 Catherine Goetzinger1,2*
Catherine Goetzinger1,2* Caroline Alleaume3
Caroline Alleaume3 Anna Schritz4
Anna Schritz4 Bernard Vrijens5Marie Préau6Guy Fagherazzi1,2Laetitia Huiart3
Bernard Vrijens5Marie Préau6Guy Fagherazzi1,2Laetitia Huiart3- 1Deep Digital Phenotyping Research Unit, Department of Precision Health, Luxembourg Institute of Health, Strassen, Luxembourg
- 2University of Luxembourg, Faculty of Science, Technology and Medicine, Esch-sur-Alzette, Luxembourg
- 3Santé Publique France, Paris, France
- 4Competence Center for Methodology and Statistics, Luxembourg Institute of Health, Strassen, Luxembourg
- 5AARDEX Group & Department of Public Health, Liège University, Liège, Belgium
- 6Institut de Psychologie, Université Lumière Lyon 2, Lyon, France
Introduction: Up to 50% of breast cancer (BC) survivors discontinue their adjuvant endocrine therapy (AET) before the recommended 5 years, raising the issue of medication non-adherence. eHealth technologies have the potential to support patients to enhance their medication adherence and may offer an effective way to complement the healthcare. In order for eHealth technologies to be successfully implemented into the healthcare system, end-users need to be willing and accepting to use these eHealth technologies.
Aim: This study aims to evaluate the current usability of eHealth technologiesin and to identify differences in BC SURVIVORS BC survivors accepting a medication adherence enhancing eHealth technology to support their AET to BC survivors that do not accept such a medication adherence enhancing eHealth technology.
Methods: This study was conducted in 2020 including volunteering BC survivors belonging to the Seintinelles Association. Eligible participants were women, diagnosed with BC within the last 10 years, and been exposed to, an AET. Univariable and multivariable logistic regression analyses were performed to investigate medication adherence enhancing eHealth technology acceptance profiles among BC survivors. The dependent variable was defined as acceptance of an electronic pillbox connected to a smartphone application (hereafter: medication adherence enhancing eHealth technology).
Results: Overall, 23% of the participants already use a connected device or health application on a regular basis. The mean age of the participants was 52.7 (SD 10.4) years. In total, 67% of 1268 BC survivors who participated in the survey declared that they would accept a medication adherence enhancing eHealth technology to improve their AET. BC survivors accepting a medication adherence enhancing eHealth technology for their AET, are younger (OR = 0.97, 95% CI [0.95; 0.98]), do take medication for other diseases (OR = 0.31, 95% CI [0.13; 0.68]), already use a medication adherence enhancing eHealth technology or technique (OR = 1.74, 95% CI [1.06; 2.94]) and are willing to possess or currently possess one or more connected devices or health applications (OR = 2.89, 95% CI [2.01; 4.19]).
Conclusion: Understanding acceptance profiles of BC survivors is fundamental for conceiving an effective eHealth technology enhancing AET among BC survivors. Hence, such profiling will foster the development of personalized medication adherence enhancing eHealth technology.
1 Introduction
Breast cancer (BC) is the most common cancer among women, as 355,000 are estimated to be diagnosed with BC each year in Europe (International Agency for Research on Cancer et al., 2020). The majority (80%) of BC patients are hormone receptor–positive and most (>90%) have stage I to III and are eligible for adjuvant endocrine therapy (AET) (Partridge et al., 2003).
The shift, that BC survivors experience from the acute phase of treatment (e.g., surgery, chemotherapy, radiotherapy) to the post-acute phase (e.g., AET), is associated with social and medical challenges (Kantsiper et al., 2009; Hurtado-de-Mendoza et al., 2017; Goetzinger et al., 2020). Patients recurrently reported the need for increased support in terms of AET management (adherence and side effects) as well as increased patient–healthcare provider communication and follow-up (Finitsis et al., 2019; Pouls et al., 2021). During this post-acute treatment period, most BC survivors report anxiety, fear, and struggle to find their way back into everyday life. In addition, BC survivors usually do not visit their oncologist for a relatively long period during the post-acute treatment phase (Ringwald et al., 2017; Goetzinger et al., 2020). Thus the value of HCP support during this survivorship period of BC patients is undebatable for medication adherence and disease management (Kini and Michael Ho, 2018).
Medication adherence is a dynamic behaviour influenced by various factors (Sabaté and World Health Organization, 2003; Kardas et al., 2013) and is defined as the process by which patients take their medication as prescribed. This medication adherence process is further categorized into three distinct phases: 1. Initiation (patient takes the first dose of prescribed medication), 2. Implementation (the extent to which a patient’s actual dosing corresponds to the prescribed dosing regimen, from initiation until the last dose is taken) and 3. Discontinuation (occurs when the patient stops taking the prescribed medication, for whatever reason(s)) (Vrijens et al., 2012). Previous work demonstrated that 30%–50% of BC survivors discontinue their AET before the recommended 5 years end depending on the AET agent and method of medication adherence measurement (Huiart et al., 2011). Moreover, it was shown that AET reduces BC recurrence rate by 50% and mortality by a third (Davies et al., 2011; Pistilli et al., 2020). Therefore, it is key to identify AET non-adherence, to reduce the risk for poorer health outcomes (Pistilli et al., 2020). To date, there is no gold standard to identify non-adherence. Indirect methods such as pharmacy prescription refills or patient-administered questionnaires are mostly used, yet fail to measure the real medication intake or even overestimate adherence (Lu et al., 2018).
