 Tamás Ágh1*
Tamás Ágh1* Job FM van Boven2
Job FM van Boven2 Björn Wettermark3,4
Björn Wettermark3,4 Enrica Menditto5
Enrica Menditto5 Hilary Pinnock6
Hilary Pinnock6 Ioanna Tsiligianni7
Ioanna Tsiligianni7 Guenka Petrova8
Guenka Petrova8 Ines Potočnjak9
Ines Potočnjak9 Fatjona Kamberi10
Fatjona Kamberi10 Przemyslaw Kardas11 European Network to Advance Best practices & technoLogy on medication adherencE (ENABLE)
Przemyslaw Kardas11 European Network to Advance Best practices & technoLogy on medication adherencE (ENABLE)- 1Syreon Research Institute, Budapest, Hungary
- 2Department of Clinical Pharmacy and Pharmacology, Medication Adherence Expertise Center of the Northern Netherlands, University Medical Center Groningen, University of Groningen, Groningen, Netherlands
- 3Department of Pharmacy, Faculty of Pharmacy, Uppsala University, Uppsala, Sweden
- 4Faculty of Medicine, Vilnius University, Vilnius, Lithuania
- 5Department of Pharmacy, CIRFF, Center of Pharmacoeconomics and Drug Utilization Research, University of Naples Federico II, Naples, Italy
- 6Usher Institute, University of Edinburgh, Edinburgh, United Kingdom
- 7Department of Social Medicine, School of Medicine, University of Crete, Crete, Greece
- 8Departement of Social Pharmacy and Pharmacoeconomics, Faculty of Pharmacy, Medical University of Sofia, Sofia, Bulgaria
- 9Institute for Clinical Medical Research and Education, University Hospital Centre Sisters of Charity, Zagreb, Croatia
- 10Faculty of Health, Research Center of Public Health, University of Vlore "Ismail Qemali", Vlore, Albania
- 11Medication Adherence Research Centre, Department of Family Medicine, Medical University of Lodz, Lodz, Poland
Maintaining healthcare for noncommunicable diseases (NCDs) is particularly important during the COVID-19 pandemic; however, diversion of resources to acute care, and physical distancing restrictions markedly affected management of NCDs. We aimed to assess the medication management practices in place for NCDs during the second wave of the COVID-19 pandemic across European countries. In December 2020, the European Network to Advance Best practices & technoLogy on medication adherencE (ENABLE) conducted a cross-sectional, web-based survey in 38 European and one non-European countries. Besides descriptive statistics of responses, nonparametric tests and generalized linear models were used to evaluate the impact on available NCD services of the number of COVID-19 cases and deaths per 100,000 inhabitants, and gross domestic product (GDP) per capita. Fifty-three collaborators from 39 countries completed the survey. In 35 (90%) countries face-to-face primary-care, and out-patient consultations were reduced during the COVID-19 pandemic. The mean ± SD number of available forms of teleconsultation services in the public healthcare system was 3 ± 1.3. Electronic prescriptions were available in 36 (92%) countries. Online ordering and home delivery of prescription medication (avoiding pharmacy visits) were available in 18 (46%) and 26 (67%) countries, respectively. In 20 (51%) countries our respondents were unaware of any national guidelines regarding maintaining medication availability for NCDs, nor advice for patients on how to ensure access to medication and adherence during the pandemic. Our results point to an urgent need for a paradigm shift in NCD-related healthcare services to assure the maintenance of chronic pharmacological treatments during COVID-19 outbreaks, as well as possible future disasters.
Introduction
Noncommunicable diseases (NCDs) are a major public health issue, responsible for 80% of all years lived with disability and 70% of all deaths worldwide [World Health Organization (WHO), 2018a; Institute for Health Metrics and Evaluation (IHME), 2020]. However, because of the COVID-19 pandemic [World Health Organization (WHO), 2020a], NCDs have not been the main priority for healthcare services during the last year, as COVID-19 infected more than 114 million individuals, with 2.5 million deaths worldwide [European Centre for Disease Prevention and Control (ECDC), 2021].
Notably, the epidemics of COVID-19 and NCDs are closely interlinked. Patients with NCDs are more susceptible to severe and fatal COVID-19 infection (Clark et al., 2020; CDC COVID-19 Response Team, 2020; Noor and Islam, 2020; Sheldon and Wright, 2020). Conversely, COVID-19 negatively affects lifestyle habits (e.g., lower physical activity, increased tobacco use); indirectly increasing the risk of developing and progression of NCDs (Palmer et al., 2020; Papachristou et al., 2020). There is also a growing body of evidence that effective management of NCDs has a protective effect against COVID-19 infection, and its severity. For example, continuous statin use during the month prior to hospital admission for COVID-19 was associated with a lower risk of developing severe infection, and a faster time to recovery (Daniels et al., 2020).
Although, the appropriate management of NCDs is important during the COVID-19 pandemic, the intensive focus on COVID-19 prevention and treatment, the lockdown and physical distancing restrictions affected NCD-related healthcare services adversely. In May 2020, World Health Organization (WHO) surveyed service delivery for NCDs across 155 countries [World Health Organization (WHO), 2020b] and found that COVID-19 markedly affected NCD services in all regions and income groups. In three-quarters of countries there was considerable disruption to NCD services (e.g., rehabilitation services, hypertension management, diabetes care, asthma services). To overcome disruption many countries adopted strategies such as telemedicine services to replace in-person consultations (61% of countries) or triage to identify priorities (64% of countries).
The continuity of medication therapy is a cornerstone for the effective management of NCDs (Böhm et al., 2013; Kluge et al., 2020). Even before the COVID-19 pandemic, about 50% of people with long-term conditions were non-adherent to their medication [World Health Organization (WHO), 2003] with potential serious health consequences for individuals (Chowdhury et al., 2013). For example, non-adherence to endocrine therapies in breast cancer patients increases the risk of metastases, disease recurrence and mortality (Font et al., 2019; Lee et al., 2019). Assuring continuous access to medication is a prerequisite of appropriate adherence, which may be compromised by disruptions of healthcare services and physical distancing restrictions due to COVID-19 crisis.
