 Margret Jensdottir1,2*
Margret Jensdottir1,2* Ole Solheim3,4
Ole Solheim3,4 Alba Corell5,6Eddie de Dios5,6†Tora Dunås5Alexander Fletcher-Sandersjöö1,2
Alba Corell5,6Eddie de Dios5,6†Tora Dunås5Alexander Fletcher-Sandersjöö1,2 Sasha Gulati3,4Klas Holmgren7,8
Sasha Gulati3,4Klas Holmgren7,8 Francesco Latini9Ruby Mahesparan10,11
Francesco Latini9Ruby Mahesparan10,11 Peter Milos12,13
Peter Milos12,13 Alice Neimantaite5
Alice Neimantaite5 Henrietta Nittby Redebrandt14,15Lars Kjelsberg Pedersen16Rickard L. Sjöberg7,8Björn Sjögren12,13Gregor Tomasevic15Øystein Vesterli Tveiten10,11
Henrietta Nittby Redebrandt14,15Lars Kjelsberg Pedersen16Rickard L. Sjöberg7,8Björn Sjögren12,13Gregor Tomasevic15Øystein Vesterli Tveiten10,11 Tomás Gómez Vecchio5Maria Zetterling9Jiri Bartek Jr1,2,17
Tomás Gómez Vecchio5Maria Zetterling9Jiri Bartek Jr1,2,17 Asgeir S Jakola4,5,6
Asgeir S Jakola4,5,6- 1Department of Clinical Neuroscience, Karolinska Institutet, Stockholm, Sweden
- 2Department of Neurosurgery, Karolinska University Hospital, Stockholm, Sweden
- 3Department of Neuromedicine and Movement Science, Faculty of Medicine and Health Sciences, Norwegian University of Science and Technology, NTNU, Trondheim, Norway
- 4Department of Neurosurgery, St. Olavs Hospital, Trondheim University Hospital, Trondheim, Norway
- 5Institute of Neuroscience and Physiology, Sahlgrenska Academy, University of Gothenburg, Gothenburg, Sweden
- 6Department of Neurosurgery, Sahlgrenska University Hospital, Gothenburg, Sweden
- 7Department of Neurosurgery, University Hospital of Northern Sweden, Umeå, Sweden
- 8Department of Clinical Sciences, Neuroscience, Umeå University, Umeå, Sweden
- 9Department of Medical Sciences, Section of Neurosurgery, Uppsala University Hospital, Uppsala, Sweden
- 10Department of Clinical Medicine, Faculty of Medicine, University of Bergen, Bergen, Norway
- 11Department of Neurosurgery, Haukeland University Hospital, Bergen, Norway
- 12Department of Neurosurgery, Linköping University Hospital, Linköping, Sweden
- 13Department of Biomedical and clinical Sciences, Linköping University, Linköping, Sweden
- 14Department of Clinical Sciences, Skåne University Hospital, Lund, Sweden
- 15Department of Neurosurgery, Skåne University Hospital, Lund, Sweden
- 16Department of Neurosurgery, University Hospital of North Norway, Tromsø, Tromsø, Sweden
- 17Department of Neurosurgery, Copenhagen University Hospital Rigshospitalet, Copenhagen, Copenhagen, Denmark
Background and objectives: Maximal safe resection is the cornerstone of diffuse low-grade glioma (dLGG) management, although epidemiological data are limited. We aim to explore surgical selection, techniques, and outcomes in a population-based cohort.
Materials and methods: This study utilized a multi-center case series (9 out of 10 neurosurgical departments in Norway and Sweden) of all adults (≥18 years) with histopathologically verified supratentorial dLGG, WHO grade 2, undergoing primary surgery from 2012-2017. Complications within 30 days and neurological outcomes at 3 months were assessed. Pre- and postoperative MRIs were reviewed centrally, blinded to patient outcome and center.
Results: Of 517 included patients, 217 (41.7%) were female, and the mean (SD) age was 44.5 (15.0) years. Biopsy only was performed in 119 (23.0%) patients (13.8-38.9% across centers), and 398 (77.0%) underwent resection (61.1-86.2%). Intraoperative neurophysiological monitoring (IONM) was used in 142 (35.7%, 0-58.7%) resections. The biopsy-only patients were older (52.7 years vs. 42.1 years, P<.001), had larger tumors (56.6 ml vs. 31.9 ml, P<.001), and these tumors were more often eloquently located (86.6% vs. 56.5%, P<.001). The median (IQR) extent of resection (EOR) was 82.9% (63.3-97.7%), 69.7-100.0% across centers. The median (IQR) residual tumor was 4.6 ml (0.5-19.9 ml), 0.0-14.1 ml across centers. Age and histopathology were the most important predictors of EOR. New/worsened neurological deficits occurred in 165 patients (41.5%), 23.1-66.7% across centers, and persisted in 19 (4.8%, 0-22.7%) at 3 months after surgery. A complication was observed in 87 patients (21.4%, 0-31.7%), with 12 patients (3.1%, 0-9.8%) having grade III-IV complications.
Conclusions: We found that surgical selection was associated with age, tumor size, and location. The median EOR in a population-based cohort was 83%, with age and tumor biology being significant predictors. EOR did not correlate with higher risks or worse neurological outcomes. We provide an epidemiological perspective demonstrating a variation in surgical selection and techniques reflecting persistent controversy in dLGG management.
Introduction
Maximal safe resection remains a key therapeutic approach for diffuse low-grade gliomas (dLGG) and provides significant survival benefits (1–5). Upfront surgery is recommended for diagnostic and therapeutic purposes. Biopsy only is an adverse prognostic factor for overall survival (6–8). Investigating surgery selection at a population level can help us understand the context of the surgical literature.
The reported risk of post-operative neurological worsening after resection varies, ranging from 2-40% (9–13). Intraoperative neurophysiological monitoring (IONM) reportedly increases tumor resection while minimizing risks of permanent neurological deficits (14, 15).
Although IONM is widely accepted in specialized centers, epidemiological data are limited. Generalizing findings from highly specialized hospitals to broader clinical settings is difficult (16, 17). Hence, controversies persist regarding the influence of surgical selection and techniques on outcome and presumed resectability of dLGG.
The aim of this multi-center study was to investigate the correlation between surgical selection and use of surgical adjuncts and the effectiveness and safety of surgery on a population level. Specifically, we focused on short term outcomes: extent of resection (EOR), adverse events, and postoperative neurological deficits. Secondarily, we aimed to explore inter-hospital variations.
Materials and methods
Ethics and approvals
The regional committee of Western Sweden (EPN reference 705/17) and The Regional Committee for Medical and Health Research Ethics in Central Norway (REC reference 2017/1780) approved the study with a waiver of informed consent.
Patient population and definition of cohort
This study is part of a Scandinavian multicenter project, including all neurosurgical departments performing glioma surgery in Norway and Sweden. The publicly funded health care systems, with compliant regional referral, practically eliminate any referral bias. The study design, population, data collection, and variables have been described previously (18).
All adults (≥18 years) with histopathologically confirmed supratentorial dLGG, World Health Organization (WHO) grade 2, undergoing primary surgery (biopsy or resection) between January 1, 2012, and December 31, 2017, were included in the database. Tumors with anaplastic features (WHO grade 3-4) were excluded. Histopathological classification was based on the classification system in use at time of surgery (WHO 2007 or WHO 2016).
This study includes all patients from centers providing radiological data for central review (9/10).
Study variables
Patient characteristics, diagnostic work-up, and surgical techniques were retrospectively retrieved from medical records and pseudonymized data entered in electronic case report forms (CRFs). IONM parameters were extracted from surgical records and neurophysiological reports and data were collected on mapping techniques, whether the patients was awake or under general anesthesia, indication for mapping (language, motor, sensory, visual, or other), and whether passive monitoring with MEP was performed. Preoperative Magnetic Resonance Imaging (MRI) was analyzed locally for tumor location, laterality, contrast enhancement, and presumed eloquent area, defined according to Chang et al. (3).
MRIs were extracted from the respective hospitals PACS (picture archiving and communication system, Sectra™), with volumetrics performed centrally. Trained raters segmented the tumor volumes on pre- and postoperative MRI from T2-weighted or FLAIR images or, in exceptional cases, contrast-enhanced T1-weighted images, using 3D Slicer software (19). All segmentations were validated by a neurosurgeon (ASJ) with significant experience in dLGG management and research, including volumetric assessment. Raters were blinded to patient clinical status and treating center at the time of segmentation.
