 Pascal Caillet1*
Pascal Caillet1* Fréderic Balusson2Nathalie Ganne-Carié3Emmanuel Oger2Charlotte Costentin4Olivier Ganry5
Fréderic Balusson2Nathalie Ganne-Carié3Emmanuel Oger2Charlotte Costentin4Olivier Ganry5- 1Department of Public Health, University Hospital of Nantes, Nantes, France
- 2Univ Rennes, Centre Hospitalier Universitaire (CHU) Rennes, Institut National de la Santé et de la Recherche Médicale (INSERM), Ecole des Hautes Etudes en Santé Publique (EHESP), (Institut de recherche en santé, Environnement et travail (IRSET), UMR, Rennes, France
- 3Department of Hepatology, Hôpitaux Universitaires Paris Seine-Saint-Denis (AP-HP), Bobigny, France
- 4Univ. Grenoble Alpes/Hepato-Gastroenterology and Digestive Oncology department, Centre Hospitalier Universitaire (CHU) Grenoble Alpes/Institute for Advanced Biosciences, Centre National de la Recherche Scientifique (CNRS) UMR 5309-Institut National de la Santé et de la Recherche Médicale (INSERM) U1209, Grenoble, France
- 5Department of Public Health, University Hospital of Amiens, Amiens, France
Objectives: Hepatocellular carcinoma (HCC) is the fourth leading cause of cancer-related death worldwide. Most cases occur in patients with an underlying cirrhosis. The French national guidelines recommend semiannual abdominal ultrasound surveillance for early HCC detection in patients with cirrhosis. The primary goal of our retrospective cohort study was to evaluate compliance with this recommendation.
Methods: We used 2007–2016 general public health insurance program (Régime Général) data from the French National Health Data System (Système National des Données de Santé, or SNDS). Included patients were 18 to 75 years old, diagnosed with liver cirrhosis between 2009 and 2013, and underwent their first ultrasound >4 months after their index date. The number of annual ultrasounds was recorded over a 3-year follow-up period. Compliance was defined as having had at least 2 ultrasounds per year over the follow-up time.
Results: Among the 66,464 patients included in the analysis, surveillance was optimal (no year with <2 ultrasounds) in 5,082 patients (7.6%), suboptimal (one year with <2 ultrasounds) in 3,928 (5.9%), and failed (remaining cases) in 57,454 (86.4%). Older age, male sex, a high Charlson Co-morbidity Index (CCI), frequent gastroenterologist/hepatologist visits, and viral etiology were associated with better surveillance, whereas low socioeconomic status, despite France’s universal health coverage, was linked to failed surveillance.
Discussion: In French patients with cirrhosis, most of cancer surveillance is failing. In order to improve surveillance, a better understanding of the social determinants of health equity is needed.
Introduction
Hepatocellular carcinoma (HCC) is the sixth and third leading component of cancer incidence and cancer death worldwide (1, 2)—behind lung, breast, colorectal, prostate, and stomach cancers—and was responsible for the death of 781,631 patients in 2018 (3). More than 70% of cases occur in Asia, 10% in Europe, 8% in Africa, and nearly 10% in the Americas. The epidemiology of HCC has changed over the past 20 years owing to fluctuations in the prevalence of known risk factors. In 80% of cases, HCC develops within cirrhotic livers (4). Patients with cirrhosis from any etiology typically have a ∼2% annual risk of developing HCC (5). Once major risks in industrialized countries, viral hepatitis B and C have been declining since the introduction of highly effective antiviral treatments and the widespread distribution of the hepatitis B vaccine. In contrast, the burden of alcohol-related cirrhosis has increased, as has the incidence of cirrhosis related to metabolic dysfunction-associated steatohepatitis (MASH), which mostly occurs in overweight or diabetic patients (2). Thus, while the leading etiology of HCC worldwide is viral, alcohol-related cirrhosis and MASH are the most common causes in Western countries such as France (6).
Despite advances in therapeutic management, overall mortality associated with HCC remains very high in France. HCC is among the seven cancers with the worst prognoses: estimated median survival is ∼8 months (2). In France, the 1- and 5-year standardized net survival rates for liver cancers diagnosed in 2015 (90% of which were HCCs) were 48% and 18% respectively (7). Survival is highly correlated with the cancer stage at diagnosis. Survival in HCC is tumor-stage dependent, with 5-year survival expected only in patients who are diagnosed at an early stage and undergo potentially curative treatments (8). However, studies suggest that as few as only <20% of patients are diagnosed at an early stage eligible for curative options (9). Semi-annual ultrasound screening is associated with early diagnosis, curative treatment, and survival in patients with cirrhosis (10). Thus, standardized and effective surveillance programs for patients with cirrhosis are urgently required.
European guidelines have consistently over the past decade recommended semiannual HCC surveillance via abdominal ultrasound for all patients at high risk of HCC, including those with cirrhosis (11). However, compliance with surveillance guidelines is low and there are significant disparities between countries and cirrhosis etiologies. Reported percentage of patients receiving monitoring per current recommendation ranges from 14% (12) to 52% (13). Compliance in the US is usually lower than that in Asian countries (14). It has been shown that compliance with surveillance guidelines is greater in patients with liver disease linked to hepatitis B or C (15), when follow-up is managed by a specialist (16), or when patients have significant comorbidities (17).
In France, data on HCC surveillance are scarce (6) and come from studies with small populations (17) or focused on patients with cirrhosis related to hepatitis B or C (10). A detailed large-scale review of HCC surveillance in France is required. The primary objective of this study was to evaluate compliance with surveillance guidelines for early HCC detection in clinical practice in patients with cirrhosis in France. The secondary objective was to identify factors predicting failed surveillance.
Materials and methods
We conducted a retrospective cohort study using the French National Health Data System (Système National des Données de Santé, or SNDS), considering data from 2007 to 2016 for the general public health insurance program (Régime Général). The SNDS combines several previously existing databases: the nationwide claims database of the French public health insurance administration (Système National d’Informations Interrégimes de l’Assurance Maladie, or SNIIRAM), the national hospital database (Programme de Médicalisation des Systèmes d’Information, or PMSI), and the national death registry (Centre d’Épidémiologie sur les Causes Médicales de Décès, or CEPIDC) (Supplementary Figure S1).
The SNDS covers more than 98% (66 million people) of the French population, from birth (or immigration) to death (or emigration), irrespective of occupational changes or retirement. It is an pseudonymized record of individual patients’ medical encounters, hospital diagnoses, drug dispensations related to outpatient medical care claims (including all reimbursed drugs), information from hospital discharge summaries, and the dates of death. SNDS is extensively used for epidemiological research, including cirrhosis epidemiology (18–20).
