 Ivan Gutierrez-Tobar1,2,3*
Ivan Gutierrez-Tobar1,2,3* Cristobal Carvajal3,4
Cristobal Carvajal3,4 Pablo Vasquez-Hoyos3,5,6,7
Pablo Vasquez-Hoyos3,5,6,7 Alejandro Díaz-Díaz3,8,9
Alejandro Díaz-Díaz3,8,9 Juan Pablo Londono Ruiz2,3
Juan Pablo Londono Ruiz2,3 Joam Andrade3,10
Joam Andrade3,10 Jhon Camacho-Cruz3,5,6,7,11,12Andrea Restrepo-Gouzy8Monica Trujillo-Honeysberg8Juan Gonzalo Mesa-Monsalve13
Jhon Camacho-Cruz3,5,6,7,11,12Andrea Restrepo-Gouzy8Monica Trujillo-Honeysberg8Juan Gonzalo Mesa-Monsalve13 Ignacio Perez14
Ignacio Perez14 Richard Von Moltke3,4
Richard Von Moltke3,4 Maria Beltran-Echeverry1,3,7Jessica F. Toro15Angela P. Niño15
Maria Beltran-Echeverry1,3,7Jessica F. Toro15Angela P. Niño15 Germán Camacho-Moreno16,17Juan Pablo Calle-Giraldo18,19,20Nancy Yhomara Cabeza18Lina Marcela Sandoval-Calle21
Germán Camacho-Moreno16,17Juan Pablo Calle-Giraldo18,19,20Nancy Yhomara Cabeza18Lina Marcela Sandoval-Calle21 Paola Perez Camacho21Jaime Patiño Niño21Paula Araque-Muñoz22,23
Paola Perez Camacho21Jaime Patiño Niño21Paula Araque-Muñoz22,23 Yazmin Rodríguez-Peña22,23Claudia Beltran-Arroyave24
Yazmin Rodríguez-Peña22,23Claudia Beltran-Arroyave24 Yamile Chaucanez-Bastidas25
Yamile Chaucanez-Bastidas25 Juan Lopez16Diego Galvis-Trujillo16
Juan Lopez16Diego Galvis-Trujillo16 Sandra Beltrán-Higuera26,27
Sandra Beltrán-Higuera26,27 Ana-Cristina Marino10Natalia González Leal28Miguel Ángel Luengas Monroy10Derly Carolina Hernandez-Moreno10
Ana-Cristina Marino10Natalia González Leal28Miguel Ángel Luengas Monroy10Derly Carolina Hernandez-Moreno10 Rosalba Vivas Trochez29,30Carlos Garces31
Rosalba Vivas Trochez29,30Carlos Garces31 Eduardo López-Medina32,33,34
Eduardo López-Medina32,33,34
- 1Department of Pediatrics, Clínica Infantil Santa Maria Del Lago, Bogotá, Colombia
- 2Department of Pediatrics, Clinica Infantil Colsubsidio, Bogotá, Colombia
- 3Staphylored LATAM, Bogotá, Colombia
- 4Universidad Finis Terrae, Santiago, Chile
- 5Department of Pediatrics, Fundacion Universitaria de Ciencias de la Salud (FUCS), Bogotá, Colombia
- 6Universidad Nacional de Colombia, Bogotá, Colombia
- 7Sociedad de Cirugía de Bogotá Hospital de San Jose, Bogotá, Colombia
- 8Department of Pediatrics, Hospital Pablo Tobon Uribe, Medellín, Colombia
- 9Department of Pediatrics, Hospital General de Medellín, Medellín, Colombia
- 10Department of Pediatrics, Hospital Militar Central, Bogotá, Colombia
- 11Department of Pediatrics, Fundación Universitaria Sanitas, Bogotá, Colombia
- 12Department of Pediatrics, Clínica Reina Sofia Pediátrica y Mujer, Bogotá, Colombia
- 13Clínica Las Americas, AUNA, Unidad de Enfermedades Infecciosas, Medellín, Colombia
- 14Universidad de los Andes, Santiago, Chile
- 15Department of Pediatrics, Clínica Medilaser, Neiva, Colombia
- 16Department of Pediatrics, Fundación Hospital de La Misericordia, Bogotá, Colombia
- 17Department of Pediatrics, Hospital Universitario Infantil de San José, Bogotá, Colombia
- 18Department of Pediatrics, Hospital San Juan de Dios, Armenia, Colombia
- 19Department of Pediatrics, Clinica Farallones, Cali, Colombia
- 20Department of Pediatrics, Clinica Versalles, Cali, Colombia
- 21Department of Pediatrics, Fundación Valle de Lili, Cali, Colombia
- 22Department of Pediatrics, Clinica Country, Bogotá, Colombia
- 23Department of Pediatrics, Clinica La Colina, Bogotá, Colombia
- 24Department of Pediatrics, Clinica El Rosario, Medellín, Colombia
- 25Department of Pediatrics, Hospital Infantil Los Ángeles, Pasto, Colombia
- 26Clinica Colsanitas, Bogotá, Colombia
- 27Department of Pediatrics, Clinica infantil Colsanitas, Bogotá, Colombia
- 28Independent Researcher, Manizales, Colombia
- 29Department of Pediatrics, Clínica Soma, Medellín, Colombia
- 30Department of Pediatrics, Hospital Universitario de San Vicente Fundación, Medellín, Colombia
- 31Department of Pediatrics, Clinica Cardiovid Medellín, Medellin, Colombia
- 32Centro de Estudios en Infectología Pediátrica, Cali, Colombia
- 33Universidad del Valle, Cali, Colombia
- 34Department of Pediatrics, Clínica Imbanaco, Cali, Colombia
Background: Staphylococcus aureus infections are a significant cause of morbidity and mortality in pediatric populations worldwide. The Staphylo Research Network conducted an extensive study on pediatric patients across Colombia from 2018 to 2021. The aim of this study was to describe the epidemiological and microbiological characteristics of S. aureus in this patient group.
Methods: We analyzed S. aureus isolates from WHONET-reporting centers. An “event” was a positive culture isolation in a previously negative individual after 2 weeks. We studied center characteristics, age distribution, infection type, and antibiotic susceptibilities, comparing methicillin sensitive (MSSA) and resistant S. aureus (MRSA) isolates.
Results: Isolates from 20 centers across 7 Colombian cities were included. Most centers (80%) served both adults and children, with 55% offering oncology services and 85% having a PICU. We registered 8,157 S. aureus culture isolations from 5,384 events (3,345 MSSA and 1,961 MRSA) in 4,821 patients, with a median age of 5 years. Blood (26.2%) and skin/soft tissue (18.6%) were the most common infection sources. Most isolates per event remained susceptible to oxacillin (63.2%), clindamycin (94.3%), and TMP-SMX (98.3%). MRSA prevalence varied by city (<0.001), with slightly higher rates observed in exclusively pediatric hospitals. In contrast, the MRSA rate was somewhat lower in centers with Antimicrobial Stewardship Program (ASP). MRSA was predominantly isolated from osteoarticular infections and multiple foci, while MSSA was more frequently associated with recurrent infections compared to MRSA.
