 Sefa Muzemil1
Sefa Muzemil1 Muhiddin Tadesse Barega
Muhiddin Tadesse Barega Shamill Eanga
Shamill Eanga- 1Department of Pediatrics and Child Health, School of Medicine, St. Peter’s Specialized Hospital, Addis Ababa, Ethiopia
- 2Department of Pediatrics and Child Health, School of Medicine, Addis Ababa University, Addis Ababa, Ethiopia
- 3Department of Midwifery, College of Medicine and Health Sciences, Wolkite University, Wolkite, Ethiopia
- 4Department of Anesthesia, College of Medicine and Health Sciences, Wolkite University, Wolkite, Ethiopia
Introduction: Nearly 2,000 children under the age of 14 die every day due to injuries, with fractures accounting for 10%–25% of these cases. The burden of pediatric fractures is significant, but neglected and many can be prevented through simple and cost-effective community-level interventions. However, no studies have been conducted in our country regarding the incidence and patterns of pediatric fractures. Without comprehensive data, it is challenging to set priorities, formulate policies, and implement preventive measures. Therefore, this study aims to determine the incidence and patterns of pediatric fractures at selected hospitals in Addis Ababa in 2024.
Materials and methods: A multi-center cross-sectional study was conducted from October 10, 2023, to February 15, 2024, in the emergency unit and pediatrics ward of three public hospitals in Addis Ababa, Ethiopia: Tikur Anbesa Specialized Hospital (TASH), Yekatit 12 Hospital, and Alert Hospital. Data was collected by bachelor's degree nurses using an interviewer-administered structured questionnaire. Data was refined, coded, and entered into Epi Info version 7 computer software, then exported into SPSS version 21 for data cleaning and analysis.
Results: From a total of 648 children who encountered trauma, 182 cases were fractures, resulting in an incidence of 28% (95% CI: 26.5–29.7). The major patterns of injury were due to falls (79%), road traffic accidents (RTAs) (15.4%), and assaults (5.6%). The upper limb was the most common site of injury (73%). Fifty-four percent of the children had injuries to two structures.
Conclusions: The overall incidence of pediatric fractures among those who encountered trauma was 28%. Male children exhibited a higher incidence of fractures than female children. The highest risk of fractures occurred in children aged 6–10 years. Upper limb fractures were observed more frequently than lower limb fractures.
Introduction
Child injury is one of the most immediate public health threats, resulting in the deaths of nearly 2,000 children under the age of 14 every day around the world (1). Fractures are extremely common in the pediatric age group. Of all these injuries, fractures account for 10%–25% (2–4). The annual incidence rates of fractures have dramatically increased in children under 16 years, rising from 3.6 per 1,000–50 per 1,000. There was a doubled risk of fracture in boys aged 13–15 compared with their female peers. Typically, the incidence peaks at ages 11–12 for girls and 13–14 for boys. The lifetime risk of sustaining a fracture during childhood is approximately 42%–64% for boys and 27%–40% for girls; however, these gender distributions may vary between bone sites (5, 6). In children, the most common sites of injury are the upper limb, elbow, and forearm (7).
Activities associated with fractures were primarily soccer and bicycling. However, when comparing the total number of injuries associated with each activity, we found a doubled risk of fractures during rollerblading/skating or snowboarding (60%) compared to playing soccer (38%) or bicycling (33%) (8). Scaphoid fractures, which are infrequent in children, accounted for 9% of all fractures resulting from rollerblading/skating (9, 10). Injuries occur in various locations during different activities, and their patterns change over time. For instance, sports participation is encouraged to increase physical activity among children in most developed countries (11, 12). In contrast, other daily activities, such as walking, tend to decrease (13, 14).
A substantial proportion of pediatric fractures are preventable. In high-income countries (HICs), there has been a general decline in injuries over the past 15 years. However, children from low- and middle-income countries (LMICs) are disproportionately affected, accounting for over 90% of unintentional injury-related deaths globally (15, 16). In LMICs, efforts have largely focused on addressing mortality from communicable illnesses, resulting in a widening gap in injury mortality (17). The burden of pediatric fractures is significant, but many can be prevented through simple and cost-effective community-level interventions aimed at children and their families (1). The Ethiopian health sector program prioritizes the prevention of injuries and violence. To address pediatric trauma, the Ministry of Health (MoH) has been implementing Emergency Triage Assessment and Treatment Plus (ETAT+) strategies (18).