EOR was calculated as [(preoperative tumor volume − postoperative tumor volume)/preoperative tumor volume] × 100%. Gross total resection (GTR) was defined as 100% EOR/0.0 ml of tumor remnant.
New postoperative neurological deficits were recorded in detail from the retrospective review of medical records. Functional outcome was assessed at 3 months with persistent deficits considered permanent. Permanent deficits were classified as minor (i.e., limited impact on daily life: can work, drive, travel, perform physical activities, and live a rather normal socioprofessional life) or major (i.e., impact on daily life: limitation with respect to work, drive, travel, and/or physical activities and thus can´t live a normal socioprofessional life). Adverse events occurring within 30 days postoperatively were categorized using the Landriel-Ibanez Classification (LIC) (20). The LIC grades severity of complications are as follows: grade I being any non-life-threatening event not expected postoperatively (e.g. new onset seizure, pneumonia, or urinary tract infection); grade II is any complication requiring intervention (e.g. lumbar drainage or re-operation due to cerebrospinal fluid leakage); grade III is any life-threatening complication (e.g. brain swelling, acute postoperative hematoma, or hydrocephalus); and grade IV is fatal. We considered grade I complications mild, grade II moderate, and grade III severe. This is a reasonable scaling since neurological deficits were reported separately, avoiding underreporting major deficits in the grade I category.
Statistics
Statistical analysis was performed in IBM SPSS Statistics for Windows, Version 25.0 (Armonk, NY: IBM Corp) and R (version 4.1.2). Normality of continuous data was explored using the Shapiro-Wilk test. Central tendencies are presented as means ± SD or median and interquartile range (IQR) for normally distributed and skewed data, respectively. Comparison between groups was performed using Mann-Whitney U test for non-parametric data and independent two samples t-test for parametric data. Chi-square tests or Fishers exact test were used in intergroup comparisons of categorical variables, and categorical data are expressed as numbers and percentages. All tests were two-sided and statistical significance was set at P <.05. Scatterplots were used to assess relationships in the data. A univariable and forced-entry multivariable logistic regression was used to identify predictors of postoperative permanent neurological deficits. To determine predictors of EOR (ranging from 0 to 100%), univariable and forced-entry zero-one inflated beta regression (ZOIB) analyses were employed. ZOIB was preferred based on the clustering nature of EOR around 100%.
Results
Patient characteristics and clinical presentation
We included 517 patients with a summary of preoperative patient characteristics, tumor classification, intraoperative techniques, and outcomes in Tables 1–3 and Supplementary Table 1. The average age was 44.5 years and 41.7% were female. Seizures were the most common presenting symptom (N = 305, 59.0%). A majority had a Karnofsky Performance Score (KPS) of 90-100 (N = 390, 74.9%). For an overview of tumor location, see Table 1 and Figures 1A-F. Tumors were presumed to involve an eloquent area in 328 patients (63.4%), ranging from 33.3-68.2% across centers.
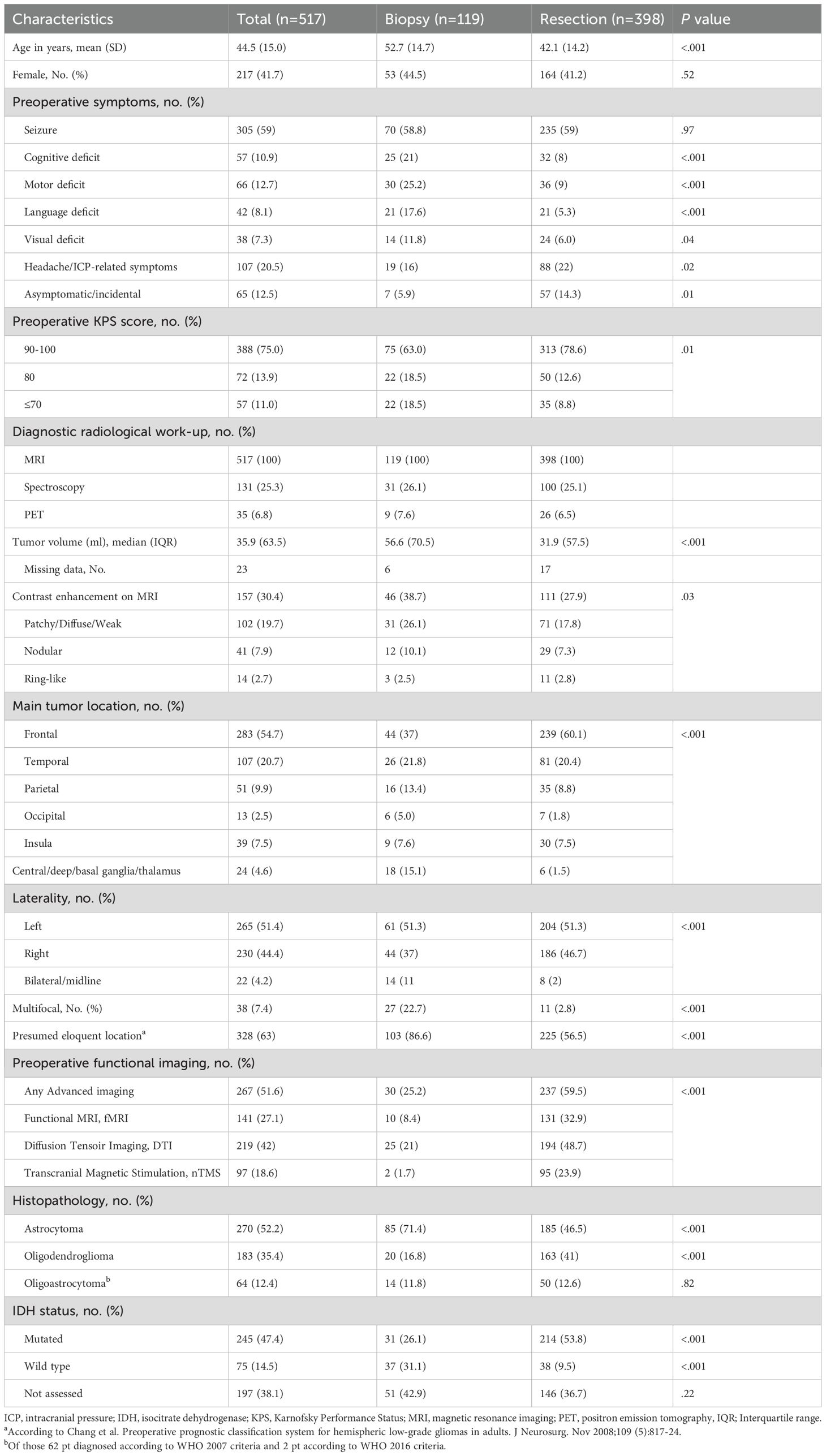
Table 1. Summary of epidemiological patient characteristics.