The World Health Organization defines eHealth ‘as the cost-effective and secure use of information and communications technologies in support of health and health-related fields, including health-care services, health surveillance, health literature, and health education, knowledge and research (World Health Organization, 2022)’. Concerning the field of medication adherence research and eHealth, medication adherence technologies (MATech) such as electronic pillboxes or smartphone applications have been developed (Ahmed et al., 2018). Car et al. highlighted that these MATechs are the future for self-management of treatment and medication adherence monitoring (Car et al., 2017). A systematic review by Nieuwlaat et al. showed that MATechs are most effective if multiple components, trying to overcome barriers to adherence by means of tailored ongoing support from allied health professionals are used (Nieuwlaat et al., 2014). Nevertheless, the most effective interventions did not lead to large improvements in adherence or clinical outcomes (Hadji et al., 2013; Finitsis et al., 2019; Rosenberg et al., 2020). This is because most of those interventions were created without the involvement of the end-user, whereas patient involvement is key in research and implantation into the healthcare setting (De Geest et al., 2020; Aguayo et al., 2021). Thus, BC survivor involvement is key to conceive effective MATechs to enhance AET. In order to personalize medication adherence enhancing interventions for subtypes of BC survivor users, it is important to profile the acceptance of BC survivors to use medication adherence enhancing eHealth technology for AET enhancement.
Therefore, the present study aims to 1) evaluate the current usability of eHealth technologies in BC survivors and to 2) identify differences in BC survivors accepting medication adherence enhancing eHealth technology to enhance their AET to BC survivors that do not accept such a medication adherence enhancing eHealth technology. In this study, we define medication adherence enhancing eHealth technology as an electronic pillbox connected to a smartphone application.
2 Method
2.1 Study design
A cross-sectional, e-survey was conducted from July to December 2020 among BC survivors from the French Seintinelles platform (www.seintinelles.com). Seintinelles is a non-profit community-based research platform, developed in collaboration with psycho-oncologists to facilitate the implication of patients into cancer research (Bauquier et al., 2017; Pannard et al., 2020). Volunteering citizens, regardless of their current health condition and/or cancer type, can participate in this platform, comprised of over 8000 BC patients (in 2020), the target population of the present study. Thus, this platform has the ability to recruit a large number of participants in a very limited time.
2.2 Recruitment and study population
Seintinelles sent an email to all its BC members, informing them about the study objectives, along with the information sheet (Supplementary Appendix 1). If they were interested in participating, they were asked to complete a short questionnaire on the website to verify that they met all the inclusion criteria (Supplementary Appendix 2). Inclusion criteria for this e-survey were:
- Women,
- BC diagnosed within the last 10 years,
- at least temporarily exposed to an AET.
If participants met all inclusion criteria and still wanted to participate, they signed an e-consent form before starting the e-survey (Supplementary Appendix 2).
2.3 e-survey
The e-survey used within the present study aims to establish a state of art on current eHealth usability and potential acceptability of medication adherence enhancing eHealth technology in BC survivors.
The e-survey consists of about 30 questions and required participants’ attention for at least 20 min. They had the option to interrupt the questionnaire, and could save their answers to continue later. There were no incentives given to participants. BC survivors (N = 2) proofread the final version of the e-survey. CG and CA as well as employees of Seintinelles pre-tested the e-survey with respect to technical errors and incorrect utilisation of question filters. While conducting the e-survey, participants could only see one question at a time. It was mandatory to answer the question in order to get to the next. This method was used to ensure that no questions was left unanswered.
2.4 Measurement
The e-survey was subdivided into five sections to collect data on socio-demographic characteristics, health status and disease experience, medication adherence, eHealth utilization and a specific section on medication adherence enhancing eHealth technology. For more information, Supplementary Appendix 3 illustrates the structure and definitions of the e-survey.
2.4.1 Sociodemographic characteristics
The first section of the e-survey collected data on participants’ age, marital status, having children and number of children. In addition, participants responded to questions asking about their educational, professional and financial status. These items were adapted from the questionnaire used in Vican 5, a French nationwide population-based questionnaire aiming to explore life 5 years after cancer diagnosis (Bauquier et al., 2017).
2.4.2 Health status and disease experience
The second section investigated participant’s general health status and their experience with BC in the acute phase of treatment. These questions were either developed by CA and CG or taken from Vican 5 (Bouhnik et al., 2015).
2.4.3 AET adherence
The third section analyzed the adherence to AET in terms of persistence and if discontinuation for which reasons. In addition, this third section investigated experienced side effects and use of support by psychologists or alternative medicine. Furthermore, current techniques or eHealth technologies used to support participants with their AET intake were investigated.
This section sums up by evaluating the patient–physician relationship and communication. CA and CG developed these questions.
2.4.4 eHealth utilization
Section 4 evaluated current eHealth utilisation. This section of the questionnaire-survey was based on a self-administered qualitative questionnaire used in social psychology science in the DISCO trial (DISpositif COnnecté’, connected device in English) investigating the use and acceptability of connected devices in breast cancer (Touillaud et al., 2021). As in the questionnaire from the DISCO trial, we provided the participant with two definitions, explaining ‘connected device’ and ‘mobile application’. In contrast to the DISCO trial questionnaire, the present study focuses more precisely on adherence to OHT in BC survivors, thus additional items, created by CG and CA, were based on the results found by Goetzinger et al. (2020).
2.4.5 Medication adherence enhancing eHealth technology
The fifth section investigated acceptability and related barriers and facilitators to acceptability and usability of a proposed medication adherence enhancing eHealth technology supporting AET management in BC survivors. This paper will only focus on the first question of this section, as it is the dependent variable used for the univariable and multivariable logistic regression analyses.
2.5 Dependent variable
The dependent variable ‘Acceptance of a Medication adherence enhancing eHealth technology (electronic pillbox connected to a smartphone application)’’ (1 = yes, 0 = no) was computed from ‘Would you accept to use an electronic blister connected to an application on your phone to support your AET treatment’. Hence, we categorized the following answers together to receive a binary variable;
‘Yes’ includes the following answer options:
• ‘Yes, I accept voluntarily’,
• ‘Yes, if my Doctor asks me to’,
• ‘Yes, depending on the information provided’.
‘No’ includes these answer options;
• ‘No, I do not trust connected devices’,
• ‘No, I don’t know how to use new technology’,
• ‘No, I don’t have a smartphone and I don’t want one’,
• ‘No, for other reasons’.
