 Martha Milade Torres Nupan
Martha Milade Torres Nupan Alberto Velez Van Meerbeke*
Alberto Velez Van Meerbeke* Claudia Alejandra López Cabra
Claudia Alejandra López Cabra Paula Marcela Herrera Gomez
Paula Marcela Herrera Gomez
- Neurosciences Research Group, Medicine and Health Sciences School, Universidad del Rosario, Bogota, Colombia
Aim: The last systematic review of research on the behavior of children with neurofibromatosis type 1 (NF1) was in 2012. Since then, several important findings have been published. Therefore, the study aim was to synthesize recent relevant work related to this issue.
Method: We conducted a systematic review of the literature. Relevant articles were identified using the electronic databases PubMed, PsycINFO, and Scopus and a manual search of references lists. Thirty of 156 articles identified met the inclusion criteria. A quality evaluation of the articles was performed and the information was synthesized using a narrative approach.
Results: Compared with controls, children and adolescents with NF1 present significant alterations in language, reading, visuospatial skills, motor function, executive function, attention, behavior, emotion, and social skills. The prevalence of attention-deficit/hyperactivity disorder (ADHD) is important and can affect cognition and executive function variables. A high prevalence of autistic traits and autistic spectrum disorder were reported. The benefits of using statins to treat cognitive deficits are unclear. However, children with NF1 and ADHD seem to benefit from methylphenidate treatment. The presence of hyperintensities in brain magnetic resonance imaging data seem to be related to poor cognitive performance. Analysis of these lesions could help to predict cognitive alterations in children with NF1.
Interpretation: There has been important progress to evaluate cognitive characteristics of children with NF1 and to determine the physiological mechanisms of the concomitant disorders. However, discrepancies in relation to intelligence, learning disabilities, attention deficits, and treatment remain. Further investigations on this topic are recommended.
Introduction
Neurofibromatosis type 1 (NF1) is an autosomal dominant genetic condition with a prevalence of 1 in 2,000–3,000 live births (1, 2). The main clinical manifestations include café-au-lait macules, skinfold freckling, and neurofibromas (3). The most common complications of NF1 are cognitive and behavioral deficits. Up to 80% of children with NF1 experience cognitive and behavioral difficulties involving different domains. However, the intelligence quotient (IQ) scores of these patients are within the normal range or only slightly lower compared with unaffected sibling controls. As a result, discrepancies between IQ and academic achievement are frequently observed (4). Parents often report poor performance in reading, written work, spelling, organizational skills, and mathematics. In addition, approximately 38% of affected children have attention-deficit/hyperactivity disorder (ADHD) and some studies have reported that 29% of children with NF1 have autism spectrum disorder (ASD) (5). It is important to understand these kinds of problems to identify particular needs of patients and provide individualized management of rehabilitation and educational processes.
In 2012, Lehtonen (6) published a systematic review of the literature on behavioral issues and attention disorders in patients with NF1, which identified the problems described above. Among the most important problems, these authors identified were alterations in memory, language, cognitive skills, intelligence, and academic performance and they raised many questions that remain to be clarified. The objective of this systematic review was to evaluate how much progress has been made in addressing these questions over the last 5 years. As there are many recent new research findings in this area, it is timely to update recommendations for the evaluation, follow-up, and management of NF1 patients.
Methods
The study methods were adapted from the systematic review by Lehtonen (6).
Eligibility Criteria
The following inclusion criteria were used: studies published from 2012 to 2016; studies with outcome variables measuring cognitive aspects, executive function, emotion, attention, or social aspects; studies that used statistical group comparisons or normative data analysis; studies using quantitative methods; studies published in peer-reviewed journals; and clinical trials. Case report studies were excluded because of potential bias. The target population was children with NF1 aged 6–17 years. Studies published in English, French, and Spanish were included.
Search Strategy
In August 2016, an electronic databases search was done using PubMed, PsycINFO, and Scopus. For PubMed, MESH headings with OR function were used: cognition, cognition disorders, executive function, attention, attention deficit and disruptive behavior disorders, attention deficit disorder with hyperactivity, memory, memory disorders, learning, learning disorders, behavior, motor skills, motor skills disorders, mental disorders, neurodevelopmental disorders, neurocognitive disorders, speech, speech disorders, language, language disorders, language development disorders. The following keywords combined with the OR function were also used: motor skills, social skills, executive function, attention, memory, cogniti$, learning, behavior, school, education, language. Finally, the MESH heading neurofibromatosis 1 was combined with the previous search using the AND function. Terms were adapted for use with the PyscINFO and Scopus electronic databases. The references of the included articles and the electronic sources Science Direct, Web of Science, and Springer Link were manually searched to identify additional literature.
Study Selection and Data Extraction Process
This systematic literature review was conducted following the PRISMA reporting guidelines for systematic reviews and meta-analyses (7). Two authors (Martha Milade Torres Nupan and Claudia Alejandra López Cabra) screened all publication titles and abstracts and eliminated irrelevant articles. The full text of the remaining papers was retrieved and evaluated. Articles that did not meet the eligibility criteria were rejected. Disagreements were resolved by discussion or in consultation with the other authors (Alberto Vélez Van Meerbeke and Paula Marcela Herrera Gomez).
Two authors extracted information on population, methods, results, outcomes, level of evidence, and study quality (Martha Milade Torres Nupan and Claudia Alejandra López Cabra) (Table 1). The Joanna Briggs Institute Levels of Evidence scale was used to evaluate evidence levels. The Scottish Intercollegiate Guidelines Network methodology checklist, the Joanna Briggs Institute Critical Appraisal Checklist for Descriptive Studies, and the National Institute of Health Quality Assessment Tool for Observational Cohort and Cross-Sectional Studies were used to evaluate the quality of studies (see supporting information) (Tables 2–6). Two authors (Alberto Vélez Van Meerbeke and Paula Marcela Herrera Gomez) verified the information extracted and discrepancies were resolved by consensus (Martha Milade Torres Nupan, Claudia Alejandra López Cabra, Alberto Vélez Van Meerbeke, and Paula Marcela Herrera Gomez). All the authors evaluated the full-text articles that were retrieved. Because of the high heterogeneity of the studies, a narrative approach rather than a meta-analysis was used.
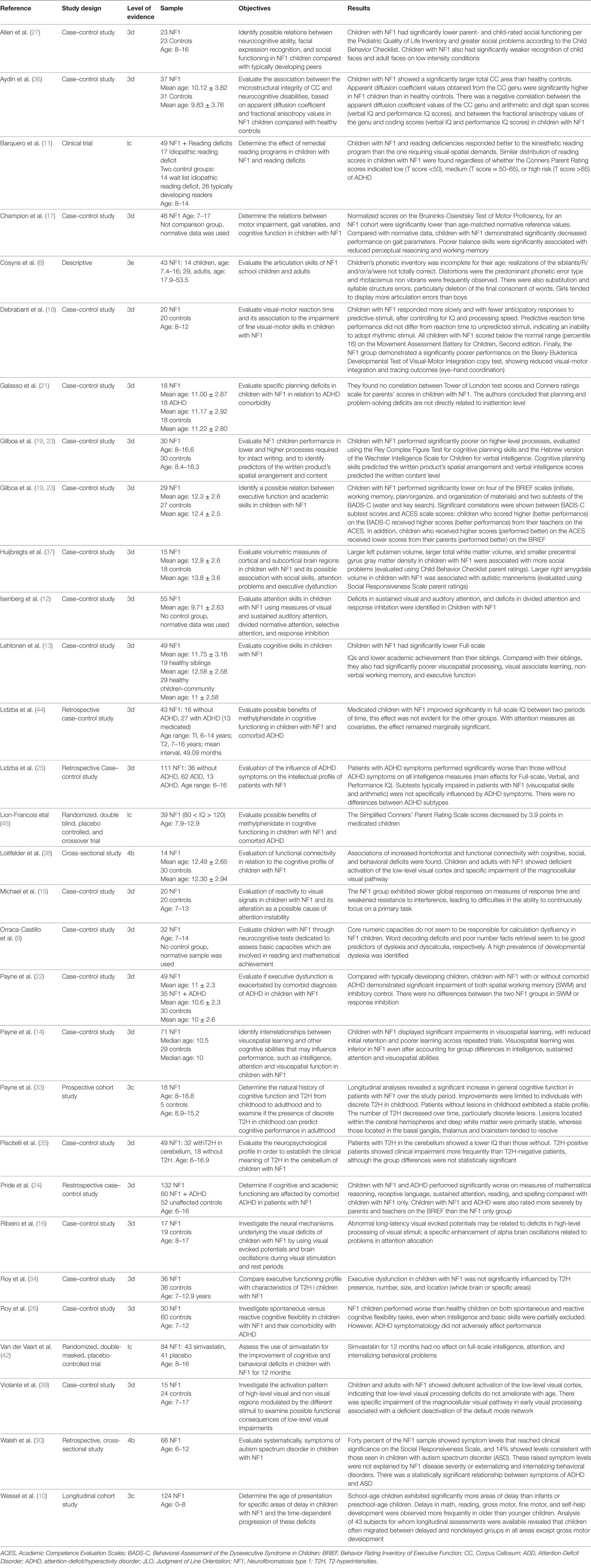
Table 1. Extraction table including study design, level of evidence (Joanna Briggs Institute levels of evidence), sample characteristics, objectives and results of the studies that addressed cognitive and behavior in children with neurofibromatosis type 1 (NF1).
