 Caroline Meijer
Caroline Meijer Raanan Shamir2
Raanan Shamir2- 1Deptartment of Pediatrics, Leiden University Medical Center, Willem Alexander Children's Hospital, Leiden, Netherlands
- 2Institute for Gastroenterology, Nutrition and Liver Diseases, Schneider Children's Medical Center, Sackler Faculty of Medicine, Tel Aviv University, Tel Aviv, Israel
- 3Department of Pediatrics, The Medical University of Warsaw, Warsaw, Poland
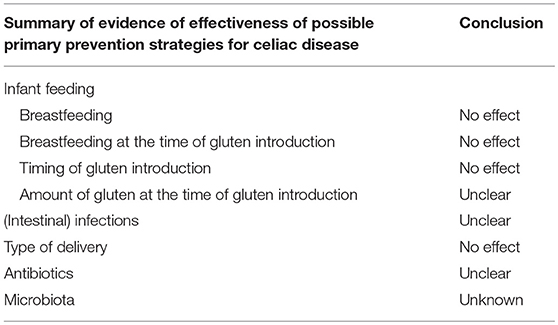
Celiac disease (CD) is a common autoimmune disorder induced by ingestion of gluten in genetically susceptible individuals. Despite the prerequisite for a genetic predisposition, only a minority of the 40% of the Caucasian population that has this genetic predisposition develops the disease. Thus, environmental and/or lifestyle factors play a causal role in the development of CD. The incidence of CD has increased over the last half-century, resulting in rising interest in identifying risk factors for CD to enable primary prevention. Early infant feeding practices have been suggested as one of the factors influencing the risk of CD in genetically susceptible individuals. However, recent large prospective studies have shown that neither the timing of gluten introduction nor the duration or maintenance of breastfeeding influence the risk of CD. Also, other environmental influences have been investigated as potential risk factors, but have not led to primary prevention strategies. Secondary prevention is possible through early diagnosis and treatment. Since CD is significantly underdiagnosed and a large proportion of CD patients are asymptomatic at the time of diagnosis, secondary prevention will not identify all CD patients, as long as mass screening has not been introduced. As following a gluten-free diet is a major challenge, tertiary prevention strategies are discussed as well.
Introduction
The incidence and prevalence of celiac disease (CD) have risen over time; this is, in part, due to the current awareness in combination with the advent of highly sensitive and specific serological tests, but it also reflects a true increase in the prevalence of CD (1, 2). The clinical presentation of CD has changed dramatically in the last decades. Patients with atypical or non-specific symptoms often report a delay in diagnosis of CD that may last for years (3) or even worse, CD remains unrecognized and, therefore, untreated (4–6). Untreated disease is associated with long-term complications, such as chronic anemia, delayed puberty, neuropsychiatric disturbances, associated autoimmune disorders, infertility, small-for-date-births, osteoporosis, and, rarely, malignancy and it can reduce the quality of life (7–9). Treatment with a gluten-free diet (GFD) reduces the burden of morbidity and mortality associated with untreated CD. Thus, prevention would be beneficial (10). Prevention is defined as any activity that reduces the burden of mortality or morbidity from disease, taking place at the primary, secondary, or tertiary level (11) (Table 1). The purpose of this review is to present the current knowledge of the preventive strategies for CD (Table 2).
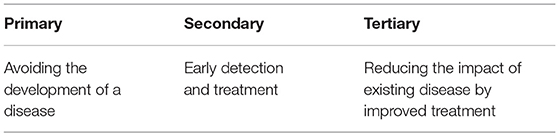
Table 1. Definition of levels of prevention.
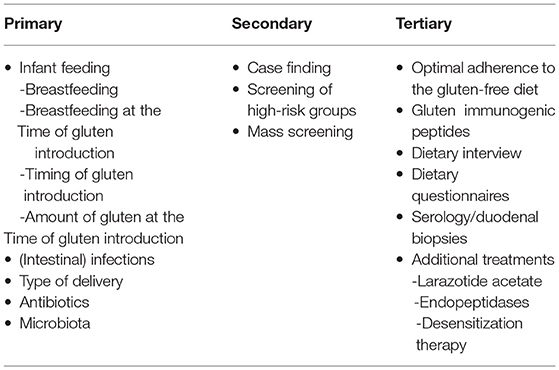
Table 2. Some possible prevention strategies for celiac disease, as discussed in this review.
Primary Prevention
Infant Feeding
Theoretically, CD could be prevented by avoiding gluten introduction into the feeding of infants genetically predisposed to CD. However, this is not a realistic strategy, because the strongest genetic predisposing factors for CD, HLA DQ2 and/or HLA-DQ8, are present in about 40% of the Caucasian population. In addition, most of these individuals do not develop CD, since the prevalence of CD is ~1%. Another reason why avoiding gluten ingestion by a large part of the population is not desirable is that gluten-containing cereals (among others wheat, barley and rye) are important sources of dietary iron, fiber, calcium, folate, and vitamin B12 (12, 13).
Much knowledge about the possible relationship between infant feeding practices and the development of CD has been obtained from “The Swedish epidemic of CD” during the mid-1980s. Between 1985 and 1987, the incidence of CD in Swedish children younger than 2 years of age increased 4-fold, followed by a rapid decline in its incidence around 1995 (14). The occurrence of the epidemic was related to new dietary recommendations: delaying the introduction of all gluten-containing foods to infants until 6 months of age and changes in breastfeeding practices. In Sweden, the incidence of CD diminished when earlier introduction of gluten (>4 months) was reintroduced (14). Many retrospective studies have investigated this hypothesis that delayed introduction of gluten leads to CD with conflicting results. Results of observational studies suggested the existence of a “window of opportunity” for primary prevention, by introducing gluten between 4 and 6 months of age to reduce the risk of CD (Table 3). This and other early feeding practices, such as breastfeeding and breastfeeding at the time of gluten introduction, have been investigated as primary prevention strategies for reducing the risk of CD as well (Tables 4, 5). A systemic review and meta-analysis, which included all of the studies published on this topic between 1966 and 2004, found that breastfed children had a 52% reduction in the risk of being affected by CD compared to those who were not breastfed during the time of gluten introduction (pooled OR 0.48; 95% CI: 0.40 to 0.59) (37). However, all of these studies were observational and retrospective.
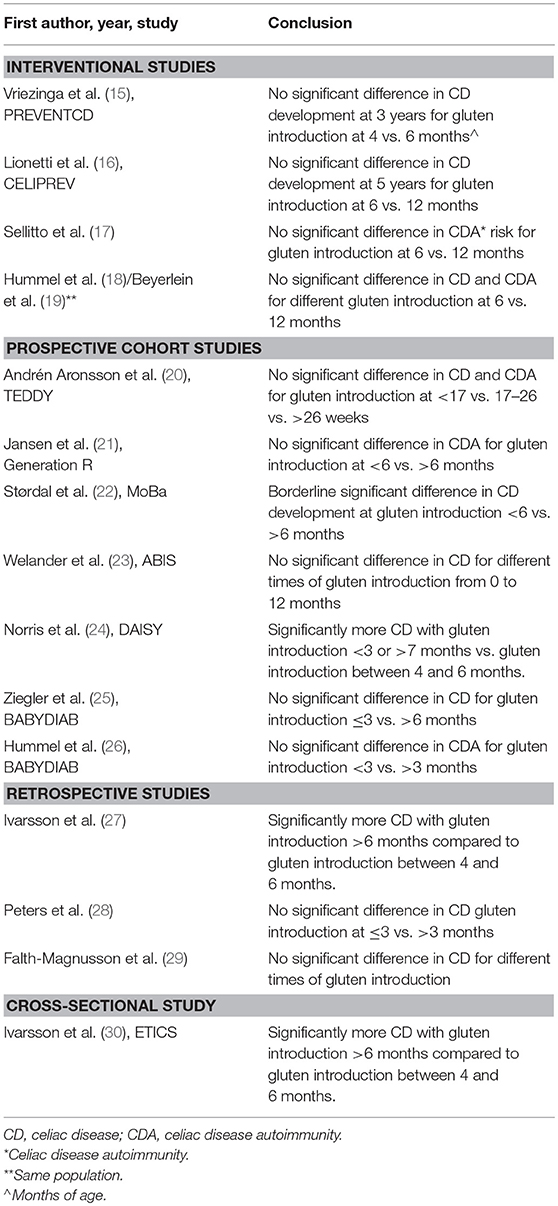
Table 3. Evidence of the effect of the timing of gluten introduction into the diet of young children and the risk of celiac disease.
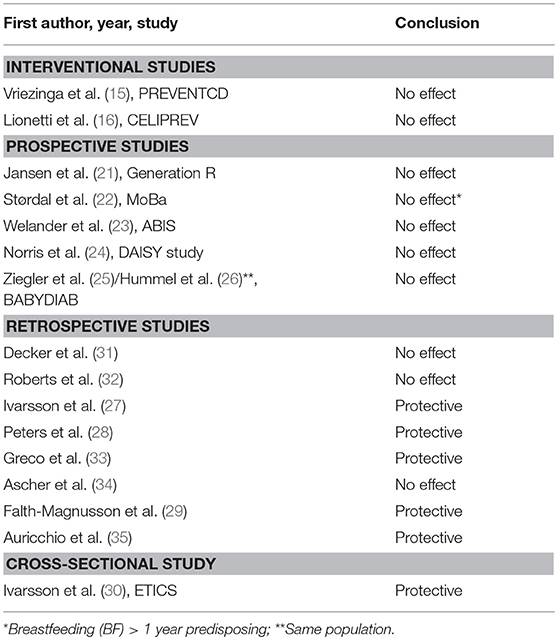
Table 4. Most important studies on the evidence of protection from celiac disease with breastfeeding.
