 Débora Familiar-Macedo1*
Débora Familiar-Macedo1* Helver Gonçalves Dias1
Helver Gonçalves Dias1 Fabiana Rabe Carvalho2
Fabiana Rabe Carvalho2 Alex Pauvolid-Corrêa3
Alex Pauvolid-Corrêa3 Mayara Neto da Silveira4
Mayara Neto da Silveira4 Mariana Cavalcante de Oliveira1
Mariana Cavalcante de Oliveira1 Rita de Cássia Ferreira Gonçalves5
Rita de Cássia Ferreira Gonçalves5 Renata Artimos de Oliveira Vianna6
Renata Artimos de Oliveira Vianna6 Claudete Aparecida Araujo Cardoso2,6
Claudete Aparecida Araujo Cardoso2,6 Raquel Tavares Boy da Silva4Anna Paula Baumblatt4
Raquel Tavares Boy da Silva4Anna Paula Baumblatt4 Luzia Maria de-Oliveira-Pinto1*
Luzia Maria de-Oliveira-Pinto1*
- 1Laboratório das Interações Vírus-Hospedeiros (LIVH), Instituto Oswaldo Cruz, Fundação Oswaldo Cruz (IOC/Fiocruz), Rio de Janeiro, Brazil
- 2Laboratório Multiusuário de Apoio à Pesquisa em Nefrologia e Ciências Médicas (LAMAP), Faculdade de Medicina, Universidade Federal Fluminense, Niterói, Brazil
- 3Laboratório de Virologia Veterinária de Viçosa (LAVEV), Departamento de Veterinária, Universidade Federal de Viçosa (UFV), Viçosa, Brazil
- 4Ambulatório Multidisciplinar de Síndrome de Down (AMBDOWN), Departamento de Pediatria, Faculdade de Ciências Médicas, Universidade Estadual do Rio de Janeiro, Rio de Janeiro, Brazil
- 5Hospital Getúlio Vargas Filho, Fundação Municipal de Saúde, Niterói, Brazil
- 6Departamento Materno Infantil, Faculdade de Medicina, Universidade Federal Fluminense, Niterói, Brazil
Background: Vaccination schedules, as well as their effectiveness and contraindications, need to be evaluated regularly, especially in specific situations. Congenital Zika Syndrome (CZS) is a severe condition that results in extensive functional and neurological impairment of fetuses and newborns due to Zika virus tropism for fetal neural progenitor cells. Down Syndrome (DS) is the leading genetic cause of intellectual disability. The immune impairment in DS has already been described, but little is known about the immune response of CZS children. Thus, CZS and DS are specific conditions that can be considered for a reassessment of the available immunizations. Here, we carried out serological analyses of attenuated vaccines-induced antibodies for measles, rubella, and yellow fever viruses in children aged 2–7, grouped into asymptomatic controls, DS children, and CZS children.
Methods: Plasma samples were taken, and vaccination records were compiled during clinical follow-up. Enzymatic immunoassays for quantifying anti-measles and anti-rubella IgG were performed to assess the response to the Measles, Mumps, and Rubella (MMR) vaccine. Plaque Reduction Neutralization Test (PRNT) was performed to investigate neutralizing antibodies in response to the Brazilian vaccine strain of yellow fever (YF-17DD).
Results: We highlight similar levels of anti-measles IgG and neutralizing antibodies for YF-17DD among CZS, DS, and asymptomatic children, although low positivity of measles data was seen in the three groups. In DS children, the 2–4-year-old group had an increased level of anti-measles IgG compared to the older group of children aged five to seven years. Lower anti-rubella IgG levels were observed in CZS and DS children compared to asymptomatic children. For anti-rubella IgG, the good performance of vaccination in asymptomatic children is due to younger ones rather than older ones.
Conclusions: There were no reports of adverse events after the use of the MMR and YF-17DD indicating that CZS and DS could continue to receive these vaccines, but our data draws attention to the necessity of monitoring the vaccination response in CZS and DS children over time and the possible need to adhere to national measles vaccination campaigns. Scientific research needs to continue to help develop appropriate CZS and DS health guidelines.
Introduction
Vaccine-preventable diseases such as tuberculosis, poliomyelitis, measles, and tetanus have declined considerably due to successful vaccination programs worldwide (1). Vaccination is one of the most fundamental advancements in public health as it significantly reduces mortality and morbidity rates due to various infectious diseases (2). However, five million children under 5 years old died in 2021, mostly from vaccine preventable infections (3, 4). On the other hand, there are still no vaccines for several infectious diseases and the effectiveness and contraindications of regular vaccination schedules need to be evaluated regularly, especially in specific situations, such as children affected by Congenital Zika Syndrome (CZS) and Down Syndrome (DS). Zika virus (ZIKV) can cross the maternal-fetal barrier and cause CZS, a serious condition due to the extent of functional impairment in children (5, 6). CZS is often associated with unique symptoms in infected fetuses and newborns, such as severe microcephaly with a partially collapsed skull: fine cerebral cortex with subcortical calcifications; hypertonia; macular scars and retinal changes due to viral tropism for fetal ocular and neural progenitor cells (5, 7, 8). Our group investigated a cohort of children between 2 and 3 years of age with a history of transplacental ZIKV infection. Only two of 17 children (12%) had ZIKV IgG and two of 15 (13%) had specific neutralizing antibodies for ZIKV (9, 10). This seropositivity was much lower than we expected. Based on this finding, we wondered whether these children would also have low antibody detection to other antigens unrelated to ZIKV. Salmeron et al. have shown that children with CZS react poorly to the tuberculin skin test, 2 years after BCG vaccination (11).
Another group of children that needs to be studied regarding vaccine efficacy is those with Down Syndrome (DS). Down syndrome is the most common genetic syndrome associated with intellectual disability as well as immune defects (12). The variability of the clinical presentation and the presence of clinical comorbidities associated with congenital heart diseases, digestive tract diseases, and thyroid dysfunctions directly influence the health problems experienced by these patients (13). In addition, individuals with DS often have a high frequency of infections, usually of the upper respiratory tract, characterized by greater severity and a prolonged course of diseases, which are attributed to deficiencies in the immune system (14) and to anatomical peculiarities of the face, such as shorter midface, a relative macroglossia and short eustachian tubes (12). They have substantial immune dysregulation encompassing innate and adaptive immune systems, including abnormalities in T and B cells, monocytes, neutrophil chemotaxis, circulating cytokines, and suboptimal antibody responses (15, 16). Due to these immunological disorders, they are eligible for broader vaccination coverage carried out in reference centers for immunobiological and special drugs (12, 17, 18).
The National Immunization Program (NIP) in Brazil offers 48 different immunobiological for the entire population, including children, adults, the elderly, and pregnant women (19). Among childhood vaccines, the triple viral vaccine against Measles, Mumps, and Rubella (MMR) is composed of attenuated viruses administered in two doses: the first dose at 12 months of age and the second at 15 months. At 15 months, the varicella (chickenpox) vaccine is added to the second dose of MMR (becoming MMRV). The NIP annually carries out National Vaccination Campaigns, against the antigens included in the regular Vaccination Calendar, allowing children who are not up to date with their regular vaccines to update their immunizations, and against Influenza, polio and measles (mainly observing the country's epidemiological conditions) for children under 5 years of age. Another vaccine given in childhood is the yellow fever vaccine (strain YF-17DD) which is also an attenuated vaccine given to children as young as nine months old with a booster dose at four years old (20).
