 Tamás Kovács
Tamás Kovács Gyula Pásztor
Gyula Pásztor Anna Rieth
Anna Rieth- 1Unit of Pediatric Surgery, Department of Pediatrics, Albert Szent-Gyorgyi Clinical Center, University of Szeged, Szeged, Hungary
- 2Department of Radiology, Albert Szent-Gyorgyi Clinical Center, University of Szeged, Szeged, Hungary
Objectives: Minimal invasive repair of pectus excavatum (MIRPE) described by Nuss is the most popular correction nowadays of this deformity. During the introduction of the bars, they can hurt or compress the internal mammary arteries (IMA). The aim of this study was to observe the prevalence of IMA compression in children after MIRPE. Also, we examined if IMA obstruction increases the risk of complications at bar removal, and if these vascular changes are reversible.
Materials and Methods: All patients operated on pectus excavatum in our tertiary pediatric surgical center between 2013 and 2019 were involved in the study. Data of age, sex, number of bars and characteristics of the deformity were examined. IMA flow was checked by Doppler ultrasound (DUS) after MIRPE and after bar removal, too.
Results: Among 41 patients with mean age of 15.2 years there were 18 asymmetrical deformities, 23 sternal rotations. Mean pectus index was 4.01. After the Nuss procedure 7(9%) stenoses and 10(12%) occlusions of IMA were found on DUS. After bar removal 3 of 4 stenoses have resolved, but all examined occlusions (3/3) persisted. There were no complications during bar removals.
Conclusion: IMA compression after MIRPE in children is uncommon, and is not influenced by severity of deformity. Obstruction of these vessels does not increase the risk of hemorrhagic complications at bar removal. Data of larger cohort are needed to determine reversibility of these changes.
Introduction
Pectus excavatum (PE) is the most common chest wall deformity, characterized by depression of the sternum and adjacent costal cartilages. It occurs in 1:400 live births, with a 1:4 male predominance. Since 1949 the surgical correction described by Ravitch has become widespread (1), until in 1998 Donald Nuss published a minimal invasive repair technique for PE (MIRPE) (2). Since then, this type of surgery has gained popularity, with some technical modifications during the years (3–9). Correction of position of the sternum is achieved by one or more shaped and retrosternally positioned bars. During the introduction of the Nuss bars, they can hurt or compress the internal mammary arteries (IMA). These vessels arise from the subclavian arteries, and descend in the thorax posteriorly and laterally to the sternum. During the Nuss procedure, the introducer and the bar pass through the intercostal space near this point, which may lead to injury, occlusion or erosion of these vessels.
Adult series have investigated the effect of the Nuss procedure on the IMA flow (10). Pre- and post-operative CT angiography was used to detect the patency of these vessels. In 44% uni- or bi-lateral obstruction was found. Our aim was to observe the changes in IMA flow in pediatric patients after minimal invasive correction of PE using Doppler ultrasound (DUS). We examined if obstruction of IMA increases the risk of complications at bar removal. Also, we have observed whether the changes in IMA flow are reversible after removing the Nuss bars.
Materials and Methods
Data of patients operated between December 2013 and September 2019 in our pediatric surgical department were analyzed after Local Ethics Committee approval. All patients have had written informed consent. All patients operated in this period with PE were involved in the study. Routine preoperative evaluation included low-dose chest CT, echocardiography, and thoracic Doppler ultrasound (DUS) examination. Data were collected regarding age at time of surgery, sex, number of bars, preoperative Haller index, symmetry of deformity, sternal rotation, and IMA flow. Ultrasound was performed by pediatric radiologists in B-mode and in color Doppler using GE Logiq S8 (GE Healthcare, Chicago, IL, USA) Disturbances of IMA flow were described as stenosis or occlusion at site of the bar. Increased velocity of blood flow at this point was defined as arterial stenosis. Moreover, in color Doppler examination aliasing was noted. Occlusion was described when the blood flow was not detectable caudally from the bar. IMA flow was examined after implanting the bar and also after bar removal.
Statistical Methods
Descriptive statistics are presented as mean and SD for continuous data and frequencies and percentages as categorical data. For the comparison of groups, Welch test (Student's unpaired t-test for unequal variances) was used for continuous variables and Fisher's exact test was used for categorical variables. Calculations were performed by SPSS for Windows software (version 26.0; SPSS Inc., Chicago, IL, USA). P-values < 0.05 were regarded as statistically significant.
