 Elke Wühl1*
Elke Wühl1* Javier Calpe2
Javier Calpe2 Dorota Drożdż3
Dorota Drożdż3 Serap Erdine4
Serap Erdine4 Fernando Fernandez-Aranda5,6
Fernando Fernandez-Aranda5,6 Adamos Hadjipanayis7,8*
Adamos Hadjipanayis7,8* Peter F. Hoyer9
Peter F. Hoyer9 Augustina Jankauskiene10
Augustina Jankauskiene10 Susana Jiménez-Murcia5,6
Susana Jiménez-Murcia5,6 Mieczysław Litwin11
Mieczysław Litwin11 Giuseppe Mancia12
Giuseppe Mancia12 Artur Mazur13
Artur Mazur13 Denes Pall14
Denes Pall14 Tomas Seeman15,16
Tomas Seeman15,16 Manish D. Sinha17
Manish D. Sinha17 Giacomo Simonetti18
Giacomo Simonetti18 Stella Stabouli19
Stella Stabouli19 Empar Lurbe6,20*
Empar Lurbe6,20*
- 1Division of Pediatric Nephrology, Center for Pediatric and Adolescent Medicine, Heidelberg University Hospital, Heidelberg, Germany
- 2Analog Devices, Inc., Paterna, Spain
- 3Department of Pediatric Nephrology and Hypertension, Pediatric Institute, Jagiellonian University Medical College, Cracow, Poland
- 4Istanbul University-Cerrahpaşa, Cerrahpaşa Faculty of Medicine, Istanbul, Turkey
- 5University Hospital of Bellvitge-IDIBELL and Department of Clinical Sciences, University of Barcelona, Barcelona, Spain
- 6CIBER Fisiopatología de Obesidad y Nutrición (CIBEROBN), Instituto de Salud Carlos III, Madrid, Spain
- 7School of Medicine, European University Cyprus, Nicosia, Cyprus
- 8Department of Paediatrics, Larnaca General Hospital, Larnaca, Cyprus
- 9Klinik für Kinderheilkunde II, Zentrum für Kinder und Jugendmedizin, Universitätsklinikum Essen, Universität Duisburg-Essen, Essen, Germany
- 10Pediatric Center, Institute of Clinical Medicine, Vilnius University, Vilnius, Lithuania
- 11Department of Nephrology and Arterial Hypertension, The Children's Memorial Health Institute, Warsaw, Poland
- 12University of Milano-Bicocca, Milano, Italy
- 13Institute of Medical Sciences, Medical College, Rzeszów University, Rzeszow, Poland
- 14Department of Medical Clinical Pharmacology and Department of Medicine, University of Debrecen, Debrecen, Hungary
- 15Division of Pediatric Nephrology, University Children's Hospital, Charles University, Prague, Czech Republic
- 16Department of Pediatrics, University Hospital Ostrava, Ostrava, Czech Republic
- 17Department of Pediatric Nephrology, Evelina London Children's Hospital, Guys and St Thomas’ NHS Foundation Trust, London, United Kingdom
- 18Institute of Pediatrics of Southern Switzerland, Ente Ospedaliero Cantonale (EOC), Bellinzona, Switzerland
- 191st Department of Pediatrics, Aristotle University of Thessaloniki, Hippokratio General Hospital of Thessaloniki, Thessaloniki, Greece
- 20Department of Pediatric, Consorcio Hospital General, University of Valencia, Valencia, Spain
The joint statement is a synergistic action between HyperChildNET and the European Academy of Pediatrics about the diagnosis and management of hypertension in youth, based on the European Society of Hypertension Guidelines published in 2016 with the aim to improve its implementation. Arterial hypertension is not only the most important risk factor for cardiovascular morbidity and mortality, but also the most important modifiable risk factor. Early hypertension-mediated organ damage may already occur in childhood. The duration of existing hypertension plays an important role in risk assessment, and structural and functional organ changes may still be reversible or postponed with timely treatment. Therefore, appropriate therapy should be initiated in children as soon as the diagnosis of arterial hypertension has been confirmed and the risk factors for hypertension-mediated organ damage have been thoroughly evaluated. Lifestyle measures should be recommended in all hypertensive children and adolescents, including a healthy diet, regular exercise, and weight loss, if appropriate. If lifestyle changes in patients with primary hypertension do not result in normalization of blood pressure within six to twelve months or if secondary or symptomatic hypertension or hypertension-mediated organ damage is already present, pharmacologic therapy is required. Regular follow-up to assess blood pressure control and hypertension-mediated organ damage and to evaluate adherence and side effects of pharmacologic treatment is required. Timely multidisciplinary evaluation is recommended after the first suspicion of hypertension. A grading system of the clinical evidence is included.
Introduction
The joint statement is a synergistic action between HyperChildNET and the European Academy of Pediatrics about the diagnosis and management of hypertension in youth, based on the European Society of Hypertension Guidelines published in 2016 with the aim to improve its implementation. The grading system of the clinical evidence reads as follows:
A Recommendations are based on randomized trials (or systematic reviews of trials) with high levels of internal validity and statistical precision, provided that the trial results can be directly applied to the patients because of similar clinical characteristics and outcomes have clinical relevance.
B Recommendations are based on randomized trials, systematic reviews, or prespecified subgroup analyses that have lower levels of precision, or need to extrapolate from studies in different populations or using validated intermediate/surrogate outcomes.
C Recommendations are based on trials that have lower levels of internal validity and/or precision, trials for which non validated surrogate outcomes were used, or results from observational studies.
D Recommendations are based on expert opinion alone.
Arterial hypertension (HTN) is the most important risk factor for cardiovascular (CV) morbidity and mortality. The duration of existing HTN also plays a role in risk assessment.
Therefore, just as in adults, appropriate therapy should be initiated in children after the diagnosis of arterial HTN is confirmed and risk factors for hypertension-mediated organ damage (HMOD) are thoroughly assessed.