The inclusion period was 2009–2013. Data from 2007 and 2008 were used to facilitate the application of the exclusion criteria by identifying incident cirrhosis. For each patient, the follow-up lasted for ≥3 years, ending no later than December 31, 2016.
The study population included patients ages 18 to 75 with an incident diagnosis of cirrhosis during the inclusion period. Diagnosis of cirrhosis was defined as the presence of at least one ICD-10 code related to cirrhosis or its complications and was associated with hospital stay during the inclusion period (Supplementary Table S1). Patients were only included if they presented with an ICD-10 code related to cirrhosis handled during hospitalization, if the date of their first cirrhosis-related ICD-10 code fell within the inclusion period, and if they were not diagnosed with cancer (including HCC) within the two years preceding inclusion.
The primary objective of this study was to assess compliance with surveillance recommendations in patients with cirrhosis. The event of interest was reimbursement for abdominal ultrasound, as indicated by the codes recorded in the SNDS (Supplementary Table S2). No examinations performed during the first four months of follow-up were counted, as they were potentially performed for diagnostic purposes rather than for surveillance. Patients for whom follow-up was <4 months after the inclusion date were excluded from the analysis.
The secondary objective was to evaluate the sociodemographic and medical factors that are believed to be associated with optimal management. Accordingly, among the additional data retrieved were patient age at the time of study inclusion, gender, universal health coverage (Couverture Maladie Universelle, or CMU) beneficiary status, indicative of low socioeconomic level; type of health facility where cirrhosis was diagnosed or managed (i.e., public university hospital, other public hospital, or private clinic); CCI, the number of times a year the patient was seen by gastroenterologists/hepatologists (during private appointments or through hospitalization in a GI department); and etiology of cirrhosis (i.e., alcohol-related, viral, or unknown). Codes used are available in the Supplementary Material File.
This study was approved—registered under number MMS/ALU/AE161145—by the Commission Nationale de l’Informatique et des Libertés (CNIL), the French data protection authority. The research was conducted on anonymized data between May 2016 and October 2018, without the possibility of indirect identification. In accordance with the relevant guidelines and regulations, all participants included in the study were informed of and agreed to the possibility of their anonymized data being used for research purposes.
The patient cohort was described using the usual position and dispersion parameters: means and standard deviations or medians and ranges, depending on the nature of the distribution. Categorical data are presented as numbers and percentages.
The primary endpoint was the number of abdominal ultrasounds performed on a patient during each year of follow-up for which the data were available. Surveillance was deemed optimal if the number of ultrasounds was never <2, suboptimal if <2 for one year alone, and failed otherwise (Table 1). Patients for whom follow-up was not available during the year, whatever the reason, were considered to have NA over that year.
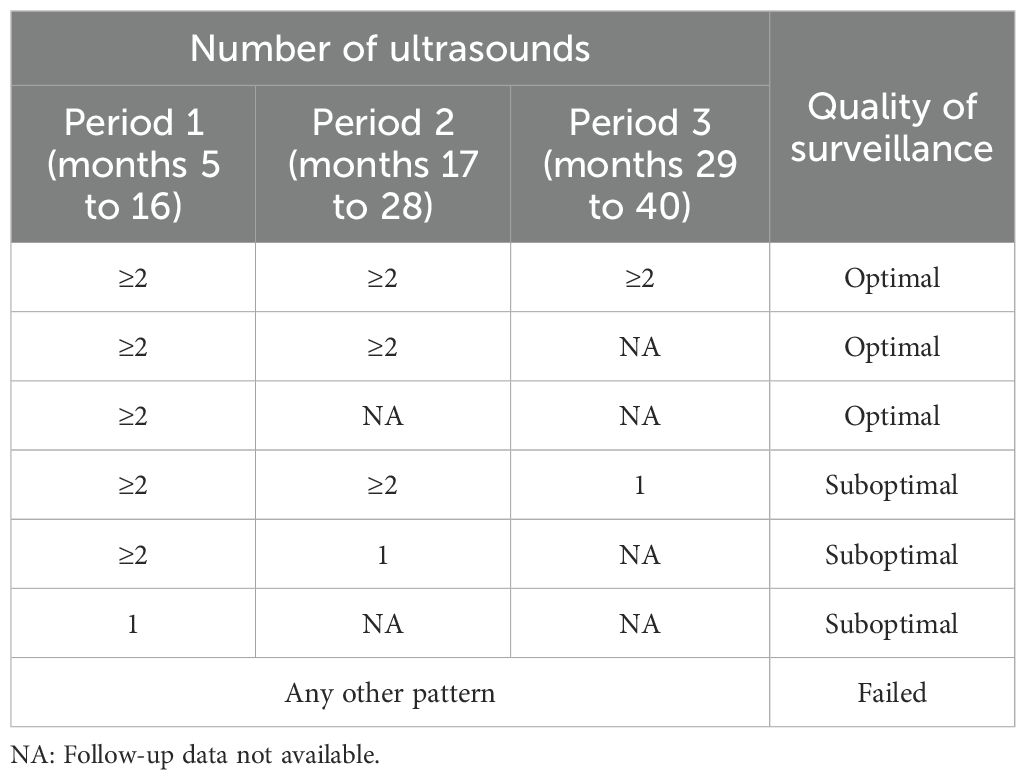
Table 1. Categorization of surveillance quality according to frequency of ultrasounds over 3-year follow-up period.
In accordance with our secondary objective of evaluating associations between surveillance level and the sociodemographic or medical variables listed above (see “Data collected”), our primary analysis compared patients with either optimal or failed surveillance, ignoring cases of suboptimal surveillance.
We constructed log-binomial models to measure associations, obtained adjusted measures with a Poisson model adapted to longitudinal data analysis (GEE), and a robust variance estimator to facilitate convergence as well as improve precision, and reported uncertainty in estimates with 95% confidence intervals. Collinearity was checked before introducing the covariates into the multivariate model. All analyses were performed using the SAS software (version 9.4).
Results
Between January 1, 2009, and December 31, 2013, 75,868 incident cases of cirrhosis were identified (Figure 1). The results are described in Table 2. The mean age of the patients at inclusion was 56 years (SD = 11), and two-thirds of them were male. The initial diagnosis took place in public university hospitals for roughly one-third of the patients and in other public hospitals for half of them. A quarter of the patients benefited from CMU health coverage and were reserved for the most economically disadvantaged in France. Nearly one-tenth of the patients had a CCI of 3 or higher.
