 Fabiane Raquel Motter
Fabiane Raquel Motter Sarah Nicole Hilmer2
Sarah Nicole Hilmer2- 1Postgraduate Program in Collective Health, University of Vale do Rio dos Sinos (UNISINOS), São Leopoldo, Brazil
- 2Kolling Institute of Medical Research, Royal North Shore 83 Hospital, St. Leonards, NSW, Australia
Purpose: The aim of the present study was to develop and validate a Potentially Inappropriate Medications (PIM) list and alternative therapies for treatment of pain and inflammation in older people adapted to the Brazilian context.
Methods: A preliminary PIM list suitable for the Brazilian market was developed on the basis of three published international PIM lists [Beers 2015, Screening Tool of Older People’s Potentially Inappropriate Prescriptions - 2015, European Union (7) PIM list]. We used the modified Delphi technique (two-round) to validate concerns of use and alternative therapies related to PIM for treatment of pain and inflammation in older adults ≥65 years in Brazil. The panel involved nine Brazilian experts in geriatric pharmacotherapy. All items with mean Likert scale score ≥4.0 (agree) and the lower limit of 95% confidence interval ≥4.0 were considered validated in this study.
Results: At the end of the consensus process, 94 (65.3%) items of 144 were validated. In total, consensus was reached for 33/35 (94.3%) concerns about drugs that should be avoided in older patients regardless of diagnosis, for 22/23 (95.7%) concerns about drugs that should be avoided in older patients with specific conditions or diseases, for 11/23 (47.8%) with special considerations of use, and for 28/63 (44.4%) of therapeutic alternatives.
Conclusion: Although these criteria are not designed to replace clinical judgement, PIM and alternative therapies lists can be useful to inform prescribers, pharmacists, and health care planners and may serve as a starting point for safe and effective use of medications in older people.
Introduction
The process of aging in a population is accompanied by a rising prevalence of chronic and degenerative diseases and, consequently, a higher incidence of conditions characterised by pain and inflammation (Horgas, 2017). Studies show that the prevalence of chronic pain among elderly people in the community ranges from 21.5% to 65.0%, depending on the study population, the sampling method, the interview method, and the definition of “chronic pain” (Hairi et al., 2013; Eggermont et al., 2014; Jackson et al., 2015; Leao Ferreira et al., 2016; Larsson et al., 2017; Cimas et al., 2018; Liberman et al., 2018; Dahlhamer et al., 2018).
Pain and inflammation management in older people is a challenge for health professionals. Older persons often have age-related physiological changes and a high number of comorbidities, and undergo a number of therapies, which increase the risk of adverse drug effects, making it difficult to establish a balance between the benefits and risks of medications used in this population (Hilmer et al., 2007; McLachlan et al., 2011). In addition, some of the most commonly prescribed medications for the treatment of pain and inflammation can confer significant risks on older adults and have been associated with the occurrence of adverse events such as falls, fractures, gastrointestinal bleeding, worsening of heart failure, cognitive impairment, and renal failure (Marcum and Hanlon, 2010; O’Neil et al., 2012).
Potentially inappropriate medication (PIM) is a term used to describe a medicine for which the risk associated with its use outweighs the potential benefits, especially when there are more effective alternatives available (Gallagher et al., 2008; Renom-Guiteras et al., 2015). Several explicit criteria have identified medications that are considered inappropriate for the treatment of pain and inflammation in older people (McLeod et al., 1997; Gallagher et al., 2008; Winit-Watjana et al., 2008; Holt et al., 2010; Kim et al., 2010; American Geriatrics Society Beers Criteria Update Expert P, 2012; Chang et al., 2012; Mann et al., 2012; Clyne et al., 2013; Renom-Guiteras et al., 2015; American Geriatrics Society Beers Criteria Update Expert P., 2015; Kim et al., 2015; O’Mahony et al., 2015; Oliveira et al., 2016). These tools were developed by expert consensus and provide an accessible resource for health professionals in different settings.
Despite the availability of information, PIMs continue to be prescribed and used as first-line medications in older people. The frequency of PIM is high across a variety of healthcare settings, including Brazil. According to Brazilian studies, 42–59% of older people use at least one PIM (Baldoni et al., 2014; Martins et al., 2015; Lutz et al., 2017; Nascimento et al., 2017). Some of most commonly PIMs are used for treating pain and inflammation. These results illustrate that more work is needed to improve the use of appropriate medications in older adults.
The first Brazilian consensus on PIMs was published in 2016 (Oliveira et al., 2016). Limitations reported by the authors included that the criteria were based on previous versions of Beers (2012) (American Geriatrics Society Beers Criteria Update Expert P, 2012) and STOPP (2008) (Gallagher et al., 2008) and did not incorporate therapeutic alternatives. Evidence-based clinical practice guidelines including the list of PIMs should be continuously updated to incorporate emerging or changing evidence as well as newly approved drugs in order to remain current in line with current evidence (Shekelle et al., 2012). In 2015, updates of Beers (American Geriatrics Society Beers Criteria Update Expert P., 2015) and STOPP (O’Mahony et al., 2015) and a new European list [EU(7)] were published (Renom-Guiteras et al., 2015). This last PIM list was based on several international PIM lists and contains suggestions for dose adjustments, special considerations of use and therapeutic alternatives.
Therefore, the aim of the present study was to develop and validate a PIM list for the treatment of pain and inflammation and their respective alternative therapies based on the three international PIM lists recently updated [Beers, STOPP, and EU(7) PIM list], applicable to Brazilian elderly individuals (Renom-Guiteras et al., 2015; American Geriatrics Society Beers Criteria Update Expert P., 2015; O’Mahony et al., 2015).
Methods
We used the modified Delphi technique to validate concerns and alternative therapies related to PIMs for the treatment of pain and inflammation in older adults aged ≥65 years in Brazil. This process combines evidence from the literature and expert opinion, and has been successful in the development of previous explicit criteria for older people (Kim et al., 2010; Chang et al., 2012; Renom-Guiteras et al., 2015; Kim et al., 2015; Oliveira et al., 2016; Aliberti et al., 2018). In this method, the search for consensus is systematic. The experts assess the information, also called propositions, presented by the researcher(s) in the form of a previously formulated questionnaire. The questionnaire is based on the literature review of a research problem and presents a synthesis of the main discussions on the subject during rounds (Dalkey, 1969; Campbell and Cantrill, 2001).