Without understanding the causes of injuries, as well as the conditions and environments in which they arise at different developmental stages, it is impossible to identify risky behaviours that can be addressed with age-appropriate preventive strategies (19). To the best of our knowledge, few studies have been conducted in Ethiopia regarding the incidence and patterns of pediatric fractures. Without comprehensive data on pediatric fractures, it is challenging to set priorities, formulate policies, and implement preventive measures. Therefore, this study aimed to determine the incidence and patterns of pediatric fractures at selected hospitals in Addis Ababa.
Materials and methods
A multi-center cross-sectional study was conducted from October 10, 2023, to February 15, 2024, in the emergency unit and pediatrics ward of three public hospitals in Addis Ababa, Ethiopia: Tikur Anbesa Specialized Hospital (TASH), Yekatit 12 Hospital, and Alert Hospital. All three hospitals serve as teaching facilities and referral centers at both the city administration and federal levels. TASH is the largest tertiary hospital in the country and functions as one of the orthopedic centers, managing approximately 1,000 pediatric fracture cases per year. Yekatit 12 Hospital (Y12H) attends to around 250 pediatric fracture cases in its emergency and pediatric surgical wards annually. Alert Hospital (AH) sees about 4,600 pediatric emergency admissions annually, with 8% of these being pediatric fractures.
All children under 15 years old who sustained trauma and were admitted to TASH, Y12H, and AH were considered as the source population. The study population included all children under 15 years old who visited and were admitted to the selected hospitals during the study period, provided their caregivers gave voluntary consent for participation, and met the inclusion criteria. Children who died on arrival, those without an attendant, and those who declined consent were excluded from the study.
Sample size determination
Since no study has been conducted in Ethiopia on the incidence of pediatric fractures, the prevalence of pediatrics fracture among our population was assumed to be 50%. The sample size was determined using a single population proportion formula, with a 5% marginal error and a 95% confidence interval (CI). The initial sample size was calculated to be 384. However, since the number of children visiting the emergency and trauma wards of the selected hospitals is less than 10,000, a correction formula was applied, resulting in a recalculated sample size of 165. After accounting for a 10% non-response rate, the final sample size was adjusted to 182.
Sampling techniques
From a total of 12 public hospitals in Addis Ababa providing pediatric fracture services, Tikur Anbesa Specialized Hospital, Alert Hospital, and Yekatit 12 Hospital were selected randomly. Proportional allocation was done, and 47, 75 and 60 pediatric patients were selected from TASH, Alert Hospital, and Yekatit 12 Hospital, respectively. Data was collected consecutively until the required sample size was achieved.
Data collection tool and procedure
After giving one day of training, data was collected by six bachelor's degree nurses from the emergency unit at selected hospitals both on working and night time using an interviewer-administered structured questionnaire to get sociodemographic information, mechanism of injury, time of injury and place of injury. The site of injury and type of fracture patterns were described by clinical evaluation and radiologic investigations. The questionnaire was initially prepared in English. The English version was translated into Amharic and translated back into English to ensure internal consistency. The questionnaire was developed from similar studies conducted in different countries (18–20).
Data quality control
To ensure data quality, questionnaires were pre-tested with 5% of the sample size at St. Paul Hospital, and necessary amendments were made based on the findings. The investigator and supervisor checked the completeness of the data, and timely corrections were done
Data processing and analysis
Data was refined, coded, and entered into Epi Info version 7 computer software, then exported into SPSS version 21 for data cleaning and analysis. Descriptive statistics were used for socio-demographic and clinical data. The incidence and pattern of pediatric fracture variables were analyzed using the Chi-square test.
Ethical approval and consent to participate
This study was carried out under the Declaration of Helsinki Ethical Principles for Medical Research involving human subjects protocol (21). Ethical approval was received from the Ethical Review Board of Addis Ababa University, College of Medicine and Health Science with protocol number SOM/23/2024 and informed oral consent were taken.
Results
Sociodemographic characteristics
From 648 total pediatrics traumas in selected hospitals, 182 were diagnosed as fractures. Three -fourths of them were male, and 37.4% of the participants were in the age group of 6–10 years, with a mean and SD of 7.75 ± 3.97 years. Half of the participants had a family size of 4–5 members. One-third of the children received primary care from their mothers, and 28.6% of the mothers were housewives. Around 41% and 48% of the mothers and fathers completed higher education, respectively. The majority of the participants were from urban areas, and half of the pediatric families had a monthly income of 5000–10000 ETB (Table 1).