Except for health complications and epidemiological risks, children with CZS and DS follow the NIP schedule (21). There is a clear need to compare the vaccination effectiveness of children with CZS and DS with asymptomatic controls so that families and health professionals can care for them with guarantees of safety in the administration of attenuated vaccines and the effectiveness of the schedule. In the present study, we sought to investigate the levels of IgG antibodies for measles and rubella vaccines and the titers of neutralizing antibodies for the yellow fever vaccine in children between 2 and 7 years old. The MMR and YFV-17DD were offered by the NIP. The data generated in this study provides us with an opportunity to assess children's ability to generate a humoral immune response to vaccines, identify possible gaps in the vaccination schedule especially in low coverage vaccination period and collaborate, based on our findings, with healthcare guidance for CZS and DS.
Methods
Study design
This is a cross-sectional study of convenience sampling. Between 2018 and 2022, we recruited 80 children between 2 and 7 years old. They were categorized into three groups based on the presence or absence of syndromes, which will be explained below. The asymptomatic group (n = 24) comprises children that do not present clinical symptoms associated with congenital syndromes due to viral infection or genetics condition. All were in good health at the time of blood collection. Some children were born to mothers who had a rash during pregnancy, and some had ZIKV detected by RT-qPCR but were born asymptomatic. All of them were negative for other congenital infections [Syphilis, Toxoplasmosis, Rubella, Cytomegalovirus (CMV) and Herpes simplex-STORCH] and to any clinical changes to date. The group of children with Congenital Zika Syndrome (CZS, n = 22), are those with a history of intrauterine exposure to ZIKV. These children were born from mothers who had a positive RT-qPCR for ZIKV and/or a confirmed clinical diagnosis of Zika infection during the pregnancy in the ZIKV epidemic in Brazil (2015–2016) and were negative for other congenital infections (STORCH). After birth, these children have a confirmatory clinical picture of CZS. These children are followed up at the Unidade de Doenças Exantemáticas do Hospital Universitário Antônio Pedro (HUAP) at Universidade Federal Fluminense (UFF) (Rio de Janeiro, Brazil) by Dr. Claudete Araújo Cardoso and team. The third group comprised children with Down Syndrome (DS, n = 34) or trisomy 21. These are children who are routinely treated at the Ambulatório Multidisciplinar de Síndrome de Down of the Hospital Universitário Pedro Ernesto (HUPE) at Universidade do Estado do Rio de Janeiro (UERJ) (Rio de Janeiro, Brazil) by Dr. Anna Paula Baumblatt and Dr. Raquel Tavares Boy da Silva. The children's vaccination records were collected after parents or legal guardians gave written consent. As an exclusion criterion, children with a history of measles, rubella, and yellow fever infection and those sick at the time or one month before blood collection were excluded from the study. According to the medical records, none of our children had history of measles, rubella, or yellow fever infection.
Ethics statement
This study was approved by the Ethics Committee of the Oswaldo Cruz Foundation (CAAE 47358821.6.0000.5248), the Ethics Committee of UFF (CAAE 47358821.6.3001.5243 and CAAE 47358821.6.3001.524) and the Ethics Committee of UERJ (CAAE 47358821.6.3002.5259). The children's legal guardians read and signed the free and informed consent form.
Blood samples collection
Approximately 10 ml of peripheral blood was collected via venipuncture using BD Vacutainer™ tubes containing acid-citrate-dextrose (Cat. # BD 364606). Plasma samples were obtained by centrifugation, divided into aliquots, and stored at −70 °C until analysis.
Anti-measles and anti-rubella IgG antibody detection by commercial kit
Enzyme immunoassays (ELISA) for quantification of anti-measles (Cat. # EI 2610-9601G Euroimmun, Lübeck, Germany) and anti-rubella (Cat. # EI 2590-9601G Euroimmun, Lübeck, Germany) IgG were performed according to the manufacturer's recommended instructions. Measles IgG is expressed in International Units per liter (IU/L), where titers below 200 IU/L are considered negative, ≥200 to <275 IU/L are borderline, and ≥275 IU/L are positive. Rubella virus IgG levels are expressed in International Units per milliliter (IU/ml). Titers below 8 IU/ml are negative, ≥8 to <11 IU/ml are borderline, and ≥11 IU/ml are positive.
YF-17DD propagation
The attenuated vaccine of yellow fever virus (YFV-17DD) strain PV027/19 was kindly provided by the Laboratório de Mosquitos Transmissores de Hematozoários (LATHEMA) of Instituto Oswaldo Cruz, Fiocruz. YF-17DD propagated in VERO cell culture (ATCC, CCL-81). Cytopathic effect (CPE) was verified daily. CPE was observed on third-day post-infection, and the culture supernatant containing the infectious virus was collected on the fifth day. Supernatant was aliquoted into working stocks, and an aliquot was subjected to RT-qPCR for YFV and other arboviruses to rule out possible contamination.
Plaque reduction neutralization test (PRNT)
For the PRNT assay, 105 VERO CCL-81 cells per well were cultured in 24-well plates and maintained in Medium 199 (Gibco, Cat.: 11150059) supplemented (10% Fetal Bovine Serum, 100 U/ml penicillin, 0.1 mg/ml streptomycin and 0.025 ug/ml amphotericin B) at 37 °C in 5% CO2. Plasma samples from vaccinated children were previously heated at 56 °C for 30 min to inactivate complement system proteins. Plasma samples were diluted at 2-fold serial dilution from 1:10 to 1:320. Diluted plasma samples were incubated in equal volumes with 40–80 plaque forming units (PFU) of YF-17DD strain for 1 h (at 37 °C in 5% CO2). After the first incubation, plasma and virus mixtures were transferred to VERO CCL-81 monolayers seeded in 24-well plates. The plates were then incubated for 1 h (at 37 °C in 5% CO2) with mixing every 10 min. Finally, after the second incubation, overlay solution composed by supplemented Medium 199, and 0.3% agarose was added to all wells, followed by a final incubation at 37 °C in 5% CO2. On the fifth day post-infection, cells were fixed in formalin for 48 h. The plates were washed, and the overlay was removed. For staining, 1% crystal violet solution was added to cell monolayers. After 1 h, the crystal violet was removed, and the plates were gently washed. Plaque forming units (PFU) were viewed and counted using a transilluminator (22, 23). Plasma samples were considered seropositive when plasma dilutions greater than 1:10 reduced 50% PFU of the YF-17DD strain. The seronegative samples reduced less than 50% PFU. In those plasma samples that had PRNT50 titers ≥320, no further titration was carried out.
Statistical analysis
Descriptive and correlated analyzes were presented by medians with an interquartile range (IQR: 25%–75%) or median and minimum and maximum values, depending on the type of variable analyzed. Chi-square and Fisher's exact tests were used to assess demographics and positivity rate. Geometric means were used for PRNT titers. Kruskal–Wallis's test of variance, followed by Dunn's multiple comparison tests, was used when comparisons were made among the three groups. The Mann–Whitney test was used to compare differences between two groups or two variables within a group. Values of p < 0.05 will be considered statistically significant. The software used for analysis will be GraphPad PRISM version 9.01 (GraphPad Software).