The European Network to Advance Best practices & technoLogy on medication adherencE (ENABLE; CA19132) is a 4-years research initiative across Europe funded by the European Cooperation in Science and Technology (COST) Action. ENABLE brings together researchers from 39 countries, among others, with the objective to evaluate current practices related to medication adherence. ENABLE thus considered it important to survey its members on medication management practices during the pandemic, following deepening concerns that European patients with NCDs may be not receiving appropriate care or access to essential medicines [World Health Organization (WHO), 2020b; Minghui et al., 2020] The aim of this study was to assess and critically evaluate the medication management practices in place for NCDs during the second wave of the COVID-19 pandemic across European countries to inform future pandemic management.
Materials and Methods
Study Design
A cross-sectional, web-based survey was carried out including all the members of ENABLE (i.e., healthcare providers and academics with medical or pharmaceutical backgrounds) across 38 European countries (i.e., Albania, Austria, Belgium, Bosnia and Herzegovina, Bulgaria, Croatia, Cyprus, Czechia, Denmark, Estonia, Finland, France, Germany, Greece, Hungary, Iceland, Ireland, Italy, Latvia, Lithuania, Luxemburg, Malta, Moldova, Montenegro, the Netherlands, North Macedonia, Norway, Poland, Portugal, Romania, Serbia, Slovakia, Slovenia, Spain, Sweden, Switzerland, Turkey and the United Kingdom) and one non-European (i.e., Israel) country. The primary outcome of the survey was a better understanding on the medication management practices for NCDs during the second wave of COVID-19 across Europe. Ethical approval was not sought as all participants were ENABLE colleagues reporting publicly available information about their country healthcare systems. No personal data were stored in relation to this study. All respondents were asked if they wished to be acknowledged in publications. This study was reported according to the Checklist for Reporting Results of Internet E-Surveys (CHERRIES) (Eysenbach, 2004).
Questionnaire Development and Data Collection
First, key elements of the medication management cycle of NCDs were defined by the working group as a result of extensive discussions (Figure 1). The questionnaire was developed based upon this framework using following domains: 1) patient and healthcare system regulations, 2) means of communication between the patient and prescriber, 3) prescriber, 4) prescription, 5) community pharmacy regulations, 6) medication, and 7) medication taking. A number of questions was generated for each domain. As part of the validation of the draft questionnaire, seven external experts were asked to assess each item individually with respect to the content, construct and criterion validity and to offer their opinions on the overall questionnaire and on the technical functionality of the electronic questionnaire. Following revision, the final version of the questionnaire contained 33 questions. The majority of questions were closed with responses: “Yes”/“Partly”/“No”/“Do not know.” Respondents were instructed to answer “Yes” if the scenario took place in >80% of cases in the given country, and “Partly” or “No” in 20–80% of cases, and <20% of cases, respectively. The case ratio for the “Partly” answer was determined based on a consensus discussion by ENABLE collaborators and was approved by the external experts.

FIGURE 1. Medication management cycle and interventions that could help continuous pharmacological management of non-communicable diseases.
The link to the validated, web-based survey was sent by email to all ENABLE collaborators (n = 92, two or three representatives from each of 39 countries) on December 15th, 2020. The invitation email informed participants about the purpose of the study, the use and storage of the data and the length of the survey. The survey was posted on SurveyMonkey.com (www. surveymonkey.com). The online questionnaire was distributed over 12 pages, with one to five items per page. A copy of the survey can be seen in Supplementary Figure S1. The average time required to answer the survey was been estimated at 10 min and the respondents were able to review and change their answers before submitting the survey. This voluntary study was sent personally to ENABLE colleagues so that access to the questionnaire by non-invited individuals was unlikely. No incentives were offered to ENABLE collaborators for completing the survey. Respondents were instructed to represent the national perspective, rather than regional, local or their own perspective; and to provide responses as of December 2020. The responses should reflect the current measures in place to support treatment of NCDs in the country, regardless of whether they had been introduced following the COVID-19 outbreak or had been in place before the pandemic. The survey was open until December 29th, 2020, reminders were sent weekly to all participants.
To prevent multiple entries from the same individual, respondents’ names were stored temporarily with the submitted survey. However, unique user identifiers were eliminated before data analysis.
Data Analysis
A completeness check was conducted after the questionnaire was submitted and only complete questionnaires (regardless of the time needed for filling the questionnaire) were analyzed. Where more than one complete response was received per country, the responses were aggregated. In the few instances where answers differed, respondents were contacted to resolve the inconsistencies prior to data analysis.
In the first step of data analysis, descriptive statistics of the responses were computed. In the next step, we evaluated the impact of three variables on the solutions available to facilitate continuity of medication for NCDs during the COVID-19 pandemic. European Centre for Disease Prevention and Control (ECDC) data were used for the number of COVID-19 cases per 100,000 inhabitants, and the number of COVID-19 deaths per 100,000 inhabitants in 2020 [European Centre for Disease Prevention and Control (ECDC), 2021]. Country income was assessed from World Bank data on gross domestic product (GDP) per capita at purchasing power parity in current international USD (data from 2019) (World Bank, 2021) (Table 1). Differences in the number of COVID-19 cases per 100,000 inhabitants [European Centre for Disease Prevention and Control (ECDC), 2021], the number of COVID-19 deaths per 100,000 inhabitants [European Centre for Disease Prevention and Control (ECDC), 2021], and GDP per capita data (World Bank, 2021) between “Yes”/“Partly”/“No”/“Do not know” response groups per each question of the survey were assessed using Kruskal-Wallis test. A significant Kruskal-Wallis test was followed up by Wilcoxon’s test to calculate pairwise comparisons between response levels with corrections for multiple testing. Poisson generalized linear models with log link using robust standard errors were used to assess the association of the number of teleconsultation approaches (“Yes” and “Partly” response groups were pooled) with the number of COVID-19 cases per 100,000 inhabitants [European Centre for Disease Prevention and Control (ECDC), 2021], the number of COVID-19 deaths per 100,000 inhabitants [European Centre for Disease Prevention and Control (ECDC), 2021], and GDP per capita data (World Bank, 2021). The same analysis was performed for the number of methods for requesting prescriptions for chronic medications (“Yes” and “Partly” response groups were pooled). In all analyses, p values of <0.05 were considered statistically significant. Data management and all statistical analyses were performed using R software (The R Foundation for Statistical Computing, Vienna, Austria; version 4.0.2). The raw data supporting the conclusions of this article will be made available by the authors on request, without undue reservation, to any qualified researcher.