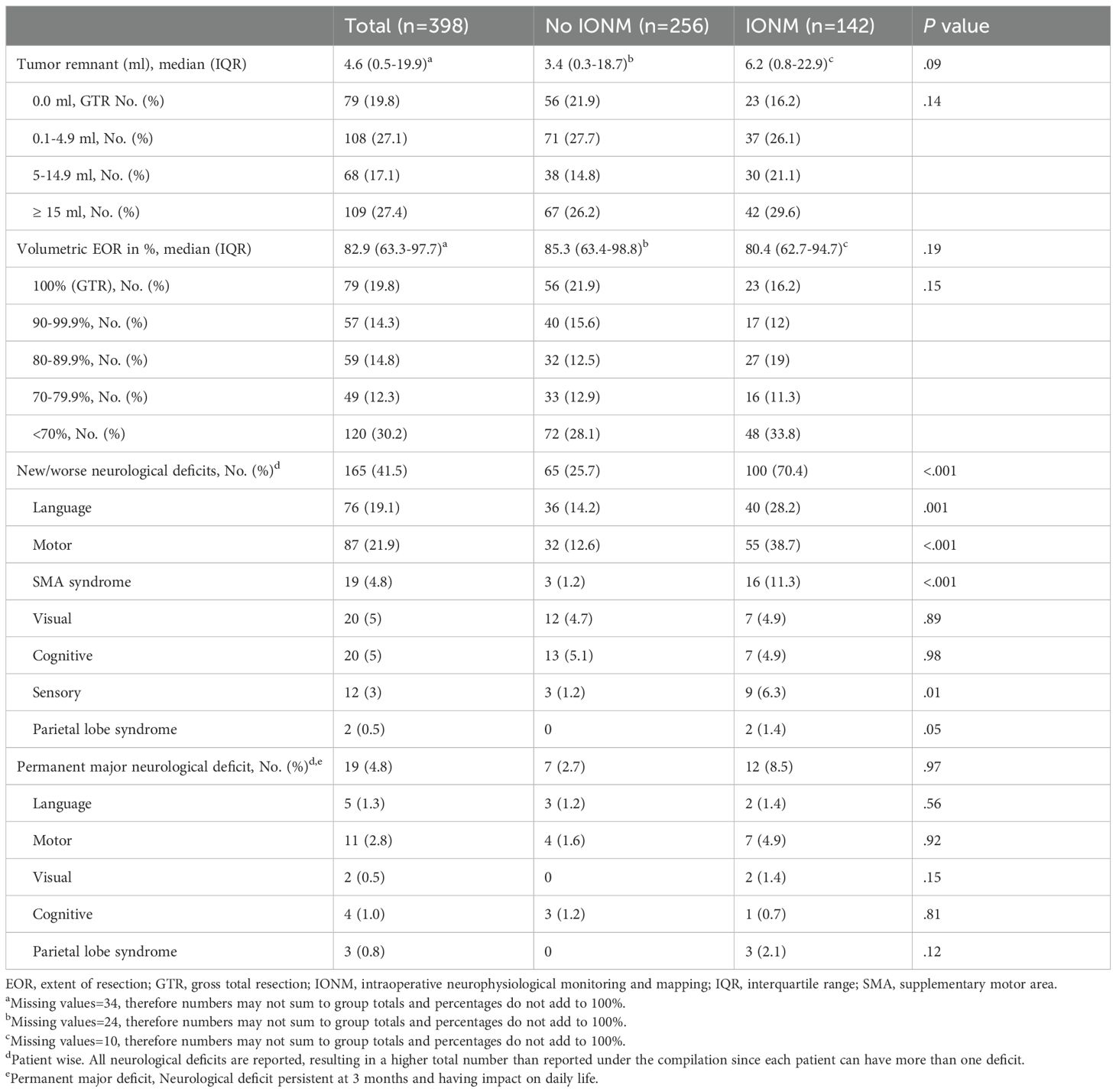
Table 2. Surgical, oncological, and functional outcomes for patients undergoing resection.
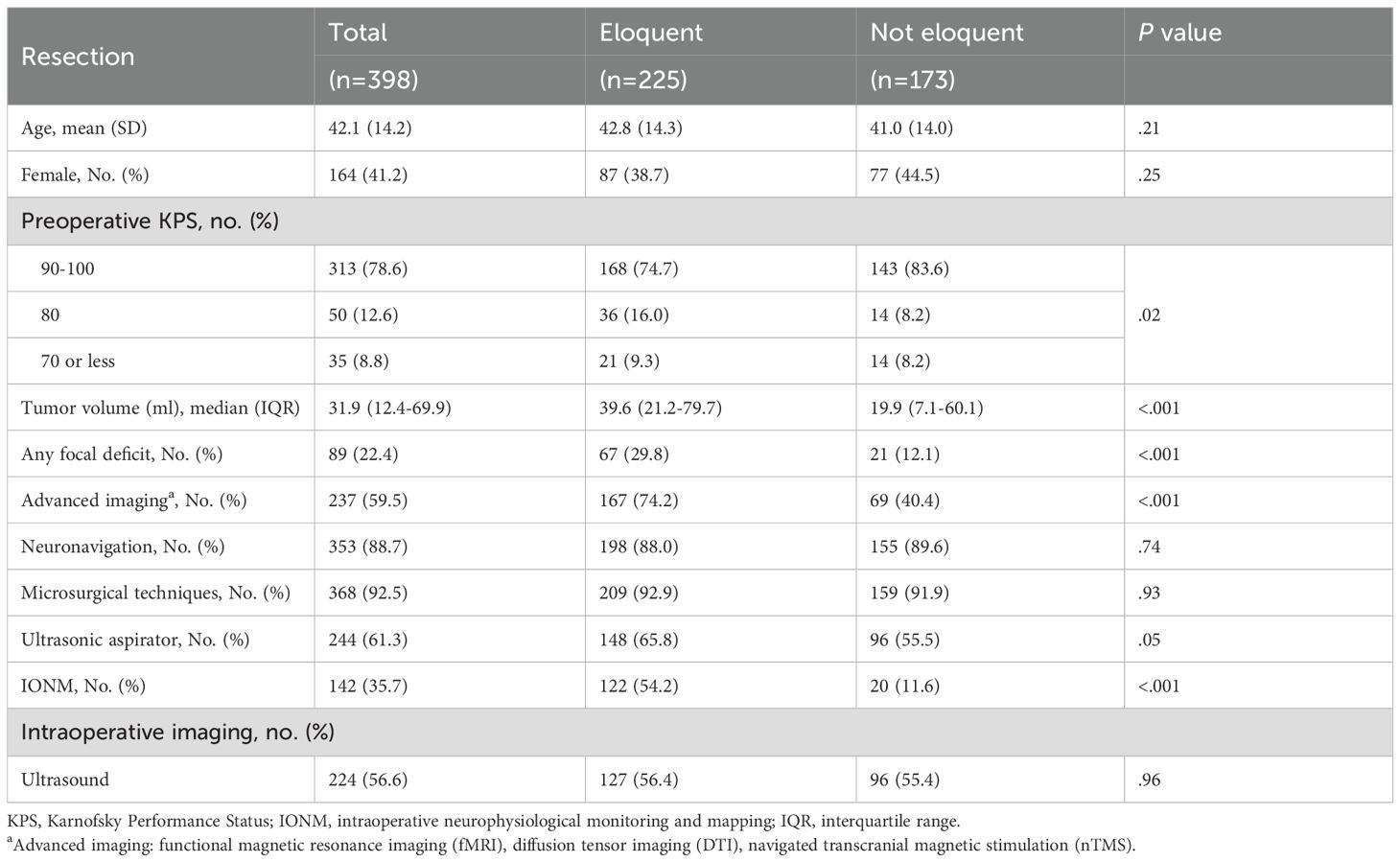
Table 3. Preoperative work up, surgical techniques, and perioperative treatment for tumors in a presumed eloquent area vs not eloquent area.