In all hypertensive children and adolescents, lifestyle interventions incorporating a healthy diet, regular exercise, and weight reduction, if necessary, should be recommended. If this does not lead to normalization of blood pressure (BP) within 6 to 12 months in patients with primary HTN, or if secondary or symptomatic HTN, or HMOD is already present, pharmacological therapy is required. The choice of medication should take into account the cause of HTN. In most cases, blockade of the renin-angiotensin system is recommended as first-line therapy. Combination therapy may be required to optimize BP control, especially in patients with secondary HTN.
Regular follow-up to evaluate BP control and HMOD, and to assess adherence to therapy and side effects of the pharmacological treatment is required.
Early referral to a childhood HTN center, ideally following initial suspicion of HTN, is encouraged to facilitate timely multidisciplinary input including cardiological and nephrological evaluation. The age of transfer to adult care services should be flexible upon patient readiness and specific needs.
Initial work-up of the hypertensive child
Patient history
Assessment of patient history should include pre- and postnatal history and a thorough assessment of patient family history including potential risk factors for hypertension, cardiovascular and cerebrovascular disease (1).
In the following materials we present assessment of patient and family history for hypertension and cardiovascular risk factors (Table 1).
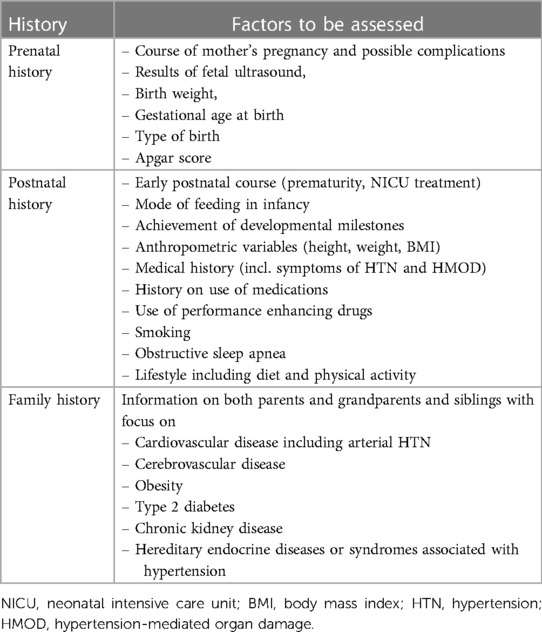
Table 1. Assessment of patient and family history for hypertension and cardiovascular risk factors.
Physical examination
Routine pediatric examination with special attention to anthropometric parameters is necessary (1) (Table 2).
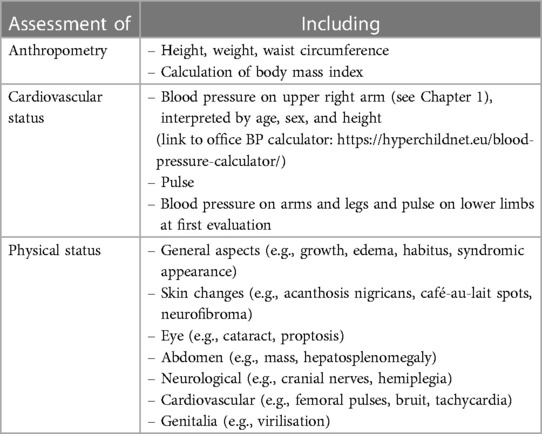
Table 2. Physical examination of hypertensive children and adolescents for underlying diseases and additional cardiovascular risk factors.
Laboratory evaluation and ultrasound
Laboratory tests should focus on kidney function and CV risk factors (Table 3).
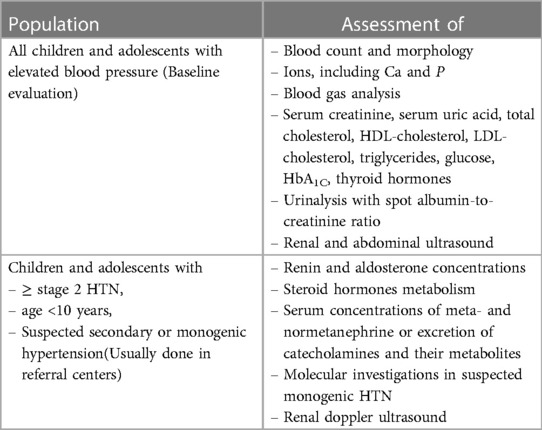
Table 3. Recommended evaluation in children and adolescents with hypertension.
Other imaging studies are usually performed in children in whom despite first step work-up, etiology of arterial HTN remains unestablished and/or in whom secondary HTN is suspected and done in referential centers (1).
When and how to assess the presence of hypertension-mediated organ damage
The main marker of HMOD is left ventricular hypertrophy (LVH) assessed by echocardiography (ECHO) (Table 4). In children up to 16 years left ventricular mass index (LVMI) should be indexed to height2.7 in meters (5).
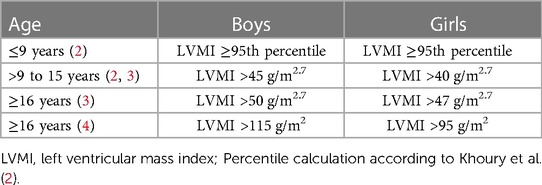
Table 4. Definitions of left ventricular hypertrophy (LVH) by age and sex.
In Table 5 we present recommendation when and how to assess the presence of hypertension-mediated organ damage.