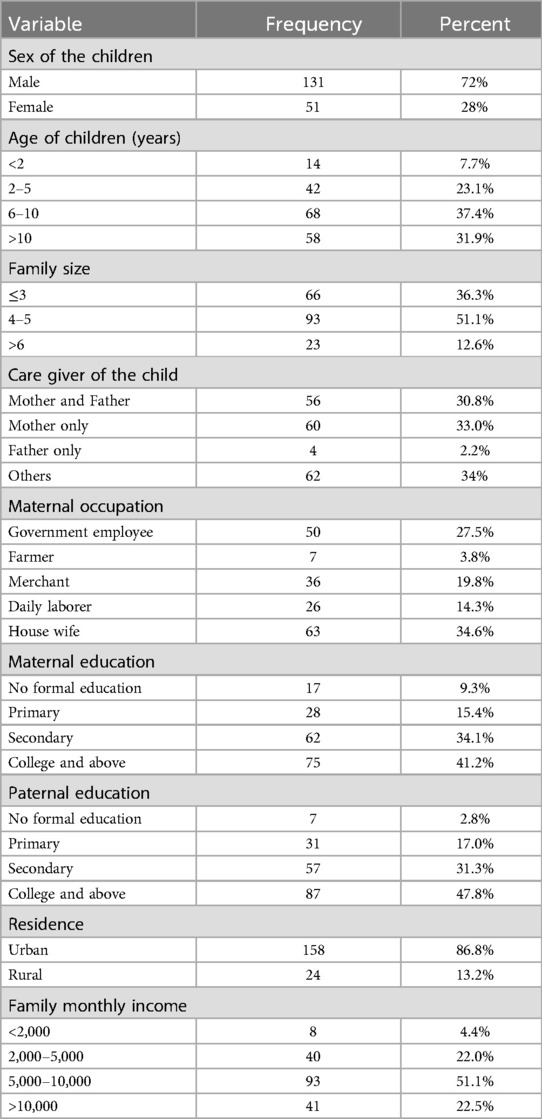
Table 1. The sociodemographic characteristics of the children and their families among pediatric fractures in selected hospitals in Addis Ababa, from October 10, 2023, to February 15, 2024 (n = 182).
The incidence of pediatrics fracture
The findings of the study showed that out of the total of 648 children who encountered trauma in the emergency and trauma centers of the selected hospitals during the study period, 182 cases were fractures, making the incidence of pediatric fractures about 28% (95% CI; 26.5–29.7).
The characteristics and pattern of injury
The major pattern of injury was falls, accounting for 79% of cases, followed by road traffic accidents (RTA) at 15.4%. In terms of injury mode, bicycle riding was responsible for 60.8% of the cases, while pedestrians accounted for 25%. Regarding the location of falls, 41.4% occurred in playgrounds, and 34.3% took place at home. Additionally, more than half of the children sustained injuries to two structures. Seventy-eight percent of the children had a single fracture, while 22% experienced multiple fractures (Table 2).
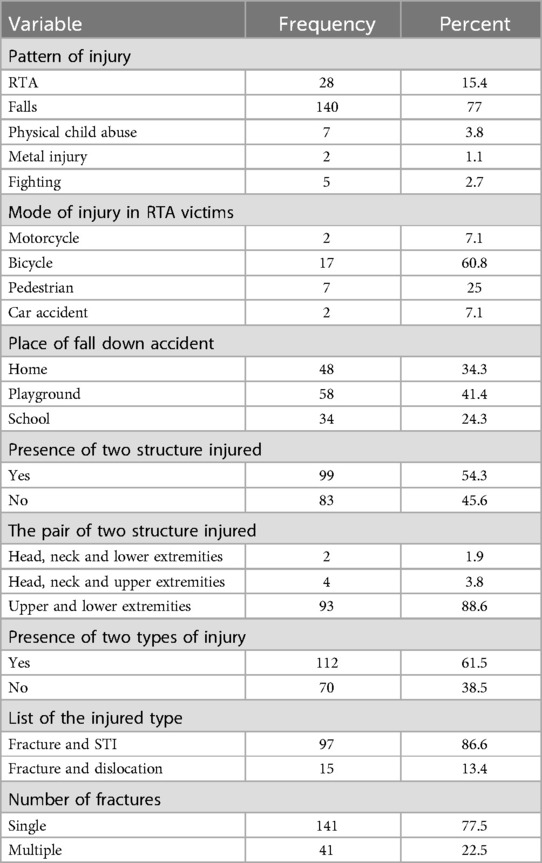
Table 2. The pattern of injury and fracture characteristics among children in selected hospitals in Addis Ababa, Ethiopia, from October 10, 2023, to February 15, 2024 (n = 182).
