 Kim Vettenranta
Kim Vettenranta Veronika Dobsinska
Veronika Dobsinska Gabriella Kertész
Gabriella Kertész Peter Svec
Peter Svec Jochen Buechner4
Jochen Buechner4 Kirk R. Schultz
Kirk R. Schultz- 1University of Helsinki and Children's Hospital, University of Helsinki, Helsinki, Finland
- 2Department of Pediatric Hematology and Oncology, National Institute of Children's Diseases, Comenius University, Bratislava, Slovakia
- 3Department of Pediatric Hematology and Stem Cell Transplantation, Central Hospital of Southern Pest – National Institute of Hematology and Infectious Diseases, Budapest, Hungary
- 4Department of Pediatric Hematology and Oncology, Oslo University Hospital, Oslo, Norway
- 5Michael Cuccione Childhood Cancer Research Program, British Columbia Children's Hospital Research Institute, University of British Columbia, Vancouver, BC, Canada
Previously, the outcome of paediatric Philadelphia-chromosome–positive (Ph+) ALL treated with conventional chemotherapy alone was poor, necessitating the use of haematopoietic stem cell transplantation (HSCT) for the best outcomes. The recent addition of tyrosine kinase inhibitors (TKIs) alongside the chemotherapy regimens for Ph+ ALL has markedly improved outcomes, replacing the need for HSCT for lower risk patients. An additional poor prognosis group of Philadelphia-chromosome–like (Ph-like) ALL has also been identified. This group also can be targeted by TKIs in combination with chemotherapy, but the role of HSCT in this population is not clear. The impact of novel targeted immunotherapies (chimeric antigen receptor T cells and bispecific or drug-conjugated antibodies) has improved the outcome of patients, in combination with chemotherapy, and made the role of HSCT as the optimal curative therapy for Ph+ ALL and Ph-like ALL less clear. The prognosis of patients with Ph+ ALL and persistent minimal residual disease (MRD) at the end of consolidation despite TKI therapy or with additional genetic risk factors remains inferior when HSCT is not used. For such high-risk patients, HSCT using total-body-irradiation–containing conditioning is currently recommended. This review aims to provide an update on the current and future role of HSCT for Ph+ ALL and addresses key questions related to the management of these patients, including the role of HSCT in first complete remission, MRD evaluation and related actions post HSCT, TKI usage post HSCT, and the putative role of HSCT in Ph-like ALL.
Introduction
Philadelphia-chromosome–positive (Ph+) acute lymphoblastic leukaemia (ALL) and, more recently, also Philadelphia-chromosome–like (Ph-like; also known as BCR-ABL–like) ALL have been identified to be associated with poor prognosis when patients receive standard chemotherapy regimens (1–3). Ph+ ALL is found in fewer than 5% of paediatric patients with ALL but in more than 20% of adults with ALL, with the incidence in adolescents falling in between. With the advent of tyrosine kinase inhibitors (TKI) (Figure 1), the prognosis for paediatric patients with Ph+ ALL treated with TKIs added to the chemotherapy backbones began to approach that of non-Ph+ ALL patients (4–8). However, subgroups of Ph+ patients (e.g., those with IKZF mutations) with a substantially less favourable prognosis have been identified (6, 9). Allogeneic haematopoietic stem cell transplantation (HSCT) for consolidation of remission in Ph+ ALL patients is now reserved for those with specific high-risk features (2, 7). The role of HSCT in Ph-like ALL is less clear. In this review, we summarize the current role of HSCT in Ph+/Ph-like ALL.
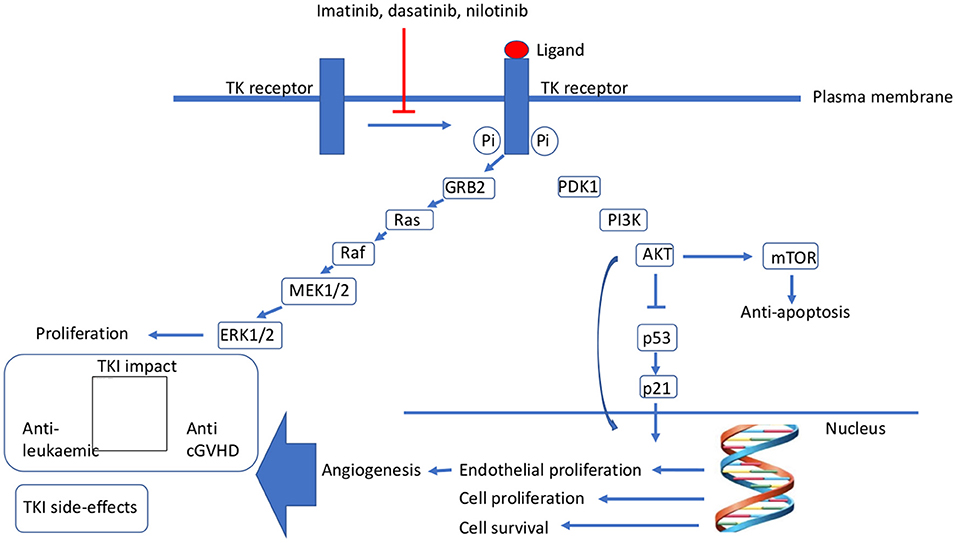
Figure 1. Mechanism of action of tyrosine kinase inhibitors. AKT, protein kinase B; cGvHD, chronic graft-vs.-host disease; ERK1/2, extracellular signal-regulated kinase 1/2; GRB2, growth factor receptor-bound protein 2; MEK1/2, mitogen-activated protein kinase 1/2; mTOR, mammalian target of rapamycin; Pi, phosphorylation; PI3K, phosphatidylinositol-3-kinase; TK, tyrosine kinase.
Recent Advances In The Chemotherapy Of Ph+ ALL And Their Impact On The Role Of HSCT
With the advent of TKIs, the role of HSCT in the treatment of paediatric Ph+ ALL has changed (summarized in Table 1) (4, 6, 8, 10–12). The non-randomized Children's Oncology Group (COG) AALL0031 trial added imatinib to an intensive chemotherapy backbone for the treatment of paediatric Ph+ ALL; only patients with a matched sibling donor (MSD) were stratified to undergo HSCT, with many patients taken off study for a matched unrelated donor (MUD) HSCT. No advantage of allogeneic HSCT was observed compared to the chemotherapy plus imatinib arm: 3-year event-free survival (EFS) was 87.7% for chemotherapy plus imatinib, 56.6% for MSD HSCT and 71.6% for MUD HSCT (5). The EsPhALL2004 trial, which also combined imatinib with chemotherapy for the treatment of paediatric Ph+ ALL, confirmed the outcome of the COG trial. In this trial, HSCT was indicated for poor-risk patients with any donor type and for good-risk patients with an MRD or MUD. When censored at the time of HSCT, the 2-year disease-free survival (DFS) was 81.2% in the good-risk group treated with imatinib vs. 65.4% in the good-risk group treated without imatinib. In the poor-risk group, in which 84% of patients underwent HSCT, the 4-year EFS was 53.5% (10). A third study in paediatric Ph+ ALL—EsPhALL2010—used a similar strategy to the AALL0031 study by giving imatinib continuously (300 mg/m2) but starting at an earlier timepoint of day 15 of the induction chemotherapy. Starting with the same HSCT indications as in the EsPhALL2004 protocol, the criteria were restricted in 2012 based on the consensus that good responders (defined by minimal residual disease [MRD] level at the end of consolidation) did not need HSCT. Thus, HSCT was reserved for the poor responders only (MRD ≥5 × 10−4). The 5-year overall survival (OS) for the group of patients undergoing HSCT in first complete remission (CR1) group was 77.3% compared to 73.6% for the non-transplanted patients (p = 0.63) (8).
