 Lucia Gozzo1,2*
Lucia Gozzo1,2* Giovanni Luca Romano2
Giovanni Luca Romano2 Serena Brancati1
Serena Brancati1 Marco Cicciù3
Marco Cicciù3 Luca Fiorillo3
Luca Fiorillo3 Laura Longo1
Laura Longo1 Daniela Cristina Vitale1
Daniela Cristina Vitale1 Filippo Drago1,2,4
Filippo Drago1,2,4- 1Clinical Pharmacology Unit/Regional Pharmacovigilance Centre, University Hospital of Catania, Catania, Italy
- 2Department of Biomedical and Biotechnological Sciences, University of Catania, Catania, Italy
- 3Department of Biomedical and Dental Sciences Morphological and Functional Images, University of Messina, AOU “G. Martino”, Messina, Italy
- 4Centre for Research and Consultancy in HTA and Drug Regulatory Affairs (CERD), University of Catania, Catania, Italy
Even for products centrally approved, each European country is responsible for national market access after European Medicines Agency (EMA) approval. This step can result in inequalities in terms of access, due to different opinions about the therapeutic value assessed by Health Technology Assessment (HTA) bodies. This study aims to provide a comparative analysis of HTA recommendations issued by EU countries (France, Germany, and Italy) for new neurological drugs following EMA approval. In the reference period, we identified 11 innovative medicines authorized in Europe for five neurological diseases (cerebral adrenoleukodystrophy, spinal muscular atrophy, metachromatic leukodystrophy, migraine, and polyneuropathy in patients with hereditary transthyretin amyloidosis), including eight drugs for genetic rare diseases. We found no agreement on the therapeutic value (in particular the “added value” compared to the standard of care) of the selected drugs. Despite the differences in terms of assessment, the access has been usually guaranteed even if with various types of limitations. The heterogeneity of the HTA assessment of clinical data among countries is probably related to the uncertainties about clinical value at the time of EMA approval and the lack of long-term data and of direct comparison with available alternatives. Given the importance of new medicines especially for rare diseases, it is crucial to understand and act on the causes of inconsistency among the HTA assessments, in order to ensure rapid and uniform access to innovation for patients who can benefit.
Introduction
According to recent data, neurology represents one of the therapeutic areas with the greatest number of development projects, perhaps reflecting scientific advances in the understanding of the basis of these diseases useful for potential novel intervention (Pankevich et al., 2014). Neurological conditions historically have been among the most difficult for which to develop effective and safe new therapies, due to the complexity in physiopathology and clinical presentation, and curative treatments for important diseases, such as neurodegenerative diseases, are still lacking (EC, 2020).
Actually, this is one of the most challenging therapeutic field in terms of likelihood of drug approval, with the longest time for review and recommendation (Arneric et al., 2018; Gribkoff and Kaczmarek, 2017; National Academies of Sciences, Engineering, and Medicine, 2016; O'Donnell et al., 2019).
A new drug (and/or an old drug for new indications) requires the authorization from a regulatory authority to be marketed (van Nooten et al., 2012; Gozzo et al., 2020a; Drago et al., 2020; Gozzo et al., 2021a; Toro et al., 2021). Moreover, price and reimbursement procedures need to be performed by competent authorities to find an agreement between companies and payers for market access (Gozzo et al., 2021a).
Today, in accordance with regulation 726/2004, in order to be marketed in the EU, the great majority of new, innovative medicines pass through a centralized procedure, which is compulsory for human medicines containing a new active substance to treat a lot of diseases, including neurodegenerative and rare diseases, for advanced-therapy medicinal products (ATMPs), and medicines derived from biotechnology processes in general (COMMUNITIES TCOTE, 1993; Regulation EC, 2004).
According to this procedure, the company submits a single marketing authorization (MA) dossier to the European Medicines Agency (EMA), and a MA for all the European Economic Area will be granted if the drug’s benefit–risk profile is positive according to the quality non-clinical and clinical data on safety and efficacy submitted by the applicant.
The aim of the centralized procedure is to enable rapid, EU-wide authorization of medicinal products (EMA, 2020a; Gozzo et al., 2020b; Gozzo et al., 2020c).
Despite the successful unification of the European procedures for drug approval, each country is responsible for national market access and pricing and reimbursement agreements, in line with national health needs and resources. This can result in access inequalities among European countries, due to differences not only in terms of willingness to pay but also in the recognition of drug therapeutic value (Ciani and Jommi, 2014; Gozzo et al., 2016; Akehurst et al., 2017; Allen et al., 2017). Indeed, in recent years, MA requests are submitted at earlier stages of development, especially for high-unmet medical need and/or rare diseases, before conclusive data are available, thus potentially leading to reduced quality of evidence and to uncertainty in terms of therapeutic value (Akehurst et al., 2017; Richardson and Schlander, 2019; Jommi et al., 2020; Brancati et al., 2021a; Brancati et al., 2021b).
The big challenge for policy makers is ensuring equitable access to medicines, balancing a timely patient access with the health system sustainability, in the era of precision medicines and advanced high-cost therapies (Drummond et al., 2008). The selection of medicines to be reimbursed is usually made by national Health Technology Assessment (HTA) bodies, based on cost-effectiveness, added value, and therapeutic need in the context of local standard of care (van Nooten et al., 2012; Angelis et al., 2018; Gozzo et al., 2021b).
In 2020, the EMA issued 78 positive opinions for new active substances (NASs), including eight medicines recommended for approval in the therapeutic area of neurology (10%) (EMA, 2020a).
This study aims to provide a review of the current evidence about innovative drugs for neurological diseases approved by the EMA in recent years and to perform a comparative analysis of HTA recommendations issued by EU countries for national pricing and reimbursement decisions.
Methods
The study included the following steps:
1) Identification of new therapies with neurological indications approved in Europe between January 2011 and July 2021 listed on the registry published on the official EMA website (EMA, 2021a); we selected medicines of interest based on the Anatomical Therapeutic Chemical Classification (ATC) code N (NERVOUS SYSTEM, excluding drugs with exclusive psychiatric indication—ICD-10-CM Codes F01-F99) and M09 (OTHER DRUGS FOR DISORDERS OF THE MUSCULO-SKELETAL SYSTEM, to include drugs for neuromuscular disorders); generics and biosimilars were excluded, as well as those not representing a potential disease-modifying therapy (e.g., me-too drugs, namely, drugs structurally related to a first-in-class compound, belonging to the same therapeutic class, and used for the same therapeutic purposes);
2) Identification of the HTA assessments of drugs currently approved in Europe by the EMA performed by EU national authorities (France, Germany, and Italy); selection of countries was based on the availability of assessments for public consultation and on the clear definition of therapeutic values through comparable rating scales;
3) Comparative analysis of national opinions; available HTA reports and official administrative act of the three EU countries have been analyzed to compare the assessments.
Medicines centrally approved by the EMA have been identified by consulting the agency’s official documents and classified by type (e.g., gene therapy, small molecule, and monoclonal antibody), according to the orphan drug designation, and by type of authorization issued by the EMA (full, conditional, and for exceptional circumstances).