Results
Cohort description
The demographic data of the 80 participants are presented in Table 1. The children's blood samples were taken during the clinical routine. None of the children were sick at collection or up to one month before the appointment. Asymptomatic children (n = 24) and children with Congenital Zika Syndrome (n = 22) or Down syndrome (n = 34) are shown. Regarding the frequency of gender or age, no difference was observed among the groups.

Table 1. Demographic profile of children aged two to seven years in Rio de janeiro, Brazil, 2018–2022.
Anti-measles IgG and anti-rubella IgG antibody levels and seropositivity in children vaccinated with MMR
With MMR vaccination, measles and rubella IgG were quantified and expressed in IU/L or IU/ml, respectively, to assess the immune status of vaccinated children. Measles IgG was considered positive with a cutoff value of 275 IU/L or higher, as recommended by the commercial kit. Asymptomatic children had a median level of 490.1 IU/L (interquartile range [IQR]: 196.8–778.4) with 66.7% positivity (16/24), children with CZS had 302.1 IU/L (118.9–5,000) with 54.5% positivity (12/22) and children with DS had 330.2 IU/L (116.9–1,208) with 55.9% positivity (19/34). There was no significant difference in anti-measles IgG measures or positivity among groups (Figures 1A,B).
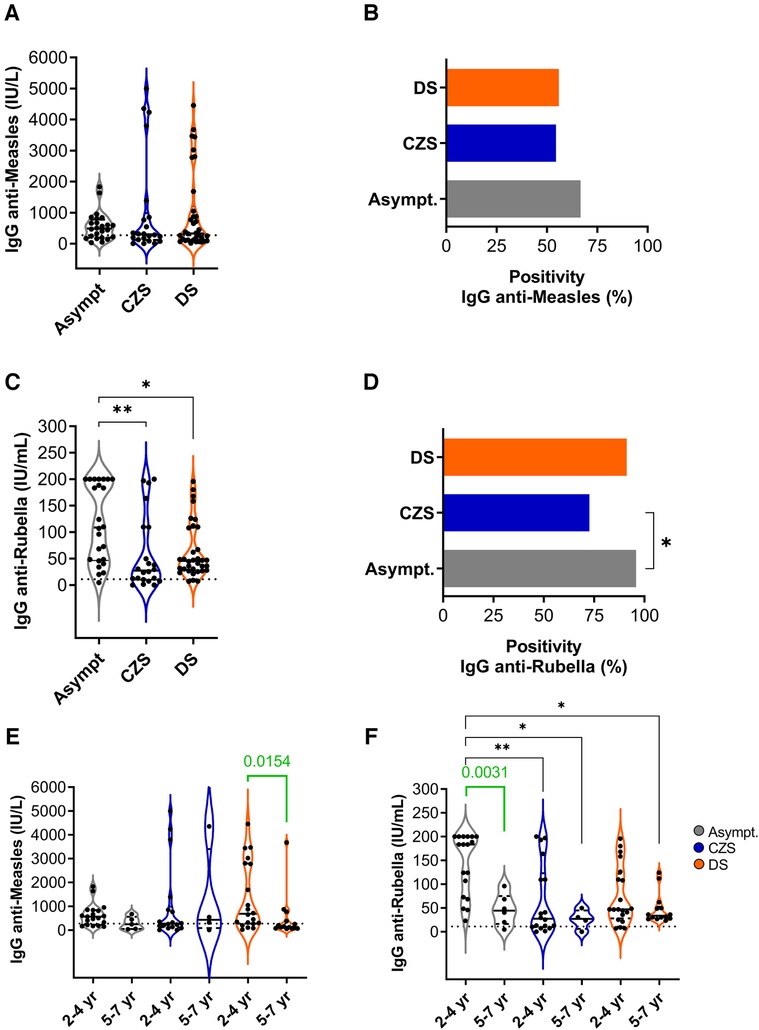
Figure 1. Measles and rubella IgG levels and seropositivity rate in MMR vaccinated children. (A) Plasma levels of anti-measles IgG (IU/L) and (B) frequency of measles positivity in asymptomatic, CZS and DS children. (C) Plasma levels of anti-rubella IgG (IU/ml) and (D) rubella positivity. (E) Anti-measles and (F) anti-rubella IgG plasma levels according to age group. Violin charts show the median (middle line) and describe numerical data distributions using density curves. Positive cutoffs are represented by dotted line. The Kruskal–Wallis's test was used, followed by the Dunn multiple comparison tests. Mann–Whitney test (green lines and values) assessed two groups. The asterisks indicate significant differences (*p < 0.05; **p < 0.01).
With a cutoff point equal to or greater than 11 IU/ml, the anti-rubella IgG dosage was considered positive, as recommended by the commercial kit. Asymptomatic children had a median of 108.7 IU/ml (46.5–200) with a positivity rate of 95.8% (23/24). In the CZS group, the mean IgG level was 27.5 IU/ml (9.7–109.6) with 72.7% positivity (16/22), and the DS group was 45.9 IU/ml (27.7–108.5) with 91.2% positivity (31/34). Disabled children had lower rubella IgG than asymptomatic children and lower positivity was observed in CZS compared to asymptomatic children (Figures 1C,D).
Age-based immune status is one of the factors that can interfere with vaccine efficacy. Although the measles data are similar in the three groups, children with DS aged 2–4 years old had an increased level of anti-measles IgG compared with older DS children aged five to seven years old (Figure 1E). For anti-rubella IgG, the good performance of vaccination in asymptomatic children is due to younger ones than older ones (Figure 1F). These data call attention to the need to evaluate the vaccine response of children according to age.
Neutralizing antibodies for YFV in children vaccinated with YF-17DD
To investigate the YFV-neutralizing antibody titer after YF-17DD vaccination, we used the PRNT50 calculation. The PRNT50 YF-17DD was considered seronegative when a titer cutoff value was lower than 10. This cutoff value was obtained from the assessment of three children known to be unvaccinated. The data shows that asymptomatic children had a geometric mean titer (GMT) of 95.3 (95% confidence interval [CI], 51.3–177.2), with 83.3% positivity (20/24), the children with CZS had 106.7 (53.9–210.9) with 77.3% positivity (17/22) and those with DS 74.5 (47.4–117.2) with 83.9% of positivity (26/31). It is possible that the GMT values were underestimated because our titer was up to 320. Plasma samples with PRNT50 titer 320 were not retested to reach endpoint titer. The data did not indicate a significant difference among groups in PRNT50 YF-17DD titers or positivity (Figures 2A,B). Analyzes by age groups did not show differences either (Figure 2C).