Conclusions: This is the largest study of pediatric S. aureus infections in Colombia. We found MSSA predominance, but resistance have important regional variations. S. aureus remains susceptible to other commonly used antibiotics such as TMP-SMX and clindamycin. Ongoing monitoring of S. aureus infections is vital for understanding their behavior in children. Prospective studies within the Staphylored LATAM are underway for a more comprehensive clinical and genetic characterization.
Introduction
Pediatric infections caused by Staphylococcus aureus represent a significant global public health issue (1). These infections span a spectrum of severity, from mild skin and soft tissue infections to more serious conditions including disseminated disease with multiorgan failure and high mortality risk (2). Clinical studies suggest that the epidemiology, susceptibility profiles, and severity of S. aureus infections can vary according to population demographics and resistance patterns (3–5).
Regional differences exist in the prevalence of Methicillin-Sensitive (MSSA) and Methicillin-Resistant Staphylococcus aureus (MRSA) (3, 4, 6, 7). While MSSA predominates in certain European regions (6). In the United States, a meta-analysis of children and adults from studies spanning 1990 to 2012 found a range of MRSA prevalence in different regions, reaching a maximum of 83% (8) Other regional variations in susceptibility profiles to different antibiotics, such as clindamycin and TMP-SMX, have also been observed (9, 10). In addition, antibiotic susceptibility patterns have shown significant variations over time, with a surge in MRSA infections observed in the 2000s, and more recent reports indicate a resurgence of MSSA (3, 11, 12). Differential severity of infections and prognosis according to susceptibility patterns are conflicting. Infections caused by MRSA strains are often more severe, a trend that has been observed in Colombia and other regions (2, 13, 14).
The increasing prevalence of Staphylococcus aureus infections in pediatric populations raises significant concerns. A notable gap exists in local comprehensive, multicentric, and longitudinal studies that cover both MSSA and MRSA cases. This study is designed to determine the frequency and antibiotic susceptibility of pediatric S. aureus infections, as well as their epidemiological profiles. Furthermore, it aims to investigate regional variations in antibiotic resistance and identify temporal trends, including changes in the prevalence of resistance to various antibiotics among diverse S. aureus infections in different Colombian cities. By examining regional differences in infection severity and utilizing robust multicentric epidemiological data, this study seeks to provide a comprehensive overview of Staphylococcus aureus infections in the pediatric population. The findings are anticipated to have significant relevance both locally in Colombia and regionally, particularly in regions confronting similar challenges with S. aureus infections.
Materials and methods
Study design and patient selection
This was a retrospective observational study conducted from 2018 to 2021, including episodes of S. aureus isolations from either sterile (blood, pleural fluid, cerebrospinal fluid, peritoneal fluid, osteomuscular or articular fluid obtained during surgical procedures) or non-sterile sites (i.e., respiratory specimens, soft tissue abscesses) in patients under 18 years of age. Data were identified and gathered using the WHONET software, a widely used tool in Colombian hospitals developed by the World Health Organization for managing microbiology data (15).
Data collection and management
Study data were collected and managed using REDCap electronic data capture tools hosted at Universidad Finis Terrae in Chile (16, 17). Hospital's participation workflow in REDCap started with email invitations to institutional referents. Each center then completed an online survey with institution characterization and uploaded four WHONET's export files (one per year). To ensure accuracy, written instructions, and a video tutorial on exporting data from WHONET were provided. A semi-automatic reactive workflow with data validations and email alerts was designed in REDCap to optimize time, security, privacy, and data quality. Online-local connections were supported through APIs (Application Programming Interfaces, which are sets of rules enabling software interactions).
Data processing and standardization
The data processing involved a systematic approach: downloading REDCap and WHONET files for each center, followed by data cleansing and normalization into the study format using R/Python. This process included standardizing WHONET data's free texts (origin, specimen, and ward type) and converting Minimum Inhibitory Concentration (MIC) free text values into clinical interpretations (susceptible, intermediate, resistant), according to CLSI recommendations (18).
Data were aggregated at a patient-center level, and a 2-week interval was calculated for each event per patient per center. The refined WHONET data was then uploaded to a separate REDCap project for positive S. aureus culture results. Biomedical Informatics MDs collaborated with Pediatric Infectious Diseases specialists in iterative data engineering cycles. Tools used included two REDCap projects, Microsoft Excel, Google Sheets, R, and Python. An independent analysis team was employed to minimize bias.
Definitions
A culture was defined as the identification of an S. aureus isolate, irrespective of its origin or if it was a repeated identification. Patients refers to individuals with at least one positive S. aureus culture. An event was defined as any instance with at least one positive S. aureus culture. Subsequent cultures within 14 days of the last positive culture were considered part of the same event, with each positive culture extending this window by an additional 14 days. A source was defined as the origin of body sites from which the isolate was identified. An event can have multiple sources, indicating that an isolate was identified from more than one body origin.
Detailed information collection
All positive S. aureus cultures were included, and information on specimen type, culture origin, identification methods, resistance patterns, culture origins, and MIC values was obtained. Patient characteristics collected included age, institution type, capacity, services offered, bed numbers, geographical regions, cities, and other indicators.
Ethical considerations
Participating centers obtained local ethical approval. The REDCap web platform was used for secure, anonymous data management, with decoding handled by the REDCap administrator at Finis Terrae University. This ensured data protection and security throughout the study.
Statistical analysis
A non-probabilistic convenience sampling method was employed. We performed a descriptive analysis, presenting qualitative variables with absolute and relative frequencies, and quantitative variables with medians and IQR. Categorical variables were analyzed by case numbers and percentages. χ2 tests, following variance distribution analysis, were used to compare MSSA and MRSA, with statistical significance set at p < 0.05. All analyses were conducted using STATA® version 17.
Results
Twenty centers from seven Colombian cities participated in the study. Most were private (17/20), cared for children and adults (16/20), had pediatric surgical services, pediatric intensive care unit (PICUs), and neonatal units. Sixteen centers performed molecular tests for S. aureus and resistance genes, and seventeen used therapeutic drug monitoring of vancomycin. Most had infectious disease departments, infection control programs, and Antimicrobial Stewardships Programs (ASPs), with variable distribution in the number of Infectious Disease specialists per bed per service (Table 1).