For each medicine, pivotal clinical trials were reviewed, analyzing the study design, the number of patients enrolled, the primary and secondary outcomes, and the main study results.
The level of clinical benefit (Service Médical Rendu—SMR) and the added therapeutic value compared to the available therapeutic alternatives (Amélioration du Service Médical Rendu—ASMR) was extracted from the official HTA documentation resulting from the assessment of the Transparency Committee (TC) of the French National Authority (Haute Autorité de santé—HAS) (SantèH-HAd, 2013; SantèH-HAd, 2014).
As regards Germany, we consulted the reports of the competent national bodies (Federal Joint Committee or Gemeinsamer Bundesausschuss, G-BA, and Institute for Quality and Efficiency in Health Care, IQWIG) containing a complete HTA on the additional therapeutic benefit of the product compared to recognized standard therapies (BundesausschussG-BG, 2010).
Finally, we identified the therapeutic need, the added therapeutic value, and the quality of the evidence from the Innovation Assessment Reports published by the Italian Medicines Agency (AIFA) (AIFADETERMINA DELL’AGENZIA ITALIANA DEL FARMACO, 2017). A direct comparison among national opinions was possible in terms of “added therapeutic value,” a measure included in all the available assessments (Supplementary Figure S1).
Results
In the reference period, we identified 11 innovative medicines authorized in Europe (three gene therapies, two small molecules, three monoclonal antibodies, two antisense oligonucleotides, and one small interfering ribonucleic acid) for five for neurological diseases (cerebral adrenoleukodystrophy, spinal muscular atrophy, metachromatic leukodystrophy, migraine, and polyneuropathy in patients with hereditary transthyretin amyloidosis; Supplementary Table S1 and Table 1). Eight out of 11 medicines received orphan designation, all for genetic rare diseases. Only ATMP Zolgensma® received a conditional approval, whereas Vindaqel® was the only one approved under exceptional circumstances (Table 1).
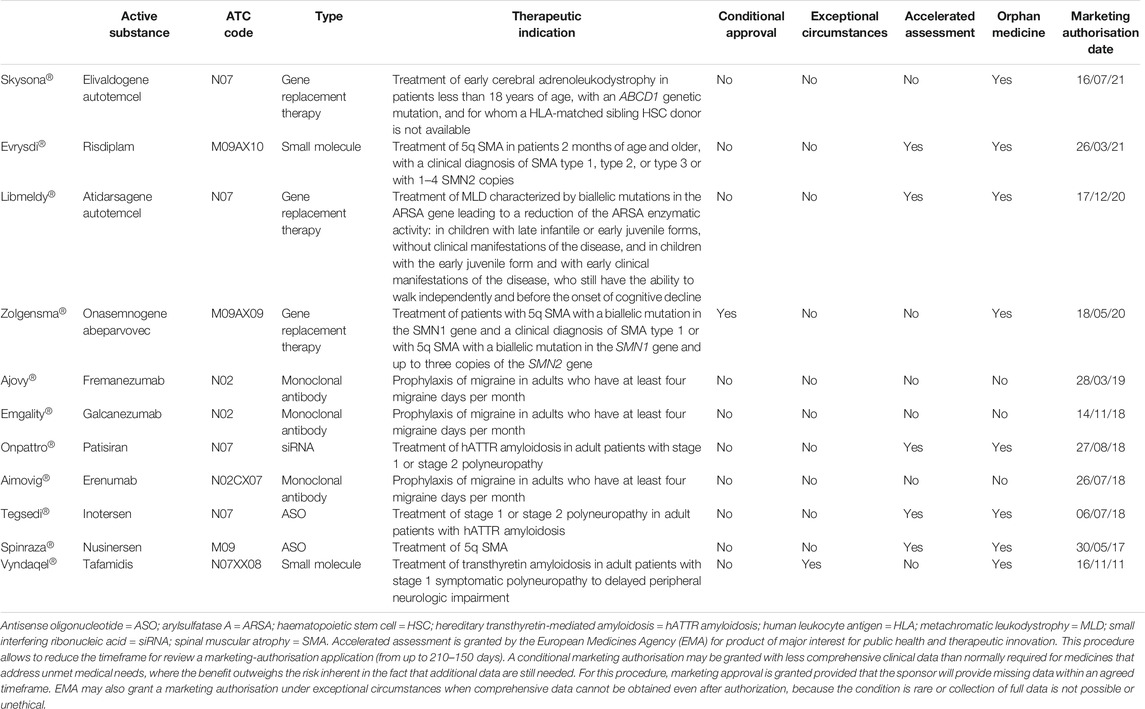
TABLE 1. Innovative drugs with neurological indication approved in Europe in the reference period (2011–2021) and approval details.
In general, for all drugs (excluding Evrysdi® and Libmeldy®), data from phase II/III trials are available, almost half randomized, double blind, placebo controlled (Table 2). The median number of patients enrolled in these studies was 118 (range 6–1,949), followed for a median of 14 months (range 0.8–96).
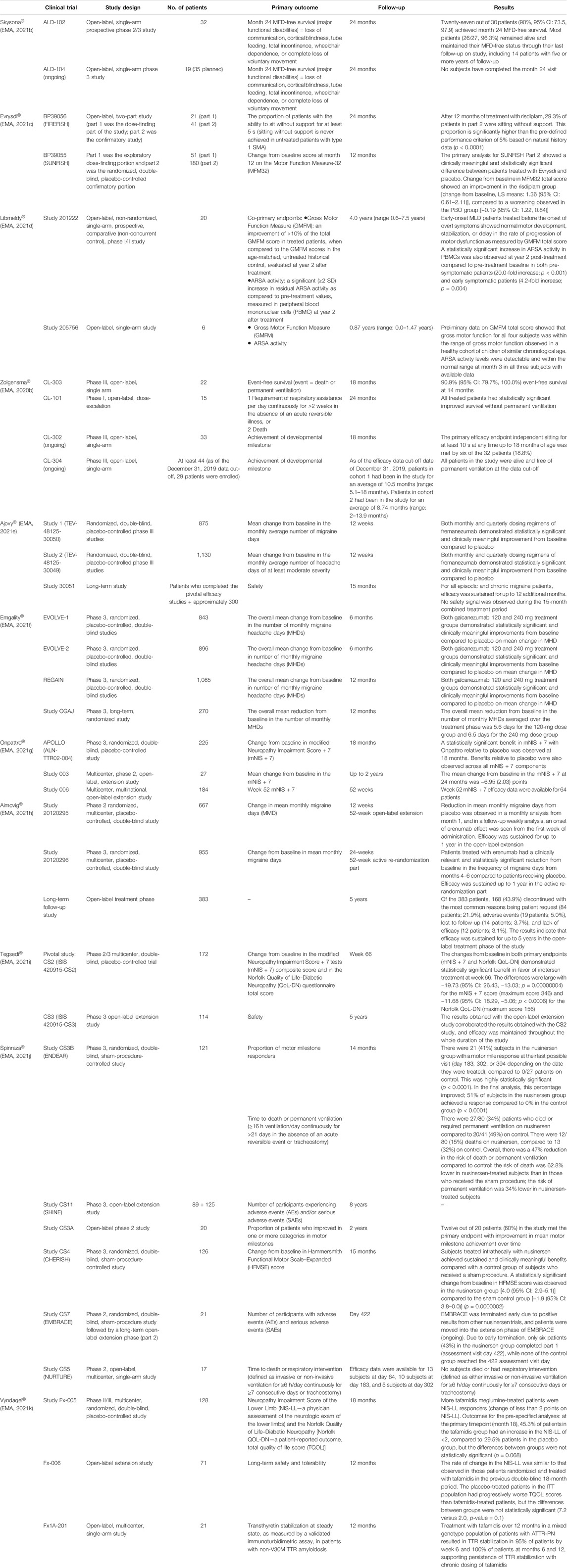
TABLE 2. Data from clinical trials for innovative drugs approved in Europe in the reference period.