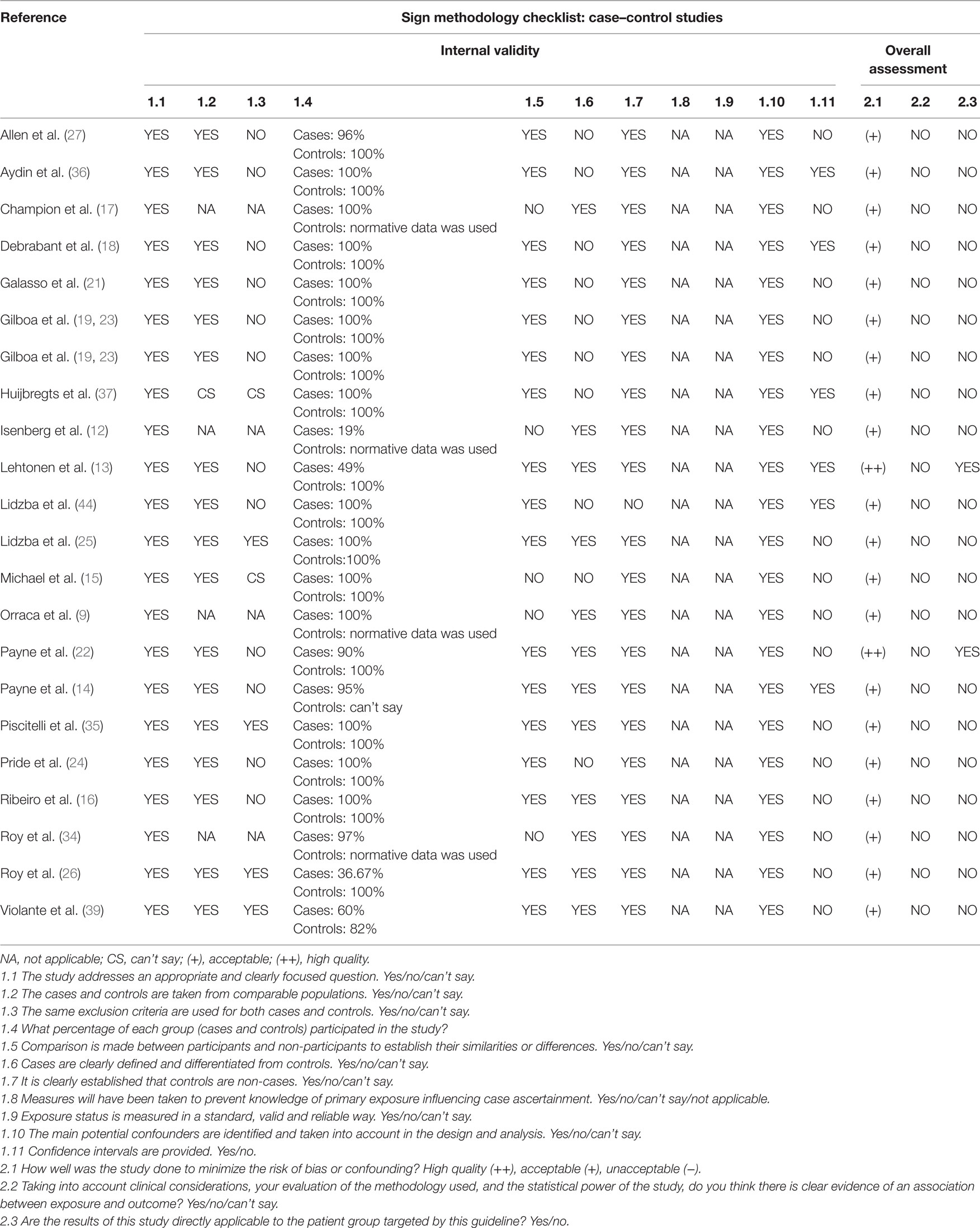
Table 2. Quality evaluation for case–control studies using the Scottish Intercollegiate Guidelines Network (SIGN).
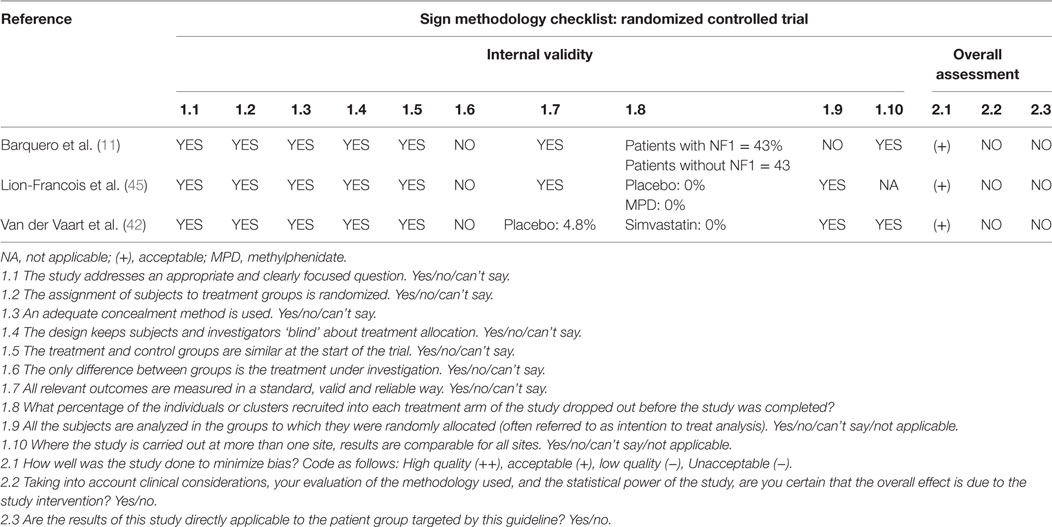
Table 3. Quality evaluation for randomized controlled trials using the Scottish Intercollegiate Guidelines Network (SIGN).
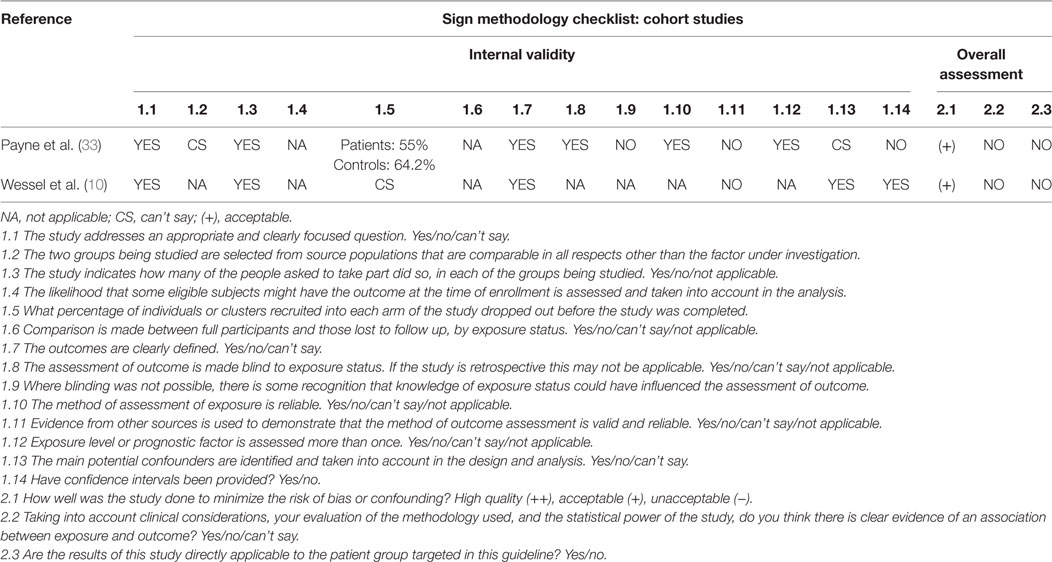
Table 4. Quality evaluation for cohort studies using the Scottish Intercollegiate Guidelines Network (SIGN).
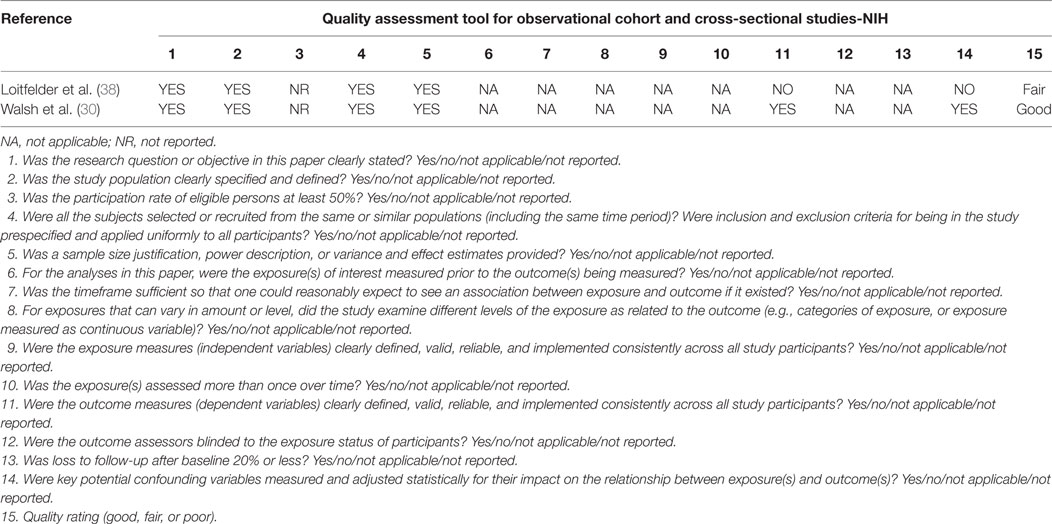
Table 5. Quality evaluation for cross sectional studies using the National Institutes of Health checklist (NIH).