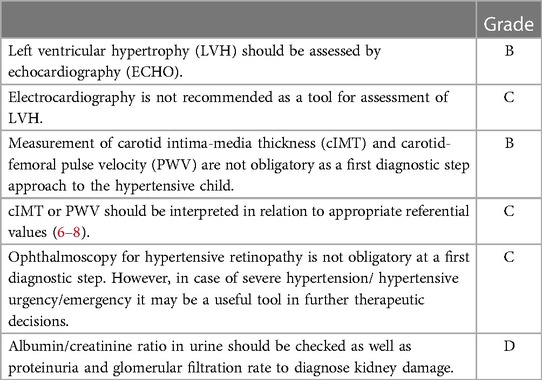
Table 5. Recommendation when and how to assess the presence of hypertension-mediated organ damage.
Treatment
Lifestyle changes
Lifestyle interventions incorporating a dietary component along with exercise or behavioural therapy can lead to improvements in both weight and cardiometabolic factors, including BP in overweight and obese children (1) (Box 1, Table 6).
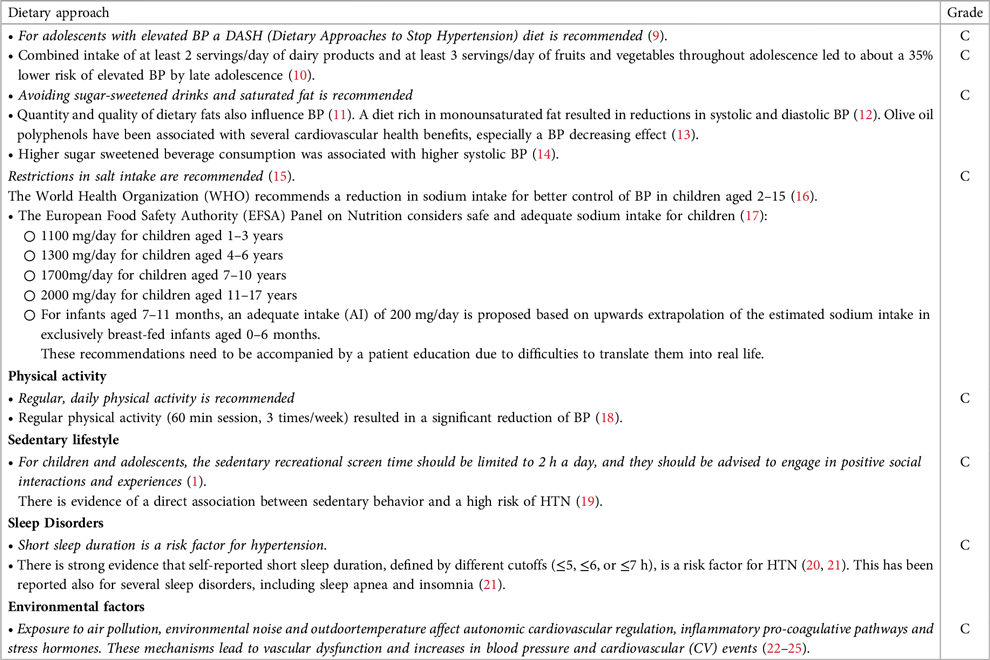
BOX 1. Lifestyle interventions for blood pressure reduction.
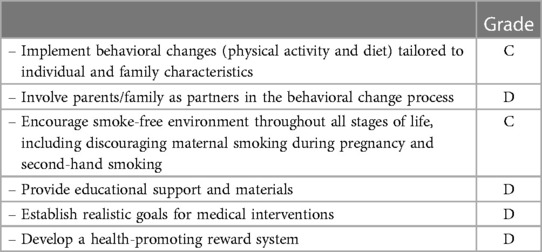
Table 6. Lifestyle recommendations to reduce high blood pressure values: goals.
There is a consensus in the literature that non-pharmacological treatment of adolescent HTN is important because lifestyle modification leads to a reduction in BP (26). However, the results of several trials confirmed that a single factor is rarely capable of controlling an elevated BP and that combined lifestyle interventions (dietary component, physical activity and behavioral therapy) accomplish the most effective reduction in BP. A personalized approach may increase the overall moderate success rate of lifestyle changes.
Pharmacological treatment
When to start
The decision to start pharmacological antihypertensive treatment in a child should not be based on BP level alone but also on the symptoms and comorbidities of the child, the etiology and duration of HTN and the presence of HMOD (Table 7).
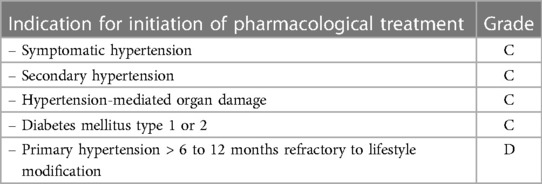
Table 7. Indications for initiation of pharmacological treatment.
It should be made clear that, unlike in adults, these recommendations are not based on randomized controlled trials showing that treatment-induced reduction in BP is associated with decreased cardiovascular morbidity and mortality. There are no mortality studies in pediatrics and they will never be performed because cardiovascular mortality in the pediatric population is negligible. However, several uncontrolled studies have shown that antihypertensive drug therapy in children is associated with a reduction in HMOD, such as left ventricular hypertrophy or microalbuminuria.
Choice of antihypertensive drugs
In contrast to adults, there are no large comparative studies on different classes of antihypertensive drugs in children. One exception is a small short-term study comparing the angiotensin receptor blocker (ARB) valsartan with the angiotensin converting enzyme -inhibitor (ACEi) enalapril, which demonstrated similar antihypertensive efficacy and adverse effects of these two agents blocking the renin-angiotensin-aldosterone system (RAAS) (27). A Cochrane review found 21 randomized controlled trials, usually of short duration and without placebo control groups. Most studies showed BP lowering effects of antihypertensive drugs without severe adverse effects (Grade B) (28). However, no pediatric randomized controlled trials have investigated the efficacy of any antihypertensive drug on the prevention or regression of HMOD.
In the absence of high-quality randomized controlled trials comparing different antihypertensive agents in children, several antihypertensive agents may be considered as first-line drugs [ACEis, ARBs, calcium-channel-blockers (CCBs), ß-blockers, and diuretics] based on the evidence available on HTN in adulthood. An exception is that of children with chronic kidney disease (renoparenchymal HTN) who have been shown to benefit from the antiproteinuric and renoprotective properties of ACE-inhibitors and ARBs.