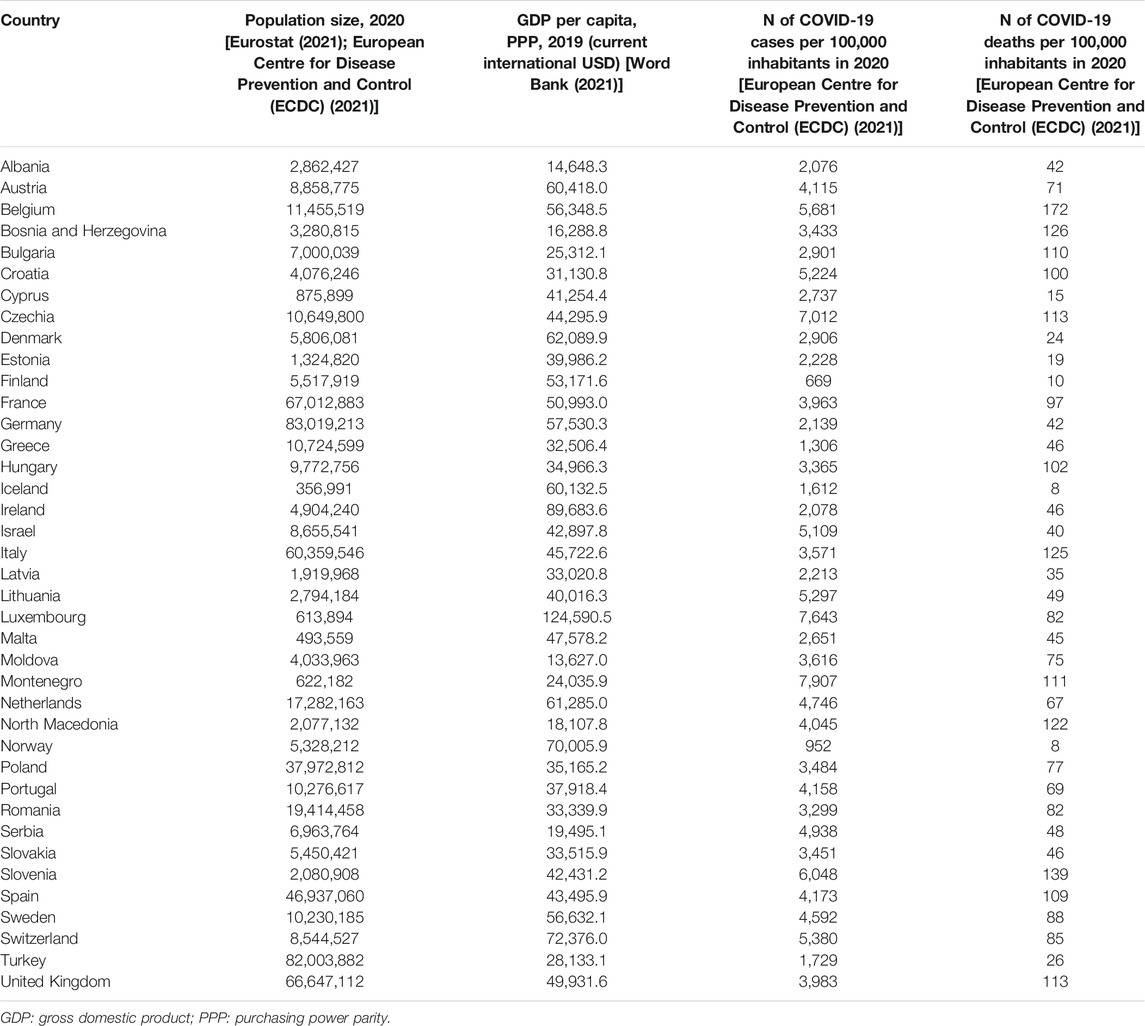
TABLE 1. Country specific population size, GDP per capita and COVID-19 burden data.
Results
A total of 53 (58%) of the 92 ENABLE collaborators from 39 countries (12 countries with more than one respondents) completed the survey. Two-thirds (n = 39) of participants’ professional background was academia (i.e., medical or pharmaceutical sciences) and half of respondents (n = 26) had more than 20 years of work experience.
Our results are reported according to the seven key domains of the medication management cycle of NCDs (Figure 1). Country-specific responses for each item of the survey questionnaire and the detailed results of the statistical analysis can be found in Supplementary Figures S2–S9 and Supplementary Tables S1–S7, respectively.
Patient and Healthcare System Regulations
All the included countries have public healthcare systems available to all citizens. Consultations in primary healthcare and other ambulatory care are fully or partially covered in all the countries. In 10 (26%) countries there were restrictions in number of consultations without fee in primary care for patients with NCDs. In these countries the mean number of COVID-19 cases per 100,000 inhabitants was significantly lower compared to countries with unlimited free primary care consultations (p = 0.017) (Table 2).