The development of this study comprised of five steps: preparation of a preliminary PIM list, the plan for a modified Delphi study (elaboration of a data collection instrument and selection of an expert panel), two rounds of survey, and the summary of consensus.
Preliminary List of PIM and Alternative Therapies for the Treatment of Pain and Inflammation
A systematic literature review was performed in order to identify possible screening tools for detection of PIMs published between January 1991 and April 2017 (Motter et al., 2018). After the review of 36 different tools, the list of PIMs related to pain and inflammation management was based on a combination of the relevant medicines from the updated Beers criteria (American Geriatrics Society Beers Criteria Update Expert P., 2015), updated STOPP criteria (O’Mahony et al., 2015), and EU(7) PIM list (Renom-Guiteras et al., 2015). These PIM lists are the most comprehensive and updated previously published lists. The original version of the PIM lists (in English) was translated into Brazilian Portuguese by two Brazilian researchers. The availability of medications and alternative therapies listed in the Brazilian market was confirmed by a medication database from the Brazilian National Health Surveillance Agency (National Agency of Sanitary Surveillance A, 2017). When a medication class was listed in a published PIM list, we identified all medications belonging to the class that were available in Brazil. The concerns about each medication/medication class were formulated using the information provided in the original list. The list of special considerations of use and alternative therapies was based on the EU(7) PIM lists (Renom-Guiteras et al., 2015).
The preliminary PIM list was organized by medication/medication class. In total, the list of 12 PIMs contained 104 items which involved: 35 concerns about medications/medication classes that should be avoided in older people regardless of diagnosis, 20 concerns about medications/medication classes that should be avoided in specific diseases or conditions, 19 dose adjustments and special considerations of use, and 30 possible therapeutic alternatives. In the second round, items suggested by experts during the first round could be added to the preliminary PIM list.
Selection of Expert Panel
The survey of experts was carried out through an initial search of the Lattes platform on the National Council for Scientific and Technological Development (CNPq) website (National Council of Technological and Scientific Development, 2016) on the 10th and 30th of August, 2016, using the following descriptors: “geriatric” and “medications.” The members were primarily selected based on their expertise in the areas of geriatric medicine and/or clinical pharmacology. Additionally, their regional location was considered in order to provide national representation and to gain national perspective on these topics. We identified 47 potential participants (geriatricians and pharmacists) who were then invited by email which contained information on the study objective and a link to access the informed consent form. They were assured that participation in the consensus process was voluntary and confidential.
First and Second Rounds
As the experts were based in disparate geographical locations across Brazil, an online two-round Delphi questionnaire was administered to facilitate efficient data collection; a link to the questionnaire on the Google Docs® website was provided. The first round took place between January and May 2017, and the second round between May and June 2017. We asked experts to assess each item of the preliminary list using a five-point Likert scale that ranged from one point (strongly disagree) to five points (strongly agree). The experts were also offered the opportunity to add items and to suggest alternative treatments. All the respondents in the first-round questionnaire were invited to participate in the second-round questionnaire. The second round included items for which no consensus had been reached in the first round (see Data Analysis section) and any new item suggested by experts in the first round. Quantitative feedback (percentage rating) from the first round of the Delphi process was incorporated into the survey questionnaire for the second round. The expert panel was instructed to consider the feedback provided while re-scoring the items contained in the second-round questionnaire. For both rounds, reminder emails were sent as necessary to encourage participation.
Data Analysis
The collected data were organized in an Excel spreadsheet and subsequently imported into STATA 12.0 statistical software (StataCorp LP, College Station, TX, USA). A descriptive analysis was performed, and the absolute and relative frequencies, means and 95% confidence interval (CI) of the study items were evaluated. At the end of the consensus process, only items with mean Likert scale ≥4.0 (agree) and lower limit of CI ≥4.0 were considered validated in this study. This cut-off point is similar to that used by Oliveira et al. (Oliveira et al., 2016) and higher than that used in another study with similar scale (Chang et al., 2012).
Results
Participants
Of the 13 experts who agreed to participate in the study, 10 were geriatricians and 3 were pharmacists. Among them, nine completed the first round while seven completed the second round. All respondents of the second round participated in first round. We were unable to identify which experts had left the panel, because the first round was conducted anonymously. At the end of the consensus process, all participants were geriatricians with more than 10 years of experience in geriatric medicine.
First and Second Rounds
In the first round, experts reached consensus on 51/104 (49.0%) items in the preliminary tool. Among these, 26/51 (51,0%) items were concerns about medication/medication classes that should be avoided in older people regardless of diagnosis, 17/51 (33,3%) were concerns about medication/medication classes that should be avoided in specific diseases or conditions, and seven were special considerations of use. Only one possible alternative therapy reached consensus in this step.
After the first round, the items were revised in concordance with the comments from the experts. Four items were modified, and 40 new items were added. The majority (32/40; 82.5%) of items suggested by the experts were possible alternative therapies. Items for which consensus was not achieved were resubmitted for the second round (N = 53).
In the second round, experts evaluated 97 items. Among these, 44/97 (45.4%) reached consensus. One modified item was validated and replaced the original item. At the end of the consensus process, 94 (65.3%) items of 144 were validated. In total, consensus was reached for 33/35 (94.3%) concerns about drugs that should be avoided in older patients regardless of diagnosis, for 22/23 (95.7%) of concerns about drugs that should be avoided in older patients in specific conditions or diseases, for 11/23 (47.8%) of special considerations of use, and for 28/63 (44.4%) of therapeutic alternatives.
Table 1 presents the medication/medication classes considered inappropriate for older people independent of their diagnosis and their respective average Likert scales and CIs. The expert panel classified nonsteroidal anti-inflammatory drugs (NSAIDs), muscle relaxants, colchicine, and opioids as PIMs regardless of the diagnosis in the study. Table 1 also provides information about dose adjustments and special considerations for medication use and alternative therapies validated by experts in this study.