Table 3 reports the reimbursement status of the selected drugs. Except for the latest approved by the EMA (Skysona® and Libmeldy®), all drugs are reimbursed in the three EU countries.
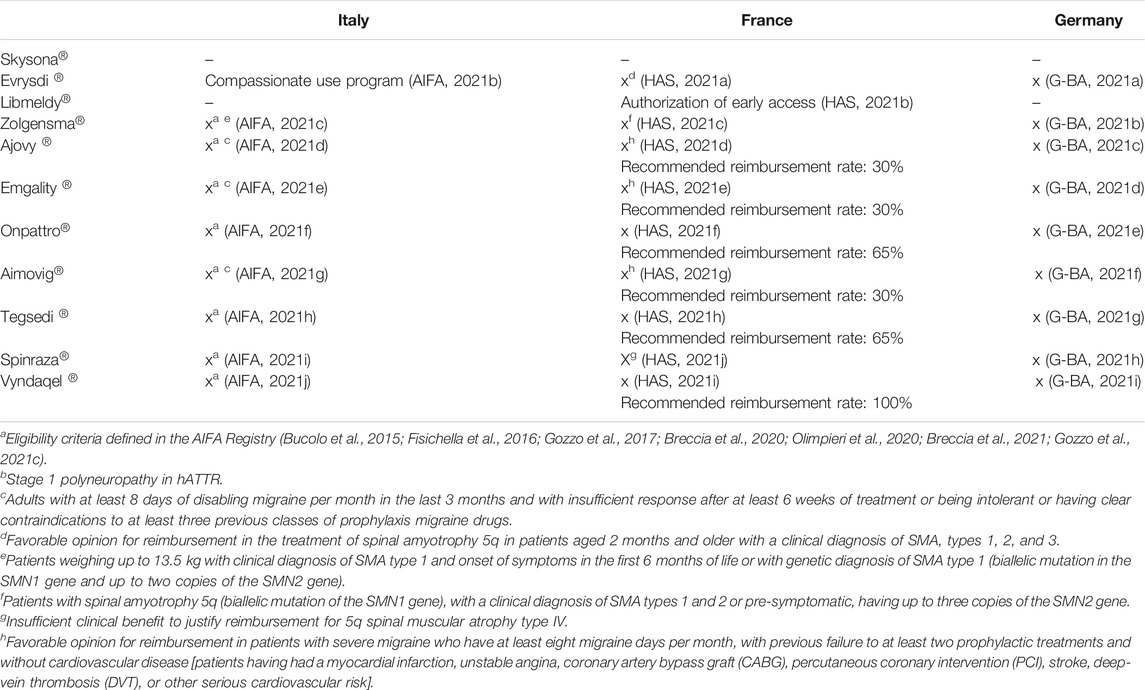
TABLE 3. Reimbursement status in France, Germany, and Italy of neurological drugs approved by the EMA (x = reimbursed; / = not reimbursed or final opinion not available).
Data analysis showed that for 10/11 medicines, at least one public HTA evaluation from at least one of the three selected countries is available, and for six of these products, HTA reports have been published by all the three countries (Table 4). At the time of the analysis, no opinion has been published for Skysona®, the last medicine approved by the EMA. The highest score (important/considerable or major/maximum added value) has been recognized only by Italy (3/11, 27%; Zolgensma®, Onpattro®, and Spinraza®) and Germany (5/11, 45%; antibody for migraine, Onpattro® and Spinraza®).
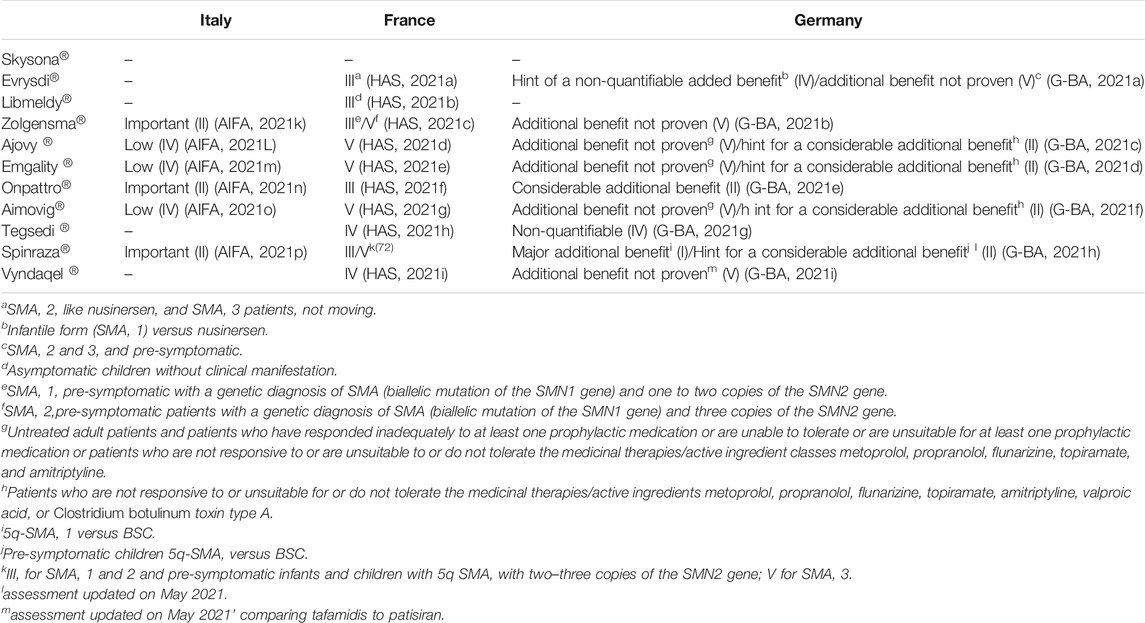
TABLE 4. Agreement among opinions about therapeutic added value issued by member states.