Results
Forty-one patients (36 male and 5 female) were involved in the study. Mean age was 15.2 ± 1.3 years at time of the operation (median age: 15.04 years, range 13–19 years). There were 23 (56.1%) symmetrical and 18 (43.9%) asymmetrical deformities, accompanied with 23 rotational deformities (5 left and 18 right rotational). Preoperative mean Haller index of the patients was 4.01 ± 0.98 (range 2.32–6.1). All patients had Nuss procedure with thoracoscopic guidance, two of them received two bars, while in 39 patients one bar was employed.
Eighty two IMAs (in 41 patients) were examined by pre- and post-operative thoracic DUS. Examination revealed patent vascular flow in 65 arteries (79%). Mean vascular flow of these unaffected arteries was 71.5 ± 38.42 cm/sec (range 31–140 cm/s) on the left, and 83.3 ± 31.06 cm/s (range 27–162 cm/s) on the right side.
Affected IMAs were noted as stenosis in seven arteries (9%), and occlusion in 10 arteries (12%). These obstructions were unilateral in 88%, and bilateral in 12%. Characteristics and data of patients are shown in Table 1.
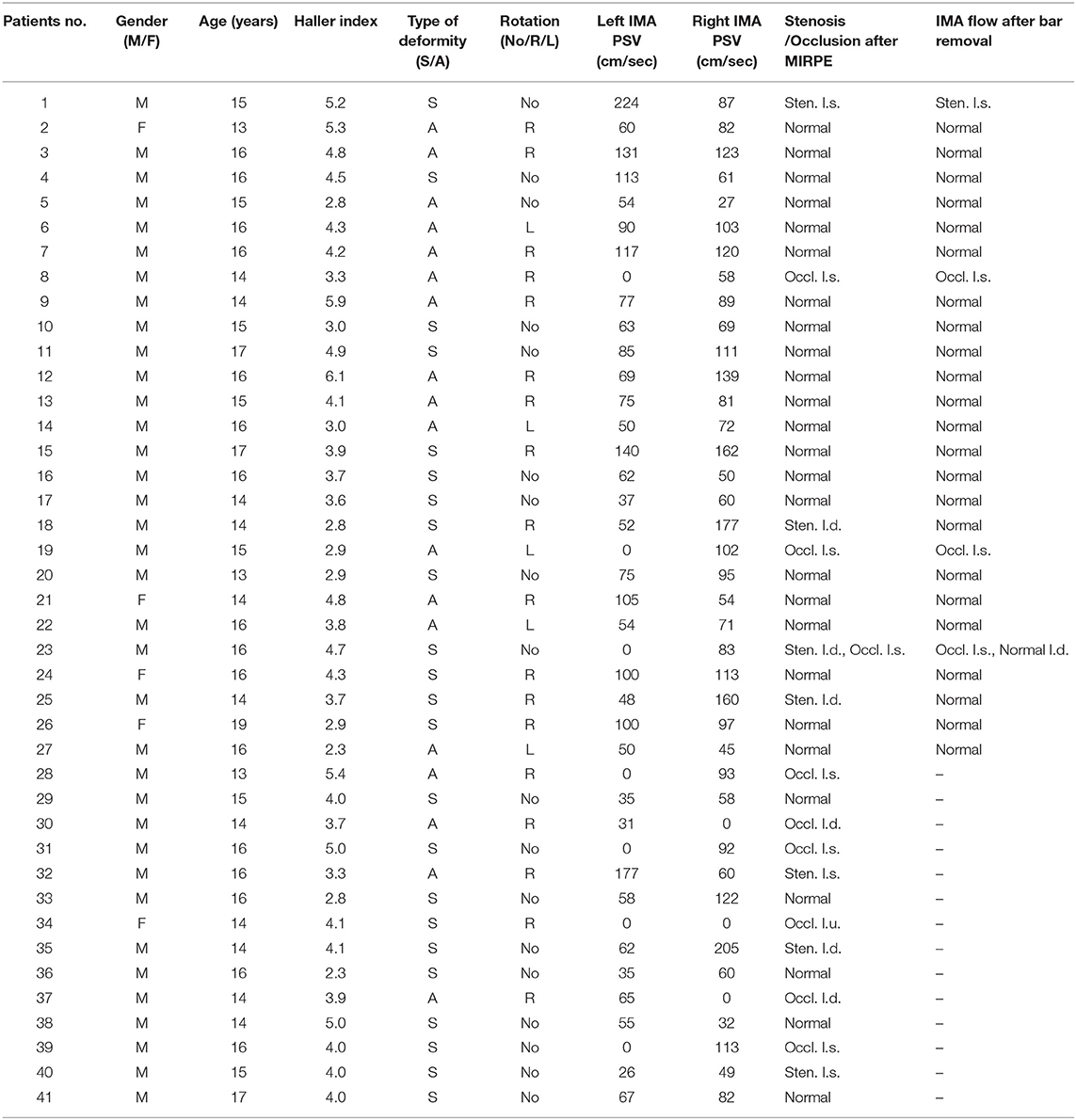
Table 1. Characteristics and data of patients.