2.6 Ethical provision
The study received approval by the National Commission for Information and Freedoms (Commission nationale de l’informatique et des libertés, CNIL: 1955704) and the Sud-EST II data protection committee (Comité de Protection des données, Numéro EudraCT: 2020-A00665-34).
2.7 Statistical analysis
This study uses descriptive statistics to characterize the study population and to highlight current patterns of eHealth use in BC survivors. Univariable and multivariable logistic regression analyses were performed to evaluate differences in BC survivors that accept an electronic blister connected to app to support AET adherence with those that do not. Odds ratios were used as the measure of association to compare the strength of the correlation between ‘Medication adherence enhancing eHealth technology acceptance’ and relative predictors. We performed a both-way stepwise logistic regression analysis to investigate factors that are significantly associated with accepting an electronic blister connected to the app to support AET adherence. The final model was retained as the lowest AIC was achieved. Significance was accepted at a p-value lower than 0.05, with a 95% Confidence Interval. We used the R software version 4.0.3 including the ‘ISwR’, ‘oddsratio’, ‘StepReg’, ‘forestplot’ and ‘dyplr’ packages to analyse the data and conceive the figure. This study used only completed questionnaires in order to avoid weighing and computation of missing values.
3 Results
Overall, 1,516 eligible Seintinelles members started the questionnaire, 1268 BC survivors responded to the complete online questionnaire and were used for the analysis. No missing values were recorded in our dataset as participants could only proceed in the questionnaire when the previous question was answered.
The overall study sample is on average 52.7 years (SD 10.4) old, over half is married (73.9%), and employed (60.3%) (Table 1). Furthermore, 46% of the overall sample reported good general health, and more than half of the study sample did not use any other medication for other diseases (52.8%). 21% of the participants were diagnosed with BC before 2012, 12% in 2015 and 21% after 2018. About a third (32.6%) of the BC survivors state that their BC does have ‘some effect’ on their life. Only 7.7% of the BC survivors evaluate themselves to be able to control their disease and almost 40% claim to have very good knowledge about the disease. Moreover, 88% highlighted that they had no BC recurrence up to the date of the questionnaire completion.
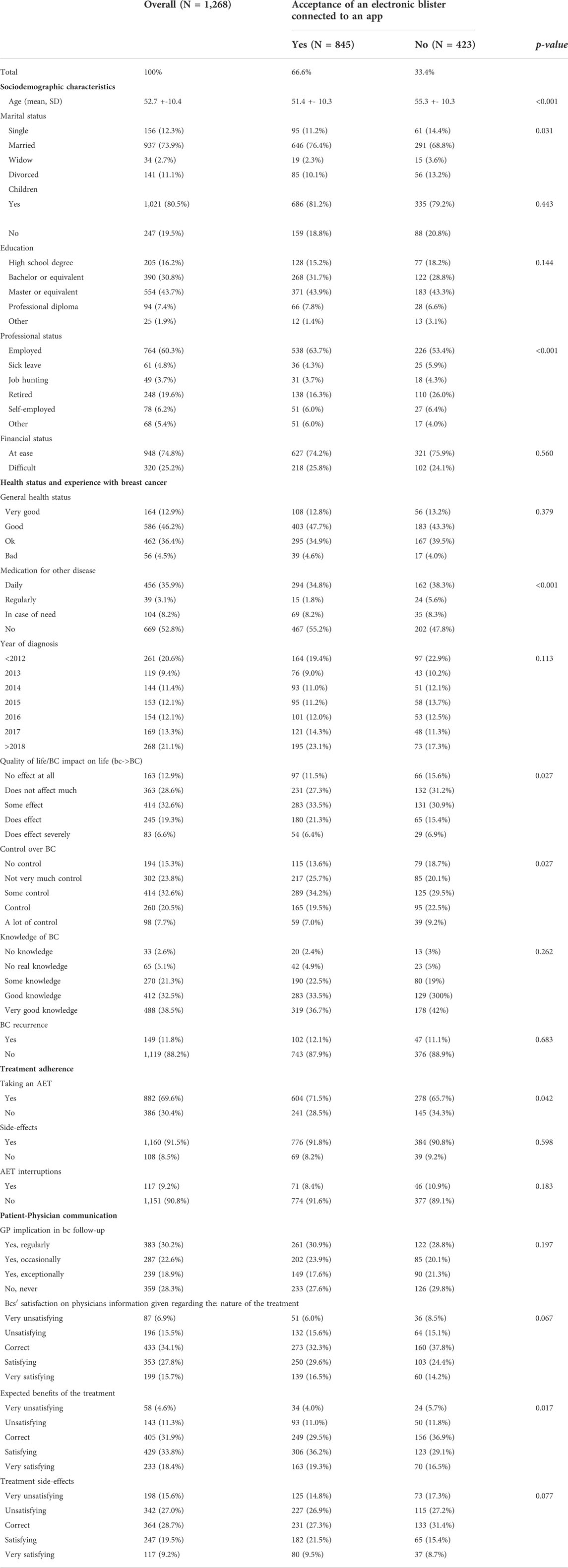
TABLE 1. Descriptive characteristics of BCS (Seintinelles study, 2020).
At the time of the questionnaire, 69.6% of the BC survivors were taking an AET, 91.5% experienced side effects and 9.2% interrupted their AET. Most women stated that their GP is somewhat implicated in their BC follow-up. A third (33.8) of the BC survivors stated that the information provided by their physician regarding the benefits of their AET is satisfying.
3.1 Current eHealth use among BC survivors
Approximately 38% of the included BC survivors did already possess one or more connected devices or health applications and 39% of those use these tools every day (Table 2). 18.7% of these women use these tools to motivate themselves, followed by 14.3% to monitor their health. Current techniques or devices to help BC survivors to adhere to their AET are specific locations to store their AET blister (47.2%), phone alarm (13.0%) and Pillbox (13.3%). About 12% of the BC survivors use at least two of those aids regularly. Most participants (90.3%) claim that these aids help them to adhere to their AET.