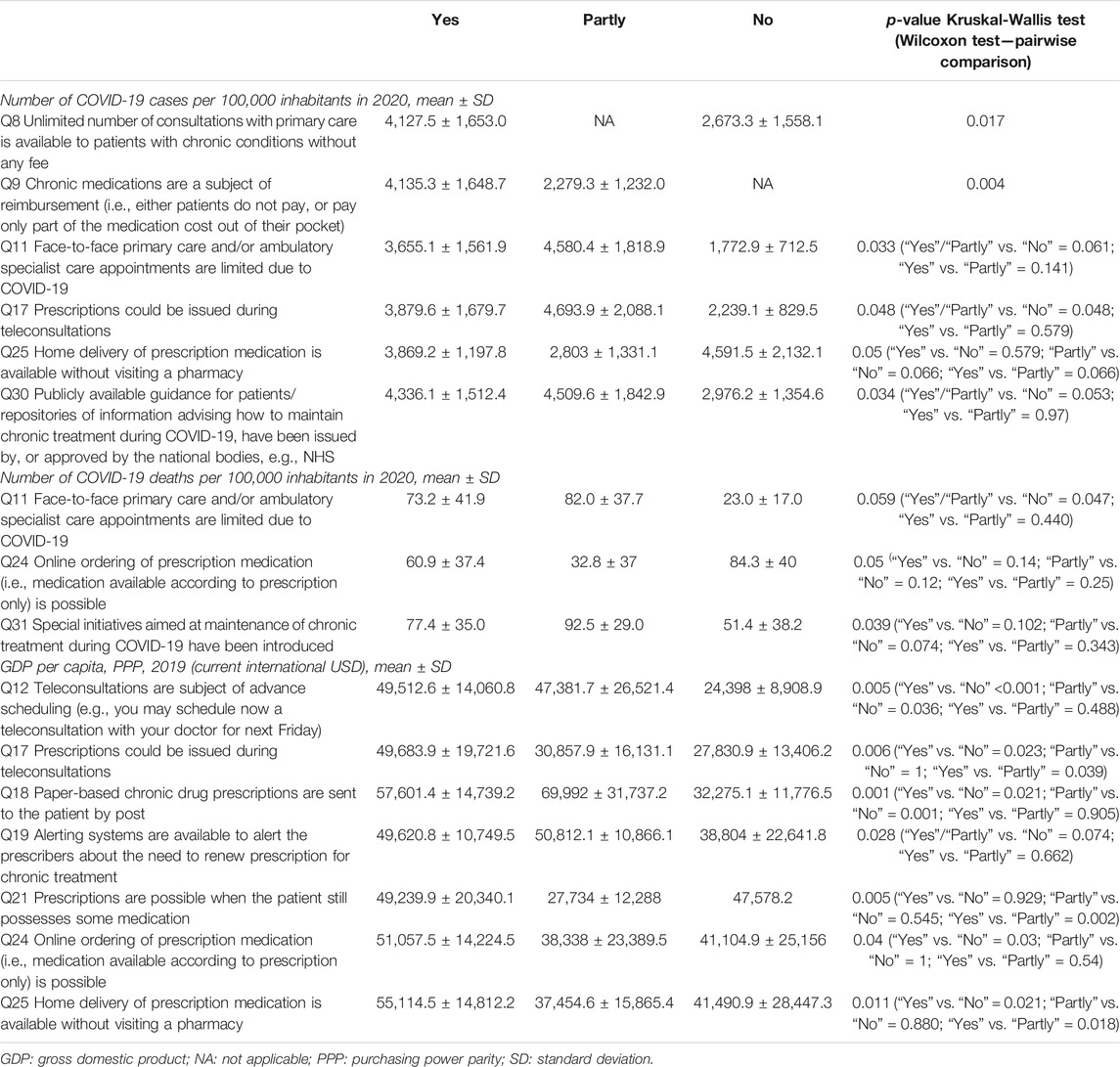
TABLE 2. Significant results of the statistical analysis on the association between the number of COVID-19 cases and deaths per 100,000 inhabitants and GDP per capita and the evaluated items of the medication management of NCDs.
In all countries the cost of chronic medications were fully (80%) or partly (20%) reimbursed. The mean number of COVID-19 cases per 100,000 inhabitants was significantly higher in countries with more extensive reimbursement for chronic pharmacotherapies (“Yes” response group vs. “Partly” response group p = 0.004) (Table 2). Electronic prescribing was available in 36 (92%) countries, and it was not found to be associated with the number of COVID-19 cases and COVID-19 deaths. Furthermore, none of the evaluated items of the patient and healthcare system regulations domain showed a significant association with GDP per capita of countries.
Means of Communication Between the Patient and Prescriber
In 35 (90%) of countries, face-to-face primary care and/or out-patient care consultations were, at least partly, limited due to the COVID-19 pandemic. The number of COVID-19 deaths per 100,000 inhabitants showed an association with the disruption of outpatient care (“Yes” response group/“Partly” response group vs. “No” response group p = 0.047) (Table 2). The same trend was seen in case of the number of COVID-19 cases between response groups (p = 0.033); however, in pairwise comparison this association was not significant anymore (Table 2).
Being able to book an advance appointment for a teleconsultation was available in 33 (85%) countries and was significantly more common in countries with higher GDP per capita (“Yes” response group vs. “No” response group p < 0.001, “Partly” response group vs. “No” response group p = 0.036) (Table 2). Across the evaluated countries the mean ± SD number of available teleconsultation services (e.g., e-mail, online chat, phone, video, and electronic health records) in the public healthcare system was 3 ± 1.3 (Figure 2A) and it was positively associated with GDP per capita of countries (p = 0.05). Furthermore, the mean ± SD number of teleconsultation methods for requesting prescriptions for chronic medications was 3.4 ± 1.6 (Figure 2B), but it did not show an association with any of the evaluated covariates.