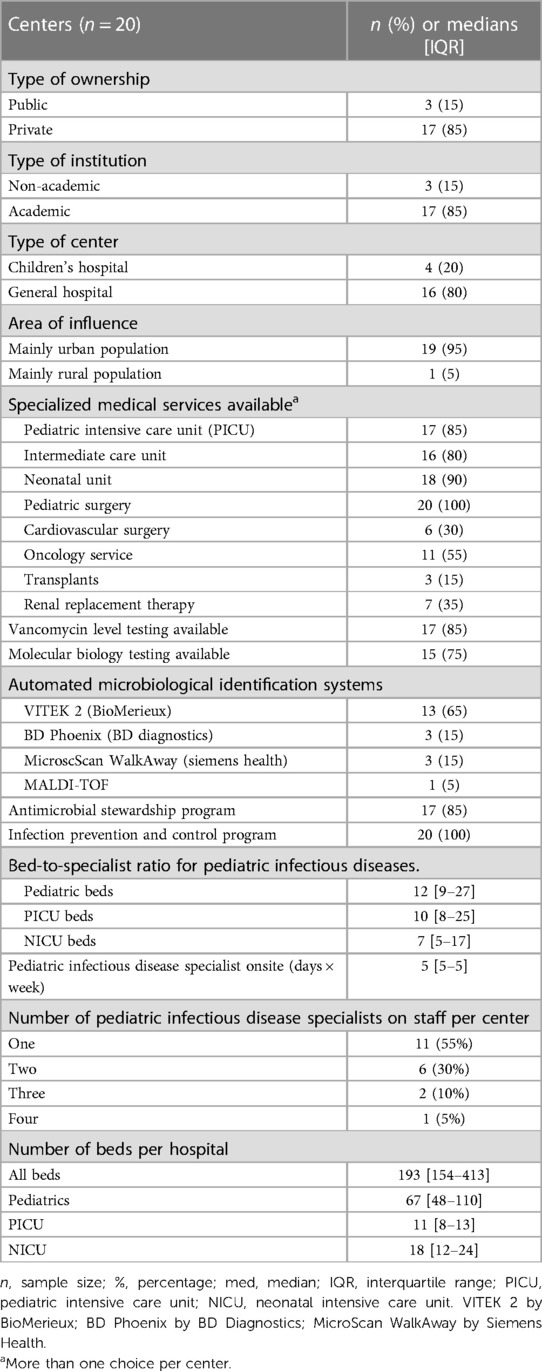
Table 1. Centers and resources for infectious diseases: key characteristics.
For the analysis, 5,384 events were included from 8,157 cultures of S. aureus that occurred in 4,821 patients (Figure 1). In the analyzed events, a total of 3,345 isolates of MSSA and 1,961 of MRSA were identified.
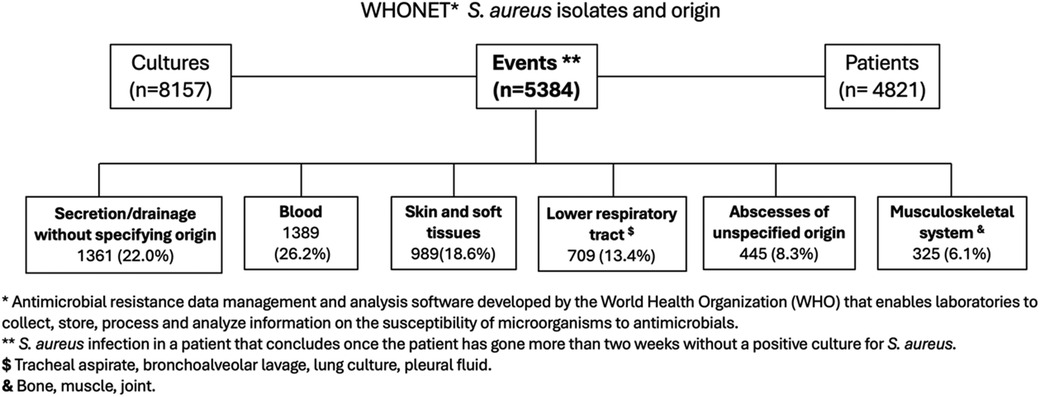
Figure 1. Source of S. aureus pediatric infections.
Blood was identified as the most frequent source, representing 1,389 (26.2%) events. Among these, 571 events (41.1%) were associated with an additional identified focus. Specifically, in 159 (27.8%), the associated focus was secretion or drainage of unidentified origin; in 119 (20.8%) events, the source was osteomuscular; and in 74 (12.9%), it originated from skin and soft tissues. Additionally, there were 989 (18.6%) events of skin and soft tissue infections and 709 (13.4%) events of lower respiratory tract infections.
Significant differences in MRSA frequency were evident across different cities (p < 0.001), with Neiva (53.8%) and Armenia (48.8%) reporting higher rates in contrast to Manizales (25.8%) and Medellín (30%). Additionally, a slight increase in the frequency of MSSA was noted among neonates compared to other age groups, as detailed in Table 2A.
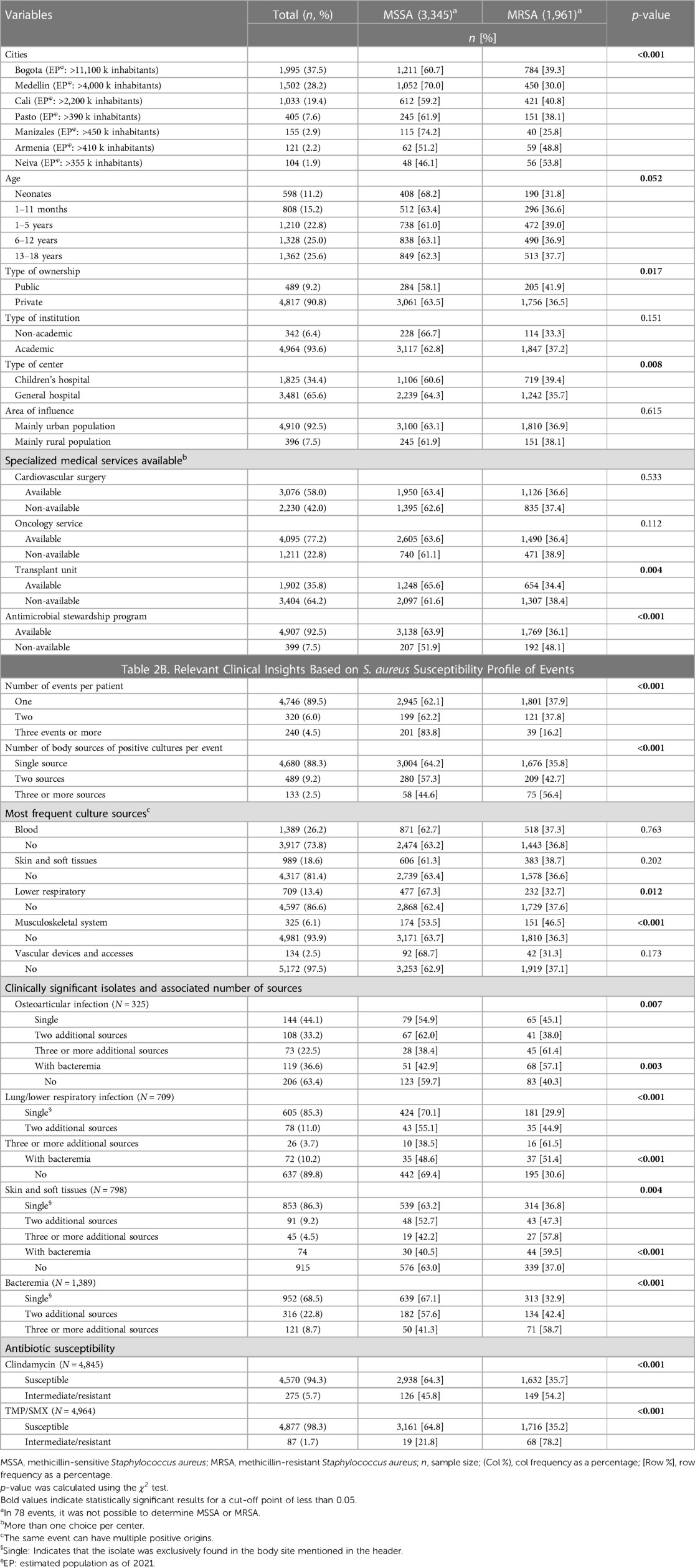
Table 2. (A) Comparison of MSSA vs. MRSA event frequencies based on center characteristics and population. (B) Relevant clinical insights based on S. aureus susceptibility profile of events.