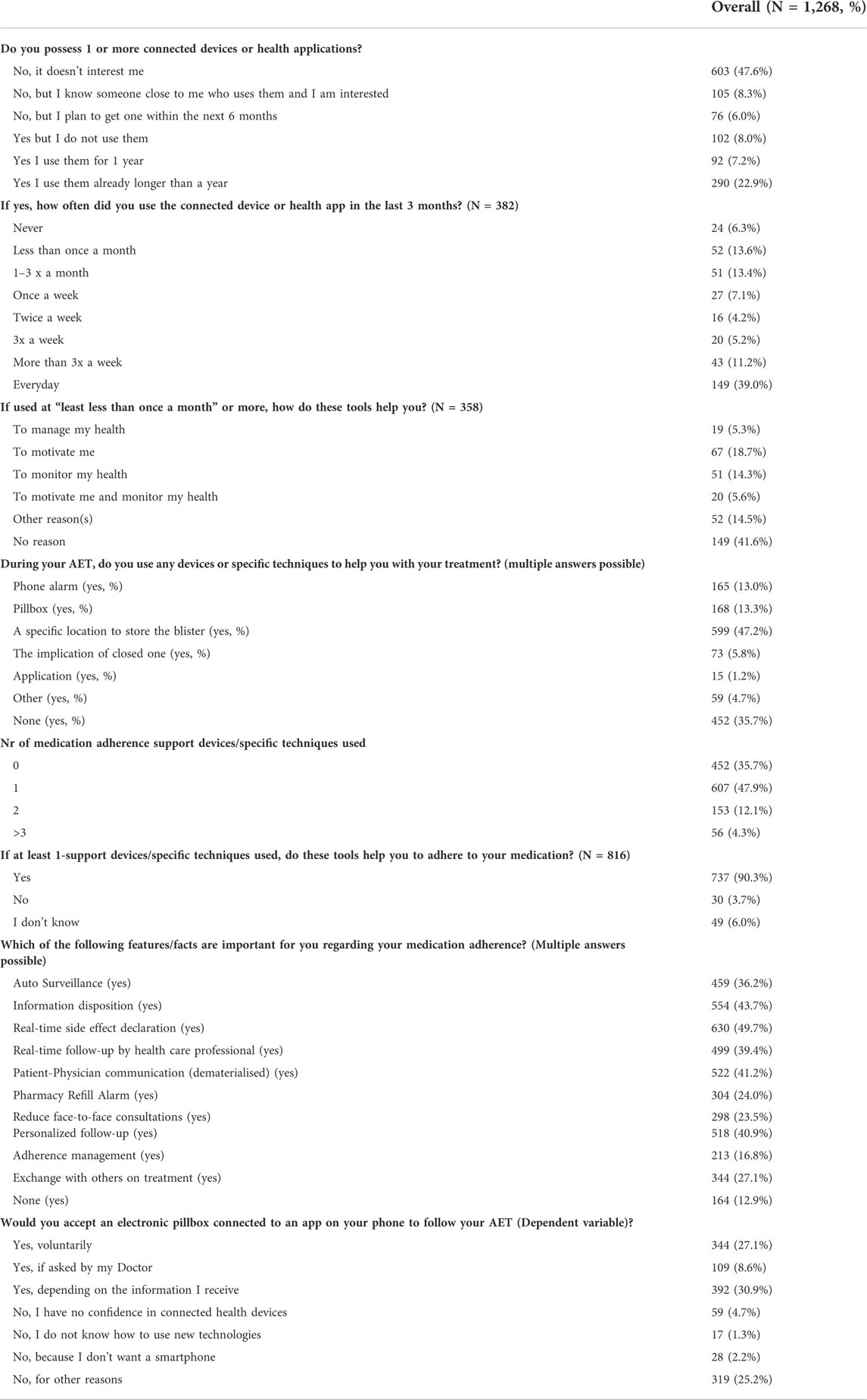
TABLE 2. Current eHealth use of BCS and acceptance to use a connected electronic blister with an app to manage AET (Seintinelles study, 2020).
3.2 Medication adherence support tool acceptance
Specific features that support medication adherence and are important for BC survivors to use real-time side effect declaration (49.7%), information disposition (43.7%) and dematerialised patient-physician communication (41.2%) among others. Finally, the study showed that 27.1% of the participants would voluntarily accept to use an electronic pillbox connected to an app on their phone to manage their AET.
3.3 Factors associated with BC survivors acceptance of an eHealth tool to manage AET
Table 3 illustrates the univariable logistic regression analysis, which analysed factors associated with accepting an electronic pillbox connected to an app to enhance AET among BC survivors. Some of the factors associated with accepting an electronic pillbox connected to an app were age (OR = 0.96, 95% CI 0.95, 0.98), being married (OR = 1.43, 95% CI 1.00, 2.02), retired (OR = 0.53, 95% CI 0.39, 0.71), taking regular medication for other diseases (OR = 0.34, 95% CI 0.17, 0.67) and using more than one support tool for AET adherence (OR = 1.53, 95%CI 0.18, 0.67).