We have compared the patients with affected and unaffected IMA flow, whether there is any difference among them in terms of age, sex, severity of deformity, symmetry, rotational deformity. As Table 2 shows there is statistically significant difference between the two groups only regarding age, but asymmetry, sternal rotation, higher Haller index do not elevate the risk of IMA compression.
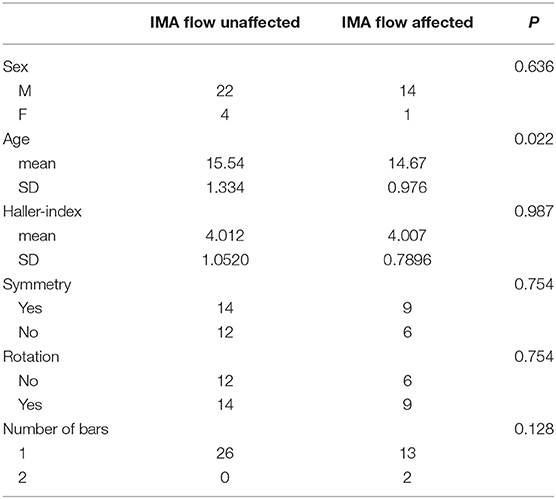
Table 2. Comparison of patients with affected and unaffected IMA flow.
So far the bars were removed from 27 of the 41 patients. Mean length between Nuss procedure and bar removal was 3.01 years (range 2.76–3.19 years). There were no complications observed during these operations. IMA flow was checked also after bar removal. Among the 27 patients there were six with IMA compression (four stenoses, three occlusions, in one patient bilateral compression). We have found that three stenoses have resolved, while one stenosis and all three occlusions were still noted on control DUS. In the other 21 patients, in whom the post- Nuss procedure DUS showed normal IMA flow also had normal flow on the US performed after bar removal.
Discussion
Nuss procedure is the gold standard treatment for PE to correct the anatomical deformity of the chest wall. The operation is safe and gives perfect cosmetic result, however it is important to know that certain mild or serious complications can occur (3). The overall incidence of these complications is reported between 2 and 20% (11); however the incidence of severe complications is fortunately only 0.1% (8). Among the latter, injury of the heart (12), major vessels (12, 13), lung (14), diaphragm (15) can occur. Predisposing factors for cardiac injury are mediastinal adhesions due to previous cardiac or thoracic surgery, and the risk of this complication can be decreased with the use of thoracoscopy, sternal elevation and substernal dissection (3, 9, 16, 17).
Another source of hemorrhage can be the intraoperative injury of vessels, most frequently the IMA. As the IMA traverse posterolateral to the sternum, the introducer or the bar might injure it. This complication can also be minimized with the use of thoracoscope, when the bar or introducer can be followed under direct visual control (11, 17). As late on-set complication, hemothorax resulting from erosion of the IMA by the Nuss bar is published, too (18, 19). In these cases the bleeding was stopped by angiographic embolization of IMA (18) or ligation of the vessel via thoracotomy (19).
The introduced bar distending to the sternum can also compress the IMA-s, causing stenosis or complete obstruction in them. Yüksel et al. used pre and postoperative CT angiography (CTA) in adults to detect the change in IMA blood flow. In 44% of patients the blood flow was affected. Among these patients 33% bilateral, 46% unilateral obstruction, and 21% unilateral stenosis was observed (10).