The median age of the patients was 5 years, with a min-max age range of 1–12 years. The age group with the highest prevalence included adolescents aged 13–18, accounting for 1,362 (25.6%) events, closely followed by the 6–12 years age group with 1,328 (25.0%) events.
The prevalence of MSSA compared to MRSA varied across different healthcare settings. In private centers, MSSA was more prevalent than in public centers (63.5% vs. 58.1%, p = 0.017). A similar pattern was observed when comparing general hospitals to pediatric hospitals (64.3% vs. 60.6%, p = 0.008), and in centers with transplant units (65.6% vs. 61.6%, p = 0.004). The presence of Antimicrobial Stewardship Programs (ASP) correlated with a higher frequency of MSSA compared to centers without ASP (63.9% vs. 51.9%, p < 0.001). However, the prevalence of MSSA vs. MRSA did not significantly differ based on urban or rural care settings or university affiliation, as detailed in Table 2A.
The frequency of MSSA vs. MRSA was similar in patients with single events (62.1% vs. 37.9%) and those with two events (62.2% vs. 37.8%). However, the presence of three events or more was associated with a higher frequency of MSSA (83.8% vs. 16.2%, p < 0.001). In contrast, MRSA was more frequent if three or more body sources had a positive culture during the same event (56.4 vs. 44.6%, p < 0.001).
While MSSA was more commonly detected across various culture sources, the identification of a pulmonary origin was significantly more associated with MSSA (p = 0.012). In contrast, musculoskeletal origins had a higher association with MRSA (p < 0.001) compared to other infection sites. Regardless of the body source of the infection, as the number of identified additional sources increased to three or more, the relationship inverted, resulting in a higher frequency of MRSA identification. Similarly, the presence of bacteremia was more frequently associated with MRSA. Regarding antibiotic susceptibility, clindamycin and TMP/SMX demonstrated high susceptibility against S. aureus, irrespective of the resistance profile. Nevertheless, MRSA isolates demonstrated a significantly higher resistance level when compared to MSSA isolates. Specifically, resistance to clindamycin was documented at 4.1% in MSSA, which increased to 8.4% in MRSA isolates. In a similar trend, resistance rates for TMP-SMX rose from 0.6% in MSSA to 3.8% in MRSA (p < 0.001), Table 2B.
Variations in antibiotic susceptibility among Staphylococcus aureus isolates were evident across different cities, as detailed in Supplementary Figure S1. No significant variations in antibiotic susceptibility were observed throughout the duration of the study, as illustrated in Figure 2.
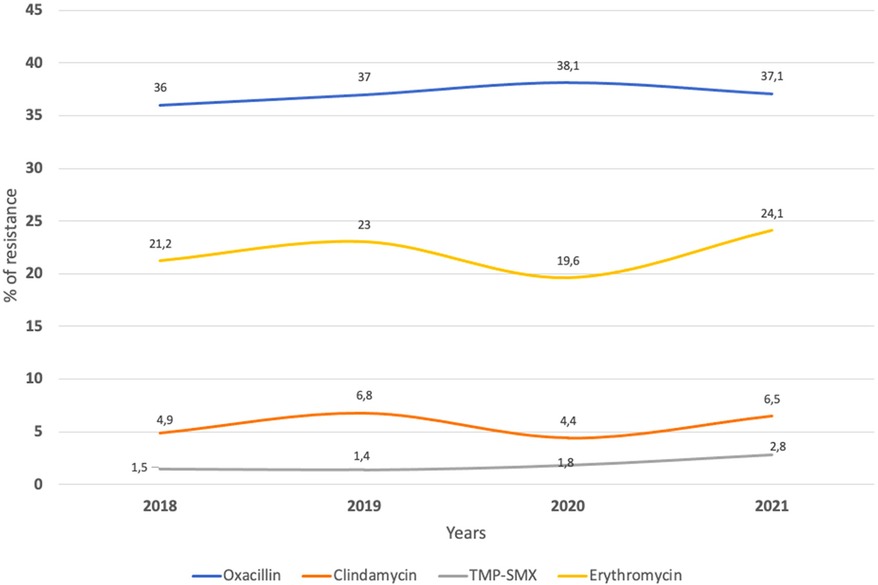
Figure 2. Percentage of resistance to different antibiotics 2018–2021 for single events (n = 5,384). TMP-SMX, trimethoprim-sulfamethoxazole.
Discussion
This multicentric study conducted across Colombia provides an analysis of the microbiological profile of S. aureus infections in the pediatric population. Analysis of positive culture reports revealed a predominance of MSSA among the subjects. However, regional, and center-specific variations were noted in antibiotic resistance patterns, with generally high levels of susceptibility to clindamycin and TMP-SMX. Notably, MRSA was associated with more severe clinical presentations. This was evidenced by an increased frequency of MRSA as the number of body sources per event rose (multifocal infections), and in all cases of bacteremia associated with another focus. Conversely, MSSA was more frequently encountered in patients with recurrent infections.
Differences in prevalence between MSSA and MRSA by location and type of centers
We found significant differences in MSSA and MRSA prevalence, and resistance patterns to other antibiotics among different cities in Colombia. Regional variations in the resistance of S. aureus by region have been previously described, with elevated MRSA rates observed in southern and eastern Europe compared to northern Europe (6). Marked regional differences have also been reported in Asia (19). In addition, higher colonization rates of MRSA have been observed in Adult Intensive Care Units (ICUs) located in the southern latitudes of the United States (20). The underlying causes for the variations in resistance patterns have not been fully identified. However, factors such as inadequate infection control measures and increased antibiotic usage are recognized as contributing to the higher prevalence of MRSA (7); although a Latin American study did not establish a clear relationship between antibiotic consumption and MRSA frequency (21) this could still be a factor associated with S. aureus susceptibility patterns. The impact of per capita income on MRSA prevalence may also have some relevance (22). Characteristics of the cities in this study, potentially influenced by patient demographics, infection control strategies, and weather among others, may contribute to these differences. Identifying the presence of different regional resistance patterns could contribute to the development of treatment recommendations for S. aureus infections tailored to specific regions, based on local data and epidemiology. These aspects could be explored in future research, and it would be valuable to analyze this phenomenon and potential regional variations as part of future phases of the Staphylored LATAM study.
Children's hospitals showed a higher frequency of MRSA prevalence compared to general hospitals (39.4% vs. 35.7%, p < 0.008). Similarly A Chicago study during the 2006 US MRSA peak reported a higher frequency of MRSA in children compared to adults (72.1% vs. 64.3%) showing greater resistance to non-beta-lactam antibiotics (23). In contrast, a Korean study found higher resistance in adults compared to children to clindamycin and ciprofloxacin, indicating that factors influencing resistance patterns vary across age groups and extend beyond oxacillin (24).