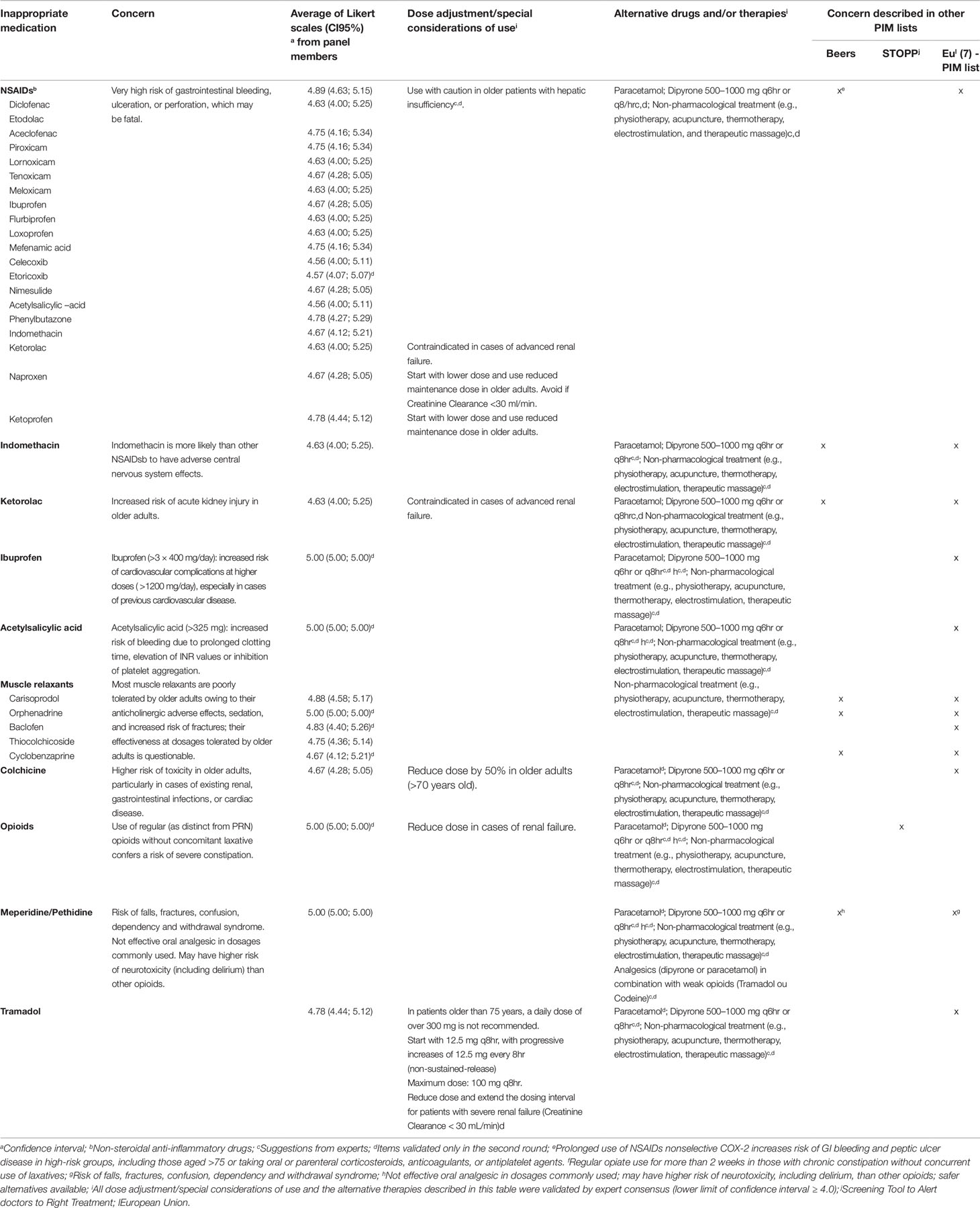
Table 1 Potentially inappropriate drugs for the older patients independent of diagnosis validated by expert consensus.
A consensus also was reached for eight medication/medication classes that should be avoided in older patients with 16 different conditions or diseases (Table 2). The use of NSAIDs was considered inappropriate for seven different conditions (long term use in osteoarthritis and gout, history of peptic ulcer disease or gastrointestinal bleeding, hypertension, heart disease, and chronic kidney disease stage IV and V or estimated glomerular filtration rate <50 ml/min per 1.73 m2) while the use of corticosteroids was considered inappropriate in five different conditions (rheumatoid arthritis, osteoarthritis, osteoporosis, diabetes, and delirium).
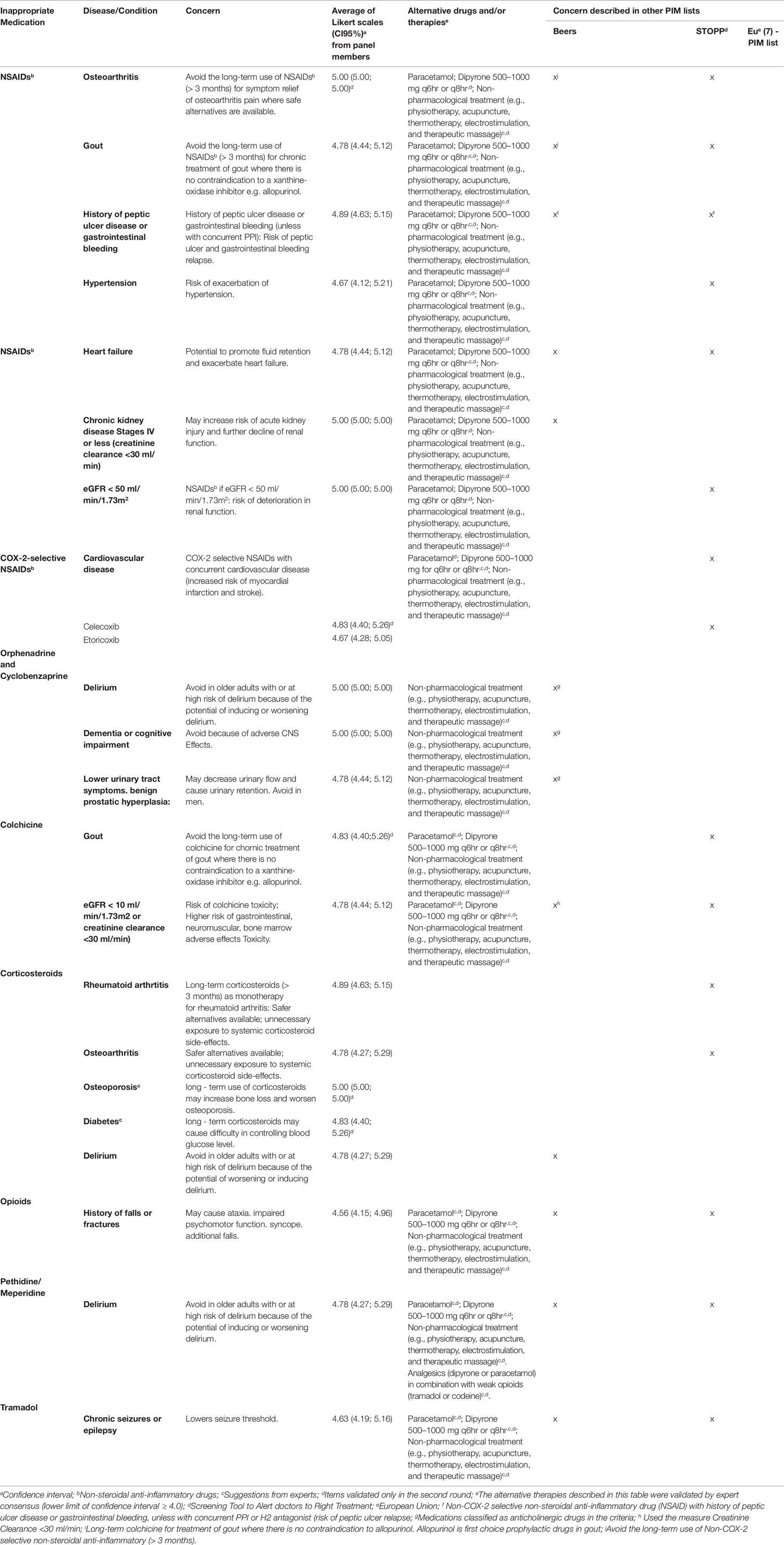
Table 2 Potentially inappropriate medication use in the older patients considering diagnoses or conditions.