In pediatric patients CTA is not advised to measure the blood flow in these vessels because of the high exposure to radiation. However, Doppler US can be perfectly used to investigate IMA flow in children. A tri-phasic curve with normal velocity shows normal flow, while elevated speed or non-tri-phasic curve means stenosis and lack of curve means complete obstruction.
According to our data IMA compression in pediatric patients after MIRPE is not common, in 79% of the cases the flow is unaffected. In 9% stenosis, while in 12% total occlusion of these vessels was detected. The alterations of the blood flow were unilateral in most cases (88%), and bilateral only in 12%. Interestingly, these changes were independent from the severity and characteristics of the deformity.
Serious, even fatal hemorrhagic complications are reported in literature at bar removal, too (11, 20). As the source of bleeding, the injury of heart, lung, aorta or sternal erosion are mentioned (11, 20–24) and it is related to mediastinal adhesions between these organs and the bar. Carlucci advises the use of thoracoscopy for bar removals in case of bar dislocation (22). Campos proposed to cover the serrated edges of the implants with a protective film at bar removal to minimize hemorrhagic complications (25). Toselli uses a safety string at all bar removals, and in case of bleeding a sponge or Sangstaken Blakemore catheter can be attached to it and can be dragged into the tunnel to control the hemorrhage (26). We have examined, whether removing those bars which were compressing the IMA-s increase the risk of intraoperative hemorrhage, and if these bar removals should be performed with extra precautions, for example, thoracoscopic control. Fortunately, so far there were no complications during these removals, and thus we don't advice any change in the operative technique in case of IMA compression.
As IMA is used in adult cardiac surgery for coronary artery bypassing grafting, it can be important to know if the changes in IMA flow are reversible after bar removal. In a pilot study among adults with bar removal after Nuss repair, Külcü published IMA occlusion in four of s patients (27). Therefore, he recommends preoperative evaluation of IMA patency in all patients with history of PE repair undergoing coronary bypass grafting. To prevent IMA compression by the Nuss bar, Sessar advices thoracoscopic mobilization of IMA at the level of bar implantation during MIRPE and pass the bar between the chest wall and the artery (28). On the other hand, this procedure might lead to adhesions and cause bleeding at bar removal (29). Cabrera recommends taking down the IMA-s from the intercostal space and placing pericardium membrane between the bar and the vessels, especially in patients with family history of coronary artery disease (30).
Our study is still in progress, but after removing more than half of the bars from our examined patients, it seems that while stenosis can be reversible (in 75% of stenoses the flow has normalized after ceasing of compression), occlusion is definitive, as flow was not detectable in any of these vessels after the bar removal. Naturally, data of a large multicenter cohort can give the exact answer, how much the circulation in these vessels can normalize after bar removal.
Conclusion
Our data shows that IMA obstruction is not common in pediatric patients after MIRPE. Stenosis and occlusion is not influenced by severity of the deformity, sternal rotation or asymmetry. IMA compression associated with MIRPE does not elevate the risk of hemorrhagic complications at bar removal. Further studies on large cohort are needed to determine the reversibility of the changes in IMA flow after removing the pectus bars.
Data Availability Statement
The original contributions presented in the study are included in the article/supplementary material, further inquiries can be directed to the corresponding author/s.
Ethics Statement
The studies involving human participants were reviewed and approved by Scientific Ethic Committee of University of Szeged. Written informed consent to participate in this study was provided by the participants' legal guardian/next of kin.
Author Contributions
TK and AR participated in collecting and interpreting of data. The manuscript was written by TK. The ultrasound examinations were performed by GP. All authors contributed to the article and approved the submitted version.
Funding
This work was supported by University of Szeged Open Access Fund (no. 5016).
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Abbreviations
CTA, computerized tomography angiography; DUS, doppler ultrasound; IMA, internal mammary artery, internal thoracic artery; MIRPE, minimally invasive repair of pectus excavatum; PE, pectus excavatum; PSV, peak systolic velocity.