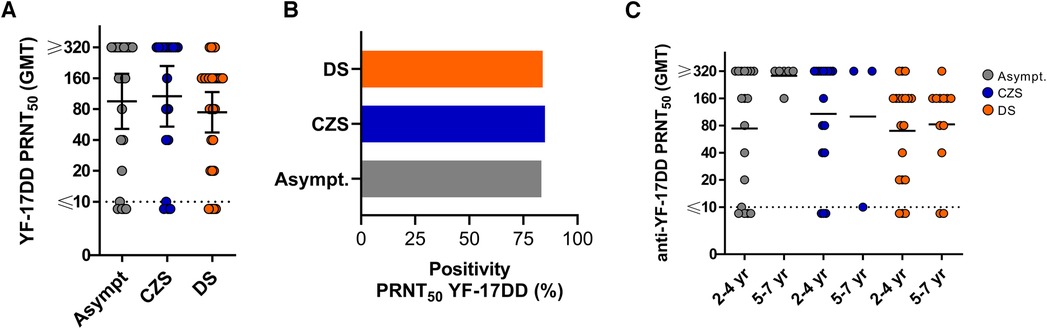
Figure 2. YF-17DD PRNT titers and positivity rate in YF-17DD-vaccinated children. (A) PRNT50 titers in asymptomatic, CZS and DS children. (B) Frequency of positivity in PRNT50. (C) PRNT50 titer in children by age group. Lines show the geometric mean and branches represents 95% CI. Positive cutoffs are represented by dotted line. The Kruskal–Wallis's test was used, followed by the Dunn multiple comparison tests. Mann–Whitney test assessed two groups. p < 0.05 were statistically significant.
Impact on the effectiveness of vaccination according to doses and duration of vaccination
Based on vaccination records, asymptomatic children took between two and four doses of the MMR vaccine, with a median of 27 months after the last dose, ranging from seven to 45 months. For YF-17DD, most asymptomatic children took between one and two doses as expected, but the median time elapsed after the last dose is 12.5 months ranging from six to 49 months (Table 2). These data indicate that all groups followed the national vaccination program schedule advocated by the Ministry of Health in Brazil. Regarding the number of doses or time elapsed from the last vaccination until the blood collection, we had a smaller number of children evaluated because some guardians did not take the vaccination cards with them. Thus, Table 2 indicates that the number of doses and the time elapsed between the last vaccination and blood collection were similar among the three groups. No children reported adverse events after receiving the attenuated vaccines evaluated in our study.
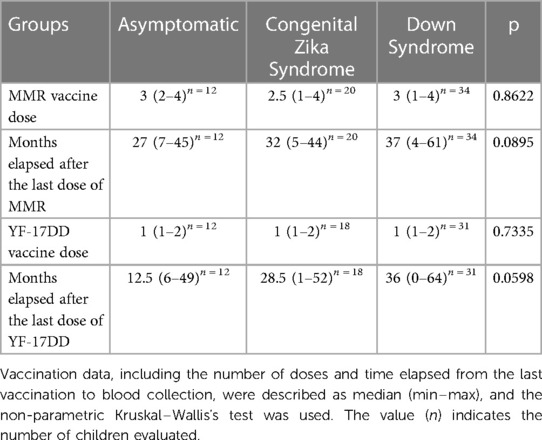
Table 2. Registration of vaccination data of children aged from 2 to 7 years old in Rio de janeiro, Brazil, 2018–2022.
We recategorized children according to the number of doses and duration of vaccination to assess the impact of these two factors on response to vaccine components (Table 3). Data in Table 3 was not statistically significant, however, we consider it an important description. Asymptomatic children and those with CZS who received three or more doses of MMR had a higher median measles IgG and frequency of positivity than those who received one or two doses. The three groups of children who took three or more doses of MMR showed an increase in the median rubella IgG and a higher frequency of positivity than those who took one or two doses, but without statistical difference. Children vaccinated with two doses of YF-17DD showed higher PRNT50 titers and positivity frequency than those who received one dose.
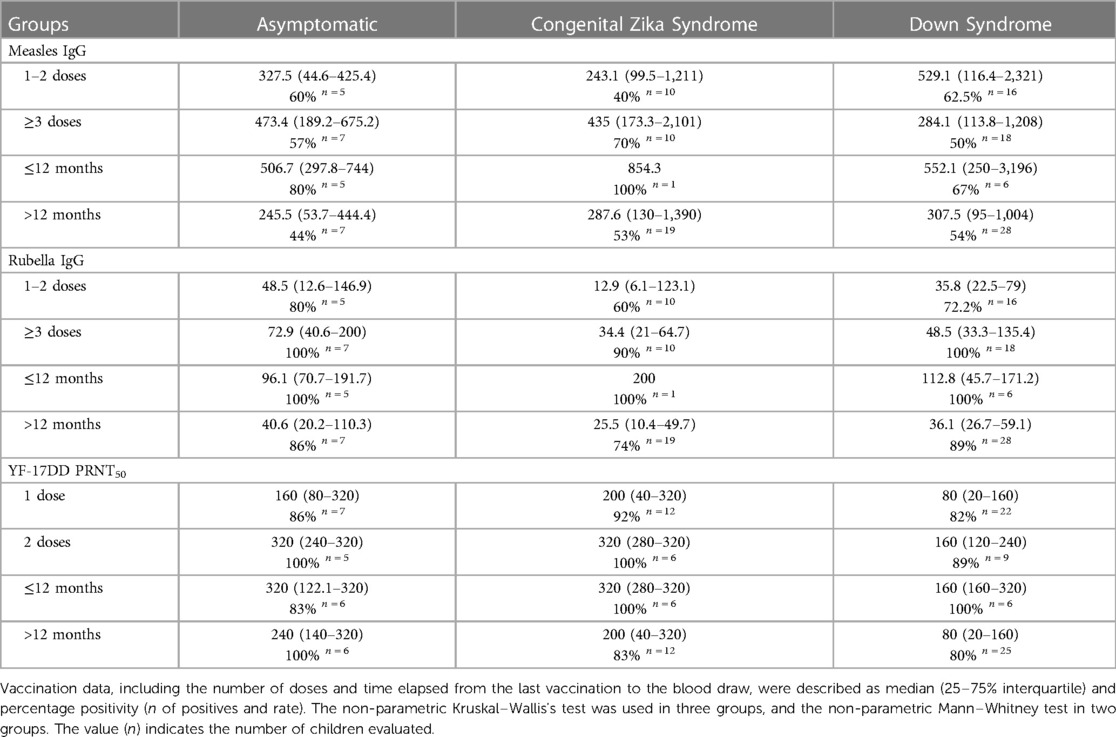
Table 3. Measles (IU/L) and rubella IgG (IU/ml) levels, YF-17DD PRNT50 titer, and positivity based on doses and timing of vaccination in children aged from 2 to 7 years old in Rio de janeiro, Brazil, 2018–2022.
The three groups of children who received the MMR and YF-17DD vaccines up to 12 months had higher levels of IgG and PRNT50, in addition to a higher frequency of positivity than those who were vaccinated more than 12 months ago, but without statistical difference. Even though it was not statistically significant, this data is still encouraging.