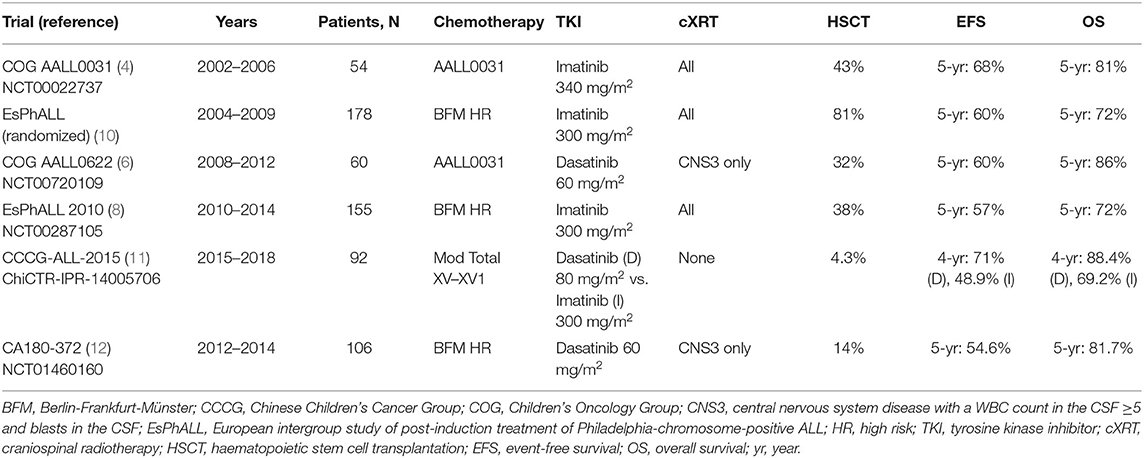
Table 1. Summary of published trials investigating TKIs for Ph+ ALL in children and adolescents.
Dasatinib in combination with chemotherapy was evaluated also in the COG AALL0622 trial of paediatric Ph+ ALL, with dasatinib added at day 15 to the identical chemotherapy backbone used in the AALL0031 trial. The 5-yr EFS was similar for the non-transplanted and transplanted groups (60 vs. 61%, respectively). The study concluded that HSCT should be limited to the high-risk group of slow responders as defined by the MRD levels. In addition, this trial suggested a potential role for transplantation in patients with additional IKZF1 deletions as a significant negative prognostic factor (6). In the COG AALL1122 phase 2 trial in paediatric Ph+ ALL, strategies from AALL0622 and EsPhALL2010 were merged and dasatinib (starting on day 15) administered with EsPhALL chemotherapy. The indication for HSCT in CR1 was restricted to patients with an MRD ≥0.05% at the end of consolidation or any MRD positivity following three additional high-risk chemotherapy blocks. An early study report showed that a substantially lower percentage of patients were transplanted in the trial compared to the percentages in the EsPhALL 2004 and 2010 trials, while similar outcomes were observed (5-year EFS was 54.6% in AALL1122 vs 60.3% in EsPhALL 2004 and 57% in EsPhALL 2010 for the whole pt cohort) (12).
With the possible benefit of dasatinib over imatinib remaining unestablished, the current EsPhALL2017/COG AALL1631 trial in paediatric Ph+ ALL (NCT03007147) was launched to study imatinib with randomization to EsPhALL (arm A) vs AALL1131-type chemo backbone using a non-inferiority design and imatinib in combination with the chemotherapy backbone. Only high-risk patients (MRD ≥5 × 104 at end of consolidation) are being allocated to allogeneic HSCT. For the HSCT patients, the study is investigating the feasibility of administering imatinib post HSCT.
HSCT in Ph+ ALL
With the success of the addition of a TKI to a chemotherapy backbone for the treatment of paediatric and adolescent Ph+ ALL, the future role of HSCT in the treatment of paediatric and adolescent Ph+ ALL remains to be delineated. HSCT represents a multimodal immune therapy for Ph+ ALL through a comprehensive immune response including T, B, natural killer (NK) and professional antigen-presenting cells. Ph+ ALL appears to respond well to immune therapy mediated by HSCT, with the overall survival rates hovering at 70–80% (8, 13) as compared with other subgroups of high-risk paediatric ALL such as hypodiploid ALL (8). Yet, HSCT is limited as a potential therapy primarily by its associated, immune-mediated toxicity as acute and chronic graft-vs.-host disease (GvHD) (Figure 1).
Currently, the majority of paediatric ALL patients undergoing HSCT receive TBI-containing conditioning (14), especially those with a very high relapse risk (15). TBI-based conditioning regimens are also widely used to prepare children with Ph+ ALL for HSCT (14). Due to the known late effects associated with the use of TBI (endocrine effects, reduced cognitive function, infertility, cataracts, and an increased risk of secondary malignancies), it has for a long time been a matter of intense debate whether chemoconditioning can effectively replace TBI. In their retrospective study, Friend et al. (14) found that ALL patients who received a non–TBI-based conditioning regimen had a lower 3-year EFS compared to those who received TBI (52 vs. 77%, respectively; p = 0.03). In their paper, but without a subgroup analysis, a small group of Ph+ patients were included, mostly in the non-TBI arm. Importantly, MRD positivity as measured by next-generation sequencing (NGS) prior to transplant was highly predictive of relapse: NGS-MRD negative patients had a 0% rate of relapse compared to a 50% relapse rate for the NGS-MRD–positive patients prior to HSCT (p = 0.04).
To further compare outcomes of TBI vs. chemoconditioning regimens, a multicentre European Society for Bone and Marrow Transplantation (EBMT) Paediatric Diseases Working Party (PDWP) retrospective study was performed. Paediatric patients with all subgroups of ALL (N = 3,054) transplanted between 2000 and 2012 were included. For children undergoing HSCT in CR1, the survival rates after TBI and chemoconditioning were not significantly different. For patients transplanted in CR2, the outcomes after TBI were superior to those after chemoconditioning with regard to leukaemia-free survival (LFS; 53.7 vs. 29.4%, respectively) and relapse incidence (30.6 vs. 49.3%, respectively) (16). The For Omitting Radiation Under Majority age (FORUM) trial—a large prospective international, randomized trial of HSCT in paediatric ALL—compared conditioning with TBI and etoposide to chemoconditioning regimens of busulfan or treosulfan in combination with fludarabine and thiotepa. This study found TBI-based conditioning to be associated with a significantly lower risk of relapse and treatment-related mortality (TRM) than either chemoconditioning regimen. In the Ph+ ALL group, TBI was superior to chemoconditioning with a 2-year EFS of 89 vs. 60%, respectively (13, 17). As a result, TBI prior to the HSCT is recommended for children ≥4 years of age with Ph+ ALL. However, TBI should be omitted in those of younger age (<4 years) due to its massive, toxic impact on the rapidly growing and developing child.