The characteristics of limb fracture patterns and fracture sites
From the total of 182 pediatric fractures, the upper limb accounts for seventy-three percent, the lower limb for 19%, and is followed by axial bone fractures (7%) (Figure 1). Thirty-nine percent of upper limb fractures were in the radius, followed by the ulna (26.7%), humerus (15%), and phalanges (7.4%). The majority of lower limb fractures were femoral fractures (55%), followed by tibial fractures (34%). Most of the fractures were of the closed (simple) type (Table 3).
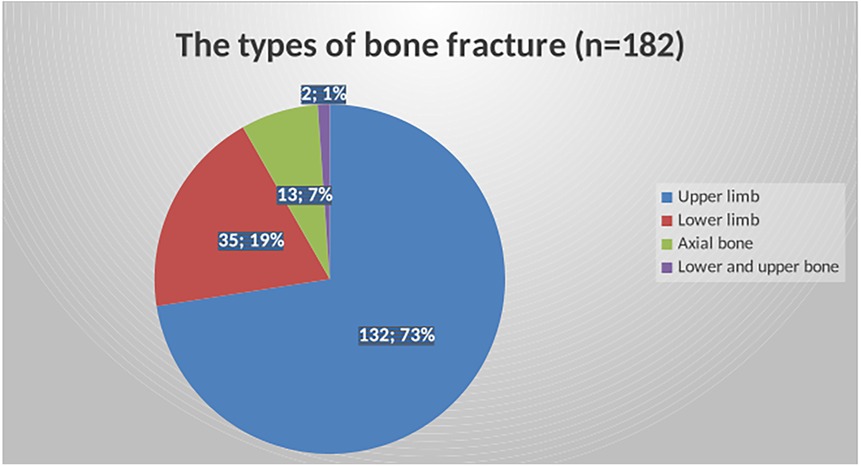
Figure 1. The patterns of fracture based on site among children in selected hospitals in Addis Ababa, Ethiopia, from October 10, 2023, to February 15, 2024 (n = 182).
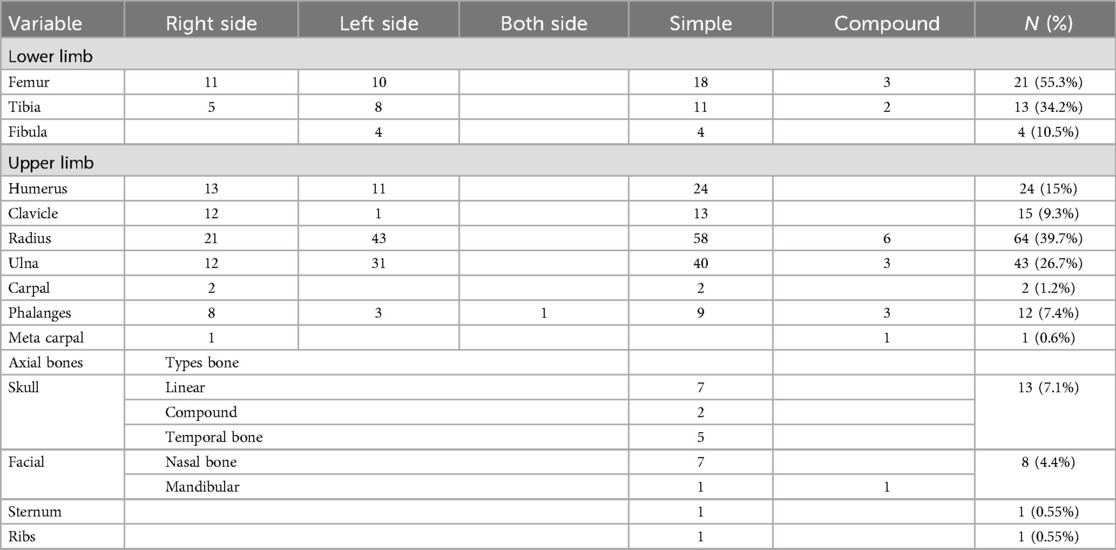
Table 3. Characteristics of fracture sites among children in selected hospitals in Addis Ababa, Ethiopia, from October 10, 2023, to February 15, 2024 (n = 182).
The relation between patterns of injury with sex and age of the children
The findings of this study showed that males have a higher incidence of fractures (72%) compared to females (28%) due to falls, road traffic accidents (RTAs), and assaults, which account for 79%, 15.4%, and 5.6% of the cases, respectively (Figure 2).