No agreements among the three EU states’ assessments were identified. German assessment was in accordance with the Italian one for Onpattro® and Spinraza®, with the French one for Tegsedi®, and at least in part for Zolgesma® and the three monoclonal antibodies for migraine.
Discussion
In this study, we selected medicines recently approved by the EMA, which represent potential innovative treatment for neurological diseases, including gene therapies for rare genetic unmet medical needs.
Advanced therapies may provide significant health benefits generally with a single administration, allowing to act on the primary cause of a disease with the possibility of complete recovery and improvement of patient outcome potentially over the long term (Gozzo et al., 2021a).
Our results showed a lack of agreement on the therapeutic value (in particular the “added value”) of drugs recently approved for neurological indications in Europe. Despite the differences in terms of assessment, the access has been guaranteed in the three countries even if with various type of limitations.
Overall, the assessments issued by the German authorities were particularly positive, since the added therapeutic value has been classified as “major” or “considerable” in five cases out of 11 (45%), corresponding to five over nine drugs for which the evaluation has been made public (55%). Similarly, the AIFA granted the therapeutic value “important” for three drugs (3/11, 27%; 3/6 drugs for which the assessment has been made public to date, 50%), in particular in the case of treatments for spinal muscular atrophy (SMA) (Zolgensma® and Spinraza®) and of one treatment for hereditary transthyretin-mediated amyloidosis (hATTR) (Onpattro®). The Italian and German assessments were in accordance only for Spinraza® and Onpattro®. No drugs were judged to have a “major” or “important” added value according to HAS.
The quality of evidence supporting drug approval is undoubtedly a key point of the HTA process. Even if almost half of the studies are well-designed randomized, double-blind, placebo-controlled trials, it is noteworthy that no direct comparisons among the selected drugs with the same indication are available. This is one of the major issues for the HTA process management, especially with medicines approved earlier and earlier, since the lack of clear and robust evidence determines uncertainty about their therapeutic value and place in therapy.
In general, a direct comparison among drugs has been considered necessary for an adequate assessment of the additional benefit in Germany. For example, the G-BA considered the additional benefit of the ATMP Zolgensma® not proven, due to the lack of direct comparison with the available alternative nusinersen, and due to the limited clinical data available so far. Therefore, the German G-BA for the first time recommended to collect real-world evidence about Zolgensma® and Spinraza® through a registry study in order to close this evidence gap (Gozzo et al., 2021a; BundesausschussG-BG, 2021). Moreover, even for the third molecule approved for SMA, risdiplam, the G-BA concluded that no meaningful results are currently available, due to the lack of direct comparative data versus existing appropriate therapeutic alternatives, and recommended to collect data within the routine practice in order to improve the evidence for the benefit assessment.
Similarly, the French institutions considered that the lack of a direct comparison in clinical trials did not allow to clearly define the place in therapy of medicines for SMA (SantèH-HAd, 2020). However, in the absence of comparative data, in type 1 SMA and in pre-symptomatic patients with up to three copies of the SMN2 gene, HAS considers Spinraza® and Zolgensma® as first-line treatments; Evrysdi® can be used as first line in symptomatic patients with type 1 SMA, but has no place in pre-symptomatic setting. The choice among these alternatives must be performed according to age, clinical status, comorbidities, different route of administration, and family choice. For example, the daily oral administration of risdiplam may be an attractive option compared to the other available modalities of administration but may not be suitable for the youngest children due to treatment compliance.
In type 2 SMA, Spinraza® and Evrysdi® are the treatment to be preferred, while in type 3, they represent the only therapeutic option.
On the contrary, the Italian agency explicitly accepted the possibility of having low-quality evidence in the case of rare and ultra-rare diseases (AIFADETERMINA DELL’AGENZIA ITALIANA DEL FARMACO, 2017), including the lack of a direct comparison with available alternatives. Indeed, in the case of Zolgensma®, the experts of the Italian Commission considered “important” the added value compared to the antisense oligonucleotide nusinersen (AIFA, 2021a), even with the limitations of the indirect comparison. Nevertheless, its use has been limited to a restricted population, specifically only in patients weighing up to 13.5 kg with clinical diagnosis of type 1 SMA and onset of symptoms during the first 6 months of life or with genetic diagnosis of SMA type 1 and up to two copies of the SMN2 gene. Indeed, this subpopulation has been identified as the one with the greatest benefit and eligible to be reimbursed.
As regards to the monoclonal antibodies approved for migraine, the regulatory authorities of the three countries were in accordance with a low or no clinical added value in the management of the disease. In addition, the German institution delivered an opinion of “hint for a considerable additional benefit” of monoclonal antibodies compared to best supportive care (BSC), such as psychotherapy or relaxation techniques, only in adults who have at least four migraine days/month and for whom other substances used for prophylaxis (metoprolol, propranolol, flunarizine, topiramate, amitriptyline, valproic acid, or Clostridium botulinum toxin type A) have failed or have not been an option and BSC is the only treatment option.
Thus, limitations for the prescription of these drugs have been introduced, different among countries despite the overall agreement about the lack of added value.
A favorable opinion for reimbursement has been issued in France only in adults with severe migraine who have at least eight migraine days per month, after failure of at least two prophylactic treatments and without cardiovascular disease.
In Italy, the prescription can be performed according to the criteria of the AIFA Registry, in particular for adults with at least 8 days of disabling migraine per month in the last 3 months and with insufficient response after at least 6 weeks of treatment or being intolerant or having clear contraindications to at least three classes of prophylaxis migraine drugs.
According to the decision of the German GBA, a prescription is possible in patients with episodic migraine if at least 5 substances from the available pharmacological groups (beta-blockers, flunarizine, topiramate, valproic acid or amitriptyline) were not effective, not tolerated, or contraindicated (Hacke, 2020).
The variability in terms of regulatory decisions determining different patients access is probably related to the uncertainties about clinical value, the lack of long-term data and the demonstration of the superiority only versus placebo, as well as other non-clinical variables such as treatment cost.
In conclusion, the HTA process is a critical point for the assessment of drug value and patient access. Universally recognized clinical criteria for HTA recommendations include unmet medical needs, relative effectiveness, and safety of the new product compared to the available standard of care (van Nooten et al., 2012). The therapeutic added value versus available treatments should be one of the key determinants of patients access to innovative medicines. However, while relying on the evaluation of the same studies, a heterogeneity of the HTA assessment of clinical data has been observed among countries (Gozzo et al., 2021a). This heterogeneity, even beyond added value, does not necessarily translate into different reimbursement decisions, but often determines different eligibility criteria for patient treatment.
Given the importance of new medicines especially for rare and serious unmet needs, it is crucial to understand and act on the causes of inconsistency among the HTA assessments, in order to ensure rapid and uniform access to innovation for patients who can benefit.