In addition, certain classes of drugs may be favorable or contraindicated in specific clinical conditions (1) (Table 8). For example, in children with obesity-related HTN, the negative metabolic adverse effects of diuretics and beta-blockers on glucose and lipid metabolism make the metabolic neutral classes of ACE-inhibitors and ARBs potentially preferable.
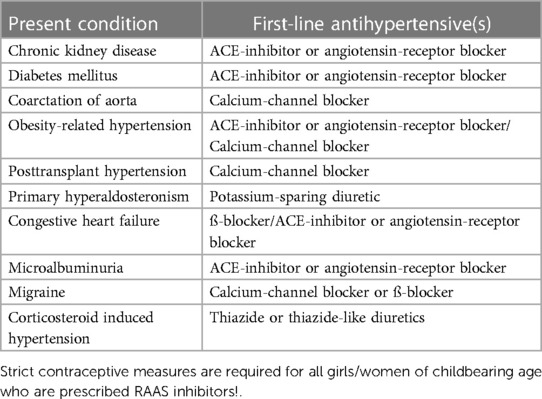
Table 8. Therapeutic approaches.
However, in females of childbearing age, RAAS inhibitors should be prescribed only under strict contraceptive measures due a potential teratogenic effect of these drugs.
Therapeutic approaches in special conditions
Combination therapy
Whenever a single agent, prescribed at the maximum recommended or tolerated dose, does not achieve target BP the use of antihypertensive combination therapy is recommended. Combinations of different drug classes with complementary modes of action should be prescribed, taking into account the underlying diseases and comorbidities of the individual patient (Tables 9, 10, Box 2). (Table 8).
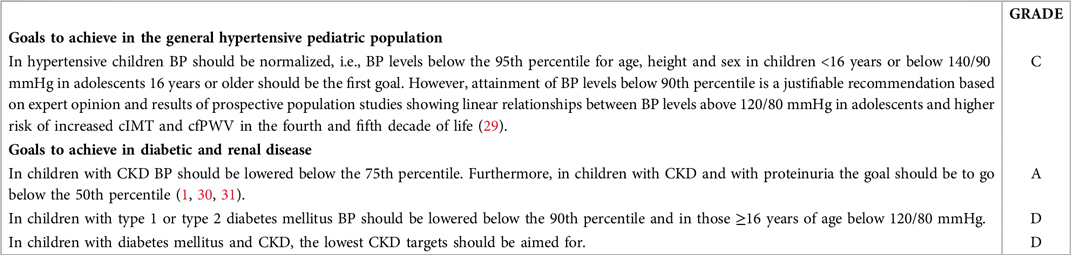
BOX 2. Goals to achieve in the general hypertensive pediatric population and in diabetic and renal disease.
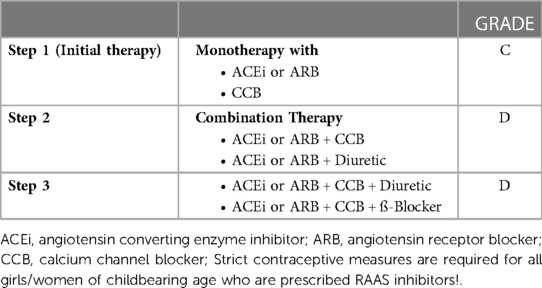
Table 9. Exemplary step scheme for combining antihypertensive drug classes.
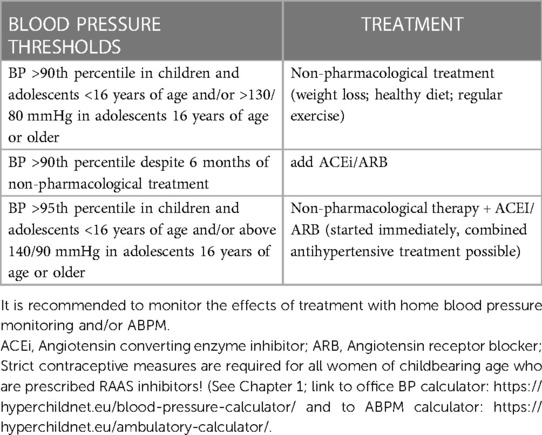
Table 10. Principles of antihypertensive therapy in children with diabetes mellitus type 1 or 2 (grade C).
Motivation strategies for patients and caregivers
Essential information
As in many other chronic diseases (32), patient adherence, the degree to which patients follow the recommendations of their health professionals, is a salient outcome of the process of care and, treatment nonadherence is a major problem in the management of hypertension. Therefore, it is important to introduce motivation strategies for patients and caregivers to increase adherence to treatment (33).
Motivation to change
Motivation to change includes the constructs that must arise from the person him/herself and that are not imposed by third parties. It is an internal state, which fluctuates according to external factors. It has a series of phases, through which the person may undergo, ranging from the decision not to change (by considering only the positive/gratifying aspects of the harmful behavior), to a complete and stable change of habits in favor of a healthier lifestyle such as an adequate diet, physical exercise, giving up tobacco, alcohol, or even increasing adherence to pharmacological treatment (34).
Motivational style
A motivational style has to be followed, on the part of the family and/or physician, by asking openly these types of questions: asking to know how the person feels (with unhealthy habits), what worries he/she has, what doubts he/she has regarding the new habits to change, why do they think it might be important to change his/her new habits, asking about his/her opinion about potential positive consequences of doing so, helping him/her to explore his/her ambivalences and discrepancies. The most important tool to achieve this motivational style is empathy, although others may be active and reflective listening (showing genuine and sincere interest in understanding their concerns and doubts in relation to the change), honesty, not judging or criticizing, being willing to go at the individual's pace, promoting self-efficacy (see Boxs 3, 4 and Table 11) (35, 36).