We presented the concerns also described in other PIM lists such as Beers (American Geriatrics Society Beers Criteria Update Expert P., 2015), STOPP criteria (O’Mahony et al., 2015) and the EU(7) PIM list (Renom-Guiteras et al., 2015) (Tables 1 and 2). Among all concerns validated in this study, about 65% were also reported in Beers consensus (American Geriatrics Society Beers Criteria Update Expert P, 2015). Lower consistency was observed when our list was compared with the STOPP criteria (47.2%) (O’Mahony et al., 2015) and the EU(7) PIM list (40.0%) (Renom-Guiteras et al., 2015).
In this study, the experts did not achieve consensus on 2/35 (5.7%) medication concerns regardless of diagnoses (phenylbutazone and tizanidine), on the use of strong opioids as first-line therapy for mild pain, and 12/23 (52.2%) dose adjustment/special considerations for medication use (i.e. special considerations for meperidine, indomethacin, and baclofen use) (Appendix I). The panel also did not reach a consensus about 35/63 (55.5%) alternatives therapies. These included medications such as ibuprofen, naproxen, and weak opioids (Appendix II).
Discussion
The consensus method allowed us to identify PIM criteria and alternative treatment options for the treatment of pain and inflammation in older people, adapted to the Brazilian context. The panel reached consensus on 94 items which contain important information about the use of medicines for the treatment of pain and inflammation in older adults. Although these criteria were not designed to replace clinical judgement, PIM, and alternative therapy lists can be useful in informing prescribers, pharmacists, and health care planners (Hanlon et al., 2015), and may serve as a starting point for the safe and effective use of medications to treat pain and inflammation in older people. To the best of our knowledge, this is the first study in which a consensus on alternative therapies to PIMs adapted to the Brazilian context was reached.
In the absence of a strong evidence to guide the optimization of medication regimens in elderly people, the consensus of experts has been used as a strategy to develop PIM lists in several countries. The elaboration of PIM lists consists of a complex, dynamic, and time-consuming process which involves the combination of systematic reviews and expert opinion. For these reasons, many researchers have combined two or more tools and added other medications that they considered were missing in order to develop and adapt existing criteria to different settings (Kim et al., 2010; Chang et al., 2012; Renom-Guiteras et al., 2015; Kim et al., 2015; Oliveira et al., 2016). Our list was based on the Beers criteria (American Geriatrics Society Beers Criteria Update Expert P, 2015), STOPP criteria (O’Mahony et al., 2015), and the EU(7) PIM lists published in 2015 (Renom-Guiteras et al., 2015). Although this last list has not been widely used compared with the Beers and STOPP criteria, it included some drugs rarely included in other PIM lists and therapeutic alternatives.
We have compared the results obtained in this consensus with previous lists: Beers criteria (American Geriatrics Society Beers Criteria Update Expert P, 2015), STOPP criteria (O’Mahony et al., 2015), EU(7) PIM list (Renom-Guiteras et al., 2015), and Brazilian PIM list (Oliveira et al., 2016). Although the list developed by Oliveira et al. (Oliveira et al., 2016) was based on previous versions of Beers (2012) (American Geriatrics Society Beers Criteria Update Expert P, 2012) and STOPP (2008) (Gallagher et al, 2008), it was the first Brazilian PIM list. Thus, the comparison between our list and previous explicit criteria may contribute to improving the knowledge on PIMs and alternative therapies which had not been previously investigated in the Brazilian setting.
In our study, consensus in the Delphi process was reached for 95% of the concerns related to the use of medications for the treatment of pain and inflammation in elderly individuals. In contrast with Beers criteria (American Geriatrics Society Beers Criteria Update Expert P., 2015) and the Brazilian PIM list (Oliveira et al., 2016), all NSAIDs were considered to be PIMs, regardless of the diagnosis, in our study. These results may be justified by the fact that our experts suggested and validated alternative therapies for these medications. They considered that one approach to reducing adverse drug reactions associated with NSAIDs is to avoid the use of these medications and use preferred alternative therapies, especially in those older adults with pre-existing diseases. There are few data informing the use of these medications in elderly who frequently have additional comorbidities and use multiple medications which increase the risk of adverse effects (Reid et al., 2011; Makris et al., 2017). On the other hand, for those patients that require an NSAID even after the use of alternative therapies, the experts also reached consensus that some NSAID should be used at the lowest effective dose. In addition, this panel incorporated two new concerns about the use of corticoids in older people who have diagnosed with osteoporosis and diabetes. These concerns were also presented in other previously published PIM lists (Winit-Watjana et al., 2008; Kim et al., 2010).