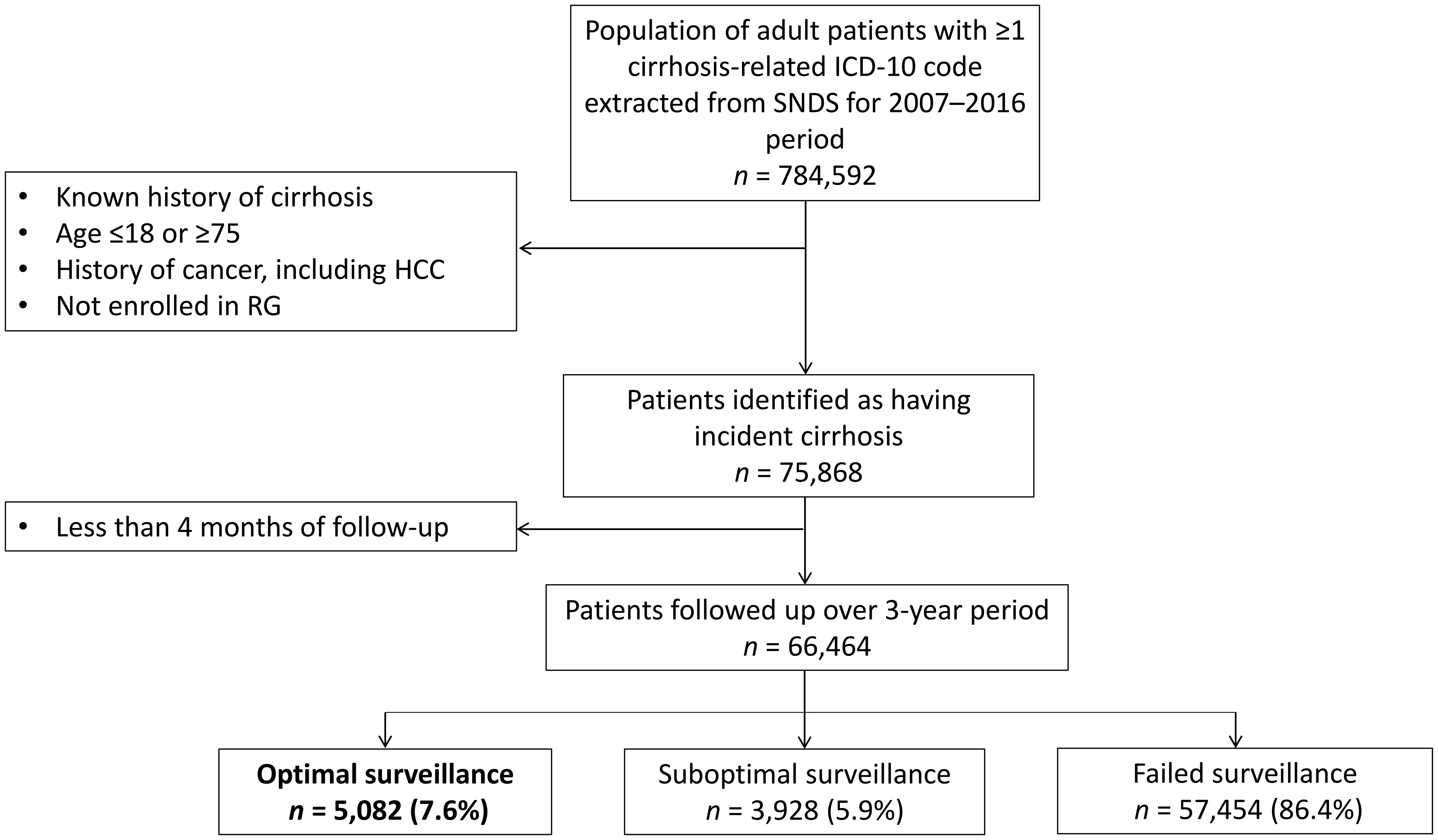
Figure 1. Study flowchart. HCC, hepatocellular carcinoma; RG, Régime Général (French general public health insurance program); SNDS, Système National des Données de Santé (French National Health Data System).
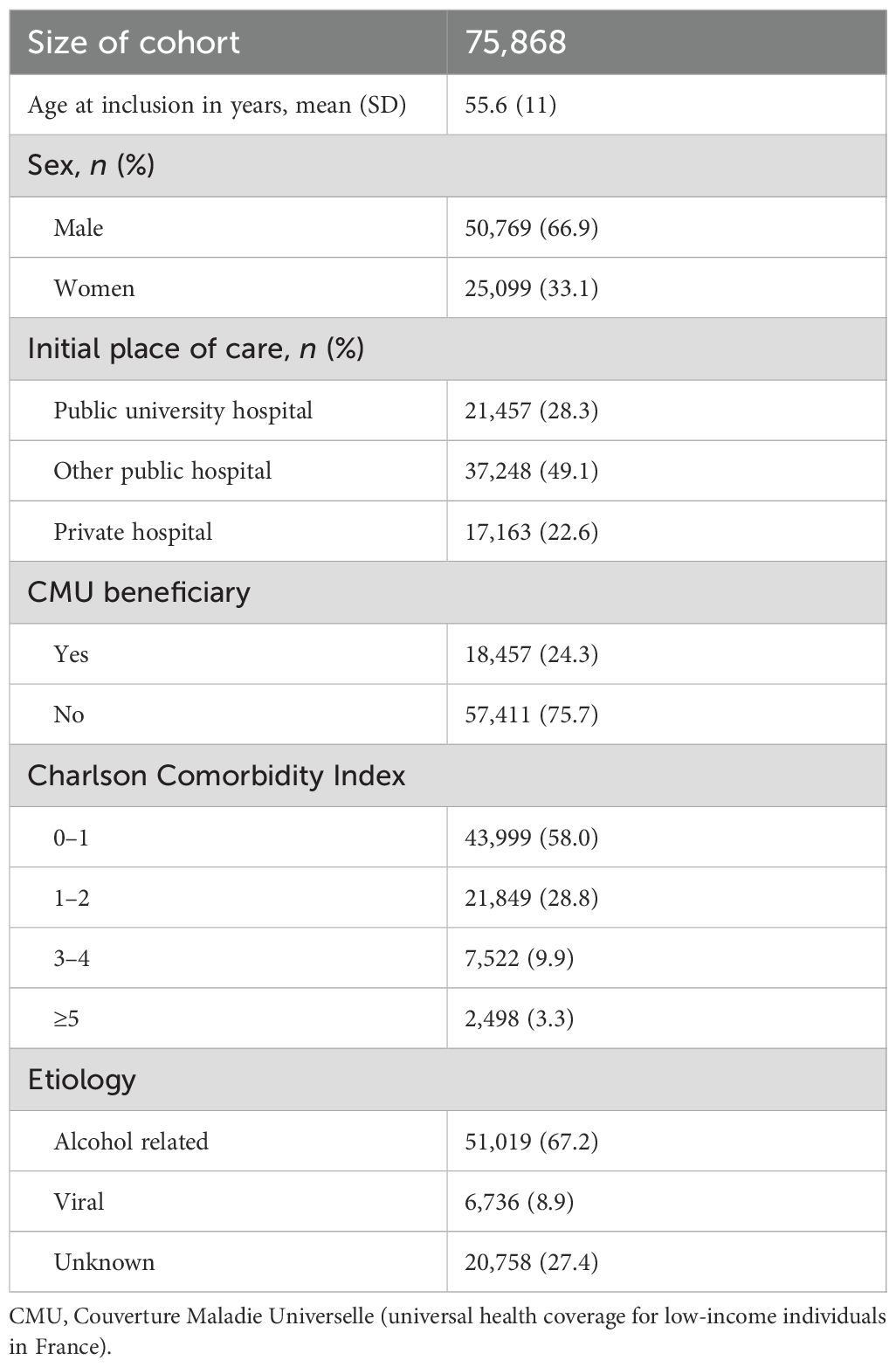
Table 2. Characteristics of inception cohort.