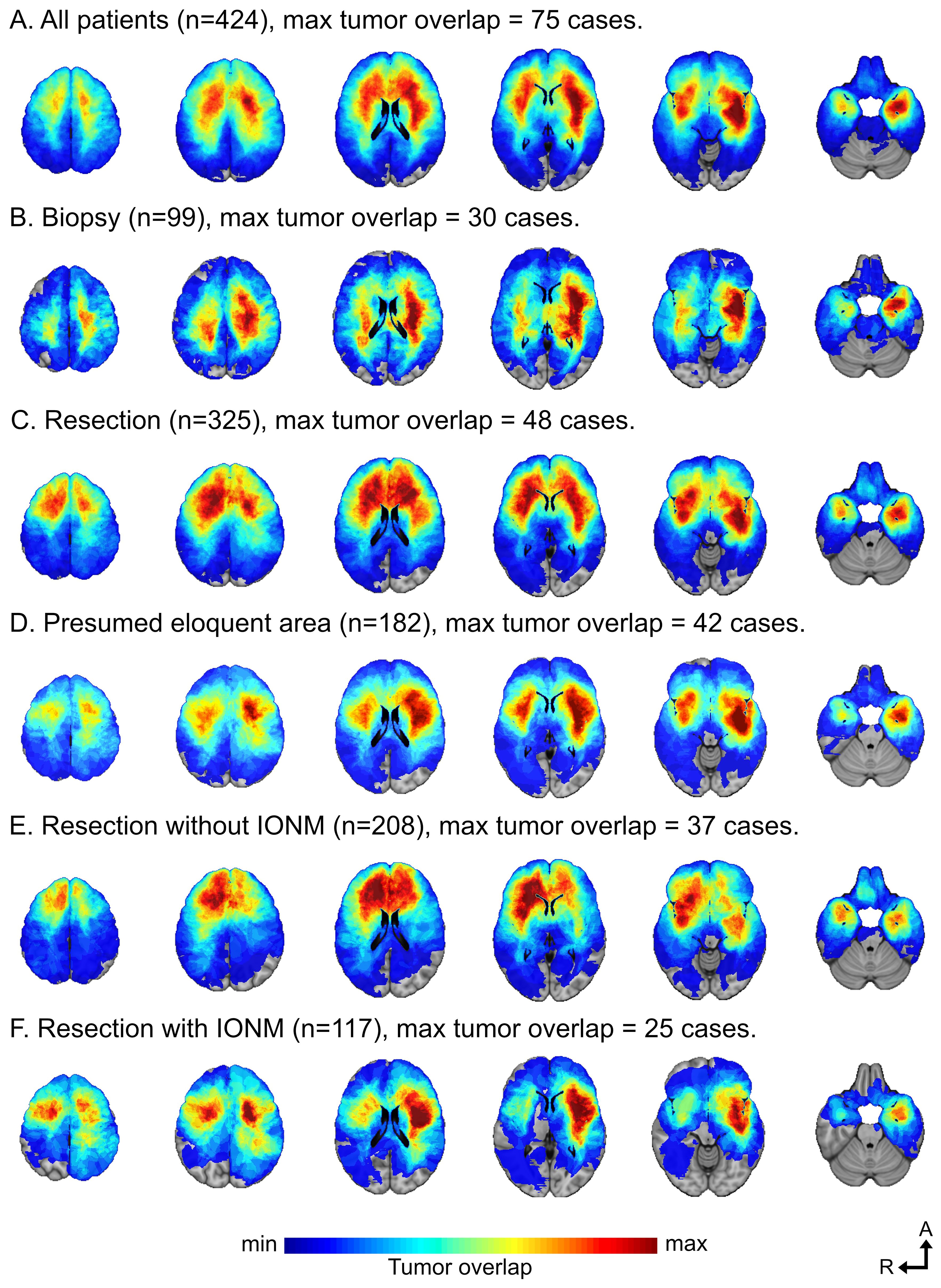
Figure 1. (A-F) A location heatmap showing spatial distribution for all tumors (A). Separate heatmaps for the tumor locations in patients selected for biopsy (B), resection (C), presumed eloquent area (D), resection without IONM (E), and resection with IONM (F). Figures based on available tumor segmentations on Montreal Neurological Institute (MNI) space (axial slices 50, 35, 20, 5, -10 and -25 mm). The scale of tumor overlap was adjusted to the maximum overlap for each group (A-F).
Preoperative work-up and surgical selection
Biopsy only was performed in 119 patients (23%, 13.8%-38.9% across centers) and 398 (77%, 61.1-86.2%) underwent resection. Advanced functional imaging (functional Magnetic Resonance Imaging (fMRI), Diffusion Tensor Imaging (DTI), or navigated Transcranial Magnetic Stimulation (nTMS)) was used in 267 patients (51.6%, 25.0-94.0%), (Table 1). IONM was employed in 142 (35.7%, 0-58.7) resected patients and only in four (3.4%) of the biopsied patients.
The patients undergoing biopsy had a cluster of negative prognostic factors including older age, lower KPS scores, larger and multifocal tumors, higher proportion of contrast enhancing tumors, and more frequent involvement of presumed eloquent brain regions. (Table 1) Further, the tumor location heatmaps demonstrate a more prominent subcortical infiltration in the biopsy cohort compared to more cortical overlap in resected patients (Figures 1B, C). In patients with available isocitrate dehydrogenase (IDH) mutation status, IDH wild-type (wt) tumors were more common. The IDH status also showed a correlation to contrast enhancement with a significantly higher proportion of contrast enhancement in IDH wt status tumors compared to IDH mutated, 32.0% and 22.4% respectively (p<0.001). Complications related to biopsies are listed in Supplementary Table 2.
Surgical techniques and outcome
Neuronavigation and microsurgical techniques were used in most resections (N = 353, 88.7% and N = 368, 92.5%, respectively). Intraoperative imaging was solely performed with ultrasound (N = 224, 56.6%, 11.5%-100% across centers). Intraoperative mapping or monitoring was performed in 142 resections (35.7%, 0-58.7% across centers). Awake surgery was performed in 62 patients (15.6%, 0-28.6% across centers), asleep mapping only in 80 patients (20.1%, 0-34.6% across centers), and three patients (0.8%) were exclusively monitored during asleep resection without any mapping with direct electrical stimulation (DES) (Supplementary Table 1).
Given the significance of IONM in dLGG surgery and the challenges of tumors located in presumed eloquent areas, we analyzed cases in depth with respect to these factors. The differences in baseline between cases in a presumed eloquent vs non-eloquent area are presented in Table 3, and Supplementary Table 1 provides a detailed description of indications and type of IONM (asleep/awake/indication for mapping/monitoring). In short, significantly more patients with a tumor in a presumed eloquent area were investigated with advanced imaging techniques and selected for resection with IONM compared to patients with tumors in a presumed non-eloquent area (Table 3).
Table 2 outlines the overall surgical outcome. The median tumor remnant was 4.6 ml (0.0-14.1 across centers) and the median EOR was 82.9% (69.7-100.0% across centers [demonstrated in Supplementary Figure 1)], with 79 patients (19.8%, 4.5-50.0%) achieving GTR. Comparing centers, we found no correlation between the EOR and either biopsy rates, the frequency of preoperative advanced imaging, or the use of IONM (Figures 2A-C). A similar pattern was observed in the subgroup of eloquent area tumors (Supplementary Figures 2D, E). In a subgroup analysis of all tumors in a presumed eloquent area, a significantly higher EOR was observed with IONM (77.0% versus 67.6%, p=0.019) and a smaller median tumor remnant (8.1 ml versus 12.5 ml, p=0.062).

Figure 2. (A-F) Scatterplots displaying relationship between key outcome parameters for all resected tumors by patient centers (dots), each center represented with a different color. (A) The relationship between proportion of biopsy and median EOR. (B) The relationship between proportion of advanced imaging and median EOR. (C) The relationship between proportion of IONM and median EOR. (D) The relationship between proportion of advanced imaging and proportion of permanent major neurological deficit. (E) The relationship between proportion of IONM and proportion of permanent major neurological deficit. (F) The relationship between median EOR and proportion of permanent major neurological deficits.
We found that age predicted a lower EOR with a -1.57 or -1.51 unit decrease in EOR for each increased year of age for all tumors and tumors in eloquent areas, respectively (Figure 3). Histopathology significantly affected EOR, with oligodendroglioma predicting a higher EOR (Figure 3). The median EOR (IQR) for oligodendroglioma was 86.2% (69.1-98.3%) and was 79.4% (56.7-98.5%) for astrocytoma. A summary of a univariable and multivariable analysis of possible predictors of EOR is provided in Supplementary Table 3.