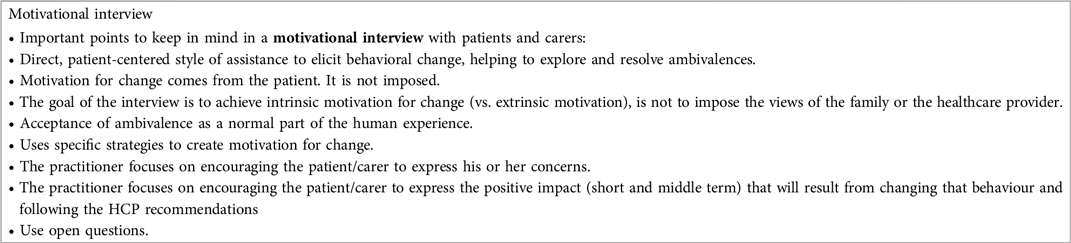
BOX 3. Motivational Interview.

BOX 4. Identifications of resistances by the patient/family member.
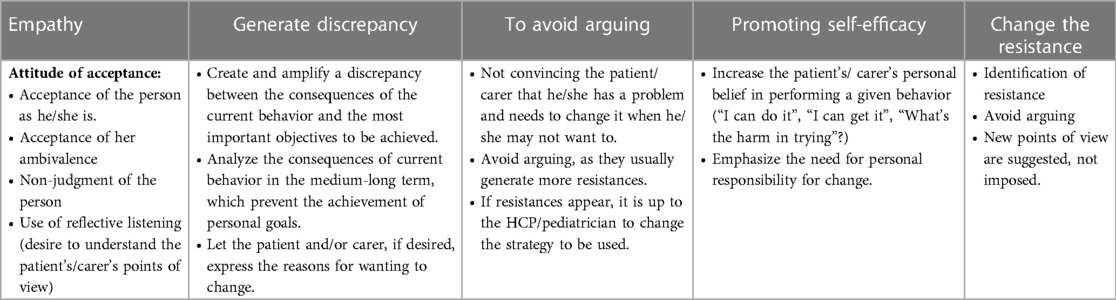
Table 11. Motivation style and recommendations .
Suggested schedule for follow-up examinations
Follow-up of hypertensive individuals is based on the underlying etiology of the high BP condition, presence of co-morbidities, severity of HTN, presence of HMOD and patient's knowledge and understanding of the rationale of the HTN management (Table 12) (1).
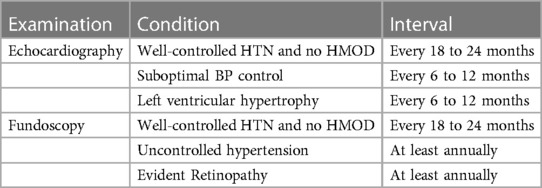
Table 12. Follow-up evaluation for HMOD in children with hypertension.
In the majority of patients with primary HTN, especially those advised non-pharmacological lifestyle changes, infrequent but regular, follow-up is advisable. In contrast, in those whose management includes both pharmacological treatment and lifestyle changes, a more frequent regular follow-up is needed. Home BP monitoring can facilitate the management of HTN. Telemedicine could additionally be helpful. Ideally, in those with chronic kidney disease or diabetes annual ABPM should be recommended to rule out BP control limited to office BP a condition that in adults is termed MUCH (masked uncontrolled HTN). Accessibility to appropriate resources to facilitate this is a key factor.
Patients with well-controlled HTN and no HMOD should be monitored in regular intervals to rule out de novo HMOD, and to assess adherence to therapy and side effects of the pharmacological treatment (1).
Optimal BP control over a prolonged period of time may justify a reduction of the number and dose of antihypertensive drugs. Healthy lifestyle changes should be maintained, the reduction of pharmacological therapy should be made gradually and the patient should frequently be monitored (at 3 to 6 months intervals) because of the risk of re-emergence of HTN (1).
Long-Term consequences of childhood hypertension
Hypertension remains the main modifiable risk factor for the risk of cardiovascular disease and death, and cardiac and vascular damage by an elevated BP begins in childhood.
Early organ damage occurs in the form of left ventricular hypertrophy, thickening and stiffening of the vascular wall, albuminuria, and cognitive dysfunction. HTN and other cardiometabolic factors cause endothelial dysfunction and are responsible for the accelerated process of atherosclerosis. At this stage, organ structural and functional changes may still be reversible or postponed with appropriate treatment.
In recent years, studies have shown both tracking of high BP into adulthood and increased cardiovascular risk in young adults with childhood onset of HTN. High normal BP and hypertensive trajectory groups have worse cardiovascular outcomes by early midlife. Higher body mass index and cigarette smoking are associated with increased BP values across trajectories, particularly in the higher BP groups that in childhood predict adult cardiovascular risk (37).
In a prospective cohort study, childhood risk factors (higher body-mass index, systolic BP, total cholesterol level, triglyceride level, and youth smoking) and the change in the combined-risk z score between childhood and adulthood were associated with cardiovascular events in midlife (38).
The goal of antihypertensive treatment is to reduce the global risk of cardiovascular events. Recognition of risk factors and early cardiovascular damage, at a time when these processes are still reversible, and development of prevention strategies are key factors for the reduction of cardiovascular morbidity and mortality in the general population (39). Long-term follow-up multicenter studies are necessary to assess cardiovascular risk stratification in children and adolescents with HTN and to develop standards for diagnostic and treatment procedures (1, 37–39).
Criteria to refer patients to pediatric specialists
Pediatric specialists for arterial HTN, usually pediatric nephrologists or cardiologists, should be involved in the management of a persistently elevated office BP in an asymptomatic healthy child, i.e., elevated BP values over at least three separate visits (Table 13) (1).