Each year, approximately 10% of the patients were censored due to death or a diagnosis of HCC or other cancers (Table 3). Of the 75,868 patients initially identified, 9,404 were censored because they had an ultrasound during the first 4 months, which is more suggestive of diagnostic procedures than surveillance. Of the remaining 66,464 patients, surveillance was optimal in only 7.6% (n = 5,082), suboptimal in 5.9% (n = 3,928), and failed in 86.4% (n = 57,454).
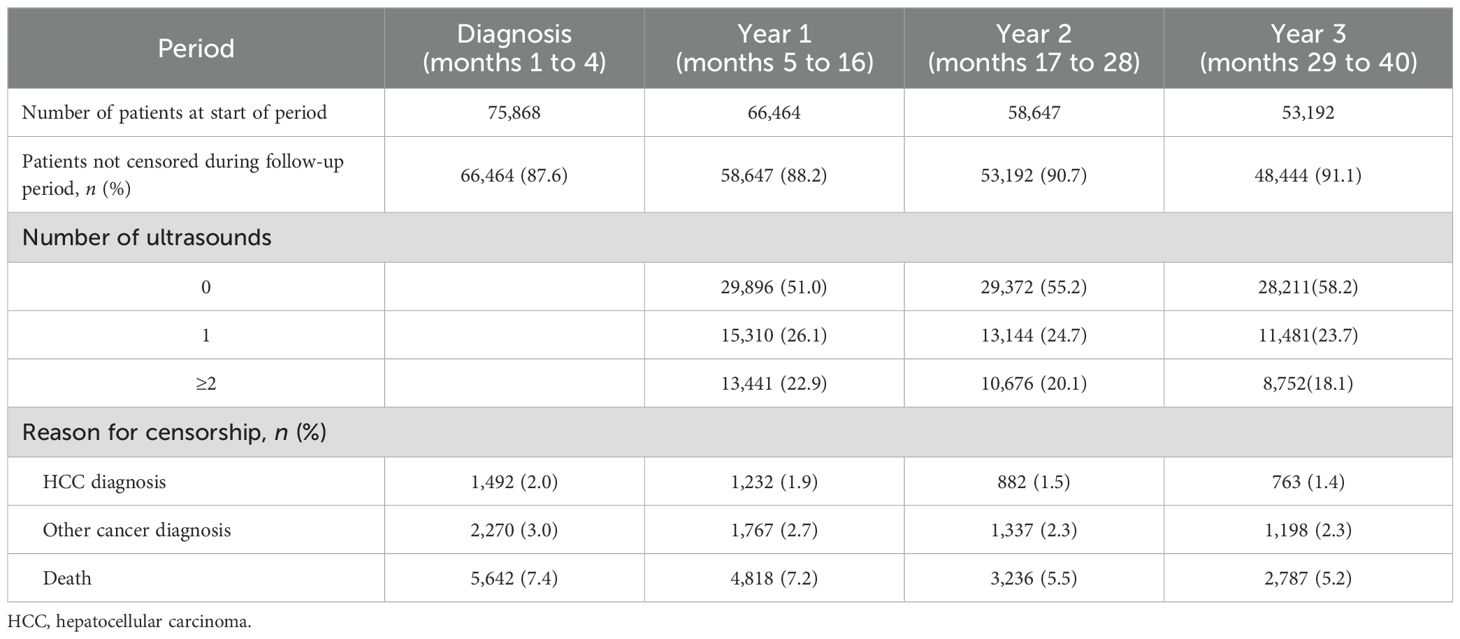
Table 3. Characteristics of follow-up.
Multivariable analysis showed that all variables of interest, other than the type of medical facility, were significantly associated with cirrhosis surveillance. Older age, male sex, high CCI, high number of annual visits to GI specialists, and viral etiology were associated with better surveillance aligned with current recommendations, while low socioeconomic status was associated with worse surveillance (Table 4). Sensitivity analysis did not reveal any substantial variation in the results using the alternative comparison pooling optimal and suboptimal surveillance versus failed surveillance.