Some concerns about medications only achieved consensus in the second round of questioning. In these cases, there was doubt about the evidence concerning the increased risk of adverse effects in elderly patients. For example, we can cite the concern about the use of celecoxib in older patients diagnosed with cardiovascular diseases, where there is conflicting data from different randomised controlled trials (Solomon et al., 2005; Nissen, 2017).
A consensus could not be reached on two concerns (phenylbutazone and tizanidine) regardless of diagnosis even after the second round. These medications were also not described as PIMs independent of diagnosis in the Brazilian list published during the Delphi process (Oliveira et al., 2016). This result may be explained by the lack of experience regarding the use of these medications in the Brazilian context, since they are not included in the national list of essential medications (RENAME) available at no cost and are thus seldom prescribed in this setting (Ministry of Health, Secretariat of ScienceTechnology and Strategic Inputs. [National List of Essential Medicines: RENAME 2017]: Ministry of Health, 2017). Regarding PIM in specific disease or conditions, the concern about the use of strong oral or transdermal opioids as first-line therapy for mild pain, also did not achieve consensus; it received the lowest media in this study. The appropriate pain assessment in older patients may be complex. Barriers such as underreporting of pain by patients and the presence of cognitive deficits and comorbidities may complicate this evaluation in older people (Horgas, 2017; Schofield, 2018). Thus, some experts may have considered that the prescription of strong opioids should incorporate individualized clinical judgement, and that a generalised statement would not be appropriate.
In contrast to other lists, the recommendation about the combined use of NSAIDs and proton pump inhibitors (PPIs) did not reach a consensus in this study. This result is also because the experts did not think NSAIDs should be used in older people. Furthermore, during the consensus process, the experts were concerned that the prescription of drugs such as PPIs represents increasing drug burden which may also put individuals at risk of other adverse events such as fractures and Clostridium difficile infection. Studies showed that the co-administration of PPIs does not prevent NSAID-induced intestinal damage but might actually aggravate it (Scarpignato et al., 2016). Thus, this result suggests that specialists prefer to use alternative therapies rather than use PPIs to avoid problems related to the use of NSAIDs for the treatment of pain and inflammation.
The panel has also addressed possible alternative therapies which may be prescribed to treat pain and inflammation. Paracetamol (acetaminophen) and dipyrone (metamizole) were identified as possible alternative therapies by experts in several concerns. Although recent literature has demonstrated the limited efficacy of paracetamol (Marcum et al., 2016), it remains recommended in guidelines as a first-line pharmacologic treatment for older adults with mild-to-moderate pain (American Geriatrics Society Panel on Pharmacological Management of Persistent Pain in Older P, 2009; Abdulla et al., 2013). With its dose-dependent hepatotoxicity, the recommended maximum daily doses should not be exceeded (3250 mg) and it should be prescribed with caution (lower doses) in patients with pre-existing liver disease, malnutrition, anorexia, heavy alcohol intake, or in patients treated by hepatic enzyme inducers (rifampicin, phenytoin, carbamazepine, or barbiturates) (Yoon et al., 2016). Regarding the use of dypirone, studies have demonstrated that for short term use, this medication appeared to be a safe choice when compared to other analgesics. However, the intermediate and long term safety of dypirone are still not well documented (Kotter et al., 2015; Andrade et al., 2016).
Interestingly, the experts agree strongly about the use of non-pharmacological interventions such as physiotherapy, acupuncture, thermotherapy, electrostimulation, and therapeutic massage as alternative therapies for the treatment of pain and inflammation in older people. Nonpharmacological approaches can help avoid drugs that have high risks of causing adverse events. For this reason, the body of evidence about nonpharmacological approaches is growing in older adults, especially, in persons with dementia and delirium (Livingston et al., 2014; Resnick et al., 2014; Hshieh et al., 2015).
The internet-based Delphi method offers a practical and cost-effective approach to identifying areas of concordance and disagreement involving a geographically dispersed group of experts. Another advantage of this method is the anonymity that encourages experts to make statements on the basis of their personal knowledge and experience. Finally, a significant advantage of the Delphi method is that participants are very much aware at each stage of the results of the previous rounds, and there is scope for each expert to provide more detailed feedback on both the process and the results. In this study, the majority of alternative therapies were suggested by the experts. Some of these differ from other previously published PIM lists (Renom-Guiteras et al., 2015; American Geriatrics Society Beers Criteria Update Expert P, 2015; O’Mahony et al., 2015). This result demonstrated the importance of set-specific country lists. In this study, we selected the most comprehensive and updated lists published based on a literature review (Motter et al., 2018). To the best of our knowledge, to date, this study is the first to validate alternative therapies to PIMs in a Brazilian setting.
In order to minimise the inclusion of controversial PIMs or alternative therapies, we decided before the development of the consensus process that an item should be included in the final list only if the lower limit of the 95% CI was ≥ 4.0. Thus, not only the mean score was taken into consideration but also the degree of discord.
There are, however, some limitations which must be acknowledged in this study. Thus, the results must be interpreted with caution. Firstly, although we carefully searched for experts who comprised the consensus process panel, the limited participation of experts and the drop out of two participants in the second round may have compromised the representativeness of some areas of expertise and geographic regions. Secondly, the lack of engagement of experts in the second round may restrict the application of the Delphi method. Finally, the authors did not perform an evaluation of the quality and strength of evidence for each concern or alternative therapies presented in this study. The items were based on information available in some consensus publications referred to. These tools were published in 2015 and new findings from recent clinical trials or systematic review (Beers PIM list was updated in 2019) were not reviewed; thus, we recognize that some PIMs might have been added to or excluded from the next version.
Conclusions
Explicit criteria summarized specific statements for identifying problems with medications in older people which make drugs easy to use by clinicians and health professionals. Condition-specific country lists are an important tool which may improve the rational use of medications among older people. In this study, we reached a consensus on 94 items that contain important information about the use of medicines used in the treatment of pain and inflammation in older adults. We believe that the application of our criteria combined with clinical judgement should contribute to helping physicians, pharmacists, and other health professionals to optimize the treatment of pain and inflammation in older patients. In this study, we also included special considerations of use and therapeutic alternatives; these may be an important addition to the screening process in caring for elderly Brazilian people. Future research should evaluate the implementation of the list among health professionals, including the usefulness of the suggestions for special considerations of medication use and alternative therapies, and apply this methodology to other therapeutic areas.