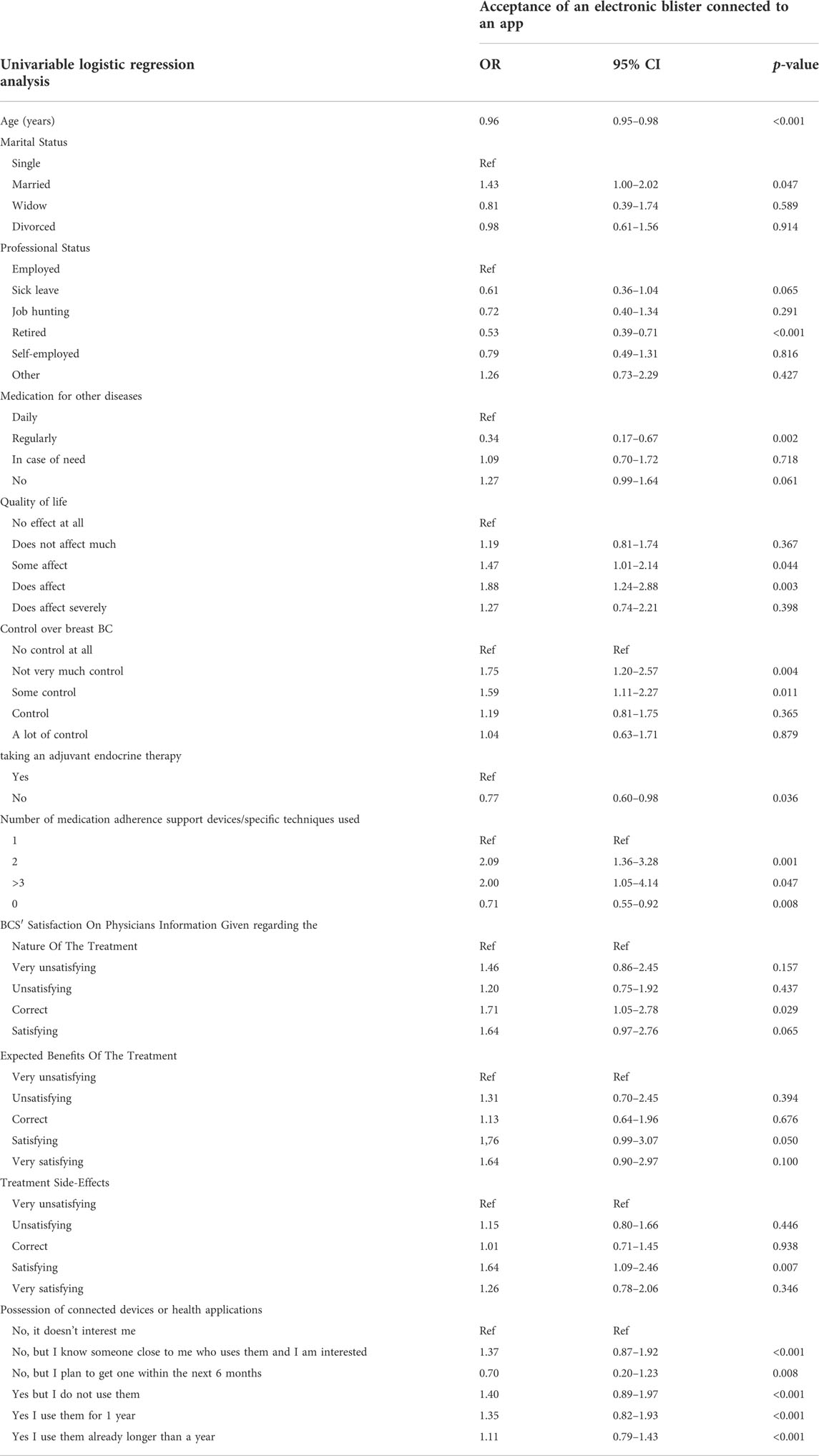
TABLE 3. Factors associated with accepting an eHealth tool to manage OHT in BCS (Seintinelles study, 2020).
Figure 1 highlights the stepwise multivariable logistic regression, presenting factors that are significantly associated with accepting an electronic pillbox connected to an app to enhance AET among BC survivors. The final adjusted model includes ‘Age’, ‘Medication intake for other diseases’, ‘Number of medication adherence support devices used’, ‘BC survivors satisfaction on physicians information given on expected benefits of the treatment’ and ‘Possession of connected devices or health applications’. We performed both forward and backward stepwise regression and both methods selected the same variables.
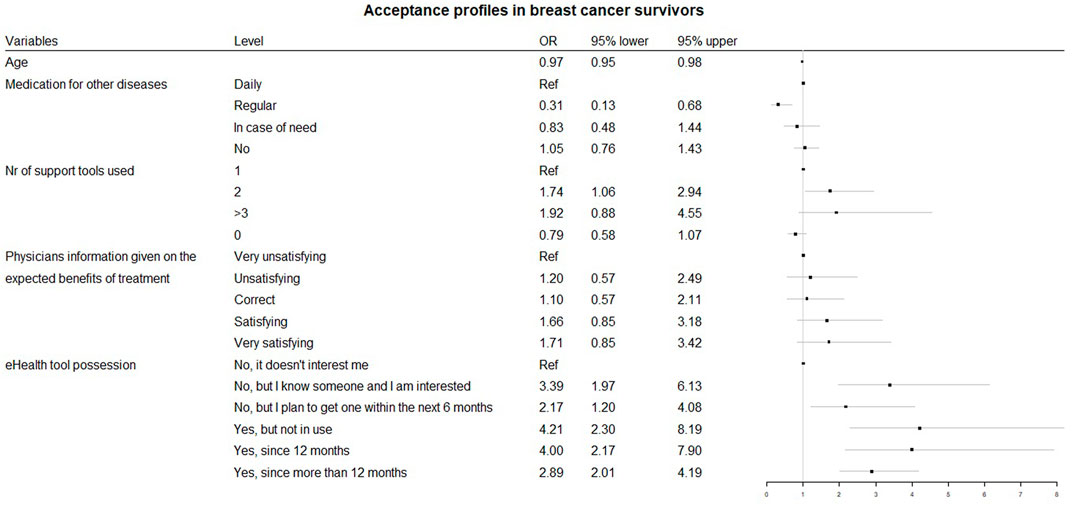
FIGURE 1. Acceptance profiles in survivors.
Hence, accepting an electronic pillbox connected to an app to enhance AET among BC survivors is inversely associated with age (OR = 0.97, 95% CI 0.95, 0.98) and the use of regular intake of other medication compared to no other medication intake (OR = 0.31, 95% CI 0.13, 0.68) (Figure 1). Using at least two medication adherence support tools increases the odds of accepting an electronic pillbox connected to an app to enhance AET among BC survivors (OR = 1.74, 95% CI 1.06, 2.94). Finally, BC survivors using connected devices for more than a year is 2.89 times (95% CI 2.01, 4.19) more likely to accept an eHealth tool to enhance AET compared to those that do not possess or are not interested in connected devices or health applications.