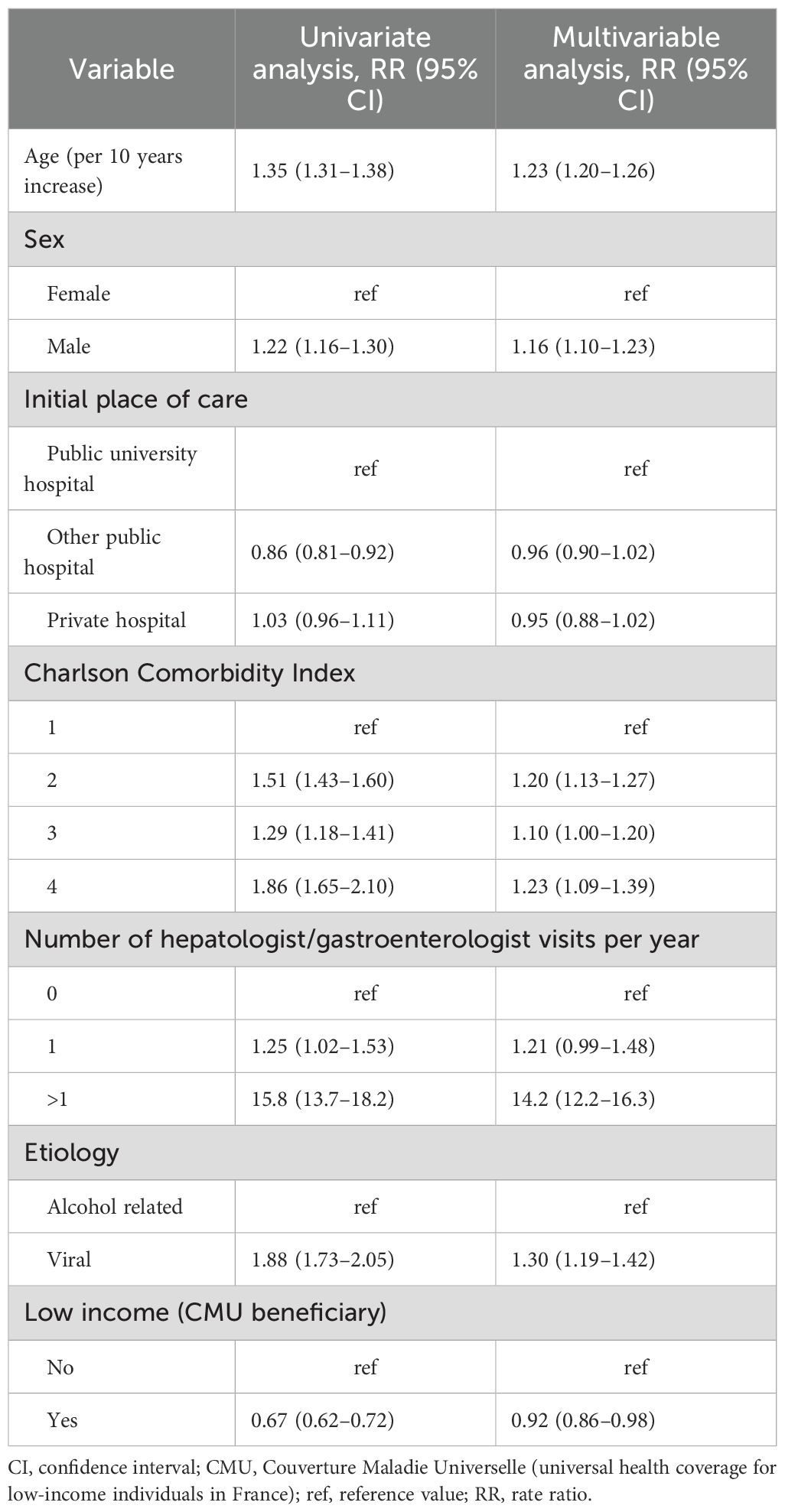
Table 4. Variables associated with optimal HCC surveillance.
Discussion
In our study, only 13.5% of the 66,464 patients with incident cirrhosis followed-up for 3 years had optimal or suboptimal surveillance, as defined by current European and French guidelines, which recommend semiannual ultrasound for early HCC detection.
Older age, male sex, a high CCI, frequent examinations by hepatologists, and viral etiology of the patient’s cirrhosis were identified as factors associated with better surveillance, whereas low socioeconomic status was associated with poorer surveillance.
The low number of patients benefiting from optimal surveillance (7.6%) is consistent with the literature. For example, Yeo et al. (14) reported that in 82,427 American patients followed up for cirrhosis over a mean period of 29 months, between 2007 and 2016, at least one HCC surveillance procedure (ultrasound, CT, or MRI) was performed every 6–12 months for 8.78% of the cases, >12–24 months for 25.32%, and >24 months for 20.47%. Another study, conducted among 597 American patients with hepatitis C virus cirrhosis enrolled in a program at an integrated health system between 2013 and 2020, only 5.0% of patients receiving usual care showed adequate surveillance, defined as at least five surveillance studies within 36 months post-enrollment (21). In a recent US database nested study conducted on claims ranging from January 2013 to June 2019 among 15,543 patients with cirrhosis, 45.8% and 58.7% had received any abdominal imaging at 6 and 12 months, respectively. Patients were up-to-date with recommended surveillance for only 31% of the median 1.3-year follow-up (22). In a recent meta-analysis, Wolf et al. reported a global surveillance rate of 24%, varying widely by study location (23). The surveillance rate in the US (17.8%) was far lower than that in Asia (34.6%).
The factors associated with surveillance have also been linked to surveillance in other countries. Across studies, the number of clinic visits and receipt of care from hepatologists were most consistently and strongly linked to adequate surveillance (23). Surveillance rates in gastroenterology and hepatology clinics is variable, as high as 75%, but also <10% in large population-based cohorts (23). In our study, >1 yearly examination by a GI specialist was the strongest driver of optimal surveillance. A positive and independent effect of hepatologist follow-up on the 5-year survival of patients with liver disease has been shown, although patients receiving GI care are highly selected (for more severe cirrhosis and viral etiologies) and may be more inclined to perform a complete follow-up at baseline (24). Surveillance rates are lower for alcohol related etiology than for viral etiology (23). This observation is of particular importance in France, where alcohol consumption related to roughly two-thirds of all HCC cases. Our findings offer new insights for better understanding the poorer prognosis of alcohol-related HCC in France (10, 25). Although we noted an association between older age and optimal surveillance, data from the literature are conflicting (23). In contrast to other reports (26), we found an association between the CCI and optimal surveillance. However, one might hypothesize that the impact of comorbidities depends on the severity of the chronic condition in question: providers may be less willing to order surveillance for patients thought to have a lower chance of long-term survival.
The most remarkable finding of our study is the negative impact of low socioeconomic status on the surveillance of patients with cirrhosis, despite the implementation of a system of universal health coverage (CMU) and complete coverage of care expenses for cirrhosis and certain other chronic diseases in France (including transportation). However, patient barriers are not related only to the costs of transport or procedures. Others have been identified, such as travel to the care facility organization, difficulty in scheduling appointments, and identifying where to receive surveillance (27), which brings up the concept of health literacy. Health literacy can be defined as “the personal characteristics and social resources needed for individuals and communities to access, understand, appraise and use information and services to make decisions about health” (28). Health literacy has been shown to be strongly associated with education, poverty, employment, having a first language different from the national language, and the level of socioeconomic deprivation in the area of residence (29). Importantly, compared to the rest of the population, CMU beneficiaries are more likely to be blue-collar workers, unemployed, and have lower educational levels. Unfortunately, we were unable to evaluate the impact of language and local socioeconomic deprivation in our study.
However, patients cannot be held accountable for all surveillance failure. Singal et al. showed that physicians frequently failed to order surveillance procedures, especially in patients with alcohol-related cirrhosis (30). This may in part reflect the persistent controversy concerning the risk-benefit ratio for surveillance in HCC (31, 32), despite cumulative evidence in its favor (3, 20, 33–35), or failure to identify individuals at risk (36). In addition, the uneven geographical distribution and shrinking numbers of hepatologists and gastroenterologists in France may also play a role, sometimes making physical access to specialized care challenging (37).
Taken together, our results, along with the existing literature, suggest that efforts should be made to improve surveillance programs by addressing these barriers. Several measures to promote HCC surveillance have already been tested with encouraging results (21, 23, 38–43). They include patient/provider education as well as both “inreach” (e.g., reminder and recall systems) and “outreach” (e.g., mailing campaigns to care providers and patients) strategies, each associated with a significant increase in surveillance procedures, albeit heterogeneous in magnitude (+9.4% to +63.6%). Shahsavari et al. and Campbell et al. advocated multilevel interventions with inreach and outreach components that account for individuals’ unique situations in addition to social policies and disparities at the local and national levels (44, 45).