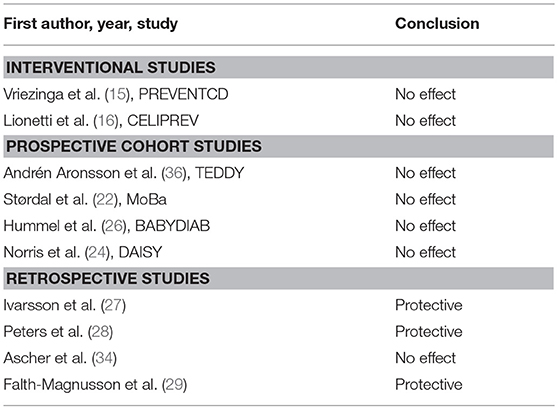
Table 5. Evidence of the effect of breastfeeding at the time of gluten introduction and risk for celiac disease.
Among the prospective studies that have been published, there are two gluten interventional ones, namely PREVENTCD and CELIPREV (15, 16) (Table 3):
• PREVENTCD is a multinational, randomized, double-blind, placebo-controlled dietary interventional study involving 944 children who had at least 1 first-degree relative with CD and HLA-DQ2 and/or DQ8. From age 4 to 6 months, 475 participants received 100 mg of vital gluten daily and 469 received placebo. After 24 weeks, intake of gluten was liberalized in both groups. CD serology was measured periodically. Children with elevated levels of CD antibodies and/or with symptoms suggestive of CD were offered small bowel biopsies to confirm the diagnosis. The results showed no significant difference between the groups receiving the early gluten intervention or placebo in the risk of developing CD at the age of 3 years.
• CELIPREV is an Italian multicenter, randomized, interventional study that compared early (at 6 months of age; n = 297) and delayed (at 12 months of age; n = 256) introduction of gluten into the diet of infants at risk for CD (first-degree relative with CD; HLA-DQ2 and/or DQ8 positivity). The results showed a reduced risk of developing CD by the age of 2 years in those with delayed introduction to gluten at 12 months, but no difference between groups in the risk of developing CD at 5 years of age.
A few of the large, prospective, observational cohort (non-interventional) studies assessing the relationship between infant feeding practices and the risk of CD and/or CD autoimmunity (CDA) pointed out the following (Tables 3–5):
• The Generation R cohort study, including 1679 genetically susceptible CD children from the general population of Rotterdam, the Netherlands, showed that neither breastfeeding for 6 months or longer nor later exposure to gluten (>6 months) compared to earlier exposure (< 6 months) was significantly associated with CDA (21).
• The Norwegian Mother and Child Cohort Study (MoBa) showed that breastfeeding longer than 12 months was associated with a higher risk of CD (22). However, this cohort only considered children with clinically diagnosed CD, so probably missed an important proportion of the children with CD.
• The BABYDIAB, a German cohort study, found no association between the duration of breastfeeding nor gluten introduction before or after 3 months of age and risk of CDA (26).
• The Environmental Determinants of Diabetes in the Young (TEDDY) project is an observational, prospective, cohort study that followed children at genetic risk for type 1 diabetes, wherein development of CD is a secondary outcome. The TEDDY study included 6,403 children with a genetic predisposition to developing CD in the United States, Finland, Germany, and Sweden. The study found that gluten introduction before 17 weeks of age or later than 26 weeks of age was not associated with an increased risk for CDA or CD; however, continuation of breastfeeding more than 1 month after gluten introduction compared with discontinuation of breastfeeding prior to gluten introduction was associated with increased risk of CDA but not of CD (20).
Two systematic reviews and meta-analyses, which included the above prospective interventional studies and large cohort studies (Tables 3–5), concluded that the timing of gluten introduction and the duration or maintenance of breastfeeding do not influence the development of CD (38, 39).
Interest in the quantity of gluten at introduction into the diet of infants was also raised based on the results of the Swedish CD epidemic. The evaluation of results of one retrospective observational study indicated that large amounts of gluten (>16 g/day) at the time of first introduction increased the risk of CD (27). The same group of investigators further compared, in the ETIC project, 2 populations born in 1993 and 1997; they found a lower risk of CD in the population born in 1997 who ingested significantly less gluten-containing cereal compared to the population born in 1993 (24 vs. 38 g/day intake, respectively, under the age of 2 years) (30). Also, the Swedish case control study from the TEDDY cohort, in which gluten intake was assessed by dietary questionnaires, found that a high intake (>5.0 g/day) of gluten during the first 2 years of life was associated with an increased risk of CD (36). However, a similar analysis of the data in the international PREVENTCD study showed that the amount of gluten consumed at 11–36 months of age did not influence the risk for CD development (40). Thus, the influence of the amount of gluten intake on CD risk remains a topic of discussion.
In accordance with the results from the above-mentioned studies, ESPGHAN has updated its guidelines for gluten introduction into the diet of young children. The current recommendation no longer suggests introducing gluten between 4 and 6 months of age; rather they recommend that gluten may be introduced into the infant's diet anytime between 4 and 12 completed months of age, since gluten introduction in these infants does not seem to influence the absolute risk of developing CDA or CD during childhood (38).
In addition to gluten and breastfeeding, other environmental factors may be involved in the risk and/or prevention of CD. Identifying and influencing these factors may lead to preventive strategies. Some of these factors are discussed below.
(Intestinal) Infections
Intestinal infections might change gut permeability and lead to the passage of immunogenic gluten peptides through the epithelial barrier, and thus, activate an autoimmune reaction. Many groups have studied the relationship between infections, both viral and bacterial, and the risk of CD, with varying results (Table 6). The role of early infections was retrospectively explored in the Swedish population-based incident case referent ETICS study. Having three or more parental-reported infections, regardless of the type of infection, during the first 6 months of life was associated with significantly increased risk of CD, even after adjusting for infant feeding and socioeconomic status (61).

Table 6. Some of the most relevant studies# on infections and the risk of celiac disease or celiac disease autoimmunity.
Results of prospective studies are contradictory. Data from the PREVENTCD study showed no significant difference in the cumulative incidence of CD between children with and without parental-reported gastrointestinal infections in the first 18 months of life (15). However, the TEDDY study found that parental-reported early gastrointestinal infections increased the risk of CDA within the following 3 months (HR 1.33; 95% CI 1.11–1.59). This effect was observed particularly in those children with non-HLA-DQ2 genotypes who had been breastfed for < 4 months, as well as in children born in winter and introduced to gluten before the age of 6 months (62). In the prospective MoBa study, children with ≥10 infections (respiratory and gastrointestinal) before 18 months of age had a higher risk of being clinically diagnosed with CD compared with children who had ≤ 4 infections, even after adjustments for antibiotic exposure (63). Viral infections have been suggested to play a role in the development of CD (Table 9), and recently, reovirus has been reported as a trigger for the disease, both in vitro as well as in vivo (60). In vitro, reovirus infection induced a disruption of intestinal immune homeostasis and initiated loss of oral tolerance and T-helper inflammatory immunity to dietary antigens. In CD patients anti-Reovirus antibodies were significantly overrepresented in comparison to health controls.
However, this disruption of the immune homeostasis may not be exclusive to reovirus and their role in the development of CD should be studied prospectively.
Type of Delivery
The mode of delivery (vaginal or cesarean section [C-section]) has a strong influence on shaping the initial gut microbiota composition. It has been hypothesized that infants born by C-section acquire different bacterial communities compared to vaginally delivered infants (64), which may influence the short- and long-term immune responses to environmental factors, thereby predisposing to autoimmunity (65). Also, the type of C-section, emergency vs. elective, has been hypothesized as a different possible influencing factor, since the cord blood immune cell phenotypes are affected by stress during vaginal delivery and this does not happen by elective C-section (66). In addition, infants born vaginally and during emergency C-section are colonized at first by fecal and vaginal bacteria of the mother, whereas infants born through elective cesarean delivery are exposed initially to bacteria originating from the hospital environment and healthcare workers. Infants born by cesarean delivery are characterized by a more slowly diversifying microbiota, with a substantial absence of Bifidobacteria species and Bacteroides and the presence of facultative anaerobes, such as Clostridium species. These differences might influence the development of the mucosal immune system, the establishment of a stable intestinal host-microbial homeostasis, as well as the mucosal barrier function and ultimately contribute to the risk of acquiring immune-mediated diseases, such as CD, later in life (67).
Some studies have identified C-section as a risk factor for the development of CD (68, 69). However, more recent prospective studies have found no association (70–73) (Table 7). Recently, a large, observational, register-based, cohort study investigated the association between the type of delivery and the risk of developing CD in two independent population cohorts (Denmark, birth cohort 1995–2010 and Norway, birth cohort 2004–2012) (74). A total of 3,314 children were diagnosed with CD. C-sections were performed in 286,640 children, and the mode of delivery was not associated with an increased risk of diagnosed CD.
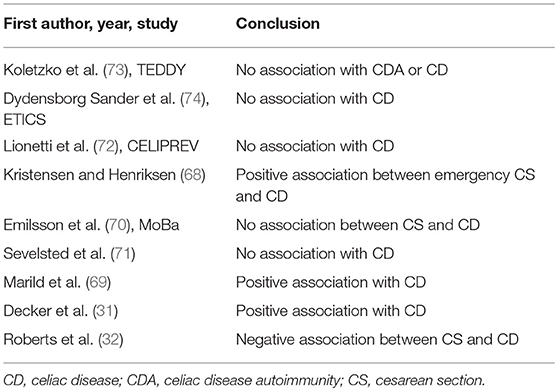
Table 7. Some of the most relevant studies on type of delivery and the risk for celiac disease.