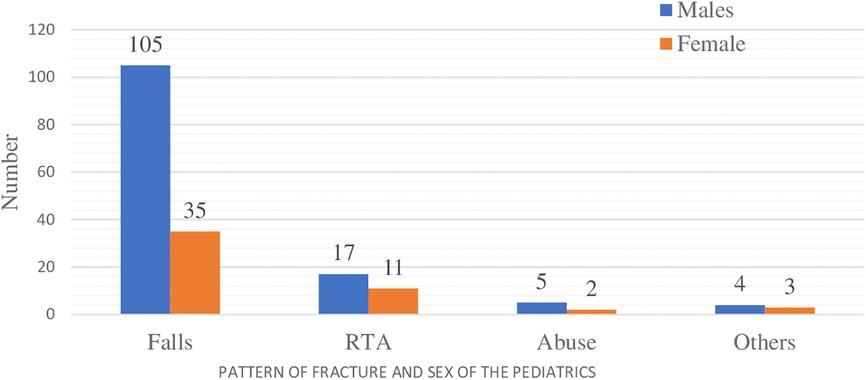
Figure 2. The patterns of fracture and sex of the children in selected hospitals in Addis Ababa, Ethiopia, from October 10, 2023, to February 15, 2024 (n = 182).
The chi-square test was conducted to assess the association between sociodemographic characteristics and the incidence of fractures. The findings indicated that children in the 6–10 age group and those from urban residences had a higher incidence of fractures, which was statistically significant (p-value <0.05) (Table 4). Our results indicated that the RTA mode of injury (p = 0.014), place of fall (p < 0.001), two-structure injury (p = 0.034), and number of fractures (p = 0.012) were statistically significant in relation to the age of the children (Table 5).
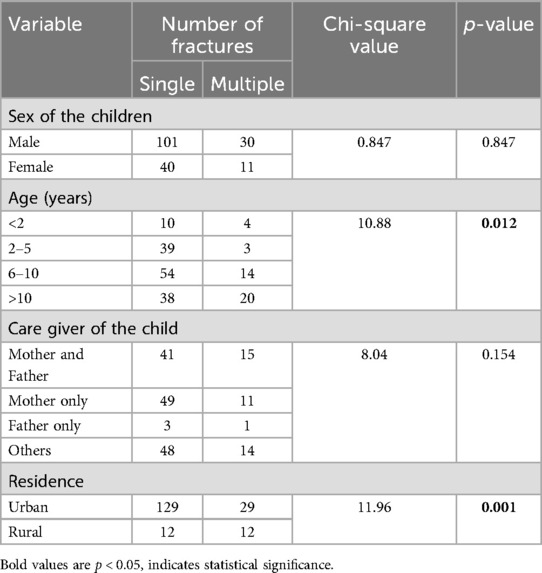
Table 4. Association between sociodemographic characteristics and the incidence of fractures among pediatric patients in selected hospitals in Addis Ababa, Ethiopia, from October 10, 2023, to February 15, 2024 (n = 182).
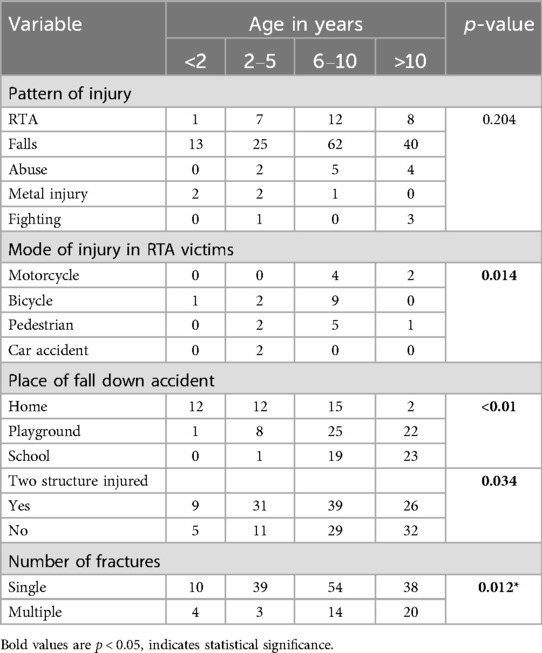
Table 5. Association between pattern of injury and age of children among pediatrics in selected hospitals in Addis Ababa, Ethiopia, from October 10, 2023 to February 15, 2024 (n = 182).
Association between the fracture site and the sex of the children
The findings of this study showed that male children had a higher incidence of radial, ulnar, and skull fractures, which were statistically significant (p < 0.05) (Table 6).