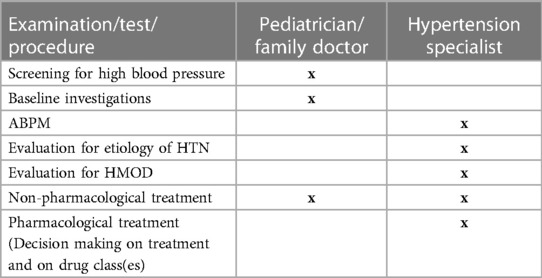
Table 13. Recommended responsibility for hypertension work-up and management in children and adolescents.
Patients should be referred to specialist management earlier (after one or two visits with a BP elevation) if stage 2 HTN is present or HTN is symptomatic. Intervals between visits should be judged on a clinical basis (1).
We encourage early referral to a childhood HTN center, ideally following initial suspicion of HTN, to facilitate timely multidisciplinary input including cardiological and nephrological evaluation. This should encourage Children's Hospitals in Europe to organize expert HTN services which will provide an opportunity for specialist care to work together with family physicians, pediatricians, the hypertensive child and their family, with a greater chance for optimal HTN management.
Reaching the age for transition to adult units. How to proceed
Essential information
Transition refers to the process of moving from pediatric to adult care services beginning in adolescence and continuing into early adulthood (Box 5). This should be done according to preplanned strategies, with the overarching goals to develop patient's readiness, increase the young people' s level of responsibility for their own health care management, engage and enhance the understanding of the conditions they are living with, and build the skills needed to navigate the adult care system. Family support and both patient and family willingness to transfer are also key elements to be considered during transition (40, 41).

BOX 5. Indications for the transition from pediatric to adult care services.
In pediatric patients with early onset of HTN the transition process may start at the age of 12–14 years, gradually introducing an individualized transition plan during adolescence (40–42) based also on the presence of HMOD and/or comorbidities. The adoption of adult thresholds for the diagnosis of HTN in adolescents ≥16 years old by the ESH 2016 guidelines (1), enable smooth transition to adult health care.
Present challenges
• Little guidance is provided in the literature, with low evidence on the effectiveness of any specific intervention on transition to improve transfer to adult health care (43).
• Involving primary care practitioners in transition. Very little is known about the impact and role of primary health providers in supporting the transition of youth with health care needs. Community services and primary care teams tend to provide holistic care and are effective for integrating social determinants of health.
Conclusions
Arterial hypertension is the most important modifiable risk factor for cardiovascular morbidity and mortality. Therefore, appropriate antihypertensive therapy including lifestyle measures and pharmacologic treatment should be initiated in children as soon as the diagnosis of arterial hypertension has been confirmed and the risk factors for hypertension-induced organ damage have been thoroughly evaluated. Early referral to a pediatric hypertension center, ideally after the first suspicion of hypertension, is recommended to allow timely multidisciplinary evaluation, including workup by pediatric cardiologists and nephrologists, and initiation of antihypertensive treatment.
Author contributions
All authors listed have made a substantial, direct, and intellectual contribution to the work, and approved it for publication. All authors contributed to the article and approved the submitted version.
Acknowledgments
Chapter 1 “How to correctly measure blood pressure in children and adolescents” and Chapter 2 “How to manage high blood pressure in children and adolescents” of the JOINT STATEMENT FOR ASSESSING AND MANAGING HIGH BLOOD PRESSURE IN CHILDREN AND ADOLESCENTS are based upon the work of the COST Action HyperChildNET (CA19115), with the support of COST (European Cooperation in Science and Technology).
Conflict of interest
JC was employed by Analog Devices Inc. The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Lurbe E, Agabiti-Rosei E, Cruickshank JK, Dominiczak A, Erdine S, Hirth A, et al. 2016 European society of hypertension guidelines for the management of high blood pressure in children and adolescents. J Hypertens. (2016) 34:1887–920. doi: 10.1097/HJH.0000000000001039
2. Khoury PR, Mitsnefes M, Daniels SR, Kimball TR. Age-specific reference intervals for indexed left ventricular mass in children. J Am Soc Echocardiogr. (2009) 22:709–14. doi: 10.1016/j.echo.2009.03.003
3. de Simone G, Devereux RB, Daniels SR, Koren MJ, Meyer RA, Laragh JH. Effect of growth on variability of left ventricular mass: assessment of allometric signals in adults and children and their capacity to predict cardiovascular risk. J Am Coll Cardiol. (1995) 25:1056–62. doi: 10.1016/0735-1097(94)00540-7
4. Lang RM, Bierig M, Devereux RB, Flachskampf FA, Foster E, Pellikka PA, et al. Recommendations for chamber quantification: a report from the American society of Echocardiography's guidelines and standards committee and the chamber quantification writing group, developed in conjunction with the European association of echocardiography, a branch of the European society of cardiology. J Am Soc Echocardiogr. (2005) 18:1440–63. doi: 10.1016/j.echo.2005.10.005