In the above-mentioned Danish cohort, the association between elective C-section and diagnosed CD was positive and reached borderline statistical significance after adjusting for year of birth, sex, maternal age, education, parity, gestational age, and weight for gestational age (OR: 1.20; 95% CI: 1.00–1.43). However, this finding was not replicated in the corresponding Norwegian cohort (OR: 0.96; 95% CI: 0.79–1.17) (74). Analysis of the data from the Swedish Medical Birth Register between 1973 and 2008, comparing cases with villous atrophy with age- and sex-matched controls from the general population, found a weak association between an elective C-section and CD in offspring (adjusted odds ratio [OR] = 1.15), but no increased risk for CD diagnoses after an emergency (adjusted OR = 1.02) or any C-section (adjusted OR = 1.06) (69). Data from a population- and national register-based cohort including all children born in Denmark from January 1997 to December 2012 showed the opposite: children delivered by emergency C-section were at an increased risk for CD (adjusted OR = 1.22), whereas children delivered by elective C-section were not (adjusted OR = 0.69) (68). Thus, despite the plausible hypothesis that mode of delivery affects risk of CD, the current literature showed no association between the type of delivery and the risk of CD (Table 7).
Antibiotics
The ETIC study found no evidence of increased CD risk with antibiotic use in the first 6 months of life (61). However, other 2 retrospective studies have shown a positive association between antibiotic use and CD risk (75, 76). A recent analysis of the TEDDY study showed that cumulative exposure to β-lactam or macrolide antibiotics, up to 6 months, during the first or second year of life and within 6 months before the seroconversion period, was not associated with CDA. Also, maternal use of antibiotics during pregnancy was also evaluated as a risk factor and did not significantly contribute to CDA risk in this study. In conclusion, the role of antibiotics in the development of CD is a topic that remains unclear and requires more research.
Microbiota
CD development has also been linked to alterations in the human gut microbiome, which is necessary for proper development of the immune system and establishment of oral tolerance in early life (65). The contributing role of perturbations in the gut microbiota, and of specific enteric bacteria, to gluten-induced immunopathology has been shown in animal models (77). PROFICEL, a prospective study of 164 healthy Spanish newborns with a first-degree relative with CD and HLA-DQ2 and/or DQ8 positivity, reported an association between the HLA-DQ genotype and the intestinal microbiota composition. In this study, the HLA-DQ2/8 genotype and the type of feeding (breastfeeding or formula) were shown to influence, in conjunction, the composition of the intestinal microbiota (78). The high-risk genotype for developing CD (HLA-DQ2, including homozygous HLA-DQ2.5 or heterozygous DQ2.5/DQ2.2 and DQ2.2/DQ7.5) was associated with reduced numbers of Bifidobacterium, specifically of the species B. Longum, compared to the rest of the lower-risk genotypes (79). Also, other studies have found similar results; the duodenal and fecal microbiota of CD patients is unbalanced, with decreased numbers of anti-inflammatory bacteria, such as Bifidobacterium spp. and increased numbers of Bacteroides spp., which are only partially normalized after a long-term gluten free diet (GFD) (80–82). In a double-blind, randomized, placebo-controlled, interventional trial performed in children with newly diagnosed CD, children were randomized to receive Bifidobacterium longum or placebo in conjunction with a GFD (83). A decrease in both the numbers of the Bacteroides fragilis group and the fecal secretory IgA concentration was found, which might further confirm the role of microbiota in the pathogenesis of CD. But, so far, studies have failed to find a distinct microbiota profile in patients with CD.
A sub-study of the PROFICEL project, including 10 CD cases and 10 matched controls, suggests altered early proportions of Firmicutes and members of the Actinobacteria phylum (B. Longum) in children who later progressed to CD (84). Hopefully, the results of the Celiac Disease Genomic, Environmental, Microbiome, and Metabolomic (CDGEMM) study, a multicenter, longitudinal study of infants at risk for CD, will provide an answer to the question regarding the role of the gut microbiome and the risk of CD (85). CDGEMM aims to enroll 500 infants aged 0–6 months with a first-degree family member with CD. Health status, anthropometrics, nutritional information, household and environmental information, and blood and stool samples are being collected regularly to understand the role of the gut microbiome as an additional factor that may play a key role in early steps involved in the development of autoimmune disease (85).
In conclusion, in the field of primary prevention, infant feeding practices have been explored by interventional studies with long-term follow up, but have shown no protection for risk of CD. Other possible influences on the development of CD, especially the role of infections and the gut microbiome, need further research.
Text box
Secondary Prevention
Case Finding
Secondary prevention focuses on early detection and treatment (Table 8). Active case finding refers to the liberal diagnostic testing of subjects with CD-associated symptoms. In the general population, this approach has led to the early diagnosis of many patients, resulting in significant health improvement after treatment, good compliance with the GFD, and good CD-related quality of life (86, 87); unfortunately, however, it does not counter the entire under-diagnosis of CD (88, 89). Only a small proportion of the undiagnosed patients are detected with this strategy, since ~50% of the children in screening-detected studies have symptoms at the time of diagnosis (15, 16, 90).
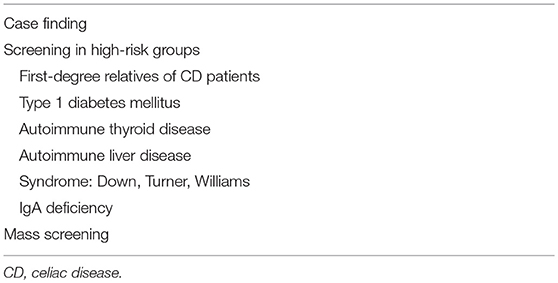
Table 8. Secondary prevention strategies for celiac disease.
Screening for Celiac Disease in High-Risk Groups
Because of the high prevalence of CD among these groups, evidence-based guidelines recommend screening for early detection of the disease (7) (Table 8). A plethora of studies are available on 2 of the populations who belong to these high-risk groups, namely first-degree relative of patients with CD and children with type 1 diabetes mellitus (T1DM).
First-Degree Relatives of CD Patients
Many studies have demonstrated that first-degree relatives (FDRs) of celiac patients have a higher risk of developing CD than the general population, with a prevalence ranging from 1.6 to 38% (91). Based on a systematic review and meta-analysis, Sing et al. (91) reported that the pooled prevalence of CD was 7.5% in 10,252 FDRs (91). The risk of developing CD among FDRs is influenced by gender and HLA haplotype (15, 16). CD occurs more often in girls (female: male ratio of 2–3:1), and HLA-DQ2 homozygous children have a significantly higher risk of developing CD than HLADQ2 heterozygous children (14.9 vs. 3.9%, respectively, at the age of 3 years) (15).
Children with Conditions/Diseases Associated with CD
The prevalence of CD in patients with T1DM has been reported by most studies as ranging between 4 and 10% (92). Many children with T1DM and CD are asymptomatic or at least symptoms of CD have not been observed. In these cases, CD may only be detected by serologic screening. However, it has been shown that strict adherence to a GFD was < 30% in children with both CD and T1DM, compared to 81% among patients with CD only (93). Maintaining a strict GFD in addition to a diabetic diet requires additional time, effort, and expense. Evidence is inconclusive as to whether the benefits of screening and potentially treating asymptomatic individuals outweigh the harms of managing a population already burdened with a serious illness. The Celiac Disease and Diabetes-Dietary Intervention and Evaluation Trial (CD-DIET) (ClinicalTrials.gov Identifier: NCT01566110) involves screening of children and adults with T1DM for asymptomatic CD, followed by randomization to a GFD or no-GFD group, to assess outcomes (including diabetes control, bone mineral density, and health-related quality of life) over 1 year to clarify effects of screening and treating asymptomatic CD in this population with a GFD (94).
Mass Screening
Screening the general population, also called mass screening, would theoretically be the best form of secondary prevention since it could potentially detect all cases of CD, including those in asymptomatic patients as well as those in patients who lack symptoms. Results from most screening studies performed in the general population suggest that symptoms are not reliable predictors of CD (15, 95, 96), reinforcing the place of mass screening as the best strategy for secondary prevention of CD enabling early treatment to reduce the burden of morbidity and mortality associated with untreated CD (97, 98).
However, mass screening for CD is still debated, partly because evidence has been lacking on the accuracy of diagnostic tests and on the health benefits after diagnosis and treatment of asymptomatic detected patients. This uncertainty also affects the cost benefit of mass screening, which is needed for implementation of mass screening for CD (99, 100). Most studies on the diagnostic accuracy of diagnostic tests for CD have been conducted in symptomatic patients (101, 102). Because the positive predictive value declines when the test is used in settings with a low pre-test prevalence, such as the general population, the sensitivity and specificity of these tests are lower in the setting of mass screening.
Recently, a prospective study performed in Rotterdam has shown a positive predictive value of 81% for CD in the general pediatric population (96). These authors also showed that undiagnosed CD is associated with a lower body mass index compared to controls at the age of 9 years (96) and associated with fetal growth restriction and lower birth and placental weight during pregnancy (8). Additional information about the importance and effectiveness of screening comes from a population-based-screening study performed in Sweden; this study showed that at 10 years of age, children with CD detected by screening already had reduced bone mineral density in the total body and spine compared with age-matched controls. These differences were not found in children with CD on a GFD from 3 years of age, indicating that children with screening-detected CD benefit from early diagnosis and treatment (103).