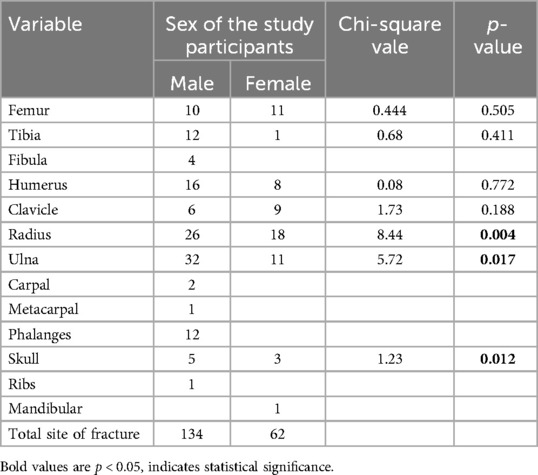
Table 6. The association between fracture site and sex of the children among pediatrics in selected hospitals in Addis Ababa, Ethiopia, from October 10, 2023 to February 15, 2024 (n = 182).
Discussion
The current study found that, from 648 pediatric trauma children, the incidence of fractures was approximately 28% (95% CI: 26.5–29.7). Males have a higher incidence of fractures (72%) compared to females (28%), in relation to falls, RTA, and assaults, which account for 79%, 15.4%, and 5.6% of cases, respectively. This finding is consistent with studies conducted in Kenya (19), Italy (20), and the United States (22). However, our results differ from a study conducted at the Children's Hospital of Michigan, where females accounted for a greater proportion in the 10–12 year age group (23). This disparity in injury incidence may be attributed to age-related behavioral changes, such as males engaging in more physically risky activities.
The findings of the study indicate that children aged 6–10 years living in urban areas have a higher incidence of fractures. The mode of injury from RTA (p = 0.014), the place of fall (p < 0.001), two-structure injuries (p = 0.034), and the number of fractures (p = 0.012) were statistically significant in relation to the age of the children. These results are consistent with other studies conducted in South Wales (5) and Britain (6). The higher frequency of fractures may be attributed to increased participation in both organized and unstructured sports, as well as generally high levels of physical activity during this age.
Regarding the anatomic site, our results showed that the upper limb was more frequently involved, accounting for over 73% of fractures. This finding aligns with studies conducted at a Sub-Saharan tertiary care center (7) and in the United States (22). In contrast, other studies have reported a higher incidence of lower limb involvement (19, 20). The increased incidence of upper limb fractures in our study may be attributed to the fact that 79% of children reported falls as the main cause, with the upper limb being more commonly injured during such incidents. When individuals fall, they instinctively use their upper limbs to protect themselves, which increases the likelihood of fractures. The arm, in particular, may be frequently involved due to its role as a protective mechanism during a fall.
The other finding of our study indicated that the radius is more commonly involved in the upper limb, this is supported by several studies (6, 20). In contrast, another study conducted at TASH & Italy found that the humerus is more frequently involved (10, 18). These discrepancies may arise from variations in the distribution of fractures across different studies and populations.
In this study, falls accounted for 79% of fracture mechanisms, making them the most common, followed by road traffic accidents (RTAs). This finding aligns with other studies (3, 18, 19, 24). The high incidence of fall-related fractures may be attributed to the various activities in which children engage, such as climbing, running, jumping, and playing, all of which increase the risk of falls.
Our study showed that bicycle riding (60.8%) and pedestrian activity (25%) are the most common modes of fracture. Regarding the location of the falls, surrounding playgrounds and homes account for the majority of cases. This finding is consistent with other studies (9, 20, 23, 24) and reflects the amount of time that preschool children spend at home, which may be greater than their active time spent outside.
Recommendations
For parents
Children should be actively supervised both at home and at playgrounds.
For health care providers
Health care providers should offer anticipatory guidance regarding home and playground injuries and advise parents on how to reduce these risks.
For policy makers
Policy makers should ensure that municipal policies on playground development and maintenance are based on established standards. Additionally, education on traffic rules and the construction of sidewalks, bridges, and tunnels to separate vehicles from pedestrians is recommended.
Strength of the study
To the best of our knowledge, this study is the only prospective cross-sectional study conducted in multicenter settings in Ethiopia.
Limitation of the study
Association was not done to identify risk factors of pediatrics fracture. Therefore, another strong study is needed to determine the incidence and risk factors of pediatrics fracture in the study setting to overcome the limitation of this study.
Conclusions
The overall incidence of pediatric fractures among those who encountered trauma in selected hospitals during study period was 28%. Male children exhibited a higher incidence of fractures than female children. The highest risk of fractures occurred in children aged 6–10 years. Upper limb fractures were more frequently observed than lower limb fractures.
Data availability statement
The original contributions presented in the study are included in the article/Supplementary Material, further inquiries can be directed to the corresponding author.