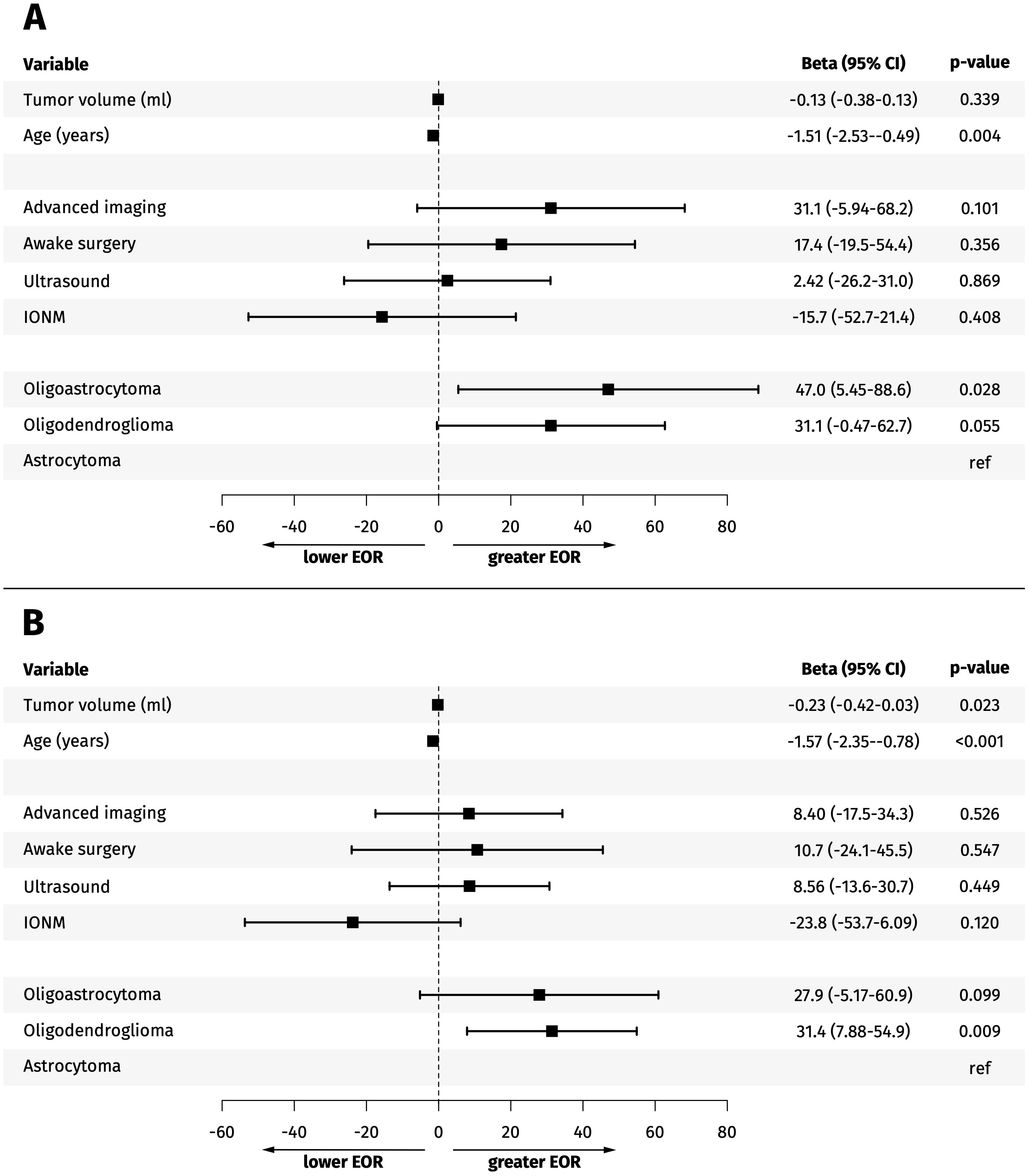
Figure 3. (A, B) Forest plot. Multivariable analysis of predictors of extent of resection (EOR) for resected tumors in a presumed eloquent area (A) and all resected tumors (B).
Functional outcome
New or worsened neurological deficits occurred in 165 patients (41.5%, 23.1-66.7% across centers), with only 19 patients (4.8%, 0.0-22.7%) suffering permanent major deficits and no correlation between deficits and EOR (Figure 2F).
Comparing resections with or without IONM showed a higher frequency of permanent major deficits (8.5% vs 2.7%) and postoperative seizures (9.2% vs 3.2%) in patients resected with IONM. A comprehensive table of neurological deficits and outcomes related to indications for IONM is available in Supplementary Tables 4, 5.
Comparing centers, we found no correlation between neurological deficits and different imaging practices or use of IONM (Figures 2D, E, Supplementary Figures 2D, E). Nor could we identify any predictors of permanent major deficits (Supplementary Table 3).
To further analyze any association between outcome and the use of IONM, we plotted the percentage of EOR versus percentage of permanent major deficits for all tumors and tumors in eloquent areas and grouped by resection with or without IONM for each center (Supplementary Figure 3). We observed a lower percentage of permanent major deficits with an increased EOR with the use of IONM in tumors in eloquent areas. Contrarily, a higher rate of permanent major deficits was observed with a lower EOR, despite use of IONM.
Surgical complications occurred in 87 resected patients (21.9%, 0.0-31.7% across centers). A detailed description is found in Supplementary Table 6. A moderate (Grade II) or severe (Grade III) complication occurred in 32 patients (8.0%, 3.6-12.2%). Severe complications were mostly postoperative hemorrhage (e.g., cavity hematoma and epidural hematoma), occurring in 11 patients (2.8%,1.6-9.8%). A single patient (0.3%) suffered from a Grade IV complication, with urosepsis as the suspected cause of death.
Discussion
This population-based cohort demonstrates that patients selected for biopsy only have a distinct profile compared to those undergoing resection, characterized by worse tumor burden, older age, and lower functional status. Further, we found that median EOR is approximately 83% without clear predictors other than age and histology. We also describe the epidemiological perspective on short-term outcomes, with transient neurological deficits and minor permanent deficits dominating.
In this study, which was not restricted to IDH-mutated tumors, IDH wildtype (IDH wt) tumors were identified as a confounder, given their association with location, contrast enhancement, age, treatment, and prognosis according to the WHO classification applicable during the study period (21, 22). As expected, IDH wt tumors were more often biopsied. However, surgical decision making is done without knowledge of dLGG subclassification, mostly influenced by age, cognitive function, KPS, tumor location, and imaging findings as negative prognostic factors (23, 24). More prominent subcortical infiltration, shown in the location heat maps, correlated with higher rates of cognitive decline and neurological symptoms. This then suggests its potential as a marker for surgical planning, as proposed by Ng et al (25),, identifying clinical, radiological, and oncological markers associated with effective onco-functional balance. This population-based setting demonstrates the biopsy group as heavily selected. Comparing biopsy with resection from a single institution, in registries etc., is intrinsically flawed unless capturing unique situations, as in Jakola et al (2, 26), who compared regions favoring different surgical strategies.
We investigated relationships between preoperative assessments, surgical adjuncts, and short-term outcomes to identify factors that could aid surgical decision-making. Particular attention was given to IONM due to its significant role in dLGG treatment within the surgical community.
As expected, a correlation was found between using IONM and advanced imaging for presumed eloquent tumors. However, a substantial variation between centers in the frequency of use is in concordance with previous studies, which show great heterogeneity in the imaging practice for dLGG in Europe, reflecting limited evidence of effectiveness (27, 28). Observed variations did not affect EOR or rates of neurological complications. This contrasts with a previous randomized trial by Wu et al (29),, who found an improved outcome with presurgical planning with DTI. Functional imaging can identify eloquent areas prior to surgery and reportedly the preoperative use of nTMS correlated with improved outcome (30, 31). This discrepancy with our findings could be attributed to selective use of advanced imaging modalities in cases where higher risks are anticipated, potentially leading to confounding by indication.
The predilection for use of IONM in presumed eloquent areas and convincing evidence at the time in favor of the use of IONM to maximize safe resection (14, 15, 32, 33) corresponds to a yearly increase in use of IONM during the study period (18). This increasing trend and learning curve for the use of IONM probably explains the overlapping location in the heatmap for biopsied patients and those resected with IONM. Only 15.6% underwent awake surgery. Given landmark studies on the contribution of awake mapping for improved functional outcome and survival (14, 34, 35) it could be argued that underutilization has occurred. We noted a variance across centers in the use of awake surgery (0-28.6%), and the yearly increase in the use of IONM may reflect that a transition was ongoing throughout these years. The reason for the low percentage of awake surgeries, particularly at some centers, may be due to institutional culture or surgeon preferences, a knowledge gap, or a more protracted learning curve outside highly specialized centers (13, 36–38). However, from our sample, it must still be emphasized that we do not see a clear signal of improved outcomes in centers more frequently performing surgeries under the guidance of IONM in general or awake surgery specifically.
The importance of awake surgery to achieve long-term functional outcomes has recently been demonstrated in a landmark paper by Ng et al. (39) In a large cohort of 600 patients with a newly diagnosed IDH mutant grade 2 glioma, awake resection contributed to a median survival of 20 years and a median preservation of KPS ≥80% of 14.7 years after surgery.