In this context, the proposal for a regulation of the European Parliament and of the Council on health technology assessment amending the Directive 2011/24/EU drafted in 2018 and modified in 2021 aims to ensure a permanent cooperation on HTA at the EU level, sharing joint clinical assessments, joint scientific consultations, horizon scanning, and voluntary cooperation in non-clinical areas (European Commission and Directorate-General for Health and Food Safety, 2021). The adoption of this new regulation on HTA would be useful to harmonize HTA methodologies, hopefully leading to reduced disparities of medicine assessment among European countries.
Data Availability Statement
The original contributions presented in the study are included in the article/Supplementary Material, further inquiries can be directed to the corresponding author.
Author Contributions
LG wrote the first draft of the manuscript. FD checked and revised the draft manuscript. All authors contributed to the article and approved the submitted version.
Funding
GR was supported by the PON AIM R&I 2014-2020-E66C18001260007.
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s Note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors, and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary Material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fphar.2021.823199/full#supplementary-material
References
AIFA (2021a). DETERMINA 10 febbraio 2021 Rinegoziazione del medicinale per uso umano «Spinraza» ai sensi dell'articolo 8, comma 10, della legge 24 dicembre 1993, n. 537. (Determina n. DG/183/2021). (21A01038) (GU Serie Generale n.43 del 20-02-2021). Available at: https://www.gazzettaufficiale.it/eli/id/2021/02/20/21A01038/sg (Accessed on September, 2021).
AIFA (2021b). DETERMINA 10 luglio 2020 Riclassificazione del medicinale per uso umano «Aimovig», ai sensi dell'articolo 8, comma 10, della legge 24 dicembre 1993, n. 537. (Determina n. DG/728/2020). (20A03784) (GU Serie Generale n.182 del 21-07-2020). Available at: https://www.gazzettaufficiale.it/atto/serie_generale/caricaDettaglioAtto/originario?atto.dataPubblicazioneGazzetta=2020-07-21&atto.codiceRedazionale=20A03784&elenco30giorni=false (Accessed on September, 2021).
AIFA (2021c). DETERMINA 10 luglio 2020 Riclassificazione del medicinale per uso umano «Ajovy», ai sensi dell'articolo 8, comma 10, della legge 24 dicembre 1993, n. 537. (Determina n. DG/730/2020). (20A03783) (GU Serie Generale n.182 del 21-07-2020). Available at: https://www.gazzettaufficiale.it/atto/serie_generale/caricaDettaglioAtto/originario?atto.dataPubblicazioneGazzetta=2020-07-21&atto.codiceRedazionale=20A03783&elenco30giorni=false (Accessed on September, 2021).
AIFA. (2021d). DETERMINA 10 luglio 2020 Riclassificazione del medicinale per uso umano «Emgality», ai sensi dell'articolo 8, comma 10, della legge 24 dicembre 1993, n. 537. (Determina n. DG/732/2020). (20A03782) (GU Serie Generale n.182 del 21-07-2020). Available at: https://www.gazzettaufficiale.it/atto/serie_generale/caricaDettaglioAtto/originario?atto.dataPubblicazioneGazzetta=2020-07-21&atto.codiceRedazionale=20A03782&elenco30giorni=false#:∼:text=Indicazioni%20terapeutiche%20oggetto%20della%20negoziazione,giorni%20di%20emicrania%20al%20mese. Accessed on September 2021. 2021.
AIFA (2021e). DETERMINA 10 marzo 2021 Regime di rimborsabilita' e prezzo del medicinale per uso umano «Zolgensma». (Determina n. DG/277/2021). (21A01554) (GU Serie Generale n.62 del 13-03-2021). Available at: https://www.gazzettaufficiale.it/atto/serie_generale/caricaDettaglioAtto/originario?atto.dataPubblicazioneGazzetta=2021-03-13&atto.codiceRedazionale=21A01554&elenco30giorni=false (Accessed on September, 2021).
AIFA (2021f). DETERMINA 15 gennaio 2020 Regime di rimborsabilita' e prezzo di vendita del medicinale per uso umano «Onpattro». (Determina n. 77/2020). (20A00545) (GU Serie Generale n.24 del 30-01-2020). Available at: https://www.gazzettaufficiale.it/atto/serie_generale/caricaDettaglioAtto/originario?atto.dataPubblicazioneGazzetta=2020-01-30&atto.codiceRedazionale=20A00545&elenco30giorni=false (Accessed on September, 2021).
AIFA (2021g). DETERMINA 15 maggio 2020 Riclassificazione del medicinale per uso umano «Tegsedi», ai sensi dell'articolo 8, comma 10, della legge 24 dicembre 1993, n. 537. (Determina n. DG/607/2020). (20A02758) (GU Serie Generale n.135 del 27-05-2020). Available at: https://www.gazzettaufficiale.it/eli/id/2020/05/27/20A02758/sg (Accessed on September, 2021).
AIFA (2021h). DETERMINA 26 novembre 2014 Riclassificazione del medicinale per uso umano «Vyndaqel (tafamidis)» ai sensi dell'art. 8, comma 10, della legge 24 dicembre 1993, n. 537. (Determina n. 1389/2014). (14A09423) (GU Serie Generale n.286 del 10-12-2014). Available at: https://www.gazzettaufficiale.it/eli/id/2014/12/10/14A09423/sg (Accessed on September, 2021).
AIFA (2021i). Farmaci a Uso Compassionevole. Evrysdi. Available at: https://www.aifa.gov.it/en/farmaci-a-uso-compassionevole (Accessed on October, 2021).
AIFA (2021j). Innovatività Aimovig. Available at: https://www.aifa.gov.it/documents/20142/1220805/AIMOVIG_13821_INNOV._v.1.0.pdf (Accessed on September, 2021).
AIFA (2021k). Innovatività Ajovy. Available at: https://www.aifa.gov.it/documents/20142/1220805/AJOVY_14435_INNOV._v.1.0.pdf (Accessed on September, 2021).
AIFA (2021L). Innovatività Emagality. Available at: https://www.aifa.gov.it/documents/20142/1220805/EMGALITY_14320_INNOV._v.1.0.pdf (Accessed on September, 2021).
AIFA (2021m). Innovatività Onpattro. Available at: https://www.aifa.gov.it/documents/20142/1184740/ONPATTRO_13833_INNOV._v.1.0.pdf (Accessed on September, 2021).
AIFA (2021n). Innovatività Spinraza. Available at: https://www.aifa.gov.it/sites/default/files/6-Spinraza_v1.0.pdf (Accessed on September, 2021).
AIFA (2021o). Innovatività Zolgensma. Available at: https://www.aifa.gov.it/documents/20142/1504529/117_Zolgensma_scheda_innovativit%C3%A0_GRADE.pdf (Accessed on September, 2021).
AIFA (2021p). Report innovatività Zolgensma. Det. n. 277 del 10/03/2021 GU Serie Generale n. 62 del 13/03/2021. Available at: https://www.aifa.gov.it/farmaci-innovativi (Accessed on April, 2021).
AIFADETERMINA DELL’AGENZIA ITALIANA DEL FARMACO (2017). Criteri per la classificazione dei farmaci innovativi e dei farmaci oncologici innovativi ai sensi dell’articolo 1, comma 402, della legge 11 dicembre 2016, 232. 31 MARZO 2017(Determina n. 519/2017). (2017).