References
1. Ravitch MM. The operative treatment of pectus excavatum. Ann Surg. (1949) 129:429–44. doi: 10.1097/00000658-194904000-00002
2. Nuss D, Kelly RE, Croitoru DP, Katz ME. A 10-year review of a minimally invasive technique for the correction of pectus excavatum. J Pediatr Surg. (1998) 33:545–52. doi: 10.1016/s0022-3468(98)90314-1
3. Nuss D, Croitoru DP, Kelly RE, Goretsky MJ, Nuss KJ, Gustin TS. Review and discussion of the complications of minimally invasive pectus excavatum repair. Eur J Pediatr Surg. (2002) 12:230–4. doi: 10.1055/s-2002-34485
4. Park HJ, Lee SY, Lee CS, Youm W, Lee KR. The Nuss procedure for pectus excavatum: evolution of techniques and early results on 322 patients. Ann Thorac Surg. (2004) 77:289–95. doi: 10.1016/s0003-4975(03)01330-4
5. Hebra A, Gauderer MW, Tagge EP, Adamson WT, Othersen HB. A simple technique for preventing bar displacement with the Nuss repair of pectus excavatum. J Pediatr Surg. (2001) 36:1266–8. doi: 10.1053/jpsu.2001.25791
6. Croitoru DP, Kelly RE, Goretsky MJ, Lawson ML, Swoveland B, Nuss D. Experience and modification update for the minimally invasive Nuss technique for pectus excavatum repair in 303 patients. J Pediatr Surg. (2002) 37:437–45. doi: 10.1053/jpsu.2002.30851
7. Notrica DM. The Nuss procedure for repair of pectus excavatum: 20 error traps and a culture of safety. Semin Pediatr Surg. (2019) 28:172–7. doi: 10.1053/j.sempedsurg.2019.04.020
8. Kelly R. E., Mellins R. B., Shamberger R. C., Mitchell K. K., Lawson M. L., Oldham K. T., et al. Multicenter study of pectus excavatum, final report: complications, static/exercise pulmonary function, and anatomic outcomes. J Am Coll Surg. (2013) 217:1080–9. doi: 10.1016/j.jamcollsurg.2013.06.019
9. Goretsky M. J., and McGuire M. M. Complications associated with the minimally invasive repair of pectus excavatum. Semin Pediatr Surg. (2018) 27:151–5. doi: 10.1053/j.sempedsurg.2018.05001
10. Yüksel M, Özalper MH, Bostanci K, Ermerak NO, Cimşit Ç, Tasali N, et al. Do Nuss bars compromise the blood flow of the internal mammary arteries? Interact Cardiovasc Thorac Surg. (2013) 17:571–5. doi: 10.1093/icvts/ivt255
11. Hebra A, Kelly RE, Ferro MM, Yüksel M, Campos JRM, Nuss D. Life-threatening complications and mortality of minimally invasive pectus surgery. J Pediatr Surg. (2018) 53:728–32. doi: 10.1016/j.jpedsurg.2017.07.020
12. Becmeur F, Ferreira CG, Haecker F-M, Schneider A, Lacreuse I. Pectus excavatum repair according to Nuss: is it safe to place a retrosternal bar by a transpleural approach, under thoracoscopic vision? J Laparoendosc Adv Surg Tech A. (2011) 21:757–61. doi: 10.1089/lap.2011.0035
13. Hoel TN, Rein KA, Svennevig JL. A life-threatening complication of the Nuss procedure for pectus excavatum. Ann Thorac Surg. (2006) 81:370–2. doi: 10.1016/j.athoracsur.2004.09.008
14. Kim DY, Jeong JY. Penetrating lung injury during Nuss procedure for pectus excavatum. J Cardiothorac Surg. (2020) 15:184. doi: 10.1186/s13019-020-01236-6
15. Marusch F, Gastinger I. [Life-threatening complication of the Nuss-procedure for funnel chest. A case report] Zentralbl Chir. (2003) 128:981–4. doi: 10.1055/s-2003-44807
16. Cheng Y-L, Lee S-C, Huang T-W, Wu C-T. Efficacy and safety of modified bilateral thoracoscopy-assisted Nuss procedure in adult patients with pectus excavatum. Eur J Cardiothorac Surg. (2008) 34:1057–61. doi: 10.1016/j.ejcts.2008.07.068