Data Availability Statement
All datasets generated for this study are included in the article/Supplementary Material.
Ethics Statement
The studies involving human participants were reviewed and approved by Ethics Committee of Universidade do Vale do Rio dos Sinos (UNISINOS) (number: 1.731.392). The patients/participants provided their written informed consent to participate in this study.
Author Contributions
FM and VP participated in all stages of this research, from the design and interpretation of data to the final write-up. FM prepared the work documents during the development process, recruited the experts and coordinated the delphi survey. FM, VP, and SH assisted with interpretation of the data and preparation of the final version of PIM list. FM drafted the manuscript, supported by VP and SH. All the authors critically reviewed and approved the final manuscript.
Funding
FM was supported by the coordination for the improvement of Higher Education Personnel – CAPES through a doctorate at University of Vale do Rio dos Sinos, Brazil (grant number: 88887159088/2017-00). FM was also supported by CAPES through a sandwich doctorate fellowship at The University of Sydney, Australia (grant number: 88881.134589/2016-01). This systematic review was funded by the National Council for Scientific and Technological Development-CNPQ (grant number: 426720/2016-4). The funders were not involved in the design or conduct of the study, collection, analysis, or interpretation of the data or preparation or approval of the manuscript.
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Acknowledgments
We are very grateful to the members of the expert panel for their individual contributions to the validation of the Brazilian PIM list for the treatment of pain and inflammation. The following members of the expert panel who agreed to be acknowledged for their participation: Giancarlo Lucchetti, MD, PhD (School of Medicine, Federal University of Juiz de Fora, Juiz de Fora, MG, Brazil); Gislaine Bonardi, MD, PhD (Hospital Moinhos de Vento, HMV, Porto Alegre,RS, Brazil); Luciana Branco da Motta, MD, PhD (Rio de Janeiro State University, UERJ, Rio de Janeiro, RJ, Brazil) Milton Luiz Gorzoni, MD, PhD (Faculty of Medical Sciences of Santa Casa de São Paulo, São Paulo, SP, Brazil.), Roberta Rigo Dalla Corte, MD, PhD (Hospital das Clínicas de Porto Alegre /Federal University of Rio Grande do Sul, Porto Alegre, RS, Brazil) Thiago Junqueira Avelino da Silva, MD, PhD (Laboratory of Medical Research in Aging (LIM-66), Hospital das Clinicas, University of São Paulo Medical School, São Paulo, SP, Brazil). Furthermore, We thank to the Coordination for the Improvement of Higher Education Personnel, National Council for Scientific and Technological Development for the support that they are providing for development of this study.
Supplementary Material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fphar.2019.01408/full#supplementary-material
References
Abdulla, A., Adams, N., Bone, M., Elliott, A. M., Gaffin, J., Jones, D., et al. (2013). Guidance on the management of pain in older people. Age Ageing 42 Suppl 1, i1–57. doi: 10.1093/ageing/afs200. PubMed PMID: 23420266
Aliberti, M. J. R., Apolinario, D., Suemoto, C. K., Melo, J. A., Fortes-Filho, S. Q., Saraiva, M. D., et al. (2018). Targeted geriatric assessment for fast-paced healthcare settings: development, validity, and reliability. J. Am. Geriatr. Soc. 66 (4), 748–754. doi: 10.1111/jgs.15303
American Geriatrics Society Beers Criteria Update Expert P. (2012). American Geriatrics Society updated Beers Criteria for potentially inappropriate medication use in older adults. J. Am. Geriatr. Soc. 60, 616–631. doi: 10.1111/j.1532-5415.2012.03923.x
American Geriatrics Society Beers Criteria Update Expert P. (2015). American geriatrics society 2015 updated beers criteria for potentially inappropriate medication use in older adults. J. Am. Geriatr. Soc. 63, 2227–2246. doi: 10.1111/jgs.13702
American Geriatrics Society Panel on Pharmacological Management of Persistent Pain in Older P (2009). Pharmacological management of persistent pain in older persons. J. Am. Geriatr. Soc. 57, 1331–1346. doi: 10.1111/j.1532-5415.2009.02376.x
Andrade, S., Bartels, D. B., Lange, R., Sandford, L., Gurwitz, J. (2016). Safety of metamizole: a systematic review of the literature. J. Clin. Pharm. Ther. 41, 459–477. doi: 10.1111/jcpt.12422
Baldoni, AdO, Ayres, L. R., Martinez, E. Z., Dewulf, NdLS, dos Santos, V., et al. (2014). Factors associated with potentially inappropriate medications use by the elderly according to Beers criteria 2003 and 2012. Int. J. Clin. Pharmacol. Ther. 36, 316–324. doi: 10.1007/s11096-013-9880-y
Campbell, S. M., Cantrill, J. A. (2001). Consensus methods in prescribing research. J. Clin. Pharm. Ther. 26, 5–14. doi: 10.1111/j.1365-2710.2001.00331.x
Chang, C. B., Yang, S. Y., Lai, H. Y., Wu, R. S., Liu, H. C., Hsu, H. Y., et al. (2012). Using published criteria to develop a list of potentially inappropriate medications for elderly patients in Taiwan. Pharmacoepidemiol. Drug Saf. 21, 1269–1279. doi: 10.1002/pds.3274
Cimas, M., Ayala, A., Sanz, B., Agullo-Tomas, M. S., Escobar, A., Forjaz, M. J. (2018). Chronic musculoskeletal pain in European older adults: Cross-national and gender differences. Eur. J. Pain 22 (2), 333–345. doi: 10.1002/ejp.1123
Clyne, B., Bradley, M. C., Hughes, C. M., Clear, D., McDonnell, R., Williams, D., et al. (2013). Addressing potentially inappropriate prescribing in older patients: development and pilot study of an intervention in primary care (the OPTI-SCRIPT study). BMC Health Serv. Res. 13, 307. doi: 10.1186/1472-6963-13-307
Dahlhamer, J., Lucas, J., Zelaya, C., Nahin, R., Mackey, S., DeBar, L., et al. (2018). Prevalence of Chronic Pain and High-Impact Chronic Pain Among Adults - United States, 2016. MMWR Morb. Mortal Wkly. Rep. 67 (36), 1001–1006. doi: 10.15585/mmwr.mm6736a2
Dalkey, N. C. (1969). The Delphi method: an experimental study of group opinion Santa Monica. CA:RAND Corporation. Available from: http://www.rand.org/pubs/research_memoranda/RM5888.