Ethics statement
Ethical clearance with protocol number SOM/23/2024 was received from the institutional review board of Addis Ababa University, College of Health Sciences. All participants provided written informed consent prior to enrolment in the study. This research was conducted ethically in accordance with the World Medical Association Declaration of Helsinki.
Author contributions
SM: Conceptualization, Data curation, Formal analysis, Investigation, Methodology, Resources, Software, Supervision, Validation, Visualization, Writing – original draft, Writing – review & editing. AM: Conceptualization, Data curation, Formal analysis, Investigation, Methodology, Resources, Software, Supervision, Validation, Visualization, Writing – original draft, Writing – review & editing. FM: Conceptualization, Data curation, Formal analysis, Investigation, Methodology, Resources, Software, Supervision, Validation, Visualization, Writing – original draft, Writing – review & editing. MB: Conceptualization, Data curation, Formal analysis, Investigation, Methodology, Resources, Software, Supervision, Validation, Visualization, Writing – original draft, Writing – review & editing. SE: Conceptualization, Data curation, Formal analysis, Investigation, Methodology, Resources, Software, Supervision, Validation, Visualization, Writing – original draft, Writing – review & editing.
Funding
The author(s) declare that no financial support was received for the research and/or publication of this article.
Acknowledgments
We appreciate the willingness of the data collectors, supervisors, and study participants to actively participate in this study, as well as the contributions of the authors of the references I cited.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Generative AI statement
The author(s) declare that Generative AI was used in the creation of this manuscript. During the preparation of this manuscript, the authors used Paperpal to rewrite the article. After utilizing this service, the authors reviewed and edited the content as needed and take full responsibility for the publication's content.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Abbreviations
AH, alert hospital; ETAT, emergency triage assessment and treatment; HIC, high-income countries; HMIS, health management information system; LMIC, low and middle-income countries; RTA, road traffic accident; SD, standard deviation; SPSS, statistical package for the social sciences; STI, sustained traumatic injury; TASH, Tikur Anbesa specialized hospital; Y12H, Yekatit 12 Hospital.
References
1. Sleet DA. The global challenge of child injury prevention. Int J Environ Res Public Health. (2018) 15(9):1921. doi: 10.3390/ijerph15091921
2. Mattila V, Parkkari J, Kannus P, Rimpelä A. Occurrence and risk factors of unintentional injuries among 12- to 18-year-old Finns – a survey of 8219 adolescents. Eur J Epidemiol. (2004) 19:437–44. doi: 10.1023/B:EJEP.0000027355.85493.cb
3. Hedström EM, Svensson O, Bergström U, Michno P. Epidemiology of fractures in children and adolescents: increased incidence over the past decade: a population-based study from northern Sweden. Acta Orthop. (2010) 81(1):148–53. doi: 10.3109/17453671003628780
4. Walsh SS, Jarvis SN, Towner EM, Aynsley-Green A. Annual incidence of unintentional injury among 54,000 children. Inj Prev. (1996) 2(1):16–20. doi: 10.1136/ip.2.1.16
5. Lyons RA, Delahunty AM, Kraus D, Heaven M, McCabe M, Allen H, et al. Children’s fractures: a population based study. Inj Prev. (1999) 5(2):129–32. doi: 10.1136/ip.5.2.129
6. Cooper C, Dennison EM, Leufkens HGM, Bishop N, van Staa TP. Epidemiology of childhood fractures in Britain: a study using the general practice research database. J Bone Miner Res. (2004) 19(12):1976–81. doi: 10.1359/jbmr.040902
7. Guifo ML, Tochie JN, Oumarou BN, Tapouh JRM, Ndoumbe A, Jemea B, et al. Paediatric fractures in a sub-saharan tertiary care center: a cohort analysis of demographic characteristics, clinical presentation, therapeutic patterns and outcomes. Pan Afr Med J. (2017) 27:46. doi: 10.11604/pamj.2017.27.46.11485