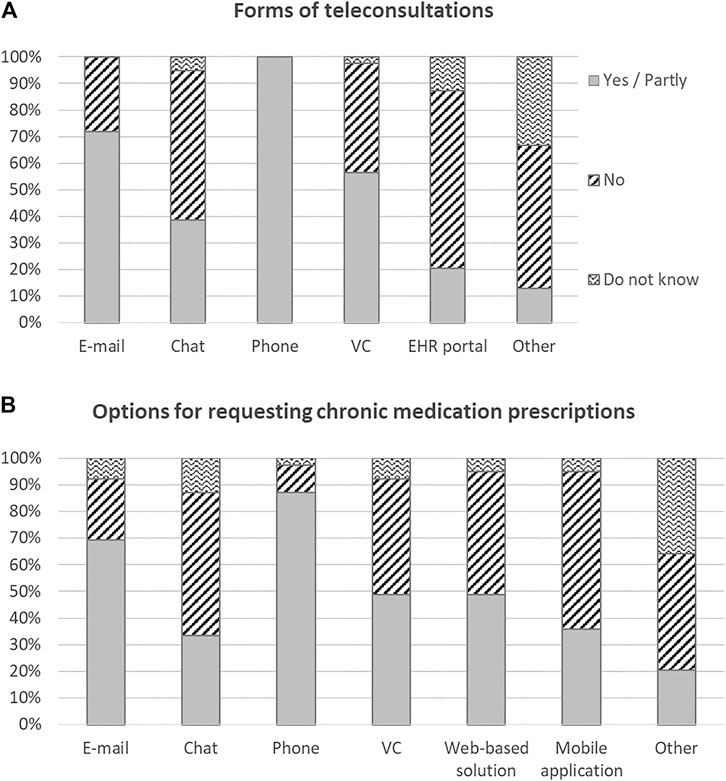
FIGURE 2. Availability of various forms of teleconsultations (A), and options for requesting chronic medication prescriptions (B) across 39 European countries, as per December 2020. VC: videoconsultation; EHR: electronic health record.
Prescriber
Access to prescribing history and/or dispensing (e.g., within electronic health record) was, at least partly, available in 33 (85%) countries and only physicians were authorized to prescribe medications in 22 (56%) countries. These items were not associated with the number of COVID-19 cases, the number of COVID-19 deaths, or country income.
Prescriptions could be issued during teleconsultations in 32 (82%) countries, significantly more common in countries with higher GDP per capita (p = 0.006) and in countries with higher number of COVID-19 cases (p = 0.048) (Table 2). Paper-based repeated drug prescriptions could be sent to the patient by post only in 9 (23%) countries. The availability of this service was associated with higher GPD per capita (“Yes” response group vs. “No” response group p = 0.021, “Partly” response group vs. “No” response group p = 0.001) (Table 2).
Systems to alert the prescribers about the need to renew prescription for chronic treatment were, at least partly, available only in 11 (28%) countries and it was found to be related to country income when comparing all response groups (p = 0.028) (Table 2). However, using pairwise comparison the association was not significant anymore.
Prescription
To prescribe chronic medications for a more than a 3-months period and when the patient still has a stock of medication was possible in 26 (67%) and 37 (95%) countries, respectively. Prescribing of specialist medicines (e.g., high-cost medicines normally prescribed by specialists only) in primary care during COVID-19 pandemic was, at least partly, allowed in 12 (31%) countries. Regarding the item of medication prescription when the patient still possesses some medication, the GDP per capita of countries in the “Yes” response group was significantly higher compared to countries in the “Partly” response group (p = 0.002) (Table 2). No further association was found between the items of this domain and the evaluated covariates.
Community Pharmacy Regulation
In 26 (67%) countries medication for NCDs could not be dispensed without a prescription. Online ordering and home delivery of prescription medication without visiting a pharmacy was, at least partly, available in 18 (46%) and 26 (67%) countries, respectively. Both items showed a positive association with GDP per capita (online ordering: “Yes” response group vs. “No” response group p = 0.03; home delivery of prescription medication: “Yes” response group vs. “No” response group p = 0.021). We also found weak associations between online ordering and the number of COVID-19 deaths per 100,000 inhabitants and between home delivery of prescription medication and the number of COVID-19 cases per 100,000 inhabitants when comparing all response groups; however, none of these associations remained significant in case of pairwise comparisons (Table 2).
Substitution of unavailable medication was, at least partly, allowed in 33 (85%) countries and dispensing of specialist medicines (e.g., high-cost medicines normally dispensed by hospitals) by community pharmacies during COVID-19 pandemic was made, at least partly, possible only in 8 (21%) countries. These items were not associated with the number of COVID-19 cases, the number of COVID-19 deaths or country income.
Medication
In 35 (90%) countries no reduction of out-of-pocket costs of medication for NCDs was applied during the COVID-19 pandemic and only 21 (54%) countries applied measures specifically to address potential shortages of medicines. No significant association was found between the items of this domain and the evaluated covariates.
Medication Taking
A national policy or specific guidance on ensuring on-going access to medication for NCDs during the COVID-19 pandemic was issued in 20 (51%) countries. In case of this variable, differences in the number of COVID-19 cases per 100,000 inhabitants between response groups were found to be significant with Kruskal-Wallis test (p = 0.034); however, in the pairwise comparison it was not significant anymore (Table 2).
Special initiatives for maintaining chronic pharmacotherapies were introduced in 20 (51%) countries, which was weakly associated with the number of COVID-19 deaths (p = 0.039), but this association did not remain significant in case of pairwise comparison (Table 2).
Discussion
Our study offers a comprehensive “snapshot” of how different European countries responded to the challenge of assuring medication management services for NCDs during the second wave of the COVID-19 pandemic. In only half of European countries were our respondents aware of any national guidelines regarding strategies for maintaining medication availability for people with NCDs, or advice for patients on how to ensure access to medication and adherence during the pandemic. Apart from a widespread switch to remote consulting, the use of e-health solutions was variable. Electronic prescriptions were available in 92% of countries, whereas online ordering and home delivery of prescription medication were only available 46 and 67% of countries, respectively.
In line with the results of the WHO survey [World Health Organization (WHO), 2020b], and a global survey of healthcare professionals (Chudasama et al., 2020), our findings highlight that the COVID-19 pandemic limited the number of face-to-face appointments for NCDs in primary care, and out-patients. Medication management of NCDs during the COVID-19 pandemic varied between countries, which was partly explained by the differences in the structure and financing of healthcare systems across Europe. In general, greater disruption in healthcare and accelerated the uptake of e-health services was associated with greater burden of COVID-19 (Table 2). However, typically various e-health solutions were not merged into a seamless system and there may have been substantial variations even within countries. For example, in more than 80% of countries, prescriptions for NCDs could be issued without a face-to-face consultation; but home delivery of prescription medications was not available in 13 countries. In these countries, despite the availability of telemedicine services and electronic prescription, patients with NCDs could still not get their medications without leaving home. Especially in the more vulnerable patients who were shielding, it would be important to reduce the number of unnecessary personal contacts in order to reduce risk.