Eggermont, L. H., Leveille, S. G., Shi, L., Kiely, D. K., Shmerling, R. H., Jones, R. N., et al. (2014). Pain characteristics associated with the onset of disability in older adults: the maintenance of balance, independent living, intellect, and zest in the Elderly Boston Study. J. Am. Geriatr. Soc. 62 (6), 1007–1016. doi: 10.1111/jgs.12848
Gallagher, P., Ryan, C., Byrne, S., Kennedy, J., O’Mahony, D. (2008). STOPP (Screening Tool of Older Person’s Prescriptions) and START (Screening Tool to Alert doctors to Right Treatment). Consensus validation. Int. J. Clin. Pharmacol. Ther. 46, 72–83. doi: 10.5414/CPP46072
Hairi, N. N., Cumming, R. G., Blyth, F. M., Naganathan, V. (2013). Chronic pain, impact of pain and pain severity with physical disability in older people–is there a gender difference? Maturitas 74 (1), 68–73. doi: 10.1016/j.maturitas.2012.10.001
Hanlon, J. T., Semla, T. P., Schmader, K. E. (2015). Alternative medications for medications in the use of high-risk medications in the elderly and potentially harmful drug-disease interactions in the elderly quality measures. J. Am. Geriatr. Soc. 63, e8–e18. doi: 10.1111/jgs.13807
Hilmer, S. N., McLachlan, A. J., Le Couteur, D. G. (2007). Clinical pharmacology in the geriatric patient. Fundam. Clin. Pharmacol. 21, 217–230. doi: 10.1111/j.1472-8206.2007.00473.x
Holt, S., Schmiedl, S., Thurmann, P. A. (2010). Potentially inappropriate medications in the elderly: the PRISCUS list. Deutsches Arzteblatt Int. 107, 543–551. doi: 10.3238/arztebl.2010.0543
Horgas, A. L. (2017). Pain Management in Older Adults. Nurs. Clinics North America 52, e1–e7. doi: 10.1016/j.cnur.2017.08.001
Hshieh, T. T., Yue, J., Oh, E., Puelle, M., Dowal, S., Travison, T., et al. (2015). Effectiveness of multicomponent nonpharmacological delirium interventions: a meta-analysis. JAMA Intern. Med. 175, 512–520. doi: 10.1001/jamainternmed.2014.7779
Jackson, T., Thomas, S., Stabile, V., Han, X., Shotwell, M., McQueen, K. (2015). Prevalence of chronic pain in low-income and middle-income countries: a systematic review and meta-analysis. Lancet 385 Suppl 2, S10. doi: 10.1016/S0140-6736(15)60805-4
Kim, D. S., Heo, S. I., Lee, S. H. (2010). Development of a list of potentially inappropriate drugs for the korean elderly using the delphi method. Healthcare Inf. Res. 16, 231–252. doi: 10.4258/hir.2010.16.4.231
Kim, S.-O., Jang, S., Kim, C.-M., Kim, Y.-R., Sohn, H. S. (2015). Consensus Validated List of Potentially Inappropriate Medication for the Elderly and Their Prevalence in South Korea. Int. J. Gerontol. 9, 136–141. doi: 10.1016/j.ijge.2015.05.013
Kotter, T., da Costa, B. R., Fassler, M., Blozik, E., Linde, K., Juni, P., et al. (2015). Metamizole-associated adverse events: a systematic review and meta-analysis. PloS One 10, e0122918. doi: 10.1371/journal.pone.0122918
Larsson, C., Hansson, E. E., Sundquist, K., Jakobsson, U. (2017). Chronic pain in older adults: prevalence, incidence, and risk factors. Scand. J. Rheumatol. 46 (4), 317–325. doi: 10.1080/03009742.2016.1218543
Leao Ferreira, K. A., Bastos, T. R., Andrade, D. C., Silva, A. M., Appolinario, J. C., Teixeira, M. J., et al. (2016). Prevalence of chronic pain in a metropolitan area of a developing country: a population-based study. Arq. Neuropsiquiatr. 74 (12), 990–998. doi: 10.1590/0004-282X20160156
Liberman, O., Freud, T., Peleg, R., Keren, A., Press, Y. (2018). Chronic pain and geriatric syndromes in community-dwelling patients aged >/ = 65 years. J. Pain Res. 11, 1171–1180. doi: 10.2147/JPR.S160847
Livingston, G., Kelly, L., Lewis-Holmes, E., Baio, G., Morris, S., Patel, N., et al. (2014). Non-pharmacological interventions for agitation in dementia: systematic review of randomised controlled trials. Br. J. Psychiatry 205, 436–442. doi: 10.1192/bjp.bp.113.141119
Lutz, B. H., Miranda, V. I. A., Bertoldi, A. D. (2017). Potentially inappropriate medications among older adults in Pelotas, Southern Brazil. Rev. Saude Publica 51, 52. doi: 10.1590/s1518-8787.2017051006556
Makris, U. E., Misra, D., Yung, R. (2017). Gaps in aging research as it applies to rheumatologic clinical care. Clinics In Geriatr. Med. 33, 119–133. doi: 10.1016/j.cger.2016.08.009
Mann, E., Bohmdorfer, B., Fruhwald, T., Roller-Wirnsberger, R. E., Dovjak, P., Duckelmann-Hofer, C., et al. (2012). Potentially inappropriate medication in geriatric patients: the Austrian consensus panel list. Wien Klin. Wochenschr. 124, 160–169. doi: 10.1007/s00508-011-0061-5
Marcum, Z. A., Hanlon, J. T. (2010). Recognizing the Risks of Chronic Nonsteroidal Anti-Inflammatory Drug Use in Older Adults. Ann. Longterm Care 18, 24–27.
Marcum, Z. A., Duncan, N. A., Makris, U. E. (2016). Pharmacotherapies in geriatric chronic pain management. Clinics In Geriatr. Med. 32, 705–724. doi: 10.1016/j.cger.2016.06.007
Martins, G. A., Acurcio Fde, A., Franceschini Sdo, C., Priore, S. E., Ribeiro, A. Q. (2015). [Use of potentially inappropriate medications in the elderly in Vicosa, Minas Gerais State, Brazil: a population-based survey]. Cad Saude Publica 31, 2401–2412. doi: 10.1590/0102-311X00128214
McLachlan, A. J., Bath, S., Naganathan, V., Hilmer, S. N., Le Couteur, D. G., Gibson, S. J., et al. (2011). Clinical pharmacology of analgesic medicines in older people: impact of frailty and cognitive impairment. Br. J. Clin. Pharmacol. 71, 351–364. doi: 10.1111/j.1365-2125.2010.03847.x
McLeod, P. J., Huang, A. R., Tamblyn, R. M., Gayton, D. C. (1997). Defining inappropriate practices in prescribing for elderly people: a national consensus panel. CMAJ 156, 385–391.