Optimal donor selection for HSCT in Ph+ ALL patients continues to be explored. An MSD is still the optimal donor but the optimal alternative donor source remains to be determined. Currently, the choices include unrelated umbilical cord blood, an MUD or mismatched unrelated donor (MMUD) or a haploidentical related donor. It has been suggested that umbilical cord blood may give a superior outcome compared to an unrelated adult donor (18) or at least a comparable outcome (19). At this time, it appears that all donor sources give similar results. One new approach has been the use of haploidentical HSCT to expand the donor availability, with strategies including in vivo T-cell depletion with post-transplant cyclophosphamide (PT-Cy) or ex vivo T-cell depletion (TCD) prior to HSCT.
In vivo depletion of the expanding, allo-reactive T cells with PT-Cy 48–72 h after transplant has been used in paediatric ALL of all subtypes (20, 21) with a reduction in both GvHD and graft rejection observed (22, 23). In adult ALL, there is no difference in the outcome between an MUD-HSCT and a PTCy haploidentical transplant (24), especially when using a TBI-containing conditioning regimen (25). The largest retrospective multicentre study on haploidentical HSCT to date analysed outcomes of 180 children with ALL after haploidentical HSCT using the PT-Cy modality (20). The estimated 2-year LFS was 65, 44, and 18.8% for patients transplanted in CR1, CR2, and CR3 or more, respectively, while 1-year LFS was 3% for those not in CR. The use of peripheral blood stem cells (PBSCs) was an independent factor associated with a decreased OS and higher NRM as opposed to bone marrow (20).
The other main approach to haploidentical HSCT is to perform ex vivo T-cell depletion prior to HSCT. Data on 343 patients with ALL who were <21 years old and who received their first allograft (αβ T-cell/B-cell depleted) after myeloablative conditioning in CR were analysed (26). The incidence of transplant-related complications was 6% with an MUD, 28% with an MMUD and 9% with a haploidentical graft. With a median follow-up of 3.3 years, the 5-year probability of LFS in the three groups was 67, 55, and 62%, respectively.
A review by Rahman and colleagues in the current Frontiers in Pediatrics supplement explores the different approaches to haploidentical HSCT in detail.
Currently, there is no evidence about which platform for haploidentical HSCT—PT-Cy or ex vivo T-cell depletion—is better, and no specific data on their use in Ph+/Ph-like ALL are available. A Spanish, multicentre, retrospective analysis of 192 children and adolescents with high-risk haematological malignancies compared the data of haploidentical HSCT using PT-Cy (n = 41) or ex vivo T-cell depletion (n = 151) in 10 centres between January 1999 and December 2016. The results of this study show that there are no statistical differences between the two approaches in terms of OS, DFS, GvHD-free, relapse-free survival, relapse, and TRM at day +100 (27).
The Role of the Graft-vs.-Leukaemia Effect in Ph+ ALL
The GvL effect is closely associated with GvHD. To date, there is no identified immune target specific to Ph+ ALL that can be used to predict the GvL effect beyond general criteria used in ALL such as the human leukocyte antigen (HLA) DP (28). However, the gene fusion BCR-ABL itself has been targeted with tumour-specific T-cell therapy (29). In the COG ASCT0431 study, the presence of grade I–III acute GvHD (aGvHD) was associated with a lower risk of relapse of B-ALL (30). This association was confirmed by the FORUM trial showing that a moderately severe aGvHD (grade II) was associated with a GvL effect (17). While the GvL effect may be achieved without GvHD, milder forms of both aGvHD and chronic GvHD (cGvHD) appear to be associated with an augmented GvL effect, with a greater impact by aGvHD for paediatric ALL (31–33).
In a large retrospective CIBMTR study, researchers examined the GvL effect as a function of GvHD in both children and adults. Among the 5,215 transplant recipients, 1,619 were paediatric ALL patients in CR1/CR2 (with 15 % Ph+), and 1,003 had advanced disease (15% with Ph+). According to this study, GvHD was associated with an enhanced GvL effect in ALL. The beneficial effect of GvHD-associated GvL on the OS was confirmed for both the adults and children in CR1/CR2 with low-grade aGvHD (hazard ratio [HR], 0.49–0.69), but not with cGvHD. In addition, a beneficial effect was shown in patients with advanced ALL and cGVHD with or without grade I or II aGvHD (reduction of mortality with HR, 0.83–0.76). The impact of pre-transplant MRD could not be evaluated as the MRD levels were unknown for 84% of patients (34).
A Japanese retrospective study on adult patients with Ph+ ALL failed to confirm the above CIBMTR study findings. The study evaluated 1,022 patients aged >15 years with Ph+ ALL who underwent HSCT to assess the impact of GvHD-associated GVL on the outcome of patients stratified by their MRD status. In contrast to the previous reports, the researchers did not observe a significantly better OS among those patients with a mild aGvHD or cGvHD regardless of MRD level (35).
What differentiates the treatment approach for Ph+ ALL from that used for other molecular subtypes of ALL is the addition of TKIs into induction therapy and, for some patients, also post-transplant. With use of post-transplant TKIs, their immunosuppressive effects become a consideration. The ability of TKIs to induce an immunomodulatory effect has been documented for T, NK and B cells. Also, regulatory T cell numbers are reduced among TKI-treated patients (36, 37). Pre-transplant TKIs increase the risk of infection, while post-transplant TKIs add to the immune suppression. The incidence and severity of cGvHD have been shown to be reduced by imatinib post HSCT (38).
The Role of HSCT in Treating Ph-like ALL
A large subgroup of patients with a similar gene expression profile to Ph+ ALL without the classic BCR-ABL fusion gene (i.e., Ph-like ALL) were reported in 2009 as having a high rate of relapse with conventional chemotherapeutic regimens (39). Yet, the blast cells of these patients had rearrangements similar to Ph+ ALL such as CRLF2 rearrangements, a JAK mutation or a variety of additional kinase alterations (ABL1, JAK2, PDGFRB, EPOR, IL7R, SH2B3, FLT3 etc.). The resulting chimeric proteins showed substantial tyrosine kinase activity, even in the absence of high ABL expression (40).
The role of HSCT as a therapy for Ph-like paediatric ALL is uncertain (13). Childhood leukaemia study groups have focused on augmenting chemotherapy in combination with either Janus kinase 2 (JAK2) specific drugs, such as ruxolitinib, or ABL/platelet-derived growth factor receptor (PDGF-R) inhibitors, such as imatinib or dasatinib. Whether Ph-like ALL is as immunogenic and responsive to the HSCT-mediated GvL effect as Ph+ ALL needs to be determined. A retrospective evaluation through the CIBMTR or EBMT databases is needed to establish the efficacy of HSCT for Ph-like ALL. If it is similar to that in either infant KMT2A-rearranged or hypodiploid ALL, and thus relatively resistant to the GvL effect offered by HSCT, the outcomes with TKI therapy may not be as good as those seen for Ph+ ALL. While early results are promising, the ability of the targeted JAK2 or ABL/PDGF-R inhibitors to attain an MRD-negative state pre HSCT, putatively also of key importance in this, novel subgroup, remains to be established. The potential use of TKI therapy post HSCT in Ph-like also needs to be evaluated urgently. Either way, HSCT for Ph-like ALL is probably an important approach to offer as “total” immune therapy for this subpopulation of paediatric patients with ALL.