The COVID-19 pandemic promoted the use of e-health technologies as social distancing prevented traditional face-to-face patient-physician appointments. The available forms of teleconsultations, and options for requesting medication prescriptions were different across the evaluated countries (Figure 2). In the majority of countries, phone and e-mail were the most commonly used modes of digital communication between patients and physicians. However, in countries with higher GDP per capita, a wider range of teleconsultation (e.g., online chat, video-consultations, communication via the electronic health record portal) and e-health services (e.g., alerts when prescriptions need to be renewed, online ordering of prescription medication) were available for the management of patients with NCDs (Table 2). These results highlight the potential of innovative models of care to meet the challenges of the pandemic (Gunasekeran et al., 2021). An example of such a solution could be an alerting system for prescribers about the need to renew prescriptions for chronic treatment, reported in 11 countries. However, even simple solutions are worth introducing, in order to make the NCD patient journey easier, such as the possibility of advance scheduling of teleconsultations (missing in six countries).
Evidence suggests that the out-of-pocket cost of drugs is a significant determinant of medication adherence (Dodd et al., 2018) and a few countries reduced medication costs to offset the economic disruption of the COVID-19 pandemic. Inability to afford drugs increases the risk of non-adherence and non-persistence to chronic treatments. Allowing longer-duration prescriptions could facilitate access to drug supplies especially for patients living in remote areas, though this needs to be balanced against the risk of supply problems with “stockpiling” during the COVID-19 lockdown. Substituting unavailable medicines by a pharmacist could be a practical solution to medicine shortages. The medication supply chain is being strained by the pandemic (Shuman et al., 2020); nevertheless, only 54% of countries reported measures specifically to address potential shortages of medicines. In addition policy interventions to improve drug coverage and behavioral support consisting in patient education can improve medication adherence among people with chronic diseases (Viswanathan et al., 2012).
The reduction in the number of face-to-face appointments, and the lack or low number of interventions assuring continuous treatment of NCDs (e.g., the absence of systems to alert prescribers about the need to renew prescriptions) during the pandemic may have significant clinical consequences. This also makes economic sense as medication non-adherence leads to higher health care use and costs despite decreased drug spending (Roebuck et al., 2011). Nevertheless, half of our respondents were unaware of any national guidelines for preserving medication supplies NCDs or for patients on how to access medication and maintain adherence during the COVID-19 pandemic. These findings suggest that there is room for a system-based approach to ensure the maintenance of treatments for NCDs during crizes (such as pandemics) to minimize the consequences on long-term condition care. A European Union vision of resilient healthcare following the COVID-19 pandemic includes strengthening primary care and mental healthcare [Expert Panel on effective ways of investing in health (EXPH), 2020], bringing some hope that this ambition will become a reality. Further studies are warranted to improve understanding of the long-term clinical and economic consequences of the disruption to NCD services during the COVID-19 pandemic.
Our survey highlights major disparities in the way different European countries are dealing with the challenge of managing NCDs during the COVID-19 pandemic, and suggests strategies for improvement. Several practical and low-cost solutions (Figure 1) could be applied, as suggested in our quick commentary (Kardas et al., 2021), including: 1) an increased range of remote services for ordering repeat prescriptions (e.g., online, via mobile app), 2) expanding the scope of professionals authorized to prescribe (or issue repeat prescriptions), 3) increasing the duration of prescriptions (though this needs to be balanced with managing shortages), 4) enabling community pharmacies to dispense medications normally restricted to hospitals, 5) allowing substitution of unavailable drugs, 6) creating e-health systems supporting patients in long-term treatment, encouraging patient empowerment and patient-centred care, and 7) providing publicly available guidance on strategies for maintaining treatment during pandemic lockdown. Our findings point to interventions worth taking during COVID-19 pandemic in order to maintain NCDs treatment. It might be hypothesized; however, that these activities are also important beyond the current pandemic, as healthcare systems adapt to an aging population with increasing multimorbidity [Chatterji et al., 2015; World Health Organization (WHO), 2018b].
Our results should be considered in light of the following limitations. The self-developed questionnaire and multiple-choice questions with closed answers allowed us to seek very specific information; however, it may be biased by the authors’ preconceived perceptions. To minimize this risk, external experts were asked to assess the questionnaire with respect to the content, construct and criterion validity. The survey was completed by members of ENABLE who were asked to provide information on the current practices in their own countries rather than regional, local or their own perspective. In 12 countries we had more than one respondent; however, in some countries information was based on the answers of one respondent, which might lead to bias. The majority of participants were working at the academic sector of medical or pharmaceutical sciences with more than 20 years of work experience, and their views represents one perspective while there may be substantial differences in primary healthcare and medicines even between regions within a country. It should also be noted that the regulations and reimbursement of primary care and pharmacy practice are changing over time, and especially digital solutions were rapidly introduced in healthcare in many countries already before the COVID-19 outbreak. Consequently, this survey represents the situation at a single point of time and the replies for some questions may have differed substantially if the survey had been distributed at another time point.
To conclude, our survey has identified marked disparities in ensuring medication management services for NCDs across Europe. This points to the need for a paradigm shift in NCD-related healthcare services to assure access and enable adherence to chronic pharmacotherapies during the current pandemic (and future disasters). E-health solutions cannot solve all the challenges of NCD care (e.g., some therapies need regular blood tests) and safe arrangements will be needed. In the short-term, we must optimize the health of NCD patients at risk of poor outcomes from COVID-19. In the long-term, maintaining access to NCD treatments could limit the negative consequences of disruptive health service events.