The EOR and tumor remnant achieved in this population compares favorably to previous reports. Capelle et al (40), in a French multicenter database, the largest cohort of dLGG to date, reports a median EOR of 76.8%, median tumor remnant of 10 ml, and 11.9% undergoing GTR. Wijnenga et al (41), report a similar median EOR of 76.1%, 10.95 ml median tumor remnant, and 15.4% GTR in a cohort of 228 patients from two Dutch centers. On the other hand, Hervey-Jumper et al (16), in a cohort of 392 patients from a large volume specialized center reports a higher median EOR (92.0%), lower median tumor remnant (2.6 ml), and 30.9% GTR, which may reflect a combination of being an experienced high-volume center and patient selection. The factors identified to correlate with EOR were tumor location and histopathology. The importance of histopathology has previously been reported and eloquent regions are more frequently found in proximity to IDH-mutated astrocytomas (42). The importance of tumor location for EOR underscores the need for objective preoperative evaluation to identify eloquent area location and estimating resectability (43, 44). This is essential for surgical decision-making where improved selection aims to avoid high-risk surgery in patients with a low chance of achieving a meaningful EOR.
The importance of surgical selection and maximal safe resection has been further consolidated by a recent publication by The Response Assessment in Neuro-Oncology (RANO) resect group (45). This is an international and multidisciplinary group, with the aim to standardize the measurement of extent of resection and its impact on survival in adult diffuse glioma, classified by WHO 2021 classification. They stress the importance of quantification of extent of resection, such as the objective volumetric assessment performed in our study, to facilitate comparison between studies.
Based on a comprehensive review of the relevant literature, Karschnia et al. have established an algorithm to help estimate expected survival gains from different degrees of resection, considering tumor subtype, patient factors, risk of deficits, etc., to guide which patients are likely to benefit most from more aggressive surgery. For slower-growing tumor types, such as IDH-mutant astrocytomas and oligodendrogliomas, these benefits unfold over years/decades (45).
We observed a significantly higher incidence of new deficits in patients who underwent resection with IONM, in concordance with the literature reporting a common occurrence of neurological worsening in presumed eloquent tumors (15, 46). Fortunately, there was no significant difference between the subgroups in terms of permanent major deficits. Additionally, no correlation between increased extent of resection (EOR) and a higher frequency of deficits or adverse events was observed. Nor did we find significant variation across centers.
The challenge is to maximize the resection in highly eloquent areas. In our subgroup analysis we found a significantly higher EOR in presumed eloquent areas when using IONM without a higher risk of permanent deficits. This finding contrasts with other studies suggesting that more extensive resection correlates with worse outcomes in eloquent areas. Coburger et al (47),, in a German multicenter study evaluating the outcome of surgery for dLGG in eloquent areas, reported 10% permanent severe deficits and increased deficits with a higher EOR. However, other studies have emphasized the tumor location in eloquent areas as a possible risk factor for survival due to less extensive resection, further emphasizing the controversies regarding the resectability of dLGG (34, 48, 49).
We observed a lower proportion of permanent major deficits with more complete resection and, contrarily, more deficits with lower extent of resection despite the use of IONM, although mainly driven by an outlier. This reflects the importance of patient selection since some patients will not benefit from resection regardless of the use of IONM due to tumor location and degree of white matter infiltration. These patients should be identified prior to surgery to avoid unnecessary risks associated with less meaningful attempts of surgical resection (43). Improvement in detecting subcortical infiltration in preoperative imaging could aid in surgical selection.
Most reported permanent deficits were considered minor, although 4.8% had deficits with an impact on their daily life. The comparison of our results to the literature is somewhat hampered due to the lack of use of standardized reporting systems.
We demonstrate that achieving a high EOR is feasible in population-based cohorts, without a high risk of major permanent deficits. These findings can aid in preoperative patient counseling by providing realistic information on expectations and risk profiles and facilitate shared decision-making.
Limitations
An inherent limitation is the retrospective nature of the study. Additionally, a variance across centers of the frequency of presumed eloquent tumors, not expected in a population-based setting, reflects some risk of bias. However, the use of tumor maps displaying the true tumor location complements this to some extent.
Comparison of our results to the current literature, with molecularly defined subgroups according to the WHO 2021 classification, is somewhat hampered by the limited availability of IDH mutation status and the histopathological classification based on the system in use at time of surgery. However, IDH mutation status was available in 63.3% of the resected patients and only a minority were IDHwt. Therefore, excluding this limited number of patients would not significantly alter the results, and the risk of bias is considered low.
The major strength is the large population-based cohort with a multi-center approach across two countries with low rates of missing data. Further, a central review of radiological data, blinded to patient functional outcome and treating center, grants the study high generalizability.
Conclusion
Age, tumor volume, and eloquence determine surgical selection. Age and histopathology, not surgical adjuncts, are the main predictors of EOR. Variation in surgical practices across centers in seemingly uniform health care systems reflect persistent controversies in dLGG management. Our results underscore the importance of careful patient selection to optimize dLGG treatment and standardized reporting from population-based settings to facilitate guidelines on surgical decision-making.
Data availability statement
The datasets presented in this article are not readily available because the data supporting findings of this study are available within the paper and its Supplementary Materials. The raw data of the study are not available due to restrictions in the ethical permits. Requests to access the datasets should be directed to bWFyZ3JldC5qZW5zZG90dGlyQGtpLnNl.
Ethics statement
The studies involving humans were approved by The Swedish Ethical Review Authority Etikprövningsmyndigheten Box 2110 750 02 Uppsala Sweden Regional Committee for Medical an Health Research Ethics in Central Norway Kongens gate 14, 0153 Oslo Norway. The studies were conducted in accordance with the local legislation and institutional requirements. The ethics committee/institutional review board waived the requirement of written informed consent for participation from the participants or the participants’ legal guardians/next of kin because Retrospective study, review of patient records. No study intervention.
Author contributions
MJ: Conceptualization, Formal Analysis, Investigation, Methodology, Writing – original draft, Writing – review & editing. OS: Conceptualization, Formal Analysis, Writing – review & editing, Methodology, Supervision. AC: Writing – review & editing. ED: Writing – review & editing. TD: Writing – review & editing. AF-S: Writing – review & editing, Formal analysis. SG: Writing – review & editing. KH: Writing – review & editing. FL: Writing – review & editing. RM: Writing – review & editing. PM: Writing – review & editing. AN: Writing – review & editing. HR: Writing – review & editing. LP: Writing – review & editing. RS: Writing – review & editing. BS: Writing – review & editing. GT: Writing – review & editing. ØT: Writing – review & editing. TV: Writing – review & editing. MZ: Writing – review & editing. JB: Writing – review & editing, Supervision. AJ: Conceptualization, Supervision, Writing – review & editing.
Funding
The author(s) declare that no financial support was received for the research and/or publication of this article.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Generative AI statement
The author(s) declare that no Generative AI was used in the creation of this manuscript.
Any alternative text (alt text) provided alongside figures in this article has been generated by Frontiers with the support of artificial intelligence and reasonable efforts have been made to ensure accuracy, including review by the authors wherever possible. If you identify any issues, please contact us.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fonc.2025.1703756/full#supplementary-material
Supplementary Figure 1 | Boxplot displaying EOR in each patient center.
Supplementary Figure 2 | Scatterplots displaying relationship between key outcome parameters in resected tumors in presumed eloquent area by patient centers (dots), with each center represented with a different color. (A) The relationship between proportion of biopsy and median EOR. (B)The relationship between proportion of advanced imaging and median EOR. (C) The relationship between proportion of IONM and median EOR. (D) The relationship between proportion of advanced imaging and proportion of permanent major neurological deficit. (E) The relationship between proportion of IONM and proportion of permanent major neurological deficit. (F) The relationship between median EOR and proportion of permanent major neurological deficits.
Supplementary Figure 3 | Bubble charts were used to illustrate the relationship between surgical and functional outcomes based on case volume and the use of IONM per center. The percentage of EOR versus percentage of permanent major deficits was plotted for all tumors and tumors in a presumed eloquent area and grouped by resection with or without IONM. Each dot represents a patient center, and the dot size represents case volume at the respective center (the scale for dot size is shown in figure legend).
Abbreviations
dLGG, diffuse low-grade glioma; EOR, extent of resection; GTR, Gross total resection; IDH, isocitrate dehydrogenase; IONM, Intraoperative neurophysiological monitoring; LIC, Landriel-Ibanez Classification.