The Role of MRD in HSCT for Ph+ and Ph-like ALL
Evaluation of treatment response in the form of sensitive MRD measurements in the post-induction period has been established as an indispensable tool for risk stratification in various ALL subtypes (41). The early European paediatric Ph+ ALL study, EsPhALL 2004, found that the achievement of MRD negativity after a consolidation phase resulted in a lower rate of relapse than that observed in patients with detectable MRD (5-year cumulative incidence of relapse: 14.3 vs. 35.3% respectively) (31). An end-of-consolidation MRD >5 × 10−4 or any MRD positivity at later timepoints stratifies patients into a high-risk arm to receive HSCT in CR1 in the current COG AALL1631/EsPhALL2017 trial. By contrast, the COG AALL0031 study using flow-cytometry–based MRD found that MRD positivity at the end of induction was not prognostic of outcome (4, 5).
In the next generation of international Ph+ ALL trials (AALL1631/EsPhALL2017 phase 3 trial), MRD measured by immunoglobulin (Ig) / T-cell receptor (TCR) real-time quantitative polymerase chain reaction (RQ-PCR) was selected as the primary method for measuring MRD (42). Although RQ-PCR quantification of genomic Ig/TCR and BCR-ABL RNA shows concordance (69% overall concordance in the EsPhALL2004 trial), BCR-ABL RQ-PCR remains more often positive at later timepoints, but without clear clinical significance, and appears to be less precise in predicting outcome (43). Use of BCR-ABL RQ-PCR was deemed impractical to measure MRD in the joint EsPhALL/ COG AALL1122 CA180-372 trial due to missing results caused by frequent, unmet assay requirements (44). The discordance between the Ig/TCR and BCR-ABL RQ-PCR results may be caused by the presence of BCR-ABL1 translocation in non-leukaemic myeloid or other cells, possibly due to a CML-like stem cell disease (45).
In the EsPhALL 2010 trial, nine (30%) of the 30 patients who were MRD negative at the end of consolidation and thus treated with imatinib plus chemotherapy relapsed vs. none of the 17 MRD-negative patients who underwent HSCT, similarly to EsPhALL 2004 (8). Thirty-three (37.8%) of the 87 MRD-negative patients treated with dasatinib plus chemotherapy in the EsPhALL/COG AALL1122 CA180-372 trial relapsed (44). This relapse rate of ≥30 % for the standard risk Ph+ ALL patients (MRD negative at the end of consolidation and no HSCT indication in CR1) suggests that the value of MRD negativity in Ph+ ALL for risk assessment is limited and differs from its role in the majority of the non-Ph+ ALL subtypes. Fortunately, a significant number of Ph+ ALL standard-risk patients can be salvaged after first relapse using TKI-containing chemotherapy regimens as bridging to HSCT (6, 8) (Figure 2).
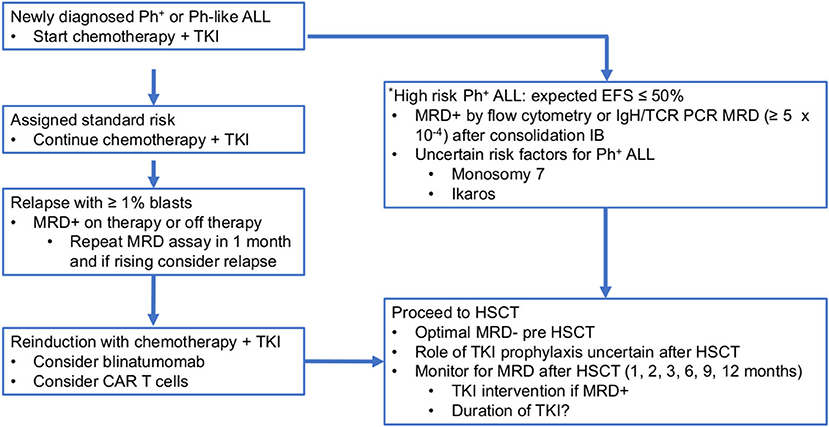
Figure 2. Proposed treatment algorithm for HSCT in paediatric Ph+ and Ph-like ALL. *There are no defined criteria for high-risk Ph-like ALL at present. ALL, acute lymphoblastic leukaemia; CAR, chimeric antigen receptor; HSCT, haematopoietic stem cell transplantation; IB, consolidation; MRD, minimal residual disease; Ph+, Philadelphia chromosome; TKI, tyrosine kinase inhibitor.
Negative MRD pre HSCT, as well as concurrent aGvHD, is predictive of a lower rate of relapse in paediatric patients with ALL overall (46, 47). This appears to be true as well for Ph+ ALL (5). The relapse rate post HSCT for patients assigned to HSCT in the EsPhALL 2010 was five of 15 (33%) (8). In the EsPhALL/COG AALL1122 CA180-372 trial it was four of 15 (44), a rate of relapse similar to other high-risk ALL patients undergoing HSCT for ALL in CR2. In the AALL0031 cohort, the 5-yr EFS rate for the MRD-negative patients after HSCT was 77% (5) and, interestingly, almost all patients in the EsPhALL2004 and EsPhALL/COG AALL1122 studies were Ig/TCR RQ-PCR negative or had low positivity before HSCT and had an excellent 5-yr EFS (86% in EsPhALL2004 and 91% in EsPhALL 2010). Thus, although MRD may not be as predictive for the outcome among patients receiving chemotherapy plus a TKI, it may be predictive for the HSCT outcomes (31). Moreover, the results of the AALL0622 study suggest that HSCT was able to abrogate the poor prognosis associated with MRD positivity at the end of consolidation (6).
The role of MRD monitoring for Ph+ ALL post HSCT is not well determined. The use of BCR-ABL PCR is uncertain and the results may come out as positive for a long time after HSCT and not predict relapse, at least not as previously described in adults (48). TCR-IgH PCR, flow cytometry or NGS are currently being utilized in several settings. While in CML peripheral blood BCR-ABL PCR correlates well with marrow measurements, evaluation of MRD in the marrow is still considered the standard for paediatric Ph+ ALL. Also uncertain is the optimal timing of MRD measurements after HSCT. Based on the high salvage rate of recurrent Ph+ ALL after chemotherapy plus TKI (6, 8), it is highly likely that patients who become MRD+ post HSCT will be reinduced into remission before a full relapse. In order to identify an early relapse post HSCT we recommend frequent monitoring of MRD after HSCT at 1, 2, 3, 6, 9, and 12 months after HSCT (c.f. Figure 2). These MRD evaluations may lead to a pre-emptive approach after HSCT although the level of MRD that should trigger the use of a TKI or another intervention is uncertain. Some experts have advised that a rise in MRD in measurements taken 2–4 weeks apart could be enough to launch a therapeutic intervention. Studies are needed to guide: (a) what method for the MRD measurement should be utilized; (b) what is an actionable “positive” MRD level; and (c) whether a TKI or other intervention is best.
Another unanswered question is for how long TKIs should be used pre-emptively in patients with MRD positivity. One year of treatment if MRD negativity is achieved is reasonable, with a close monitoring of the MRD once the TKI is discontinued. Another factor to consider is the impact of TKIs on haematopoiesis and immune responses, i.e., early TKI administration post HSCT (48) may require a lower dose than is standard. We expect that most clinicians would recommend imatinib as the preferred TKI to be used in a post-HSCT MRD-positive setting because it is the least marrow suppressive.
The role of HSCT for patients with BCR-ABL-like ALL is currently not known. Studies have been limited by data on the patients having a BCR-ABL-like translocation only recently being included in the data captured by the large HSCT databases of the CIBMTR and EBMT. Moreover, data on alternative immune therapies such as blinatumomab or CAR-T cell is only now being collected. It is reasonable to conclude that allogeneic HSCT is an excellent option for recurrent or refractory BCR-ABL-like ALL. Only through prospective clinical trials and retrospective analyses of the CIBMTR and EBMT databases with enough data will the relative efficacy of HSCT for this subtype of ALL be determined.