ENABLE Collaborators Participating in the Study Were
Darinka Gjorgieva Ackova, Tamás Ágh, Adriana Baban, Martina Bago, Juris Barzdins, Noemi Bitterman, Gregor Bond, Job FM van Boven, Yasemin Çayır, Ioanna Chouvarda, Maria Cordina, Alexandru Corlateanu, Jaime Correia de Sousa, Petra Denig, Dragana Drakul, Natasa Duborija-Kovacevic, Çi̇ğdem GamzeÖzkan, Cristina Ghiciuc, Catherine Goetzinger, Anne Gerd Granas, Joao Gregorio, Jolanta Gulbinovic, Maja Ortner Hadžiabdić, Freyja Jónsdóttir, Przemyslaw Kardas, Maria Kamusheva, Elena Kkolou, Mitja Kos, Ott Laius, Fedor Lehocki, Francisca Leiva, Urska Nabergoj Makovec, Katerina Mala-Ladova, Enrica Menditto, Vildan Mevsim, Jovan Mihajlovic, Valentina Orlando, Christos Petrou, Guenka Petrova, Hilary Pinnock, Mitar Popović, Richard Reilly, Susanne Reventlow, Marie Schneider, Ivana Tadic, Ugo Trama, Indre Treciokiene, Ioanna Tsiligianni, Esra Uslu, Eric van Ganse, Jiří Vlček, Daisy Volmer, Vesna Vujic-Aleksic, Björn Wettermark.
Data Availability Statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Author Contributions
PK, TÁ, JB, BW, EM, HP, IT, GP, IP, and FK contributed to conception and design of the study. PK, TÁ, JB, BW, EM, HP and IT developed the first draft of the survey questionnaire. TÁ and PK aggregated responses to the survey and organized the database. TÁ performed the statistical analysis. TÁ and PK wrote the first draft of the manuscript. JB, BW, EM, HP, IT, GP, IP, and FK wrote sections of the manuscript. All authors contributed to manuscript revision, read, and approved the submitted version.
Funding
This article is based upon work from COST Action CA19132 “ENABLE,” supported by COST (European Cooperation in Science and Technology). The funder had no role in the study design, data analysis, interpretation, preparation, or writing of the manuscript.
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Acknowledgments
Authors would like to express their thanks to external experts in adherence research who participated in the process of the survey questionnaire validation: Caitriona Cahir, Filipa Alves da Costa, Giuseppe Limongelli, Elizabeth Manias, Andrew M. Peterson, Ulrika Winblad, Leah Zullig.
Supplementary Material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fphar.2021.685696/full#supplementary-material
References
Böhm, M., Schumacher, H., Laufs, U., Sleight, P., Schmieder, R., Unger, T., et al. (2013). Effects of Nonpersistence with Medication on Outcomes in High-Risk Patients with Cardiovascular Disease. Am. Heart J. 166 (2), 306–314. doi:10.1016/j.ahj.2013.04.016
CDC COVID-19 Response Team (2020). Preliminary Estimates of the Prevalence of Selected Underlying Health Conditions Among Patients with Coronavirus Disease 2019 - United States, February 12-March 28, 2020. MMWR Morb Mortal Wkly Rep. 69 (13), 382–386. doi:10.15585/mmwr.mm6913e2
Chatterji, S., Byles, J., Cutler, D., Seeman, T., and Verdes, E. (2015). Health, Functioning, and Disability in Older Adults-Present Status and Future Implications. The Lancet 385 (9967), 563–575. doi:10.1016/S0140-6736(14)61462-8
Chowdhury, R., Khan, H., Heydon, E., Shroufi, A., Fahimi, S., Moore, C., et al. (2013). Adherence to Cardiovascular Therapy: a Meta-Analysis of Prevalence and Clinical Consequences. Eur. Heart J. 34 (38), 2940–2948. doi:10.1093/eurheartj/eht295
Chudasama, Y. V., Gillies, C. L., Zaccardi, F., Coles, B., Davies, M. J., Seidu, S., et al. (2020). Impact of COVID-19 on Routine Care for Chronic Diseases: A Global Survey of Views from Healthcare Professionals. Diabetes Metab. Syndr. Clin. Res. Rev. 14 (5), 965–967. doi:10.1016/j.dsx.2020.06.042
Clark, A., Jit, M., Warren-Gash, C., Guthrie, B., Wang, H. H. X., Mercer, S. W., et al. (2020). Global, Regional, and National Estimates of the Population at Increased Risk of Severe COVID-19 Due to Underlying Health Conditions in 2020: a Modelling Study. Lancet Glob. Health 8 (8), e1003–1017. doi:10.1016/S2214-109X(20)30264-3
Daniels, L. B., Sitapati, A. M., Zhang, J., Zou, J., Bui, Q. M., Ren, J., et al. (2020). Relation of Statin Use Prior to Admission to Severity and Recovery Among COVID-19 Inpatients. Am. J. Cardiol. 136, 149–155. doi:10.1016/j.amjcard.2020.09.012
Dodd, R., Palagyi, A., Guild, L., Jha, V., and Jan, S. (2018). The Impact of Out-Of-Pocket Costs on Treatment Commencement and Adherence in Chronic Kidney Disease: a Systematic Review. Health Policy Plan 33 (9), 1047–1054. doi:10.1093/heapol/czy081
European Centre for Disease Prevention and Control (ECDC) (2021). Situation Updates on COVID-19. Available at: https://www.ecdc.europa.eu/en/covid-19/situation-updates (Accessed March 7, 2021).
Eurostat (2021). Population Projections. Available at: https://ec.europa.eu/eurostat (Accessed January 07, 2021).
Expert Panel on effective ways of investing in health (EXPH) (2020). The Organisation of Resilient Health and Social Care Following the COVID-19 Pandemic. Luxembourg: Publications Office of the European Union.
Eysenbach, G. (2004). Improving the Quality of Web Surveys: The Checklist for Reporting Results of Internet E-Surveys (CHERRIES). J. Med. Internet Res. 6 (3), e34. doi:10.2196/jmir.6.3.e34
Font, R., Espinas, J. A., Barnadas, A., Izquierdo, A., Galceran, J., Saladie, F., et al. (2019). Influence of Adherence to Adjuvant Endocrine Therapy on Disease-free and Overall Survival: a Population-Based Study in Catalonia, Spain. Breast Cancer Res. Treat. 175 (3), 733–740. doi:10.1007/s10549-019-05201-3
Gunasekeran, D. V., Tham, Y.-C., Ting, D. S. W., Tan, G. S. W., and Wong, T. Y. (2021). Digital Health during COVID-19: Lessons from Operationalising New Models of Care in Ophthalmology. The Lancet Digital Health 3 (2), e124–e134. doi:10.1016/S2589-7500(20)30287-9
Institute for Health Metrics and Evaluation (IHME) (2020). GBD Results Tool. Available at: http://ghdx.healthdata.org/gbd-results-tool (Accessed February 3, 2021).