On the other hand, the availability of certain services, such as transplantation, was associated with lower frequency of MRSA, while this was not seen for other units like oncology and cardiovascular surgery. McNeil et al. at Texas Children's Hospital in the United States, identified 41 S. aureus infections in solid organ transplantation patients, with a similar percentage of MRSA and MSSA infections (47.5% and 52.5%) (25). The same group had previously described a predominance of MSSA infections in pediatric oncology patients (26).
Unique factors in children, such as different environments, daycare and school attendance, specific behaviors, and distinct antibiotic use, may influence these differences in antibiotic resistance. Similarly, centers with transplant units, despite potentially higher antibiotic consumption, often maintain higher standards of care and employ strategies for cross-transmission prevention, which could contribute to a decrease in MRSA frequency. Further research is imperative to unravel the contributing factors to the heightened MRSA prevalence in certain pediatric populations and possibly to develop targeted strategies for infection control and antibiotic stewardship in diverse healthcare environments. These findings underscore the complex dynamics of MRSA prevalence throughout time in different hospital settings.
We found a lower frequency of MRSA in institutions with established Antimicrobial Stewardship Programs (ASPs) (27, 28), highlighting the potential role these programs may play in not only reducing the frequency of MRSA but also potentially curbing the transmission of MRSA and other resistant bacteria (29). Interestingly, a lower frequency of MSSA was also noted in private institutions. These findings reinforce the hypothesis that dedicated strategies and resources for infection prevention and the rational use of antibiotics appear to impact MRSA frequencies. This should encourage efforts to optimize such programs. Investment in resources to enhance ASPs could also influence the patterns of resistance, including MRSA. The correlation between the presence of ASPs and lower MRSA rates underscores the need for robust infection control practices and policies, especially in managing antibiotic resistance, which remains a global healthcare challenge.
Trends in oxacillin resistance
In our study, we observed an overall oxacillin resistance rate of 36%, with minimal variation across different years. Similar trends of non-significant variations over time have been reported in our country. According to data from the Bacterial Resistance Control Group (GREBO) in Bogota, the MRSA rate in pediatric settings ranged from 34.3% to 46.1% in 2011 (26), 34.8%–42.1% in 2015 (30) and increased to 46.2%–49.2% in 2021 (31). Montes et al. also found MRSA rates between 40% and 50% in pediatric isolates from 2009 to 2017, which aligns with the stable 45% MRSA rates in adults reported by Castro-Orozco et al. during a similar time period (32, 33).
The epidemiology of community and hospital-acquired MRSA has undergone significant changes. Initially more common in hospitals, MRSA became widespread in the late 1990s and early 2000s, driven by clonal types like the USA300 clone, resulting in over 60% oxacillin resistance in certain populations (11). However, recent studies have observed a decline in methicillin resistance in both pediatric and adult infections (3, 10). Khamash et al. reported a significant decrease in methicillin resistance in community-onset (48%–15%; p < 0.01) and hospital-onset (32%–13%; p < 0.01) infections (9), in another US pediatric study, oxacillin susceptibility declined from 59.4% in 2005 to a low point of 53.6% in 2007, but steadily increased to 68% by 2014 (12). Similarly, Hulten K et al. demonstrated changes in community-acquired S. aureus infections in a large pediatric hospital in Texas from 2007 to 2014. The prevalence of CA-MRSA infections, primarily affecting the skin and soft tissue, decreased by 60%, while MSSA remained stable over time and accounted for 66% of invasive infections by 2014 (33, 34).
Recent data has shown stable trends in oxacillin susceptibility among pediatric community-onset MRSA infections in the US. In a multicenter retrospective study conducted between 2015 and 2020, the overall oxacillin susceptibility rate was 67%, with no significant changes over time (71.5% in 2015 and 70.8% in 2020, p = 0.71). Overall, changes in MRSA and MSSA epidemiology can vary by region and over time. While some regions have seen a decline in MRSA infections, others have identified specific clones that have predominated. This can be influenced by a combination of factors such as infection prevention strategies (which have been effective in reducing hospital onset infections and transmission), changes in treatment principles, variations in virulence and genetic diversity, and differences in the types of infections captured (invasive vs. non-invasive, or community vs. hospital-acquired) (4, 9, 34, 35). Despite the prevalence of MSSA, the reasons behind the lack of a notable decline in MRSA frequency—a finding that contradicts existing literature—within the studied cities remain unclear. Furthermore, since our study did not identify any distinction between community-acquired (CA) and hospital-acquired (HA) infections, we cannot ascertain any differential behavior based on their origin. It is crucial to maintain surveillance in order to determine whether, as observed in other regions, there will be a greater and more progressive increase in MSSA prevalence in the coming years.
Other antibiotics and their trends in susceptibility over time
S. aureus had a high susceptibility (>90%) to clindamycin overtime. This pattern has previously been reported in the pediatric population in Colombia (31). We also found that the susceptibility to clindamycin in the MSSA group is significantly higher than in the MRSA group (95.9% vs. 91.6%). However, both groups maintained a susceptibility >90%, which differs from what has been reported in a pediatric US population, in whom the sensitivity to clindamycin was 75% (36). These variations in susceptibility patterns may be due to various contributing factors. The first factor is the circulation of the ST8-MRSA-IVc clone (USA300-LV) in our country, which has been associated with this susceptibility pattern (36). The second factor could be the limited availability of pediatric formulations of clindamycin in our country, leading to its reduced usage and potentially exerting less selective pressure on the development of resistance to this antibiotic. We plan to conduct phylogenetic studies within the Staphyred to further understand the nature of these differences.
These findings support the use of clindamycin as an adequate empiric treatment option for S. aureus infections in the pediatric population, especially for osteoarticular infections, and skin and soft tissue infections, as recommended by national and international guidelines (37, 38). TMP-SMX was also highly susceptible in both MSSA and MRSA isolates. These findings also differ from previous national and US antimicrobial resistance reports indicating increase in the resistance to TMP-SMX by S. aureus (9, 31) Locally, TMS-SMX is currently recommended for skin and soft tissue infections (37). Additionally, TMP-SMX could also be an option for consolidation therapy in pediatric osteoarticular infections, especially in our setting, where clindamycin oral suspension is limited or not available.
Clinical differences between MRSA vs. MSSA
We were able to explore some clinical differences between MRSA and MSSA. The most remarkable finding was that MRSA was associated with a greater number of infection foci within the same event, particularly in the setting of bacteremia, where we observed a higher frequency of MRSA regardless of the infection focus. A previous study conducted in Bogotá, Colombia, reported that MRSA bacteremia was more frequent than MSSA when the associated focus was osteoarticular, showing prevalence rates of 73% compared to 53%. Meanwhile, the same study identified that MSSA was more prevalent in bacteremias associated with soft tissue infections, with a prevalence rate of 21% compared to 6% for MRSA (2). Another study comparing MSSA vs. MRSA in children did not find a difference in the frequency of bacteremia (39). From a clinical perspective, these findings may suggest potential treatment approaches, as the presence of multifocal disease and associated bacteremia appears to be more frequently associated with MRSA. Consequently, in specific cases and considering local epidemiology, this type of clinical presentation could guide empirical antibiotic management.