The data on the benefits and harms of screening are limited. Only one randomized trial evaluated the effectiveness of GFD vs. no GFD in apparently asymptomatic adults with screen-detected CD and found that initiation of a GFD in screen-detected adults with unrecognized symptoms was associated with improved gastrointestinal symptoms (104).
Other traditional reason against mass screening are that adherence to the GFD in minimally or asymptomatic patients would be lower than in symptomatic patients and that the quality of life is decreased in screening-detected CD patients following a GFD. However, 10 years of follow up among Dutch children and the results of a sub-study from the ETICS project showed similar adherence rates to the GFD in screening-detected children compared with clinically detected children (105, 106). No significant differences in health-related quality of life (HRQoL) were observed between screening-detected and symptom-detected adult patients (107, 108). Furthermore, a systematic review and meta-analysis on dietary adherence and HRQoL in adult patients with CD detected by screening showed a significantly lower HRQoL after 1 year of treatment with a GFD in symptom-detected patients compared to screening-detected patients (109). Despite the aforementioned literature that is positive about screening of the general population, the current literature recommending mass screening is limited.
Tertiary Prevention
Gluten-Free Diet (GFD)
Tertiary prevention focuses on reducing the impact of existing disease by improved treatment (Table 9). One of these strategies involves optimizing adherence to the GFD. Complete removal of gluten from the diet is a challenge, as gluten is present in a wide variety of foods. However, since the introduction of allergen labeling in the European Union (EU) in 2005, gluten cannot be hidden in products. The amount of gluten capable of initiating an antigenic reaction has been estimated to be >20 mg/kg (or parts per million = ppm) of gluten, and contamination below 20 ppm is considered safe over a wide range of foods in daily consumption.
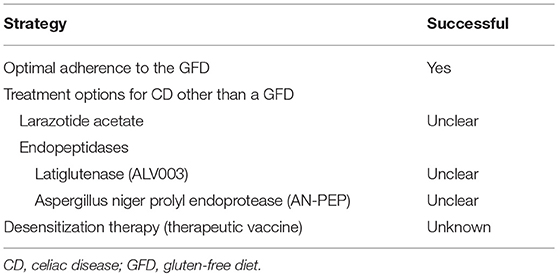
Table 9. Tertiary prevention strategies for celiac disease.
Improving Monitoring of and Adherence to the GFD
Dietitian
Due to the complexity of the GFD, it is essential that newly diagnosed patients be referred to a dietitian with expertise in CD. A delay in referral, or no referral at all, increases the likelihood of the patient obtaining inaccurate information from the Internet, health food stores, alternative health practitioners, family, friends, and other sources, often resulting in confusion, frustration, and insufficient knowledge regarding CD and the GFD (110).
Gluten-containing cereals, such as wheat, barley, and rye, are important sources of dietary iron, calcium, folate, and vitamin B12. As the treatment of CD with a GFD can lead to nutritional deficiencies, the support of a dietitian is necessary to avoid these deficiencies. Also, consultation with someone with knowledge in the field of replacement (gluten-free) products, such as amaranth, buckwheat, quinoa, sorghum and teff, is of great importance and could improve intakes of protein, iron, calcium, and fiber by patients with CD (111).
Validated Food Questionnaires
A dietary interview to assess compliance with the GFD is the best way to detect errors in GFD adherences among children and young adults, but it is timue-consuming (20–30 min per patient) and requires expert personnel. Several short questionnaires have been developed to measure GFD adherence in order to save time, and while some are not sensitive enough, others are useful in assessing compliance to the diet (112). With the increasing use of self-assessment and alternative follow-up methods for CD patients, including electronic patient records and E-health tolls, completing questionnaires before or during a medical consultation should be easily implemented in the healthcare of children and young adults with CD (113).
Measurement of Gluten Immunogenic Peptides (GIPs)
Available methods to assess GFD compliance are time-consuming and are also insufficiently sensitive to detect occasional dietary transgressions that may cause gut mucosal damage. Determination of serum TG2A is usually used during the follow-up of a patient on a GFD, as this marker improves with gluten elimination (114). However, it has been reported that even while following a GFD, children and women with CD have a much higher prevalence of gastrointestinal symptoms than controls, and they also use healthcare services more often (115). As mucosal damage may still persist without TG2A, antibody testing may be negative in patients with only partial adherence to the GFD (116). Therefore, it is necessary to have a non-invasive biomarker to monitor compliance with the GFD. Certain GIPs are resistant to gastrointestinal digestion and can interact with the immune system of patients with CD to trigger an autoimmune response against transglutaminase and other antigens. A proportional fraction of the GIPs absorbed in the gastrointestinal tract make it to the circulation and are excreted in urine. GIPs are detectable in concentrated urines and may be useful in clinical practice as a monitoring tool to follow-up compliance with the GFD. GIPs are detected in urine samples 6–48 h after gluten intake (>25 mg) and remained detectable for 1–2 days (117).
Treatment Options for CD Other Than the GFD
Several other treatments aimed at different pathogenic targets of CD have been studied in recent years: modification of gluten to produce non-immunogenic gluten, endoluminal therapies to degrade gluten in the intestinal lumen, increasing gluten tolerance, modulation of intestinal permeability, and regulation of the adaptive immune response. However, not all of these therapies have been tested in clinical trials (yet). The most advanced studies are devoted to larazotide acetate and prolyl-endopeptidases degrading toxic gluten peptides and to therapeutic vaccination.
Larazotide Acetate
Patients with active CD have increased intestinal permeability. Zonulin, a modulator of epithelial tight junctions, is overexpressed in these patients. Release of zonulin in response to binding between gliadin peptides and a specific chemokine receptor (CXCR3) results in a measurable reduction in the usual intestinal barrier and allows enhanced passage of gliadin. This mechanism has been the target of advanced research that led to the development of larazotide acetate (AT-1001), an octapeptide that inhibits gliadin-induced intestinal permeability. Several phase I and II clinical trials have confirmed the safety of this agent and suggest a potential beneficial effect of larazotide (118, 119). Additionally, patients who were treated with larazotide acetate had significantly fewer symptoms (patient reported Celiac Disease Gastrointestinal System Rating Score) compared with those taking a placebo (120–122). A dose-response effect was not seen, with the most benefit encountered at the lowest (0.5 mg) of 4 dosages administered (121); however, this study did not measure histologic endpoints, and larazotide had no significant effect on serologic levels of specific CD antibodies as TG2A.
Endopeptidases
The gluten peptides, which are responsible for inducing the immunological response in CD patients, are rich in proline and are highly resistant to enzymatic proteolysis within the digestive tract. For many years, there have been studies conducted to investigate the effectiveness of orally administered prolyl oligo-peptidases in the degradation of toxic gliadin peptides before they reach the mucosa of the small intestine.
Latiglutenase (ALV003, Alvine Pharmaceuticals, San Carlos, CA, USA) is an orally administered mixture of 2 recombinant gluten-specific proteases—a cysteine protease (EP-B2) and a prolyl endopeptidase (PEP)—which have been shown in vitro to degrade gluten (123). Both endopeptidases are active and stable at gastric pH (124). In a Phase 2 study with ALV003, adults with biopsy-proven CD were randomly assigned to groups receiving ALV003 or placebo, together with a daily 2 g gluten challenge. Upper endoscopy was performed at baseline and after the gluten challenge. Primary endpoint included the villus height to crypt depth ratio and CD3+ intra-epithelial lymphocytes (IEL) density. Serologic markers and symptoms were also assessed. In the ALV003 group, there were no changes in histological measures, while in the placebo group, evidence of mucosal injury was shown after gluten challenge. In contrast, no differences were seen in symptoms and serologic markers of CD in both groups. In a phase 2 study involving patients with symptomatic CD and histologic evidence of significant duodenal mucosal injury, ALV003 did not improve histologic and symptom scores when compared with placebo (125). However, a subgroup-analysis of the study showed a statistically significant, dose-dependent reduction in the severity and frequency of symptoms in seropositive but not in seronegative patients (126).
Aspergillus niger prolyl endoprotease (AN-PEP; DSM, Heerlen, The Netherlands) is also an endopeptidase, isolated from the fungus Aspergillus niger. The enzyme is active between a pH of 2 and 8, with an optimum activity at pH 4–5, thus, in the stomach and small intestine (127). In a randomized, placebo-controlled, crossover study, 18 self-reported gluten-sensitive subjects consumed a porridge containing 0.5 g gluten together with two tablets containing either a high or low dose of AN-PEP or placebo. Gastric and duodenal contents were sampled over 180 min. The primary outcome was defined as the efficacy of the high dose of AN-PEP compared with placebo in degrading at least 50% of gluten, based on the amount of gluten detected in the duodenum. The researchers concluded that the AN-PEP enzyme is effective in degrading small amounts of gluten as part of a complex meal in the stomach, but it is not intended to replace a GFD in patients with gluten-related disease (128). In a Phase 2a double-blinded, placebo-controlled, randomized trial, 16 CD patients on a GFD, who were in serological and histopathological clinical remission, were administered AN-PEP or a placebo with gluten-containing toast (~7 g/day gluten). The mean score for the gastrointestinal subcategory of the CD quality (CDQ) was relatively high throughout the study, indicating that AN-PEP was well-tolerated. In the efficacy phase, the CDQ scores of patients consuming gluten with placebo or gluten with AN-PEP did not significantly deteriorate and, moreover, no differences between the groups were observed.
Larazotide and PEPs will not become an alternative to the GFD and their potential role as therapeutic agents for CD remain unclear.