Kardas, P., van Boven, J. F. M., Pinnock, H., Menditto, E., Wettermark, B., Tsiligianni, I., et al. (2021). Disparities in European Healthcare System Approaches to Maintaining Continuity of Medication for Non-communicable Diseases during the COVID-19 Outbreak. The Lancet Reg. Health Europe 4, 100099. doi:10.1016/j.lanepe.2021.100099
Kluge, H. H. P., Wickramasinghe, K., Rippin, H. L., Mendes, R., Peters, D. H., Kontsevaya, A., et al. (2020). Prevention and Control of Non-communicable Diseases in the COVID-19 Response. The Lancet 395 (10238), 1678–1680. doi:10.1016/S0140-6736(20)31067-9
Lee, Y., Park, Y. R., Lee, J. S., Lee, S. B., Chung, I. Y., Son, B. H., et al. (2019). Prescription Refill gap of Endocrine Treatment from Electronic Medical Records as a Prognostic Factor in Breast Cancer Patients. J. Breast Cancer 22 (1), 86–95. doi:10.4048/jbc.2019.22.e14
Minghui, R., Simao, M., Mikkelsen, B., Kestel, D., Ball, A., and Szilagyi, Z. (2020). Gaps in Access to Essential Medicines and Health Products for Noncommunicable Diseases and Mental Health Conditions. Bull. World Health Organ. 98, 582–582A. doi:10.2471/BLT.20.272658
Noor, F. M., and Islam, M. M. (2020). Prevalence and Associated Risk Factors of Mortality Among COVID-19 Patients: A Meta-Analysis. J. Community Health 45 (6), 1270–1282. doi:10.1007/s10900-020-00920-x
Palmer, K., Monaco, A., Kivipelto, M., Onder, G., Maggi, S., Michel, J.-P., et al. (2020). The Potential Long-Term Impact of the COVID-19 Outbreak on Patients with Non-communicable Diseases in Europe: Consequences for Healthy Ageing. Aging Clin. Exp. Res. 32 (7), 1189–1194. doi:10.1007/s40520-020-01601-4
Papachristou, S., Stamatiou, I., Stoian, A. P., and Papanas, N. (2020). New-onset Diabetes in COVID-19: Time to Frame its Fearful Symmetry. Diabetes Ther. 12 (2), 461–464. doi:10.1007/s13300-020-00988-7
Roebuck, M. C., Liberman, J. N., Gemmill-Toyama, M., and Brennan, T. A. (2011). Medication Adherence Leads to Lower Health Care Use and Costs Despite Increased Drug Spending. Health Aff. 30 (1), 91–99. doi:10.1377/hlthaff.2009.1087
Sheldon, T. A., and Wright, J. (2020). Twin Epidemics of Covid-19 and Non-communicable Disease. BMJ 369, m2618. doi:10.1136/bmj.m2618
Shuman, A. G., Fox, E. R., and Unguru, Y. (2020). COVID-19 and Drug Shortages: a Call to Action. J. Manag. Care Spec. Pharm. 26 (8), 945–947. doi:10.18553/jmcp.2020.26.8.945
Viswanathan, M., Golin, C. E., Jones, C. D., Ashok, M., Blalock, S. J., Wines, R. C. M., et al. (2012). Interventions to Improve Adherence to Self-Administered Medications for Chronic Diseases in the United States. Ann. Intern. Med. 157 (11), 785–795. doi:10.7326/0003-4819-157-11-201212040-00538
World Bank (2021). GDP Per Capita at PPP in Current International USD. Available at: https://data.worldbank.org (Accessed January 07, 2021).
World Health Organization (WHO) (2003). Adherence to Long-Term Therapies: Evidence for Action. Geneva: World Health Organization.
World Health Organization (WHO) (2018a). Global Health Estimates 2016: Deaths by Cause, Age, Sex, by Country and by Region, 2000–2016. Geneva: World Health Organization.
World Health Organization (WHO) (2018b). Noncommunicable Diseases Country Profiles 2018. Geneva: World Health Organization.
World Health Organization (WHO) (2020b). The Impact of the COVID-19 Pandemic on Noncommunicable Disease Resources and Services: Results of a Rapid Assessment. Geneva: World Health Organization.
World Health Organization (WHO) (2020a). WHO Director-General's Opening Remarks at the media Briefing on COVID-19 - 11 March 2020. Available at: https://www.who.int/director-general/speeches/detail/who-director-general-s-opening-remarks-at-the-media-briefing-on-covid-19---11-march-2020 (Accessed February 3, 2021).
Keywords: noncommunicable diseases, drug therapy, persistence, medication adherence, COVID-19, pandemic, healthcare system, medication management
Citation: Ágh T, van Boven JF, Wettermark B, Menditto E, Pinnock H, Tsiligianni I, Petrova G, Potočnjak I, Kamberi F and Kardas P (2021) A Cross-Sectional Survey on Medication Management Practices for Noncommunicable Diseases in Europe During the Second Wave of the COVID-19 Pandemic. Front. Pharmacol. 12:685696. doi: 10.3389/fphar.2021.685696
Received: 25 March 2021; Accepted: 24 May 2021;
Published: 07 June 2021.
Edited by:
Joseph O. Fadare, Ekiti State University, NigeriaReviewed by:
Mohamed Izham Mohamed Ibrahim, Qatar University, QatarNicolas Widmer, Pharmacie des Hôpitaux de l'Est Lémanique, Switzerland
Copyright © 2021 Ágh, van Boven, Wettermark, Menditto, Pinnock, Tsiligianni, Petrova, Potočnjak, Kamberi and Kardas. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Tamás Ágh, dGFtYXMuYWdoQHN5cmVvbi5ldQ==