Ministry of Health, Secretariat of ScienceTechnology and Strategic Inputs. [National List of Essential Medicines: RENAME 2017]: Ministry of Health (2017). [cited 2017 10 August]. 210]. Available from: http://bvsms.saude.gov.br/bvs/publicacoes/relacao_nacional_medicamentos_rename_2017.pdf.
Motter, F. R., Fritzen, J. S., Hilmer, S. N., Paniz, E. V., Paniz, V. M. V. (2018). Potentially inappropriate medication in the elderly: a systematic review of validated explicit criteria. Eur. J. Clin. Pharmacol. 74 (6), 679–700. doi: 10.1007/s00228-018-2446-0
Nascimento, M. M., Mambrini, J. V., Lima-Costa, M. F., Firmo, J. O., Peixoto, S. W., de Loyola Filho, A. I., et al. (2017). Potentially inappropriate medications: predictor for mortality in a cohort of community-dwelling older adults. Eur. J. Clin. Pharmacol. 73 (5), 615–621. doi: 10.1007/s00228-017-2202-x
National Agency of Sanitary Surveillance A. (2017). The Consultation of Regularized Products - Medicines Available from: https://consultas.anvisa.gov.br/#/medicamentos/.
National Council of Technological and Scientific Development. (2016). Lattes platform. Brasília: CNpq. Available from: http://lattes.cnpq.br/.
Nissen, S. E. (2017). Cardiovascular safety of celecoxib, naproxen, or ibuprofen for arthritis. New Engl. J. Med. 376, 1390. doi: 10.1056/NEJMc1702534
O’Mahony, D., O’Sullivan, D., Byrne, S., O’Connor, M. N., Ryan, C., Gallagher, P. (2015). STOPP/START criteria for potentially inappropriate prescribing in older people: version 2. Age Ageing 44, 213–218. doi: 10.1093/ageing/afu145
O’Neil, C. K., Hanlon, J. T., Marcum, Z. A. (2012). Adverse effects of analgesics commonly used by older adults with osteoarthritis: focus on non-opioid and opioid analgesics. Am. J. Geriatr. Pharmacother. 10, 331–342. doi: 10.1016/j.amjopharm.2012.09.004
Oliveira, M. G., Amorin, W. W., Oliveira, C. R. B., Coqueiro, H. L., Gusmao, L. C., Passos, L. C. (2016). [Brazilian consensus of potentially inappropriate medication for elderly people]. Geriatr. Gerontol. Aging 10, 168–181. doi: 10.5327/Z2447-211520161600054
Reid, M. C., Bennett, D. A., Chen, W. G., Eldadah, B. A., Farrar, J. T., Ferrell, B. (2011). Improving the pharmacologic management of pain in older adults: identifying the research gaps and methods to address them. Pain Med. 12, 1336–1357. doi: 10.1111/j.1526-4637.2011.01211.x
Renom-Guiteras, A., Meyer, G., Thurmann, P. A. (2015). The EU(7)-PIM list: a list of potentially inappropriate medications for older people consented by experts from seven European countries. Eur. J. Clin. Pharmacol. 71, 861–875. doi: 10.1007/s00228-015-1860-9
Resnick, B., Kolanowski, A. M., Van Haitsma, K. (2014). Promoting positive behavioral health: a nonpharmacological toolkit for senior living communities. J. Gerontol. Nurs. 40, 2–3. doi: 10.3928/00989134-20131206-01
Scarpignato, C., Gatta, L., Zullo, A., Blandizzi, C., Group, S-A-FItalian Society of Pharmacology tIAoHG (2016). Effective and safe proton pump inhibitor therapy in acid-related diseases - A position paper addressing benefits and potential harms of acid suppression. BMC Med. 14, 179. doi: 10.1186/s12916-016-0718-z
Schofield, P. (2018). The assessment of pain in older people: UK National Guidelines. Age Ageing 47 Suppl 1, i1–i22. doi: 10.1093/ageing/afx192
Shekelle, P., Woolf, S., Grimshaw, J. M., Schunemann, H. J., Eccles, M. P. (2012). Developing clinical practice guidelines: reviewing, reporting, and publishing guidelines; updating guidelines; and the emerging issues of enhancing guideline implementability and accounting for comorbid conditions in guideline development. Implement. Sci.: IS 7, 62. doi: 10.1186/1748-5908-7-62
Solomon, S. D., McMurray, J. J., Pfeffer, M. A., Wittes, J., Fowler, R., Finn, P., et al. (2005). Cardiovascular risk associated with celecoxib in a clinical trial for colorectal adenoma prevention. New Engl. J. Med. 352, 1071–1080. doi: 10.1056/NEJMoa050405
Winit-Watjana, W., Sakulrat, P., Kespichayawattana, J. (2008). Criteria for high-risk medication use in Thai older patients. Arch. Gerontol. Geriatr. 47, 35–51. doi: 10.1016/j.archger.2007.06.006
Keywords: inappropriate prescribing, potentially inappropriate medications list, pain management, deprescriptions, aged, Brazil
Citation: Motter FR, Hilmer SN and Paniz VMV (2019) Pain and Inflammation Management in Older Adults: A Brazilian Consensus of Potentially Inappropriate Medication and Their Alternative Therapies. Front. Pharmacol. 10:1408. doi: 10.3389/fphar.2019.01408
Received: 31 July 2019; Accepted: 05 November 2019;
Published: 02 December 2019.
Edited by:
Luciane Cruz Lopes, Universidade de Sorocaba, BrazilReviewed by:
Monique M. Elseviers, University of Antwerp, BelgiumMarlon Aliberti, University of São Paulo, Brazil
Copyright © 2019 Motter, Hilmer and Paniz. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Fabiane Raquel Motter, ZmFiaWFuZW1vdHRlckBnbWFpbC5jb20=