Akehurst, R. L., Abadie, E., Renaudin, N., and Sarkozy, F. (2017). Variation in Health Technology Assessment and Reimbursement Processes in Europe. Value Health 20 (1), 67–76. doi:10.1016/j.jval.2016.08.725
Allen, N., Liberti, L., Walker, S. R., and Salek, S. (2017). A Comparison of Reimbursement Recommendations by European HTA Agencies: Is There Opportunity for Further Alignment. Front. Pharmacol. 8, 384. doi:10.3389/fphar.2017.00384
Angelis, A., Lange, A., and Kanavos, P. (2018). Using Health Technology Assessment to Assess the Value of New Medicines: Results of a Systematic Review and Expert Consultation across Eight European Countries. Eur. J. Health Econ. 19 (1), 123–152. doi:10.1007/s10198-017-0871-0
Arneric, S. P., Kern, V. D., and Stephenson, D. T. (2018). Regulatory-accepted Drug Development Tools Are Needed to Accelerate Innovative CNS Disease Treatments. Biochem. Pharmacol. 151, 291–306. doi:10.1016/j.bcp.2018.01.043
Brancati, S., Gozzo, L., Longo, L., Vitale, D. C., and Drago, F. (2021a). Rituximab in Multiple Sclerosis: Are We Ready for Regulatory Approval. Front. Immunol. 12, 661882. doi:10.3389/fimmu.2021.661882
Brancati, S., Gozzo, L., Longo, L., Vitale, D. C., Russo, G., and Drago, F. (2021b). Fertility Preservation in Female Pediatric Patients with Cancer: A Clinical and Regulatory Issue. Front. Oncol. 11, 641450. doi:10.3389/fonc.2021.641450
Breccia, M., Celant, S., Olimpieri, P. P., Olimpieri, O. M., Pane, F., Iurlo, A., et al. (2021). Mortality Rate in Patients with Chronic Myeloid Leukemia in Chronic Phase Treated with Frontline Second Generation Tyrosine Kinase Inhibitors: a Retrospective Analysis by the Monitoring Registries of the Italian Medicines Agency (AIFA). Ann. Hematol. 100 (2), 481–485. doi:10.1007/s00277-021-04406-1
Breccia, M., Olimpieri, P. P., Olimpieri, O., Pane, F., Iurlo, A., Foggi, P., et al. (2020). How many Chronic Myeloid Leukemia Patients Who Started a Frontline Second-Generation Tyrosine Kinase Inhibitor Have to Switch to a Second-Line Treatment? A Retrospective Analysis from the Monitoring Registries of the Italian Medicines agency (AIFA). Cancer Med. 9 (12), 4160–4165. doi:10.1002/cam4.3071
Bucolo, C., Musumeci, M., Salomone, S., Romano, G. L., Leggio, G. M., Gagliano, C., et al. (2015). Effects of Topical Fucosyl-Lactose, a Milk Oligosaccharide, on Dry Eye Model: An Example of Nutraceutical Candidate. Front. Pharmacol. 6, 280. doi:10.3389/fphar.2015.00280
Bundesausschuss G-Bg (2021). Resolution of the Federal Joint Committee (G-BA) on the Amendment of the Pharmaceuticals Directive (AM-RL): Onasemnogene Abeparvovec (Spinal Muscular Atrophy); Requirement of Routine Data Collection and Evaluations. Available at: https://www.g-ba.de/downloads/39-1464-4702/2021-02-04_AM-RL-XII_Onasemnogen-Abeparvovec_AADCE_EN.pdf (Accessed on March, 2021).
Bundesausschuss G-Bg (2010). The Benefit Assessment of Medicinal Products in Accordance with the German Social Code, Book Five (SGB V), Section 35a. Available at: https://www.g-ba.de/english/benefitassessment/(Accessed on March, 2021).
Ciani, O., and Jommi, C. (2014). The Role of Health Technology Assessment Bodies in Shaping Drug Development. Drug Des. Devel Ther. 8, 2273–2281. doi:10.2147/DDDT.S49935
COMMUNITIES TCOTE (1993). Council Regulation (EEC) No 2309/93 of 22 July 1993 Laying Down Community Procedures for the Authorization and Supervision of Medicinal Products for Human and Veterinary Use and Establishing a European Agency for the Evaluation of Medicinal Products.
Drago, F., Gozzo, L., Li, L., Stella, A., and Cosmi, B. (2020). Use of Enoxaparin to Counteract COVID-19 Infection and Reduce Thromboembolic Venous Complications: A Review of the Current Evidence. Front. Pharmacol. 11, 579886. doi:10.3389/fphar.2020.579886
Drummond, M. F., Schwartz, J. S., Jönsson, B., Luce, B. R., Neumann, P. J., Siebert, U., et al. (2008). Key Principles for the Improved Conduct of Health Technology Assessments for Resource Allocation Decisions. Int. J. Technol. Assess. Health Care 24 (3), 244–248. ; discussion 362-8. doi:10.1017/S0266462308080343
EC (2020). COMMUNICATION from the COMMISSION to the EUROPEAN PARLIAMENT, the COUNCIL, the EUROPEAN ECONOMIC and SOCIAL COMMITTEE and the COMMITTEE of the REGIONS Pharmaceutical Strategy for Europe COM/2020/761 Final. Available at: https://eur-lex.europa.eu/legal-content/EN/TXT/?uri=CELEX%3A52020DC0761 (Accessed on November, 2021).
EMA (2020a). ANNUAL REPORT 2020. Available at: https://www.ema.europa.eu/en/documents/annual-report/2020-annual-report-european-medicines-agency_en.pdf (Accessed on November 2021).
EMA (2021a). Assessment Report Onpattro. Available at: https://www.ema.europa.eu/en/search/search?search_api_views_fulltext=Onpattro (Accessed on September, 2021).
EMA (2021b). Assessment Report Ajovy. Available at: https://www.ema.europa.eu/en/medicines/human/EPAR/ajovy (Accessed on September, 2021).
EMA (2021c). Assessment Report Emgality. Available at: https://www.ema.europa.eu/en/medicines/human/EPAR/emgality (Accessed on September, 2021).
EMA (2021d). Assessment Report Evrysdi. Available at: https://www.ema.europa.eu/en/medicines/human/EPAR/evrysdi (Accessed on September, 2021).
EMA (2021e). Assessment Report Libmeldy. Available at: https://www.ema.europa.eu/en/medicines/human/EPAR/libmeldy (Accessed on September, 2021).
EMA (2021f). Assessment Report Skysona. Available at: https://www.ema.europa.eu/en/medicines/human/EPAR/skysona (Accessed on September, 2021).
EMA (2021g). Assessment Report Spinraza. Available at: https://www.ema.europa.eu/en/medicines/human/EPAR/spinraza (Accessed on September, 2021).