A strength of our study was the use of the national SNDS database, which provided a nearly complete picture of medical service consumption by French patients identified as having cirrhosis during the study period.
Our study had some limitations. First, SNDS does not permit the identification of patients with cirrhosis who were not hospitalized during the recruitment period of our study, resulting in an overrepresentation of severe cases in our sample. Second, the SNDS does not provide data on factors such as patient- or physician-reported barriers, or an in-depth clinical profile of each patient that could impact surveillance rates. The results of this study have several implications. First, we may have failed to accurately identify all the cases of incident cirrhosis. Second, the clinical context in which cirrhosis was diagnosed may have prompted the decision not to implement follow-up HCC surveillance, as current guidelines do not recommend HCC surveillance in patients with decompensated liver disease who are not candidates for liver transplantation, or for whom frailty and co-morbidities would preclude curative treatment of early HCC.
Another limitation stems from the stringent definition of optimal follow-up, which we chose to be as close as possible to institutional guidelines. First, we did not account for a delay over the six month that defined a period, although an ultrasound occurring shortly afterward may be clinically relevant to declare the period as with surveillance. This may have directly impacted our estimates in a pessimistic manner. Second, we did not consider magnetic resonance imaging (MRI) or scanners (CT) during the periods that could have triggered the decision not to perform ultrasound. It is plausible that a fraction of patients having received recently CT or MRI were falsely identified as not non-compliant with guidelines, although this fraction appeared limited in other similar studies (5%, see Singal et al. (42)). Third, we did not distinguish patients receiving no surveillance at all from patients seldom receiving an ultrasound, which have been classified within the same “failed” surveillance group, although the clinical interpretation of each situation may be different.
Follow-up ended in 2016, well before the COVID-19 pandemic, which is suspected to have had a devastating impact on HCC surveillance (46), albeit transitory (47). Future interventions aimed at evaluating and promoting surveillance should consider the short- and long-term consequences of the pandemic (48).
In conclusion, our data demonstrated that HCC surveillance in France between 2009 and 2016 was seldom optimal for patients, despite health coverage in France. The greatest predictor of optimal surveillance was frequent examinations by GI specialists. Considering the expected decrease in the number of GI specialists over the next 5–10 years, there is an urgent need to design alternative care pathways to promote and support optimal surveillance in patients with cirrhosis. Equally important, in light of the observed association between low socioeconomic status and failed surveillance, policies aimed at reducing this healthcare disparity need to be implemented, especially knowing that the pandemic has only exacerbated such disparities worldwide.
Data availability statement
Data are available from the National Bureau of the French Public Health Insurance Administration (Caisse Nationale de l’Assurance Maladie, or CNAM) for researchers who meet the criteria for access to confidential data set by France’s data protection authority (Commission Nationale de l’Informatique et des Libertés, or CNIL). Authorization was sought from the CNIL (www.cnil.fr) and the French Health Data Hub (www.health-data-hub.fr). Requests to access these datasets should be directed to www.health-data-hub.fr.
Ethics statement
This study is a pseudonymized claims data analysis, approved by France’s data protection authority (CNIL) under ID MMS/ALU/AE 161145. The study was conducted in accordance with the local legislation and institutional requirements. Written informed consent for participation was not required from the participants or the participants’ legal guardians/next of kin in accordance with the national legislation and institutional requirements.
Author contributions
PC: Writing – original draft, Investigation, Conceptualization, Resources, Funding acquisition, Visualization, Validation, Writing – review & editing, Methodology, Supervision, Project administration. FB: Writing – original draft, Methodology, Software, Data curation, Validation, Writing – review & editing, Formal Analysis, Conceptualization. NG-C: Conceptualization, Writing – original draft, Writing – review & editing. EO: Project administration, Validation, Methodology, Conceptualization, Writing – review & editing, Writing – original draft, Supervision. CC: Writing – original draft, Writing – review & editing. OG: Writing – original draft, Methodology, Investigation, Funding acquisition, Conceptualization, Writing – review & editing.
Funding
The author(s) declare financial support was received for the research and/or publication of this article. This study was funded by the French National Institute of Cancer (SHSESP15-010). The funder had no role in study design, data collection and analysis, decision to publish, or manuscript preparation.
Acknowledgments
We thank Jason Miller for language editing and comments that greatly improved the manuscript and Eric Nguyen-Khac, Jean-Claude Barbare, and Melanie Duval for their useful guidance and proposals.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Generative AI statement
The author(s) declare that no Generative AI was used in the creation of this manuscript.
Any alternative text (alt text) provided alongside figures in this article has been generated by Frontiers with the support of artificial intelligence and reasonable efforts have been made to ensure accuracy, including review by the authors wherever possible. If you identify any issues, please contact us.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fonc.2025.1722277/full#supplementary-material
References
1. Bray F, Laversanne M, Sung H, Ferlay J, Siegel RL, Soerjomataram I, et al. Global cancer statistics 2022: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. (2024) 74:229–63. doi: 10.3322/caac.21834
2. Llovet JM, Kelley RK, Villanueva A, Singal AG, Pikarsky E, Roayaie S, et al. Hepatocellular carcinoma. Nat Rev Dis Primer. (2021) 7:6. doi: 10.1038/s41572-020-00240-3
3. Pascual S, Miralles C, Bernabé JM, Irurzun J, and Planells M. Surveillance and diagnosis of hepatocellular carcinoma: A systematic review. World J Clin Cases. (2019) 7:2269–86. doi: 10.12998/wjcc.v7.i16.2269
4. Valery PC, Laversanne M, Clark PJ, Petrick JL, McGlynn KA, and Bray F. Projections of primary liver cancer to 2030 in 30 countries worldwide. Hepatol Baltim Md. (2018) 67:600–11. doi: 10.1002/hep.29498
5. Kanwal F, Khaderi S, Singal AG, Marrero JA, Loo N, Asrani SK, et al. Risk factors for HCC in contemporary cohorts of patients with cirrhosis. Hepatol Baltim Md. (2023) 77:997–1005. doi: 10.1002/hep.32434
6. Costentin C, Ganne-Carrié N, Rousseau B, Gérolami R, and Barbare J-C. Care pathway of patients with hepatocellular carcinoma in France: State of play in 2017. Bull Cancer (Paris). (2017) 104:752–61. doi: 10.1016/j.bulcan.2017.06.008
7. Bouvier V, Nousbaum JB, Bouvier AM, Lecoffre C, Lafay L, Mounier M, et al. Survie des personnes atteintes de cancer en France métropolitaine 1989-2018. (2020). (Saint‑Maurice (Fra): Sante publique France).