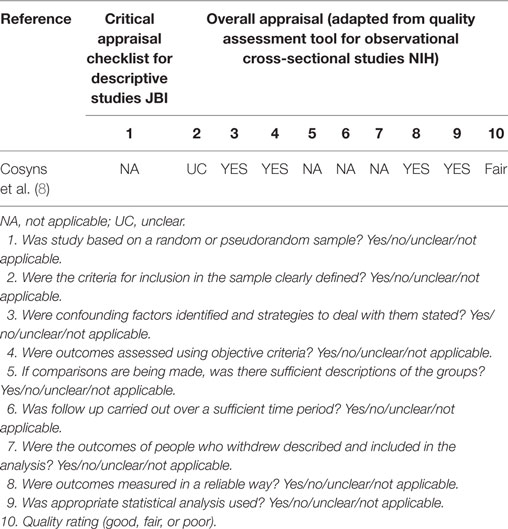
Table 6. Quality evaluation for descriptive studies using the Joanna Briggs Institute (JBI) Critical Appraisal Checklist.
Results
The database search identified 158 papers (Figure 1). Thirty additional articles were identified from other sources. After remove duplicates, the titles and abstracts of 156 articles were screened. During the first selection process, 90 studies were excluded. Sixty-six full-text articles were assessed for eligibility; of these, 36 were excluded because of different age groups and outcomes. Thirty articles that fulfilled the inclusion criteria were taken into account for the qualitative analysis.
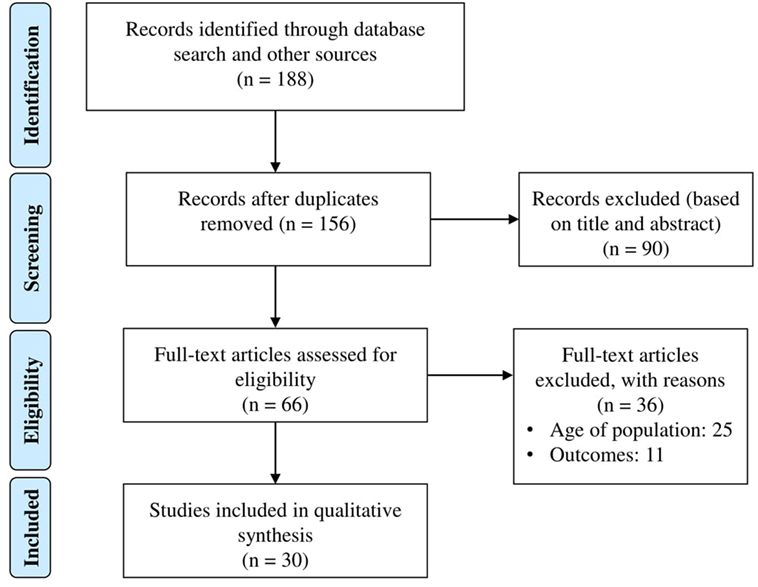
Figure 1. Systematic review flow diagram.
Language, Reading, and Mathematics
Several studies have shown deficits in language, reading, and reading comprehension in children with NF1. However, evaluations of these abilities differ, making it difficult to identify problems in specific aspects of each ability. Revising current literature, there is a lack of information (in both English and other languages) on speech production in children with NF1 with only one article related to this topic in the last 5 years. In this article, Cosyns (8) studied phonetic articulation in 29 Flemish adults and 14 schoolchildren (>7 years) with NF1 using a standardized speech test for Flemish single speech sounds. They found that the children’s phonetic inventory was incomplete for their age: realizations of the sibilants/R/and/or/a/were not correct. Distortions were the predominant phonetic error type and rhotacismus non-vibrant were frequently observed. There were also substitution and syllable structure errors, particularly deletion of the final consonant of words. Girls tended to display more articulation errors than boys did. More studies in different languages are needed to obtain a deeper understanding of this aspect of speech production.
Orraca-Castillo (9) evaluated mathematics and reading skills in 32 NF1 children using the Mathematics Attainment Test and the Reading and Comprehension Attainment Test. They also used two computer-based tests to measure simple reaction times from the Basic Numerical Battery and the word and pseudoword-reading task from the Batería de Trastornos de la Lectura. Lexical/phonological skills and mental arithmetic were significant predictors of individual differences in reading achievement and math. The sample showed no deficits in core numeric capacities, suggesting that these are not responsible for calculation dysfluency. Word decoding deficits and poor number facts retrieval seem to be good predictors of dyslexia and dyscalculia, respectively. Interestingly, Orraca-Castillo found no gender differences and identified a 50% prevalence of developmental dyslexia in their sample, a cooccurrence almost three times higher than dyscalculia (18.8%). In concordance with these results, Wessel (10) using a sample of 124 NF1 participants between 0 and 8 years, showed that school-age children with NF1 exhibited significantly more delays in reading and math than infants or preschool-age children with NF1, using the Parents’ Evaluation of Developmental Status as a tool of assessment. These findings are in line with previous reports that NF1 patients show a high prevalence of learning disorders not related to IQ achievement discrepancies.
Barquero et al. (11) conducted the first evaluation of an intervention for reading deficiencies in 49 children with NF1. Some children received remedial reading instruction from a kinesthetic reading program and others used a program that required greater visuospatial demands. Children with NF1 and reading deficiencies responded better to the kinesthetic reading program. However, the baseline mean reading score of the group using the program that required greater visuospatial demands was significantly higher than that of the group receiving the kinesthetic treatment.
Visuospatial Functioning
Visuospatial deficits are considered a “hallmark” phenotypic characteristic of patients with NF1. The Judgment of Line Orientation (JLO) is one of the main tests used to assess these deficits because it is more consistent than other tools. Using the JLO test, Isenberg et al. (12) and Lehtonen et al. (13) compared the visuospatial processing of children with NF1 to their siblings or healthy children. Lehtonen et al. (13) showed that children with NF1 performed significantly poorer than their siblings. Isenberg et al. (12) found that the visuospatial processing of children with NF1 was below the age-based normative data, although the SD range was relatively large, indicating a high variability within the study.
Lehtonen et al. (13) and Payne et al. (14) compared visuospatial learning in children with NF1 with that of their siblings using the paired associate learning task from the Cambridge Automated Neuropsychological Test Assessment Battery. Lehtonen (13) found that NF1 children made more mistakes than their siblings on the total number of errors, but this difference was not statistically significant. Payne et al. (14) found that children with NF1 showed important deficits in visuospatial learning, with bad initial memorization and poorer learning in repeated trials, even after explaining group differences in intelligence, sustained attention, and visuospatial skills. Defective visuospatial learning was identified as a major phenotypic trait in children with NF1.
Michael et al. (15) compared reactivity to visual signals in 20 children with NF1 against 20 controls. They used a visual discrimination task with targets and distractors taken from the Living English Structure for Schools pictures. The NF1 group exhibited slower global responses on measures of response time and weakened resistance to interference, leading to difficulties in the ability to continuously focus on a primary task. The authors suggest that NF1 is characterized by over-reactivity to, and longer inspection of, visual signals occurring outside the current focus of attention and that this might be partially responsible for instability in attentional focus and lower interference resistance.
Electrophysiological tools have also been used to study the mechanisms of visuospatial deficits. Ribeiro et al. (16) studied the neural mechanisms underlying visual deficits in children with NF1. He found abnormal long-latency visual evoked potentials that may be related to deficits in process visual stimuli; in addition, they identified an increase of alpha brain oscillations probably due to problems in attention allocation.
Visuomotor Function, Motor Control, and Coordination
Children with NF1 show motor impairments, such as alterations in simple and complex motor tasks and deficits in visuomotor function. However, the associations between these characteristics remain unclear. Regarding motor performance, Champion (17) found that normalized scores on the Bruininks–Oseretsky Test of Motor Proficiency, Second edition, for an NF1 cohort of 46 participants, were lower than the normative reference-age valuescompared with normative data; children with NF1 demonstrated a significant decrease in speed, cadence, stride length, individual support and support base. A longer step time and double support were also observed. This study also showed that poor balance skills are associated with difficulties in perceptual reasoning and working memory. The decrease in speed in running and agility were related to worse spatial working memory (SWM), working memory, and perceptual reasoning. The authors found a significant association between walking gait width with SWM decrease and the same between short steps with a poorer SWM strategy.
Debrabant et al. (18) evaluated visual-motor reaction time and its association with the grade of impaired fine visual-motor skills and compared these parameters in 20 NF1 children against 20 controls. After controlling for IQ and processing speed, it was shown that the response of children with NF1 was slower with fewer anticipatory responses to predictive stimuli. Also, the predictive performance of the reaction time did not differ from reaction time to unexpected stimuli, indicating an inability to take rhythmic stimuli. Furthermore, all children with NF1 had abnormal scores (<16th percentile) on the battery of the assessment of movement for children, second edition. Finally, NF1 group demonstrated a significantly poor performance in the Beery-Buktenica developmental test of visual-motor integration, which is interpreted as a reduction of visual-motor integration and tracing outcomes (hand–eye coordination).
Wessel et al. (10) studied developmental delays in 124 children with NF1 using the Parents’ Evaluation of Developmental Status. In relation to motor control, they found delays in the development of gross motor, fine motor, and self-help. This was mainly observed in school-age children when compared to preschool children or infants. Longitudinal evaluations of 43 subjects revealed that children often exchanged from the delayed group to the not delayed one, in all areas except gross motor development.