Desensitization Therapy (Therapeutic Vaccine)
NexVax2 from ImmusanT is a desensitizing vaccine that uses three dominant gluten peptides administered subcutaneously to induce an immune response in CD patients who carry the immune recognition gene HLA-DQ2.5, which accounts for disease in 80–90% of patients. The aim of the vaccine is to use peptide-based immunotherapy to shift the T-cell response from pro-inflammatory to regulatory, in order to restore immune tolerance to gluten. Phase 1b clinical trials of this vaccine have recently been completed supporting the safety, tolerability and relevant bioactivity of Nexvax2 (129).
Conclusions
• Celiac disease is a common autoimmune disorder induced by ingestion of gluten in genetically susceptible individuals.
• Only a minority of those who are at genetic risk develop the disease.
• The incidence of CD has increased over the last half-century, resulting in rising interest in identifying risk factors for CD to enable prevention.
• Environmental and/or lifestyle factors play a causal role in the development of CD.
• For primary prevention (i.e., interventions before CD occurs), early feeding practices seem to have no impact on the risk of developing CD during childhood. Other environmental influences have been investigated as potential risk factors; however, they have not yet led to primary prevention strategies.
• Secondary prevention is possible through early diagnosis and treatment; however, it will not identify all CD patients as long as mass screening has not been introduced.
• As a gluten-free diet is a major challenge, tertiary prevention strategies are under evaluation; however, none of these measures are currently recommended as treatment.
Author Contributions
CM: Corresponding author, primary responsibility for communication with the journal during the manuscript submission, drafting the work, final approval of the version to be published, agreement to be accountable for all aspects of the work. RS: Critical revision of the article, final approval of the version to be published, agreement to be accountable for all aspects of the work. HS: Critical revision of the article, final approval of the version to be published, agreement to be accountable for all aspects of the work. LM: Drafting the work, supervising corresponding author, final approval of the version to be published, agreement to be accountable for all aspects of the work.
Conflict of Interest Statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
References
1. Ludvigsson JF, Rubio-Tapia A, Van Dyke CT, Melton LJ III, Zinsmeister AR, Lahr BD, et al. Increasing incidence of celiac disease in a North American population. Am J Gastroenterol. (2013) 108:818–24. doi: 10.1038/ajg.2013.60
2. Lohi S, Mustalahti K, Kaukinen K, Laurila K, Collin P, Rissanen H, et al. Increasing prevalence of coeliac disease over time. Aliment Pharmacol Ther. (2007) 26:1217–25. doi: 10.1111/j.1365-2036.2007.03502.x
3. Vavricka SR, Vadasz N, Stotz M, Lehmann R, Studerus D, Greuter T, et al. Celiac disease diagnosis still significantly delayed—doctor's but not patients' delay responsive for the increased total delay in women. Dig Liver Dis. (2016) 48:1148–54. doi: 10.1016/j.dld.2016.06.016
4. Csizmadia CGDA, Mearin ML, von Blomberg BM, Brand R, Verloove-Vanhorick SP. An iceberg of childhood coeliac disease in the Netherlands. Lancet (1999) 353:813–4. doi: 10.1016/S0140-6736(99)00243-3
5. Fasano A, Catassi C. Current approaches to diagnosis and treatment of coeliac disease: am involving spectrum. Gastroenterology (2001) 120:636–51. doi: 10.1053/gast.2001.22123
6. Mearin ML. Celiac disease among children and adolescents. Curr Probl Pediatr Adolesc Health Care (2007) 37:86–105. doi: 10.1016/j.cppeds.2007.01.001
7. Husby S, Koletzko S, Korponay-Szabó IR, Mearin ML, Phillips A, Shamir R, et al. European Society for Pediatric Gastroenterology, Hepatology, and Nutrition guidelines for the diagnosis of coeliac disease. J Pediatr Gastroenterol Nutr. (2012) 54:136–60. doi: 10.1097/MPG.0b013e31821a23d0
8. Kiefte-de Jong JC, Jaddoe VW, Uitterlinden AG, Steegers EA, Willemsen SP, Hofman A, et al. Levels of antibodies against tissue transglutaminase during pregnancy are associated with reduced fetal weight and birth weight. Gastroenterology (2013) 144:726–35. doi: 10.1053/j.gastro.2013.01.003
9. Green PHR, Jabri B. Coeliac disease. Lancet (2003) 362:383–91. doi: 10.1016/S0140-6736(03)14027-5
10. Mearin ML. The prevention of coeliac disease. Best Pract Res Clin Gastroenterol. (2015) 29:493–501. doi: 10.1016/j.bpg.2015.04.003
11. Maars van der PJ, Mackenbach JP. Volksgezondheid en Gezondheidszorg. Elsevier; Bunge (1999). Tweede druk [Dutch].
12. Hopman EG, le Cessie S, von Blomberg BM, Mearin ML. Nutritional management of the gluten-free diet in young people with celiac disease in The Netherlands. J Pediatr Gastroenterol Nutr. (2006) 43:102–8. doi: 10.1097/01.mpg.0000228102.89454.eb
13. Ohlund K, Olsson C, Hernell O, Ohlund I. Dietary shortcomings in children on a gluten-free diet. J Hum Nutr Diet. (2010) 23:294–300. doi: 10.1111/j.1365-277X.2010.01060.x
14. Ivarsson A, Persson LA, Nyström L, Ascher H, Cavell B, Danielsson L, et al. Epidemic of coeliac disease in Swedish children. Acta Paediatr. (2000) 89:165–71. doi: 10.1111/j.1651-2227.2000.tb01210.x
15. Vriezinga SL, Auricchio R, Bravi E, Castillejo G, Chmielewska A, Crespo Escobar P, et al. Randomized feeding intervention in infants at high risk for celiac disease. N Engl J Med. (2014) 371:1304–15. doi: 10.1056/NEJMoa1404172
16. Lionetti E, Castellaneta S, Francavilla R, Pulvirenti A, Tonutti E, Amarri S, et al. Introduction of gluten, HLA status, and the risk of celiac disease in children. N Engl J Med. (2014) 371:1295–303. doi: 10.1056/NEJMoa1400697
17. Sellitto M, Bai G, Serena G, Fricke WF, Sturgeon C, Gajer P, et al. (2012). Proof of concept of microbiome-metabolome analysis and delayed gluten exposure on celiac disease autoimmunity in genetically at-risk infants. PLoS ONE 7:e33387. doi: 10.1371/journal.pone.0033387
18. Hummel S, Pflüger M, Hummel M, Bonifacio E, Ziegler AG. Primary dietary intervention study to reduce the risk of islet autoimmunity in children at increased risk for type 1 diabetes: the BABYDIET study. Diabetes Care (2011) 34:1301–5. doi: 10.2337/dc10-2456
19. Beyerlein A, Chmiel R, Hummel S, Winkler C, Bonifacio E, Ziegler AG. Timing of gluten introduction and islet autoimmunity in young children: updated results from the BABYDIET study. Diabetes Care (2014) 37:e194–5. doi: 10.2337/dc14-1208
20. Andrén Aronsson CA, Lee HS, Liu E, Uusitalo U, Hummel S, Yang J, et al. Age at gluten introduction and risk of celiac disease. Pediatrics (2015) 135:239–45. doi: 10.1542/peds.2014-1787
21. Jansen MA, Tromp II, Kiefte-de Jong JC, Jaddoe VW, Hofman A, Escher JC, et al. Infant feeding and anti-tissue transglutaminase antibody concentrations in the Generation R Study. Am J Clin Nutr. (2014) 100:1095–101. doi: 10.3945/ajcn.114.090316
22. Størdal K, White RA, Eggesbo M. Early feeding and risk of celiac disease in a prospective birth cohort. Pediatric (2013) 132:1202–9. doi: 10.1542/peds.2013-1752
23. Welander A, Tjernberg AR, Montgomery SM, Ludvigsson J, Ludvigsson JF. Infectious disease and risk of later celiac disease in childhood. Pediatrics (2010) 125:e530–e536. doi: 10.1542/peds.2009-1200
24. Norris JM, Barriga K, Hoffenberg EJ, Taki I, Miao D, Haas JE, et al. Risk of celiac disease autoimmunity and timing of gluten introduction in the diet of infants at increased risk of disease. JAMA (2005) 293:2343–51. doi: 10.1001/jama.293.19.2343