8. Sidali S, Trépo E, Sutter O, and Nault J. New concepts in the treatment of hepatocellular carcinoma. United Eur Gastroenterol J. (2022) 10:765–74. doi: 10.1002/ueg2.12286
9. Walker M, El-Serag HB, Sada Y, Mittal S, Ying J, Duan Z, et al. Cirrhosis is under-recognised in patients subsequently diagnosed with hepatocellular cancer. Aliment Pharmacol Ther. (2016) 43:621–30. doi: 10.1111/apt.13505
10. Costentin CE, Layese R, Bourcier V, Cagnot C, Marcellin P, Guyader D, et al. Compliance with hepatocellular carcinoma surveillance guidelines associated with increased lead-time adjusted survival of patients with compensated viral cirrhosis: A multi-center cohort study. Gastroenterology. (2018) 155:431–442.e10. doi: 10.1053/j.gastro.2018.04.027
11. Wu G, Bajestani N, Pracha N, Chen C, and Makary MS. Hepatocellular carcinoma surveillance strategies: major guidelines and screening advances. Cancers. (2024) 16:3933. doi: 10.3390/cancers16233933
12. Ahmed Mohammed HA, Yang JD, Giama NH, Choi J, Ali HM, Mara KC, et al. Factors influencing surveillance for hepatocellular carcinoma in patients with liver cirrhosis. Liver Cancer. (2017) 6:126–36. doi: 10.1159/000450833
13. Zhao C, Jin M, Le RH, Le MH, Chen VL, Jin M, et al. Poor adherence to hepatocellular carcinoma surveillance: A systematic review and meta-analysis of a complex issue. Liver Int Off J Int Assoc Study Liver. (2018) 38:503–14. doi: 10.1111/liv.13555
14. Yeo YH, Hwang J, Jeong D, Dang N, Kam LY, Henry L, et al. Surveillance of patients with cirrhosis remains suboptimal in the United States. J Hepatol. (2021) 75:856–64. doi: 10.1016/j.jhep.2021.04.042
15. Aby E, Phan J, Truong E, Grotts J, and Saab S. Inadequate hepatocellular carcinoma screening in patients with nonalcoholic steatohepatitis cirrhosis. J Clin Gastroenterol. (2019) 53:142–6. doi: 10.1097/MCG.0000000000001075
16. Goldberg DS, Taddei TH, Serper M, Mehta R, Dieperink E, Aytaman A, et al. Identifying barriers to hepatocellular carcinoma surveillance in a national sample of patients with cirrhosis: Hepatobiliary Malignancies. Hepatology. (2017) 65:864–74. doi: 10.1002/hep.28765
17. Jiar N, Slama J-L, and Ganne-Carrié N. Screening of hepatocellular carcinoma in patients with uncomplicated cirrhosis in real life: Practices survey of general practionners from three towns of Seine-Saint-Denis (north-east suburb of Paris). Bull Cancer (Paris). (2017) 104:618–24. doi: 10.1016/j.bulcan.2017.06.004
18. Tuppin P, Rudant J, Constantinou P, Gastaldi-Ménager C, Rachas A, de Roquefeuil L, et al. Value of a national administrative database to guide public decisions: From the système national d’information interrégimes de l’Assurance Maladie (SNIIRAM) to the système national des données de santé (SNDS) in France. Rev Epidemiol Sante Publique. (2017) 65 Suppl 4:S149–67. doi: 10.1016/j.respe.2017.05.004
19. Moore N, Blin P, Lassalle R, Thurin N, Bosco-Levy P, and Droz C. National Health Insurance Claims Database in France (SNIRAM), Système Nationale des Données de Santé (SNDS) and Health Data Hub (HDH). In: Sturkenboom M and Schink T, editors. Databases for pharmacoepidemiological research. Springer International Publishing, Cham (2021). p. 131–40. doi: 10.1007/978-3-030-51455-6_10
20. Cadier B, Bulsei J, Nahon P, Seror O, Laurent A, Rosa I, et al. Early detection and curative treatment of hepatocellular carcinoma: A cost-effectiveness analysis in France and in the United States. Hepatol Baltim Md. (2017) 65:1237–48. doi: 10.1002/hep.28961
21. Bui H, Kumar NG, Singal AG, Boparai J, Mukhtar NA, Tran D, et al. Implementation of a hepatocellular carcinoma surveillance program in a community-based integrated health system in patients with hepatitis C cirrhosis. Am J Gastroenterol. (2024) 119:1506–14. doi: 10.14309/ajg.0000000000002704
22. Nguyen MH, Roberts LR, Engel-Nitz NM, Bancroft T, Ozbay AB, and Singal AG. Gaps in hepatocellular carcinoma surveillance in a United States cohort of insured patients with cirrhosis. Curr Med Res Opin. (2022) 38:2163–73. doi: 10.1080/03007995.2022.2124070
23. Wolf E, Rich NE, Marrero JA, Parikh ND, and Singal AG. Use of hepatocellular carcinoma surveillance in patients with cirrhosis: A systematic review and meta-analysis. Hepatol Baltim Md. (2021) 73:713–25. doi: 10.1002/hep.31309
24. Mellinger JL, Moser S, Welsh DE, Yosef MT, Van T, McCurdy H, et al. Access to subspecialty care and survival among patients with liver disease. Am J Gastroenterol. (2016) 111:838–44. doi: 10.1038/ajg.2016.96
25. Costentin CE, Sogni P, Falissard B, Barbare J-C, Bendersky N, Farges O, et al. Geographical disparities of outcomes of hepatocellular carcinoma in France: the heavier burden of alcohol compared to hepatitis C. Dig Dis Sci. (2020) 65:301–11. doi: 10.1007/s10620-019-05724-1
26. Al Hasani F, Knoepfli M, Gemperli A, Kollar A, Banz V, Kettenbach J, et al. Factors affecting screening for hepatocellular carcinoma. Ann Hepatol. (2014) 13:204–10. doi: 10.1016/S1665-2681(19)30883-X
27. Singal AG, Tiro JA, Murphy CC, Blackwell J-M, Kramer JR, Khan A, et al. Patient-reported barriers are associated with receipt of hepatocellular carcinoma surveillance in a multicenter cohort of patients with cirrhosis. Clin Gastroenterol Hepatol Off Clin Pract J Am Gastroenterol Assoc. (2021) 19:987–995.e1. doi: 10.1016/j.cgh.2020.06.049
28. World Health Organization. Regional Office for South-East Asia. Optimizing health literacy: Improving health and reducing health inequities (2015). New Delhi: WHO Regional Office for South-East Asia. Available online at: https://www.who.int/publications/i/item/9789290224747 (Accessed November 10, 2025).