EMA (2021h). Assessment Report Tegsedi. Available at: https://www.ema.europa.eu/en/medicines/human/EPAR/tegsedi (Accessed on September, 2021).
EMA (2021i). Assessment Report Vyndaqel. Available at: https://www.ema.europa.eu/en/medicines/human/EPAR/vyndaqel (Accessed on September, 2021).
EMA (2020b). Assessment Report Zolgensma. Available at: https://www.ema.europa.eu/en/documents/assessment-report/zolgensma-epar-public-assessment-report_en.pdf (Accessed on March, 2021).
EMA (2021j). Assessment Report Aimovig. Available at: https://www.ema.europa.eu/en/medicines/human/EPAR/aimovig (Accessed on September, 2021).
EMA (2021k). Table of All EPARs for Human and Veterinary Medicines. Available at: https://www.ema.europa.eu/en/medicines/download-medicine-data (Accessed on September, 2021).
European Commission, Directorate-General for Health and Food Safety (2021). Proposal for a Regulation of the European Parliament and of the Council on Health Technology Assessment and Amending Directive 2011/24/EU - Partial Mandate for Negotiations with the European Parliament. 24 March 2021.
Fisichella, V., Giurdanella, G., Platania, C. B., Romano, G. L., Leggio, G. M., Salomone, S., et al. (2016). TGF-β1 Prevents Rat Retinal Insult Induced by Amyloid-β (1-42) Oligomers. Eur. J. Pharmacol. 787, 72–77. doi:10.1016/j.ejphar.2016.02.002
G-BA (2021a). Nutzenbewertungsverfahren Zum Wirkstoff Erenumab. Available at: https://www.g-ba.de/bewertungsverfahren/nutzenbewertung/679/(Accessed on October, 2021).
G-BA (2021b). Nutzenbewertungsverfahren Zum Wirkstoff Fremanezumab. Available at: https://www.g-ba.de/bewertungsverfahren/nutzenbewertung/462/(Accessed on September, 2021).
G-BA (2021c). Nutzenbewertungsverfahren Zum Wirkstoff Galcanezumab. Available at: https://www.g-ba.de/bewertungsverfahren/nutzenbewertung/450/(Accessed on September, 2021).
G-BA (2021d). Nutzenbewertungsverfahren Zum Wirkstoff Inotersen. Available at: https://www.g-ba.de/bewertungsverfahren/nutzenbewertung/390/(Accessed on September, 2021).
G-BA (2021e). Nutzenbewertungsverfahren Zum Wirkstoff Nusinersen. Available at: https://www.g-ba.de/bewertungsverfahren/nutzenbewertung/625/#english (Accessed on September, 2021).
G-BA (2021f). Nutzenbewertungsverfahren Zum Wirkstoff Onasemnogen-Abeparvovec. Available at: https://www.g-ba.de/bewertungsverfahren/nutzenbewertung/689/(Accessed on November, 2021).
G-BA (2021g). Nutzenbewertungsverfahren Zum Wirkstoff Patisiran. Available at: https://www.g-ba.de/bewertungsverfahren/nutzenbewertung/389/(Accessed on September, 2021).
G-BA (2021h). Nutzenbewertungsverfahren Zum Wirkstoff Risdiplam. Available at: https://www.g-ba.de/bewertungsverfahren/nutzenbewertung/680/#english (Accessed on October, 2021).
G-BA (2021i). Nutzenbewertungsverfahren Zum Wirkstoff Tafamidis. Available at: https://www.g-ba.de/bewertungsverfahren/nutzenbewertung/621/(Accessed on September, 2021).
Gozzo, L., Di Lenarda, A., Mammarella, F., Olimpieri, P. P., Cirilli, A., Cuomo, M., et al. (2021). Starting Dose and Dose Adjustment of Non-vitamin K Antagonist Oral Anticoagulation Agents in a Nationwide Cohort of Patients with Atrial Fibrillation. Sci. Rep. 11 (1), 20689. doi:10.1038/s41598-021-99818-4
Gozzo, L., Longo, L., Vitale, D. C., and Drago, F. (2020). Dexamethasone Treatment for Covid-19, a Curious Precedent Highlighting a Regulatory Gap. Front. Pharmacol. 11, 621934. doi:10.3389/fphar.2020.621934
Gozzo, L., Longo, L., Vitale, D. C., and Drago, F. (2020). The Regulatory Challenges for Drug Repurposing during the Covid-19 Pandemic: The Italian Experience. Front. Pharmacol. 11, 588132. doi:10.3389/fphar.2020.588132
Gozzo, L., Navarria, A., Benfatto, G., Longo, L., Mansueto, S., Sottosanti, L., et al. (2017). Safety of Antiplatelet Agents: Analysis of 'Real-World' Data from the Italian National Pharmacovigilance Network. Clin. Drug Investig. 37 (11), 1067–1081. doi:10.1007/s40261-017-0566-4
Gozzo, L., Navarria, A., Drago, V., Longo, L., Mansueto, S., Pignataro, G., et al. (2016). Linking the Price of Cancer Drug Treatments to Their Clinical Value. Clin. Drug Investig. 36 (7), 579–589. doi:10.1007/s40261-016-0403-1
Gozzo, L., Romano, G. L., Romano, F., Brancati, S., Longo, L., Vitale, D. C., et al. (2021). Health Technology Assessment of Advanced Therapy Medicinal Products: Comparison Among 3 European Countries. Front. Pharmacol. 12, 755052. doi:10.3389/fphar.2021.755052
Gozzo, L., Vetro, C., Brancati, S., Longo, L., Vitale, D. C., Romano, G. L., et al. (2021). Off-Label Use of Venetoclax in Patients with Acute Myeloid Leukemia: Single Center Experience and Data from Pharmacovigilance Database. Front. Pharmacol. 12 (3212), 748766. doi:10.3389/fphar.2021.748766
Gozzo, L., Viale, P., Longo, L., Vitale, D. C., and Drago, F. (2020). The Potential Role of Heparin in Patients with COVID-19: Beyond the Anticoagulant Effect. A Review. Front. Pharmacol. 11, 1307. doi:10.3389/fphar.2020.01307
Gribkoff, V. K., and Kaczmarek, L. K. (2017). The Need for New Approaches in CNS Drug Discovery: Why Drugs Have Failed, and what Can Be Done to Improve Outcomes. Neuropharmacology 120, 11–19. doi:10.1016/j.neuropharm.2016.03.021
Hacke, W. (2020). Neurological Research and Practice: the First Year. Neurol. Res. Pract. 2, 5. doi:10.1186/s42466-020-0054-9
HAS (2021a). AVIS SUR LES MÉDICAMENTS - Mis en ligne le 23 sept. 2020. AJOVY. Available at: https://www.has-sante.fr/jcms/p_3202357/fr/ajovy-fremanezumab (Accessed on September, 2021).