Intelligence and Thinking
Children with NF1 have a slightly lower performance on intelligence tests than healthy children, and generally show mean or below-average scores on IQ. Champion et al. (17) and Lehtonen et al. (13) evaluated intellectual ability in NF1 children and comparison groups using the Wechsler Intelligence Scale for Children. Lehtonen et al. (13) found that children with NF1 had a mean full-scale IQ of 91, whereas the sibling comparison group had a mean IQ score of 99 (a statistically significant difference). NF1 children also showed lower academic achievement. Champion et al. (17) found that children with NF1 had a mean IQ of 86 and had scores significantly below normative data on all IQ variables.
Gilboa et al. (19) have shown that children with NF1 performed significantly poorer on higher-level processes, evaluated using the Rey Complex Figure Test for cognitive planning skills and the Hebrew version of the Wechsler Intelligence Scale for Children for verbal intelligence. Cognitive planning skills predicted the spatial arrangement of the written product and verbal intelligence scores predicted the level of written content. In contrast, participants in the Isenberg study (12) showed an average intellectual capacity in the Peabody Picture Vocabulary Test.
Executive Function
The executive functions comprise all the processes that help to monitor and regulate cognitive processes during complex tasks and include planning, self-regulation, behavior organization, cognitive flexibility, working memory, error detection and correction, inhibition, sustained attention, and resistance to interference. As different measures have been used to evaluate executive functions, it is hard to make comparative validations of distinct scales and evidence remains inconclusive (6, 20). Comorbidity with ADHD is also thought to affect executive function assessment, although this correlation is not well understood.
Lehtonen et al. (13) and Champion et al. (17) evaluated executive function in children with NF1 against comparison groups using the Behavior Rating Inventory of Executive Function (BRIEF). Lehtonen et al. (13) reported poorer performance of NF1 children, who scored 1.5 SDs or more, below the normative mean. Champion et al. (17) examined parent ratings of the functional executive skills of children and adolescents with NF1. Assessments were made using the Behavioral Regulation Index, the Metacognition Index, and the Global Executive Composite. They found that participants showed significantly more behavioral executive difficulties than expected from the normative data.
Galasso et al. (21) studied individual features of executive function as planning aspects and their association with attention. They found no correlation between Tower of London test scores and Conners ratings scale for parents’ scores in children with NF1. The authors concluded that planning and problem-solving deficits are not directly related to inattention level. In concordance with these results, Payne et al. (22) showed that executive dysfunction occurred with the same severity in children with NF1, whether or not they had a comorbid diagnosis of ADHD (10).
Gilboa et al. (23) evaluated executive function in 29 children with NF1 and 27 typically developing controls using the Behavioral Assessment of the Dysexecutive Syndrome in Children (BADS-C) and the BRIEF parent questionnaires. The Academic Competence Evaluation Scales (ACES) were used to evaluate academic success. Children with NF1 performed significantly lower on four of the BRIEF scales (initiate, working memory, plan/organize, and organization of materials) and two subtests of the BADS-C (water and key search). Academic skills scores of children with NF1 and typically developing controls fluctuated significantly on the ACES teacher questionnaire variables. Significant correlations were shown between BADS-C subtest scores and ACES scale scores: children who scored higher (better performance) on the BADS-C received higher scores (better performance) from their teachers on the ACES. In addition, children who performed better in the ACES also obtained better performance in the BRIEF questionnaire conducted by the parents.
Attention
Attention deficits have been linked to the NF1 phenotype and show an incidence of 40–50% in NF1 patients (6). The presence of ADHD in children with NF1 is associated with poorer performance in cognitive function, learning, social skills, and academic achievement. However, the impact of ADHD on these abilities, and its association with executive dysfunction, require further study.
Isenberg et al. (12) compared the performance of 55 children with NF1 with normative data for specific measures of attention. They compared mean scores for NF1 patients on each of the dependent Test of Everyday Attention for Children subtest variables with the population means. Sustained auditory attention and divided auditory attention evaluated using the score and score DT, respectively, differed significantly. The Conners Continuous Performance Test—2nd Edition was also used to evaluate attention. NF1 children’s scores showed greater omissions and commissions compared with the general population mean. No significant differences were found for hit reaction time, block change, or hit standard error block change. Based on parental responses on the Conners 3rd Edition—Parent scale, a large portion (23 of the 55 participants) of the sample met the ADHD criteria of the Diagnostic and Statistical Manual of Mental Disorders—4th Edition, Text Revision, but children with NF1 and ADHD did not differ significantly from children without ADHD on attention measures.
Pride et al. (24) showed that NF1 and ADHD children had a poorer performance in measures of mathematical reasoning, receptive language, sustained attention, reading, and spelling compared with children with NF1 only. In addition, he found that visuospatial planning and skills (assessed using the Tower of London and JLO tests, respectively) predicted academic performance in children with NF1 only. On the BRIEF test, parents and teachers also rated children with NF1 and ADHD more severely than in the NF1 only group. ADHD symptom severity (Conners ADHD/DSM-IV Scales—inattentive index) and a measure of attentional control (Test of Everyday Attention for Children—creature counting) were the best tests to predict academic performance in both groups. In children with NF1 and ADHD, BRIEF scores (Global Executive parent version) was more effective in predicting academic performance. Supporting these findings, Lidzba et al. (25) showed that patients with ADHD symptoms had significantly worse outcomes than those without ADHD symptoms in main effects full-scale, verbal, and performance-related IQ, with no differences between ADHD subtypes.
However, usually ADHD symptoms were not influenced by poor outcomes of the subtest in patients with NF1 (visuospatial skills and arithmetic). Although further cognitive impairment could be predicted in children with NF1 and concomitant ADHD, some studies have shown no difference in specific skills between NF1 children with ADHD and children with NF1 only. Moreover, Barquero et al. (11) found that scores for ADHD symptoms according to Conners Parent Rating were similar in the four reading groups assessed (NF1 and reading impairment, idiopathic reading deficit, reading deficit reading group, and typical development). In addition, Payne et al. (22) studied SWM and inhibitory control in NF1 children with and without comorbid ADHD. Compared with typically, developing children, both groups demonstrated significant impairments in these aspects and there were no between-group differences. Finally, Roy et al. (26) reported that NF1 children had worse outcomes than control children on tasks of spontaneous and reactive cognitive flexibility, even when intelligence and basic skills were partially excluded. However, ADHD symptoms did not negatively impact performance on tests.
Emotionality, Behavior Problems, and Social Competence
Parent evaluations of NF1 children are an appropriate indicator of behavioral, social, and emotional performance. In relation to theses aspects, Allen et al. (27) reported that scores on the Pediatric Quality of Life Inventory indicated that children with NF1 had significantly lower parent- and child-rated social functioning and lower overall parent-rated emotional functioning. Scores on the Child Behavior Checklist showed that these children also displayed more internalizing and externalizing problems and greater social problems than typically developing peers. A trend was noted for parents’ ratings on social problems and inattention in NF1 children, indicating a positive association between inattention and social problems. Participants also completed a measure of facial expression recognition, the Diagnostic Analysis of Nonverbal Accuracy–Revised. Children with NF1 recognized less the faces of children and adults in low intensity conditions.
Autism
Neurofibromatosis type 1 children show poorer social skills and social competence and a high percentage of individuals with NF1 have social deficits. Attention deficits have an important effect on poor social outcomes (5, 28–30). However, the link between attention and social competence deficits in children with NF1 remains unclear. Several articles on ASD in patients with NF1 have been written in recent years. Here, we report only the findings of Walsh et al. (30), as this article was the only one that met the inclusion criteria.
Walsh et al. (30) evaluated ASD symptomatology in 66 children with NF1. Forty percent of the children with NF1 presented symptoms at levels with clinical significance on the Social Responsiveness Scale, and 14% of this group showed symptoms at the levels observed in children with ASD. The increased of the symptom levels was not explained byNF1 severity or externalizing and internalizing behavioral. The relationship between symptoms of ADHD and ASD was statistically significant. There were also interesting relationships between ADHD and deficits in the social domain of conscience and motivation.
Neuroimaging
One of the findings described in magnetic resonance imaging (MRI) are circumscribed areas of hyperintensity in T2-weighted imaging (T2H). These lesions seem to represent areas of demyelination or increased fluid within the myelin sheath and have been associated with cognitive impairment. However, these lesions tend to disappear over time and the relation between lesion presence, lesion quantity, and cognitive impairment is unclear (31, 32). Payne et al. (33) followed the course of T2H and cognitive function in 18 children with NF1 for 18 years. They found a significant improvement in general cognitive function in NF1 patients over the follow-up. The increase in cognitive function was restricted to participants with discrete T2H in childhood. Patients without lesions in childhood exhibited unchanged performance in cognitive function. The amount of T2H, mainly in the case of discrete lesions, decreased over time. Lesions in the cerebral hemispheres and deep white matter remained stable. The lesions located in the basal ganglia, thalamus, and brainstem resolved in many cases. The authors suggest that the presence of T2H can predict cognitive performance in childhood but not in adulthood.
Two articles reported additional interesting results related to T2H. Roy et al. (34) found that the presence, number, size, or location of T2H lesions did not affect executive dysfunction in NF1 children. On the other hand, Piscitelli et al. (35) found that patients with T2H in the cerebellum showed a lower IQ than patients without T2H in that brain location, possibly because of impaired visuospatial ability and language. Clinical impairment was more frequent in patients with T2H in comparison with those without these lesions, although the group differences were not statistically significant.