29. Rowlands G, Protheroe J, Winkley J, Richardson M, Seed PT, and Rudd R. A mismatch between population health literacy and the complexity of health information: an observational study. Br J Gen Pract J R Coll Gen Pract. (2015) 65:e379–386. doi: 10.3399/bjgp15X685285
30. Singal AG, Yopp AC, Gupta S, Skinner CS, Halm EA, Okolo E, et al. Failure rates in the hepatocellular carcinoma surveillance process. Cancer Prev Res Phila Pa. (2012) 5:1124–30. doi: 10.1158/1940-6207.CAPR-12-0046
31. Taylor-Robinson SD, Wong J, Crossey MME, and Khan SA. Evidence is weak to support hepatocellular carcinoma screening in chronic liver disease. Evid Based Med. (2015) 20:59. doi: 10.1136/ebmed-2014-110107
32. Hernaez R and El-Serag HB. Hepatocellular carcinoma surveillance: The road ahead: Hernaez and El-serag. Hepatology. (2017) 65:771–3. doi: 10.1002/hep.28983
33. Taylor EJ, Jones RL, Guthrie JA, and Rowe IA. Modeling the benefits and harms of surveillance for hepatocellular carcinoma: Information to support informed choices. Hepatol Baltim Md. (2017) 66:1546–55. doi: 10.1002/hep.29315
34. Hanouneh IA, Alkhouri N, and Singal AG. Hepatocellular carcinoma surveillance in the 21st century: Saving lives or causing harm? Clin Mol Hepatol. (2019) 25:264–9. doi: 10.3350/cmh.2019.1001
35. Singal AG, Daher D, Narasimman M, Yekkaluri S, Liu Y, Cerda V, et al. Benefits and harms of hepatocellular carcinoma screening outreach in patients with cirrhosis: a multicenter randomized clinical trial. J Natl Cancer Inst. (2025) 117:262–9. doi: 10.1093/jnci/djae228
36. Wong LL. Surveillance of hepatocellular cancer-why can’t we do better? Hepatobiliary Surg Nutr. (2019) 8:662–3. doi: 10.21037/hbsn.2019.07.20
37. CNHG. Livre Blanc de l’Hépato-gastroentérologie - Les chiffres clés (2020). Available online at: https://www.cnp-hge.fr/wp-content/uploads/2020/03/LIVRE-BLANC_HGE.pdf (Accessed November 10, 2025).
38. Beste LA, Ioannou GN, Yang Y, Chang MF, Ross D, and Dominitz JA. Improved surveillance for hepatocellular carcinoma with a primary care-oriented clinical reminder. Clin Gastroenterol Hepatol Off Clin Pract J Am Gastroenterol Assoc. (2015) 13:172–9. doi: 10.1016/j.cgh.2014.04.033
39. Del Poggio P, Olmi S, Ciccarese F, Mazzoleni M, Jazzetti M, Jamoletti C, et al. A training program for primary care physicians improves the effectiveness of ultrasound surveillance of hepatocellular carcinoma. Eur J Gastroenterol Hepatol. (2015) 27:1103–8. doi: 10.1097/MEG.0000000000000404
40. Farrell C, Halpen A, Cross TJS, Richardson PD, Johnson P, and Joekes EC. Ultrasound surveillance for hepatocellular carcinoma: service evaluation of a radiology-led recall system in a tertiary-referral centre for liver diseases in the UK. Clin Radiol. (2017) 72:338.e11–338.e17. doi: 10.1016/j.crad.2016.10.019
41. Nazareth S, Leembruggen N, Tuma R, Chen S-L, Rao S, Kontorinis N, et al. Nurse-led hepatocellular carcinoma surveillance clinic provides an effective method of monitoring patients with cirrhosis. Int J Nurs Pract. (2016) 22 Suppl 2:3–11. doi: 10.1111/ijn.12472
42. Singal AG, Tiro JA, Marrero JA, McCallister K, Mejias C, Adamson B, et al. Mailed outreach program increases ultrasound screening of patients with cirrhosis for hepatocellular carcinoma. Gastroenterology. (2017) 152:608–615.e4. doi: 10.1053/j.gastro.2016.10.042
43. Brahmania M, Congly S, Sachar Y, Burak KW, Lethebe B, Szostakiwskyj JH, et al. Dedicated automatic recall hepatocellular cancer surveillance programme demonstrates high retention: A population-based cohort study. Liver Int Off J Int Assoc Study Liver. (2025) 45:e70020. doi: 10.1111/liv.70020
44. Shahsavari H, Matourypour P, Ghiyasvandian S, and Nejad MRG. Medical Research Council framework for development and evaluation of complex interventions: A comprehensive guidance. J Educ Health Promot. (2020) 9:88. doi: 10.4103/jehp.jehp_649_19
45. Campbell NC, Murray E, Darbyshire J, Emery J, Farmer A, Griffiths F, et al. Designing and evaluating complex interventions to improve health care. BMJ. (2007) 334:455–9. doi: 10.1136/bmj.39108.379965.BE
46. Toyoda H, Yasuda S, Kiriyama S, Tanikawa M, Hisanaga Y, Kanamori A, et al. Impact of COVID-19 pandemic on surveillance of hepatocellular carcinoma: a study in patients with chronic hepatitis C after sustained virologic response. GastroHep. (2020) 2:247–52. doi: 10.1002/ygh2.418
47. Makuza JD, Wong S, Morrow RL, Binka M, Darvishian M, Jeong D, et al. Impact of COVID-19 pandemic on hepatocellular carcinoma surveillance in British Columbia, Canada: An interrupted time series study. J Viral Hepat. (2024) 31:592–600. doi: 10.1111/jvh.13980
Keywords: cirrhosis, hepatocellular carcinoma surveillance, cohort study, prevention, ultrasound
Citation: Caillet P, Balusson F, Ganne-Carié N, Oger E, Costentin C and Ganry O (2025) Three-year of hepatocellular carcinoma surveillance in patients with cirrhosis diagnosed between 2009 and 2013: a cohort study based on the French National Health Data System (SNDS) claims data. Front. Oncol. 15:1722277. doi: 10.3389/fonc.2025.1722277
Received: 10 October 2025; Accepted: 31 October 2025;
Published: 20 November 2025.
Edited by:
Abdelbaset Mohamed Elasbali, Jouf University, Saudi ArabiaReviewed by:
Stephen Barclay, NHS Greater Glasgow and Clyde, United KingdomEman El Azab, Al Jouf University, Saudi Arabia
Copyright © 2025 Caillet, Balusson, Ganne-Carié, Oger, Costentin and Ganry. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Pascal Caillet, cGFzY2FsLmNhaWxsZXRAY2h1LW5hbnRlcy5mcg==