17. Mennie N, Frawley G, Crameri J, King SK. The effect of thoracoscopy upon the repair of pectus excavatum. J Pediatr Surg. (2018) 53:740–3. doi: 10.1016/j.jpedsurg.2017.07.019
18. Adam LA, Meehan JJ. Erosion of the Nuss bar into the internal mammary artery 4 months after minimally invasive repair of pectus excavatum. J Pediatr Surg. (2008) 43:394–7. doi: 10.1016/j.jpedsurg.2007.10.002
19. Barsness K, Bruny J, Janik JS, Partrick DA. Delayed near-fatal hemorrhage after Nuss bar displacement. J Pediatr Surg. (2005) 40:e5–6. doi: 10.1016/j.jpedsurg.2005.07.038
20. Haecker Fm, Berberich T, Mayr J, Gambazzi F. Near-fatal bleeding after transmyocardial ventricle lesion during removal of the pectus bar after the Nuss procedure. J Thorac Cardiovasc Surg. (2008) 138:1240–1. doi: 10.1016/j.jtcvs.2008.07.027
21. Cohen NS, Goretsky MJ, Obermeyer RJ. Bleeding at removal of nuss bar: rare but sometimes significant. J Laparoendosc Adv Surg Tech A. (2018) 28:1393–6. doi: 10.1089/lap.2018.0175
22. Carlucci M, Torre M, Jasonni V. An uncommon complication of Nuss bar removal: Is blind removal a safe procedure? J Pediatr Surg Case Rep. (2013) 1:34–5. doi: 10.1016/j.epsc.2013.02.014
23. Jemielity M, Pawlak K, Piwkowski C, Dyszkiewicz W. Life-threatening aortic hemorrhage during pectus bar removal. Ann Thorac Surg. (2011) 91:593–5. doi: 10.1016/j.athoracsur.2010.07.041
24. Notrica DM, McMahon LE, Johnson KN, Velez DA, McGill LC, Jaroszewski DE. Life-threatening hemorrhage during removal of a Nuss bar associated with sternal erosion. Ann Thorac Surg. (2014) 98:1104–6. doi: 10.1016/j.athoracsur.2013.10.097
25. de Campos JRM, Das-Neves-Pereira J-C, Lopes KM, Jatene FB. Technical modifications in stabilisers and in bar removal in the Nuss procedure. Eur J Cardiothorac Surg. (2009) 36:410–2. doi: 10.1016/j.ejcts.2009.03061
26. Toselli L, Munzón GB, Martinez J, Vallee M, Sanjurjo D, Peirano MN, et al. Safety-string: a handy maneuver to control pectus bar removal bleeding complications. J Ped Surg. (2020) 55:1162–4. doi: 10.1016/j.jpedsurg.2020.01.058
27. Külcü K, Elenbaas TW, Nguyen DT, Verhees RPM, Mihl C, Verberkmoes, et al. Patency of the internal mammary arteries after removal of the Nuss bar: an initial report. Interact Cardiovasc Thorac Surg. (2014) 19:6–9. doi: 10.1093/icvts/ivu083
28. Sersar SI. eComment. Suggestions that may prevent internal mammary artery obstruction after thoracoscopic Nuss bar repair of pectus. Interact Cardiovasc Thorac Surg. (2014) 19:9–10. doi: 10.1093/icvts/ivu136
29. Wurtz A, Hysi I, Benhamed L, Vincentelli A. eComment. Nuss pectus excavatum repair: a hurdle for the treatment of coronary disease Interact. Cardiovasc Thorac Surg. (2014) 19:10. doi: 10.1093/icvts/ivu150
Keywords: complications, Doppler ultrasound, pectus excavatum, bar removal, internal mammary artery
Citation: Kovács T, Pásztor G and Rieth A (2021) Internal Mammary Artery Compression After Pectus Excavatum Repair Does Not Increase Risk of Hemorrhagic Complications in Pediatric Patients. Front. Pediatr. 8:619065. doi: 10.3389/fped.2020.619065
Received: 19 October 2020; Accepted: 07 December 2020;
Published: 05 January 2021.
Edited by:
Jürgen Schleef, IRCCS Materno Infantile Burlo Garofolo (IRCCS), ItalyReviewed by:
Ciro Esposito, University of Naples Federico II, ItalyRadoica Radivoje Jokic, University of Novi Sad, Serbia
Copyright © 2021 Kovács, Pásztor and Rieth. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Tamás Kovács, a292YWNzLnRhbWFzQG1lZC51LXN6ZWdlZC5odQ==