Intracranial manifestations of NF1 are also of interest, but their pathogenesis and effects on neurocognitive function have not been clearly described. Regarding this aspect, Aydin et al. (36) studied the relationship between corpus callosum (CC) characteristics and neurocognitive impairment in children with NF1 using diffusion tensor imaging features. Children with NF1 showed a significantly larger total CC area than healthy controls. The values of apparent diffusion coefficient for the CC genu were significantly higher in NF1 participants in comparison with healthy controls. The correlations between the values of apparent diffusion coefficient for the CC genu and the digit and arithmetic span scores (verbal IQ and performance IQ scores) was negative, and between the fractional anisotropy values of the genu and coding scores (verbal IQ and performance IQ scores) in NF1 participants were negative. Huijbregts et al. (37) used MRI scanning to study cerebral volumetric abnormalities in children with NF1. They found that larger left putamen volume, larger total white matter volume, and smaller precentral gyrus gray matter density in children with NF1 were associated with a higher rate of social problems (evaluated using Child Behavior Checklist parent ratings). Larger right amygdala volume in children with NF1 was associated with autistic mannerisms (evaluated using Social Responsiveness Scale parent ratings).
Resting-state functional imaging has been used to assess the integrity of brain functional connectivity networks, as abnormal function is related to neurocognitive deficits. Using resting-state functional scanning, Loitfelder et al. (38) studied functional connectivity. In patients with NF1, there were associations between the frontal and temporo-frontal functional connectivity of the ventral anterior cingulate ventral cortex, bilateral amygdala, bilateral orbitofrontal cortex, and posterior cingulate cortex with cognitive, social, and behavioral deficit. Violante et al. (39) using functional MRI to study early visual cortical pathways found that children and adults with NF1 showed poor activation of the low-level visual cortex. This may be interpreted, as that low-level visual processing disorder do not improve over time. There was a specific impairment of the magnocellular visual pathway in early visual processing related to poor default network deactivation. This evidence may help to understand the neural substrate for higher order (specifically, visuospatial and attentional) cognitive deficits present in NF1.
Pharmacological Interventions
Statins such as lovastatin, which inhibit HMG-CoA reductase, acted on synaptic plasticity and improved learning and attention deficits in a mouse model of NF1 (40). Payne et al. (41) evaluated the effects of lovastatin in children with NF1 who previously demonstrated impairments of visuospatial learning and attention. Lovastatin had no significant effect on primary outcomes (visuospatial learning and sustained attention) after 16 weeks of treatment. The medication was well tolerated and did not increase adverse events compared with a placebo. Van der Vaart et al. (42) studied the results of simvastatin use on cognitive deficits and behavioral disorders in patients with NF1. Twelve months of treatment had no effect on intelligence, attention, and internalizing of behavioral problems. However, more studies in humans are needed to evaluate these effects.
Methylphenidate (MPD), a psychostimulant frequently used for ADHD due to its action on dopamine and the noradrenergic system (43), may have beneficial effects in patients with NF1 (43). Lidzba et al. (44) studied the effects of MPD on cognition in children with NF1 and ADHD. They showed that the full-scale IQ of medicated children with NF1 improved between two periods, an effect not evident in other groups. When attention measures were used as covariates, the effect remained marginally significant. Lion-Francois et al. (45) also studied the effects of MPD in NF1 children with ADHD-like symptoms. They found that Simplified Conners’ Parent Rating Scale scores decreased by 3.9 points in medicated children. In contrast to these results, Isenberg et al. (12) found that parental responses on the Conners 3rd Edition—Parent scale indicated that children on treatment with stimulant medication were more inattentive and oppositional than children not on medication.
Discussion
Cognitive Skills and Intelligence
Neurofibromatosis type 1 children show to some extent, lower performance than their typically developing peers on intelligence tests do, with 90% IQ scores between low and average range. However, up to 40% of NF1 children present learning disabilities. Difficulties with academic performance are also common. Cognitive impairment in these children may be related to social difficulties, attention deficit, behavioral and emotional problems (4, 6, 46, 47). Disagreement persists about the precise IQ profile of children with NF1. Most articles included in this review indicated a slightly below average performance on all IQ variables. However, significantly lower full-scale IQ has also been reported (17). In particular, articles mentioned poor performance in cognitive planning skills, verbal intelligence, and working and non-working memory. Klein-Tasman et al. (48) found similar results for young children (3–6 years of age) with NF1, almost half of who showed cognitive vulnerabilities.
In relation to language, deficits in phonological skills and receptive language have been described in children with NF1. There are insufficient studies to confirm the consistency of these findings and the nature of deficits in specific areas of linguistic development is still unclear. Recent findings support earlier results showing significant alterations in language, reading, and spelling in children with NF1 (4, 6, 47). School-age children exhibit significantly more delays in reading and math than preschool-age children (10). Competence related to lexical/phonological strategies and mental arithmetic seems to be a significant predictor of differences among individuals in the acquisition of reading skills and math (9). Orraca-Castillo et al. (9) replicated the findings of Watt et al. (49) and showed a high prevalence of dyslexia (greater than 50%) in this population.
Speech production in children with NF1 has not been widely studied. We reviewed a study by Cosyns et al. (8) on speech quality in Flemish adults and children. Their findings supported previous work by Alivuotila et al. (50) who showed that difficulties experienced by children with NF1 in producing speech sounds do not seem to be language dependent, but may be a particular trait of this condition. Brei et al. (51) reported that young children of 4–6 years had an increased risk of language difficulties. Although deficits in the auditory temporal processing have demonstrated an association with cognitive impairment and language deficits (52), these aspects have not been well studied in recent years.
In relation to visuospatial function in children with NF1 (53), recent evaluations using the JLO test showed poor performance compared with healthy siblings (12, 13). Evaluations of visuospatial learning using paired associate learning tests from the Cambridge Automated Neuropsychological Test Assessment Battery also indicate significant impairment in children with NF1 (13, 14). Research on the neural mechanisms of visuospatial deficits indicates that abnormal long-latency visual evoked potentials and specific enhancement of alpha brain oscillations are related to problems in attention allocation (16). Slower global responses and weakened resistance to interference in reactivity to visual signals have also been reported (15).
Recent studies on motor function indicate deficits in motor skills associated with poorer reasoning and working memory indexes (17), supporting previous results (54). Reduced visual-motor integration and poor tracing outcomes evaluated using the Beery–Buktenica Developmental Test of Visual-Motor Integration copy test have also been reported (18). Wessel et al. (10) found delays in gross and fine motor responses. Interestingly, using longitudinal assessments, they showed that children changed frequently between delayed and non-delayed groups in most areas excluding gross motor development. These patients also showed an inability to adopt rhythmic stimuli. A study by Iannuzzi et al. (55) (not included because of age criteria) suggested that fine motor skills impairment in young NF1 children may result from a comorbidity between NF1 and language disorders. More studies are needed to understand this possible correlation.
Executive Function and Attention
Evaluations using the BRIEF tests have shown poor executive function in children with NF1. Reports also indicate greater executive behavioral difficulties than expected (13, 17), but no correlations between the planning aspects of executive function and attention. Impairment of executive function seems to be independent of attention (21, 22). Lehtonen et al. (6) had suggested the importance of studying academic achievement in relation to executive function. Gilboa et al. (23) examined these abilities and found a significant correlation between poor executive function and academic difficulties, suggesting that academic performance depends on several cognitive and behavioral domains (4). Studies of adolescents have shown similar significant correlations between executive dysfunction and academic achievement (56). Executive function deficits have been reported as a core feature of NF1, not a secondary effect derived from other variables (57).
Some research indicates that compared with children with NF1 only, children with NF1 and ADHD have a poorer performance on all cognitive attentional measures and on executive function (24, 25). In contrast, several studies indicate the presence of attention deficits in children with NF1 that do not seem to affect the performance of specific skills compared with children with NF1 only. Reading (11), spontaneous and reactive cognitive flexibility tasks (26), SWM and inhibitory control (22) were not adversely affected by ADHD symptomatology. The association between attention deficits and motor skills has not been well studied. A study by Casnar et al. (58) (not included here because of age criteria) found no correlation between fine motor skills and parental reports of attention in younger NF1 patients. Further studies in this area are needed.
Emotionality, Behavior Problems, and Social Competence
Research findings on emotion, behavior, and social competence have been replicated by Allen et al. (27). Generally, children with NF1 show lower emotional and social functioning and more internalizing and externalizing problems. Facial expression recognition is weaker in low-intensity conditions and inattention is related to greater social problems in children with NF1. Importantly, it has been demonstrated that NF1 patients also experience a higher degree of loneliness than siblings (59) and lower participation in activities that require development of specific skills, including physical activity (60), more anxiety symptoms (61, 62), and more sleep disturbances (63). In particular, children with NF1 and plexiform neurofibromas have positive scores in the significant risk/clinical ranges on several parent and teacher subscales of the Behavior Assessment System for Children—Second Edition, including somatization, attention problems, depression, and withdrawal (64). These problems should be considered, as they contribute to poorer cognitive performance, social interaction, and emotional function. Children with NF1 could benefit from interventions focused on social skills and emotional support.