The Impact of TKIs Post HSCT in Ph+ HSCT
The post-HSCT use of TKIs in both adult and paediatric Ph+ ALL has not been studied in a controlled way. In an EBMT retrospective study in adult with Ph+ ALL, a multivariate analysis found prophylactic TKI to significantly improve the LFS (hazard ratio, 0.44; p = 0.002) and lower the relapse incidence (hazard ratio, 0.40; p = 0.01) (49). On the other hand, the only randomized trial of post-transplant TKI reported that prophylactic and pre-emptive use of imatinib is equally effective in preventing relapse after allogeneic HSCT (50). A recent systematic review of 17 trials showed that the use of TKIs after allogeneic HSCT for patients in CR1 improved the OS when given either as a prophylactic or pre-emptive regimen but were of no benefit in patients with Ph+ ALL in CR2 or higher (51). Similarly, a retrospective analysis on 850 adult patients by the Japan Society for HSCT concluded that TKI prophylaxis was not associated with a decreased risk of relapse or superior OS in either MRD-negative or -positive patients in CR1 at HSCT (52). Also of importance are the immunosuppressive effects of TKIs, as demonstrated by imatinib's efficacy as a salvage treatment for steroid refractory cGvHD (53). While the EBMT retrospective study found a lower incidence of relapse only with aGvHD (49), a smaller retrospective study found that post-HSCT TKI prophylaxis was associated with a reduction in cGvHD (38). As opposed to the adult studies described above, no studies have evaluated the impact of post-HSCT prophylaxis or pre-emptive therapy on relapse and GvHD in children.
When the TKIs are administered post HSCT, the optimal type, timing and duration remain to be decided for both the adult and paediatric patients. Limited data support the use of the newer generation TKIs for patients after HSCT (50, 51, 54). Examination of the mutational status and amplification of the ABL kinase gene is recommended in relapsed and non-responding patients. The initiation of TKI post HSCT requires a stable graft function to tolerate the myelosuppressive effect of the TKIs, usually seen from 2 months after HSCT (54). A reasonable duration of the TKI treatment is 6 months to 1 year of MRD negativity (51, 54). A retrospective analysis on the stopping of the TKIs post HSCT found that administration for more than 6 months tended to be associated with a superior relapse-free survival (55). Stopping TKIs post HSCT is often not a planned decision, as illustrated by a single prospective randomized trial on prophylactic vs. pre-emptive TKI post HSCT, where most patients in each group (67 and 71%) discontinued the treatment prematurely (48). Since the outcomes are similar for prophylactic vs. pre-emptive TKI therapy, the less-toxic pre-emptive strategy appears to be favourable but a strict MRD monitoring schedule needs to be implemented. The decision to use pre-emptive TKI therapy may be guided by an assessment of the pre- and post-HSCT relapse risk (51, 54). In conclusion, currently available data do not support the use of prophylactic TKI post HSCT. We recommend a pre-emptive approach based on the post-HSCT MRD analysis for those Ph+ ALL patients who are MRD negative at transplant (Figure 3).
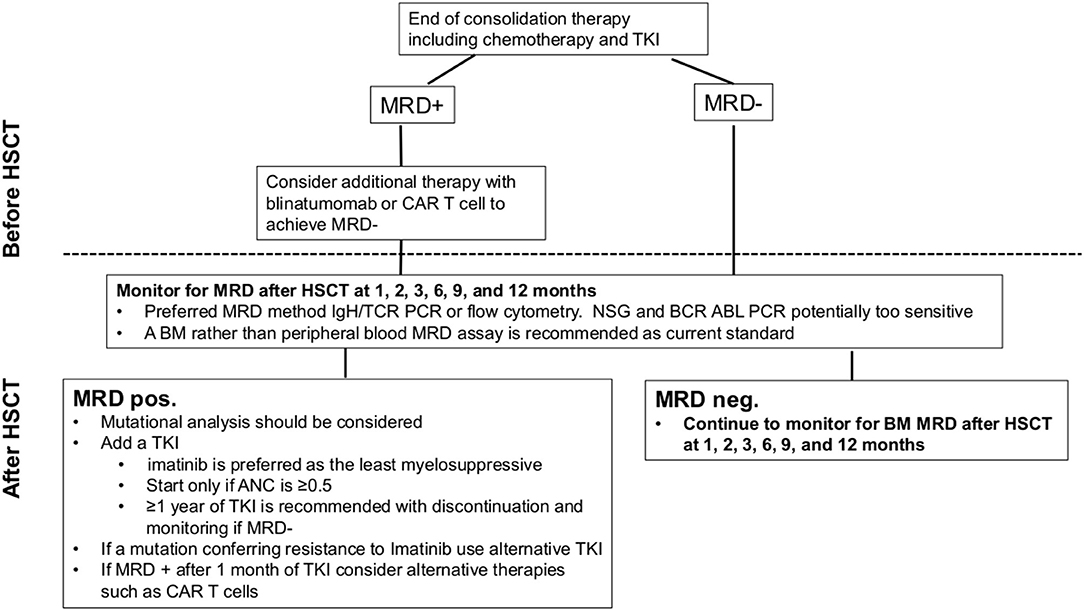
Figure 3. Our recommendations for the use of MRD to plan HSCT in paediatric Ph+ and Ph-like ALL. ANC, absolute neutrophil count; ALL, acute lymphoblastic leukaemia; BM, bone marrow; CAR, chimeric antigen receptor; HSCT, haematopoietic stem cell transplantation; IgH, immunoglobulin H; MRD, minimal residual disease; NGS, next-generation sequencing; PCR, polymerase chain reaction; Ph+, Philadelphia chromosome; TCR, T cell receptor; TKI, tyrosine kinase inhibitor.
Approaches to Persistent MRD Positivity After HSCT in Ph+ and Ph-like ALL
One of the biggest challenges for the HSCT physician is when a patient remains MRD positive post HSCT after a TKI is implemented. Other targeted agents may become more commonly used, especially when MRD positivity persists after the implementation of a TKI and there is no mutation to suggest TKI resistance.
The Role of Novel Immunotherapeutic Approaches in HSCT for Ph+ ALL
There are a number of targeted immune therapies that putatively will impact the role of HSCT in the treatment for high-risk Ph+ or Ph-like ALL in the paediatric population. One of the big questions to be answered is: “can HSCT be used to further improve outcomes in patients receiving a novel agent or can the novel immune therapies be used after HSCT to improve the outcome?”. The use of CAR T cells, blinatumomab or inotuzumab ozogamicin either to induce MRD negativity pre HSCT or as post HSCT prophylaxis or pre-emptive therapy remains to be elucidated. Their use in combination with TKIs may lead to novel approaches to achieve lower toxicity and higher efficacy in combination with HSCT.
Recommendations and Conclusions
Our recommendations for HSCT in paediatric patients with Ph+ and Ph-like ALL are shown in Table 2. In summary, HSCT continues to offer an important therapeutic option for r/r Ph+ ALL in children and adolescents. However, the role of HSCT in Ph-like ALL, if any, is not clear, and additional studies are needed to establish the role of HSCT in this high-risk subpopulation. The role of TKIs in combination with HSCT for Ph-like paediatric ALL also requires further study.