References
1. Roelz R, Strohmaier D, Jabbarli R, Kraeutle R, Egger K, Coenen VA, et al. Residual tumor volume as best outcome predictor in low grade glioma - A nine-years near-randomized survey of surgery vs. Biopsy. Sci Rep. (2016) 6:32286. doi: 10.1038/srep32286
2. Jakola AS, Myrmel KS, Kloster R, Torp SH, Lindal S, Unsgard G, et al. Comparison of a strategy favoring early surgical resection vs a strategy favoring watchful waiting in low-grade gliomas. JAMA. (2012) 308:1881–8. doi: 10.1001/jama.2012.12807
3. Chang EF, Smith JS, Chang SM, Lamborn KR, Prados MD, Butowski N, et al. Preoperative prognostic classification system for hemispheric low-grade gliomas in adults. J Neurosurg. (2008) 109:817–24. doi: 10.3171/JNS/2008/109/11/0817
4. McGirt MJ, Chaichana KL, Attenello FJ, Weingart JD, Than K, Burger PC, et al. Extent of surgical resection is independently associated with survival in patients with hemispheric infiltrating low-grade gliomas. Neurosurgery. (2008) 63:700–7; author reply 7–8. doi: 10.1227/01.NEU.0000325729.41085.73
5. Smith JS, Chang EF, Lamborn KR, Chang SM, Prados MD, Cha S, et al. Role of extent of resection in the long-term outcome of low-grade hemispheric gliomas. J Clin Oncol. (2008) 26:1338–45. doi: 10.1200/JCO.2007.13.9337
6. Weller M, van den Bent M, Preusser M, Le Rhun E, Tonn JC, Minniti G, et al. EANO guidelines on the diagnosis and treatment of diffuse gliomas of adulthood. Nat Rev Clin Oncol. (2021) 18:170–86. doi: 10.1038/s41571-020-00447-z
7. Youland RS, Schomas DA, Brown PD, Nwachukwu C, Buckner JC, Giannini C, et al. Changes in presentation, treatment, and outcomes of adult low-grade gliomas over the past fifty years. Neuro Oncol. (2013) 15:1102–10. doi: 10.1093/neuonc/not080
8. Sanai N, Chang S, and Berger MS. Low-grade gliomas in adults. J Neurosurg. (2011) 115:948–65. doi: 10.3171/2011.7.JNS101238
9. Gravesteijn BY, Keizer ME, Vincent A, Schouten JW, Stolker RJ, and Klimek M. Awake craniotomy versus craniotomy under general anesthesia for the surgical treatment of insular glioma: choices and outcomes. Neurol Res. (2018) 40:87–96. doi: 10.1080/01616412.2017.1402147
10. Gupta DK, Chandra PS, Ojha BK, Sharma BS, Mahapatra AK, and Mehta VS. Awake craniotomy versus surgery under general anesthesia for resection of intrinsic lesions of eloquent cortex–a prospective randomised study. Clin Neurol Neurosurg. (2007) 109:335–43. doi: 10.1016/j.clineuro.2007.01.008
11. Hervey-Jumper SL, Li J, Lau D, Molinaro AM, Perry DW, Meng L, et al. Awake craniotomy to maximize glioma resection: methods and technical nuances over a 27-year period. J Neurosurg. (2015) 123:325–39. doi: 10.3171/2014.10.JNS141520
12. Magill ST, Han SJ, Li J, and Berger MS. Resection of primary motor cortex tumors: feasibility and surgical outcomes. J Neurosurg. (2018) 129:961–72. doi: 10.3171/2017.5.JNS163045
13. Nossek E, Matot I, Shahar T, Barzilai O, Rapoport Y, Gonen T, et al. Failed awake craniotomy: a retrospective analysis in 424 patients undergoing craniotomy for brain tumor. J Neurosurg. (2013) 118:243–9. doi: 10.3171/2012.10.JNS12511
14. Duffau H, Lopes M, Arthuis F, Bitar A, Sichez JP, Van Effenterre R, et al. Contribution of intraoperative electrical stimulations in surgery of low grade gliomas: a comparative study between two series without (1985-96) and with (1996-2003) functional mapping in the same institution. J Neurol Neurosurg Psychiatry. (2005) 76:845–51. doi: 10.1136/jnnp.2004.048520
15. De Witt Hamer PC, Robles SG, Zwinderman AH, Duffau H, and Berger MS. Impact of intraoperative stimulation brain mapping on glioma surgery outcome: a meta-analysis. J Clin Oncol. (2012) 30:2559–65. doi: 10.1200/JCO.2011.38.4818
16. Hervey-Jumper SL, Zhang Y, Phillips JJ, Morshed RA, Young JS, McCoy L, et al. Interactive effects of molecular, therapeutic, and patient factors on outcome of diffuse low-grade glioma. J Clin Oncol. (2023) 41:2029–42. doi: 10.1200/JCO.21.02929
17. Scherer M, Ahmeti H, Roder C, Gessler F, Jungk C, Pala A, et al. Surgery for diffuse WHO grade II gliomas: volumetric analysis of a multicenter retrospective cohort from the german study group for intraoperative magnetic resonance imaging. Neurosurgery. (2020) 86:E64–e74. doi: 10.1093/neuros/nyz397
18. Munkvold BKR, Solheim O, Bartek J Jr., Corell A, de Dios E, Gulati S, et al. Variations in the management of diffuse low-grade gliomas-A Scandinavian multicenter study. Neurooncol Pract. (2021) 8:706–17. doi: 10.1093/nop/npab054
19. Fedorov A, Beichel R, Kalpathy-Cramer J, Finet J, Fillion-Robin JC, Pujol S, et al. 3D Slicer as an image computing platform for the Quantitative Imaging Network. Magn Reson Imaging. (2012) 30:1323–41. doi: 10.1016/j.mri.2012.05.001
20. Landriel Ibanez FA, Hem S, Ajler P, Vecchi E, Ciraolo C, Baccanelli M, et al. A new classification of complications in neurosurgery. World Neurosurg. (2011) 75:709–15; discussion 604–11. doi: 10.1016/j.wneu.2010.11.010
21. Metellus P, Coulibaly B, Colin C, de Paula AM, Vasiljevic A, Taieb D, et al. Absence of IDH mutation identifies a novel radiologic and molecular subtype of WHO grade II gliomas with dismal prognosis. Acta Neuropathol. (2010) 120:719–29. doi: 10.1007/s00401-010-0777-8
22. Qi S, Yu L, Li H, Ou Y, Qiu X, Ding Y, et al. Isocitrate dehydrogenase mutation is associated with tumor location and magnetic resonance imaging characteristics in astrocytic neoplasms. Oncol Lett. (2014) 7:1895–902. doi: 10.3892/ol.2014.2013
23. Pignatti F, van den Bent M, Curran D, Debruyne C, Sylvester R, Therasse P, et al. Prognostic factors for survival in adult patients with cerebral low-grade glioma. J Clin Oncol. (2002) 20:2076–84. doi: 10.1200/JCO.2002.08.121
24. Corell A, Carstam L, Smits A, Henriksson R, and Jakola AS. Age and surgical outcome of low-grade glioma in Sweden. Acta Neurol Scand. (2018) 138:359–68. doi: 10.1111/ane.12973
25. Ng S and Duffau H. Brain plasticity profiling as a key support to therapeutic decision-making in low-grade glioma oncological strategies. Cancers (Basel). (2023) 15. doi: 10.3390/cancers15143698
26. Jakola AS, Pedersen LK, Skjulsvik AJ, Myrmel K, Sjåvik K, and Solheim O. The impact of resection in IDH-mutant WHO grade 2 gliomas: a retrospective population-based parallel cohort study. J Neurosurg. (2022) 137:1321–1328. doi: 10.3171/2022.1.JNS212514
27. Freyschlag CF, Krieg SM, Kerschbaumer J, Pinggera D, Forster MT, Cordier D, et al. Imaging practice in low-grade gliomas among European specialized centers and proposal for a minimum core of imaging. J Neurooncol. (2018) 139:699–711. doi: 10.1007/s11060-018-2916-3
28. Fouke SJ, Benzinger T, Gibson D, Ryken TC, Kalkanis SN, and Olson JJ. The role of imaging in the management of adults with diffuse low grade glioma. J Neuro-Oncol. (2015) 125:457–79. doi: 10.1007/s11060-015-1908-9