There are several recent articles on ASD in patients with NF1. Here, we report only the results of Walsh et al. (30), as this was the only article that met the age criteria. Generally, studies suggest a higher prevalence of autistic traits and ASD among patients with NF1 (5, 30, 65, 66) and the cooccurrence of ASD symptoms with ADHD symptoms (30, 66). Some researchers have tried to characterize the phenotypic profile of ASD in patients with NF1. Findings indicate that children with NF1 who have ASD symptoms tend to show more social impairment than restrictive/repetitive behaviors (28, 29). Regarding screening tools for ASD symptoms in children with NF1, no significant differences in screen-positive rates between children with NF1 and controls have been reported (67).
Neuroimaging
Previous studies indicate that children with NF1 and T2H have lower IQ scores and poorer visuospatial and fine motor skills (68, 69). Severe impairment is particularly associated with lesions in the thalamus (70, 71). Recent studies of T2H mention findings in relation to presence, location, and cognitive impairment. NF1 patients with T2H in the cerebellum show lower IQs than those without (35). However, executive function is not influenced by T2H in NF1 children (34). One study not included here because of age criteria reported no correlation between the presence of T2H in MRI of any brain region and ratings on the social/emotional parameters of the Strengths and Difficulties Questionnaire in children with NF1 (72).
Evidence of improvement in cognitive ability over time in NF1 patients with T2H remains controversial. In 2003, Hyman et al. (31) reported a significant decrease of T2H in terms of number, size, and intensity over an 8-year period in NF1 children that was not related to changes of cognitive ability in adulthood. In contrast, another study found improvements in cognitive function over an 18-year period in children with discrete T2H (33). The disparity in these results may be related to the time of follow-up and the characteristics of T2H. More studies are needed to clarify this association.
Regarding intracranial manifestations of NF1, positive associations have been found between volume of specific brain structures and social problems (assessed using Child Behavior Checklist parent ratings and Social Responsiveness Scale ratings of autistic mannerisms) (36, 37). Based on previous reports of CC enlargement in children with NF1, Aydin et al. (36) examined the association between CC integrity and cognitive disabilities in children with NF1 and healthy controls. Diffusion tensor imaging showed no association between larger CC area and IQ scores but (compared with controls) there was a negative correlation between higher apparent diffusion coefficient and fractional anisotropy values of the genu and poorer arithmetic and verbal performances. Loitfelder et al. (38) used resting-state functional imaging and found associations of increased frontofrontal and functional connectivity with impairment at social, cognitive, and behavioral levels. Children and adults with NF1 showed weak activation of the low-level visual cortex and specific impairment of the magnocellular visual pathway (39).
Pharmacological Interventions
Although lovastatin reverses learning deficits in a mouse model of NF1 (40), the benefits of this medication have not been clearly demonstrated in humans. The studies we reviewed of statins did not show positive effects on children with NF1. Lovastatin did not have a significant effect on visuospatial learning and sustained attention in NF1 children and simvastatin did not have on attention, full-scale intelligence, and internalizing behavioral problems. A recent study of lovastatin and neurobehavioral function (not included here because of age criteria) showed beneficial effects of this medication on some functions related to learning and memory and on internalizing symptoms in patients aged 10–50 years (73). Further studies are needed to identify possible benefits in humans.
Methylphenidate has shown benefits by decreasing ADHD symptomatology and has a good risk-benefit profile (43, 74, 75). Therefore, the effects of MPD on cognition in children with NF1 and ADHD have been evaluated. The full-scale IQ scores of medicated children with NF1 improved significantly and MPD also decreased simplified Conners scores (45). In contrast, one study reported that children taking stimulant medication were more inattentive and oppositional than children not on medication according to Conners 3rd Edition—Parent ratings (12). More studies are needed to corroborate these effects.
Methodological Issues
Most of the studies recruited samples from medical centers, clinics, schools, and clinical trial websites. In some studies, the method of recruitment was not completely clear and information about the number of participants at the start and end of the study was lacking. Siblings, community, and normative data were used as comparison groups. It is important to point out that it is not always easy to interpret results and establish correlations owing to differences between samples and comparison groups (6).
Several studies included in this review did not control for IQ differences in analyses [only three studies controlled for IQ (13, 18, 27)]. Whether IQ should be controlled as a covariate remains controversial. Dennis et al. (76) found that several anomalous results in neurocognitive function studies have been caused by using IQ as a covariate. It has also been suggested that many differences disappear when IQ is controlled for; however, there are no recommendations of when IQ control should be used (6). Another concern is the adequacy of the tools to measure cognitive and behavioral functions. These constructs are complex and aspects of these functions (particularly executive function) frequently overlap. Evaluating the theoretical background of these constructs remains important (6). We did not include ongoing and unpublished studies and we did not identify any non-English language articles that met the inclusion criteria.
Future Directions
Future research on NF1 should evaluate those aspects of the disorder for which findings remain inconclusive. Analysis of the interaction between cognitive and social processes may generate important information that could guide social interventions (27). In addition, reading interventions could be conducted with larger samples and in combination with pharmaceutical interventions, such as lovastatin (11, 73) and MPD, which have shown some benefits for cognitive function (45). More studies on motor skills are needed to clarify the interdependency between these skills and neurocognitive performance (17), attention deficits (58), and language (55). Systematic investigation of metacognitive constructs to obtain more conclusive results remains an important issue (6). Given the suggested relation between deficits in executive function and poor academic performance in NF1 children, the study of interventions to improve executive skills could make an important contribution to the management and follow-up of these patients (56). Finally, investigations using neuroimaging techniques could provide a better understanding of the mechanisms involved in cognitive and social functioning in children with NF1 (35, 37).
Author Contributions
AM and PG provided conceptual guidance on the manuscript. MN, AM, PG, and CC wrote the manuscript.
Conflict of Interest Statement
The authors declared no potential conflicts of interest in relation to the research, authorship, and publication of this article.
Acknowledgments
We acknowledge the support of Universidad Del Rosario to write this article.
Funding
Universidad Del Rosario supported this research article.
Abbreviations
ACES, academic competence evaluation scales; ADHD, attention-deficit/hyperactivity disorder; ASD, autism spectrum disorder; BADS-C, behavioral assessment of the dysexecutive syndrome in children; BRIEF, behavior rating inventory of executive function; CC, corpus callosum; JLO, judgment of line orientation; MPD, methylphenidate; MRI, magnetic resonance imaging; NF1, neurofibromatosis type 1; SWM, spatial working memory; T2H, T2-hyperintensities.
References
1. Evans DG, Howard E, Giblin C, Clancy T, Spencer H, Huson SM, et al. Birth incidence and prevalence of tumor-prone syndromes: estimates from a UK family genetic register service. Am J Med Genet A (2010) 152A(2):327–32. doi:10.1002/ajmg.a.33139
2. Lammert M, Friedman JM, Kluwe L, Mautner VF. Prevalence of neurofibromatosis 1 in German children at elementary school enrollment. Arch Dermatol (2005) 141(1):71–4. doi:10.1001/archderm.141.1.71
3. DeBella K, Szudek J, Friedman JM. Use of the national institutes of health criteria for diagnosis of neurofibromatosis 1 in children. Pediatrics (2000) 105(3 Pt 1):608–14. doi:10.1542/peds.105.3.608