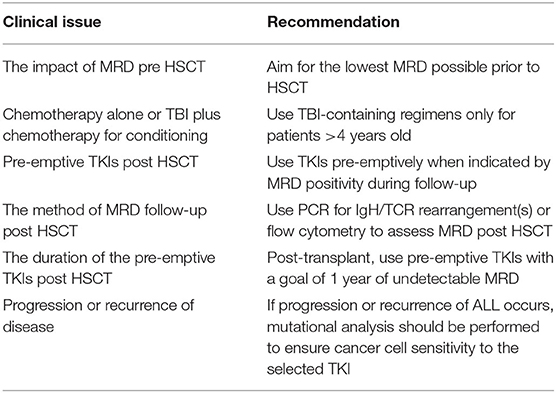
Table 2. Key recommendations for the use of HSCT in paediatric Ph+ and Ph-like ALL.
Optimal outcomes of HSCT for Ph+ ALL require the use of conditioning regimens with the lowest possible toxicity to establish MRD negativity pre HSCT, but should include TBI. Outcomes are similar for all donor sources. A better GvL effect may be achieved if either a low-grade aGvHD or cGvHD occurs after HSCT.
Routine MRD measurement are needed after HSCT and probably best performed by PCR for the IgH/TCR rearrangements or NGS rather than BCR-ABL PCR testing (56). There are currently no established data to support the consistent use of prophylactic TKIs post HSCT and, consequently, a pre-emptive approach based on close MRD monitoring post HSCT is probably the less toxic approach.
Author Contributions
All authors listed have made a substantial, direct, and intellectual contribution to the work and approved it for publication.
Funding
This study received funding from the St. Anna Children's Cancer Research Institute, Vienna, Austria. The funders were not involved in the study design, collection, analysis, interpretation of data, the writing of this article, or the decision to submit it for publication.
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's Note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Acknowledgments
Editorial support in the preparation of this manuscript was provided by Hannah Bridges of HB Health Comms Limited.
References
1. Moorman A. The clinical relevance of chromosomal and genomic abnormalities in B-cell precursor acute lymphoblastic leukemia. Blood Rev. (2012) 26:123–35. doi: 10.1016/j.blre.2012.01.001
2. Arico M, Schrappe M, Hunger SP, Carroll WL, Conter V, Galimberti S, et al. Clinical outcome of children with newly diagnosed Philadelphia chromosome-positive acute lymphoblastic leukemia treated between 1995 and 2005. J Clin Oncol. (2010) 31:4755–61. doi: 10.1200/JCO.2010.30.1325
3. Cario G, Leoni V, Conter V, Baruchel A, Schrappe M, Biondi A. BCR-ABL1-like acute lymphoblastic leukemia in childhood and targeted therapy. Haematologica. (2020) 9:2200–4. doi: 10.3324/haematol.2018.207019
4. Schultz KR, Bowman WP, Aledo A, Slayton WB, Sather H, Devidas M, et al. Improved early event-free survival with imatinib in Philadelphia chromosome-positive acute lymphoblastic leukemia: a Children's Oncology Group study. J Clin Oncol. (2009) 27:5185–81. doi: 10.1200/JCO.2008.21.2514
5. Schultz KR, Carroll A, Heerema NA, Bowman WP, Aledo A, Slayton WB, et al. Long-term follow-up of imatinib in pediatric Philadelphia chromosome-positive acute lymphoblastic leukemia: Children's Oncology Group study AALL0031. Leukemia. (2014) 28:1467–71. doi: 10.1038/leu.2014.30
6. Slayton WB, Schultz KR, Kairalla JA, Devidas M, Mi X, Pulsipher MA, et al. Dasatinib plus intensive chemotherapy in children, adolescents, and young adults with Philadelphia chromosome-positive acute lymphoblastic leukemia: Results of Children's Oncology Group trial AALL0622. J Clin Oncol. (2018) 36:2306–14. doi: 10.1200/JCO.2017.76.7228
7. Pui CH, Yang JJ, Hunger SP, Pieters R, Schrappe M, Biondi A, et al. Childhood acute lymphoblastic leukemia: Progress through collaboration. J Clin Oncol. (2015) 33:2938–48. doi: 10.1200/JCO.2014.59.1636
8. Biondi A, Gandemer V, De Lorenzo P, Cario G, Campbell M, Castor A, et al. Imatinib treatment of paediatric Philadelphia chromosome-positive acute lymphoblastic leukemia (EsPhALL2010): a prospective, intergroup, open-label, single-arm clinical trial. Lancet Haematol (2018) 5:e641–52. doi: 10.1016/S2352-3026(18)30173-X
9. Moorman A. New and emerging prognostic and predictive genetic biomarkers in B-cell precursor acute lymphoblastic leukemia. Haematologica. (2016) 101:407–16. doi: 10.3324/haematol.2015.141101
10. Biondi A, Schrappe M, De Lorenzo P, Castor A, Lucchini G, Gandemer V, et al. Imatinib after induction for treatment of children and adolescents with Philadelphia-chromosome-positive acute lymphoblastic leukaemia (EsPhALL): A randomised, open-label, intergroup study. Lancet Oncol. (2012) 13:936–45. doi: 10.1016/S1470-2045(12)70377-7
11. Shen S, Chen X, Cai J, Yu J, Gao J, Hu S, et al. Effect of dasatinib vs imatinib in the treatment of pediatric Philadelphia chromosome-positive acute lymphoblastic leukemia: a randomized clinical trial. JAMA Oncol. (2020) 6:358–66. doi: 10.1001/jamaoncol.2019.5868
12. Hunger S, Saha V, Devidas M, Valsecchi M, Gastier-Foster J, Cazzaniga G, et al. Final results of CA180-372/COG AALL1122 phase 2 trial of dasatinib and chemotherapy in pediatric patients with newly-diagnosed Philadelphia chromosome positive acute lymphoblastic leukemia (PH plus ALL). Pediatr Blood Cancer. (2020) 67:S15–6.