Discussion
Vaccination is among the best strategies to reduce infant mortality and morbidity. Even benefiting from vaccination, immunocompromised or a high-risk children's groups need to be constantly assessed regarding the immunogenicity, efficacy/effectiveness and safety of routine vaccines, especially attenuated vaccines. This article aims to compare responses to vaccines against measles, rubella, and yellow fever in children with CZS, DS and asymptomatic controls. Although there are already some studies in children with DS, there are no clear guidelines regarding vaccination in children with CZS. It is important to consider that the mortality rate in children affected by CZS is 11.3 times greater than that in asymptomatic children in the first three years of life (24). It is necessary to evaluate the safety parameters, the protective response and to monitor it, even reassessing the national vaccination calendar to discuss the need for additional doses and shorter vaccination intervals, which could translate into better vaccine responses.
The immunogenicity of some vaccines has been explored in children with DS. Kusters et al. (2011) found that DS children have a decreased anti-tetanus toxoid (TT) humoral immune response, lasting difficulties with specific anti-TT-antibody formation impaired at ages, although “protective levels” for TT are being reached (25). In the same sense, Kusters and colleagues described that only 27% of children with DS who were vaccinated against influenza A/H1N1 achieved a hemagglutination inhibition (HI) titer ≥110 after two doses of the vaccine, this titer was described as sufficient to confer conventional clinical protection (26). Another very interesting study was undertaken by Eijsvoogel et al. The authors demonstrated that children with DS present significantly lower anti-hepatitis B (anti-HBs) titers after hepatitis B vaccination when compared to control children. It is very interesting that up to 3 years of age, 100% of children had a protective anti-HBs titer, but for children over 10 years of age this titer dropped to 31.9% (27). A final study for this discussion was carried out with children with DS and their siblings. All were vaccinated against seasonal flu and received a booster dose of the pneumococcal glycoconjugate vaccine. After primary vaccination, DS children generated significantly fewer memory-specific B cells than their siblings. Following the booster dose, the response was comparable in both groups. Interestingly, specific antibody production was equally effective in SD and controls after primary and secondary immunization (28). In view of the data above published by other authors, vaccination protocols adapted to children with DS are necessary to reduce the burden of infections throughout life. To date, only Influenza, pneumococcal type 23, Varicella-Zoster (VZ), Haemophilus influenzae type b (Hib), hepatitis A (HA) and meningococcal C vaccines have been added/replaced in the routine schedule of children with down syndrome in Brazil (29). It is of great importance to evaluate in DS children the immunogenicity of other vaccines present in the immunization schedule in order to offer better guideline.
Regarding vaccination of CZS children, to date, there are no specific guideline for vaccination and there are few studies published about their immune response to vaccines. The group of Salmeron et al. reported that CZS children showed low tuberculin skin test reactivity after 2 years of BCG vaccination (11). Much like the notion of low tuberculin skin test reactivity in CZS, this response may also translate into other impaired vaccine responses.
The present study is the first to evaluate and compare the serological response in asymptomatic children to CZS and DS children after MMR and YF-17DD vaccination. A very important concern for the scientific community is the potential for immunity against all vaccine components, as is the case with MMR. As is already known and confirmed by Rasheed et al., lower levels of anti-mumps IgG were observed in young adults vaccinated with MMR vaccine compared to rubella levels (30). Because of that, here, we evaluate the response to the rubella and measles components given the epidemiological importance related to the reduction in MMR vaccination coverage in recent years that lead to the increase of confirmed cases of measles infection in Brazil and all over the world (31, 32).
After MMR vaccination, our data demonstrated an anti-measles antibody detection rate below 70% in all three groups of children. Estofolete et al. demonstrated that 60.7% and 79.8% of the children over 10 years old vaccinated with MMR had anti-measles IgG and anti-rubella IgG detected, respectively. These data were like ours, considering that 66.7% of asymptomatic control children were positive to anti-measles IgG. However, higher than those found in children with CZS, which was 54.5%, and in those with DS, which was 55.9%. Another study in Brazil demonstrated a global prevalence of 75.8% of children aged 1–15 years with antibodies against measles. Among children who had some comorbidity (immunosuppression, genetic syndrome, etc.), 72.2% had anti-measles IgG (33). The authors discuss that Brazilian children may have lower detection of IgG against measles than that observed in children from other countries, which is above 90% positivity (34, 35). The authors question the effectiveness of immunization against measles in the Brazilian population in general (36). Another previous study like ours described measles antibody seroprevalence in Mexico in 2012 and risk factors associated with susceptibility. It was a national survey representative of the general population (adults, teenagers, and children). Antibody titers against measles were evaluated by the Plaque Reduction Neutralization Test (PRNT) and classified into protective (>120 mIU/ml) or susceptible (≤120 mIU/ml) levels. The group we were interested in this study were children aged between 1 and 4 years, of which 2.18% were susceptible to measles. The authors concluded that susceptibility was associated with young age, living in Mexico City, living in crowded households, and unknown or unvaccinated status among children ages 1–5 years, and drew attention to the importance of timely administration of the first dose of the vaccine at 12 months of age (37). Therefore, seroprevalence studies in the vaccinated population are important to assess the risks, show the real epidemiological conditions and indicate the reevaluation of the current immunization program in the country.
There are few studies indicating protective limit values for IgG or PRNT antibody titers in vaccinated children for Rubella and Measles. The Rubella Subcommittee of the National Committee on Clinical Laboratory Standards in 1996 proposed the breakpoint for defining rubella immunity of 15 to 10 IU/ml. Beyond this threshold, sporadic cases of viremia and/or reinfection among previously vaccinated people with low antibody levels have been reported. Proven cases of reinfection in people with titers greater than or equal to the 15 IU/ml limit have also been reported. However, the risk is still very small compared to the high risk of rubella infection among unvaccinated people [revised by (38)]. Another study defined 200,000 International Units as the supposed level of protection for clinical measle (39). Here, the commercial kits we use indicate “antibody detection ranges”, but “the protective threshold values of IgG for measles and rubella viruses” were neither established by the kits, nor by us.
Evaluating the rubella response after the MMR vaccination, our data demonstrate that children with CZS and DS had lower IgG titers against rubella than asymptomatic control children, and lower positivity was observed in CZS (72.7%) compared to asymptomatic children (95.8%), although no statistical difference was observed in those with DS (91.2%). Our study did not demonstrate PRNT assays for measles or rubella, which may be of interest to confirm the results obtained in the ELISA assays. On the other hand, we intend to perform an additional assay on in vitro B cell response to measles, rubella, and yellow fever antigens to better understand the humoral response of children with CZS and DS.