4 Discussion
This study investigated differences in BC survivors that accept an electronic pillbox connected to an app to enhance AET with those who do not.
Drewes et al. analysed the correlation between sociodemographic factors, the health status of BC patients and the willingness to use the Internet and apps (Drewes et al., 2016). They found that decisive factors influencing BC patients’ willingness to use new communication technologies are younger, have a large number of people per household, and a short time since breast cancer diagnosis. Other commonly reported barriers to medication adherence across diseases, patient beliefs/perceptions, comorbidities and poor patient–provider communication among others (Konstantinou et al., 2020). We found similar results and add to the current knowledge that polypharmacy positively effects acceptance of a medication adherence enhancing eHealth technology. Furthermore, we found that those patients that have already created an AET adherence habit/technique or are willing to use a smartphone or health applications are more likely to use an AET enhancing eHealth tool. Similar eHealth acceptance trends can be found for patients with cardiometabolic diseases, mental health disorders, infectious diseases (Talal et al., 2019; AshaRani et al., 2021; Gire et al., 2021).
In our study, we found that at the time of the survey, only 1.2% actively used an app yet 67% of the BC survivors would accept to use the proposed electronic pillbox connected to an app to enhance their AET. As Car et al. mentioned, eHealth is the future of medications management in terms of personalisation, monitoring and adherence (Car et al., 2017). To date, digitally delivered interventions including components such as medication and condition education, motivational interviewing, reinforcement and motivational messages led to improvements in medication adherence (Hadji et al., 2013; Nieuwlaat et al., 2014; Finitsis et al., 2019; Rosenberg et al., 2020; Pouls et al., 2021). In addition, qualitative papers showed that patients are ready and willing to integrate eHealth technologies into their daily life to monitor and enhance their health status and medication intake (Currie et al., 2015; Goetzinger et al., 2020). Yet, the challenge we face is to conceive effective eHealth intervention for end-users and implement them into the healthcare sector (Car et al., 2012). Thus integrating patients into the development phase of these eHealth technologies is key to creating feasible tools for the end-user that are implementable into the healthcare setting (Ross et al., 2016; Bauquier et al., 2017; Pannard et al., 2020; Aguayo et al., 2021).
Understanding the disease and/or patient profiles will allow personalising healthcare in the future. Characterising patient groups will allow defining new strategies for individual patients benefiting their needs to optimise health outcomes. Recent research, using profiling principles, found that healthcare for patients with cardiometabolic disease could benefit from more targeted and tailored strategies for the prevention of cardiometabolic diseases at a population level (Fagherazzi et al., 2021). Eventually, post-acute treatment for BC survivors using a medication adherence enhancing eHealth technology can move from a “one-size-fits-all” vision to a tailored follow-up strategy, personalizing care to each BC survivor.
This study evaluated the association between BC survivors characteristics and the acceptance of an eHealth intervention among BC survivors. Hence, the results produced will be fundamental when conceiving an eHealth support tool to enhance AET among BC survivors. Using patient acceptance profiling strategies will allow them to provide them with personalised care and develop effective, sustainable, and implementable eHealth support tools. Future studies should have a closer look into the specific features of such an AET support tool, examine the acceptable time point(s) of intervention and evaluate the implication of HCP. In addition, implementation strategies to adopt these eHealth technologies into the healthcare system need to be investigated.
4.1 Limitations
The present study entails several limitations. Also, the present study deals with selection bias, as the Seintinelles platform only includes volunteering members. Meaning the participants showed interest in the study topic, also we observed a high educational level among the study sample. The present study thus provides only a snapshot of characteristics for accepting eHealth tools. Some categories have a small sample and should be regarded with caution.
5 Conclusion
This study found that although 1.2% currently used and health related app over two thirds would accept to use a medication adherence enhancing eHealth technology to enhance their AET. BC survivors are accepting to and willing to be supported during their AET, yet, the medication adherence enhancing eHealth technology needs to fit their needs and profiles. Thus, understanding acceptance profiles among BC survivors is fundamental for conceiving an effective medication adherence enhancing eHealth technology enhancing AET among BC survivors.
Data availability statement
The datasets presented in this article are not readily available because participants could be identifiable. The included tables provide the anonymized and summarized data. Requests to access the datasets should be directed to the corresponding author, Y2F0aGVyaW5lLmdvZXR6aW5nZXJAZ21haWwuY29t.
Ethics statement
The studies involving human participants were reviewed and approved by National Commission for Information and Freedoms (Commission nationale de l’informatique et des libertés, CNIL: 1955704) and the Sud-EST II data protection committee (Comité de Protection des données, Numéro EudraCT: 2020-A00665-34). The patients/participants provided their written informed consent to participate in this study.
Author contributions
CG contributed to the study conception and design, data analysis and interpretation, and manuscript preparation. CG, CA, MP, and LH contributed to the study conception and design. AS and BV contributed to the data analysis and interpretation. GF contributed to manuscript preparation and editing. All authors contributed to the manuscript review.
Funding
CG was supported by a PhD grant financed by the Action LIONS Vaincre le Cancer.
Acknowledgments
The authors are thankful to all the volunteering participants from the Seintinelles platform, as well as the staff working at Seintinelles. We thank the Luxembourg Institute of Health for having provided the possibility to conduct the present research project.
Conflict of interest
BV was employed by AARDEX Group.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Supplementary Material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fphar.2022.889695/full#supplementary-material
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Abbreviations
BC, Breast Cancer; AET, Adjuvant endocrine therapy.