5. de Simone G, Daniels SR, Devereux RB, Meyer RA, Roman MJ, de Divitiis O, et al. Left ventricular mass and body size in normotensive children and adults: assessment of allometric relations and impact of overweight. J Am Coll Cardiol. (1992) 20:1251–60. doi: 10.1016/0735-1097(92)90385-Z
6. Elmenhorst J, Hulpke-Wette M, Barta C, Dalla Pozza R, Springer S, Oberhoffer R. Percentiles for central blood pressure and pulse wave velocity in children and adolescents recorded with an oscillometric device. Atherosclerosis. (2015) 238:9–16. doi: 10.1016/j.atherosclerosis.2014.11.005
7. Doyon A, Kracht D, Bayazit AK, Deveci M, Duzova A, Krmar RT, et al. Carotid artery intima-media thickness and distensibility in children and adolescents: reference values and role of body dimensions. Hypertension. (2013) 62:550–6. doi: 10.1161/HYPERTENSIONAHA.113.01297
8. Reusz GS, Cseprekal O, Temmar M, Kis E, Cherif AB, Thaleb A, et al. Reference values of pulse wave velocity in healthy children and teenagers. Hypertension. (2010) 56:217–24. doi: 10.1161/HYPERTENSIONAHA.110.152686
9. Couch SC, Saelens BE, Levin L, Dart K, Falciglia G, Daniels SR. The efficacy of a clinic-based behavioral nutrition intervention emphasizing a DASH-type diet for adolescents with elevated blood pressure. J Pediatr. (2008) 152:494–501. doi: 10.1016/j.jpeds.2007.09.022
10. Moore LL, Bradlee ML, Singer MR, Qureshi MM, Buendia JR, Daniels SR. Dietary approaches to stop hypertension (DASH) eating pattern and risk of elevated blood pressure in adolescent girls. Br J Nutr. (2012) 108:1678–85. doi: 10.1017/S000711451100715X
11. Svetkey LP, Simons-Morton D, Vollmer WM, Appel LJ, Conlin PR, Ryan DH, et al. Effects of dietary patterns on blood pressure: subgroup analysis of the dietary approaches to stop hypertension (DASH) randomized clinical trial. Arch Intern Med. (1999) 159:285–93. doi: 10.1001/archinte.159.3.285
12. Rasmussen BM, Vessby B, Uusitupa M, Berglund L, Pedersen E, Riccardi G, et al. Effects of dietary saturated, monounsaturated, and n-3 fatty acids on blood pressure in healthy subjects. Am J Clin Nutr. (2006) 83:221–6. doi: 10.1093/ajcn/83.2.221
13. Moreno-Luna R, Munoz-Hernandez R, Miranda ML, Costa AF, Jimenez-Jimenez L, Vallejo-Vaz AJ, et al. Olive oil polyphenols decrease blood pressure and improve endothelial function in young women with mild hypertension. Am J Hypertens. (2012) 25:1299–304. doi: 10.1038/ajh.2012.128
14. Nguyen S, Choi HK, Lustig RH, Hsu CY. Sugar-sweetened beverages, serum uric acid, and blood pressure in adolescents. J Pediatr. (2009) 154:807–13. doi: 10.1016/j.jpeds.2009.01.015
15. Wojcik M, Koziol-Kozakowska A. Obesity, sodium homeostasis, and arterial hypertension in children and adolescents. Nutrients. (2021) 13:4032. doi: 10.3390/nu13114032
16. World Health Organisation: Guideline: Sodium Intake for Adults and Children. Available online: http://www.who.int/nutrition/publications/guidelines/sodium_intake/en (2012). Accessed 08 January 2023.
18. Farpour-Lambert NJ, Aggoun Y, Marchand LM, Martin XE, Herrmann FR, Beghetti M. Physical activity reduces systemic blood pressure and improves early markers of atherosclerosis in pre-pubertal obese children. J Am Coll Cardiol. (2009) 54:2396–406. doi: 10.1016/j.jacc.2009.08.030
19. Beunza JJ, Martinez-Gonzalez MA, Ebrahim S, Bes-Rastrollo M, Nunez J, Martinez JA, et al. Sedentary behaviors and the risk of incident hypertension: the SUN cohort. Am J Hypertens. (2007) 20:1156–62. doi: 10.1016/j.amjhyper.2007.06.007
20. St-Onge MP, Grandner MA, Brown D, Conroy MB, Jean-Louis G, Coons M, et al. Sleep duration and quality: impact on lifestyle behaviors and cardiometabolic health: a scientific statement from the American heart association. Circulation. (2016) 134:e367–e86. doi: 10.1161/CIR.0000000000000444
21. Bock JM, Vungarala S, Covassin N, Somers VK. Sleep duration and hypertension: epidemiological evidence and underlying mechanisms. Am J Hypertens. (2022) 35:3–11. doi: 10.1093/ajh/hpab146
22. Brook RD, Rajagopalan S, Pope CA 3rd, Brook JR, Bhatnagar A, Diez-Roux AV, et al. Particulate matter air pollution and cardiovascular disease: an update to the scientific statement from the American heart association. Circulation. (2010) 121:2331–78. doi: 10.1161/CIR.0b013e3181dbece1
23. Aydin Y, Kaltenbach M. Noise perception, heart rate and blood pressure in relation to aircraft noise in the vicinity of the Frankfurt airport. Clin Res Cardiol. (2007) 96:347–58. doi: 10.1007/s00392-007-0507-y
24. Thiesse L, Rudzik F, Kraemer JF, Spiegel K, Leproult R, Wessel N, et al. Transportation noise impairs cardiovascular function without altering sleep: the importance of autonomic arousals. Environ Res. (2020) 182:109086. doi: 10.1016/j.envres.2019.109086
25. Marti-Soler H, Gonseth S, Gubelmann C, Stringhini S, Bovet P, Chen PC, et al. Seasonal variation of overall and cardiovascular mortality: a study in 19 countries from different geographic locations. PloS One. (2014) 9:e113500. doi: 10.1371/journal.pone.0113500
26. Katona E, Zrinyi M, Komonyi E, Lengyel S, Paragh G, Zatik J, et al. Factors influencing adolescent blood pressure: the debrecen hypertension study. Kidney Blood Press Res. (2011) 34:188–95. doi: 10.1159/000326115
