, Kokko R, et al. Adjuvant capecitabine, docetaxel, cyclophosphamide, and epirubicin for early breast cancer: final analysis of the randomized FinXX trial. J Clin Oncol. (2012) 30:11–8. doi: 10.1200/JCO.2011.35.4639
19. Haller DG, Cassidy J, Clarke SJ, Cunningham D, Van Cutsem E, Hoff PM, et al. Potential regional differences for the tolerability profiles of fluoropyrimidines. J Clin Oncol. (2008) 26:2118–23. doi: 10.1200/JCO.2007.15.2090
20. Rothwell PM. External validity of randomised controlled trials: “to whom do the results of this trial apply? Lancet. (2005) 365:82–93. doi: 10.1016/S0140-6736(04)17670-8
21. Farmer H, McCabe H, Lord CJ, Tutt AN, Johnson DA, Richardson TB, et al. Targeting the DNA repair defect in BRCA mutant cells as a therapeutic strategy. Nature. (2005) 434:917–21. doi: 10.1038/nature03445
22. Graeser M, McCarthy A, Lord CJ, Savage K, Hills M, Salter J, et al. A marker of homologous recombination predicts pathologic complete response to neoadjuvant chemotherapy in primary breast cancer. Clin Cancer Res. (2010) 16:6159–68. doi: 10.1158/1078-0432.CCR-10-1027
23. Von Minckwitz G, Schneeweiss A, Loibl S, Salat C, Denkert C, Rezai M, et al. Neoadjuvant carboplatin in patients with triple-negative and HER2-positive early breast cancer (GeparSixto; GBG 66): a randomised phase 2 trial. Lancet Oncol. (2014) 15:747–56. doi: 10.1016/S1470-2045(14)70160-3
24. Sikov WM, Berry DA, Perou CM, Singh B, Cirrincione CT, Tolaney SM, et al. Impact of the addition of carboplatin and/or bevacizumab to neoadjuvant once-per-week paclitaxel followed by dose-dense doxorubicin and cyclophosphamide on pathologic complete response rates in stage II to III triple-negative breast cancer: CALGB 40603 (Alliance). J Clin Oncol. (2014) 33:13. doi: 10.1200/JCO.2014.57.0572
25. Telli ML, Hellyer J, Audeh W, Jensen KC, Bose S, Timms KM, et al. Homologous recombination deficiency (HRD) status predicts response to standard neoadjuvant chemotherapy in patients with triple-negative or BRCA1/2 mutation-associated breast cancer. Breast Cancer Res Treat. (2018) 168:625–30. doi: 10.1007/s10549-017-4624-7
26. Mayer IA, Zhao F, Arteaga CL, and Arteaga WF. Randomized phase III postoperative trial of platinum-based chemotherapy versus capecitabine in patients with residual triple-negative breast cancer following neoadjuvant chemotherapy: ECOG-ACRIN EA1131. J Clin Oncol. (2021) 39:2539. doi: 10.1200/JCO.21.00976
27. Schmid P, Cortes J, Dent R, McArthur H, Pusztai L, Kümmel S, et al. Overall survival with pembrolizumab in early-stage triple-negative breast cancer. N Engl J Med. (2024) 391:1981–91. doi: 10.1056/NEJMoa2409932
28. Tutt ANJ, Garber JE, Kaufman B, Viale G, Fumagalli D, Rastogi P, et al. Adjuvant olaparib for patients with BRCA1- or BRCA2-mutated breast cancer. N Engl J Med. (2021) 384:2394–405. doi: 10.1056/NEJMoa2105215
29. Geyer CE, Garber JE, Gelber RD, Yothers G, Taboada M, Ross L, et al. Overall survival in the OlympiA phase III trial of adjuvant olaparib in patients with germline pathogenic variants in BRCA1/2 and high-risk, early breast cancer. Ann Oncol. (2022) 33:1250–68. doi: 10.1016/j.annonc.2022.09.159
30. Morganti S, Bychkovsky BL, Poorvu PD, Garrido-Castro AC, Weiss A, Block CC, et al. Adjuvant olaparib for germline BRCA carriers with HER2-negative early breast cancer: evidence and controversies. Oncologist. (2023) 28:565–74. doi: 10.1093/oncolo/oyad123
Keywords: triple negative breast cancer, pathological complete response, adjuvant capecitabine, early breast cancer, CreateX, CIBOMA, BRCA1, BRCA2
Citation: Godoy-Ortíz A, Lendínez-Sánchez G, Zalabardo M, Pascual J, López-Pascual A, Cantero A, Ribelles N, Iglesias M, Villar E, Pajares B, Díaz-Redondo T, Domínguez-Recio ME, Carabantes F, Bermejo MJ, Rueda-Domínguez A, Alba E and Sánchez-Muñoz A (2025) Real-world data analysis of adjuvant capecitabine for triple-negative breast cancer after neoadjuvant chemotherapy. Front. Oncol. 15:1648272. doi: 10.3389/fonc.2025.1648272
Received: 16 June 2025; Accepted: 27 October 2025;
Published: 17 November 2025.
Edited by:
Xudong Zhu, University of Kentucky, United StatesCopyright © 2025 Godoy-Ortíz, Lendínez-Sánchez, Zalabardo, Pascual, López-Pascual, Cantero, Ribelles, Iglesias, Villar, Pajares, Díaz-Redondo, Domínguez-Recio, Carabantes, Bermejo, Rueda-Domínguez, Alba and Sánchez-Muñoz. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Gonzalo Lendínez-Sánchez, Z29ubGVuc2FAaG90bWFpbC5jb20=
†These authors have contributed equally to this work and share first authorship