References
Aguayo, G. A., Goetzinger, C., Scibilia, R., Fischer, A., Till, S., Tran, V.-T., et al. (2021). Methods to generate innovative research ideas and improve patient and public involvement in modern epidemiological research: Review, patient viewpoint, and guidelines for implementation of a digital cohort study. J. Med. Internet Res. 23 (12), e25743. doi:10.2196/25743
Ahmed, I., Ahmad, N. S., Ali, S., George, A., Danish, H. S., Uppal, E., et al. (2018). Medication adherence apps: Review and content analysis. JMIR Mhealth Uhealth 6 (3), e62. doi:10.2196/mhealth.6432
AshaRani, P. V., Jue Hua, L., Roystonn, K., Siva Kumar, F. D., Peizhi, W., Ying Jie, S., et al. (2021). Readiness and acceptance of eHealth services for diabetes care in the general population: Cross-sectional study. J. Med. Internet Res. 23 (9), e26881. doi:10.2196/26881
Bauquier, C., Pannard, M., and Préau, M. (2017). The seintinelles: An innovative approach to promoting community-based research and sustaining health democracy in oncology. Sante publique 29 (4), 547–550. doi:10.3917/spub.174.0547
Bouhnik, A.-D., Bendiane, M.-K., Cortaredona, S., Sagaon Teyssier, L., Rey, D., Berenger, C., et al. members of VICAN Group (2015). The labour market, psychosocial outcomes and health conditions in cancer survivors: Protocol for a nationwide longitudinal survey 2 and 5 Years after cancer diagnosis (the VICAN survey). BMJ Open 5 (3), e005971. doi:10.1136/bmjopen-2014-005971
Car, J., Huckvale, K., and Hermens, H. (2012). Telehealth for long term conditions. BMJ 344, e4201. doi:10.1136/bmj.e4201
Car, J., Tan, W. S., Huang, Z., Sloot, P., and Franklin, B. D. (2017). eHealth in the future of medications management: Personalisation, monitoring and adherence. BMC Med. 15 (1), 73. doi:10.1186/s12916-017-0838-0
Currie, M., Philip, L. J., and Roberts, A. (2015). Attitudes towards the use and acceptance of eHealth technologies: A case study of older adults living with chronic pain and implications for rural healthcare. BMC Health Serv. Res. 15, 162. doi:10.1186/s12913-015-0825-0
Davies, C., Godwin, J., Gray, R., Clarke, M., Cutter, D., Darby, S., et al. Early Breast Cancer Trialists’ Collaborative Group (EBCTCG) (2011). Relevance of breast cancer hormone receptors and other factors to the efficacy of adjuvant tamoxifen: Patient-level meta-analysis of randomised trials. Lancet 378 (9793), 771–784. doi:10.1016/s0140-6736(11)60993-8
De Geest, S., Zúñiga, F., Brunkert, T., Deschodt, M., Zullig, L. L., Wyss, K., et al. (2020). Powering Swiss health care for the future: Implementation science to bridge ‘the valley of death. Swiss Med. Wkly. 150, w20323. doi:10.4414/smw.2020.20323
Drewes, C., Kirkovits, T., Schiltz, D., Schinkoethe, T., Haidinger, R., Goldmann-Posch, U., et al. (2016). EHealth acceptance and new media preferences for therapy assistance among breast cancer patients. JMIR cancer 2 (2), e13. doi:10.2196/cancer.5711
Fagherazzi, G., Zhang, L., Aguayo, G., Pastore, J., Goetzinger, C., Fischer, A., et al. (2021). Towards precision cardiometabolic prevention: Results from a machine learning, semi-supervised clustering approach in the nationwide population-based ORISCAV-LUX 2 study. Sci. Rep. 11 (1), 16056. doi:10.1038/s41598-021-95487-5
Finitsis, D. J., Vose, B. A., Mahalak, J. G., and Salner, A. L. (2019). Interventions to promote adherence to endocrine therapy among breast cancer survivors: A meta-analysis. Psychooncology. 28 (2), 255–263. doi:10.1002/pon.4959
Gire, N., Caton, N., McKeown, M., Mohmed, N., Duxbury, J., Kelly, J., et al. (2021). Care co-ordinator in my pocket': A feasibility study of mobile assessment and therapy for psychosis (TechCare). BMJ open 11 (11), e046755. doi:10.1136/bmjopen-2020-046755
Goetzinger, C. B., Vrijens, G., Fagherazzi, M., Preau, J., Mancini, M. K., Ben-Diane, , et al. (2021). “Beliefs and attitudes towards an ehealth tool to improve medication adherence in breast cancer survivors” in In Abstracts of the 24th Annual Meeting of ESPACOMP, the International Society for Medication Adherence, November 10–20, 2020. Int J Clin Pharm 43, 286–308. doi:10.1007/s11096-020-01213-Y
Hadji, P., Blettner, M., Harbeck, N., Jackisch, C., Lück, H-J., Windemuth-Kieselbach, C., et al. (2013). The patient’s Anastrozole compliance to therapy (pact) program: A randomized, in-practice study on the impact of a standardized information program on persistence and compliance to adjuvant endocrine therapy in postmenopausal women with early breast cancer. Ann. Oncol. 24, 1505–1512. doi:10.1093/annonc/mds653
Huiart, L., Dell'Aniello, S., and Suissa, S. (2011). Use of tamoxifen and aromatase inhibitors in a large population-based cohort of women with breast cancer. Br. J. Cancer 104 (10), 1558–1563. doi:10.1038/bjc.2011.140
Hurtado-de-Mendoza, A., Jensen, R. E., Jennings, Y., and Sheppard, V. B. (2017). Understanding breast cancer survivors' beliefs and concerns about adjuvant hormonal therapy: Promoting adherence. J. Cancer Educ. 33, 436–439. doi:10.1007/s13187-017-1180-0
International Agency for Research on Cancer, European Network of Cancer Registries, Joint Reserach Center. 2020 Cancer incidence and mortality in EU-27 countries 2020. Available from: https://ec.europa.eu/jrc/en/news/2020-cancer-incidence-and-mortality-eu-27-countries. Accessed date 22/07/2020.