29. Wu JS, Zhou LF, Tang WJ, Mao Y, Hu J, Song YY, et al. Clinical evaluation and follow-up outcome of diffusion tensor imaging-based functional neuronavigation: a prospective, controlled study in patients with gliomas involving pyramidal tracts. Neurosurgery. (2007) 61:935–48; discussion 48–9. doi: 10.1227/01.neu.0000303189.80049.ab
30. Ille S, Sollmann N, Butenschoen VM, Meyer B, Ringel F, and Krieg SM. Resection of highly language-eloquent brain lesions based purely on rTMS language mapping without awake surgery. Acta Neurochir (Wien). (2016) 158:2265–75. doi: 10.1007/s00701-016-2968-0
31. Sollmann N, Kelm A, Ille S, Schröder A, Zimmer C, Ringel F, et al. Setup presentation and clinical outcome analysis of treating highly language-eloquent gliomas via preoperative navigated transcranial magnetic stimulation and tractography. Neurosurg Focus. (2018) 44:E2. doi: 10.3171/2018.3.FOCUS1838
32. Bello L, Gallucci M, Fava M, Carrabba G, Giussani C, Acerbi F, et al. Intraoperative subcortical language tract mapping guides surgical removal of gliomas involving speech areas. Neurosurgery. (2007) 60:67–80; discussion –2. doi: 10.1227/01.NEU.0000249206.58601.DE
33. Soffietti R, Baumert BG, Bello L, von Deimling A, Duffau H, Frénay M, et al. Guidelines on management of low-grade gliomas: report of an EFNS-EANO Task Force. Eur J Neurol. (2010) 17:1124–33. doi: 10.1111/j.1468-1331.2010.03151.x
34. Chang EF, Clark A, Smith JS, Polley MY, Chang SM, Barbaro NM, et al. Functional mapping-guided resection of low-grade gliomas in eloquent areas of the brain: improvement of long-term survival. Clinical article. J Neurosurg. (2011) 114:566–73. doi: 10.3171/2010.6.JNS091246
35. Sanai N, Mirzadeh Z, and Berger MS. Functional outcome after language mapping for glioma resection. N Engl J Med. (2008) 358:18–27. doi: 10.1056/NEJMoa067819
36. Lau D, Hervey-Jumper SL, Han SJ, and Berger MS. Intraoperative perception and estimates on extent of resection during awake glioma surgery: overcoming the learning curve. J Neurosurg. (2018) 128:1410–8. doi: 10.3171/2017.1.JNS161811
37. Mandonnet E, De Witt Hamer P, Poisson I, Whittle I, Bernat AL, Bresson D, et al. Initial experience using awake surgery for glioma: oncological, functional, and employment outcomes in a consecutive series of 25 cases. Neurosurgery. (2015) 76:382–9; discussion 9. doi: 10.1227/NEU.0000000000000644
38. Jensdottir M, Beniaminov S, Jakola AS, Persson O, Norrelgen F, Hylin S, et al. Standardized reporting of adverse events and functional status from the first 5 years of awake surgery for gliomas: a population-based single-institution consecutive series. Acta Neurochirurgica. (2022) 164:1995–2008. doi: 10.1007/s00701-022-05191-0
39. Ng S, Rigau V, Moritz-Gasser S, Gozé C, Darlix A, Herbet G, et al. Long-term autonomy, professional activities, cognition, and overall survival after awake functional-based surgery in patients with IDH-mutant grade 2 gliomas: a retrospective cohort study. Lancet Reg Health Eur. (2024) 46:101078. doi: 10.1016/j.lanepe.2024.101078
40. Capelle L, Fontaine D, Mandonnet E, Taillandier L, Golmard JL, Bauchet L, et al. Spontaneous and therapeutic prognostic factors in adult hemispheric World Health Organization Grade II gliomas: a series of 1097 cases: clinical article. J Neurosurg. (2013) 118:1157–68. doi: 10.3171/2013.1.JNS121
41. Wijnenga MMJ, French PJ, Dubbink HJ, Dinjens WNM, Atmodimedjo PN, Kros JM, et al. The impact of surgery in molecularly defined low-grade glioma: an integrated clinical, radiological, and molecular analysis. Neuro Oncol. (2018) 20:103–12. doi: 10.1093/neuonc/nox176
42. Gómez Vecchio T, Neimantaite A, Corell A, Bartek J Jr., Jensdottir M, Reinertsen I, et al. Lower-grade gliomas: an epidemiological voxel-based analysis of location and proximity to eloquent regions. Front Oncol. (2021) 11:748229. doi: 10.3389/fonc.2021.748229
43. Hendriks EJ, Idema S, Hervey-Jumper SL, Bernat AL, Zwinderman AH, Barkhof F, et al. Preoperative resectability estimates of nonenhancing glioma by neurosurgeons and a resection probability map. Neurosurgery. (2019) 85:E304–e13. doi: 10.1093/neuros/nyy487
44. Kommers I, Bouget D, Pedersen A, Eijgelaar RS, Ardon H, Barkhof F, et al. Glioblastoma surgery imaging-reporting and data system: standardized reporting of tumor volume, location, and resectability based on automated segmentations. Cancers (Basel). (2021) 13. doi: 10.3390/cancers13122854
45. Karschnia P, Gerritsen JKW, Teske N, Cahill DP, Jakola AS, van den Bent M, et al. The oncological role of resection in newly diagnosed diffuse adult-type glioma defined by the WHO 2021 classification: a Review by the RANO resect group. Lancet Oncol. (2024) 25:e404–e19. doi: 10.1016/S1470-2045(24)00130-X
46. Sawaya R, Hammoud M, Schoppa D, Hess KR, Wu SZ, Shi WM, et al. Neurosurgical outcomes in a modern series of 400 craniotomies for treatment of parenchymal tumors. Neurosurgery. (1998) 42:1044–55; discussion 55–6. doi: 10.1097/00006123-199805000-00054
47. Coburger J, Onken J, Rueckriegel S, von der Brelie C, Nadji-Ohl M, Forster MT, et al. Eloquent lower grade gliomas, a highly vulnerable cohort: assessment of patients’ Functional outcome after surgery based on the loG-glio registry. Front Oncol. (2022) 12:845992. doi: 10.3389/fonc.2022.845992
48. Jakola AS, Senft C, Unsgaard G, and Solheim O. Surgical management of eloquent supratentorial low-grade gliomas with special emphasis on intraoperative imaging. J Neurol Surg A Cent Eur Neurosurg. (2015) 76:149–59. doi: 10.1055/s-0034-1393925
Keywords: extent of resection, glioma, low-grade glioma, neurological deficits, neurosurgery, oncology, surgical outcomes
Citation: Jensdottir M, Solheim O, Corell A, de Dios E, Dunås T, Fletcher-Sandersjöö A, Gulati S, Holmgren K, Latini F, Mahesparan R, Milos P, Neimantaite A, Redebrandt HN, Pedersen LK, Sjöberg RL, Sjögren B, Tomasevic G, Tveiten ØV, Vecchio TG, Zetterling M, Bartek J Jr and Jakola AS (2025) Patient selection and outcome in low-grade glioma surgery. Front. Oncol. 15:1703756. doi: 10.3389/fonc.2025.1703756
Received: 11 September 2025; Accepted: 02 October 2025;
Published: 27 November 2025.
Edited by:
Marion Rapp, Beta Clinic, GermanyReviewed by:
Franziska Staub-Bartelt, University Hospital of Düsseldorf, GermanyMichael Sabel, Brain Cancer Center BetaKlinik, Germany
Copyright © 2025 Jensdottir, Solheim, Corell, de Dios, Dunås, Fletcher-Sandersjöö, Gulati, Holmgren, Latini, Mahesparan, Milos, Neimantaite, Redebrandt, Pedersen, Sjöberg, Sjögren, Tomasevic, Tveiten, Vecchio, Zetterling, Bartek and Jakola. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Margret Jensdottir, bWFyZ3JldC5qZW5zZG90dGlyQGtpLnNl
†Present addresses: Eddie de Dios, Department of Radiology, Institute of Clinical Sciences, Sahlgrenska Academy, University of Gothenburg, Sweden Department of Radiology, Sahlgrenska University Hospital, Gothenburg, Sweden