We found that as the number of events per patient increased (recurrence), the frequency of MSSA also increased. Different studies have provided variable findings regarding recurrence and S. aureus resistance. Bae et al. in South Korea, revealed a significant association between MRSA infections and higher recurrence rates (70.6% vs. 50.3%, p < 0.001) (13). Similarly, Bocchini et al. from Texas Children's Hospital reported an increased likelihood of subsequent MRSA infections compared to MSSA infections (p < 0.001) (36). In contrast, Michelle S. Hsiang et al. did not find any difference in S. aureus resistance profile and recurrence frequency (39). On the other hand, studies focusing on recurrent skin and soft tissue infections, more frequently identified MSSA as the primary causative agent in recurrences, especially in cases with the presence of PVL-positive strains (40, 41). Notably, a particularly high frequency of PVL has been described in MSSA in Colombia (40). Although we don't have data on the source of recurrences, since skin and soft tissues were one of the most frequent isolations, it could be hypothesized that this phenomenon is related to a higher frequency of infections from this source. This information is worth analyzing in more detail in later phases of Staphylored.
Altogether, our findings suggest a link between recurrence and severity according to resistance patterns. However, this study only considered WHONET-reported information, excluding clinical determinants like comorbidities and infection origin. A future Staphylored LATAM, Colombia project will prospectively evaluate these factors. Further research is also needed to explore associations between severe S. aureus isolates, recurrence, and virulence mechanisms like PVL and enterotoxins, often observed in MRSA (35).
Limitations
This retrospective study has several limitations, including the lack of clinical data, patient outcomes, and risk factors. It relies on automated microbiology systems, which may have errors in sample origin and labeling. This issue is particularly significant for the inability to determine the exact origin in cases of “abscess” or “drainage or secretion”. Interpretation of recurrence analysis should be cautious, as new cases at different institutions may not be accurately classified as recurrences. Primary blood isolates, though highlighted, are infrequent in pediatric S. aureus infections and may represent primary foci where no cultures were obtained. Detailed blood-related analysis is needed. Institutional and city data may not represent individual behavior of S. aureus infections in Colombian pediatric populations. Given the retrospective nature of the study and the fact that the information was obtained from cultures without a review of the clinical record, it is not possible to determine whether cultures from non-sterile sites represent colonization or infection. However, considering that only inpatient cultures were selected, this possibility might be reduced. Despite these limitations, our work is groundbreaking for our region and lays the foundation for prospective clinical collaborations.
Conclusions
This multicenter study, across Colombia, reveals a predominance of MSSA isolates, with some variations observed among centers and regions. The prevalence of MRSA appears to remain stable over time. MRSA is more frequently observed in cases of higher severity, such as multiple infections, bacteremia, and osteoarticular infections, while MSSA is more common in recurrent cases. TMP-SMX and clindamycin demonstrate excellent sensitivity in different regions and serve as effective alternatives in non-severe cases or step-down therapy. Ongoing monitoring of S. aureus infections in pediatric settings, including epidemiological, microbiological, and clinical characteristics, is necessary. The next phase of the Staphylored LATAM study will continue to assess the clinical characteristics, progression, and outcomes of S. aureus infections in pediatric patients across Colombia and potentially in other regions of LATAM. Including genotyping analysis in this phase aims to improve our understanding of these infections, which could contribute to more effective management approaches in pediatric care.
Data availability statement
The data analyzed in this study is subject to the following licenses/restrictions: The datasets can be shared if the editors consider it, however, they cannot be publicly shared because they correspond to data from each participating institution. Requests to access these datasets should be directed to IG-T,aXZhbmZlbGlwZWd1dGllcnJlenRAZ21haWwuY29t.
Ethics statement
The studies involving humans were approved by 1. Hospital Militar Central. 2. Clínica del Country. 3. Clínica de la Colina. 4. Clinica Infantil Santa María del Lago. 5. HOMI. Fundación Hospital Pediátrico la Misericordia. 6. Hospital San José Centro. 7. Clínica Pediátrica Colsanitas. 8. Clínica Infantil Colsubsidio. 9. Clinica El Rosario. 10. Hospital Pablo Tobón Uribe. 11. Clínica Las Américas. 12. Hospital General. 13. Clínica Soma. 14. Hospital Infantil de La Cruz Roja. 15. Clinica Farallones. 16. Clinica Versalles. 17. Fundación Valle de Lili. 18. Hospital Infantil Los Ángeles. 19. Hospital San Juan de Dios. 20. Clínica Medilaser. The studies were conducted in accordance with the local legislation and institutional requirements. Written informed consent for participation was not required from the participants or the participants’ legal guardians/next of kin in accordance with the national legislation and institutional requirements.
Author contributions
IG-T: Conceptualization, Formal Analysis, Investigation, Project administration, Writing – original draft, Writing – review & editing. CC: Investigation, Methodology, Project administration, Software, Visualization, Writing – original draft, Writing – review & editing. PV-H: Writing – review & editing, Writing – original draft. AD-D: Writing – original draft, Writing – review & editing. JL: Writing – original draft, Writing – review & editing. JA: Writing – original draft, Writing – review & editing. JC-C: Writing – original draft, Writing – review & editing. AR-G: Data curation, Investigation, Methodology, Writing – review & editing. MT-H: Data curation, Investigation, Methodology, Writing – review & editing. JM-M: Conceptualization, Investigation, Methodology, Writing – original draft, Writing – review & editing. IP: Writing – original draft, Writing – review & editing. RV: Writing – review & editing, Writing – original draft. MB-E: Writing – original draft, Writing – review & editing. JT: Writing – original draft, Writing – review & editing. AN: Writing – original draft, Writing – review & editing. GC-M: Writing – original draft, Writing – review & editing. JC-G: Writing – original draft, Writing – review & editing. NC: Writing – review & editing, Writing – original draft. LS-C: Writing – original draft, Writing – review & editing. PP: Writing – review & editing, Writing – original draft. JP: Writing – original draft, Writing – review & editing. PA-M: Writing – review & editing, Writing – original draft. YR-P: Writing – review & editing, Writing – original draft. CB-A: Writing – original draft, Writing – review & editing. YC-B: Writing – review & editing, Writing – original draft. JL: Writing – original draft, Writing – review & editing. DG-T: Writing – original draft, Writing – review & editing. SB-H: Writing – review & editing, Writing – original draft. A-CM: Writing – original draft, Writing – review & editing. NG: Writing – original draft, Writing – review & editing. ML: Writing – original draft, Writing – review & editing. DH-M: Writing – original draft, Writing – review & editing. RV: Writing – review & editing, Writing – original draft. CG: Writing – original draft, Writing – review & editing. EL-M: Writing – original draft, Writing – review & editing.