27. Schaefer F, Litwin M, Zachwieja J, Zurowska A, Turi S, Grosso A, et al. Efficacy and safety of valsartan compared to enalapril in hypertensive children: a 12-week randomized, double-blind, parallel study. J Hypertens. (2011) 29:2484–90. doi: 10.1097/HJH.0b013e32834c625c
28. Chaturvedi S, Lipszyc DH, Licht C, Craig JC, Parekh RS. Cochrane in context: pharmacological interventions for hypertension in children. Evid Based Child Health. (2014) 9:581–3. doi: 10.1002/ebch.1975
29. Juhola J, Magnussen CG, Berenson GS, Venn A, Burns TL, Sabin MA, et al. Combined effects of child and adult elevated blood pressure on subclinical atherosclerosis: the international childhood cardiovascular cohort consortium. Circulation. (2013) 128:217–24. doi: 10.1161/CIRCULATIONAHA.113.001614
30. Wühl E, Trivelli A, Picca S, Litwin M, Peco-Antic A, Zurowska A, et al. Strict blood pressure control and renal failure progression in children. N Engl J Med. (2009) 361:1639–50. doi: 10.1056/NEJMoa0902066
31. Dionne JM, Jiang S, Ng DK, Flynn JT, Mitsnefes MM, Furth SL, et al. Mean arterial pressure and chronic kidney disease progression in the CKiD cohort. Hypertension. (2021) 78:65–73. doi: 10.1161/HYPERTENSIONAHA.120.16692
32. Desai N. The role of motivational interviewing in children and adolescents in pediatric care. Pediatr Ann. (2019) 48:e376–e9. doi: 10.3928/19382359-20190816-01
33. Feldman ECH, Durkin LK, Greenley RN. Family support is associated with fewer adherence barriers and greater intent to adhere to oral medications in pediatric IBD. J Pediatr Nurs. (2021) 60:58–64. doi: 10.1016/j.pedn.2021.01.026
34. Verbeeten KC, Chan J, Sourial N, Courtney JM, Bradley BJ, McAssey K, et al. Motivational stage at continuous glucose monitoring (CGM) initiation in pediatric type 1 diabetes is associated with current glycemic control but does not predict future CGM adherence or glycemic control. Can J Diabetes. (2021) 45:466–72.e4. doi: 10.1016/j.jcjd.2021.04.004
35. Powell PW, Hilliard ME, Anderson BJ. Motivational interviewing to promote adherence behaviors in pediatric type 1 diabetes. Curr Diab Rep. (2014) 14(10):531. doi: 10.1007/s11892-014-0531-z
36. Halford JCG, Bereket A, Bin-Abbas B, Chen W, Fernandez-Aranda F, Garibay Nieto N, et al. Misalignment among adolescents living with obesity, caregivers, and healthcare professionals: ACTION teens global survey study. Pediatr Obes. (2022) 17(11):e12957. doi: 10.1111/ijpo.12957
37. Theodore RF, Broadbent J, Nagin D, Ambler A, Hogan S, Ramrakha S, et al. Childhood to early-midlife systolic blood pressure trajectories: early-life predictors, effect modifiers, and adult cardiovascular outcomes. Hypertension. (2015) 66:1108–15. doi: 10.1161/HYPERTENSIONAHA.115.05831
38. Jacobs DR Jr., Woo JG, Sinaiko AR, Daniels SR, Ikonen J, Juonala M, et al. Childhood cardiovascular risk factors and adult cardiovascular events. N Engl J Med. (2022) 386:1877–88. doi: 10.1056/NEJMoa2109191
39. Drozdz D, Alvarez-Pitti J, Wojcik M, Borghi C, Gabbianelli R, Mazur A, et al. Obesity and cardiometabolic risk factors: from childhood to adulthood. Nutrients. (2021) 13:4176. doi: 10.3390/nu13114176
40. American Academy of Pediatrics, American Academy of Family Physicians, American College of Physicians, Transitions Clinical Report Authoring Group, Cooley WC, Sagerman PJ. Supporting the health care transition from adolescence to adulthood in the medical home. Pediatrics. (2011) 128:182–200. doi: 10.1542/peds.2011-0969
41. Pape L, Ernst G. Health care transition from pediatric to adult care: an evidence-based guideline. Eur J Pediatr. (2022) 181:1951–8. doi: 10.1007/s00431-022-04385-z
42. White PH, Cooley WC, Transitions Clinical Report Authoring Group, American Academy Of Pediatrics, American Academy Of Family Physicians, American College of Physicians. Supporting the health care transition from adolescence to adulthood in the medical home. Pediatrics. (2018) 142:e20182587. doi: 10.1542/peds.2018-2587
Keywords: adolescents, blood pressure, children, hypertension, monitoring, treatment, hypertension-mediated organ damage
Citation: Wühl E, Calpe J, Drożdż D, Erdine S, Fernandez-Aranda F, Hadjipanayis A, Hoyer PF, Jankauskiene A, Jiménez-Murcia S, Litwin M, Mancia G, Mazur A, Pall D, Seeman T, Sinha MD, Simonetti G, Stabouli S and Lurbe E (2023) Joint statement for assessing and managing high blood pressure in children and adolescents: Chapter 2. How to manage high blood pressure in children and adolescents. Front. Pediatr. 11:1140617. doi: 10.3389/fped.2023.1140617
Received: 9 January 2023; Accepted: 20 March 2023;
Published: 12 April 2023.
Edited by:
Ruan Kruger, North-West University, South AfricaReviewed by:
Joshua Alex Samuels, University of Texas Health Science Center at Houston, United StatesAftab S. Chishti, University of Kentucky, United States
© 2023 Wühl, Calpe, Drożdż, Erdine, Fernandez-Aranda, Hadjipanayis, Hoyer, Jankauskiene, Jiménez-Murcia, Litwin, Mancia, Mazur, Pall, Seeman, Sinha, Simonetti, Stabouli and Lurbe. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Elke Wühl ZWxrZS53dWVobEBtZWQudW5pLWhlaWRlbGJlcmcuZGU= Empar Lurbe ZW1wYXIubHVyYmVAdXYuZXM= Adamos Hadjipanayis YWRhbW9zQHBhaWRpYXRyb3MuY29t
Specialty Section: This article was submitted to General Pediatrics and Pediatric Emergency Care, a section of the journal Frontiers in Pediatrics