Regarding the YFV-17DD vaccination, in all groups, there were children who received only one dose of YF-17DD vaccine. During the 2017 yellow fever outbreak in Brazil, the fractional dose for YF-17DD vaccine was approved for outbreak control due to its ability to induce seroconversion in seronegative participants (40). In addition, maintenance of memory CD4 and CD8 T cells and neutralizing antibodies was observed after 8 years of vaccination with a fractional dose of YF-17DD in adults (41). After ten years, individuals who received the YF-17DD vaccine still had virus-neutralizing antibodies, which motivated the World Health Organization to recommend the administration of a single dose of the YF-17DD vaccine, regardless of the individual's age (42). However, Noronha et al. showed that the proportion of seropositive and titers fell by 28% after 31–72 months and 51% after 73–100 months after the first dose, leaving a substantial proportion of children potentially unprotected (43). The authors highlight the importance of booster doses, especially in children who received the first dose in the first 2 years and reside in areas at risk for yellow fever. Following the study by Noronha et al., a second dose of YF-17DD administered at four years of age was returned to the national immunization schedule. Even so, it maintained the single dose from five years of age onwards. In the same way of MMR vaccination, the protective limit values to PRNT antibody titers in YF-vaccinated adults or children still need to be more discussed. Reis et al. conducted a retrospective study to assess the impact of age on immunity from YF-17DD vaccination. The authors considered an antibody titer ≥100 as a cutoff point and their results demonstrated that seropositivity rates were higher in adults than in children (44). Here, as we evaluated three children known to be unvaccinated by YF-17DD and they presented titers lower than 10, so we considered PRNT50 YF-17DD seropositive when the titer cutoff value was equal or greater than 10. We are still not confident about making a protective cut. Perhaps by using a greater number of samples, in parallel with other experimental approaches with longitudinal studies of response to vaccination, we can assume these values.
Based on the year of fraction-dose application, almost the same year that part of the children received the first YFV-17DD dose, it is possible that the families assumed that the reduced dose in children would follow the same immunological response observed in adults and, therefore, the children ended up not receiving the second dose. Furthermore, the attenuated YF-17DD vaccine is contraindicated to individuals that present congenital or secondary immunodeficiency or thymic diseases (45). As already described, 50% of DS children may have congenital heart problems that require surgical repairs (46). The thymectomy, partial or complete removal of the thymus, is usually associated with early surgical interventions for congenital heart defects in DS children (47). Here, regarding the clinical results of children with DS and consulting their medical records, 29.6% of children underwent cardiac surgery in the first years of life. We cannot guarantee that all 29.6% had their thymus compromised because we do not have access to this data. Furthermore, children with DS had median [25%–75% interquartile] values of 6,220 [5,225–8,480] leukocytes/microliter (µl), while reference values are between 3,600 and 12,000 /µl. For lymphocytes, the DS showed 2,338 [2,038–3,233] cells/µl, and the reference values are between 1,600 and 8,400 /µl. Therefore, both the median leukocyte count, and lymphocyte count in DS children were within reference values. In the case of CZS children, families reported to us during ambulatories follow-up that they found difficulties to vaccinate their children at public health centers since there is no specific protocol to follow CZS cases and YF-17DD could be contraindicated. The lack of previous experience led to limited guidance in CZS care because the knowledge continues to grow along with the children's growth (48, 49). Therefore, scientific research needs to go on to help develop appropriate healthcare guidance for CZS.
Unfortunately, the main limitations of our study were the unavailability of retrieving some medical/vaccination records information from the participants because some guardians did not have the children's vaccination cards at the time of blood collection that leads to a smaller sample size. Because of that, mainly, the understanding of the impact of doses and time elapsed since the last vaccination dose were limited. Additionally, the child recruitment was affected by the COVID-19 pandemic, leading to a smaller sample size than originally proposed. We would like to highlight that this is the first study that evaluate the serological response to MMR and YF-17DD vaccine in CZS and DS children and that this study continues, so we hope to reevaluate some points and reduce its limitations.
Our data draw attention to the need to evaluate children's vaccine response according to age. Moreover, a follow-up in rubella IgG response especially in CZS and DS children is strongly recommended. This work reinforces the need to evaluate the immune response to vaccines offered by the Brazilian national immunization program in CZS and DS children to improve the guidance in healthcare for these children.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statement
The studies involving humans were approved by the Ethics Committee of the Fundação Oswaldo Cruz (CAAE 47358821.6.0000.5248), the Ethics Committee of UFF (CAAE 47358821.6.3001.5243 and CAAE 47358821.6.3001.524) and the Ethics Committee of UERJ (CAAE 47358821.6.3002.5259). Written informed consent for participation in this study was provided by the participants' legal guardians/next of kin. The studies were conducted in accordance with the local legislation and institutional requirements.
Author contributions
Conceptualization, DF-M and Ld-O-P; methodology, DF-M, HD, MO; validation, AP-C, Ld-O-P; formal analysis, DF-M and Ld-O-P; data curation, FC, MS, RB, AB and CC; Writing Original draft preparation, DF-M; writing—review and editing, Ld-O-P; supervision, AP-C, AB, RB, RF, CC, and Ld-O-P; project administration, Ld-O-P; funding acquisition, Ld-O-P. All authors contributed to the article and approved the submitted version.
Funding
Funding was obtained from the Programa de Ações Estratégicas para o Desenvolvimento e Fortalecimento dos Laboratórios Credenciados e das Áreas de Apoio À Pesquisa (PAEF), Edital de geração de conhecimento: COVID-19, Programa Inova Fiocruz (#VPPCB-005-FIO20-2-58), Fundação de Amparo à Pesquisa do Estado do Rio de Janeiro (FAPERJ) (#E-26/211.460/2021); Ld-O-P is a productivity fellow by the Conselho Nacional de Desenvolvimento Científico e Tecnológico (CNPq) (#309367/2021-2); CNPq and the Coordenação de Aperfeiçoamento de Pessoal de Nível Superior (CAPES) financed scholarships for DF-M and HD.
Acknowledgments
We would like to thank the families and hospital staff from the ZIKA project and families from Ambulatório Multidisciplinar de Síndrome de Down for participation in this project. We are grateful to the contribution made by Sariane Marçal de Jesus, Gabriela Gomes Vieira and Natany Ezequiel Santos from Ambulatório Multidisciplinar de Síndrome de Down, Natália Valente for the support with Vero cell culture and the Laboratório de Mosquitos Transmissores de Hematozoários (LATHEMA)-Fiocruz for the strain YF-17DD donation.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Shukla VV, Shah RC. Vaccinations in primary care. Indian J Pediatr. (2018) 85(December):1118–27. doi: 10.1007/s12098-017-2555-2
2. Centers for Disease Control and Prevention (CDC). Ten great public health achievements—United States, 1900–1999. Morb Mortal Wkly Rep. (1999) 48(12):241–3.
3. Alkema L, Chao F, You D, Pedersen J, Sawyer CC. National, regional, and global sex ratios of infant, child, and under-5 mortality and identification of countries with outlying ratios: a systematic assessment. Lancet Glob Health. (2014) 2(9):e521–30. doi: 10.1016/S2214-109X(14)70280-3
4. UNICEF. Under-five Mortality. Available at: https://data.unicef.org/topic/child-survival/under-five-mortality/ (Cited June 12, 2023).