25. Ziegler AG, Schmid S, Huber D, Hummel M, Bonifacio E, et al. Early infant feeding and risk of developing type 1 diabetes-associated autoantibodies. JAMA (2003) 290:1721–8. doi: 10.1001/jama.290.13.1721
26. Hummel S, Hummel M, Banholzer J, Hanak D, Mollenhauer U, Bonifacio E, et al. Development of autoimmunity to transglutaminase C in children of patients with type 1 diabetes: relationship to islet autoantibodies and infant feeding. Diabetologia (2007) 50:390–4. doi: 10.1007/s00125-006-0546-3
27. Ivarsson A, Hernell O, Stenlund H, Persson LA. Breast-feeding protects against celiac disease. Am J Clin Nutr. (2002) 75:914–21. doi: 10.1093/ajcn/75.5.914
28. Peters U, Schneeweiss S, Trautwein EA, Erbersdobler HF. A case-control study of the effect of infant feeding on celiac disease. Ann Nutr Metab. (2001) 45:135–42. doi: 10.1159/000046720
29. Falth-Magnusson K, Franzen L, Jansson G, Laurin P, Stenhammar L. Infant feeding history shows distinct differences between Swedish celiac and reference children. Pediatr Allergy Immunol. (1996) 7:1–5. doi: 10.1111/j.1399-3038.1996.tb00098.x
30. Ivarsson A, Myléus A, Norström F, van der Pals M, Rosén A, Högberg L, et al. Prevalence of childhood celiac disease and changes in infant feeding. Pediatrics (2013) 131:e687–94. doi: 10.1542/peds.2012-1015
31. Decker E, Engelmann G, Findeisen A, Gerner P, Laass M, Ney D, et al. Cesarean delivery is associated with celiac disease but not inflammatory bowel disease in children. Pediatrics (2010) 125:e1433–40. doi: 10.1542/peds.2009-2260
32. Roberts SE, Williams JG, Meddings D, Davidson R, Goldacre MJ. Perinatal risk factors and coeliac disease in children and young adults: a record linkage study. Aliment Pharmacol Ther. (2009) 29:222–31. doi: 10.1111/j.1365-2036.2008.03871.x
33. Greco L, Auricchio S, Mayer M, Grimaldi M. Case control study on nutritional risk factors in celiac disease. J Pediatr Gastroenterol Nutr. (1988) 7:395–9. doi: 10.1097/00005176-198805000-00013
34. Ascher H, Krantz I, Rydberg L, Nordin P, Kristiansson B. Influence of infant feeding and gluten intake on coeliac disease. Arch Dis Child. (1997) 76:113–7. doi: 10.1136/adc.76.2.113
35. Auricchio S, Follo D, de Ritis G, Giunta A, Marzorati D, Prampolini L, et al. Does breast feeding protect against the development of clinical symptoms of celiac disease in children? J Pediatr Gastroenterol Nutr. (1983) 2:428–33. doi: 10.1097/00005176-198302030-00006
36. Andrén Aronsson C, Lee HS, Koletzko S, Uusitalo U, Yang J, Virtanen SM, et al. TEDDY Study Group. Effects of gluten intake on risk of celiac disease: a case-control study on a Swedish Birth Cohort. Clin Gastroenterol Hepatol. (2016) 14:403–9. doi: 10.1016/j.cgh.2015.09.030
37. Akobeng AK, Ramanan AV, Buchan I, Heller RF. Effect of breast feeding on risk of coeliac disease: a systematic review and meta-analysis of observational studies. Arch Dis Child. (2006) 91:39–43. doi: 10.1136/adc.2005.082016
38. Szajewska H, Shamir R, Chmielewska A, Pieścik-Lech M, Auricchio R, Ivarsson A, et al. PREVENTCD Study Group. Systematic review with meta-analysis: early infant feeding and coeliac disease–update 2015. Aliment Pharmacol Ther. (2015) 41:1038–54. doi: 10.1111/apt.13163
39. Silano M, Agostoni C, Sanz Y, Guandalini S. Infant feeding and risk of developing celiac disease: a systematic review. BMJ Open (2016) 6:e009163. doi: 10.1136/bmjopen-2015-009163
40. Crespo-Escobar P, Mearin ML, Hervás D, Auricchio R, Castillejo G, Gyimesi J, et al. The role of gluten consumption at an early age in celiac disease development: a further analysis of the prospective PreventCD cohort study. Am J Clin Nutr. (2017) 105:890–6. doi: 10.3945/ajcn.116.144352
41. Stene LC, Honeyman MC, Hoffenberg EJ, Haas JE, Sokol RJ, Emery L, et al. Rotavirus infection frequency and risk of celiac disease autoimmunity in early childhood: a longitudinal study. Am J Gastroenterol. (2006) 101:2333–40. doi: 10.1111/j.1572-0241.2006.00741.x
42. Thevenot T, Denis J, Jouannaud V, Monnet E, Renou C, Labadie H, et al. Coeliac disease in chronic hepatitis C: a French multicentre prospective study. Aliment Pharmacol Ther. (2007) 26:1209–16. doi: 10.1111/j.1365-2036.2007.03499.x
43. Gravina AG, Federico A, Masarone M, Cuomo A, Tuccillo C, Loguercio C, et al. Coeliac disease and C virus-related chronic hepatitis: a non association. BMC Res Notes (2012) 5:533. doi: 10.1186/1756-0500-5-533
44. Jansen MA, van den Heuvel D, van der Zwet KV, Jaddoe VW, Hofman A, Escher JC, et al. Herpesvirus infections and transglutaminase type 2 antibody positivity in childhood: the Generation R Study. J Pediatr Gastroenterol Nutr. (2016) 63:423–30. doi: 10.1097/MPG.0000000000001163
45. Kårhus LL, Gunnes N, Størdal K, Bakken IJ, Tapia G, Stene LC, et al. Influenza and risk of later celiac disease: a cohort study of 2.6 million people. Scand J Gastroenterol. (2018) 53:15–23. doi: 10.1080/00365521.2017.1362464
46. Dore MP, Salis R, Loria MF, Villanacci V, Bassotti G, Pes GM. Helicobacter pylori infection and occurrence of celiac disease in subjects HLA-DQ2/DQ8 positive: a prospective study. Helicobacter (2018) 23:e12465. doi: 10.1111/hel.12465
47. Lähdeaho ML, Parkkonen P, Reunala T, Mäki M, Lehtinen M. Antibodies to E1b protein-derived peptides of enteric adenovirus type 40 are associated with celiac disease and dermatitis herpetiformis. Clin Immunol Immunopathol. (1993) 69:300–5. doi: 10.1006/clin.1993.1184
48. Vesy CJ, Greenson JK, Papp AC, Snyder PJ, Qualman SJ, Prior TW. Evaluation of celiac disease biopsies for adenovirus 12 DNA using a multiplex polymerase chain reaction. Mod Pathol. (1993) 6:61–4.
49. Kagnoff MF, Paterson YJ, Kumar PJ, Kasarda DD, Carbone FR, Unsworth DJ, et al. Evidence for the role of a human intestinal adenovirus in the pathogenesis of coeliac disease. Gut. (1987) 28:995–1001. doi: 10.1136/gut.28.8.995
50. Mahon J, Blair GE, Wood GM, Scott BB, Losowsky MS, Howdle PD. Is persistent adenovirus 12 infection involved in coeliac disease? A search for viral DNA using the polymerase chain reaction. Gut (1991) 32:1114–6. doi: 10.1136/gut.32.10.1114
51. Fine KD, Ogunji F, Saloum Y, Beharry S, Crippin J, Weinstein J. Celiac sprue: another autoimmune syndrome associated with hepatitis C. Am J Gastroenterol. (2001) 96:138–45. doi: 10.1111/j.1572-0241.2001.03464.x
52. Carlsson AK, Lindberg BA, Bredberg AC, Hyöty H, Ivarsson SA. Enterovirus infection during pregnancy is not a risk factor for celiac disease in the offspring. J Pediatr Gastroenterol Nutr. (2002) 35:649–52. doi: 10.1097/00005176-200211000-00011
53. Villalta D, Girolami D, Bidoli E, Bizzaro N, Tampoia M, Liguori M, et al. High prevalence of celiac disease in autoimmune hepatitis detected by anti-tissue tranglutaminase autoantibodies. J Clin Lab Anal. (2005) 19:6–10. doi: 10.1002/jcla.20047
54. Ruggeri C, La Masa AT, Rudi S, Squadrito G, Di Pasquale G, Maimone S, et al. Celiac disease and non-organ-specific autoantibodies in patients with chronic hepatitis C virus infection. Dig Dis Sci. (2008) 53:2151–5. doi: 10.1007/s10620-007-0146-1
55. Sarmiento L, Galvan JA, Cabrera-Rode E, Aira L, Correa C, Sariego S, et al. Type 1 diabetes associated and tissue transglutaminase autoantibodies in patients without type 1 diabetes and coeliac disease with confirmed viral infections. J Med Virol. (2012) 84:1049–53. doi: 10.1002/jmv.23305
56. Tjernberg AR, Ludvigsson JF. Children with celiac disease are more likely to have attended hospital for prior respiratory syncytial virus infection. Dig Dis Sci. (2014) 59:1502–8. doi: 10.1007/s10620-014-3046-1
57. Abid SG, Aboud RS, Fadil HY, Aboud AS. Relationship between chronic hepatitis B virus and pathogenicity of celiac disease in the Iraqi patients. J Pharm Chem Biol Sci. (2016) 3:578–83.