Funding
The authors declare that no financial support was received for the research, authorship, and/or publication of this article.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fped.2024.1386310/full#supplementary-material
References
1. Collaborators. GAR. Global mortality associated with 33 bacterial pathogens in 2019: a systematic analysis for the global burden of disease study 2019. Lancet. (2022) 400(10369):2221–48. doi: 10.1016/S0140-6736(22)02185-7
2. Camacho-Cruz J, Gutiérrez IF, Brand-López K, Sosa-Rodríguez YA, Vásquez-Hoyos P, Gómez-Cortés LC, et al. Differences between methicillin-susceptible versus methicillin-resistant Staphylococcus aureus infections in pediatrics: multicenter cohort study conducted in Bogotá, Colombia, 2014–2018. Pediatr Infect Dis J. (2022) 41(1):12–9. doi: 10.1097/INF.0000000000003349
3. Diekema DJ, Richter SS, Boyken L, Heilmann K, Riahi F, Tendolkar S, et al. 297: Trends in Staphylococcus aureus (SA) isolation in 28 US hospitals, 2009–2013. Open Forum Infect Dis. (2014) 1(Suppl 1):S124. doi: 10.1093/ofid/ofu052.163
4. Dulon M, Haamann F, Peters C, Schablon A, Nienhaus A. MRSA prevalence in European healthcare settings: a review. BMC Infect Dis. (2011) 11:138. doi: 10.1186/1471-2334-11-138
5. Kang CI, Song JH, Chung DR, Peck KR, Ko KS, Yeom JS, et al. Clinical impact of methicillin resistance on outcome of patients with Staphylococcus aureus infection: a stratified analysis according to underlying diseases and sites of infection in a large prospective cohort. J Infect. (2010) 61(4):299–306. doi: 10.1016/j.jinf.2010.07.011
6. Control ECfDPa. Antimicrobial resistance in the EU/EEA (EARS-Net): annual epidemiological report for 2020 (2021).
7. Falagas ME, Karageorgopoulos DE, Leptidis J, Korbila IP. MRSA in Africa: filling the global map of antimicrobial resistance. PLoS One. (2013) 8(7):e68024. doi: 10.1371/journal.pone.0068024
8. Dukic VM, Lauderdale DS, Wilder J, Daum RS, David MZ. Epidemics of community-associated methicillin-resistant Staphylococcus aureus in the United States: a meta-analysis. PLoS One. (2013) 8(1):e52722. doi: 10.1371/journal.pone.0052722
9. Khamash DF, Voskertchian A, Tamma PD, Akinboyo IC, Carroll KC, Milstone AM. Increasing clindamycin and trimethoprim-sulfamethoxazole resistance in pediatric Staphylococcus aureus infections. J Pediatric Infect Dis Soc. (2019) 8(4):351–3. doi: 10.1093/jpids/piy062
10. Kourtis AP, Hatfield K, Baggs J, Mu Y, See I, Epson E, et al. Vital signs: epidemiology and recent trends in methicillin-resistant and in methicillin-susceptible Staphylococcus aureus bloodstream infections—United States. MMWR Morb Mortal Wkly Rep. (2019) 68(9):214–9. doi: 10.15585/mmwr.mm6809e1
11. Klein EY, Sun L, Smith DL, Laxminarayan R. The changing epidemiology of methicillin-resistant Staphylococcus aureus in the United States: a national observational study. Am J Epidemiol. (2013) 177(7):666–74. doi: 10.1093/aje/kws273
12. Sutter DE, Milburn E, Chukwuma U, Dzialowy N, Maranich AM, Hospenthal DR. Changing susceptibility of Staphylococcus aureus in a US pediatric population. Pediatrics. (2016) 137(4):e20153099. doi: 10.1542/peds.2015-3099
13. Bae S, Kim ES, Kim HS, Yang E, Chung H, Lee YW, et al. Risk factors of recurrent infection in patients with Staphylococcus aureus bacteremia: a competing risk analysis. Antimicrob Agents Chemother. (2022) 66(7):e0012622. doi: 10.1128/aac.00126-22
14. Perez MG, Martiren S, Escarra F, Reijtman V, Mastroianni A, Varela-Baino A, et al. Risk factors for the appearance of secondary foci of infection in children with community-acquired Staphylococcus aureus bacteraemia. Cohort study 2010–2016. Enferm Infecc Microbiol Clin. (2018) 36(8):493–7. doi: 10.1016/j.eimc.2017.10.007
15. Hospital WCCfSoARaBaWs. WHONET2023. Available online at: https://whonet.org (Accessed November, 2023).
16. Harris PA, Taylor R, Minor BL, Elliott V, Fernandez M, O'Neal L, et al. The REDCap consortium: building an international community of software platform partners. J Biomed Inform. (2019) 95:103208. doi: 10.1016/j.jbi.2019.103208
17. Harris PA, Taylor R, Thielke R, Payne J, Gonzalez N, Conde JG. Research electronic data capture (REDCap)–a metadata-driven methodology and workflow process for providing translational research informatics support. J Biomed Inform. (2009) 42(2):377–81. doi: 10.1016/j.jbi.2008.08.010
18. (CLSI) CaLSI. Performance standards for antimicrobial susceptibility testing (2022). Report No.: M100.
19. Chen CJ, Huang YC. New epidemiology of Staphylococcus aureus infection in Asia. Clin Microbiol Infect. (2014) 20(7):605–23. doi: 10.1111/1469-0691.12705
20. Blanco N, Perencevich E, Li SS, Morgan DJ, Pineles L, Johnson JK, et al. Effect of meteorological factors and geographic location on methicillin-resistant Staphylococcus aureus and vancomycin-resistant enterococci colonization in the US. PLoS One. (2017) 12(5):e0178254. doi: 10.1371/journal.pone.0178254
21. Boni S, Marin GH, Campaña L, Marin L, Corso A, Risso-Patron S, et al. Disparities in antimicrobial consumption and resistance within a country: the case of beta-lactams in Argentina. Rev Panam Salud Publica. (2021) 45:e76. doi: 10.26633/RPSP.2021.76
22. Lim WW, Wu P, Bond HS, Wong JY, Ni K, Seto WH, et al. Determinants of methicillin-resistant Staphylococcus aureus (MRSA) prevalence in the Asia-Pacific region: a systematic review and meta-analysis. J Glob Antimicrob Resist. (2019) 16:17–27. doi: 10.1016/j.jgar.2018.08.014
23. David MZ, Crawford SE, Boyle-Vavra S, Hostetler MA, Kim DC, Daum RS. Contrasting pediatric and adult methicillin-resistant Staphylococcus aureus isolates. Emerg Infect Dis. (2006) 12(4):631–7. doi: 10.3201/eid1204.050960
24. Park JY, Jin JS, Kang HY, Jeong EH, Lee JC, Lee YC, et al. A comparison of adult and pediatric methicillin-resistant Staphylococcus aureus isolates collected from patients at a university hospital in Korea. J Microbiol. (2007) 45(5):447–52.17978805
25. McNeil JC, Munoz FM, Hultén KG, Mason EO, Kaplan SL. Staphylococcus aureus infections among children receiving a solid organ transplant: clinical features, epidemiology, and antimicrobial susceptibility. Transpl Infect Dis. (2015) 17(1):39–47. doi: 10.1111/tid.12331
26. McNeil JC, Hulten KG, Kaplan SL, Mahoney DH, Mason EO. Staphylococcus aureus infections in pediatric oncology patients: high rates of antimicrobial resistance, antiseptic tolerance and complications. Pediatr Infect Dis J. (2013) 32(2):124–8. doi: 10.1097/INF.0b013e318271c4e0
27. Nickel N, Brooks S, Mize C, Messina A. Reducing Staphylococcus aureus infections in the neonatal intensive care unit. J Perinatol. (2022) 42(11):1540–5. doi: 10.1038/s41372-022-01407-4
28. Rödenbeck M, Ayobami O, Eckmanns T, Pletz MW, Bleidorn J, Markwart R. Clinical epidemiology and case fatality due to antimicrobial resistance in Germany: a systematic review and meta-analysis, 1 January 2010–31 December 2021. Euro Surveill. (2023) 28(20):2200672. doi: 10.2807/1560-7917.ES.2023.28.20.2200672
29. Popovich KJ, Aureden K, Ham DC, Harris AD, Hessels AJ, Huang SS, et al. SHEA/IDSA/APIC practice recommendation: strategies to prevent methicillin-resistant Staphylococcus aureus transmission and infection in acute-care hospitals: 2022 update. Infect Control Hosp Epidemiol. (2023) 44(7):1039–67. doi: 10.1017/ice.2023.102
30. Arturo C, Jorge Á, Cortes María A, Ovalle V, Gualteros S, Camacho G, et al. (n.d.). Boletín informativo GREBO (2016).