4. Schwetye KE, Gutmann DH. Cognitive and behavioral problems in children with neurofibromatosis type 1: challenges and future directions. Expert Rev Neurother (2014) 14(10):1139–52. doi:10.1586/14737175.2014.953931
5. Garg S, Green J, Leadbitter K, Emsley R, Lehtonen A, Evans DG, et al. Neurofibromatosis type 1 and autism spectrum disorder. Pediatrics (2013) 132(6):e1642–8. doi:10.1542/peds.2013-1868
6. Lehtonen A, Howie E, Trump D, Huson SM. Behaviour in children with neurofibromatosis type 1: cognition, executive function, attention, emotion, and social competence. Dev Med Child Neurol (2013) 55(2):111–25. doi:10.1111/j.1469-8749.2012.04399.x
7. Moher D, Liberati A, Tetzlaff J, Altman DG. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. PLoS Med (2009) 6(7):e1000097. doi:10.1016/j.ijsu.2010.02.007
8. Cosyns M, Mortier G, Janssens S, Bogaert F, D’Hondt S, Van Borsel J. Articulation in schoolchildren and adults with neurofibromatosis type 1. J Commun Disord (2012) 45(2):111–20. doi:10.1016/j.jcomdis.2011.11.002
9. Orraca-Castillo M, Estevez-Perez N, Reigosa-Crespo V. Neurocognitive profiles of learning disabled children with neurofibromatosis type1. Front Hum Neurosci (2014) 8:386. doi:10.3389/fnhum.2014.00386
10. Wessel LE, Gao F, Gutmann DH, Dunn CM. Longitudinal analysis of developmental delays in children with neurofibromatosis type 1. J Child Neurol (2013) 28(12):1689–93. doi:10.1177/0883073812462885
11. Barquero LA, Sefcik AM, Cutting LE, Rimrodt SL. Teaching reading to children with neurofibromatosis type 1: a clinical trial with random assignment to different approaches. Dev Med Child Neurol (2015) 57(12):1150–8. doi:10.1111/dmcn.12769
12. Isenberg JC, Templer A, Gao F, Titus JB, Gutmann DH. Attention skills in children with neurofibromatosis type 1. J Child Neurol (2013) 28(1):45–9. doi:10.1177/0883073812439435
13. Lehtonen A, Garg S, Roberts SA, Trump D, Evans DG, Green J. Cognition in children with neurofibromatosis type 1: data from a population-based study. Dev Med Child Neurol (2015) 57(7):645–51. doi:10.1111/dmcn.12734
14. Payne JM, Barton B, Shores EA, North KN. Paired associate learning in children with neurofibromatosis type 1: implications for clinical trials. J Neurol (2013) 260(1):214–20. doi:10.1007/s00415-012-6620-5
15. Michael GA, Garcia S, Herbillon V, Lion-Francois L. Reactivity to visual signals in neurofibromatosis type 1: is everything ok? Neuropsychology (2014) 28(3):423–8. doi:10.1037/neu0000046
16. Ribeiro MJ, d’Almeida OC, Ramos F, Saraiva J, Silva ED, Castelo-Branco M. Abnormal late visual responses and alpha oscillations in neurofibromatosis type 1: a link to visual and attention deficits. J Neurodev Disord (2014) 6:4. doi:10.1186/1866-1955-6-4
17. Champion JA, Rose KJ, Payne JM, Burns J, North KN. Relationship between cognitive dysfunction, gait, and motor impairment in children and adolescents with neurofibromatosis type 1. Dev Med Child Neurol (2014) 56(5):468–74. doi:10.1111/dmcn.12361
18. Debrabant J, Plasschaert E, Caeyenberghs K, Vingerhoets G, Legius E, Janssens S, et al. Deficient motor timing in children with neurofibromatosis type 1. Res Dev Disabil (2014) 35(11):3131–8. doi:10.1016/j.ridd.2014.07.059
19. Gilboa Y, Josman N, Fattal-Valevski A, Toledano-Alhadef H, Rosenblum S. Underlying mechanisms of writing difficulties among children with neurofibromatosis type 1. Res Dev Disabil (2014) 35(6):1310–6. doi:10.1016/j.ridd.2014.03.021
20. Gilboa Y, Rosenblum S, Fattal-Valevski A, Toledano-Alhadef H, Rizzo AS, Josman N. Using a virtual classroom environment to describe the attention deficits profile of children with neurofibromatosis type 1. Res Dev Disabil (2011) 32(6):2608–13. doi:10.1016/j.ridd.2011.06.014
21. Galasso C, Lo-Castro A, Di Carlo L, Pitzianti MB, D’Agati E, Curatolo P, et al. Planning deficit in children with neurofibromatosis type 1: a neurocognitive trait independent from attention-deficit hyperactivity disorder (ADHD)? J Child Neurol (2014) 29(10):1320–6. doi:10.1177/0883073813517001
22. Payne JM, Arnold SS, Pride NA, North KN. Does attention-deficit-hyperactivity disorder exacerbate executive dysfunction in children with neurofibromatosis type 1? Dev Med Child Neurol (2012) 54(10):898–904. doi:10.1111/j.1469-8749.2012.04357.x
23. Gilboa Y, Rosenblum S, Fattal-Valevski A, Toledano-Alhadef H, Josman N. Is there a relationship between executive functions and academic success in children with neurofibromatosis type 1? Neuropsychol Rehabil (2014) 24(6):918–35. doi:10.1080/09602011.2014.920262
24. Pride NA, Payne JM, North KN. The impact of ADHD on the cognitive and academic functioning of children with NF1. Dev Neuropsychol (2012) 37(7):590–600. doi:10.1080/87565641.2012.695831
25. Lidzba K, Granstrom S, Lindenau J, Mautner VF. The adverse influence of attention-deficit disorder with or without hyperactivity on cognition in neurofibromatosis type 1. Dev Med Child Neurol (2012) 54(10):892–7. doi:10.1111/j.1469-8749.2012.04377.x
26. Roy A, Barbarot S, Roulin JL, Charbonnier V, Fasotti L, Stalder JF, et al. Is executive function specifically impaired in children with neurofibromatosis type 1? A neuropsychological investigation of cognitive flexibility. Appl Neuropsychol Child (2014) 3(2):94–102. doi:10.1080/21622965.2012.704185
27. Allen T, Willard VW, Anderson LM, Hardy KK, Bonner MJ. Social functioning and facial expression recognition in children with neurofibromatosis type 1. J Intellect Disabil Res (2016) 60(3):282–93. doi:10.1111/jir.12248
28. Plasschaert E, Descheemaeker MJ, Van Eylen L, Noens I, Steyaert J, Legius E. Prevalence of autism spectrum disorder symptoms in children with neurofibromatosis type 1. Am J Med Genet B Neuropsychiatr Genet (2015) 168B(1):72–80. doi:10.1002/ajmg.b.32280
29. Garg S, Plasschaert E, Descheemaeker MJ, Huson S, Borghgraef M, Vogels A, et al. Autism spectrum disorder profile in neurofibromatosis type I. J Autism Dev Disord (2015) 45(6):1649–57. doi:10.1007/s10803-014-2321-5
30. Walsh KS, Velez JI, Kardel PG, Imas DM, Muenke M, Packer RJ, et al. Symptomatology of autism spectrum disorder in a population with neurofibromatosis type 1. Dev Med Child Neurol (2013) 55(2):131–8. doi:10.1111/dmcn.12038
31. Hyman SL, Gill DS, Shores EA, Steinberg A, Joy P, Gibikote SV, et al. Natural history of cognitive deficits and their relationship to MRI T2-hyperintensities in NF1. Neurology (2003) 60(7):1139–45. doi:10.1212/01.WNL.0000055090.78351.C1
32. Gill DS, Hyman SL, Steinberg A, North KN. Age-related findings on MRI in neurofibromatosis type 1. Pediatr Radiol (2006) 36(10):1048–56. doi:10.1007/s00247-006-0267-2
33. Payne JM, Pickering T, Porter M, Oates EC, Walia N, Prelog K, et al. Longitudinal assessment of cognition and T2-hyperintensities in NF1: an 18-year study. Am J Med Genet A (2014) 164A(3):661–5. doi:10.1002/ajmg.a.36338
34. Roy A, Barbarot S, Charbonnier V, Gayet-Delacroix M, Stalder JF, Roulin JL, et al. Examining the frontal subcortical brain vulnerability hypothesis in children with neurofibromatosis type 1: are T2-weighted hyperintensities related to executive dysfunction? Neuropsychology (2015) 29(3):473–84. doi:10.1037/neu0000151
35. Piscitelli O, Digilio MC, Capolino R, Longo D, Di Ciommo V. Neurofibromatosis type 1 and cerebellar T2-hyperintensities: the relationship to cognitive functioning. Dev Med Child Neurol (2012) 54(1):49–51. doi:10.1111/j.1469-8749.2011.04139.x
36. Aydin S, Kurtcan S, Alkan A, Guler S, Filiz M, Yilmaz TF, et al. Relationship between the corpus callosum and neurocognitive disabilities in children with NF-1: diffusion tensor imaging features. Clin Imaging (2016) 40(6):1092–5. doi:10.1016/j.clinimag.2016.06.013
37. Huijbregts SCJ, Loitfelder M, Rombouts SA, Swaab H, Verbist BM, Arkink EB, et al. Cerebral volumetric abnormalities in neurofibromatosis type 1: associations with parent ratings of social and attention problems, executive dysfunction, and autistic mannerisms. J Neurodev Disord (2015) 7(1):1–9. doi:10.1186/s11689-015-9128-3
38. Loitfelder M, Huijbregts SC, Veer IM, Swaab HS, Van Buchem MA, Schmidt R, et al. Functional connectivity changes and executive and social problems in neurofibromatosis type I. Brain Connect (2015) 5(5):312–20. doi:10.1089/brain.2014.0334
39. Violante IR, Ribeiro MJ, Cunha G, Bernardino I, Duarte JV, Ramos F, et al. Abnormal brain activation in neurofibromatosis type 1: a link between visual processing and the default mode network. PLoS One (2012) 7(6):e38785. doi:10.1371/journal.pone.0038785
40. Li W, Cui Y, Kushner SA, Brown RA, Jentsch JD, Frankland PW, et al. The HMG-CoA reductase inhibitor lovastatin reverses the learning and attention deficits in a mouse model of neurofibromatosis type 1. Curr Biol (2005) 15(21):1961–7. doi:10.1016/j.cub.2005.09.043
41. Payne JM, Barton B, Ullrich NJ, Cantor A, Hearps SJ, Cutter G, et al. Randomized placebo-controlled study of lovastatin in children with neurofibromatosis type 1. Neurology (2016) 87(24):2575–84. doi:10.1212/WNL.0000000000003435