5. Freitas DA, Souza-Santos R, Carvalho LMA, Barros WB, Neves LM, Brasil P, et al. Congenital Zika syndrome: a systematic review. PLoS One. (2020) 15:1–27. doi: 10.1371/journal.pone.0242367
6. Marbán-Castro E, Goncé A, Fumadó V, Romero-Acevedo L, Bardají A. Zika virus infection in pregnant women and their children: a review. Eur J Obstet Gynecol Reprod Biol. (2021) 265:162–8. doi: 10.1016/j.ejogrb.2021.07.012
7. de Vries LS. Viral infections and the neonatal brain. Semin Pediatr Neurol. (2019) 32:100769. doi: 10.1016/j.spen.2019.08.005
8. Massetti T, Herrero D, Alencar J, Silva T, Moriyama C, Gehrke F, et al. Clinical characteristics of children with congenital Zika syndrome: a case series. Arq Neuropsiquiatr. (2020) 78(7):403–11. doi: 10.1590/0004-282X20200020
9. Badolato-Corrêa J, Carvalho FR, Paiva IA, Familiar-Macedo D, Dias HG, Pauvolid-Corrêa A, et al. Differential longevity of memory CD4 and CD8 T cells in a cohort of the mothers with a history of ZIKV infection and their children. Front Immunol. (2021) 12:1–17. doi: 10.3389/fimmu.2021.610456
10. Paiva IA, Familiar-Macedo D, Badolato-Corrêa J, Carvalho FR, Dias HG, Pauvolid-Corrêa A, et al. Involvement of Th1Th17 cell subpopulations in the immune responses of mothers who gave birth to children with congenital Zika syndrome (CZS). Viruses. (2022) 14(2):1–24. doi: 10.3390/v14020250
11. Salmeron ACA, Bezerra WP, de Souza RLL, Pereira LC, do Nascimento LM, Branco ACCC, et al. Immunological imbalance in microcephalic children with congenital Zika virus syndrome. Med Microbiol Immunol. (2022) 211(5–6):219–35. doi: 10.1007/s00430-022-00746-5
12. Ram G, Chinen J. Infections and immunodeficiency in down syndrome. Clin Exp Immunol. (2011) 164(1):9–16. doi: 10.1111/j.1365-2249.2011.04335.x
13. Antonarakis SE, Skotko BG, Rafii MS, Strydom A, Pape SE, Bianchi DW, et al. Down syndrome. Nat Rev Dis Primers. (2020) 6(1):1–43. doi: 10.1038/s41572-019-0143-7
14. Danopoulos S, Deutsch GH, Dumortier C, Mariani TJ, Al Alam D. Lung disease manifestations in down syndrome. Am J Physiol Lung Cell Mol Physiol. (2021) 321(5):L892–9. doi: 10.1152/ajplung.00434.2020
15. Cruz NV, Mahmoud SA, Chen H, Lowery-Nordberg M, Berlin K, Bahna SL. Follow-up study of immune defects in patients with dysmorphic disorders. Ann Allergy Asthma Immunol. (2009) 102(5):426–31. doi: 10.1016/S1081-1206(10)60516-9
16. Joshi AY, Abraham RS, Snyder MR, Boyce TG. Immune evaluation and vaccine responses in down syndrome: evidence of immunodeficiency? Vaccine. (2011) 29(31):5040–6. doi: 10.1016/j.vaccine.2011.04.060
17. Ministério da Saúde. Manual dos Centros de Referência para Imunobiológicos Especiais (2019). Available at: http://bvsms.saude.gov.br/bvs/publicacoes/manual_centros_imunobiologicos_ (Accessed June 18, 2023).
18. Huggard D, Doherty DG, Molloy EJ. Immune dysregulation in children with down syndrome. Front Pediatr. (2020) 8:1–10. doi: 10.3389/fped.2020.00073
19. Ministério da Saúde. Calendário Nacional de Vacinação—Ministério da Saúde (2022). Available at: https://www.gov.br/saude/pt-br/assuntos/saude-de-a-a-z/c/calendario-nacional-de-vacinacao (Accessed June 12, 2023).
20. Ministério da Saúde. Calendário Nacional de Vacinação Infantil (2022). Available at: https://www.gov.br/saude/pt-br/assuntos/saude-de-a-a-z/c/calendario-nacional-de-vacinacao/calendario-vacinal-2022/anexo-calendario-de-vacinacao-da-crianca_atualizado_-final-20-09-2022.pdf (Accessed June 6, 2023).
21. Calendários de Vacinação Pacientes Especiais 2022–2023. Available at: https://sbim.org.br/images/calendarios/calend-sbim-pacientes-especiais.pdf (Accessed June 27, 2023).
22. Simões M, Camacho LAB, Yamamura AMY, Miranda EH, Cajaraville ACRA, da Silva Freire M. Evaluation of accuracy and reliability of the plaque reduction neutralization test (micro-PRNT) in detection of yellow fever virus antibodies. Biologicals. (2012) 40(6):399–404. doi: 10.1016/j.biologicals.2012.09.005
23. Baer A, Kehn-Hall K. Viral concentration determination through plaque assays: using traditional and novel overlay systems. J Vis Exp. (2014) 93:52065. doi: 10.3791/52065
24. Paixao ES, Cardim LL, Costa MDCN, Brickley EB, Carvalho-Sauer RDCOD, Carmo EH, et al. Congenital Zika syndrome: a nationwide cohort study in Brazil, 2015–2018. N Engl J Med. (2022) 386(8):757. doi: 10.1056/NEJMoa2101195
25. Kusters MA, Jol-Van Der Zijde CM, Van Tol MJ, Bolz WE, Bok LA, Visser M, et al. Impaired avidity maturation after tetanus toxoid booster in children with down syndrome. Pediatr Infect Dis J. (2011) 30(4):357–9. doi: 10.1097/INF.0b013e3181ff85a8
26. Kusters MA, Bok VLA, Bolz WEA, Huijskens EGW, Peeters MF, De Vries E. Influenza A/H1N1 vaccination response is inadequate in down syndrome children when the latest cut-off values are used. Pediatr Infect Dis J. (2012) 31(12):1284–5. doi: 10.1097/INF.0b013e3182737410
27. Eijsvoogel NB, Hollegien MI, Bok VLA, Derksen-Lubsen AG, Dikken FPJ, Leenders SACAP, et al. Declining antibody levels after hepatitis B vaccination in down syndrome: a need for booster vaccination? J Med Virol. (2017) 89(9):1682–5. doi: 10.1002/jmv.24813
28. Valentini D, Marcellini V, Bianchi S, Villani A, Facchini M, Donatelli I, et al. Generation of switched memory B cells in response to vaccination in down syndrome children and their siblings. Vaccine. (2015) 33(48):6689–96. doi: 10.1016/j.vaccine.2015.10.083
29. Brasil. Ministério da Saúde. Secretaria de Vigilância em Saúde. Departamento de Imunização e Doenças Transmissíveis. Manual dos Centros de Referência para Imunobiológicos Especiais [recurso eletrônico]/Ministério da Saúde, Secretaria de Vigilância em Saúde, Departamento de Imunização e Doenças Transmissíveis, Coordenação-Geral do Programa Nacional de Imunizações.—5. ed.—Brasília: Ministério da Saúde, 2019.
30. Rasheed MAU, Hickman CJ, McGrew M, Sowers SB, Mercader S, Hopkins A, et al. Decreased humoral immunity to mumps in young adults immunized with MMR vaccine in childhood. Proc Natl Acad Sci U S A. (2019) 116(38):19071–6. doi: 10.1073/pnas.1905570116
31. Godin A, Pescarini JM, Raja AI, Paixao ES, Ichihara MY, Sato APS, et al. Municipality-level measles, mumps, and rubella (MMR) vaccine coverage and deprivation in Brazil: a nationwide ecological study, 2006 to 2020. PLOS Glob Public Health. (2023) 3(8):e0002027. doi: 10.1371/journal.pgph.0002027
32. Pan American Health Organization/World Health Organization. Epidemiological update: Measles. Washington, D.C.: PAHO/WHO (2020). Available at: https://www.paho.org/en/documents/epidemiological-update-measles-28-february-2020 (Cited November 01, 2023).