58. Tarish HR, Hameed WS, Abdul-Mehdi RJ, Alsherees HAA. Role of previous adenovirus infection and its association with IFN-α in occurrence of celiac disease in Iraqi patients. J Med Sci Clin Res. (2016) 4:10326–30. doi: 10.18535/jmscr/v4i4.58
59. Alaedini A, Lebwohl B, Wormser GP, Green PH, Ludvigsson JF. Borrelia infection and risk of celiac disease. BMC Med. (2017) 15:169. doi: 10.1186/s12916-017-0926-1
60. Bouziat R, Hinterleitner R, Brown JJ, Stencel-Baerenwald JE, Ikizler M, Mayassi T, et al. Reovirus infection triggers inflammatory responses to dietary antigens and development of celiac disease. Science (2017) 356:44–50. doi: 10.1126/science.aah5298
61. Myléus A, Hernell O, Gothefors L, Hammarström ML, Persson LÅ, Stenlund H, et al. Early infections are associated with increased risk for celiac disease: an incident case-referent study. BMC Pediatr. (2012) 12:194. doi: 10.1186/1471-2431-12-194
62. Kemppainen KM, Lynch KF, Liu E, Lönnrot M, Simell V, Briese T, et al. TEDDY Study Group. Factors that increase risk of celiac disease autoimmunity after a gastrointestinal infection in early life. Clin Gastroenterol Hepatol. (2017) 15:694–702. doi: 10.1016/j.cgh.2016.10.033
63. Mårild K, Kahrs CR, Tapia G, Stene LC, Størdal K. Infections and risk of celiac disease in childhood: a prospective nationwide cohort study. Am J Gastroenterol. (2015) 110:1475–84. doi: 10.1038/ajg.2015.287
64. Dominguez-Bello MG, Costello EK, Contreras M, Magris M, Hidalgo G, Fierer N, et al. Delivery mode shapes the acquisition and structure of the initial microbiota across multiple body habitats in newborns. Proc Natl Acad Sci USA. (2010) 107:11971–5. doi: 10.1073/pnas.1002601107
65. McLean MH, Dieguez D Jr, Miller LM, Young HA. Does the microbiota play a role in the pathogenesis of autoimmune diseases? Gut (2015) 64:332–41. doi: 10.1136/gutjnl-2014-308514
66. Thysen AH, Larsen JM, Rasmussen MA, Stokholm J, Bønnelykke K, Bisgaard H, et al. Prelabor cesarean section bypasses natural immune cell maturation. J Allergy Clin Immunol. (2015) 136:1123–5. doi: 10.1016/j.jaci.2015.04.044
67. Penders J, Thijs C, Vink C, Stelma FF, Snijders B, Kummeling I, et al. Factors influencing the composition of the intestinal microbiota in early infancy. Pediatrics (2006) 118:511–21. doi: 10.1542/peds.2005-2824
68. Kristensen K, Henriksen L. Cesarean section and disease associated with immune function. J Allergy Clin Immunol. (2016) 137:587–90. doi: 10.1016/j.jaci.2015.07.040
69. Mårild K, Stephansson O, Montgomery S, Murray JA, Ludvigsson JF. Pregnancy outcome and risk of celiac disease in offspring: a nationwide case-control study. Gastroenterology (2012) 142:39–45. doi: 10.1053/j.gastro.2011.09.047
70. Emilsson L, Magnus MC, Stordal K. Perinatal risk factors for development of celiac disease in children, based on the prospective Norwegian Mother and Child Cohort Study. Clin Gastroenterol Hepatol. (2015) 13:921–7. doi: 10.1016/j.cgh.2014.10.012
71. Sevelsted A, Stokholm J, Bønnelykke K, Bisgaard H. Cesarean section and chronic immune disorders. Pediatrics (2015) 135:e92–8. doi: 10.1542/peds.2014-0596
72. Lionetti E, Castellaneta S, Francavilla R, Pulvirenti A, Catassi C, SIGENP Working Group of Weaning and CD Risk Mode of delivery and risk of celiac disease: risk of celiac disease and age at gluten introduction cohort study. J Pediatr. (2017) 184:81–6. doi: 10.1016/j.jpeds.2017.01.023
73. Koletzko S, Lee HS, Beyerlein A, Aronsson CA, Hummel M, Liu E, et al. TEDDY Study Group. Cesarean section on the risk of celiac disease in the offspring: the Teddy study. J Pediatr Gastroenterol Nutr. (2018) 66:417–24. doi: 10.1097/MPG.0000000000001682
74. Dydensborg Sander S, Hansen AV, Størdal K, Andersen AN, Husby S. Mode of delivery is not associated with celiac disease. Clin Epidemiol. (2018) 10:323–32. doi: 10.2147/CLEP.S152168
75. Mårild K, Ye W, Lebwohl B, Green PH, Blaser MJ, Card T, et al. Antibiotic exposure and the development of coeliac disease: a nationwide case-control study. BMC Gastroenterol. (2013) 13:109. doi: 10.1186/1471-230X-13-109
76. Canova C, Zabeo V, Pitter G, Romor P, Baldovin T, Zanotti R, et al. Association of maternal education, early infections, and antibiotic use with celiac disease: a population-based birth cohort study in northeastern Italy. Am J Epidemiol. (2014) 180:76–85. doi: 10.1093/aje/kwu101
77. Galipeau HJ, McCarville JL, Huebener S, Litwin O, Meisel M, Jabri B, et al. Intestinal microbiota modulates gluten-induced immunopathology in humanized mice. Am J Pathol. (2015) 185:2969–82. doi: 10.1016/j.ajpath.2015.07.018
78. Olivares M, Neef A, Castillejo G, Palma GD, Varea V, Capilla A, et al. The HLA-DQ2 genotype selects for early intestinal microbiota composition in infants at high risk of developing coeliac disease. Gut. (2015) 64:406–17. doi: 10.1136/gutjnl-2014-306931
79. Palma GD, Capilla A, Nova E, Castillejo G, Varea V, Pozo T, et al. Influence of milk-feeding type and genetic risk of developing coeliac disease on intestinal microbiota of infants: the PROFICEL study. PLoS ONE (2012) 7:e30791. doi: 10.1371/journal.pone.0030791
80. Nadal I, Donat E, Ribes-Koninckx C, Calabuig M, Sanz Y. Imbalance in the composition of the duodenal microbiota of children with coeliac disease. J Med Microbiol. (2007) 56:1669–74. doi: 10.1099/jmm.0.47410-0
81. Collado MC, Donat E, Ribes-Koninckx C, Calabuig M, Sanz Y. Imbalances in faecal and duodenal Bifidobacterium species composition in active and non-active coeliac disease. BMC Microbiol. (2008) 8:232. doi: 10.1186/1471-2180-8-232
82. Sanz Y, De Palma G, Laparra M. Unraveling the ties between celiac disease and intestinal microbiota. Int Rev Immunol. (2011) 30:207–18. doi: 10.3109/08830185.2011.599084
83. Olivares M, Castillejo G, Varea V, Sanz Y. Double- blind, randomised, placebo-controlled intervention trial to evaluate the effects of Bifidobacterium longum CECT 7347 in children with newly diagnosed coeliac disease. Br J Nutr. (2014) 112:30–40. doi: 10.1017/S0007114514000609
84. Olivares M, Walker AW, Capilla A, Benítez-Páez A, Palau F, Parkhill J, et al. Gut microbiota trajectory in early life may predict development of celiac disease. Microbiome (2018) 6:36. doi: 10.1186/s40168-018-0415-6
85. Leonard MM, Camhi S, Huedo-Medina TB, Fasano A. Celiac disease genomic, environmental, microbiome, and metabolomic (CDGEMM) study design: approach to the future of personalized prevention of celiac disease. Nutrients (2015) 7:9325–36. doi: 10.3390/nu7115470
86. Virta LJ, Kaukinen K, Collin P. Incidence and prevalence of diagnosed coeliac disease in Finland: results of effective case finding in adults. Scand J Gastroenterol. (2009) 44:933–8. doi: 10.1080/00365520903030795
87. Catassi C, Kryszak D, Louis-Jacques O, Duerksen DR, Hill I, Crowe SE, et al. Detection of Celiac disease in primary care: a multicenter case-finding study in North America. Am J Gastroenterol. (2007) 102:1454–60. doi: 10.1111/j.1572-0241.2007.01173.x
88. Rosen A. Usefulness of symptoms to screen for celiac disease? Pediatrics (2014) 133. doi: 10.1542/peds.2012-3765
89. Hujoel IA, v Dyke CT, Brantner T, Larson J, King KS, Sharma A, et al. Natural history and clinical detection of undiagnosed coeliac disease in a North American community. Aliment Pharmacol Ther. (2018) 47:1358–66. doi: 10.1111/apt.14625
90. Kivelä L, Kaukinen K, Huhtala H, Lähdeaho ML, Mäki M, Kurppa K. At-risk screened children with celiac disease are comparable in disease severity and dietary adherence to those found because of clinical suspicion: a large cohort study. J Pediatr. (2017) 183:115–21. doi: 10.1016/j.jpeds.2016.12.077
91. Singh P, Arora S, Lal S, Strand TA, Makharia GK. Risk of celiac disease in the first- and second degree relatives of patients with celiac disease: a systematic review and meta-analysis. Am J Gastroenterol. (2015) 110:1539–48. doi: 10.1038/ajg.2015.296
92. Elfström P, Sundström J, Ludvigsson JF. Systematic review with meta-analysis: associations between coeliac disease and type 1 diabetes. Aliment Pharmacol Ther. (2014) 40:1123–32. doi: 10.1111/apt.12973
93. Sud S, Marcon M, Assor E, Palmert MR, Daneman D, Mahmud FH. Celiac disease and pediatric type 1 diabetes: diagnostic and treatment dilemmas. Int J Pediatr Endocrinol. (2010) 2010:161285. doi: 10.1155/2010/161285
94. Mahmud FH, De Melo EN, Noordin K, Assor E, Sahota K, Davies-Shaw J, et al. The celiac disease and diabetes-dietary intervention and evaluation trial (CD-DIET) protocol: a randomised controlled study to evaluate treatment of asymptomatic coeliac disease in type 1 diabetes. BMJ Open (2015) 5:e008097. doi: 10.1136/bmjopen-2015-008097
95. vd Windt DA, Jellema P, Mulder CJ, Kneepkens CM, vd Horst HE. Diagnostic testing for CD among patients with abdominal symptoms: a systematic review. JAMA (2010) 303:1738–46. doi: 10.1001/jama.2010.549