13. Tasian SK, Peters C. Targeted therapy or transplantation for paediatric ABL-class Ph-like acute lymphocytic leukaemia? Lancet Haematol. (2020) 7:e858–9. doi: 10.1016/S2352-3026(20)30369-0
14. Friend BD, Bailey-Olson M, Melton A, Shimano KA, Kharbanda S, Higham C, et al. The impact of total body irradiation-based regimens on outcomes in children and young adults with acute lymphoblastic leukemia undergoing allogeneic hematopoietic stem cell transplantation. Pediatr Blood Cancer. (2020) 67:e28079. doi: 10.1002/pbc.28079
15. Dalle J-H, Balduzzi A, Bader P, Pieczonka A, Yaniv I, Lankester A, et al. The impact of donor type on the outcome of pediatric patients with very huge risk acute lymphoblastic leukemia. A study of the ALL SCT 2003 BFM-SG and 2007-BFM-International SG. Bone Marrow Transpl. (2021) 56:257–66. doi: 10.1038/s41409-020-01014-x
16. Willasch AM, Peters C, Sedláček P, Dalle JH, Kitra-Roussou V, Yesilipek A. et al. Myeloablative conditioning for allo-HSCT in pediatric ALL: FTBI or chemotherapy?—A multicenter EBMT-PDWP study. Bone Marrow Transplant. (2020) 55:1540–51. doi: 10.1038/s41409-020-0854-0
17. Peters C, Dalle JH, Locatelli F, Poetschger U, Sedlacek P, Buechner J, et al. Total body irradiation or chemotherapy conditioning in childhood ALL: a multinational, randomized, noninferiority phase III study. J Clin Oncol. (2021) 39:295–307. doi: 10.1200/JCO.20
18. Onishi Y, Sasaki O, Ichikawa S, Inokura K, Katsuoka Y, Ohtsuka Ohba R, et al. Favorable outcome of unrelated cord blood transplantation for Philadelphia chromosome-positive acute lymphoblastic leukemia. Biol Blood Marrow Transpl. (2011) 17:1093–7. doi: 10.1016/j.bbmt.2011.01.010
19. Konuma T, Kato S, Ooi J, Oiwa-Monna M, Tojo A, Takahashi S. Myeloablative unrelated cord blood transplantation for Philadelphia chromosome-positive acute lymphoblastic leukemia: comparison with other graft sources from related and unrelated donors. Ann Hematol. (2015) 94:289–96. doi: 10.1007/s00277-014-2195-9
20. Ruggeri A, Galimard JE, Paina O, Fagioli F, Tbakhi A, Yesilipek A, et al. Outcomes of unmanipulated haploidentical transplantation using post-transplant cyclophosphamide (PT-Cy) in pediatric patients with acute lymphoblastic leukemia. Transplant Cell Ther. (2021) 27:424e1–9. doi: 10.1016/j.jtct.2021.01.016
21. Klein OR, Buddenbaum J, Tucker N, Chen AR, Gamper CJ, Loeb D, et al. Nonmyeloablative haploidentical bone marrow transplantation with post-transplantation cyclophosphamide for pediatric and young adult patients with high-risk hematologic malignancies. Biol Blood Marrow Transpl. (2017) 23:325–32. doi: 10.1016/j.bbmt.2016.11.016
22. Luznik L, O'Donnell PV, Symons HJ, Chen AR, Leffell MS, Zahurak M, et al. HLA-haploidentical bone marrow transplantation for hematologic malignancies using nonmyeloablative conditioning and high-dose, posttransplantation cyclophosphamide. Biol Blood Marrow Transpl. (2008) 14:641–50. doi: 10.1016/j.bbmt.2008.03.005
23. Raiola AM, Dominietto A, Ghiso A, Di Grazia C, Lamparelli T, Gualandi F, et al. Unmanipulated haploidentical bone marrow transplantation and posttransplantation cyclophosphamide for hematologic malignancies after myeloablative conditioning. Biol Blood Marrow Transpl. (2013) 19:117–22. doi: 10.1016/j.bbmt.2012.08.014
24. Sanz J, Galimard JE, Labopin M, Afanasyev B, Angelucci E, Ciceri F, et al. Post-transplant cyclophosphamide after matched sibling, unrelated and haploidentical donor transplants in patients with acute myeloid leukemia: a comparative study of the ALWP EBMT. J Hematol Oncol. (2020) 13:46. doi: 10.1186/s13045-020-00882-6
25. Dholaria B, Savani BN, Hamilton BK, Oran B, Liu HD, Tallman MS, et al. Hematopoietic cell transplantation in the treatment of newly diagnosed adult acute myeloid leukemia: an evidence-based review from the American Society of Transplantation and Cellular Therapy. Transplant Cell Ther. (2021) 27:6–20. doi: 10.1016/j.bbmt.2020.09.020
26. Bertaina A, Zecca M, Buldini B, Sacchi N, Algeri M, Saglio F, et al. Unrelated donor vs HLA-haploidentical (α/β) T-cell- and B-cell-depleted HSCT in children with acute leukemia. Blood. (2018) 132:2594–607. doi: 10.1182/blood-2018-07-861575
27. Perez-Martinez A, Ferreras C, Pascual A, Gonzalez-Vicent M, Alonso A, Badell I, et al. Haploidentical transplantation in high-risk pediatric leukemia: a retrospective comparative analysis on behalf of the Spanish working Group for bone marrow transplantation in children (GETMON) and the Spanish Group for hematopoietic transplantation (GETH). Am J Hematol. (2020) 95:28–37. doi: 10.1002/ajh.25661
28. van Besien KW, Orfali N. Alternative donor transplantation for lymphoid malignancies: How far have we come? J Clin Oncol. (2020) 129:582–6. doi: 10.1200/JCO.20.00177
29. Comoli P, Basso S, Riva G, Barozzi P, Guido I, Gurrado A, et al. BCR-ABL-specific T-cell therapy in Ph+ ALL patients on tyrosine-kinase inhibitors. Blood. (2017) 129:582–6. doi: 10.1182/blood-2016-07-731091
30. Pulsipher MA, Langholz B, Wall DA, Schultz KR, Bunin N, Carroll WL, et al. A randomized trial of sirolimus-based graft versus host disease (GVHD) prophylaxis after hematopoietic stem cell transplantation (HSCT) in selected patients with CR1 and CR2 ALL: results from Children's Oncology Group Study ASCT0431. Blood. (2014) 123:2017–25. doi: 10.1182/blood-2013-10-534297
31. Cazzaniga G, De Lorenzo P, Alten J, Röttgers S, Hancock J, Saha V, et al. Predictive value of minimal residual disease in Philadelphia-chromosome-positive acute lymphoblastic leukemia treated with imatinib in the European intergroup study of post-induction treatment of Philadelphia-chromosome-positive acute lymphoblastic leukemia, based on immunoglobulin/T-cell receptor and BCR/ABL1 methodologies. Haematologica. (2018) 103:107–15. doi: 10.3324/haematol.2017.176917
32. Stern M, de Wreede LC, Brand R, van Biezen A, Dreger P, Mohty M, et al. (2014). Sensitivity of hematological malignancies to graft-versus-host effects: an EBMT megafile analysis. Leukemia. (2014) 28:2235–40. doi: 10.1038/leu.2014.145
33. Kataoka I, Kami M, Takahashi S, Kodera Y, Miyawaki S, Hirabayashi N, et al. Clinical impact of graft-versus-host disease against leukemias not in remission at the time of allogeneic hematopoietic stem cell transplantation from related donors. The Japan society for hematopoietic cell transplantation working party. Bone Marrow Transpl. (2004) 34:711–9. doi: 10.1038/sj.bmt.1704659
34. Yeshurun M, Weisdorf D, Rowe JM, Tallman MS, Zhang MJ, Wang HL, et al. The impact of the graft-versus-leukemia effect on survival in acute lymphoblastic leukemia. Blood Adv. (2019) 3:670–80. doi: 10.1182/bloodadvances.2018027003
35. Akahoshi Y, Igarashi A, Fukuda T, Uchida N, Tanaka M, Ozawa Y, et al. Impact of graft-versus-host disease and graft-versus-leukemia effect based on minimal residual disease in Philadelphia chromosome-positive acute lymphoblastic leukemia. Br J Haematol. (2020) 190:84–92. doi: 10.1111/bjh.16540