33. Estofolete CF, de Andrade Gandolfi F, de Aguiar Milhim BH, da Silva GCD, Dourado FS, dos Santos BF, et al. Reduced prevalence of measles antibodies in a cohort of Brazilian children under 15 years of age. Vaccines (Basel). (2022) 10(10):1570–8. doi: 10.3390/vaccines10101570
34. Lebo EJ, Kruszon-Moran DM, Marin M, Bellini WJ, Schmid S, Bialek SR, et al. Seroprevalence of measles, mumps, rubella and varicella antibodies in the United States population, 2009–2010. Open Forum Infect Dis. (2015) 2(1):1–5. doi: 10.1093/ofid/ofv006
35. Prymula R, Povey M, Brzostek J, Cabrnochova H, Chlibek R, Czajka H, et al. Ten-year follow-up on efficacy, immunogenicity and safety of two doses of a combined measles-mumps-rubella-varicella vaccine or one dose of monovalent varicella vaccine: results from five East European countries. Vaccine. (2021) 39(19):2643–51. doi: 10.1016/j.vaccine.2021.03.085
36. Estofolete CF, Milhim BHGA, de França CCG, da Silva GCD, Augusto MT, Terzian ACB, et al. Prevalence of measles antibodies in São José do Rio Preto, São Paulo, Brazil: a serological survey model. Sci Rep. (2020) 10(1):1–8. doi: 10.1038/s41598-020-62151-3
37. Díaz-Ortega JL, Ferreira-Guerrero E, Cruz-Hervert LP, Delgado-Sánchez G, Ferreyra-Reyes L, Yanes-Lane M, et al. Seroprevalence of measles antibodies and factors associated with susceptibility: a national survey in Mexico using a plaque reduction neutralization test. Sci Rep. (2020) 10(1):17488. doi: 10.1038/s41598-020-73618-8
38. Skendzel LP. Rubella immunity. Defining the level of protective antibody. Am J Clin Pathol. (1996) 106(2):170–4. doi: 10.1093/ajcp/106.2.170
39. Miller E, Hill A, Morgan-Capner P, Forsey T, Rush M. Antibodies to measles, mumps and rubella in UK children 4 years after vaccination with different MMR vaccines. Vaccine. (1995) 13(9):799–802. doi: 10.1016/0264-410x(94)00086-3
40. Casey RM, Harris JB, Ahuka-Mundeke S, Dixon MG, Kizito GM, Nsele PM, et al. Immunogenicity of fractional-dose vaccine during a yellow fever outbreak—final report. N Engl J Med. (2018) 381(5):444–54. doi: 10.1056/nejmoa1710430
41. Da Costa-Rocha IA, Campi-Azevedo AC, Peruhype-Magalhães V, Coelho-Dos-Reis JG, Fradico JRB, Souza-Lopes T, et al. Duration of humoral and cellular immunity 8 years after administration of reduced doses of the 17DD-yellow fever vaccine. Front Immunol. (2019) 10:1211. doi: 10.3389/fimmu.2019.01211
42. Vaccines and vaccination against yellow fever. WHO position paper—june 2013. Wkly Epidemiol Rec. (2013) 88(27):269–83. Available at: https://pubmed.ncbi.nlm.nih.gov/23909008/23909008
43. de Noronha TG, de Lourdes de Sousa Maia M, Geraldo Leite Ribeiro J, Campos Lemos JA, Maria Barbosa de Lima S, Martins-Filho OA, et al. Duration of post-vaccination humoral immunity against yellow fever in children. Vaccine. (2019) 37(48):7147–54. doi: 10.1016/j.vaccine.2019.09.051
44. Reis LR, Costa-Rocha IAD, Campi-Azevedo AC, Peruhype-Magalhães V, Coelho-Dos-Reis JG, Costa-Pereira C, et al. Exploratory study of humoral and cellular immunity to 17DD yellow fever vaccination in children and adults residents of areas without circulation of yellow fever virus. Vaccine. (2022) 40(5):798–810. doi: 10.1016/j.vaccine.2021.12.029
45. Instituto de Tecnologia em Imunobiológicos—BIO-MANGUINHOS, Fundação Oswaldo Cruz. Bula da vacina febre amarela (atenuada) 5 e 10 doses. Available at: https://www.bio.fiocruz.br/en/images/stories/pdfs/bulas/fa/BM_BUL_045_00_V_190702_FA10Nacional.pdf (Accessed June 12, 2023).
46. Benhaourech S, Drighil A, El Hammiri A. Congenital heart disease and down syndrome: various aspects of a confirmed association. Cardiovasc J Afr. (2016) 27(5):287–90. doi: 10.5830/CVJA-2016-019
47. Stosio M, Ruszkowski J, Mikosik-Roczyńska A, Haponiuk I, Witkowski JM. The significance of neonatal thymectomy for shaping the immune system in children with congenital heart defects. Kardiochir Torakochirurgia Pol. (2017) 14(4):258. doi: 10.5114/kitp.2017.72231
48. Russell K, Oliver SE, Lewis L, Barfield WD, Cragan J, Meaney-Delman D, et al. Update: interim guidance for the evaluation and management of infants with possible congenital Zika virus infection—united States, August 2016. MMWR Morb Mortal Wkly Rep. (2019) 65(33):870–8. doi: 10.15585/mmwr.mm6533e2
Keywords: Congenital Zika Syndrome, down syndrome, immunogenicity, MMR vaccine, YF-17DD vaccine
Citation: Familiar-Macedo D, Dias HG, Carvalho FR, Pauvolid-Corrêa A, da Silveira MN, Oliveira MCd, Gonçalves RdCF, Vianna RAdO, Cardoso CAA, Boy da Silva RT, Baumblatt AP and de-Oliveira-Pinto LM (2023) Serological investigation of vaccine-induced antibodies for measles, rubella, and yellow fever viruses in children vertically exposed to Zika virus or with down syndrome. Front. Pediatr. 11:1250059. doi: 10.3389/fped.2023.1250059
Received: 29 June 2023; Accepted: 28 November 2023;
Published: 14 December 2023.
Edited by:
Nicola Cotugno, Bambino Gesù Children's Hospital (IRCCS), ItalyReviewed by:
Jeffrey Connell, University College Dublin, IrelandMaaike Kusters, Great Ormond Street Hospital, United Kingdom
© 2023 Familiar-Macedo, Dias, Carvalho, Pauvolid-Corrêa, da Silveira, Oliveira, Gonçalves, Vianna, Cardoso, Boy da Silva, Baumblatt and de-Oliveira-Pinto. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Débora Familiar-Macedo ZGVib3JhZmFtaWxpYXJAZ21haWwuY29t Luzia Maria de-Oliveira-Pinto bHBpbnRvQGlvYy5maW9jcnV6LmJy