96. Jansen M, Zelm M, Groeneweg M, Jaddoe V, Dik W, Schreurs M, et al. The identification of celiac disease in asymptomatic children: the Generation R Study. J Gastroenterol. (2018) 53:377–86. doi: 10.1007/s00535-017-1354-x
97. Choung RS, Murray JA. The US Preventive Services Task Force recommendation on screening for asymptomatic celiac disease: a dearth of evidence. JAMA (2017) 317:1221–3. doi: 10.1001/jama.2017.1105
98. Crowe SE. Celiac disease. Ann Intern Med. (2011) 154:2–16. doi: 10.7326/0003-4819-154-9-201105030-01005
99. Shamir R, Hernell O, Leshno M. Cost-effectiveness analysis of screening for celiac disease in the adult population. Med Decis Making (2006) 26:282–93. doi: 10.1177/0272989X06289012
100. Hershcovici T, Leshno M, Goldin E, Shamir R, Israeli E. Cost effectiveness of mass screening for coeliac disease is determined by time-delay to diagnosis and quality of life on a gluten-free diet. Aliment Pharmacol Ther. (2010) 31:901–10. doi: 10.1111/j.1365-2036.2010.04242.x
101. Nevoral J, Kotalova R, Hradsky O, Valtrova V, Zarubova K, Lastovicka J, et al. Symptom positivity is essential from omitting biopsy in children with suspected CD according to the new ESPGHAN guidelines. Eur J Pediatr. (2013) 173:497–502. doi: 10.1007/s00431-013-2215-0
102. Mansour AA, Najeeb AA. Coeliac disease in Iraqi type 1 diabetic patients. Arab J Gastroenterol. (2011) 12:103–5. doi: 10.1016/j.ajg.2011.04.007
103. Björck S, Brundin C, Karlsson M, Agardh D. Reduced bone mineral density in children with screening-detected celiac disease. JPGN (2017) 65:526–32. doi: 10.1097/MPG.0000000000001568
104. Kurppa K, Paavola A, Collin P, Sievänen H, Laurila K, Huhtala H, et al. Benefits of a gluten-free diet for asymptomatic patients with serologic markers of celiac disease. Gastroenterology (2014) 147:610–7.e7. doi: 10.1053/j.gastro.2014.05.003
105. van Koppen EJ, Schweizer JJ, Csizmadia CGDS, Krom Y, Hylkema HB, Van Geel AM, et al. Long-term health and quality-of life consequences of mass screening for childhood celiac disease: a 10-year follow-up study. Pediatrics (2009) 123:582–8. doi: 10.1542/peds.2008-2221
106. Webb C, Myleus A, Norstrom F, Hammarroth S, Hogberg L, Lagerqvist C, et al. High adherence to a gluten-free diet in adolescents with screening-detected celiac disease. JPGN (2015) 60:54–9. doi: 10.1097/MPG.0000000000000571
107. Vilppula A, Kaukinen K, Luostarinen L, Krekelä I, Patrikainen H, Valve R, et al. Clinical benefit of gluten-free diet in screen-detected older celiac disease patients. BMC Gastroenterol. (2011) 11:136. doi: 10.1186/1471-230X-11-136
108. Johnston SD, Rodgers C, Watson RG. Quality of life in screen-detected and typical coeliac disease and the effect of excluding dietary gluten. Eur J Gastroenterol Hepatol. (2004) 16:1281–6. doi: 10.1097/00042737-200412000-00008
109. Burger JPW, de Brouwer B, IntHout J, Wahab PJ, Tummers M, Drenth JPH. Systematic review with meta-analysis: dietary adherence influences normalization of health-related quality of life in coeliac disease. Clin Nutr. (2017) 36:399–406. doi: 10.1016/j.clnu.2016.04.021
110. Dennis M, Case S. Going gluten-free: a primer for clinicians. Pract Gastroenterol. (2004) 28:86–104.
111. Lee AR, Ng DL, Dave E, Ciaccio EJ, Green PH. The effect of substituting alternative grains in the diet on the nutritional profile of the gluten-free diet. J Hum Nutr Diet. (2009) 22:359–63. doi: 10.1111/j.1365-277X.2009.00970.x
112. Wessels MMS, Te Lintelo M, Vriezinga SL, Putter H, Hopman EG, Mearin ML. Assessment of dietary compliance in celiac children using a standardized dietary interview. Clin Nutr. (2018) 37:1000–4. doi: 10.1016/j.clnu.2017.04.010
113. Vriezinga S, Borghorst A, van den Akker-van Marle E, Benninga M, George E, Hendriks D, et al. E-healthcare for celiac disease–a multicenter randomized controlled trial. J Pediatr. (2018) 195:154–60. doi: 10.1016/j.jpeds.2017.10.027
114. Hogen Esch CE, Wolters VM, Gerritsen SA, Putter H, von Blomberg BM, van Hoogstraten IM, et al. Specific celiac disease antibodies in children on a gluten free diet. Pediatrics (2011) 128:547–52. doi: 10.1542/peds.2010-3762
115. Roos S, Wilhelmsson S, Hallert C. Swedish women with coeliac disease in remission use more health care services than other women: a controlled study. Scand J Gastroenterol. (2011) 46:13–9. doi: 10.3109/00365521.2010.516448
116. Rubio-Tapia A, Rahim M, See J, Lahr B, Wu T, Murray J. Mucosal recovery and mortality in adults with celiac disease after treatment with a gluten-free diet. Am J Gastroenterol. (2010) 105:1412–20. doi: 10.1038/ajg.2010.10
117. Moreno ML, Cebolla Á, Muñoz-Suano A, Carrillo-Carrion C, Comino I, Pizarro Á, et al. Detection of gluten immunogenic peptides in the urine of patients with coeliac disease reveals transgressions in the gluten-free diet and incomplete mucosal healing. Gut (2017) 66:250–7. doi: 10.1136/gutjnl-2015-310148
118. Paterson BM, Lammers KM, Arrieta MC, Fasano A, Meddings JB. The safety, tolerance, pharmacokinetic and pharmacodynamic effects of single doses of AT-1001 in coeliac disease subjects: a proof of concept study. Aliment Pharmacol Ther. (2007) 26:757–66. doi: 10.1111/j.1365-2036.2007.03413.x
119. Gopalakrishnan S, Durai M, Kitchens K, Tamiz AP, Somerville R, Ginski M, et al. Larazotide acetate regulates epithelial tight junctions in vitro and in vivo. Peptides (2012) 35:86–94. doi: 10.1016/j.peptides.2012.02.015
120. Leffler DA, Kelly CP, Abdallah HZ, Colatrella AM, Harris LA, Leon F, et al. A randomized, double-blind study of larazotide acetate to prevent the activation of celiac disease during gluten challenge. Am J Gastroenterol. (2012) 107:1554–62. doi: 10.1038/ajg.2012.211
121. Leffler DA, Kelly CP, Green PH, Fedorak RN, DiMarino A, Perrow W, et al. Larazotide acetate for persistent symptoms of celiac disease despite a gluten-free diet: a randomized controlled trial. Gastroenterology. (2015) 148:1311–9. doi: 10.1053/j.gastro.2015.02.008
122. Kelly CP, Green PH, Murray JA, Dimarino A, Colatrella A, Leffler DA, et al. Larazotide Acetate Celiac Disease Study Group. Larazotide acetate in patients with coeliac disease undergoing a gluten challenge: a randomised placebo-controlled study. Aliment Pharmacol Ther. (2013) 37:252–62. doi: 10.1111/apt.12147
123. Gass J, Bethune MT, Siegel M, Spencer A, Khosla C. Combination enzyme therapy for gastric digestion of dietary gluten in patients with celiac sprue. Gastroenterology (2007) 133:472–80. doi: 10.1053/j.gastro.2007.05.028
124. Bethune MT, Strop P, Tang Y, Sollid LM, Khosla C. Heterologous expression, purification, refolding, and structural-functional characterization of EP-B2, a self-activating barley cysteine endoprotease. Chem Biol. (2006) 13:637–47. doi: 10.1016/j.chembiol.2006.04.008
125. Murray JA, Kelly CP, Green PHR, Marcantonio A, Wu TT, Mäki M, et al. CeliAction Study Group of Investigators. No difference between Latiglutenase and placebo in reducing villous atrophy or improving symptoms in patients with symptomatic celiac disease. Gastroenterology (2017) 152:787–98. doi: 10.1053/j.gastro.2016.11.004
126. Syage JA, Murray JA, Green PHR, Khosla C. Latiglutenase improves symptoms in seropositive celiac disease patients while on a gluten-free diet. Dig Dis Sci. (2017) 62:2428–32. doi: 10.1007/s10620-017-4687-7
127. Stepniak D, Spaenij-Dekking L, Mitea C, Moester M, de Ru A, Baak-Pablo R, et al. Highly efficient gluten degradation with a newly identified prolyl endoprotease: implications for celiac disease. Am J Physiol Gastrointest Liver Physiol. (2006) 291:G621–G629. doi: 10.1152/ajpgi.00034.2006
128. König J, Holster S, Bruins MJ, Brummer RJ. Randomized clinical trial: effective gluten degradation by Aspergillus niger-derived enzyme in a complex meal setting. Sci Rep. (2017) 7:13100. doi: 10.1038/s41598-017-13587-7
129. Goel G, King T, Daveson AJ, Andrews JM, Krishnarajah J, Krause R, et al. Epitope-specific immunotherapy targeting CD4-positive T cells in coeliac disease: two randomised, double-blind, placebo-controlled phase 1 studies. Lancet Gastroenterol Hepatol. (2017) 2:479–93. doi: 10.1016/S2468-1253(17)30110-3
Keywords: celiac disease, prevention, preventive strategies, environmental factors, tertiary prevention
Citation: Meijer C, Shamir R, Szajewska H and Mearin L (2018) Celiac Disease Prevention. Front. Pediatr. 6:368. doi: 10.3389/fped.2018.00368
Received: 23 August 2018; Accepted: 12 November 2018;
Published: 30 November 2018.
Edited by:
Ron Shaoul, Rambam Health Care Campus, IsraelCopyright © 2018 Meijer, Shamir, Szajewska and Mearin. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Caroline Meijer, Yy5yLm1laWplci1ib2VrZWxAbHVtYy5ubA==