Kantsiper, M., McDonald, E. L., Geller, G., Shockney, L., Snyder, C., and Wolff, A. C. (2009). Transitioning to breast cancer survivorship: Perspectives of patients, cancer specialists, and primary care providers. J. General Intern. Med. 24 (2), 459–466. doi:10.1007/s11606-009-1000-2
Kardas, P., Pawel, L., and Matyjaszczyk, M. (2013). Determinants of patient Adherence: A review of systematic reviews. Front. Pharmacol. 4, 91. doi:10.3389/fphar.2013.00091
Kini, V., and Michael Ho, P. (2018). Interventions to improve medication adherence: A review. JAMA J. Am. Med. Assoc. 320, 2461–2473. doi:10.1001/jama.2018.19271
Konstantinou, P., Kassianos, A. P., Georgiou, G., Panayides, A., Papageorgiou, A., Almas, I., et al. (2020). Barriers, facilitators, and interventions for medication adherence across chronic conditions with the highest non-adherence rates: A scoping review with recommendations for intervention development. Transl. Behav. Med. 10 (6), 1390–1398. doi:10.1093/tbm/ibaa118
Lu, C. Y., Zhang, F., Wagner, A. K., Nekhlyudov, L., Earle, C. C., Callahan, M., et al. (2018). Impact of high-deductible insurance on adjuvant hormonal therapy use in breast cancer. Breast Cancer Res. Treat. 171 (1), 235–242. doi:10.1007/s10549-018-4821-z
Nieuwlaat, R., Wilczynski, N., Navarro, T., Hobson, N., Jeffery, R., Keepanasseril, A., et al. (2014). Interventions for enhancing medication adherence. Cochrane Database Syst. Rev. 2014 (11), Cd000011. doi:10.1002/14651858.CD000011.pub4
Pannard, M., Bauquier, C., Bassoleil, L., Sablone, L., Jacob, G., Reyal, F., et al. (2020). Citizens who volunteer as participants for cancer research-results of the Seintinelles Barometer 2018. Bull. Cancer 107 (3), 333–343. doi:10.1016/j.bulcan.2019.11.012
Partridge, A. H., Wang, P. S., Winer, E. P., and Avorn, J. (2003). Nonadherence to adjuvant tamoxifen therapy in women with primary breast cancer. J. Clin. Oncol. 21 (4), 602–606. doi:10.1200/JCO.2003.07.071
Pistilli, B., Paci, A., Ferreira, A. R., Di Meglio, A., Poinsignon, V., Bardet, A., et al. (2020). Serum detection of nonadherence to adjuvant tamoxifen and breast cancer recurrence risk. J. Clin. Oncol. 38 (24), 2762–2772. doi:10.1200/JCO.19.01758
Pouls, B. P. H., Vriezekolk, J. E., Bekker, C. L., Linn, A. J., van Onzenoort, H. A. W., Vervloet, M., et al. (2021). Effect of interactive ehealth interventions on improving medication adherence in adults with long-term medication: Systematic review. J. Med. Internet Res. 23 (1), e18901. doi:10.2196/18901
Ringwald, J., Marwedel, L., Junne, F., Ziser, K., Schäffeler, N., Gerstner, L., et al. (2017). Demands and needs for psycho-oncological eHealth interventions in women with cancer: Cross-sectional study. JMIR cancer 3 (2), e19. doi:10.2196/cancer.7973
Rosenberg, S. M., Petrie, K. J., Stanton, A. L., Ngo, L., Finnerty, E., and Partridge, A. H. (2020). Interventions to enhance adherence to oral antineoplastic agents: A scoping review. J. Natl. Cancer Inst. 112 (5), 443–465. doi:10.1093/jnci/djz244
Ross, J., Stevenson, F., Lau, R., and Murray, E. (2016). Factors that influence the implementation of E-health: A systematic review of systematic reviews (an update). Implement. Sci. 11 (1), 146. doi:10.1186/s13012-016-0510-7
Sabaté, E.World Health Organization (2003). Adherence to long-term therapies: Evidence for action. Geneva, Switzerland: World Health Organization.
Talal, A. H., McLeod, A., Andrews, P., Nieves-McGrath, H., Chen, Y., Reynolds, A., et al. (2019). Patient reaction to telemedicine for clinical management of hepatitis C virus integrated into an opioid treatment program. Telemed. J. E. Health. 25 (9), 791–801. doi:10.1089/tmj.2018.0161
Touillaud, M., Fournier, B., Pérol, O., Delrieu, L., Maire, A., Belladame, E., et al. (2021). Connected device and therapeutic patient education to promote physical activity among women with localised breast cancer (DISCO trial): Protocol for a multicentre 2×2 factorial randomised controlled trial. BMJ Open 11 (9), e045448. doi:10.1136/bmjopen-2020-045448
Vrijens, B., De Geest, S., Hughes, D. A., Przemyslaw, K., Demonceau, J., Ruppar, T., et al. (2012). A new taxonomy for describing and defining adherence to medications. Br. J. Clin. Pharmacol. 73 (5), 691–705. doi:10.1111/j.1365-2125.2012.04167.x
World Health Organization (2022) World health organization - regional office for the eastern mediterranean, Available at: http://www.emro.who.int/health-topics/ehealth/. Accessed July 25, 2022.
Keywords: medication adherence, medication adherence enhancing interventions, eHealth, breast cancer, user-centered design, patient adherence
Citation: Goetzinger C, Alleaume C, Schritz A, Vrijens B, Préau M, Fagherazzi G and Huiart L (2022) Analysing breast cancer survivors’ acceptance profiles for using an electronic pillbox connected to a smartphone application using Seintinelles, a French community-based research tool. Front. Pharmacol. 13:889695. doi: 10.3389/fphar.2022.889695
Received: 04 March 2022; Accepted: 05 September 2022;
Published: 27 September 2022.
Edited by:
Tamas Agh, Syreon Research Institute, HungaryReviewed by:
Ivana Tadic, University of Belgrade, SerbiaKabelo Leonard Mauco, Botho University, Botswana
Copyright © 2022 Goetzinger, Alleaume, Schritz, Vrijens, Préau, Fagherazzi and Huiart. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Catherine Goetzinger, Y2F0aGVyaW5lLmdvZXR6aW5nZXJAZ21haWwuY29t