8. Monget F, Sapienza M, McCracken KL, Nectoux E, Fron D, Andreacchio A, et al. Clinical characteristics and distribution of pediatric fractures at a tertiary hospital in northern France: a 20-year-distance comparative analysis (1999–2019). Medicina (Kaunas). (2022) 58(5):610. doi: 10.3390/medicina58050610
9. Brudvik C, Hove LM. Childhood fractures in Bergen, Norway: identifying high-risk groups and activities. J Pediatr Orthop. (2003) 23(5):629–34. doi: 10.1097/00004694-200309000-00010
10. Randsborg P-H, Gulbrandsen P, Benth JŠ, Sivertsen EA, Hammer O-L, Fuglesang HF, et al. Fractures in children: epidemiology and activity-specific fracture rates. JBJS. (2013) 95(7):e42. doi: 10.2106/JBJS.L.00369
11. Johnston BD, Ebel BE. Child injury control: trends, themes, and controversies. Acad Pediatr. (2013) 13(6):499–507. doi: 10.1016/j.acap.2013.04.016
12. Booth VM, Rowlands AV, Dollman J. Physical activity temporal trends among children and adolescents. J Sci Med Sport. (2015) 18(4):418–25. doi: 10.1016/j.jsams.2014.06.002
13. Faulkner G, Goodman J, Adlaf E, Irving H, Allison K, Dwyer J. Participation in high school physical education–Ontario, Canada, 1999–2005. Morb Mortal Wkly Rep. (2007) 56(3):52–5. Available online at: https://go.gale.com/ps/i.do?p=AONE&u=anon~4e0bca5d&id=GALE%7CA158958544&v=2.1&it=r&sid=googleScholar&asid=c2c4c6b2
14. McDonald NC, Brown AL, Marchetti LM, Pedroso MS. U.S. school travel, 2009: an assessment of trends. Am J Prev Med. (2011) 41(2):146–51. doi: 10.1016/j.amepre.2011.04.006
15. Sethi D, Aldridge E, Rakovac I, Makhija A. Worsening inequalities in child injury deaths in the WHO European region. Int J Environ Res Public Health. (2017) 14(10):1128. doi: 10.3390/ijerph14101128
16. Tupetz A, Friedman K, Zhao D, Liao H, Isenburg MV, Keating EM, et al. Prevention of childhood unintentional injuries in low- and middle-income countries: a systematic review. PLoS One. (2020) 15(12):e0243464. doi: 10.1371/journal.pone.0243464
17. Adeloye D, Bowman K, Chan KY, Patel S, Campbell H, Rudan I. Global and regional child deaths due to injuries: an assessment of the evidence. J Glob Health. (2018) 8(2):1–11. doi: 10.7189/jogh.08.021104
18. Admassie D, Ayana B, Girma S. Childhood limb fracture at tikur anbessa specialised hospital (TASH), Addis Ababa, Ethiopia. East Cent Afr J Surg. (2015) 20(1):27–31.
19. Ali B, Kassim K, Ndanya SW, Gitonga SW, Kirengo TO. Paediatric fracture patterns in patients admitted in a Kenyan Level 5 hospital. In: The Surgical Society of Kenya 15th Annual Scientific Conference and Silver Jubilee. Embu: Embu Level 5 Hospital (2015).
20. Valerio G, Gallè F, Mancusi C, Di Onofrio V, Colapietro M, Guida P, et al. Pattern of fractures across pediatric age groups: analysis of individual and lifestyle factors. BMC Public Health. (2010) 10:1–9. doi: 10.1186/1471-2458-10-656
21. World Medical Association. World Medical Association declaration of Helsinki: ethical principles for medical research involving human subjects. JAMA. (2013) 310(20):2191–4. doi: 10.1001/jama.2013.281053
22. Wolfe JA, Wolfe H, Banaag A, Tintle S, Perez Koehlmoos T. Early pediatric fractures in a universally insured population within the United States. BMC Pediatr. (2019) 19:1–6. doi: 10.1186/s12887-019-1725-y
23. Arora R, Fichadia U, Hartwig E, Kannikeswaran N. Pediatric upper-extremity fractures. Pediatr Ann. (2014) 43(5):196–204. doi: 10.3928/00904481-20140417-12
Keywords: fractures, incidence, pattern, pediatrics, hospitals, Ethiopia
Citation: Muzemil S, Mekasha A, Muzemil F, Barega MT and Eanga S (2025) Incidence and patterns of pediatric fractures at selected hospitals in Addis Ababa, Ethiopia, 2024: a multi-center cross-sectional study. Front. Pediatr. 13:1501900. doi: 10.3389/fped.2025.1501900
Received: 11 October 2024; Accepted: 8 July 2025;
Published: 24 July 2025.
Edited by:
Pengpeng Ye, Chinese Center For Disease Control and Prevention, ChinaReviewed by:
Marco Sapienza, University of Catania, ItalyPascal Chigblo, Centre National Hospitalier et Universitaire Hubert Koutoukou MAGA, Benin
Copyright: © 2025 Muzemil, Mekasha, Muzemil, Barega and Eanga. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Shamill Eanga, ZWFuZ2FzaGFtaWxsNjdAZ21haWwuY29t