HAS (2021b). AVIS SUR LES MÉDICAMENTS - Mis en ligne le 29 oct. 2021. ZOLGENSMA. Available at: https://www.has-sante.fr/jcms/p_3291799/fr/zolgensma-2-x-10-13-genomes-du-vecteur/ml-onasemnogene-abeparvovec (Accessed on October, 2021).
HAS (2021c). AVIS SUR LES MÉDICAMENTS - Mis en ligne le 30 avr. 2021. LIBMELDY. Available at: https://www.has-sante.fr/jcms/p_3263243/fr/libmeldy-population-autologue-enrichie-en-cellules-cd34-qui-contient-des-cellules-souches-progenitrices-hematopoietiques-transduites-ex-vivo-avec-un-vecteur-lentiviral-codant-le-gene-de-l-arylsulfatase-a-humaine (Accessed on September, 2021).
HAS (2021d). AVIS SUR LES MÉDICAMENTS - Mis en ligne le 30 sept. 2021. EVRYSDI. Available at: https://www.has-sante.fr/jcms/p_3289078/fr/evrysdi-0-75-mg/ml-risdiplam (Accessed on September, 2021).
HAS (2021e). MÉDICAMENT - Mis en ligne le 02 sept. 2020. SPINRAZA. Available at: https://www.has-sante.fr/jcms/pprd_2983397/fr/spinraza-nusinersen (Accessed on September, 2021).
HAS (2021f). MÉDICAMENT - Mis en ligne le 16 oct. 2019. AIMOVIG. Available at: https://www.has-sante.fr/jcms/pprd_2982839/fr/aimovig-erenumab (Accessed on September, 2021).
HAS (2021g). MÉDICAMENT - Mis en ligne le 16 oct. 2020. VYNDAQEL. Available at: https://www.has-sante.fr/jcms/pprd_2985026/fr/vyndaqel-tafamidis (Accessed on September, 2021).
HAS (2021h). MÉDICAMENT - Mis en ligne le 22 janv. 2020. ONPATTRO. Available at: https://www.has-sante.fr/jcms/pprd_2982827/fr/onpattro-patisiran (Accessed on September, 2021).
HAS (2021i). MÉDICAMENT - Mis en ligne le 29 juin 2020. EMGALITY. Available at: https://www.has-sante.fr/jcms/p_3191590/fr/emgality-galcanezumab (Accessed on September, 2021).
HAS (2021j). MÉDICAMENT - Mis en ligne le 30 sept. 2019. TEGSEDI. Available at: https://www.has-sante.fr/jcms/pprd_2982780/fr/tegsedi-inotersen (Accessed on September, 2021).
Jommi, C., Armeni, P., Costa, F., Bertolani, A., and Otto, M. (2020). Implementation of Value-Based Pricing for Medicines. Clin. Ther. 42 (1), 15–24. doi:10.1016/j.clinthera.2019.11.006
National Academies of Sciences, Engineering, and Medicine (2016). Neuroscience Trials of the Future: Proceedings of a Workshop. Washington (DC): The National Academies Press. doi:10.17226/23502
O'Donnell, P., Rosen, L., Alexander, R., Murthy, V., Davies, C. H., and Ratti, E. (2019). Strategies to Address Challenges in Neuroscience Drug Discovery and Development. Int. J. Neuropsychopharmacol. 22 (7), 445–448. doi:10.1093/ijnp/pyz027
Olimpieri, P. P., Di Lenarda, A., Mammarella, F., Gozzo, L., Cirilli, A., Cuomo, M., et al. (2020). Non-vitamin K Antagonist Oral Anticoagulation Agents in Patients with Atrial Fibrillation: Insights from Italian Monitoring Registries. Int. J. Cardiol. Heart Vasc. 26, 100465. doi:10.1016/j.ijcha.2019.100465
Pankevich, D. E., Altevogt, B. M., Dunlop, J., Gage, F. H., and Hyman, S. E. (2014). Improving and Accelerating Drug Development for Nervous System Disorders. Neuron 84 (3), 546–553. doi:10.1016/j.neuron.2014.10.007
Regulation EC (2004). Regulation (EC) No 726/2004 of the European Parliament and of the Council of 31 March 2004 Laying Down Community Procedures for the Authorisation and Supervision of Medicinal Products for Human and Veterinary Use and Establishing a European Medicines Agency (Text with EEA Relevance).
Richardson, J., and Schlander, M. (2019). Health Technology Assessment (HTA) and Economic Evaluation: Efficiency or Fairness First. J. Mark Access Health Pol. 7 (1), 1557981. doi:10.1080/20016689.2018.1557981
Santè H-HAd (2013). Le service médical rendu (SMR) et l’amélioration du service médical rendu (ASMR). Available at: https://www.has-sante.fr/jcms/r_1506267/fr/le-service-medical-rendu-smr-et-l-amelioration-du-service-medical-rendu-asmr (Accessed on March, 2021).
Santè H-HAd (2014). Pricing & Reimbursement of Drugs and HTA Policies in France. Available at: https://www.has-sante.fr/upload/docs/application/pdf/2014-03/pricing_reimbursement_of_drugs_and_hta_policies_in_france.pdf (Accessed on March, 2021).
Santè H-HAd (2020). Zolgensma_16122020_AVIS_CT18743. Available at: https://www.has-sante.fr/upload/docs/evamed/CT-18743_ZOLGENSMA_PIC_INS_AvisDef_CT18743.pdf (Accessed on March, 2021).
Toro, M. D., Gozzo, L., Tracia, L., Cicciù, M., Drago, F., Bucolo, C., et al. (2021). New Therapeutic Perspectives in the Treatment of Uveal Melanoma: A Systematic Review. Biomedicines 9 (10), 1311. doi:10.3390/biomedicines9101311
van Nooten, F., Holmstrom, S., Green, J., Wiklund, I., Odeyemi, I. A., and Wilcox, T. K. (2012). Health Economics and Outcomes Research within Drug Development: Challenges and Opportunities for Reimbursement and Market Access within Biopharma Research. Drug Discov. Today 17 (11-12), 615–622. doi:10.1016/j.drudis.2012.01.021
Keywords: orphan drugs, neurological diseases, access, added therapeutic benefit, drug value
Citation: Gozzo L, Romano GL, Brancati S, Cicciù M, Fiorillo L, Longo L, Vitale DC and Drago F (2022) Access to Innovative Neurological Drugs in Europe: Alignment of Health Technology Assessments Among Three European Countries. Front. Pharmacol. 12:823199. doi: 10.3389/fphar.2021.823199
Received: 26 November 2021; Accepted: 29 December 2021;
Published: 04 February 2022.
Edited by:
Domenico Criscuolo, Italian Society of Pharmaceutical Medicine, ItalyReviewed by:
YoTsen Liu, Taipei Veterans General Hospital, TaiwanGeorgi Iskrov, Plovdiv Medical University, Bulgaria
Copyright © 2022 Gozzo, Romano, Brancati, Cicciù, Fiorillo, Longo, Vitale and Drago. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Lucia Gozzo, bHVjaWFnb3p6bzg2QGljbG91ZC5jb20=