36. Steegmann JL, Cervantes F, le Coutre P, Porkka K, Saglio G. Off-target effects of BCR-ABL1 inhibitors and their potential long-term implications on patients with chronic myeloid leukemia. Leuk Lymphoma. (2012) 53:2351–61. doi: 10.3109/10428194.2012.695779
37. Hayashi Y, Nakamae H, Katayama T, Nakane T, Koh H, Nakamae M, et al. Different immunoprofiles in patients with chronic myeloid leukemia treated with imatinib, nilotinib or dasatinib. Leuk Lymphoma. (2012) 53:1084–9. doi: 10.3109/10428194.2011.647017
38. Nakasone H, Kanda Y, Takasaki H, Nakaseko C, Sakura T, Fujisawa S, et al. Prophylactic impact of imatinib administration after allogeneic stem cell transplantation on the incidence and severity of chronic graft versus host disease in patients with Philadelphia chromosome-positive leukemia. Leukemia. (2010) 24:1236–9. doi: 10.1038/leu.2010.83
39. den Boer ML, van Slegtenhorst M, De Menezes RX, Cheok MH, Buijs-Gladdines JGCAM, Peters STCJM, et al. A subtype of childhood acute lymphoblastic leukaemia with poor treatment outcome: a genome-wide classification study. Lancet Oncol. (2009) 10:125–34. doi: 10.1016/S1470-2045(08)70339-5
40. den Boer ML, Cario G, Moorman AV, Boer JM, de Groot-Kruseman HA, Fiocco M, et al. Outcomes of paediatric patients with B-cell acute lymphocytic leukemia with ABL-class fusion in the pre-tyrosine-kinase inhibitor era: a multicentre, retrospective, cohort study. Lancet Haematol. (2021) 8:e55–66. doi: 10.1016/S2352-3026(20)30353-7
41. Bader P, Kreyenberg H, von Stackelberg A, Eckert C, Salzmann-Manrique E, Meisel R, et al. Monitoring of minimal residual disease after allogeneic stem-cell transplantation in relapsed childhood acute lymphoblastic leukemia allows for the identification of impending relapse: results of the ALL-BFM-SCT 2003 trial. J Clin Oncol. (2015) 33:1275–84. doi: 10.1200/JCO.2014.58.4631
42. Slayton WB, Shultz KR, Silverman LB, Hunger SP. How we approach Philadelphia chromosome-positive acute lymphoblastic leukemia in children and young adults. Ped Blood Cancer. (2020) 67:e28543. doi: 10.1002/pbc.28542
43. Ladetto M, Bruggemann M, Monitillo L, Ferrero S, Pepin F, Drandi D, et al. Next-generation sequencing and real-time quantitative PCR for minimal residual disease detection in B-cell disorders. Leukemia. (2014) 28:1299–307. doi: 10.1038/leu.2013.375
44. Reshmi S, Stonerock E, Borowitz M, Geese WJ, Healey D, Gastier-Foster JM, et al. International laboratory comparison of methodologies for determining minimal residual disease (MRD) in childhood Philadelphia chromosome-positive acute lymphoblastic leukemia (Ph+ ALL). Blood. (2015) 126:2612. doi: 10.1182/blood.V126.23.2612.2612
45. Hovorkova L, Zaliova M, Venn NC, Bleckmann K, Trkova M, Potuckova E, et al. Monitoring of childhood ALL using BCR-ABL1 genomic breakpoints identifies a subgroup with CML-like biology. Blood. (2017) 129:2771–81. doi: 10.1182/blood-2016-11-749978
46. Pulsipher MA, Wayne AS, Shultz KR. New frontiers in pediatric allo-SCT: Novel approaches for children and adolescents with ALL. Bone Marrow Transpl. (2014) 49:1259–65. doi: 10.1038/bmt.2014.114
47. Bader P, Salzmann-Manrique E, Balduzzi A, Dalle J-H, Woolfrey AE, Bar M, et al. More precisely defining risk peri-HCT in pediatric ALL: pre- vs post-MRD measures, serial positivity, and risk modeling. Blood Adv. (2019) 3:3393–405. doi: 10.1182/bloodadvances.2019000449
48. Carpenter PA, Snyder DS, Flowers ME, Sanders JE, Gooley TA, Martin PJ, et al. Prophylactic administration of imatinib after hematopoietic cell transplantation for high-risk Philadelphia chromosome–positive leukemia. Blood. (2007) 109:2791–3. doi: 10.1182/blood-2006-04-019836
49. Brissot E, Labopin M, Beckers MM, Socie G, Rambaldi A, Volin L, et al. Tyrosine kinase inhibitors improve long-term outcome of allogeneic hematopoietic stem cell transplantation for adult patients with Philadelphia chromosome positive acute lymphoblastic leukemia. Haematologica. (2015) 100:392–9. doi: 10.3324/haematol.2014.116954
50. Pfeifer H, Wassmann B, Bethge W, Dengler J, Bornhäuser M, Stadler M, et al. Randomized comparison of prophylactic and minimal residual disease-triggered imatinib after allogeneic stem cell transplantation for BCR-ABL1-positive acute lymphoblastic leukemia. Leukemia. (2013) 27:1254–62. doi: 10.1038/leu.2012.352
51. Warraich Z, Tenneti P, Thai T, Hubben A, Amin H, McBride A, et al. Relapse prevention with tyrosine kinase inhibitors after allogeneic transplantation for Philadelphia chromosome-positive acute lymphoblastic leukemia: a systematic review. Biol Blood Marrow Transplant. (2020) 26:e55–64. doi: 10.1016/j.bbmt.2019.09.022
52. Akahoshi Y, Nishiwaki S, Mizuta S, Ohashi K, Uchida N, Tanaka M, et al. Tyrosine kinase inhibitor prophylaxis after transplant for Philadelphia chromosome-positive acute lymphoblastic leukemia. Cancer Sci. (2019) 110:3255–66. doi: 10.1111/cas.14167
53. Olivieri A, Locatelli F, Zecca M, Sanna A, Cimminiello M, Raimondi R, et al. Imatinib for refractory chronic graft-versus-host disease with fibrotic features. Blood. (2009) 114:709–18. doi: 10.1182/blood-2009-02-204156
54. Giebel S, Czyz A, Ottmann O, Baron F, Brissot E, Ciceri F, et al. Use of tyrosine kinase inhibitors to prevent relapsed after allogeneic hematopoietic stem cell transplantation for patients with Philadelphia chromosome-positive acute lymphoblastic leukemia: a position statement of the Acute Leukemia Working Party of the EBMT. Cancer. 122:2941–51. doi: 10.1002/cncr.30130
55. Nakasone H, Kako S, Mori T, Takahashi S, Onizuka M, Fujiwara SI, et al. Stopping tyrosine kinase inhibitors started after allogeneic HCT in patients with Philadelphia chromosome-positive leukemia. Bone Marrow Transpl. (2021) 56:1402–12. doi: 10.1038/s41409-020-01206-5
Keywords: haematopoietic stem cell transplantation, tyrosine kinase inhibitors, Philadelphia chromosome, acute lymphoblastic leukaemia, BCR-ABL-like ALL, graft-vs.-host disease, graft-vs.-leukaemia effect
Citation: Vettenranta K, Dobsinska V, Kertész G, Svec P, Buechner J and Schultz KR (2022) What Is the Role of HSCT in Philadelphia-Chromosome–Positive and Philadelphia-Chromosome–Like ALL in the Tyrosine Kinase Inhibitor Era? Front. Pediatr. 9:807002. doi: 10.3389/fped.2021.807002
Received: 01 November 2021; Accepted: 16 December 2021;
Published: 02 February 2022.
Edited by:
Christina Peters, St. Anna Children's Cancer Research Institute (CCRI), AustriaReviewed by:
Sarah K. Tasian, Children's Hospital of Philadelphia, United StatesAlix Eden Seif, Children's Hospital of Philadelphia, United States
Copyright © 2022 Vettenranta, Dobsinska, Kertész, Svec, Buechner and Schultz. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Kim Vettenranta, a2ltLnZldHRlbnJhbnRhQGh1cy5maQ==