42. van der Vaart T, Plasschaert E, Rietman AB, Renard M, Oostenbrink R, Vogels A, et al. Simvastatin for cognitive deficits and behavioural problems in patients with neurofibromatosis type 1 (NF1-SIMCODA): a randomised, placebo-controlled trial. Lancet Neurol (2013) 12(11):1076–83. doi:10.1016/S1474-4422(13)70227-8
43. Engert V, Pruessner JC. Dopaminergic and noradrenergic contributions to functionality in ADHD: the role of methylphenidate. Curr Neuropharmacol (2008) 6(4):322–8. doi:10.2174/157015908787386069
44. Lidzba K, Granstroem S, Leark RA, Kraegeloh-Mann I, Mautner VF. Pharmacotherapy of attention deficit in neurofibromatosis type 1: effects on cognition. Neuropediatrics (2014) 45(4):240–6. doi:10.1055/s-0034-1368117
45. Lion-Francois L, Gueyffier F, Mercier C, Gerard D, Herbillon V, Kemlin I, et al. The effect of methylphenidate on neurofibromatosis type 1: a randomised, double-blind, placebo-controlled, crossover trial. Orphanet J Rare Dis (2014) 9:142. doi:10.1186/s13023-014-0142-4
46. Levine TM, Materek A, Abel J, O’Donnell M, Cutting LE. Cognitive profile of neurofibromatosis type 1. Semin Pediatr Neurol (2006) 13(1):8–20. doi:10.1016/j.spen.2006.01.006
47. Acosta MT, Gioia GA, Silva AJ. Neurofibromatosis type 1: new insights into neurocognitive issues. Curr Neurol Neurosci Rep (2006) 6(2):136–43. doi:10.1007/s11910-996-0036-5
48. Klein-Tasman BP, Janke KM, Luo W, Casnar CL, Hunter SJ, Tonsgard J, et al. Cognitive and psychosocial phenotype of young children with neurofibromatosis-1. J Int Neuropsychol Soc (2014) 20(1):88–98. doi:10.1017/S1355617713001227
49. Watt SE, Shores A, North KN. An examination of lexical and sublexical reading skills in children with neurofibromatosis type 1. Child Neuropsychol (2008) 14(5):401–18. doi:10.1080/09297040701595505
50. Alivuotila L, Hakokari J, Visnapuu V, Korpijaakko-Huuhka AM, Aaltonen O, Happonen RP, et al. Speech characteristics in neurofibromatosis type 1. Am J Med Genet A (2010) 152A(1):42–51. doi:10.1002/ajmg.a.33178
51. Brei NG, Klein-Tasman BP, Schwarz GN, Casnar CL. Language in young children with neurofibromatosis-1: relations to functional communication, attention, and social functioning. Res Dev Disabil (2014) 35(10):2495–504. doi:10.1016/j.ridd.2014.06.016
52. Batista PB, Lemos SM, Rodrigues LO, de Rezende NA. Auditory temporal processing deficits and language disorders in patients with neurofibromatosis type 1. J Commun Disord (2014) 48:18–26. doi:10.1016/j.jcomdis.2013.12.002
53. Hyman SL, Shores A, North KN. The nature and frequency of cognitive deficits in children with neurofibromatosis type 1. Neurology (2005) 65(7):1037–44. doi:10.1212/01.wnl.0000179303.72345.ce
54. Huijbregts S, Swaab H, de Sonneville L. Cognitive and motor control in neurofibromatosis type I: influence of maturation and hyperactivity-inattention. Dev Neuropsychol (2010) 35(6):737–51. doi:10.1080/87565641.2010.508670
55. Iannuzzi S, Albaret JM, Chignac C, Faure-Marie N, Barry I, Karsenty C, et al. Motor impairment in children with neurofibromatosis type 1: effect of the comorbidity with language disorders. Brain Dev (2016) 38(2):181–7. doi:10.1016/j.braindev.2015.08.001
56. Janke KM, Klein-Tasman BP, Garwood MM, Davies WH, Trapane P, Holman KS. Relations between executive functioning and academic performance in adolescents with neurofibromatosis-1. J Dev Phys Disabil (2014) 26(4):431–50. doi:10.1007/s10882-014-9375-3
57. Plasschaert E, Van Eylen L, Descheemaeker MJ, Noens I, Legius E, Steyaert J. Executive functioning deficits in children with neurofibromatosis type 1: the influence of intellectual and social functioning. Am J Med Genet B Neuropsychiatr Genet (2016) 171B(3):348–62. doi:10.1002/ajmg.b.32414
58. Casnar CL, Janke KM, van der Fluit F, Brei NG, Klein-Tasman BP. Relations between fine motor skill and parental report of attention in young children with neurofibromatosis type 1. J Clin Exp Neuropsychol (2014) 36(9):930–43. doi:10.1080/13803395.2014.957166
59. Ejerskov C, Lasgaard M, Ostergaard JR. Teenagers and young adults with neurofibromatosis type 1 are more likely to experience loneliness than siblings without the illness. Acta Paediatr (2015) 104(6):604–9. doi:10.1111/apa.12946
60. Johnson BA, Sheng X, Perry AS, Stevenson DA. Activity and participation in children with neurofibromatosis type 1. Res Dev Disabil (2014) 36C:213–21. doi:10.1016/j.ridd.2014.10.004
61. Pasini A, Lo-Castro A, Di Carlo L, Pitzianti M, Siracusano M, Rosa C, et al. Detecting anxiety symptoms in children and youths with neurofibromatosis type I. Am J Med Genet B Neuropsychiatr Genet (2012) 159B(7):869–73. doi:10.1002/ajmg.b.32095
62. Wolters PL, Burns KM, Martin S, Baldwin A, Dombi E, Toledo-Tamula MA, et al. Pain interference in youth with neurofibromatosis type 1 and plexiform neurofibromas and relation to disease severity, social-emotional functioning, and quality of life. Am J Med Genet A (2015) 167A(9):2103–13. doi:10.1002/ajmg.a.37123
63. Licis AK, Vallorani A, Gao F, Chen C, Lenox J, Yamada KA, et al. Prevalence of sleep disturbances in children with neurofibromatosis type 1. J Child Neurol (2013) 28(11):1400–5. doi:10.1177/0883073813500849
64. Martin S, Wolters P, Baldwin A, Gillespie A, Dombi E, Walker K, et al. Social-emotional functioning of children and adolescents with neurofibromatosis type 1 and plexiform neurofibromas: relationships with cognitive, disease, and environmental variables. J Pediatr Psychol (2012) 37(7):713–24. doi:10.1093/jpepsy/jsr124
65. Constantino JN, Zhang Y, Holzhauer K, Sant S, Long K, Vallorani A, et al. Distribution and within-family specificity of quantitative autistic traits in patients with neurofibromatosis type I. J Pediatr (2015) 167(3):621–6.e1. doi:10.1016/j.jpeds.2015.04.075
66. Garg S, Lehtonen A, Huson SM, Emsley R, Trump D, Evans DG, et al. Autism and other psychiatric comorbidity in neurofibromatosis type 1: evidence from a population-based study. Dev Med Child Neurol (2013) 55(2):139–45. doi:10.1111/dmcn.12043
67. Tinker J, Carbone PS, Viskochil D, Mathiesen A, Ma KN, Stevenson DA. Screening children with neurofibromatosis type 1 for autism spectrum disorder. Am J Med Genet A (2014) 164A(7):1706–12. doi:10.1002/ajmg.a.36549
68. Chabernaud C, Sirinelli D, Barbier C, Cottier JP, Sembely C, Giraudeau B, et al. Thalamo-striatal T2-weighted hyperintensities (unidentified bright objects) correlate with cognitive impairments in neurofibromatosis type 1 during childhood. Dev Neuropsychol (2009) 34(6):736–48. doi:10.1080/87565640903265137
69. Feldmann R, Denecke J, Grenzebach M, Schuierer G, Weglage J. Neurofibromatosis type 1: motor and cognitive function and T2-weighted MRI hyperintensities. Neurology (2003) 61(12):1725–8. doi:10.1212/01.WNL.0000098881.95854.5F
70. Feldmann R, Schuierer G, Wessel A, Neveling N, Weglage J. Development of MRI T2 hyperintensities and cognitive functioning in patients with neurofibromatosis type 1. Acta Paediatr (2010) 99(11):1657–60. doi:10.1111/j.1651-2227.2010.01923.x
71. Hyman SL, Gill DS, Shores EA, Steinberg A, North KN. T2 hyperintensities in children with neurofibromatosis type 1 and their relationship to cognitive functioning. J Neurol Neurosurg Psychiatry (2007) 78(10):1088–91. doi:10.1136/jnnp.2006.108134
72. Cohen R, Steinberg T, Kornreich L, Aharoni S, Halevy A, Shuper A. Brain imaging findings and social/emotional problems in Israeli children with neurofibromatosis type 1. Eur J Pediatr (2015) 174(2):199–203. doi:10.1007/s00431-014-2366-7
73. Bearden CE, Hellemann GS, Rosser T, Montojo C, Jonas R, Enrique N, et al. A randomized placebo-controlled lovastatin trial for neurobehavioral function in neurofibromatosis I. Ann Clin Transl Neurol (2016) 3(4):266–79. doi:10.1002/acn3.288
74. Gilmore A, Milne R. Methylphenidate in children with hyperactivity: review and cost-utility analysis. Pharmacoepidemiol Drug Saf (2001) 10(2):85–94. doi:10.1002/pds.564
75. Schachter HM, Pham B, King J, Langford S, Moher D. How efficacious and safe is short-acting methylphenidate for the treatment of attention-deficit disorder in children and adolescents? A meta-analysis. CMAJ (2001) 165(11):1475–88.
Keywords: neurofibromatosis, neurofibromatosis type 1, cognitive functioning, behavior, attention-deficit/hyperactivity disorder, autism spectrum disorder, executive functions, visuospatial functioning
Citation: Torres Nupan MM, Velez Van Meerbeke A, López Cabra CA and Herrera Gomez PM (2017) Cognitive and Behavioral Disorders in Children with Neurofibromatosis Type 1. Front. Pediatr. 5:227. doi: 10.3389/fped.2017.00227
Received: 06 June 2017; Accepted: 05 October 2017;
Published: 30 October 2017
Edited by:
Carl E. Stafstrom, University of Wisconsin-Madison, United StatesReviewed by:
D. Mishra, Maulana Azad Medical College, IndiaBrahim Tabarki, University of Sousse, Tunisia
Copyright: © 2017 Torres Nupan, Velez Van Meerbeke, López Cabra and Herrera Gomez. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) or licensor are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Alberto Velez Van Meerbeke, YWxiZXJ0by52ZWxlekB1cm9zYXJpby5lZHUuY28=