32. Castro-Orozco R, Consuegra-Mayor C, Mejía-Chávez G, Hernández-Escolar J, Alvis-Guzmán N. Antimicrobial resistance trends in methicillin-resistant and methicillin—susceptible Staphylococcus aureus and Staphylococcus epidermidis isolates obtained from patients admitted to intensive care units. 2010–2015. Rev Fac Med. (2019) 67(3):221–8. doi: 10.15446/revfacmed.v67n3.65741
33. Montes O, Hernández J, Correa O, Reyes J, Pinzon H, Reyes N. Clonal distribution and antibiotic susceptibility of Staphylococcus aureus from pediatric patients: 8-year trends in a children’s hospital in Colombia. J Trop Pediatr. (2021) 67(6):fmab105. doi: 10.1093/tropej/fmab105
34. Hultén KG, Mason EO, Lamberth LB, Forbes AR, Revell PA, Kaplan SL. Analysis of invasive community-acquired methicillin-susceptible Staphylococcus aureus infections during a period of declining community acquired methicillin-resistant Staphylococcus aureus infections at a large children’s hospital. Pediatr Infect Dis J. (2018) 37(3):235–41. doi: 10.1097/INF.0000000000001753
35. Zúñiga M, Passalacqua S, Benadof D, Conca N, Acuña M, Zúñiga M, et al. Staphylococcus aureus sensible a meticilina, productor de leucocidina de Panton Valentine. A propósito de dos casos pediátricos de infección osteoarticular. Revista Chilena de Infectología. (2021) 38:300–2. doi: 10.4067/S0716-10182021000200300
36. Jiménez JN, Ocampo AM, Vanegas JM, Rodriguez EA, Mediavilla JR, Chen L, et al. CC8 MRSA strains harboring SCCmec type IVc are predominant in Colombian hospitals. PLoS One. (2012) 7(6):e38576. doi: 10.1371/journal.pone.0038576
37. Gutiérrez-Tobar IF, Palacios-Ariza MA, Luna-Solarte DA, Niño-Uribe WH, González-Garzón AC, Beltrán-Higuera SJ, et al. Guía de práctica clínica colombiana para el tratamiento de infecciones bacterianas de piel y tejidos blandos superficiales en Población pediátrica. Infectio. (2023) 27:114–31. doi: 10.22354/24223794.1131
38. Woods CR, Bradley JS, Chatterjee A, Copley LA, Robinson J, Kronman MP, et al. Clinical practice guideline by the pediatric infectious diseases society and the infectious diseases society of America: 2021 guideline on diagnosis and management of acute hematogenous osteomyelitis in pediatrics. J Pediatric Infect Dis Soc. (2021) 10(8):801–44. doi: 10.1093/jpids/piab027
39. Hsiang MS, Shiau R, Nadle J, Chan L, Lee B, Chambers HF, et al. Epidemiologic similarities in pediatric community-associated methicillin-resistant and methicillin-sensitive Staphylococcus aureus in the San Francisco bay area. J Pediatric Infect Dis Soc. (2012) 1(3):200–11. doi: 10.1093/jpids/pis061
40. Correa-Jiménez O, Pinzón-Redondo H, Reyes N. High frequency of panton-valentine leukocidin in Staphylococcus aureus causing pediatric infections in the city of Cartagena-Colombia. J Infect Public Health. (2016) 9(4):415–20. doi: 10.1016/j.jiph.2015.10.017
Keywords: Colombia, LATAM countries, MSSA (methicillin-susceptible Staphylococcus aureus), MRSA—methicillin-resistant Staphylococcus aureus, pediatric infections, epidemiology, S. aureus
Citation: Gutierrez-Tobar I, Carvajal C, Vasquez-Hoyos P, Díaz-Díaz A, Londono Ruiz JP, Andrade J, Camacho-Cruz J, Restrepo-Gouzy A, Trujillo-Honeysberg M, Mesa-Monsalve JG, Perez I, Von Moltke R, Beltran-Echeverry M, Toro JF, Niño AP, Camacho-Moreno G, Calle-Giraldo JP, Cabeza NY, Sandoval-Calle LM, Perez Camacho P, Patiño Niño J, Araque-Muñoz P, Rodríguez-Peña Y, Beltran-Arroyave C, Chaucanez-Bastidas Y, Lopez J, Galvis-Trujillo D, Beltrán-Higuera S, Marino A-C, González Leal N, Luengas Monroy MÁ, Hernandez-Moreno DC, Vivas Trochez R, Garces C and López-Medina E (2024) Epidemiological and microbiological characteristics of S. aureus pediatric infections in Colombia 2018–2021, a national multicenter study (Staphylored Colombia). Front. Pediatr. 12:1386310. doi: 10.3389/fped.2024.1386310
Received: 15 February 2024; Accepted: 13 May 2024;
Published: 4 June 2024.
Edited by:
Christopher Montgomery, Nationwide Children's Hospital, United StatesReviewed by:
Stephanie Fritz, Washington University in St. Louis, United StatesMichael Zdenek David, University of Pennsylvania, United States
© 2024 Gutierrez-Tobar, Carvajal, Vasquez-Hoyos, Díaz-Díaz, Londono Ruiz, Andrade, Camacho-Cruz, Restrepo-Gouzy, Trujillo-Honeysberg, Mesa-Monsalve, Perez, Von Moltke, Beltran-Echeverry, Toro, Niño, Camacho-Moreno, Calle-Giraldo, Cabeza, Sandoval-Calle, Perez Camacho, Patiño Niño, Araque-Muñoz, Rodríguez-Peña, Beltran-Arroyave, Chaucanez-Bastidas, Lopez, Galvis-Trujillo, Beltrán-Higuera, Marino, González Leal, Luengas Monroy, Hernandez-Moreno, Vivas Trochez, Garces and López-Medina. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Ivan Gutierrez-Tobar, aXZhbmZlbGlwZWd1dGllcnJlenRAZ21haWwuY29t